Embed Size (px)
Citation preview

2016Blue Medicare Rx (PDP)
(PDP)Enrollment kit
Prescription drug coverage forMedicare beneficiaries
Y0079_7237 CMS Accepted 09052015U5073a, 8/15

Thank you for your interest in Blue Medicare Rx (PDP).This kit has all the information you need to enroll today.
ContentsYour guide to Blue Medicare Rx (PDP) .................. 3
Eligibility & enrollment .................................................... 7
Important information ..................................................... 9
Summary of benefits ........................................................ 19
Enrollment information ................................................... 31
Disclaimers .......................................................................... 53
What you get+ Extensive list of covered prescription drugs
+ Additional savings with our Preferred Pharmacy Network
+ Virtually no paperwork when you use a network pharmacy
+ Enhanced plan has no deductible and has gap coverage when you purchase preferred generic drugs
Important dates+ October 15, 2015 First day you can enroll in a Medicare Part D plan for 2016, or the first day you can elect to switch to
a different Medicare Part D plan (unless you qualify for a special election period).
+ December 7, 2015 Last day you can enroll in a Medicare Part D plan for 2016, or the last day you can elect to
switch to a different Medicare Part D plan (unless you qualify for a special election period).
+ January 1, 2016 First day coverage begins (if you join a plan or switch plans by December 7, 2015).
Note:Formulary and pharmacy networks may change at any time. You will receive notice when necessary.
The information described in this brochure is for 2016 and may change on January 1, 2017. Blue Cross and Blue Shield of North Carolina is a PDP plan with a Medicare contract. Enrollment inBlue Cross and Blue Shield of North Carolina depends on contract renewal. Benefits, formulary,pharmacy network, premium and/or copayments/coinsurance may change on January 1 of each year.
PAGE 2 of 56

(PDP)
Medicare prescription drug coverage helps cover your drug costs
Designed to make prescriptions more affordableBlue Cross and Blue Shield of North Carolina (BCBSNC) offers Medicare prescription drug coverage to help you pay for prescription drugs at local and network pharmacies and through mail order. Sometimes referred to as Medicare Part D, Medicare prescription drug coverage must be approved by Medicare and provided through private companies like BCBSNC. Coverage is designed to make filling prescriptions more affordable.
Preferred Pharmacy NetworkAt BCBSNC, we offer two Medicare Prescription Drug plans: Blue Medicare Rx (PDP) Standard and Blue Medicare Rx (PDP) Enhanced. BCBSNC’s Preferred Pharmacy Network is designed to help save you money on your prescription copayments. This select network of national and local independent pharmacies has worked with BCBSNC to get you the savings and value that you are looking for by offering lower costs and better value from your prescription plan, without sacrificing convenience.
Filling your prescriptionsOur pharmacy network includes most national
chains as well as local pharmacies around the state. You can save even more time and avoid the line by using our mail order pharmacy services. Your prescriptions will be mailed to your door and we handle the paperwork for you. When you enroll in one of our Medicare Prescription Drug (Part D) plans, we verify enrollment with Medicare, and Medicare helps pay your prescription costs. Please review the preferred and non-preferred charts to understand our Part D benefits.
Eligibility and types of coverage for beneficiariesEveryone who is entitled to Medicare benefits under Part A, or enrolled in Part B, is eligible for this coverage; however, you are not enrolled automatically. You must join a plan to receive the coverage.1 This voluntary program is coverage that you may choose to purchase annually.
Unlike Medicare Part A and Part B, this coverage is available solely through private companies like BCBSNC. Medicare requires that all companies that provide Medicare Part D coverage offer the Medicare standard coverage. Companies may also choose to provide enhanced coverage, like the Blue Medicare Rx (PDP) Enhanced plan.
Footnotes:1 You must join a plan to receive the coverage unless you are eligible for both Medicare and Medicaid.
Contact your State Medicaid or medical assistance office if you have questions about your eligibility.
PAGE 3 of 56

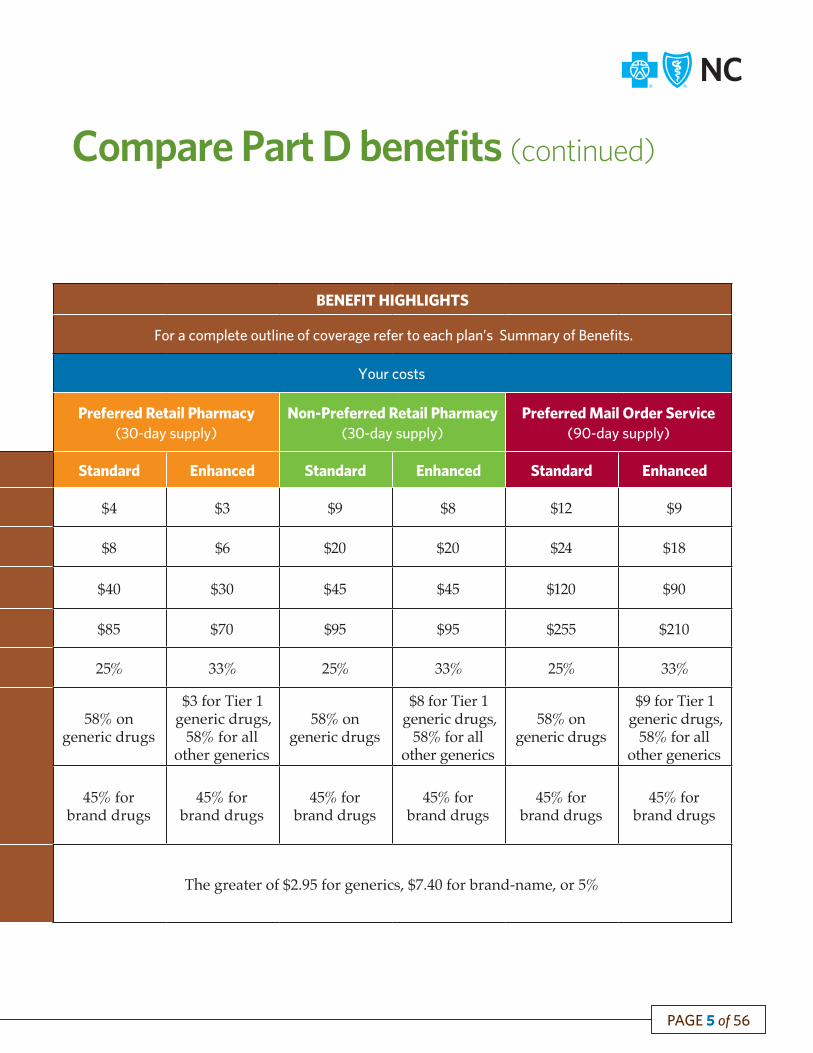
BENEFIT HIGHLIGHTS
For a complete outline of coverage refer to each plan’s Summary of Benefits.
Your costs
Preferred Retail Pharmacy(30-day supply)
Non-Preferred Retail Pharmacy(30-day supply)
Preferred Mail Order Service(90-day supply)
Initial Coverage Stage Standard Enhanced Standard Enhanced Standard Enhanced
Tier 1 – Preferred generic $4 $3 $9 $8 $12 $9
Tier 2 – Generic $8 $6 $20 $20 $24 $18
Tier 3 – Preferred brand $40 $30 $45 $45 $120 $90
Tier 4 – Non-preferred brand $85 $70 $95 $95 $255 $210
Tier 5 – Specialty 25% 33% 25% 33% 25% 33%
Coverage Gap Stage (after drug costs reach $3,310)
58% on generic drugs
$3 for Tier 1 generic drugs,
58% for all other generics
58% on generic drugs
$8 for Tier 1 generic drugs,
58% for all other generics
58% on generic drugs
$9 for Tier 1 generic drugs,
58% for all other generics
45% for brand drugs
45% for brand drugs
45% for brand drugs
45% for brand drugs
45% for brand drugs
45% for brand drugs
Catastrophic (after you have paid $4,850 out-of-pocket)
The greater of $2.95 for generics, $7.40 for brand-name, or 5%
MEMBER BENEFITS
BCBSNC offers 2 Part D prescriptions plans:
Standard Enhanced
Premium2 $68.40/month $107.40/monthDeductible $225 $0
Compare Part D benefits
(PDP)
PAGE 4 of 56
Our Preferred network includes many national chains and local pharmacies. Please see our pharmacy list at bcbsnc.com/medicare to find a pharmacy near you.
Please refer to the chart to review our Blue Medicare Rx (PDP) plans. The total amount you spend on prescription drugs increases during the calendar year as you move through some or all of the phases of coverage. Remember, you must always present your plan’s member ID card to fill your prescriptions. Note: For members who qualify for low-income assistance, benefits may vary.
Note: Limitations, copayments and restrictions may apply. The benefit information provided is a brief summary, not a complete description of benefits. For more information, contact the plan.
Footnotes:2 If you have Medicare Part B, you must continue to pay your Medicare Part B premium, if not otherwise paid for under Medicaid, or by another third party.
BENEFIT HIGHLIGHTS
For a complete outline of coverage refer to each plan’s Summary of Benefits.
Your costs
Preferred Retail Pharmacy(30-day supply)
Non-Preferred Retail Pharmacy(30-day supply)
Preferred Mail Order Service(90-day supply)
Initial Coverage Stage Standard Enhanced Standard Enhanced Standard Enhanced
Tier 1 – Preferred generic $4 $3 $9 $8 $12 $9
Tier 2 – Generic $8 $6 $20 $20 $24 $18
Tier 3 – Preferred brand $40 $30 $45 $45 $120 $90
Tier 4 – Non-preferred brand $85 $70 $95 $95 $255 $210
Tier 5 – Specialty 25% 33% 25% 33% 25% 33%
Coverage Gap Stage (after drug costs reach $3,310)
58% on generic drugs
$3 for Tier 1 generic drugs,
58% for all other generics
58% on generic drugs
$8 for Tier 1 generic drugs,
58% for all other generics
58% on generic drugs
$9 for Tier 1 generic drugs,
58% for all other generics
45% for brand drugs
45% for brand drugs
45% for brand drugs
45% for brand drugs
45% for brand drugs
45% for brand drugs
Catastrophic (after you have paid $4,850 out-of-pocket)
The greater of $2.95 for generics, $7.40 for brand-name, or 5%
Compare Part D benefits (continued)
PAGE 5 of 56

(PDP)
Prescription drugs covered by the plans
Here are three ways to find out if your prescriptions are
covered by our formulary
Search online for specific drugs by visiting the Blue Medicare Rx (PDP) section of bcbsnc.com/medicare(You may also download the complete formulary in PDF format)
Call or visit your local Authorized Sales Representative
Call 1-800-661-5518, 7 days a week, 8 a.m. – 8 p.m. and speak to an authorized agentHearing and speech impaired (TTY/TDD) users call 1-800-922-3140Representatives can help you determine whether or not a specific drug is covered
1
2
3
Extensive network of pharmacies makes getting your medications easyExcept under certain non-routine circumstances, you need to use a network pharmacy to obtain the full benefit of your Medicare Part D plan. Quantity limitations and restrictions may apply. BCBSNC offers an extensive network of pharmacies of the following types: local retail, national chains, mailorder, extended supply, home infusion, long-term care or Indian Health Service/Tribal/Urban Indian Health Program (I/T/U) pharmacies.
You can use our mail order pharmacyYou can save even more time and avoid the lineby using our mail order pharmacy services. Your prescriptions will be mailed to your door and we handle the paperwork for you.
Many of the most commonly used drugs are coveredThe Blue Medicare Rx (PDP) Enhanced plan and the Blue Medicare Rx (PDP) Standard plan have a formularies that list the generic, brand-name and specialty drugs covered by the plans. The formularies cover many drugs eligible for coverage under Medicare Part D .
Medicare Part D plans do not cover certain drugs, or classes of drugs, that are excluded by law, such as over-the-counter medications and prescription vitamins.
PAGE 6 of 56

(PDP)
Eligibility requirements for enrolling in a planYou can join a Medicare Part D plan any time during your initial enrollment period for Medicare. Generally, a Medicare beneficiary’s initial enrollment is a seven-month period: three months prior to becoming Medicare eligible, the month you become Medicare eligible, and three months following the month you become Medicare eligible.
Eligibility for beneficiariesEveryone who is entitled to Medicare benefits under Part A, or enrolled in Part B, is eligible for this coverage; however, you are not enrolled automatically. This voluntary program is coverage that you may choose to purchase annually. This product is available to Medicare beneficiaries living in North Carolina.
Additional enrollment criteriaYou may enroll in only one Part D plan at a time. If you are enrolled in a Medicare Advantage plan, your enrollment in either of the PDP plans from BCBSNC may automatically disenroll you from your Medicare Advantage plan, and re-enroll you in Original Medicare for medical coverage. Check with your plan for more information.
Changing Medicare Part D plansCongress designed Medicare prescription drug coverage to work on an annual enrollment cycle. This means that each year you will have the option to remain with your existing Medicare Part D plan, or change plans between October 15 and December 7.
You may also have another opportunity during the year to switch plans under limited circumstances. For example, if you move out of your plan’s service area, you will have an opportunity to choose another plan that serves your new area. Please contact BCBSNC if you would like more information about other situations in which you may qualify for coverage, or changes in coverage outside the annual enrollment cycle.
Annual enrollment periodOctober 15 through December 7 of every year
Special enrollment period If you are enrolling at a different time of year, theeffective date of your coverage will depend onyour situation, and whether or not you qualify fora special election period.
PAGE 7 of 56

Enrollment is easy with these simple steps Choose a plan
Before you select a plan, gather any documentation you may have on your prescription drug purchases over the past year. This information will help you determine how much you might save with a Medicare Part D plan. Then you can choose a plan that best fits your needs and your budget.
Complete the enrollment form + Fill out the enrollment form. You must complete one enrollment form per person. + Sign and date the form.
+ Check the appropriate box beside the plan you choose.
+ Return the form in the envelope provided.
You will be enrolled in the Medicare Part D plan you select, and Medicare will be informed that you have enrolled.
3
4
1
2
Option – Enroll onlineIf you want to enroll online, please visit bcbsnc.com/medicare.
Enrollment confirmation You will receive acknowledgement of your enrollment request via mail.
Note: There are some limits set by the Federal Government on when and how often Medicare beneficiaries may enroll in, or change, Medicare Advantage and Medicare Prescription Drug plans. For more information on these enrollment rules, refer to “Enrollment Periods” on page 7, or call the BCBSNC Sales Department for more information.
Blue Cross and Blue Shield of North Carolina
Phone 1-800-661-5518
TTY/TDD 1-800-922-3140
Hours 7 days a week, 8 a.m. – 8 p.m.
Online bcbsnc.com/medicare
PAGE 8 of 56

Important informationPenalties for late enrollment
When do penalties apply?If you were eligible for Medicare on or prior to January 1, 2006, and did not enroll in a Medicare Part D plan or Medicare Advantage Prescription Drug plan by May 15, 2006, you may have to pay a penalty for late enrollment. This penalty will not apply to Medicare beneficiaries who have equal or better prescription drug benefits through their employer or another plan. As of January 1, 2009, these penalties no longer apply to Medicare individuals with Low Income Subsidy (LIS).
Financial assistance
Financial assistance availablePeople with limited incomes may qualify for Extra Help to pay for their prescription drug costs. If you qualify, Medicare could pay for up to seventy-five (75) percent or more of your drug costs, including monthly prescription drug premiums, annual deductibles, and coinsurance. Additionally, those who qualify will not be subject to the coverage gap or a late enrollment penalty. Many people are eligible for these savings and don’t even know it. For more information about this Extra Help, see the contact information below.
Here are three ways to find out if you qualify to receive
financial assistance
Call Medicare at 1-800-MEDICARE (1-800-633-4227), 24 hours a day/ 7 days a weekHearing and speech impaired (TTY/TDD) users call 1-877-486-2048Or, visit Medicare’s website www.medicare.gov and click the ”Get help with costs” link
Call the Social Security Administration at 1-800-772-1213 between 7 a.m. and 7 p.m., Mon. through Fri.Hearing and speech impaired (TTY/TDD users) call 1-800-325-0778
Call your State Medicaid Office
1
2
3
PAGE 9 of 56

Important informationCoverage determination
What is a coverage determination?When we make a coverage determination, we are making a decision about whether or not to provide or pay for a Part D drug and what your share of the cost is for the drug (also see the description of the exceptions process on page 12). You must contact us if you would like to request a coverage determination, including an exception. You cannot request an appeal if we have not issued a coverage determination.
Examples of when you may ask us for a coverage determination
If you are not getting a prescription drug that you believe may be covered by us.
If you have received a Part D prescription drug that you believe may be covered by us while you were a member, but we have refused to pay for the drug.
If you are being told that coverage for a Part D prescription drug that you have been getting will be reduced or stopped, and you believe you have special circumstances that should exclude you from the reduction/non-coverage.
If there is a limit on the quantity (or dose) of the drug, and you disagree with the requirement or dosage limitation.
If you bought a drug at a pharmacy that is not in our network, and you want to request reimbursement for the expense.
PAGE 10 of 56

Important informationCoverage determination (continued)
How do I make a request for coverage determination?Standard: To ask for a standard decision, you, your physician, or your appointed representative may call our Customer Service Department at the numbers listed below. You can also mail a written request to the below address.
Fast: To ask for a fast decision, you, your physician, or your appointed representative may call the Customer Service Department at the numbers listed below. You can also mail a written request to the below address.
Contact information
Phone 1-888-247-4142
TTY/TDD 1-888-247-4145
Hours 7 days a week, 8 a.m. – 8 p.m.
Mail BCBSNCPO Box 17509Winston-Salem, NC 27116-7509
Fax Request 1-888-446-8440
Note: You cannot ask for a fast decision on a request for coverage of a drug already purchased.
For some reviews, we may require a supporting statement from your doctor that explains why the drug you are asking coverage for is medically necessary.
After regular business hours, you should consult with a network pharmacy regarding your need for an emergency or temporary supply of medication until you can contact the Plan the next business day. You may also call our Customer Service Department and leave a message on the Part D After Hours Exception Request voicemail. Be sure to ask for a “fast,” “expedited,” or “24-hour” review.
When will I hear back with a decision?Standard: Generally, we must give you our decision no later than 72 hours after we have received your request, but we will make it sooner if your health condition requires.
Fast: If you get a fast review, we will give you our decision within 24 hours after you or your doctor ask for a fast review – sooner if your health requires.
PAGE 11 of 56

Important informationExceptions process
What is an exception request?Exception requests are a kind of coverage determination. You, your authorized representative, or your prescribing physician may request an exception to seek coverage of a drug that:
+ Is not on the formulary (list of drugs the plan covers)
+ Requires prior authorization+ Has quantity limitations
Example of an exception request:If the Plan’s formulary does not include a drug that you or your prescribing physician feel is necessary, then you or your prescribing physician may request an exception so that you may obtain coverage of this drug. If the Plan does not grant the requested exception, then you or your prescribing physician may file an appeal.
How do I make an exception request?You or your prescribing physician may request an exception to the coverage rules for your Medicare Prescription Drug plan. A specific form is not required for you to make an exception request. The request must include your prescribing physician’s statement that he/she has determined that the preferred drug either would not be as effective, or would have adverse effects for you.
For your convenience, forms are available at bcbsnc.com/content/medicare/member/index.htm
Contact information
Mail BCBSNCAttn: Part D Coverage DeterminationsPO Box 17509Winston-Salem, NC 27116-7509
Phone 1-888-247-4142
Physicians, call 1-888-298-7552
TTY/TDD 1-888-247-4145
Hours 7 days a week, 8 a.m. – 8 p.m.
When will I receive a decision on my exception request?If your exception request includes a formulary exception, or an exception from utilization management rules such as dosage or quantity limits, we must make our decision no later than 72 hours after we have received your doctor’s supporting statement. The supporting statement must explain why the drug you are asking for is medically necessary.
If you have asked for a fast or expedited exception request, we must make our decision no later than 24 hours after we get your doctor’s supporting statement.
You will be notified by phone, followed by a written notice, of our decision. If the decision is not in your favor, you have the right to appeal.
PAGE 12 of 56

Important informationAppeals process
What is an appeal?An appeal is your opportunity to request a redetermination of an adverse coverage determination, which includes denied exception requests.
Example of an appeal:If we deny your request for an exception to cover a non-formulary drug, then you may file an appeal of the denial. An appeal can only be filed after an exception has been requested and denied by the Plan.
How do I file an appeal?If you receive a coverage determination denial, you or your appointed representative, or your doctor, or other prescriber may file an appeal. A specific form is not required for you to file an appeal. An appeal must be filed within 60 calendar days of the date of a denial notice, and must be in writing, unless you are filing an expedited or fast appeal. You must submit it via mail, fax, or in person.
When will I receive a decision on my appeal?
We will perform a standard review of your appeal within seven calendar days of receipt of your appeal, or sooner, if your health requires. We will review requests for an expedited or fast appeal as soon as possible, but no later than 72 hours following our receipt of the request. An individual who was not involved with your original coverage determination will make a decision on your appeal.
You will receive a written response to your appeal. The decision on an expedited appeal will be provided by phone, followed by the written notice. If our decision is to deny the appeal, the notice will advise you of your right to submit your appeal to the Independent Review Entity (IRE), with instructions on how to do so. If we miss our time frames for claims adjudication, or review of the appeal, we will automatically forward the appeal to the IRE for a decision. There may be additional levels of appeal available to you. We will inform you of your additional rights in the notice, or you may refer to your Evidence of Coverage for further details.
Contact information
Mail BCBSNCAttn: Medicare Appeals & GrievancesPO Box 17509Winston-Salem, NC 27116-7509
Fax 1-888-375-8836 or 1-336-794-8836
In Person
BCBSNC5660 University Pkwy.Winston-Salem, NC 27105
Email [email protected]
PAGE 13 of 56

Important informationGrievance process
What is a grievance?A grievance is a complaint that you may file if you are dissatisfied with the Plan, or a contracted provider for reasons other than a decision on a coverage determination. Grievances also include complaints regarding the timeliness, appropriateness, access to, or setting of a covered prescription drug.
Example of a grievance:If you are dissatisfied with the service you received from a pharmacist or plan representative, then you could file a grievance.
How do I file a grievance?The grievance must be filed within 60 days after the event or incident that caused you to be dissatisfied. A specific form is not required for you to file a grievance. You or your appointed representative may file a grievance via the phone, by mail, fax, or in person.
When will I receive a decision on my grievance?The resolution of a grievance will be made as quickly as your concern requires, but no more than 30 calendar days after our receipt of the grievance. We may extend the time frame by up to 14 calendar days if you request the extension, or if we justify a need for additional information and the delay is in your best interest.
If you request a written response to an oral grievance, one will be provided within 30 days after receipt of the grievance. A written response will be provided to all written grievances. Our decision on a grievance is final and is not subject to an appeal.
You have the right to an expedited review of a grievance concerning our refusal to grant an expedited coverage determination or expedited appeal. This type of grievance will be responded to within 24 hours after our receipt of the grievance.
Contact information
Phone 1-888-247-4142
Fax 1-888-375-8836 or 1-336-794-8836
Hours 7 days a week, 8 a.m. – 8 p.m.
Mail BCBSNCAttn: Medicare Appeals & Grievances PO Box 17509Winston-Salem, NC 27116-7509
In Person
BCBSNC5660 University Pkwy.Winston-Salem, NC 27105
PAGE 14 of 56

Important informationQuality improvement
What if I have a concern about the quality of services I received?If you have a concern relating to the quality of services that you received under the Medicare Part D plan, then in addition to our review, you can also request a review by the following organizations:
KEPRO Quality Improvement Organization (QIO) in North CarolinaKEPRO is a nonprofit, medical care quality improvement organization. KEPRO has been designated by the Centers for Medicare & Medicaid Services as the Quality Improvement Organization for North Carolina. The QIO conducts case reviews to ensure that Medicare beneficiaries receive the quality of medical care that they expect, and to which they are entitled. KEPRO serves as an independent, impartial third party to review Medicare beneficiary complaints.
Quality of care complaints filed with the QIO must be made in writing to the address below. Assistance is also available via phone or online.
KEPRO
Mail KEPRO
5201 W. Kennedy Blvd., Suite 900 Tampa, FL 33609
Phone 1-844-455-8708
TTY/TDD 1-855-843-4776
Hours Monday – Friday, 8 a.m. – 5 p.m.
Web inquiries www.keproqio.com
Seniors’ Health Insurance Information Program (SHIIP)SHIIP is a state consumer division of the North Carolina Department of Insurance. SHIIP assists senior citizens with Medicare, Medicare Part D, Medicare Advantage, Medicare Supplement, Medicare fraud and abuse, and long-term care insurance questions. Assistance is available via phone or online.
Seniors’ Health Insurance Information Program (SHIIP)
Phone 1-855-408-1212
TYY/TDD 1-800-735-2962
Hours Monday – Friday, 8 a.m. – 5 p.m.
Email [email protected]
Online www.ncshiip.com
Blue Cross and Blue Shield of North Carolina is an independent licensee of the Blue Cross and Blue Shield Association.
PAGE 15 of 56

Notes
PAGE 16 of 56

Notes
PAGE 17 of 56

Notes
PAGE 18 of 56

Summary of Benefits
Y0079_6792 PA 08052014U10159, 8/14


(PDP)
2016 Summary of benefits for our Medicare prescription drug plans (Standard and Enhanced)
Contract S5540, Plans 002 and 004 January 1, 2016 – December 31, 2016
Y0079_7238 CMS Accepted 08312015
U5073b,8/15
PAGE 19 of 56

PAGE 20 of 56
Section I - Introduction to
Summary of benefits
This booklet gives you a summary of what wecover and what you pay. It doesn’t list every service that we cover or list every limitation or exclusion. To get a complete list of services we cover, call us and ask for the “Evidence of Coverage.”
You have choices about how to get your Medicare prescription drug benefits
n One choice is to get prescription drug coverage through a Medicare Prescription Drug Plan, like Blue Medicare Rx (PDP) plans.
n Another choice is to get your prescription drug coverage through a Medicare Advantage Plan (like an HMO or PPO) or another Medicare health plan that offers Medicare prescription drug coverage. You get all of your Part A and Part B coverage, and prescription drug coverage (Part D), through these plans.
Tips for comparing your Medicare choices
This Summary of Benefits booklet gives you a summary of what Blue Medicare Rx (PDP) plans cover and what you pay.
n If you want to compare our plan with other Medicare health plans, ask the other plans for their Summary of Benefits booklets. Or, use the Medicare Plan Finder on http://www.medicare.gov.
n If you want to know more about the coverage and costs of Original Medicare, look in your current “Medicare & You” handbook. View it online at http://www.medicare.gov or get a copy by calling 1-800-MEDICARE (1-800-633-4227), 24 hours a day, 7 days a week. TTY users should call 1-877-486-2048.
Sections in this booklet
n Things to know about Blue Medicare Rx (PDP) plans
n Monthly Premium, Deductible, and Limits on How Much You Pay for Covered Services
n Prescription Drug BenefitsThis document is available in other formats such as Braille and large print.This document may be available in a non-English language. For additional information, call us at 1-800-661-5518 (TTY / TDD 1-800-922-3140.
Things to know about Blue Medicare Rx (PDP) plans
Hours of operation
You can call us 7 days a week from 8:00 a.m. to 8:00 p.m. Eastern time.
Blue Medicare Rx (PDP) plans phone numbers and website
n If you are a member of this plan, call toll-free 1-888-247-4142 (TTY / TDD 1-888-247-4145). n If you are not a member of this plan, call toll-free 1-800-661-5518 (TTY / TDD 1-800-922-3140). n Our website: http://www.bcbsnc.com/ medicare
Who can join?
To join Blue Medicare Rx (PDP) plans, you must be entitled to Medicare Part A, and/or be enrolled in Medicare Part B, and live in our service area. Our service area includes the following: North Carolina.

PAGE 21 of 56
Section I - Introduction to
Summary of benefits (continued)
Which drugs are covered?
You can see the complete plan formulary (list of Part D prescription drugs) and any restrictions on our website (www.bcbsnc.com/medicare). Or, call us and we will send you a copy of the formulary.
How will I determine my drug costs?
Our plan groups each medication into one of five “tiers.” You will need to use your formulary to locate what tier your drug is on to determine how much it will cost you. The amount you pay depends on the drug’s tier and what stage of the benefit you have reached. Later in this document we discuss the benefit stages that occur after you meet your deductible if applicable: Initial Coverage, Coverage Gap, and Catastrophic Coverage.
Which pharmacies can I use?
We have a network of pharmacies and you must generally use these pharmacies to fill your prescriptions for covered Part D drugs.
Some of our network pharmacies have preferred cost-sharing. You may pay less if you use these pharmacies.
You can see our plan’s pharmacy directory at our website (www.myprime.com/MyRx/MyPrime/MedicareD/pharmacy/BCBSNC). Or, call us and we will send you a copy of the pharmacy directory.

PAGE 22 of 56
Section II – Summary of Benefits
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$4 copay $8 copay $12 copay
Tier 2(Generic)
$8 copay $16 copay $24 copay
Tier 3 (Preferred Brand)
$40 copay $80 copay $120 copay
Tier 4 (Non- Preferred Brand)
$85 copay $170 copay $255 copay
Tier 5 (Specialty Tier)
25% of the cost 25% of the cost 25% of the cost
BenefitBlue Medicare Rx Standard (PDP)(Plan 002)
Blue Medicare Rx Enhanced (PDP)(Plan 004)
MONTHLY PREMIUM, DEDUCTIBLE, AND LIMITS ON HOW MUCH YOU PAY FOR COVERED SERVICES
How much is the monthlypremium?
$68.40 per month $107.40 per month
How much is thedeductible?
$225 per year for Part D prescription drugs. This plan does not have a deductible.
Blue Cross and Blue Shield of North Carolina is a PDP plan with a Medicare contract. Enrollment in Blue Cross and Blue Shield of North Carolina depends on contract renewal.
PRESCRIPTION DRUG BENEFITS
Initial Coverage After you pay your yearly deductible, you pay the following until your total yearly drug costs reach $3,310. Total yearly drug costs are the total drug costs paid by both you and our Part D plan.
You may get your drugs at network retail pharmacies and mail order pharmacies.
Preferred Retail Cost-Sharing
You pay the following until your total yearly drug costs reach $3,310. Total yearly drug costs are the total drug costs paid by both you and our Part D plan.
You may get your drugs at network retail pharmacies and mail order pharmacies.
Preferred Retail Cost-Sharing

TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1(PreferredGeneric)
$4 copay $8 copay $12 copay
Tier 2(Generic)
$8 copay $16 copay $24 copay
Tier 3(Preferred Brand)
$40 copay $80 copay $120 copay
Tier 4(Non- PreferredBrand)
$85 copay $170 copay $255 copay
Tier 5(Specialty Tier)
25% of the cost 25% of the cost 25% of the cost
Blue Medicare Rx Enhanced (PDP)(Plan 004)
$107.40 per month
This plan does not have a deductible.
You pay the following until your total yearly drug costs reach $3,310. Total yearly drug costs are the total drug costs paid by both you and our Part D plan.
You may get your drugs at network retail pharmacies and mail order pharmacies.
Preferred Retail Cost-Sharing
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$3 copay $6 copay $9 copay
Tier 2(Generic)
$6 copay $12 copay $18 copay
Tier 3 (Preferred Brand)
$30 copay $60 copay $90 copay
Tier 4 (Non- Preferred Brand)
$70 copay $140 copay $210 copay
Tier 5 (Specialty Tier)
33% of the cost 33% of the cost 33% of the cost
BenefitBlue Medicare Rx Standard (PDP)(Plan 002)
MONTHLY PREMIUM, DEDUCTIBLE, AND LIMITS ON HOW MUCH YOU PAY FOR COVERED SERVICES
How much is the monthlypremium?
$68.40 per month
How much is thedeductible?
$225 per year for Part D prescription drugs.
Blue Cross and Blue Shield of North Carolina is a PDP plan with a Medicare contract. Enrollment in Blue Cross and Blue Shield of North Carolina depends on contract renewal.
PRESCRIPTION DRUG BENEFITS
Initial Coverage After you pay your yearly deductible, you pay the following until your total yearly drug costs reach $3,310. Total yearly drug costs are the total drug costs paid by both you and our Part D plan.
You may get your drugs at network retail pharmacies and mail order pharmacies.
Preferred Retail Cost-Sharing
PAGE 23 of 56

Section II – Summary of Benefits (continued)
BenefitBlue Medicare Rx Standard (PDP)(Plan 002)
Blue Medicare Rx Enhanced (PDP)(Plan 004)
PRESCRIPTION DRUG BENEFITS (continued)
Standard Retail Cost-Sharing Standard Retail Cost-Sharing
Preferred Mail Order Cost-Sharing Preferred Mail Order Cost-Sharing
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$9 copay $18 copay $27 copay
Tier 2(Generic)
$20 copay $40 copay $60 copay
Tier 3 (Preferred Brand)
$45 copay $90 copay $135 copay
Tier 4 (Non- Preferred Brand)
$95 copay $190 copay $285 copay
Tier 5 (Specialty Tier)
25% of the cost 25% of the cost 25% of the cost
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$4 copay $8 copay $12 copay
Tier 2(Generic)
$8 copay $16 copay $24 copay
Tier 3 (Preferred Brand)
$40 copay $80 copay $120 copay
Tier 4 (Non- Preferred Brand)
$85 copay $170 copay $255 copay
Tier 5 (Specialty Tier)
25% of the cost 25% of the cost 25% of the cost
PAGE 24 of 56

PAGE 25 of 56
BenefitBlue Medicare Rx Standard (PDP)(Plan 002)
Blue Medicare Rx Enhanced (PDP)(Plan 004)
PRESCRIPTION DRUG BENEFITS (continued)
Standard Retail Cost-Sharing Standard Retail Cost-Sharing
Preferred Mail Order Cost-Sharing Preferred Mail Order Cost-Sharing
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$9 copay $18 copay $27 copay
Tier 2(Generic)
$20 copay $40 copay $60 copay
Tier 3 (Preferred Brand)
$45 copay $90 copay $135 copay
Tier 4 (Non- Preferred Brand)
$95 copay $190 copay $285 copay
Tier 5 (Specialty Tier)
25% of the cost 25% of the cost 25% of the cost
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$8 copay $16 copay $24 copay
Tier 2(Generic)
$20 copay $40 copay $60 copay
Tier 3 (Preferred Brand)
$45 copay $90 copay $135 copay
Tier 4 (Non- Preferred Brand)
$95 copay $190 copay $285 copay
Tier 5 (Specialty Tier)
33% of the cost 33% of the cost 33% of the cost
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$4 copay $8 copay $12 copay
Tier 2(Generic)
$8 copay $16 copay $24 copay
Tier 3 (Preferred Brand)
$40 copay $80 copay $120 copay
Tier 4 (Non- Preferred Brand)
$85 copay $170 copay $255 copay
Tier 5 (Specialty Tier)
25% of the cost 25% of the cost 25% of the cost
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$3 copay $6 copay $9 copay
Tier 2(Generic)
$6 copay $12 copay $18 copay
Tier 3 (Preferred Brand)
$30 copay $60 copay $90 copay
Tier 4 (Non- Preferred Brand)
$70 copay $140 copay $210 copay
Tier 5 (Specialty Tier)
33% of the cost 33% of the cost 33% of the cost

PAGE 26 of 56
Section II – Summary of Benefits (continued)
BenefitBlue Medicare Rx Standard (PDP)(Plan 002)
Blue Medicare Rx Enhanced (PDP)(Plan 004)
PRESCRIPTION DRUG BENEFITS (continued)
Standard Mail Order Cost-Sharing
If you reside in a long-term care facility, you pay the same as at aretail pharmacy.
You may get drugs from an out-of-network pharmacy, but may pay more than you pay at an in-network pharmacy.
Standard Mail Order Cost-Sharing
If you reside in a long-term care facility, you pay the same as at aretail pharmacy.
You may get drugs from an out-of-network pharmacy, but may pay more than you pay at an in-network pharmacy.
Coverage Gap Most Medicare drug plans have a coverage gap (also called the “donut hole”). This means that there’s a temporary change in what you will pay for your drugs. The coverage gap begins after the total yearly drug cost (including what our plan has paid and what you have paid) reaches $3,310.After you enter the coverage gap, you pay 45% of the plan’s cost for covered brand name drugs and 58% of the plan’s cost for covered generic drugs until your costs total $4,850, which is the end of the coverage gap. Not everyone will enter the coverage gap.
Most Medicare drug plans have a coverage gap (also called the “donut hole”). This means that there’s a temporary change in what you will pay for your drugs. The coverage gap begins after the total yearly drug cost (including what our plan has paid and what you have paid) reaches $3,310.
After you enter the coverage gap, you pay 45% of the plan’s cost for covered brand name drugs and 58% of the plan’s cost for covered generic drugs until your costs total $4,850, which is the end of the coverage gap. Not everyone will enter the coverage gap.
Under this plan, you may pay even less for the brand and generic drugs on the formulary. Your cost varies by tier. You will need to use your formulary to locate your drug’s tier. See the chart that follows to find out how much it will cost you.
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$9 copay $18 copay $27 copay
Tier 2(Generic)
$20 copay $40 copay $60 copay
Tier 3 (Preferred Brand)
$45 copay $90 copay $135 copay
Tier 4 (Non- Preferred Brand)
$95 copay $190 copay $285 copay
Tier 5 (Specialty Tier)
25% of the cost 25% of the cost 25% of the cost

BenefitBlue Medicare Rx Standard (PDP)(Plan 002)
Blue Medicare Rx Enhanced (PDP)(Plan 004)
PRESCRIPTION DRUG BENEFITS (continued)
Standard Mail Order Cost-Sharing
If you reside in a long-term care facility, you pay the same as at aretail pharmacy.
You may get drugs from an out-of-network pharmacy, but may pay more than you pay at an in-network pharmacy.
Standard Mail Order Cost-Sharing
If you reside in a long-term care facility, you pay the same as at aretail pharmacy.
You may get drugs from an out-of-network pharmacy, but may pay more than you pay at an in-network pharmacy.
Coverage Gap Most Medicare drug plans have a coverage gap (also called the “donut hole”). This means that there’s a temporary change in what you will pay for your drugs. The coverage gap begins after the total yearly drug cost (including what our plan has paid and what you have paid) reaches $3,310.After you enter the coverage gap, you pay 45% of the plan’s cost for covered brand name drugs and 58% of the plan’s cost for covered generic drugs until your costs total $4,850, which is the end of the coverage gap. Not everyone will enter the coverage gap.
Most Medicare drug plans have a coverage gap (also called the “donut hole”). This means that there’s a temporary change in what you will pay for your drugs. The coverage gap begins after the total yearly drug cost (including what our plan has paid and what you have paid) reaches $3,310.
After you enter the coverage gap, you pay 45% of the plan’s cost for covered brand name drugs and 58% of the plan’s cost for covered generic drugs until your costs total $4,850, which is the end of the coverage gap. Not everyone will enter the coverage gap.
Under this plan, you may pay even less for the brand and generic drugs on the formulary. Your cost varies by tier. You will need to use your formulary to locate your drug’s tier. See the chart that follows to find out how much it will cost you.
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$9 copay $18 copay $27 copay
Tier 2(Generic)
$20 copay $40 copay $60 copay
Tier 3 (Preferred Brand)
$45 copay $90 copay $135 copay
Tier 4 (Non- Preferred Brand)
$95 copay $190 copay $285 copay
Tier 5 (Specialty Tier)
25% of the cost 25% of the cost 25% of the cost
TierOne-month
supplyTwo-month
supplyThree-month
supply
Tier 1 (Preferred Generic)
$8 copay $16 copay $24 copay
Tier 2(Generic)
$20 copay $40 copay $60 copay
Tier 3 (Preferred Brand)
$45 copay $90 copay $135 copay
Tier 4 (Non- Preferred Brand)
$95 copay $190 copay $285 copay
Tier 5 (Specialty Tier)
33% of the cost 33% of the cost 33% of the cost
PAGE 27 of 56

Section II – Summary of Benefits (continued)
BenefitBlue Medicare Rx Standard (PDP)(Plan 002)
Blue Medicare Rx Enhanced (PDP)(Plan 004)
PRESCRIPTION DRUG BENEFITS (continued)
Preferred Retail Cost-Sharing
Standard Retail Cost-Sharing
Preferred Mail Order Cost-Sharing
Standard Mail Order Cost-Sharing
Catastrophic Coverage After your yearly out-of-pocket drug costs (including drugspurchased through your retail pharmacy and through mail order) reach $4,850, you pay the greater of:n 5% of the cost, orn $2.95 copay for generic (including brand drugs treated as generic)
and a $7.40 copay for all other drugs.
After your yearly out-of-pocket drug costs (including drugspurchased through your retail pharmacy and through mail order) reach $4,850, you pay the greater of:n 5% of the cost, orn $2.95 copay for generic (including brand drugs treated as generic) and a $7.40 copay for all other drugs.
PAGE 28 of 56

BenefitBlue Medicare Rx Standard (PDP)(Plan 002)
Blue Medicare Rx Enhanced (PDP)(Plan 004)
PRESCRIPTION DRUG BENEFITS (continued)
Preferred Retail Cost-Sharing
Standard Retail Cost-Sharing
Preferred Mail Order Cost-Sharing
Standard Mail Order Cost-Sharing
Catastrophic Coverage After your yearly out-of-pocket drug costs (including drugspurchased through your retail pharmacy and through mail order) reach $4,850, you pay the greater of:n 5% of the cost, orn $2.95 copay for generic (including brand drugs treated as generic)
and a $7.40 copay for all other drugs.
After your yearly out-of-pocket drug costs (including drugspurchased through your retail pharmacy and through mail order) reach $4,850, you pay the greater of:n 5% of the cost, orn $2.95 copay for generic (including brand drugs treated as generic) and a $7.40 copay for all other drugs.
Tier Drugs Covered
One-month supply
Two-month supply
Three-month supply
Tier 1 (Preferred Generic)
All $3 copay $6 copay $9 copay
Tier Drugs Covered
One-month supply
Two-month supply
Three-month supply
Tier 1 (Preferred Generic)
All $8 copay $16 copay $24 copay
Tier Drugs Covered
One-month supply
Two-month supply
Three-month supply
Tier 1 (Preferred Generic)
All $3 copay $6 copay $9 copay
Tier Drugs Covered
One-month supply
Two-month supply
Three-month supply
Tier 1 (Preferred Generic)
All $8 copay $16 copay $24 copay
PAGE 29 of 56

Notes
PAGE 30 of 56

Enrollment Information
Y0079_6792 PA 08052014U10159, 8/14


PAGE 31 of 56
2016 Individual Enrollment Form for Medicare Prescription Drug PlanPlease contact BCBSNC if you need information in another language or format (Braille).
PO Box 17168 Winston Salem, NC 27116-7168 (PDP)
A. To enroll in BCBSNC, please provide the following information:
First Name Middle Initial Last Name Jr., Sr.
Birth Date (MM/DD/YYYY) Sex Home Phone NumberMale/ / - -Female
Permanent Residence Street Address (P.O. Box is not allowed)
City State Zip Code
County Alternate Phone Number (Optional)
- -
Mailing Address (only if different from your permanent residence address)
City State Zip Code
Emergency Contact (Optional)
Relationship To You Phone Number- -
Please take out your Medicare card and complete this section. Please fill in these blanks so they match your red, white and blue Medicare card, or attach a copy of your Medicare card or your letter from Social Security or the Railroad Retirement Board.
You must have Medicare Part A or Part B (or both) to join a Medicare Prescription drug plan.
B. Please check which plan you want to enroll in
C. Please provide your Medicare insurance information
Blue Medicare Rx Standard .............$ 68.40 per monthEnhanced ...........$ 107.40 per month
Medicare Claim Number
Is EntitledTo:
Hospital (Part A):Medical (Part B):
Effective Date (MM/DD/YYYY)
/
/
/
/
An independent licensee of the Blue Cross and Blue Shield Association.
®, SM Marks of the Blue Cross and Blue Shield Association. D168, 8/15Y0079_7192 CMS Approved 08112015
PAGE 1 of 6

D. Paying your plan premium
You can pay your monthly plan premium (including any late enrollment penalty you may owe) by mail each month. You can also choose to pay your premium by automatic deduction from your Social Security or Railroad Retirement Board benefit check each month. If you are assessed a Part D-Income Related Monthly Adjustment Amount, you will be notified by Social Security Administration. You will be responsible for paying this extra amount in addition to your plan premium. You will either have the amount withheld from your Social Security or Railroad Retirement Board benefit check or be billed directly by Medicare. DO NOT pay BCBSNC the Part D-IRMMA extra amount to Blue Medicare Rx. People with limited incomes may qualify for extra help to pay for their prescription drug costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who qualify won’t have a coverage gap or a late enrollment penalty. Many people are eligible for these savings and don’t even know it. For more information about this extra help, contact your local Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-325-0778. You can also apply for extra help online at www.socialsecurity.gov/prescriptionhelp. If you qualify for extra help with your Medicare prescription drug coverage costs, Medicare will pay all or part of your plan premium. If Medicare pays only a portion of this premium, we will bill you for the amount that Medicare doesn’t cover. If you don’t select a payment option, you will get a bill each month. If you have Medicare Part B, you must continue to pay your Medicare Part B premium if not otherwise paid for under Medicaid or by another third party.
Receive a bill each month.
Automatic deduction from your monthly Social Security/Railroad Retirement Board benefit check. (The Social Security/Railroad Retirement Board deduction may take two or more months to begin. In most cases, if Social Security/Railroad Retirement Board accepts your request for automatic deduction, the first deduction from your Social Security/Railroad Retirement Board benefit check will include all premiums due from your enrollment effective date up to the point withholding begins. If Social Security/the Railroad Retirement Board does not approve your request for automatic deduction, we will send you a paper bill for your monthly premiums.)
If you are a part of a list bill, please fill out the following:
Entity Name:
Group #
E. Please answer the following question
1. Some individuals may have other drug coverage, including other private insurance,YesTRICARE, Federal Employee health benefits coverage, VA benefits, or State
pharmaceutical assistance programs. Will you have other prescription drug Nocoverage in addition to Blue Medicare Rx?
If “yes,” please list your other coverage and your identification (ID) number(s) for this coverage:
Name of other coverage
ID # for this coverage
Group # for this coverage
PAGE 32 of 56

PAGE 33 of 56
PAGE 3 of 6
F. Eligibility for an enrollment period
Typically, you may enroll in a Medicare Prescription Drug Plan only during the annual enrollment period from October 15 through December 7 of each year. Additionally, there are exceptions that may allow you to enroll in a Medicare Prescription drug Plan outside of the annual enrollment period.Please read the following statements carefully and check the box if the statement applies to you. By checking any of the following boxes you are certifying that, to the best of your knowledge, you are eligible for an Enrollment Period. If we later determine that this information is incorrect, you may be disenrolled.
AEP (Annual Enrollment Period). Your effective date will be January 1.
I am new to Medicare. Please choose an effective date: / /
(MM/DD/YYYY)I recently moved outside the service area for my current plan or I recently moved and this plan
is a new option for me. I moved on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I have both Medicare and Medicaid or my state helps pay for my Medicare premiums.
Please choose an effective date: / /
(MM/DD/YYYY)
I get extra help paying for Medicare prescription drug coverage.
Please choose an effective date: / /
(MM/DD/YYYY)
I no longer qualify for extra help paying for my Medicare prescription drug coverage.
I stopped receiving extra help on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I am moving into, live in, or recently moved out of a Long-Term Care Facility (for example, a nursing home or long-term care facility). I moved/will move out of the facility on:
/ /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I recently left a PACE program on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)

PAGE 34 of 56
I recently involuntarily lost my creditable prescription drug coverage (as good as Medicare’s).
I lost my drug coverage on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I am leaving employer or union coverage on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I belong to a pharmacy assistance program provided by my state.
/ /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I recently returned to the United States after living permanently outside of the U.S..
I returned to the U.S. on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
My plan is ending its contract with Medicare, or Medicare is ending its contract with my plan.
My plan is ending on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
My plan is with:
I am making this enrollment request between January 1 and February 14, and I recently ended my enrollment in a Medicare Advantage plan. I left my Medicare Advantage plan on:
/ /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
None of these statements applies to me.*
Other SEP reason:
* Please contact BCBSNC at 1-800-661-5518 to see if you are eligible to enroll. We are open 8 a.m. - 8 p.m., 7 days a week. TTY users should call 1-800-922-3140.
PAGE 4 of 6

PAGE 35 of 56
PAGE 5 of 6
G. Applicant Agreement
I understand that my signature (or the signature of the person authorized to act on my behalf under the State law of where I live) on this application means that I have read and understand the contents of this application. If signed by an authorized individual, this signature certifies that: 1) this person is authorized under State law to complete this enrollment and 2) documentation of this authority is available upon request or by Medicare.
Today’s / /Your Signature Date(MM/DD/YYYY)
If you are the authorized representative, you must sign above and provide the following information:Name
Address
City State Zip Code
Phone Relationship to Enrollee- -
If you prefer us to send you information in a language other than English or in another format (e.g., Braille, audio tape or large print): Please contact BCBSNC at 1-800-661-5518. Our office hours are 8 a.m. to 8 p.m., 7 days a week. TTY users should call 1-800-922-3140.
LICENSED AGENT USE ONLY
Agents must submit a signed enrollment form within 24 hours of receipt.
Agent’s Signature Date App Received
Print Agent’s Name Telephone Number
Agent Number NPN# (required)

PAGE 36 of 56
Please Read This Important Information
If you are a member of a Medicare Advantage Plan (like an HMO or PPO), you may already have prescription drug coverage from your Medicare Advantage Plan that will meet your needs. By joining BCBSNC, your membership in your Medicare Advantage Plan may end. This will affect both your doctor and hospital coverage as well as your prescription drug coverage. Read the information that your Medicare Advantage Plan sends you and if you have questions, contact your Medicare Advantage Plan.
If you currently have health coverage from an employer or union, joining BCBSNC could affect your employer or union health benefits. You could lose your employer or union health coverage if you join BCBSNC. Read the communications your employer or union sends you. If you have questions, visit their website, or contact the office listed in their communications. If there isn’t information on whom to contact, your benefits administrator or the office that answers questions about your coverage can help.
Statement of UnderstandingBy completing this enrollment application, I agree to the following:1. Blue Cross and Blue Shield of North Carolina is a PDP plan with a Medicare contract. Enrollment
in Blue Cross and Blue Shield of North Carolina depends on contract renewal. I understand that this prescription drug coverage is in addition to my coverage under Medicare; therefore, I will need to keep my Medicare Part A or Part B coverage. It is my responsibility to inform BCBSNC of any prescription drug coverage that I have or may get in the future.
2. I can only be in one Medicare prescription drug plan at a time - if I am currently in a Medicare Prescription Drug Plan, my enrollment in Blue Medicare Rx will end that enrollment.
3. Enrollment in this plan is generally for the entire year. Once I enroll, I may leave this plan or make changes if an enrollment period is available, generally during the Annual Enrollment Period (October 15 - December 7), unless I qualify for certain special circumstances.
4. Blue Medicare Rx serves a specific service area. If I move out of the area that BCBSNC serves, I need to notify the plan so I can disenroll and find a new plan in my new area. I understand that I must use network pharmacies, except in an emergency when I cannot reasonably use Blue Medicare Rx network pharmacies.
5. Once I am a member of BCBSNC, I have the right to appeal plan decisions about payment or services if I disagree.
6. I will read the Evidence of Coverage document from BCBSNC when I get it to know which rules I must follow to get coverage.
7. I understand that if I leave this plan and don’t have or get other Medicare prescription drug coverage or creditable prescription drug coverage (as good as Medicare’s), I may have to pay a late enrollment penalty in addition to my premium for Medicare prescription drug coverage in the future.
8. I understand that if I am getting assistance from a sales agent, broker, or other individual employed by or contracted with BCBSNC, he/she may be paid based on my enrollment in BCBSNC.
9. Counseling services may be available in my state to provide advice concerning Medicare supplement insurance or other Medicare Advantage or Prescription Drug Plan options, medical assistance through the state Medicaid program and the Medicare Savings Program.
Release of Information1. By joining this Medicare prescription drug plan, I acknowledge that Blue Medicare Rx will
release my information to Medicare and other plans as is necessary for treatment, payment and health care operations.
2. I also acknowledge that BCBSNC will release my information including my prescription drug event data to Medicare, who may release it for research and other purposes which follow all applicable Federal statutes and regulations.
3. The information on this enrollment form is correct to the best of my knowledge. I understand that if I intentionally provide false information on this form, I will be disenrolled from the plan.
STOP
PAGE 6 of 6

Notes
PAGE 37 of 56

Notes
PAGE 38 of 56

PAGE 39 of 56
2016 Individual Enrollment Form for Medicare Prescription Drug PlanPlease contact BCBSNC if you need information in another language or format (Braille).
PO Box 17168 Winston Salem, NC 27116-7168 (PDP)
A. To enroll in BCBSNC, please provide the following information:
First Name Middle Initial Last Name Jr., Sr.
Birth Date (MM/DD/YYYY) Sex Home Phone NumberMale/ / - -Female
Permanent Residence Street Address (P.O. Box is not allowed)
City State Zip Code
County Alternate Phone Number (Optional)
- -
Mailing Address (only if different from your permanent residence address)
City State Zip Code
Emergency Contact (Optional)
Relationship To You Phone Number- -
Please take out your Medicare card and complete
Medicare Claim Number
Is EntitledTo:
Hospital (Part A):Medical (Part B):
Effective Date (MM/DD/YYYY)
/
/
/
/
this section. Please fill in these blanks so they match your red, white and blue Medicare card, or attach a copy of your Medicare card or your letter from Social Security or the Railroad Retirement Board.
You must have Medicare Part A or Part B (or both) to join a Medicare Prescription drug plan.
B. Please check which plan you want to enroll in
C. Please provide your Medicare insurance information
Blue Medicare Rx Standard .............$ 68.40 per monthEnhanced ...........$ 107.40 per month
An independent licensee of the Blue Cross and Blue Shield Association.
®, SM Marks of the Blue Cross and Blue Shield Association. D168, 8/15Y0079_7192 CMS Approved 08112015
PAGE 1 of 6

PAGE 40 of 56
D. Paying your plan premium
You can pay your monthly plan premium (including any late enrollment penalty you may owe) by mail each month. You can also choose to pay your premium by automatic deduction from your Social Security or Railroad Retirement Board benefit check each month. If you are assessed a Part D-Income Related Monthly Adjustment Amount, you will be notified by Social Security Administration. You will be responsible for paying this extra amount in addition to your plan premium. You will either have the amount withheld from your Social Security or Railroad Retirement Board benefit check or be billed directly by Medicare. DO NOT pay BCBSNC the Part D-IRMMA extra amount to Blue Medicare Rx. People with limited incomes may qualify for extra help to pay for their prescription drug costs. If you qualify, Medicare could pay for 75% or more of your drug costs including monthly prescription drug premiums, annual deductibles, and co-insurance. Additionally, those who qualify won’t have a coverage gap or a late enrollment penalty. Many people are eligible for these savings and don’t even know it. For more information about this extra help, contact your local Social Security office, or call Social Security at 1-800-772-1213. TTY users should call 1-800-325-0778. You can also apply for extra help online at www.socialsecurity.gov/prescriptionhelp. If you qualify for extra help with your Medicare prescription drug coverage costs, Medicare will pay all or part of your plan premium. If Medicare pays only a portion of this premium, we will bill you for the amount that Medicare doesn’t cover. If you don’t select a payment option, you will get a bill each month. If you have Medicare Part B, you must continue to pay your Medicare Part B premium if not otherwise paid for under Medicaid or by another third party.
Receive a bill each month.
Automatic deduction from your monthly Social Security/Railroad Retirement Board benefit check. (The Social Security/Railroad Retirement Board deduction may take two or more months to begin. In most cases, if Social Security/Railroad Retirement Board accepts your request for automatic deduction, the first deduction from your Social Security/Railroad Retirement Board benefit check will include all premiums due from your enrollment effective date up to the point withholding begins. If Social Security/the Railroad Retirement Board does not approve your request for automatic deduction, we will send you a paper bill for your monthly premiums.)
If you are a part of a list bill, please fill out the following:
Entity Name:
Group #
E. Please answer the following question
1. Some individuals may have other drug coverage, including other private insurance,YesTRICARE, Federal Employee health benefits coverage, VA benefits, or State
pharmaceutical assistance programs. Will you have other prescription drug Nocoverage in addition to Blue Medicare Rx?
If “yes,” please list your other coverage and your identification (ID) number(s) for this coverage:
Name of other coverage
ID # for this coverage
Group # for this coverage
PAGE 2 of 6

PAGE 41 of 56
PAGE 3 of 6
F. Eligibility for an enrollment period
Typically, you may enroll in a Medicare Prescription Drug Plan only during the annual enrollment period from October 15 through December 7 of each year. Additionally, there are exceptions that may allow you to enroll in a Medicare Prescription drug Plan outside of the annual enrollment period.Please read the following statements carefully and check the box if the statement applies to you. By checking any of the following boxes you are certifying that, to the best of your knowledge, you are eligible for an Enrollment Period. If we later determine that this information is incorrect, you may be disenrolled.
AEP (Annual Enrollment Period). Your effective date will be January 1.
I am new to Medicare. Please choose an effective date: / /
(MM/DD/YYYY)I recently moved outside the service area for my current plan or I recently moved and this plan
is a new option for me. I moved on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I have both Medicare and Medicaid or my state helps pay for my Medicare premiums.
Please choose an effective date: / /
(MM/DD/YYYY)
I get extra help paying for Medicare prescription drug coverage.
Please choose an effective date: / /
(MM/DD/YYYY)
I no longer qualify for extra help paying for my Medicare prescription drug coverage.
I stopped receiving extra help on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I am moving into, live in, or recently moved out of a Long-Term Care Facility (for example, a nursing home or long-term care facility). I moved/will move out of the facility on:
/ /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I recently left a PACE program on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)

PAGE 42 of 56
I recently involuntarily lost my creditable prescription drug coverage (as good as Medicare’s).
I lost my drug coverage on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I am leaving employer or union coverage on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I belong to a pharmacy assistance program provided by my state.
/ /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
I recently returned to the United States after living permanently outside of the U.S..
I returned to the U.S. on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
My plan is ending its contract with Medicare, or Medicare is ending its contract with my plan.
My plan is ending on: / /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
My plan is with:
I am making this enrollment request between January 1 and February 14, and I recently ended my enrollment in a Medicare Advantage plan. I left my Medicare Advantage plan on:
/ /
(MM/DD/YYYY)
Please choose an effective date: / /
(MM/DD/YYYY)
None of these statements applies to me.*
Other SEP reason:
* Please contact BCBSNC at 1-800-661-5518 to see if you are eligible to enroll. We are open 8 a.m. - 8 p.m., 7 days a week. TTY users should call 1-800-922-3140.
PAGE 4 of 6

PAGE 43 of 56
PAGE 5 of 6
G. Applicant Agreement
LICENSED AGENT USE ONLY
I understand that my signature (or the signature of the person authorized to act on my behalf under the State law of where I live) on this application means that I have read and understand the contents of this application. If signed by an authorized individual, this signature certifies that: 1) this person is authorized under State law to complete this enrollment and 2) documentation of this authority is available upon request or by Medicare.
Today’s / /Your Signature Date(MM/DD/YYYY)
If you are the authorized representative, you must sign above and provide the following information:Name
Address
City State Zip Code
Phone Relationship to Enrollee- -
If you prefer us to send you information in a language other than English or in another format (e.g., Braille, audio tape or large print): Please contact BCBSNC at 1-800-661-5518. Our office hours are 8 a.m. to 8 p.m., 7 days a week. TTY users should call 1-800-922-3140.
Agents must submit a signed enrollment form within 24 hours of receipt.
Agent’s Signature Date App Received
Print Agent’s Name Telephone Number
Agent Number NPN# (required)

PAGE 44 of 56
Please Read This Important Information
If you are a member of a Medicare Advantage Plan (like an HMO or PPO), you may already have prescription drug coverage from your Medicare Advantage Plan that will meet your needs. By joining BCBSNC, your membership in your Medicare Advantage Plan may end. This will affect both your doctor and hospital coverage as well as your prescription drug coverage. Read the information that your Medicare Advantage Plan sends you and if you have questions, contact your Medicare Advantage Plan.
If you currently have health coverage from an employer or union, joining BCBSNC could affect your employer or union health benefits. You could lose your employer or union health coverage if you join BCBSNC. Read the communications your employer or union sends you. If you have questions, visit their website, or contact the office listed in their communications. If there isn’t information on whom to contact, your benefits administrator or the office that answers questions about your coverage can help.
Statement of UnderstandingBy completing this enrollment application, I agree to the following:1. Blue Cross and Blue Shield of North Carolina is a PDP plan with a Medicare contract. Enrollment
in Blue Cross and Blue Shield of North Carolina depends on contract renewal. I understand that this prescription drug coverage is in addition to my coverage under Medicare; therefore, I will need to keep my Medicare Part A or Part B coverage. It is my responsibility to inform BCBSNC of any prescription drug coverage that I have or may get in the future.
2. I can only be in one Medicare prescription drug plan at a time - if I am currently in a Medicare Prescription Drug Plan, my enrollment in Blue Medicare Rx will end that enrollment.
3. Enrollment in this plan is generally for the entire year. Once I enroll, I may leave this plan or make changes if an enrollment period is available, generally during the Annual Enrollment Period (October 15 - December 7), unless I qualify for certain special circumstances.
4. Blue Medicare Rx serves a specific service area. If I move out of the area that BCBSNC serves, I need to notify the plan so I can disenroll and find a new plan in my new area. I understand that I must use network pharmacies, except in an emergency when I cannot reasonably use Blue Medicare Rx network pharmacies.
5. Once I am a member of BCBSNC, I have the right to appeal plan decisions about payment or services if I disagree.
6. I will read the Evidence of Coverage document from BCBSNC when I get it to know which rules I must follow to get coverage.
7. I understand that if I leave this plan and don’t have or get other Medicare prescription drug coverage or creditable prescription drug coverage (as good as Medicare’s), I may have to pay a late enrollment penalty in addition to my premium for Medicare prescription drug coverage in the future.
8. I understand that if I am getting assistance from a sales agent, broker, or other individual employed by or contracted with BCBSNC, he/she may be paid based on my enrollment in BCBSNC.
9. Counseling services may be available in my state to provide advice concerning Medicare supplement insurance or other Medicare Advantage or Prescription Drug Plan options, medical assistance through the state Medicaid program and the Medicare Savings Program.
Release of Information1. By joining this Medicare prescription drug plan, I acknowledge that Blue Medicare Rx will
release my information to Medicare and other plans as is necessary for treatment, payment and health care operations.
2. I also acknowledge that BCBSNC will release my information including my prescription drug event data to Medicare, who may release it for research and other purposes which follow all applicable Federal statutes and regulations.
3. The information on this enrollment form is correct to the best of my knowledge. I understand that if I intentionally provide false information on this form, I will be disenrolled from the plan.
STOP
PAGE 6 of 6

PAGE 45 of 56
MEMBER’S PROTECTED HEALTH INFORMATION (PHI)
REQUEST FORM
You may give Blue Cross Blue Shield of North Carolina (BCBSNC) written authorization to disclose your protected health information (PHI) to anyone that you designate and for any purpose. If you want to authorize a person or entity to receive your PHI upon their request, please provide the information below. Completion of this form is not a condition or requirement of coverage and will not change the way that BCBSNC communicates with you. For example, we will continue to send explanation of benefits (EOB) statements to you upon request. However, if your adult child calls BCBSNC to inquire about you, your protected health information will not be shared with your adult child unless you have given BCBSNC permission to do so by completion of this form.
Please print: Member’s Name:
Member’s Date of Birth ______/ ______/ ______ BCBSNC ID Number
At my request, I authorize BCBSNC to disclose my Protected Health Information (PHI) to: (If you choose, you may designate more than one person.)
Name: Address:
Phone: Relationship to Member:
Name: Address:
Phone: Relationship to Member:
We request that you provide the following information to the person you have authorized so that we may verify the person’s identity and authority to receive your PHI: a) your ID number, b) your date of birth, and c) your address.
I authorize BCBSNC to disclose only the following Protected Health Information to the person designated above. (Check all that apply.)
Any information requested Benefit information Premium Payment Information Explanation of Benefits information All claims information Enrollment information All services from a specific health care provider (List provider’s name): Other (Please list specific PHI):
Blue Medicare HMO and PPO Members: To authorize disclosure of your PHI about mental health/substance abuse services, please call the Mental Health/SA telephone number on the back of your ID card to request a separate authorization form.
I want the designated person to have access to my PHI until my policy expires OR until the specified date of ______/______/______.
Continued on back Y0079_6520 PA 11062013

PAGE 46 of 56
I understand that I may revoke this authorization at any time by giving BCBSNC written notice mailed to the address provided. However, if I revoke this authorization, I also understand that the revocation will not affect any action BCBSNC took while this authorization was valid before BCBSNC received my written notice of revocation.
I also understand that I do not have to authorize anyone to receive my PHI as a condition or requirement for coverage by BCBSNC.
I also understand that if the persons or entities I have authorized to receive my PHI are not health plans, covered health care providers, or health care clearing houses subject to the Health Insurance Portability and Accountability Act (HIPAA), or other federal health information privacy laws, they may further disclose my PHI and it may no longer be protected by HIPAA or federal health information privacy laws.
__________________________________________________________ ______/______/______ Signature of Member Date
OR
__________________________________________________________ ______/______/______ Signature of Personal Representative Date
If signed by a Personal Representative, please:
a) Print your full name: _____________________________________________ AND
b) Describe your authority to act for the member (e.g., durable power of attorney, court order, parent of minor child, etc.) __________________________________________________________________________
ANDc) Attach the legal document naming you as the personal representative when you return this
form.
Note: We will consider the effective date of this authorization to be the date we enter this authorization into our computer system, typically 5 days following receipt. If you would like this authorization to become effective on a date after BCBSNC enters the authorization into its system, please provide the date here: ______/______/______.
RETURN THIS AUTHORIZATION TO:
Attention: Data Operations BCBSNC
P.O. Box 17509 Winston-Salem, NC 27116-7509
5/09Blue Cross and Blue Shield of North Carolina is an HMO, PPO and PDP plan with a Medicare contract. Enrollment in Blue Cross and Blue Shield of North Carolina depends on contract renewal. 5/09

PAGE 47 of 56
Post-Enrollment Timeline
Thank you for choosing Blue Cross and Blue Shield of North Carolina as your health insurance provider. We are a local company, and proud to provide reliable, affordable health insurance to North Carolinians for more than 80 years.
To keep you informed, the steps below describe what you can expect after you submit your enrollment/application form:
Once you submit your enrollment form, you will receive:
+ Anacknowledgementletter– We will mail this letter to you within 10 days of receiving your completed enrollment form. It acknowledges that we have indeed received your enrollment form.
Once your enrollment has been approved by Medicare, you will receive: + A confirmation letter – Once we have received
confirmation from Medicare of your enrollment, we will send you a letter letting you know you have been enrolled. You should receive this letter and your member materials approximately 2 weeks after we receive your completed enrollment request – this usually occurs after your effective date.
+ A verification letter – You should receive this letter within 15 days of receipt of your enrollment form. This letter informs you of your plan choice, monthly premium and co-payments.
When your membership begins, you will receive:
+ A Welcome Kit* – The kit includes the “Evidence of Coverage” (EOC). The EOC gives you details about what the plan covers, how much you pay and more. You’ll also get a provider/pharmacy directory and formulary – a list of the prescription drugs covered by your prescription drug plan.
+ BCBSNC ID Card
*Welcome kit content varies depending on the plan you choose.
Blue Cross and Blue Shield of North Carolina (BCBSNC) is an HMO, PPO, and PDP plan with a Medicare contract. Enrollment in Blue Cross and Blue Shield of North Carolina depends on contract renewal. This is an advertisement.
® Marks of the Blue Cross and Blue Shield Association, an association of independent Blue Cross and Blue Shield Plans. Blue Cross and Blue Shield of North Carolina is an independent licensee of the Blue Cross and Blue Shield Association. U10172b, 8/15
Y0079_7261 CMS Accepted 09032015

PAGE 48 of 56
This page was left intentionally blank

Scope of Sales Appointment Confirmation FormThe Centers for Medicare and Medicaid Services requires agents to document the scope of a marketing appointment prior to any face-to-face sales meeting to ensure understanding of what will be discussed between the agent and the Medicare beneficiary (or their authorized representative). All information provided on this form is confidential and should be completed by each person with Medicare or his/her authorized representative.
Please initial below beside the type of product(s) you want the agent to discuss.
Stand-alone Medicare Prescription Drug Plans (Part D)
Medicare Prescription Drug Plan (PDP) — A stand-alone drug plan that adds prescription drug coverage to Original Medicare, some Medicare Cost Plans, some Medicare Private Fee-for-Service Plans, and Medicare Medical Savings Account Plans.
Medicare Advantage Plans (Part C) and Cost Plans
Medicare Health Maintenance Organization (HMO) — A Medicare Advantage Plan that provides all Original Medicare Part A and Part B health coverage and sometimes covers Part D prescription drug coverage. In most HMOs, you can only get your care from doctors or hospitals in the plan’s network (except in emergencies).
Medicare Preferred Provider Organization (PPO) Plan — A Medicare Advantage Plan that provides all Original Medicare Part A and Part B health coverage and sometimes covers Part D prescription drug coverage. PPOs have network doctors and hospitals but you can also use out-of-network providers, usually at a higher cost.
Medicare Private Fee-For-Service (PFFS) Plan — A Medicare Advantage Plan in which you may go to any Medicare-approved doctor, hospital and provider that accepts the plan’s payment, terms and conditions and agrees to treat you— not all providers will. If you join a PFFS Plan that has a network, you can see any of the network providers who have agreed to always treat plan members. You will usually pay more to see out-of-network providers.
Medicare Special Needs Plan (SNP) — A Medicare Advantage Plan that has a benefit package designed for people with special health care needs. Examples of the specific groups served include people who have both Medicare and Medicaid, people who reside in nursing homes, and people who have certain chronic medical conditions.
Medicare Medical Savings Account (MSA) Plan — MSA Plans combine a high deductible health plan with a bank account. The plan deposits money from Medicare into the account. You can use it to pay your medical expenses until your deductible is met.
Medicare Cost Plan — In a Medicare Cost Plan, you can go to providers both in and out of network. If you get services outside of the plan’s network, your Medicare-covered services will be paid for under Original Medicare but you will be responsible for Medicare coinsurance and deductibles.
Y0079_6382 CMS Accepted 09042013 PAGE 1 of 2
P.O. Box 17509 • Winston-Salem, NC 27116
PAGE 49 of 56

PAGE 50 of 56
By signing this form, you agree to a meeting with a sales agent to discuss the types of products you initialed above. Please note, the person who will discuss the products is either employed or contracted by a Medicare plan. They do not work directly for the Federal government. This individual may also be paid based on your enrollment in a plan.
Signing this form does NOT obligate you to enroll in a plan, affect your current enrollment, or enroll you in a Medicare plan.
Beneficiary or Authorized Representative Signature and Signature Date:
Signature: Signature Date:
If you are the authorized representative, please sign above and print below:
Representative’s Name:
Your Relationship to the Beneficiary:
To be completed by Agent:
Agent Name: Agent Phone:
Beneficiary Name: Beneficiary Phone (Optional):
Beneficiary Address (Optional):
Initial Method of Contact:(Indicate here if beneficiary was a walk-in)
Agent’s Signature: Date Appointment Completed:
Plan(s) the agent represented during this meeting:
[Plan Use Only:]
*Scope of Appointment (SOA) documentation is subject to CMS record retention requirements *
Agent, if the form was signed by the beneficiary at time of appointment, provide explanation why SOA was not documented prior to meeting:
Blue Cross and Blue Shield of North Carolina (BCBSNC) is an HMO and PPO plan with a Medicare contract. Enrollment in Blue Cross and Blue Shield of North Carolina depends on contract renewal. Blue Cross and Blue Shield of North Carolina is a PDP plan with a Medicare contract. Enrollment in Blue Cross and Blue Shield of North Carolina depends on contract renewal. An independent licensee of the Blue Cross and Blue Shield Association. U6161b, 9/13
Y0079_6382 CMS Accepted 09042013 PAGE 2 of 2

Scope of Sales Appointment Confirmation FormThe Centers for Medicare and Medicaid Services requires agents to document the scope of a marketing appointment prior to any face-to-face sales meeting to ensure understanding of what will be discussed between the agent and the Medicare beneficiary (or their authorized representative). All information provided on this form is confidential and should be completed by each person with Medicare or his/her authorized representative.
Please initial below beside the type of product(s) you want the agent to discuss.
Stand-alone Medicare Prescription Drug Plans (Part D)
Medicare Prescription Drug Plan (PDP) — A stand-alone drug plan that adds prescription drug coverage to Original Medicare, some Medicare Cost Plans, some Medicare Private Fee-for-Service Plans, and Medicare Medical Savings Account Plans.
Medicare Advantage Plans (Part C) and Cost Plans
Medicare Health Maintenance Organization (HMO) — A Medicare Advantage Plan that provides all Original Medicare Part A and Part B health coverage and sometimes covers Part D prescription drug coverage. In most HMOs, you can only get your care from doctors or hospitals in the plan’s network (except in emergencies).
Medicare Preferred Provider Organization (PPO) Plan — A Medicare Advantage Plan that provides all Original Medicare Part A and Part B health coverage and sometimes covers Part D prescription drug coverage. PPOs have network doctors and hospitals but you can also use out-of-network providers, usually at a higher cost.
Medicare Private Fee-For-Service (PFFS) Plan — A Medicare Advantage Plan in which you may go to any Medicare-approved doctor, hospital and provider that accepts the plan’s payment, terms and conditions and agrees to treat you— not all providers will. If you join a PFFS Plan that has a network, you can see any of the network providers who have agreed to always treat plan members. You will usually pay more to see out-of-network providers.
Medicare Special Needs Plan (SNP) — A Medicare Advantage Plan that has a benefit package designed for people with special health care needs. Examples of the specific groups served include people who have both Medicare and Medicaid, people who reside in nursing homes, and people who have certain chronic medical conditions.
Medicare Medical Savings Account (MSA) Plan — MSA Plans combine a high deductible health plan with a bank account. The plan deposits money from Medicare into the account. You can use it to pay your medical expenses until your deductible is met.
Medicare Cost Plan — In a Medicare Cost Plan, you can go to providers both in and out of network. If you get services outside of the plan’s network, your Medicare-covered services will be paid for under Original Medicare but you will be responsible for Medicare coinsurance and deductibles.
Y0079_6382 CMS Accepted 09042013 PAGE 1 of 2
P.O. Box 17509 • Winston-Salem, NC 27116
PAGE 51 of 56

Disclaimers
By signing this form, you agree to a meeting with a sales agent to discuss the types of products you initialed above. Please note, the person who will discuss the products is either employed or contracted by a Medicare plan. They do not work directly for the Federal government. This individual may also be paid based on your enrollment in a plan.
Signing this form does NOT obligate you to enroll in a plan, affect your current enrollment, or enroll you in a Medicare plan.
Beneficiary or Authorized Representative Signature and Signature Date:
Signature: Signature Date:
If you are the authorized representative, please sign above and print below:
Representative’s Name:
Your Relationship to the Beneficiary:
To be completed by Agent:
Agent Name: Agent Phone:
Beneficiary Name: Beneficiary Phone (Optional):
Beneficiary Address (Optional):
Initial Method of Contact:(Indicate here if beneficiary was a walk-in)
Agent’s Signature: Date Appointment Completed:
Plan(s) the agent represented during this meeting:
[Plan Use Only:]
*Scope of Appointment (SOA) documentation is subject to CMS record retention requirements *
Agent, if the form was signed by the beneficiary at time of appointment, provide explanation why SOA was not documented prior to meeting:
Blue Cross and Blue Shield of North Carolina (BCBSNC) is an HMO and PPO plan with a Medicare contract. Enrollment in Blue Cross and Blue Shield of North Carolina depends on contract renewal. Blue Cross and Blue Shield of North Carolina is a PDP plan with a Medicare contract. Enrollment in Blue Cross and Blue Shield of North Carolina depends on contract renewal. An independent licensee of the Blue Cross and Blue Shield Association. U6161b, 9/13
Y0079_6382 CMS Accepted 09042013 PAGE 2 of 2
PAGE 52 of 56

Disclaimers
Y0079_6792 PA 08052014U10159, 8/14


PAGE 53 of 56
U5073d, 7/15
Multi-language Interpreter Services
Y0079_7186 CMS Accepted 08022015
1-800-665-8037
(PDP)

PAGE 54 of 56

Blue Cross and Blue Shield of North Carolina is a PDP plan with a Medicare contract. Enrollment in Blue Cross and Blue Shield of North Carolina depends on contract renewal.
Y0079_7353 CMS Accepted 10182015 U7346, 10/15
3.5 Stars
3.5 Stars
Blue Cross and Blue Shield of North Carolina - S5540
2016 Medicare Star Ratings*
The Medicare Program rates all health and prescription drug plans each year, based on a plan's quality and performance. Medicare Star Ratings help you know how good a job our plan is doing. You can use these Star Ratings to compare our plan's performance to other plans. The two main types of Star Ratings are:
1. An Overall Star Rating that combines all of our plan's scores.
2. Summary Star Rating that focuses on our medical or our prescription drug services.
Some of the areas Medicare reviews for these ratings include:
• How our members rate our plan's services and care;
• How well our doctors detect illnesses and keep members healthy;
• How well our plan helps our members use recommended and safe prescription medications.
For 2016, Blue Cross and Blue Shield of North Carolina received the following Overall Star Rating from Medicare.
We received the following Summary Star Rating for Blue Cross and Blue Shield of North Carolina's health/drug plan services:
Health Plan Services: Not Offered
Drug Plan Services:
The number of stars shows how well our plan performs.
5 stars - excellent 4 stars - above average 3 stars - average 2 stars - below average 1 star - poor
Learn more about our plan and how we are different from other plans at www.medicare.gov.
You may also contact us 7 days a week from 8:00 a.m. to 8:00 p.m. Eastern time at 800-661-5518 (toll-free) or 800-922-3140 (TTY).
Current members please call 888-247-4142 (toll-free) or 888-247-4145 (TTY).
*Star Ratings are based on 5 Stars. Star Ratings are assessed each year and may change from one year to thenext.
PAGE 55 of 56

PAGE 56 of 58
This page was left intentionally blank

PAGE 57 of 58

PAGE 58 of 58





























