Embed Size (px)
Citation preview

Blood pressure

Blood pressure (BP)
Blood pressure
• is the lateral pressure exerted by circulating blood on the vessel wall
• the term blood pressure usually refers to the arterial pressure
in the brachial artery measured at a person's upper arm
Systolic blood pressure (SBP)
• maximal blood pressure within cardiac cycle
(which is during systole)
Diastolic blood pressure (DBP)
• minimal blood pressure within cardiac cycle
(which is at the end of diastole)
SBP
DBP
• during the cardiac cycle the arterial BP oscillates in the range of

Pulse pressure = SBP - DBP
• difference between systolic and diastolic pressure
Mean arterial pressure (MP) = 1/3 SBP + 2/3 DBP
- weighed mean - because systole lasts 1/3 of the cardiac cycle, diastole only 2/3
SBP
DBP
MP
pulse pressure

SBP
DBP
Elastic arteries and BP
• elastic arterial wall expands during systole
(due to ejected blood volume/pressure)
• in diastole the vessel wall returns to initial
diameter (due to its elasticity) - this results in
- a continuous blood flow without stopping
- maintenance of BP during diastole
(diastolic pressure in the venticles = 0)

Flow of blood in the cardiovascular system is
• directly proportional to the pressure gradient
- blood flows down the pressure gradient (from higher pressure to lower pressure)
- heart systole creates high pressure
Higher P1 Lower P2
Flow
P1 P2 P
• inversely proportional to
the resistance (R) to flow
• resistance (R) is
– proportional to length (L) of the tube (blood vessel)
– proportional to viscosity () of the fluid (blood)
– inversely proportional to the fourth power of the tube radius (r4)
• small changes in the vessel diameter cause major changes in blood flow
• blood flow (Q) – amount of blood passing a given point in a circulation
8L____r4
R
r4
____
8LQ Hagen-Poiseuille’s Law
Blood pressure – driving force of the blood flow

Blood flow in the vessels
Laminar
- streamline movement of blood.
- blood flows in layers which move parallel to the long
axis of the blood vessel
- velocity is highest for the layer at the center of the
vessel lumen
- blood flow in most vessels of the body is laminar
Turbulent
- non-layered flow, turbulences
- increases the energy required to drive blood
(turbulence - loss of energy in the form of friction,
which generates heat)
- occurs
- normally in large arteries at branch points,
- diseased and narrowed arteries
Reynolds number – if < 2000, the blood flow is laminar , if >4000 blod flow turbulent
blood density X velocity of blood flow X vessel diameter____________________________________________
blood viscosity
Re= https://simplemed.co.uk/images/Cardiovascular/Blood_flow_in_
blood_vessels_-_Laminar_and_Turbulent_flow_SimpleMed.jpg

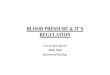
Figure 15.6
SYSTEMIC CIRCULATION PRESSURES
Pressure waves created by ventricular contraction travel into the
blood vessels. Pressure in the arterial side of the circulation cycles
but the pressure waves diminish in amplitude with distance and
disappear at the capillaries.
Systolic pressure
Pulse
pressure
Mean arterial
pressureDiastolic
pressure
Pre
ssu
re (
mm
Hg
)120
100
80
60
40
20
Left
ventricleArteries Arterioles Capillaries Venules,
veinsRight
atrium
• the mean systemic BP due to resistance in blood vessels decreases as the blood
moves away from the heart through arteries
• large areries – oscilations of
– BP(systole/diastole)
– velocity of the blood flow
Pressure gradient across systemic circulation
• from small arterioles
onwards
• constant BP
• constant blood
flow velocity

1. Cardiac output (L/min)
= the volume of blood that is ejected from the heart into aorta / minute
(the more blood enters aorta, the higher the BP)
= stroke volume x frequency
Stroke volume is influenced by:
Preload
- initial stretching of the cardiac myocytes prior to contraction
(Frank-Starling mechanism)
- depends on the amount of ventricular filling
- the greater the stretch (within certain limits), the greater the
force of contraction
Contractility
- increased contractility – increased CO
Afterload
- the pressure against which the heart must work to eject blood
during systole (as afterload increases, the CO decreases)- resistence to systolic ejection- depends on elasticity of aorta, peripheral resistance, etc.
Factors determining blood pressure

https://image.slidesharecdn.com/vtonetpfsn-nw2012-130701061807-
phpapp02/95/vascular-tone-and-tissue-perfusion-21-638.jpg?cb=1372660004
2.Peripheral resistance
- is determined by the smooth muscle tone in vessels (arterioles)
- determines blood outflow to the periphery
- influences the BP
- low resistance – more blood flows to the periphery – a larger decrease in DBP
- high resistance – less blood flows to the periphery, smaller decrease in DBP
- impacts the afterload

3. Blood volume
- normal volume - normal pressure
- low volume - low pressure (e.g. hemorrhagia)
- high volume - high pressure
https://image.slidesharecdn.com/vtonetpfsn-nw2012-130701061807-
phpapp02/95/vascular-tone-and-tissue-perfusion-21-638.jpg?cb=1372660004
high volume -high pressure
low volume -
low pressure

Measurement of arterial blood pressure
• measurement of BP - routine clinical examination
• the term blood pressure usually refers to the arterial pressure in the brachial
artery measured at a person's upper arm
• simple and useful indicator of cardiovascular status
Classification of blood pressure for adults (European Society of Cariology)
SBP mmHg DBP mmHg
Hypotension < 90 < 60
Optimum 90 – 120 and 60 – 80
Normal 120 – 129 or 80 – 84
Higher normal 130 – 139 or 85 – 89
Hypertension* ≥ 140 or ≥ 90
• hypertension is classified as mild, moderate, or severe depending on the BP values
• about 30- 45% of adult population have hypertension, prevalence is rising with age
• high BP – risk factor of stroke, myocardial infarction

1. Age
- children – lower values, increase with age
- from puberty onwards – normal „adult“ values
- elderly– increase in BP (atherosclerosis - loss of arterial elasticity/ increase of stiffness)
BP is not static - undergoes natural variations due to:
2. Gender
– mean BP in males is slightly higher on average
3. Respiration
– respiratory arrthymia inspiration – a mild increase of BP
expiration – a mild decrease of BP

4. Circadian rhythm
- in sleep the BP drops down
(mainly in non-REM sleep)
Non-dipper
- a person in whom there is an absence
of the normal nocturnal fall (dip) in blood
pressure
- an additional risk factor for the
development of adverse cardiovascular
events
Dipper
- a person with normal nocturnal drop in BP
5. Stress, physical activity – increase in BP

Measurement of the arterial
blood pressure

- Indirect method – with sphygmomanometer
• a cuff that is placed on the arm
• attached mercury manometer indicates values of blood pressure (BP)
- Direct method – canulla is inserted into an artery and connected to a monitor

Procedure
- before the measurement the patient should be
in rest for about 15 minutes (avoiding physical
activity or stress)
- patient is in sitting or lying position,
forearm/hand is on a table
- the cuff is wrapped around the arm 2 cm above
fossa cubiti
- stethoscope bell is placed below the cuff
/partially under
- the bag inside the cuff is inflated by a repeated squeezing a rubber bulb
- the pressure in bag is indicated by the attached manometer
- inflate to approx by 20 mm Hg higher value than the predicted value of BP
in subjects with normal BP to approx to 150
in hypertension approx to 180-200 or even more
http://www.jagranjosh.com/imported/images/E/Articles/measuring-blood-pressure.jpg

slowly release the screw of the pump and listen carefully
the pressure in the cuff will decrease
when you start hearing a sound of heart beat - read the pressure = SBP
- at the beginning the sound is like a murmur
- read the value when you hear clear heartbeat
continue releasing the screw – the pressure in manometer will be further
decreasing
the sound (heartbeat) will remain for some time audible – the sound will
undergo changes in loudness
the pressure at which the sounds disappear read the diastolic pressure
sound disappears
- silence
sound appears
„hearbeats“silence

- when it falls just below the SBP a small
spurt of blood escapes through the artery
- blood flows through a narrow space -
the blood flow is turbulent (loud)
- slight tapping sounds occur with each
heartbeat (Korotkoff sounds) – indicate
the value of SBP
- when the pressure in the cuff is equal to
the diastolic pressure, the blood flow
becomes laminar (silent) and the sound
disappears
Principle of the measurement :
- sufficiently inflated cuff – the pressure in bag exceeds blood pressure in brachial
artery – artery occluded (no blood flow)
- as the screw is released, the pressure in bag falls

Task:
- measure the blood pressure in 2 people
- repeat the measurement in each subject 3 times
Result and conclusion
- record and evaluate the values – compare the 3 measurements
- calculate the mean pressure and the pulse pressure
White-coat hypertension (WCH)
• for some patients the measurement taken in a doctor's office is higher than their
typical BP
• can result from anxiety related to an examination by a health care professional.
• A 24 h ABPM – ambulatory blood pressure monitorng monitoring is recommended
to determine valid values

Control of the cardiovascular system
Control of the cardiac function
- Frank-Starling mechanism
- Nervous regulation (sympathetic, parasympathetic)
- Humoral regulation (hormones, other humoral factors)
Regulation of the circulation
- Systemic nervous regulation (vasomotor centre)
- mainly sympathetic regulation (higher/lower tone)
- parasympathetic only in some organs (glands, genitals)
- Systemic humoral regulation (hormones, other humoral factors)
- Vasodilating agents: natriuretic peptides, epinephrine (b - receptors)
- Vasoconstricting agents: ADH, angiotensin II, epinephrine (a - receptors)
- Regulation of the blood volume
- Increase: ADH, aldosterone
- Decrease: atrial natriuretic peptide
- Local regulatory factors
A/ short-term – aimed at suffcient blood supply
B/ long-term – aimed at the maintenance of the BP

Baroreflex (baroreceptor reflex)
• one of the body's homeostatic mechanisms that helps to maintain blood
pressure at nearly constant levels
• provides a rapid negative feedback loop in which
– an elevated blood pressure reflexively
• inhibits the heart rate heart rate (via parasympathetic) and
• causes vascular dilation (inhibition of sympathetic) –
• as a result the blood pressure to decreases
– decreased blood pressure causes
• heart rate to increase
• vascular constriction to restore blood pressure levels
• very rapid - can begin to act in fractions of a second (short-term regulation)
• baroreflex adjustments are key factors in dealing with postural hypotension, the
tendency for blood pressure to decrease on standing due to gravity

This map shows the reflex
response to an increase in
mean arterial pressure.
Bloodpressure
Sensory neurons
Firing of baroreceptors incarotid arteries and aorta
Cardiovascularcontrol center
in medullaoblongata
Sympathetic output Parasympathetic output
less NE released
a-receptor b1-receptor b1-receptor
more ACh onmuscarinic receptor
Arteriolar smooth muscle
Vasodilation
Bloodpressure
Peripheral resistance Cardiac output
Heart rate
SA nodeVentricular myocardium
Force of contraction
Negativefeedback
KEY
Stimulus
Sensor
Afferent pathway
Integrating center
Output signal
Target
Tissue response
Systemic response

Cardiovascular Control
KEY
Stimulus
Sensor
Integrating center
Output signal
Target
Medullarycardiovascular
controlcenter
Parasympatheticneurons
Changein bloodpressure
Carotid and aorticbaroreceptors
Sympatheticneurons SA node
Ventricles
Veins
Arterioles
FIGURE QUESTION
Name the neurotransmitters
and receptors for each of
the target tissues.
© 2013 Pearson Education, Inc.

Orthostatic test
Principle
- reaction of CVS to a load represented by a change of position
- can be used as a screening method

Procedure
• stay in lying position for 5 minutes (resting peacefully, fully relaxed)
• measure your heart rate (HR 1) and blood pressure (BP1)
• stand up and immediately after change of position measure
– the heart rate (HR 2)
– the blood pressure (BP2)
- change from lying to standing position
- redistribution of blood volume
- systolic blood pressure decreases and heart rate increases
- the peak heart rate is found approximately 15 sec after standing up
Result
difference in heart rate = HR 2 – HR 1
Evaluation
• 6 – 12 beats per minute: adequate reaction
• 13 – 19 beats per minute: acceptable reaction
• 20 and more beats per minute: inadequate reaction

A few notes to the orthostatic test.....
• heart rate reactions are very individual - individual baseline measurement is needed
• may be used in sports medicine
• previous orthostatic test results are always the best reference for each person
Orthostatic hypotension
- defined as a decrease
- in systolic blood pressure of 20 mm Hg
- or a decrease in diastolic blood pressure of 10 mm Hg
- within three minutes of standing when compared with blood pressure from the
sitting or supine position
- results from an inadequate physiologic response to postural changes in blood
pressure
- may be acute or chronic, as well as symptomatic or asymptomatic
Case
- every time when Mary stands up, she feels dizziness, she has blurred vision,
weakness, nausea, palpitations
- It takes about half a minute until she feels good again

The Ruffier test
- in a simple way and with sufficient rate of reliability sets the functional
state of the cardiovascular system and readiness of organism for load

1. rest in sitting position for 5 minutes
• measure your heart rate per minute (HR 1)
2. do 30 squats in 30 seconds (terminate the exercise even if you do not succeed
to do 30 sqats)
• immediately after exercise measure HR 2
– measure HR over six seconds and multiply by 10 to get the number of
beats per minute
3. sit down
• one minute after the end of the effort, measure HR 3
– measure HR over six seconds and multiply by 10 to get the number of
beats per minute

Result:
calculate your index:
Index of physical fitness = [ (HR1 + HR2 + HR3)-200 ] /10
Conclusion
• 0 excellent
• up to 5 very good
• up to 10 good
• up to 15 average
• over 15 poor

Local control of the blood flow
Myogenic theory of autoregulation
- Increased blood pressure – dilation of the vessel wall – reflex contraction
Metabolic autoregulation - tissue metabolic products with vasodilating effect
- Increase in: H+, CO2, K+, lactate, histamine, adenosine, decrease in O2
Endothelium derived vasoactive substances
- endothelial cells - active tissue, cells respond according to their needs by production of
- vasodilating agents: NO, prostacyclins (PGI2), prostaglandins (PGE2)
- vasoconstricting agents: endothelines, trhomboxane A2, prostaglandines (PGH2)
Autoregulation - the tissues are able to control their blood flow

Reactive hyperemia
Hyperaemia
- an increase of blood flow to a part of the body
- hyperemia in the skin capillaries – red colour
a/ Active
b/ Reactive

Active hyperemia matches blood flow to increased metabolism.
Mechanism
Tissue
metabolism
Release of metabolic vasodilators into ECF
Arterioles dilate.
Resistance creates
blood flow.
O2 and nutrient supply to tissue
increases as long as metabolism
is increased.

Tissue
blood flow due
to occlusion
Metabolic vasodilators accumulate in ECF.
Arterioles dilate, but occlusion prevents blood flow.
Resistance creates
blood flow.
As vasodilators wash away, arterioles constrict
and blood flow returns to normal.
Remove
occlusion
Reactive hyperemia follows a period of decreased blood flow
Mechanism

Task: Observe reactive hyperaemia
Procedure:
- observe the colour of the examinee's skin on both hands, it should be
light pink
- attach the tourniquet of a manometer to the left arm
- the examinee lifts his hand above his head
- the cuff of the manometer is inflated up to approx. 165 mm Hg
- this procedure decreases the blood flow into the area below
- the examinee puts the hand on the table
• observe the colour of the hands
expected: (right – normal, left – pale to purple - hypoxia)
• after the tourniquet is removed, observe again the colour of the hands
expected: right normal, left – red for transient time
Result and conclusion:
describe the observations, explain the changes in colour of the arm

Figure 15.21
Normal arterial wall
Fatty streak
Stable fibrous plaque
Vulnerable plaque
Endothelial cells
Elastic connective tissue
Smooth muscle cells
LDL-cholesterol accumulates between the
endothelium and connective tissue and is
oxidized.
Macrophages ingest cholesterol and
become foam cells.
Smooth muscle cells, attracted by
macrophage cytokines, begin to divide
and take up cholesterol.
A lipid core accumulates beneath
the endothelium.
Fibrous scar tissue forms to wall off
the lipid core.
Smooth muscle cells divide and
contribute to thickening of the intima.
Calcifications are deposited within
the plaque.
Macrophages may release enzymes that
dissolve collagen and convert stable
plaques to unstable plaques.
Platelets that are exposed to collagen
activate and initiate a blood clot.
Atherosclerosis – underlying process of many cardiovascular diseases

Cardiovascular Disease: Risk Factors
• Not controllable
– Gender
– Age
– Family history
Some risk factors can be modified by lifestyle
- healthy diet - physical activity
Together with
- control of BP - control of blood lipid levels
• Controllable- Smoking
- Obesity
- Bad diet
- Sedentary lifestyle
- Untreated hypertension
- Dyslipidaemia
- a heart attack occurs when the flow of blood to the heart is
blocked,
- the interrupted blood flow can damage or destroy part of the
heart muscle
- mostly due to atherosclerosis
Risk Factors