Embed Size (px)
Citation preview
Blood Management in Cardiac SurgeryUsing
Multidisciplinary Multimodality Approaches
Global Blood Resources LLC
www.mybloodfirst.com
Roadmap
Discuss Blood ConservationWhere we are today with blood
The multidisciplinary players
Their multimodality approaches
What Perfusionists Can Do
Changing the Paradigm
What else can we do !
Disclosure statement:GBR is the maker of the Hemobag® for ATS
ETHICS OF BLOOD MANAGEMENT
-First Do No Harm “Primum Non Nocere”
-Transfuse only when absolutely necessary
-Transfuse Only what’s Required / Sparingly-The Freshest Components Possible- Minimal Blood Draws Sampling-Avoid Waste/ Recover as much Autologous as poss-Use POC Labs to Justify Transfusions-Use Evidence Based Medicine in Decisions
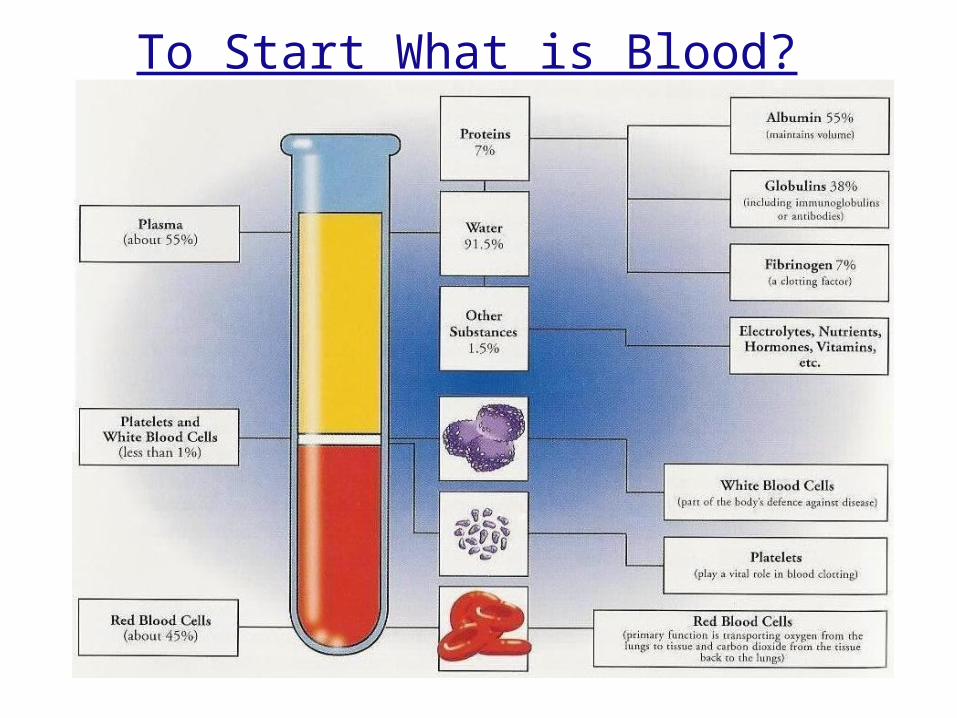
To Start What is Blood?
First, A Surprise Quiz!Don’t ponder, just raise your hand
if you Generally Agree with the question• Do you feel like you have an excellent report with your Surgeons in surgery ? Do they listen ? • Do you feel like you have an excellent report with Anesth in surgery and do they listen ?• Do your Anesthesiologists use pressors to keep the SVR up instead of Volume ?• Do you feel like your Anesthesiologists gives too much crystalloid in general ?• Do you feel that most of your Surgeons really try to avoid giving any donor products?• Do you feel that most of your Anes really try to avoid giving any donor blood products?• Do you RAP before going on bypass and does Anesthesia help and the Surgeon wait ?• Do you use Osmitrol/Mannitol or Albumin? More than once ?• Do you use the pump sucker during the case to return blood to the ECC in Valve cases ?• Do you use the pump sucker during the case to return blood to the ECC in CABG cases ?• Do you use the pump sucker during the case to return blood to the ECC in Aortic cases ?• Do you feel that your processing too much cell washer volume by the end of the case ?• Do you have a waste sucker in the field, and do they use it ?• Do you use a Hemoconcentrator on at least 20% of your cases, 40%, >40% of the time ?• Do you use a Hemoconcentrator to salvage the ECC at the end of the case, or Bag the Vol ?• Is your Transfusion trigger on CPB generally < 7gm Hgb or < 8gm Hgb ?• Do you feel that a transfusion is an organ transplant ?

Bank Blood Costs• Cost of blood products rising with no direct reimbursement.
MC does not pay until 4th unit…
Red Blood Cell Units: $500 – $1,000Platelet Pheresis pack: $536Plasma Units FFP: (4) $300+Cryoprecipitate:(5+fee) $250
• Transfusion reactions: Infections, viruses and most importantly Immunosupression / Immunomodulation
• Incidence of TRALI (>1:2,000 donor exposures)• Nationwide range of “blood admin charges per discharge:” $2,240
DeAnda, Spiess, et al. $1,422 / PRBC unit
JC will be evaluating blood management as part of AccreditationJoint Commission Perspectives on Pt. Safety: Jan. Vol. 7:1, 2007
Allogeneic Blood Problems!
Morbidity and mortality risk associated with red blood cell and blood-component transfusion in isolated coronary artery bypass grafting* April 2006
Koch CG, Li L, Duncan AI, Mihaljevic T, Cosgrove DM, Loop FD, Starr NJ, Blackstone EH.From the Departments of Cardiothoracic Anesthesia (CGK, AID, NJS), Quantitative Health Sciences (LL, EHB), and Thoracic and Cardiovascular Surgery (TM, DMC, FDL, EHB), The Cleveland Clinic Foundation; Cleveland, OH.
MEASUREMENTS AND MAIN RESULTS: 12K 48.6% were transfused. Transfusion of red blood cells was associated with a risk-adjusted increased risk for every postoperative morbid event: mortality 95% [CI], renal failure, prolonged ventilatory support, serious infection, cardiac complications & neurological events. CONCLUSIONS: Perioperative red blood cell transfusion is the single factor most reliably associated with increased risk of postoperative morbid events after isolated coronary artery bypass grafting. Each unit of red cells transfused is associated with incrementally increased risk for adverse outcome.
Transfusions blamed for deaths after heart bypass
NEW YORK (Reuters Life) - Getting a blood transfusion during or after heart bypass surgery may raise the risk of dying in the next few months after the operation, new research suggests.Moreover, this may explain in part why women are more likely than men to die after coronary artery bypass grafting (CABG), since women more commonly need transfusions than men do."To the best of our knowledge, this is the first study to state that ... transfusions may be the reason why women have a greater post-CABG mortality than men," Dr. Mary A. M. Rogers, from the University of Michigan in Ann Arbor, said in a statement.In a study of Michigan Medicare beneficiaries, 88 percent of female CABG patients received a blood transfusion compared with 67 percent of male patients.Patients who received a blood transfusion were 5.6-times more likely to die within 100 days of undergoing heart bypass surgery than were non-transfused patients,the report indicates. © Reuters 2007. All Rights Reserved.
Duration of red-cell storage and complications after cardiac surgery. N England J Med 2008 Mar 20;358(12):1229-39. Koch CG, et al.
BACKGROUND: Stored red cells undergo progressive structural and functional changes over time. We tested the hypothesis that serious complications and mortality after cardiac surgery are increased when transfused red cells are stored for more than 2 weeks.
METHODS: We examined data from patients given red-cell transfusions during coronary-artery bypass grafting, heart-valve surgery, or both between June 30, 1998, and January 30, 2006. A total of 2872 patients received 8802 units of blood that had been stored for 14 days or less ("newer blood"), and 3130 patients received 10,782 units of blood that had been stored for more than 14 days ("older blood"). Multivariable logistic regression with propensity-score methods was used to examine the effect of the duration of storage on outcomes. Survival was estimated by the Kaplan-Meier method and Blackstone's decomposition method.
RESULTS: The median duration of storage was 11 days for newer blood and 20 days for older blood. Patients who were given older units had higher rates of in-hospital mortality (2.8% vs. 1.7%, P=0.004), intubation beyond 72 hours (9.7% vs. 5.6%, P<0.001), renal failure (2.7% vs. 1.6%, P=0.003), and sepsis or septicemia (4.0% vs. 2.8%, P=0.01). A composite of complications was more common in patients given older blood (25.9% vs. 22.4%, P=0.001). Similarly, older blood was associated with an increase in the risk-adjusted rate of the composite outcome (P=0.03). At 1 year, mortality was significantly less in patients given newer blood (7.4% vs. 11.0%, P<0.001).
CONCLUSIONS: In patients undergoing cardiac surgery, transfusion of red cells that had been stored for more than 2 weeks was associated with a significantly increased risk of postoperative complications as well as reduced short-term and long-term survival.
Older Blood carries Greater Morbidity and Mortality
Increased mortality, postoperative morbidity, and cost after red blood cell transfusion in patients having cardiac surgery.
Circulation 2007 Nov 12 Murphy GJ, Reeves BC, Rogers CA,
BACKGROUND: Red blood cell transfusion can both benefit and harm. To inform decisions about transfusion, we aimed to quantify associations of transfusion with clinical outcomes and cost in patients having cardiac surgery. Methods and RESULTS: Clinical, hematology, and blood transfusion databases were linked with the UK population register. Additional hematocrit information was obtained from intensive care unit charts. Composite infection (respiratory or wound infection or septicemia) and ischemic outcomes (myocardial infarction, stroke, renal impairment, or failure) were prespecified as co-primary end points. Secondary outcomes were resource use, cost, and survival. Associations were estimated by regression modeling with adjustment for potential confounding. All adult patients having cardiac surgery between April 1, 1996, and December 31, 2003, with key exposure and outcome data were included (98%). Adjusted odds ratios for composite infection (737 of 8516) and ischemic outcomes (832 of 8518) for transfused versus non-transfused patients were 3.38 (95% confidence interval [CI], 2.60 to 4.40) and 3.35 (95% CI, 2.68 to 4.35), respectively. Transfusion was associated with increased relative cost of admission (any transfusion, 1.42 times [95% CI, 1.37 to 1.46], varying from 1.11 for 1 U to 3.35 for >9 U). At any time after their operations, transfused patients were less likely to have been discharged from hospital (hazard ratio [HR], 0.63; 95% CI, 0.60 to 0.67) and were more likely to have died (0 to 30 days: HR, 6.69; 95% CI, 3.66 to 15.1; 31 days to 1 year: HR, 2.59; 95% CI, 1.68 to 4.17; >1 year: HR, 1.32; 95% CI, 1.08 to 1.64). CONCLUSIONS. Red blood cell transfusion in patients having cardiac surgery is strongly associated with both infection and ischemic postoperative morbidity, hospital stay, increased early and late mortality, and hospital costs.
Blood transfusions may be killing some of the people they are intended to save
Dr. Sunny Rao Duke Cardiologist 2004IF THERE were any sure bets in medicine, you might think that “blood transfusions save lives” would be one of them. But there aren't. Even though deaths caused in the 1980s by accidental HIV infection mean that donated blood is now screened meticulously to keep it free of infectious agents, there is still a nagging feeling that something is wrong.
In 2004, Sunil Rao of Duke University Medical Centre, in North Carolina, carried out a retro study of 24K people suffering from acute coronary syndrome. One conclusion drawn from his research was that unnecessary blood transfusions might be causing tens of thousands of deaths in America alone. Rao found that patients who had had a transfusion because of a low red blood-cell count had an 8% chance of dying within 30 days, and those without a transfusion, only 3% died. Those numbers need to be treated with caution. As Dr Rao points out, the patients who underwent transfusion were, on average, sicker and older than those who did not. Nevertheless, this study is not the only indication of something amiss with transfused Allogeneic blood products.
What are expert thoughts about the recent articles on Nitric Oxide and banked blood?
Neil Blumberg, Prof of Path & Lab Med, Univ of Rochester MC
"I think it is well established in the scientific literature that stored red cells do weird things to the microcirculation. It is also well established in observational studies that patients with acute coronary syndromes (e.g., MI, unstable angina) seem to do markedly worse when transfused than not transfused at similar hematocrits. Red cells that are nitric oxide poor will presumably scavenge nitric oxide, a vasodilator, and thus cause vasoconstriction and reduced oxygen delivery and thus impair its delivery. Most of the clinical correlative studies in the literature mentioned above involve patients getting non-leukoreduced transfusions rich in inflammatory, pro-thrombotic mediators, as well as residual platelet microparticles, white cell membranes and microparticles, and Lord knows what else. So it's not clear how much either factor, nitric oxide scavenging and infusion of a mixture of deleterious mediators contributes to the clinical observations. My bet is on both. What is clear to me and some others in the field is that fewer patients should be transfused and we are doing more harm than good with our current transfusion practices in many cases."
So how can we manage blood better and who are the Multidisciplinary Players involved?
Primary Doctor
Cardiologist
Admission Care Team
Pre Game Plan with the Big Three
*Surgeon, Anesthesia, Perfusion*
Anesthesia
Surgeon
Perfusion (Its not your fault !) GWH
ICU Care Team, Nurses
Administrators
The Primary Doctors Office
Baseline lab work (preferably 6 wks early)
Micro-sampling (Peds Tubes)
Iron therapy 50% of the Population are Low
Epo therapy 2-3 weeks to raise Hct 2-3%
Help patient to select best Hospital
Help patient to select best Cardiologist
Help guide patient to select best Surgeon
The Cardiologist
Minimal Labs with Micro Sampling at all times
Meticulous attn to blood loss during Cath, Rao MD
Minimize the use of Heparin and ACT’s < 999
The Use of Anti-Platelet drugs like Plavix < is best
Identify the best hospital to have Surgery done atIdentify the best Surgeon to do the Case (specialist)
No more than 2 easy Stents w/o Stent Jail please or send me to Surgery as grafts last longer!
DES=5.5% BMS=7.8% On Pump CABG= 2.8%@3yr
The Admission Care Team
Preferably the day of surgery
Micro Sampling for Labs (a must)
That first I.V. Line (Let the games begin)
For every 1 liter of Crystalloid given
Only 250 mls will stay Intravascular within 30 minutes, the rest of the 750mls will cross extravascularly causing Organ Edema/Dysfx dropping the Viscosity and COP. It’s a lot easier to add volume than it is to take it off!

The “Epicenter” of Life & Fluid Balance

Permeability varies with type of capillary
Capillary type varies with organ function
1. Tight (brain) 2. Continuous (skeletal muscle, skin) 3. Fenestrated (secretory glands, kidney, gut) 4. Discontinuous (liver, spleen, bone marrow)
Capillary "Type"
Edema:Edema: Most common clinical manifestation of an imbalance of forces at the capillary wall
Excess accumulation of fluid in the interstitial space that has not been readsorbed into capillaries or taken up by the lymphatics
Causes include• Obstruction • Permeability or change in reflection coefficient
Increased protein permeability results in an imbalance – Occurs in trauma, thermal injury, inflammation– Life threatening manifestations - endotoxic shock, ARDS
• Plasma Protein– Reduction in circulating plasma proteins, especially albumin– Liver dysfunction, malnutrition, or acute alteration of fluid status
• Albumin attenuates extravasation of fluid out of intravascular space to interstitial space
• Capillary pressure
Pre Game Plan (The Big 3)• When ever possible the members of the
Cardiac surgical team (The Surgeon, Anesthesia, and Perfusion) should meet prior to surgery and discuss the best course of action for optimizing the case and avoiding Allogeneic Blood Products.
• The Team Approach to Blood Management !
Anesthesia
Meticulous placement of Lines to function correctly and not loose any blood or make any extra holes.
Limit the amount of Crystalloid given during the case and opt for Colloids like Albumin instead for Volume.
Vascular Tone (SVR) use Pressors as tolerated by cardiac output to achieve a normal SVR of between 800-1200.
ANH Acute Normovolemic Hemodilution, usually 1-2 units or more can be removed safely and still keep a good Hct while on Pump. This should be the first vol seen post CPB.
Targeted Pharmacotherapy (Amicar, Aprotinin, DDAVP, rFVIIa Novo 7, Vitamin K and other recombinant factors)
*8 gm – 10 gm Hgb DUKE 2006 / Henry Ford 2009
No Benefit and No Harm
Red Cell Mass Contributes to Red Cell Mass Contributes to Hemostasis By Pushing the Hemostasis By Pushing the
Platelets out to the EndotheliumPlatelets out to the Endothelium
HCT OF AT LEAST 24%
AnesthesiaContinued
Hypotension is NOT Hypovolemia! (Chappell Fluid Article)
Push the SVR not the Starling Curve! normal 800-1200.
Hemodilution is the Enemy! It leads to Organ Edema and Organ Dysfunction that leads to Morbidity and Mortality!
HD creates to a Dilutional Anemia and a Dilutional Coagulopathy that leads to Blood Products leads to M&M!
Give No Volume and keep Patient tight till the H/C Volume

The Surgeon
Communicate clearly during the case and work diligently
Have patience with the Perfusionists while they are RAP’ing
Refrain from cooling as much, as it stuns/hurts the Platelets
Meticulous surgical technique should be employed throughout the surgical procedure when bleeding
When ever there is obvious surgical bleeding the surgeon should stop to tie down or cauterize the area to reduce the waste of blood. (And also fix the venous air) Micro-bubbles !
Remember that transfusion of any Allogeneic blood or blood products is an “Organ Transplant", and not just another medication that is without side-effects. Treat everyone like a JW !
**The** Perfusionist
Condense your Circuit Prime down safely to 1000 - 1400mls !
Calculate the Post-Dilutional Hct, Protein, COP values
RAP/VAP (Auto Prime) both sides of your Circuit with the help of Anesthesia and the Surgeon. This is not only proven very effective in many studies, and its $$$ economical as it costs nothing.
Add Albumin / Osmitrol to Increase the COP / Diuresis of the patient.
Limit the Cell Washer to the Pre and Post Heparinization periods!
Use the pump’s Coronary Sucker during the Heparinization period to preserve frank Autologous Whole Blood lost outside the heart inside the pericardium and return it to back to the patient’s circulation.
A waste sucker should be kept in the field for undesirable shed blood and irrigant solutions (or a cell washer for this as well).

On-site coagulation monitoring like the thromboelastography TEG, Sonoclot and Heparin concentration determination like the Hepcon are essential tools in determining the Hemostasis.
Targeted pharmacotherapy (antifibrinolytics and desmopressin acetate) are an integral part to prevent empiric transfusions of allogenic blood and blood products.
Hemoconcentration should be considered for use to reverse excess fluid administration perioperatively, eliminate undesirable byproducts including antiplatelet medications and concentrate the patient’s red cell mass and plasma proteins during the case.
Once safely off bypass Salvage the CPB circuit with Ultrafiltration so you don’t waste any of the patient’s OWN viable and vital blood cell fractions and components to a waste bag.
Perfusion Cont.
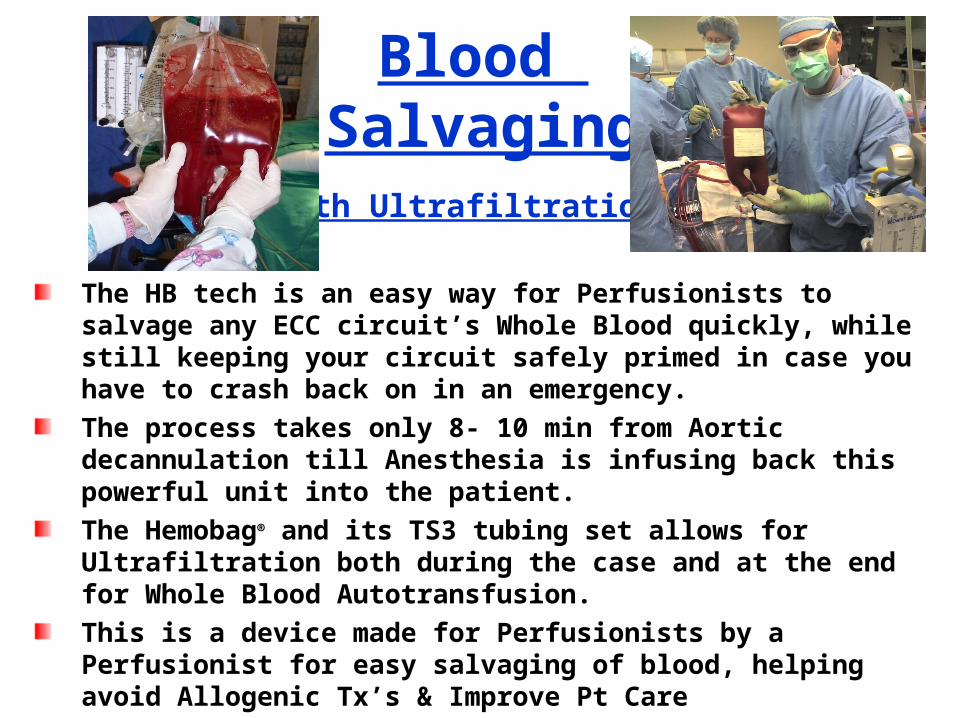
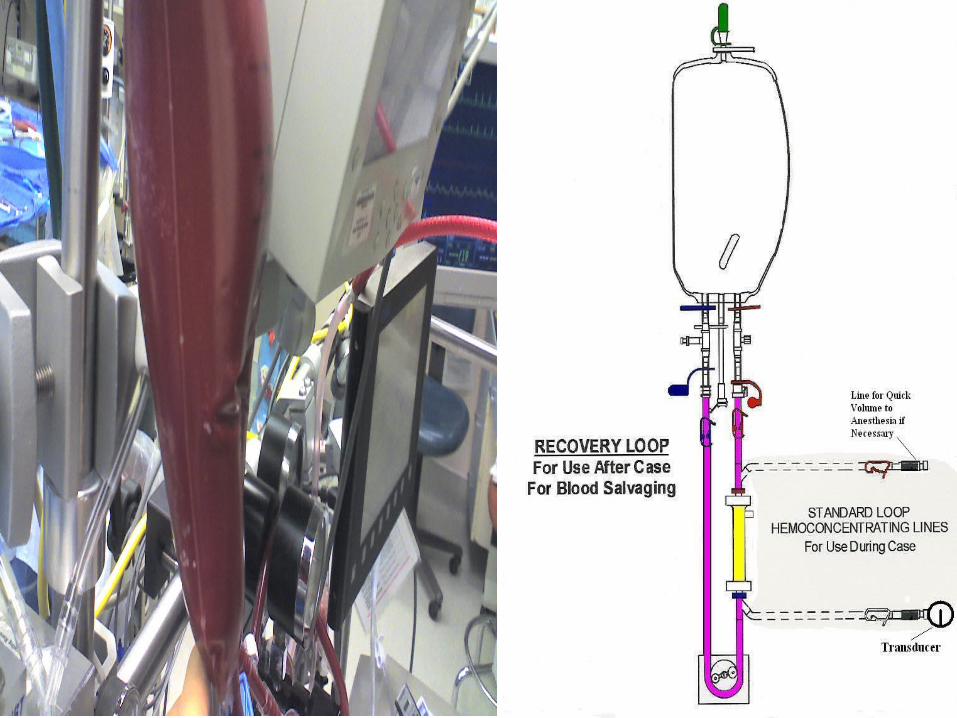
Blood Salvaging
With Ultrafiltration
The HB tech is an easy way for Perfusionists to salvage any ECC circuit’s Whole Blood quickly, while still keeping your circuit safely primed in case you have to crash back on in an emergency.
The process takes only 8- 10 min from Aortic decannulation till Anesthesia is infusing back this powerful unit into the patient.
The Hemobag® and its TS3 tubing set allows for Ultrafiltration both during the case and at the end for Whole Blood Autotransfusion.
This is a device made for Perfusionists by a Perfusionist for easy salvaging of blood, helping avoid Allogenic Tx’s & Improve Pt Care
The end product is a hyperoncotic Autologous Whole Blood packed with viably functioning Platelets, Clotting Factors, Albumin, Plasma Proteins and RBC’s with no morbidity or side effects.
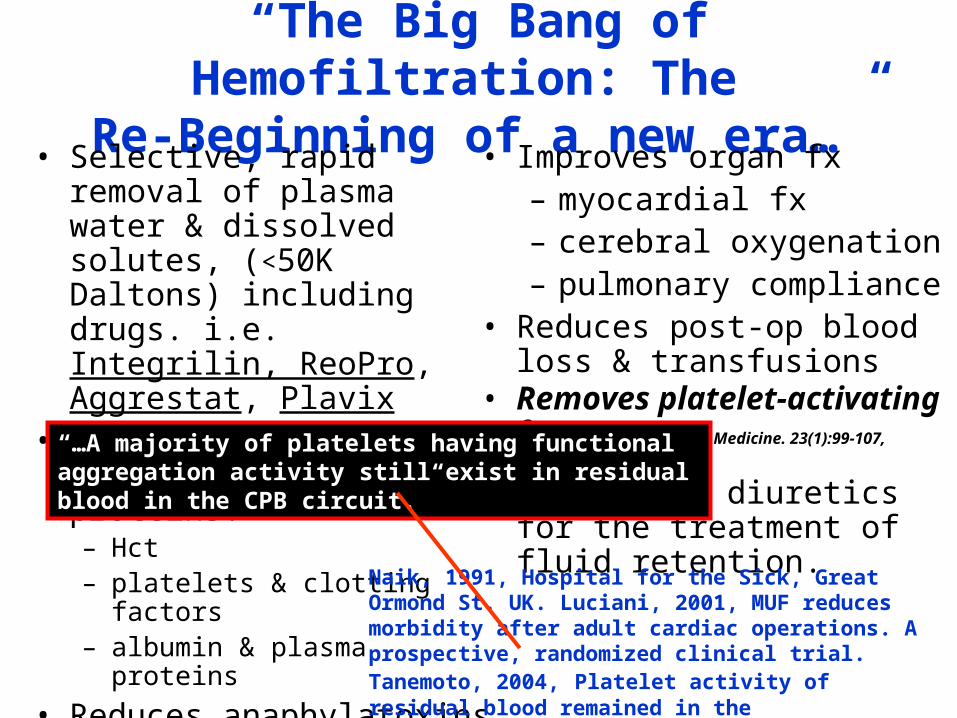
“The Big Bang of Hemofiltration: The Re-Beginning of a new era…”
• Selective, rapid removal of plasma water & dissolved solutes, (<50K Daltons) including drugs. i.e. Integrilin, ReoPro, Aggrestat, Plavix
• Conservation cellular blood components & proteins. – Hct– platelets & clotting factors– albumin & plasma proteins
• Reduces anaphylatoxins– C3a, C4a, C5a– IL-1, IL-2, IL-6, IL-8,– TNF, TNF– MDF, bradykinins
• Improves organ fx– myocardial fx– cerebral oxygenation– pulmonary compliance
• Reduces post-op blood loss & transfusions
• Removes platelet-activating factor Critical Care Medicine. 23(1):99-107, January 1995
• Adjunct to diuretics for the treatment of fluid retention.
Naik, 1991, Hospital for the Sick, Great Ormond St. UK. Luciani, 2001, MUF reduces morbidity after adult cardiac operations. A prospective, randomized clinical trial. Tanemoto, 2004, Platelet activity of residual blood remained in the cardiopulmonary bypass circuit after cardiac surgery
“…A majority of platelets having functional aggregation activity still exist in residual blood in the CPB circuit.”
30
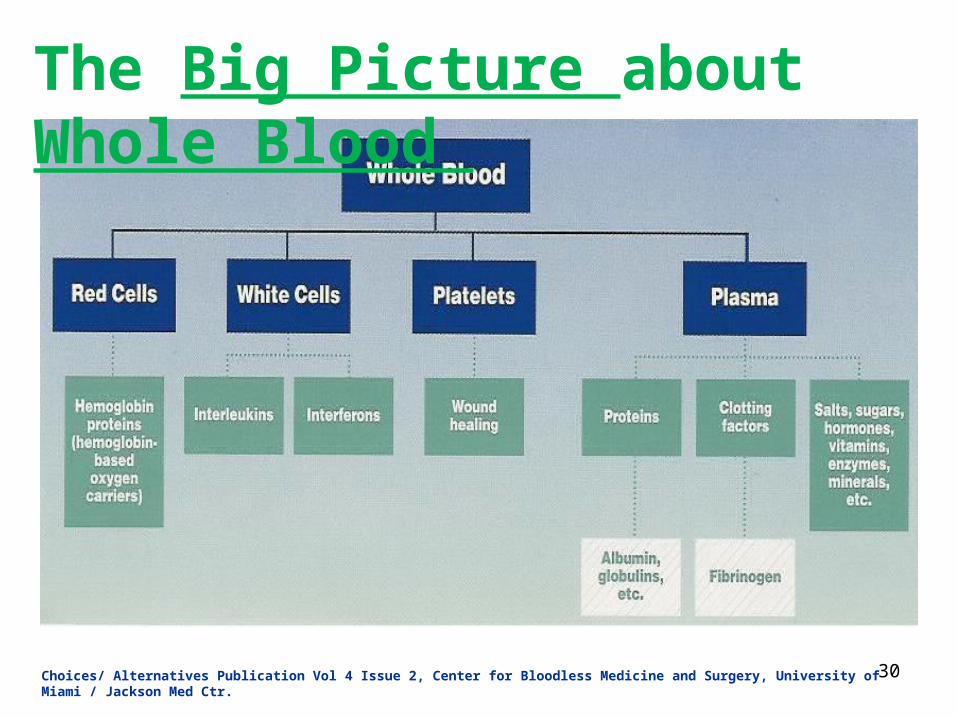
The Big Picture about Whole Blood
Choices/ Alternatives Publication Vol 4 Issue 2, Center for Bloodless Medicine and Surgery, University of Miami / Jackson Med Ctr.
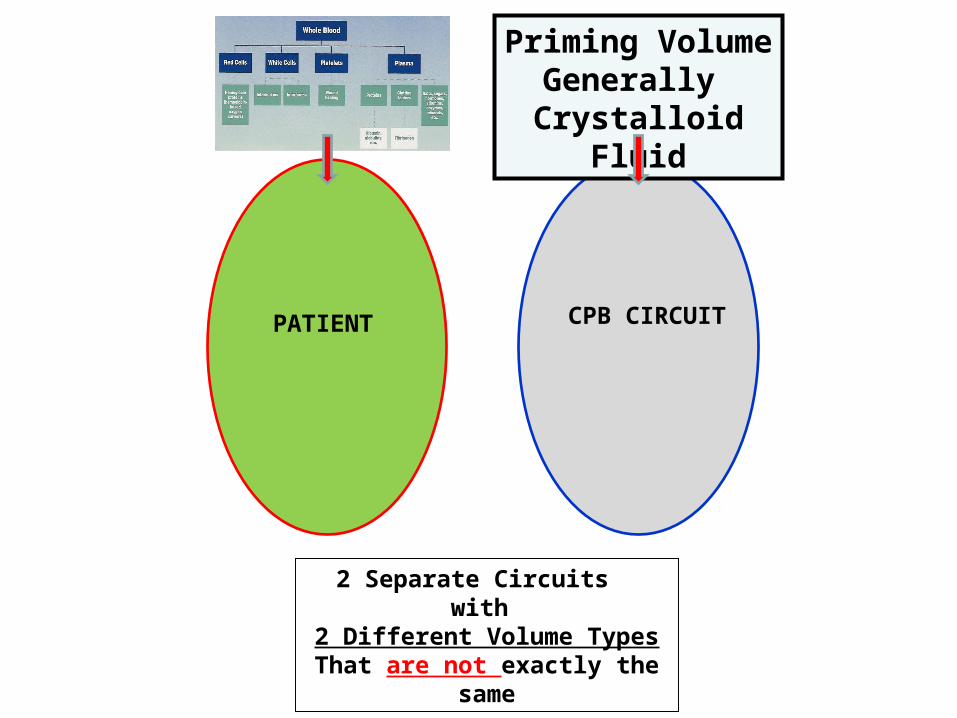
PATIENT CPB CIRCUIT
2 Separate Circuits with
2 Different Volume TypesThat are not exactly the same
Priming VolumeGenerally
Crystalloid Fluid
On CPB
Now Only 1 (ONE) Circuit with the
Same Volume TypeThat is exactly the Same
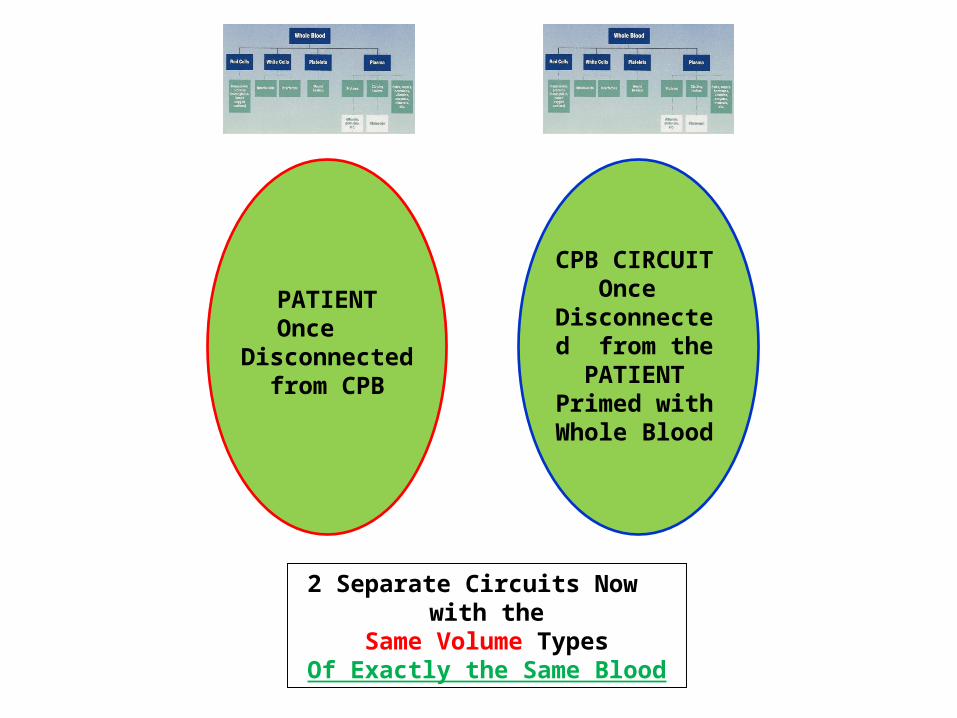
PATIENTOnce
Disconnected from CPB
CPB CIRCUITOnce
Disconnected from the PATIENT
Primed with Whole Blood
2 Separate Circuits Now with the
Same Volume TypesOf Exactly the Same Blood
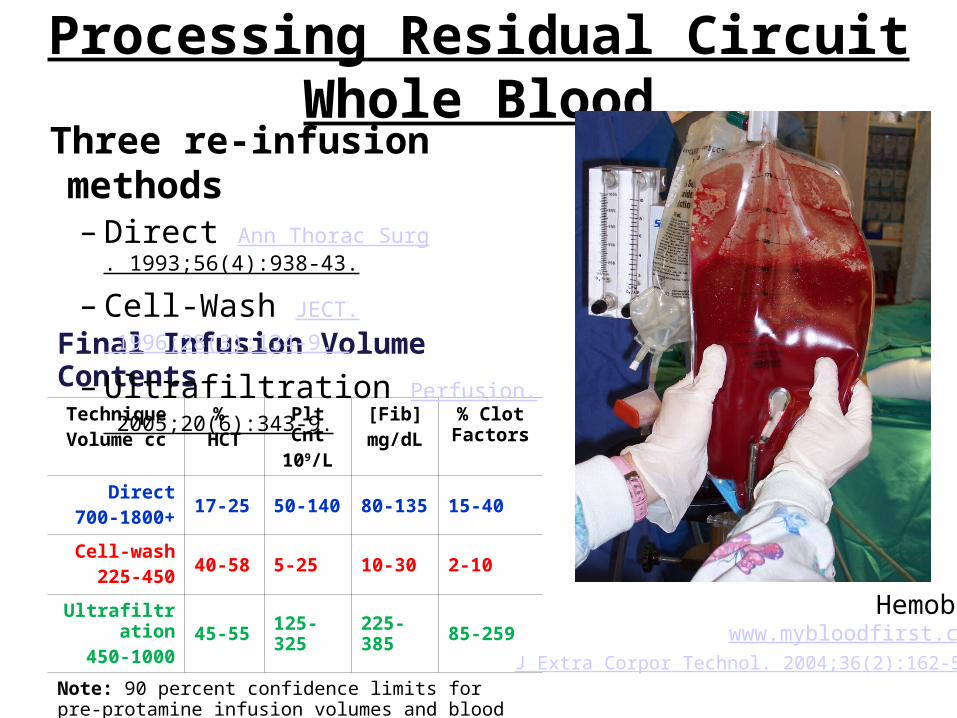
Processing Residual Circuit Whole Blood
Final Infusion Volume ContentsTechniqueVolume cc
% HCT
Plt Cnt109/L
[Fib]mg/dL
% Clot Factors
Direct700-1800+
17-25 50-140 80-135 15-40
Cell-wash225-450
40-58 5-25 10-30 2-10
Ultrafiltration450-1000
45-55 125-325 225-385 85-259
Note: 90 percent confidence limits for pre-protamine infusion volumes and blood component values(Proc Amer Soc Extra Corpor Technol. 2006)
Three re-infusion methods– Direct Ann Thorac Surg. 1993;56(4):938-43.
– Cell-Wash JECT. 1996;28(3):134-9.
– Ultrafiltration Perfusion. 2005;20(6):343-9.
Hemobag®
www.mybloodfirst.com/J Extra Corpor Technol. 2004;36(2):162-5.

Ultrafiltration Versus Cell WashingResidual CPB Circuit Whole Blood
Issue Ultrafiltration Cell-WashingClotting factor preservation Concentrates remaining factors Discards clotting factors
Protein (fibrinogen) preservation Concentrates Albumin and Fibrinogen Discard albumin and fibrinogen
Allogeneic transfusion avoidance Helps to avoid use of PRBCs and component therapy
Helps to avoid use of PRBCs; May increase the use of
component therapy
Heparin / drug removal Concentrates some drugs Removes many drugs
Platelet / RBC / WBC preservation Concentrates Functional Blood Cells May waste or activate Platelets,
WBCs and RBCs
Interleukin / complement removal Removes some ILs complements Removes some ILs or complements
Contamination Should not introduce bacteria CW product contains bacteria
Fat removal May remove some fat Removes some fat
Cost-savings Cost savings with decreased allogeneic component therapy
Some cost savings with reduced allogeneic PRBC use
1 Roeder. J Extra Corpor Technol. 2004;36(2):162-5. 2 Samolyk. Perfusion. 2005;20(6):343-9. 3 Jackson. J Extra Corpor Technol. 2006;38(1);A86.4 Beckmann. J Extra Corpor Technol. 2007;39(2):103-8.5 Riley. J Extra Corpor Technol. 2007;39(1)A3.
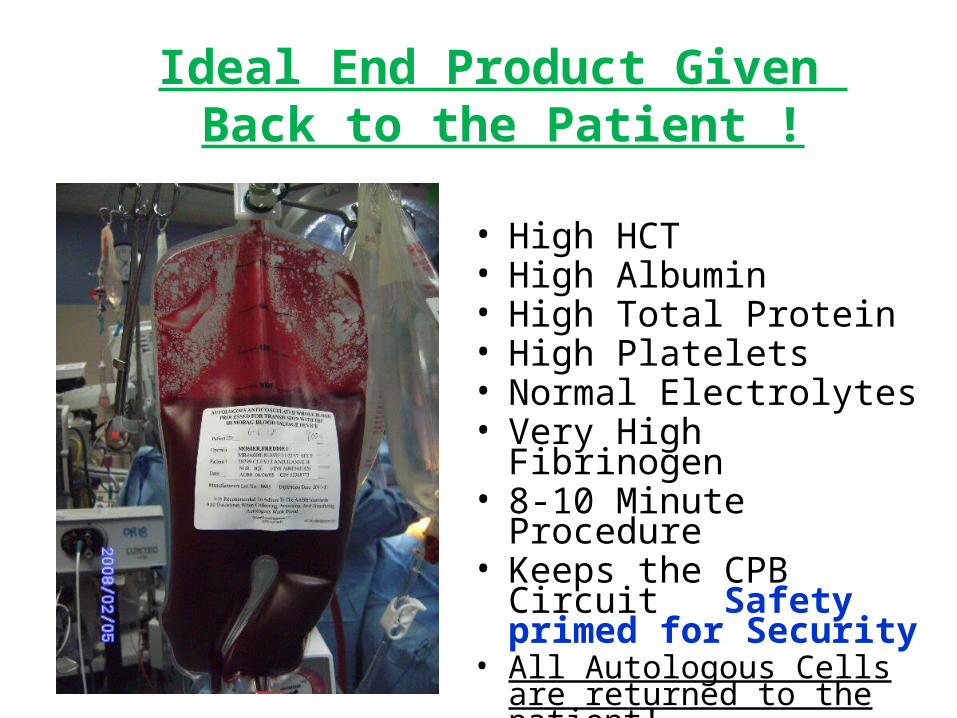
Ideal End Product Given Back to the Patient !
• High HCT• High Albumin• High Total Protein• High Platelets• Normal Electrolytes• Very High Fibrinogen• 8-10 Minute Procedure• Keeps the CPB Circuit
Safety primed for Security
• All Autologous Cells are returned to the patient!

What’s the Next Evolution of Autotransfusion for ECC’s in CV Surgery
Cell Washer Waste Whole Blood
ULTRAFILTRATION has the benefit of
Concentrating Whole Blood
quickly & easilySaving All the Plasma as well as the RBC’s !
So How Can We Make It Really Easy
ULTRAFILTRATION
FDA Cleared Device Specifically made for Perfusionists for
Autotransfusion and Blood Conservation
Using “Multipass Ultrafiltration”
A Universal Blood Reservoir for Salvaging and Concentrating
Autologous Whole Blood from any Extracorporeal Circuit or any anticoagulated blood Reservoir
*In compliance with Jehovah’s Witness patients wishes & guidelines
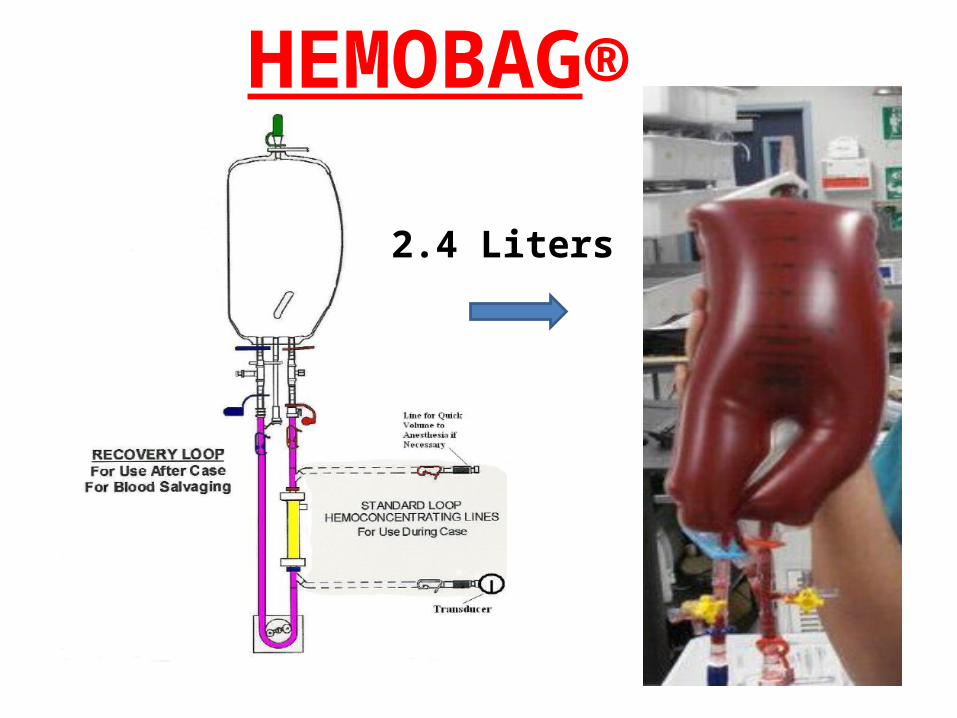
HEMOBAG®
2.4 Liters
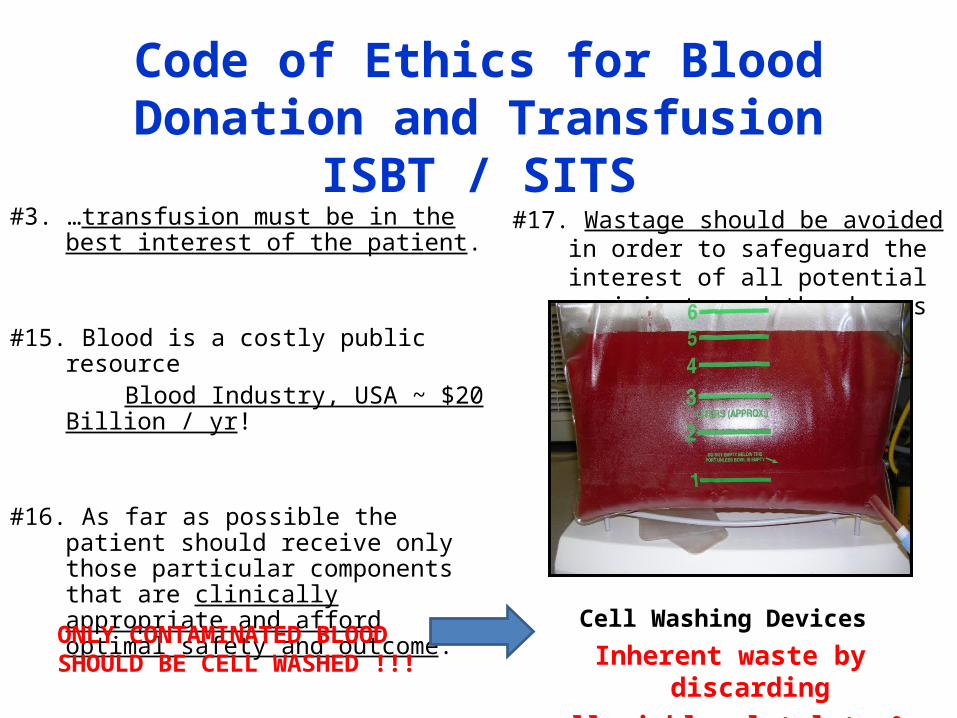
Code of Ethics for Blood Donation and TransfusionISBT / SITS
#3. …transfusion must be in the best interest of the patient.
#15. Blood is a costly public resource Blood Industry, USA ~ $20 Billion / yr!
#16. As far as possible the patient should receive only those particular components that are clinically appropriate and afford optimal safety and outcome.
#17. Wastage should be avoided in order to safeguard the interest of all potential recipients and the donors
Cell Washing Devices
Inherent waste by discarding all viable platelets & plasma
~280-300ml per bowl
ONLY CONTAMINATED BLOOD SHOULD BE CELL WASHED !!!
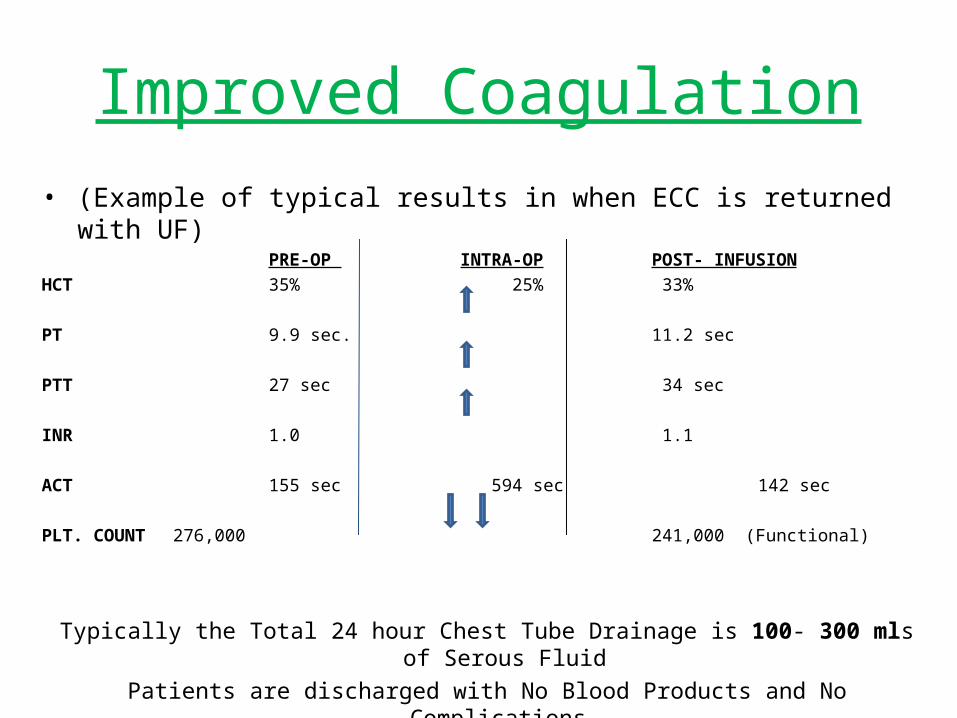
Improved Coagulation• (Example of typical results in when ECC is returned with UF) =
PRE-OP INTRA-OP POST- INFUSIONHCT 35% 25% 33%
PT 9.9 sec. 11.2 sec
PTT 27 sec 34 sec
INR 1.0 1.1
ACT 155 sec 594 sec 142 sec
PLT. COUNT 276,000 241,000 (Functional)
Typically the Total 24 hour Chest Tube Drainage is 100- 300 mls of Serous FluidPatients are discharged with No Blood Products and No Complications.
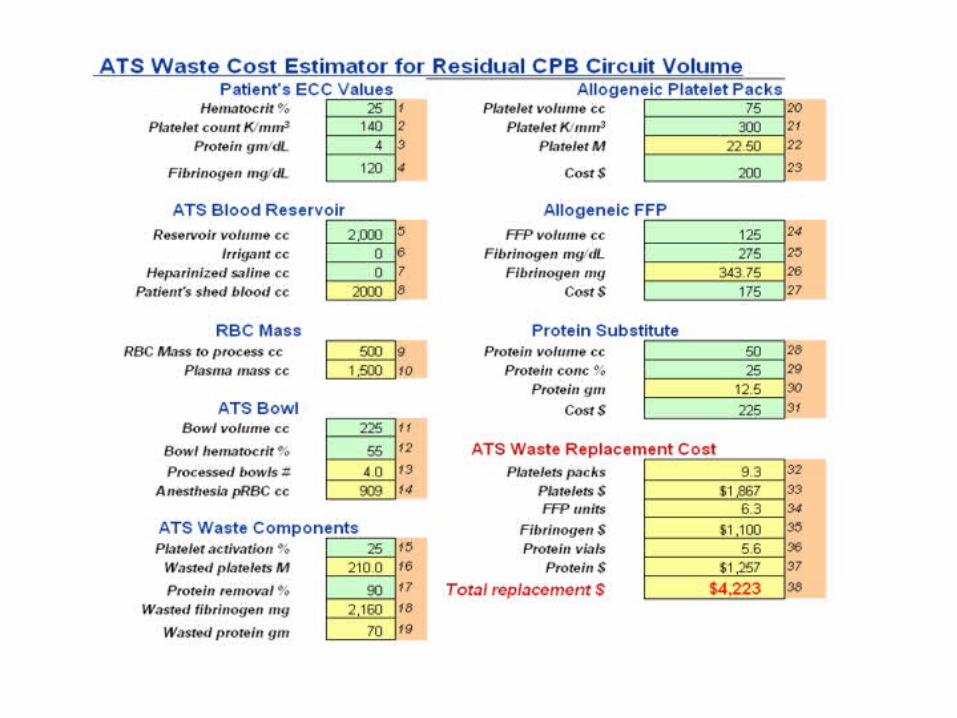
ATS Waste Calculator (JECT 2007)


Clotting FactorsFactor I Fibrinogen Half life 3-5 days)Factor II Pro-thrombinFactor III Tissue Thromboplastin (TT)Factor IV CalciumFactor V Labile factor (proaccelerin)Factor VI not assignedFactor VII Stable factor (proconvertin)Factor VIII Anti-hemophilic factor A (AHF)Factor IX Christmas FactorFactor X Stuart - Prower FactorFactor XI Plasma Thromboplastin antecedentFactor XII Hageman factorFactor XIII Fibrin Stabilizing factor
The higher up the cascade the clotting factor deficiency is the worse and more detrimental the coagulopathy can be

The Clotting Cascades
FFP & FIBRINOGEN FACTS• Fibrinogen is produced by the Liver (340 kDa)• It is the main protein of blood coagulation and the mainstay in
treatment of inherited coagulopathies• Frozen for up to 1 year, must be used within 24hrs of thawing• Fibrinogen meshes with the Platelet plug and converts to a stable
Fibrin clot • Normal blood levels are 150- 400 mg/dl• Normal concentrations in plasma are about 3mg/ml• Ea unit of FFP 200-300mls has 1-2mg/ml of Fibrinogen• It’s an important parameter in the diagnosis of CAD.• FFP use is up over 40% here in the USA since 1979• Use and demand has continued to grow each year• The USA uses 3 times as much as Europe does!• Plasma Tx is not benign it can cause TRALI, TACO, TRIM and other Immunological consequences!

Do in vitro coagulation tests predict bleeding?The relationship between clotting factors and the PT is Exponential !
10%
45%
Dzik WH, in Mintz PC ed. Transfusion therapy: principles and practice, 2nd edition. AABB Press, 2005
Equivalent Fibrinogen VolumeAverage from HB 500 cases
• Frozen Plasma: – 1 Average Hemobag ≈ 3.4 units of FFP (300ml @ 325mg) for Fbg. equivalency to one
average Hemobag reinfusion (800ml. @ 450mg/dl)• Cryoprecipitate:
– 1 Average Hemobag ≈ 37 units of Cryo. (60ml. @150mg pooled units) for Fbg equivalency to one average Hemobag reinfusion (800ml. @ 450mg/dl)
** FFP usage in the United States is rising each year and rising at a rate faster than RBC's. 30% of FFP transfusions do not meet current guidelines.
[Transfusion Vol. 45: July, 2005. Dr. Dzik]
Current trend nationwide FFP usage:‘03: 2.7M u.‘04: 3.3M u.’05: ↑ M u.
’06: ↑↑M.u

Circulation
Lymphatics
Fluid Volume Management
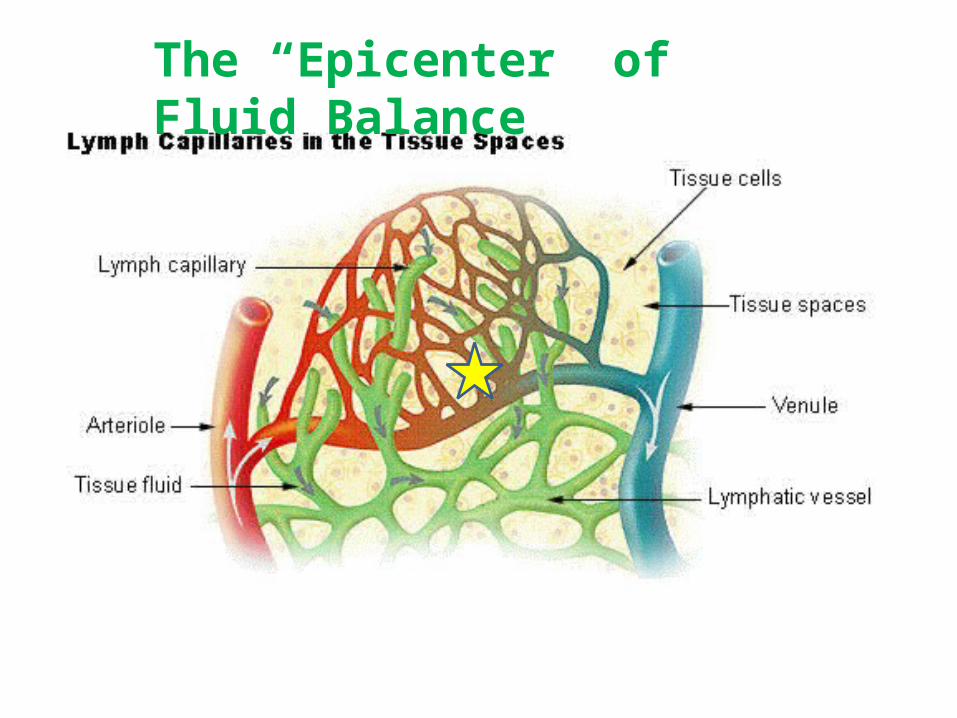
The “Epicenter” of Fluid Balance

STARLINGS LAW

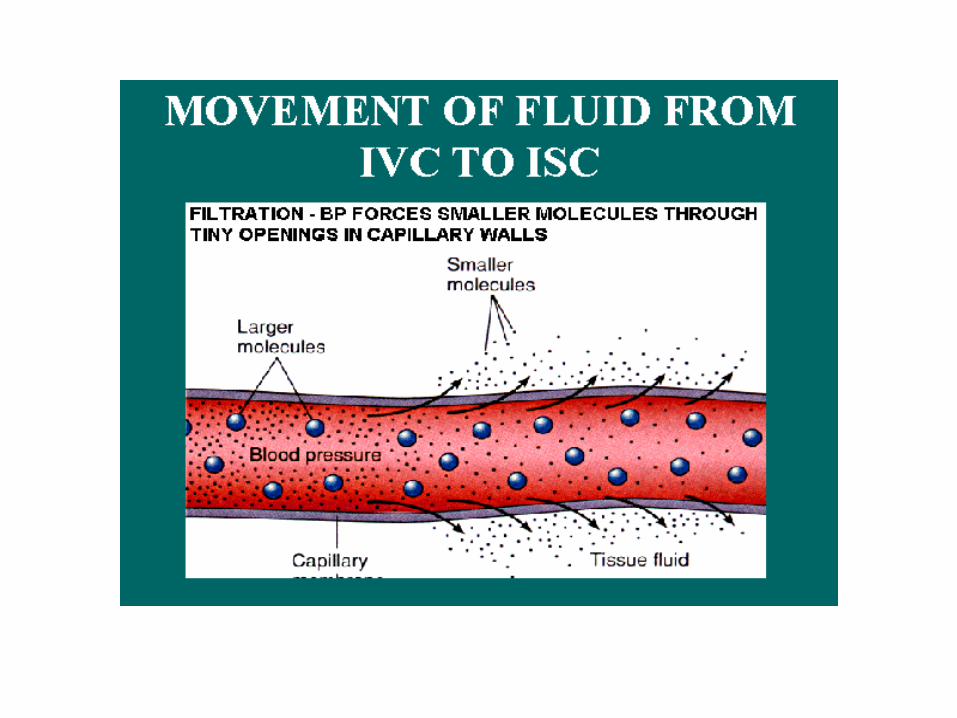
Fluid Movement Between Compartments

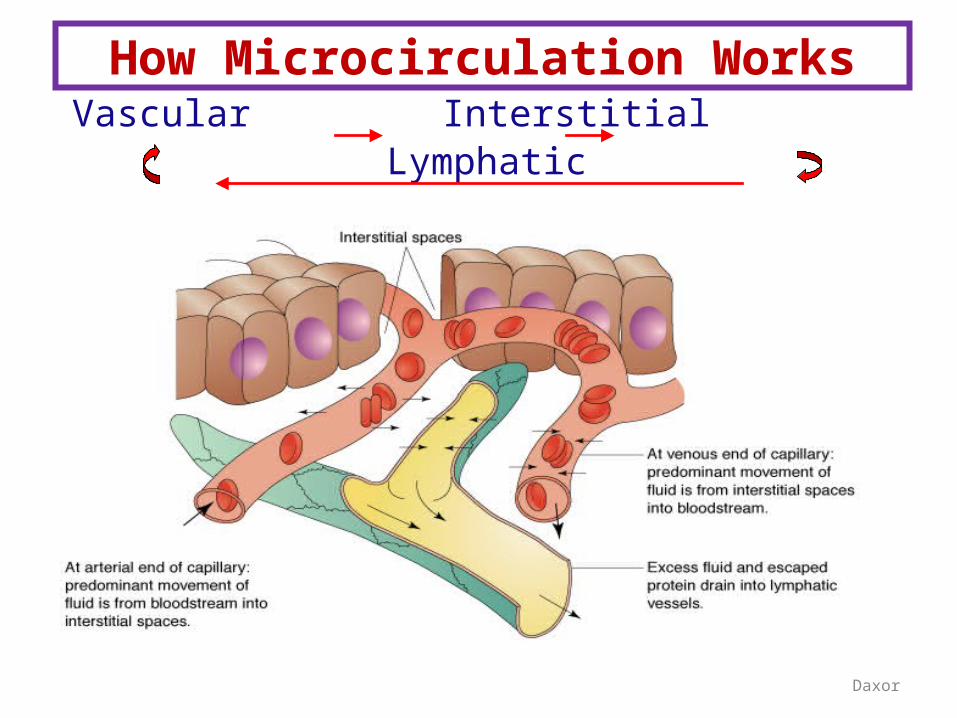
How Microcirculation Works
Daxor
Vascular Interstitial Lymphatic
The Lymphatic System Is a network of conduits that carry a clear fluid called lymph. It also includes the lymphoid tissue that the lymph travels through. Lymphoid tissue is found in many organs, particularly the lymph nodes, and in the lymphoid follicles associated with the digestive system such as the tonsils. The system also includes all the structures dedicated to the circulation and production of lymphocytes, which includes the spleen, thymus, bone marrow and the lymphoid tissue associated with the digestive system.
The dissolved constituents of the blood do not directly come in contact with the cells and tissues in the body, but first enter the interstitial fluid, and then the cells of the body. Lymph is the fluid that is formed when interstitial fluid enters the conduits of the
lymphatic system. The lymph is not pumped through the body like blood, it is moved predominately by the contractions and movements of skeletal musclesThe lymphatic system has three interrelated functions. It is responsible for the removal of interstitial fluid from tissues. It absorbs and transports fatty acids and fats as chyle to the circulatory system. The last function of the lymphatic system is the production of immune cells, such as lymphocytes, including antibody & producing monocytes. Diseases and dysfunction/obstruction of the lymphatic system can cause swelling , edema and other symptoms. Problems with the system can impair the body's ability to fight.

The Lymphatic System

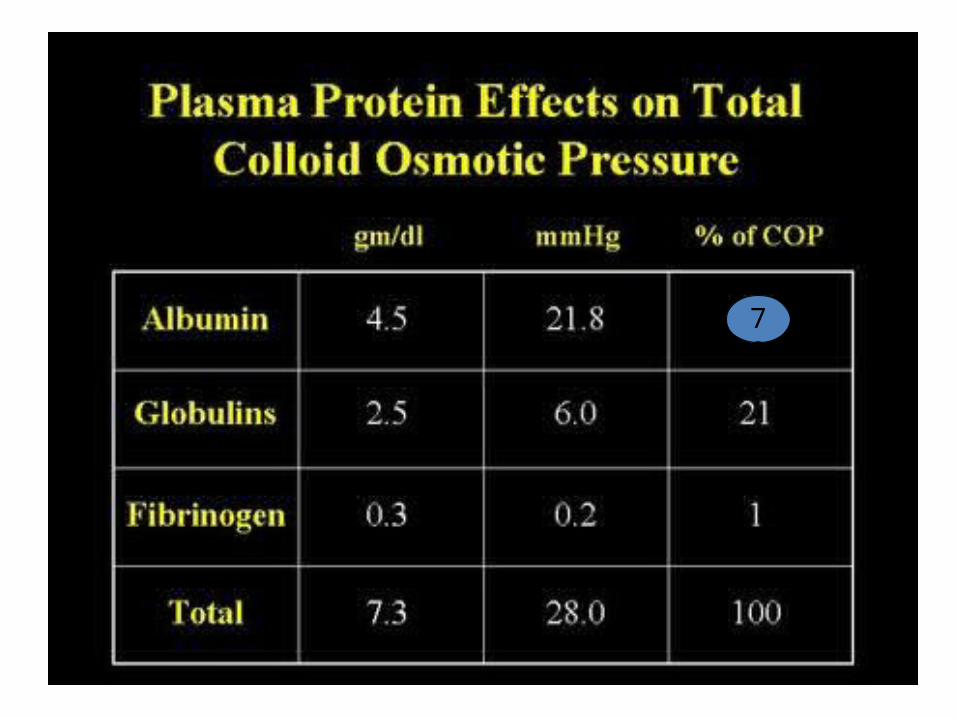
Plasma Protein Effects on Total Colloid Osmotic Pressure (COP)
Albumin 4.5 21.8 78
Globulins 2.5 6.0 21
Fibrinogen 0.3 0.2 1
Total 7.3 28.0 100
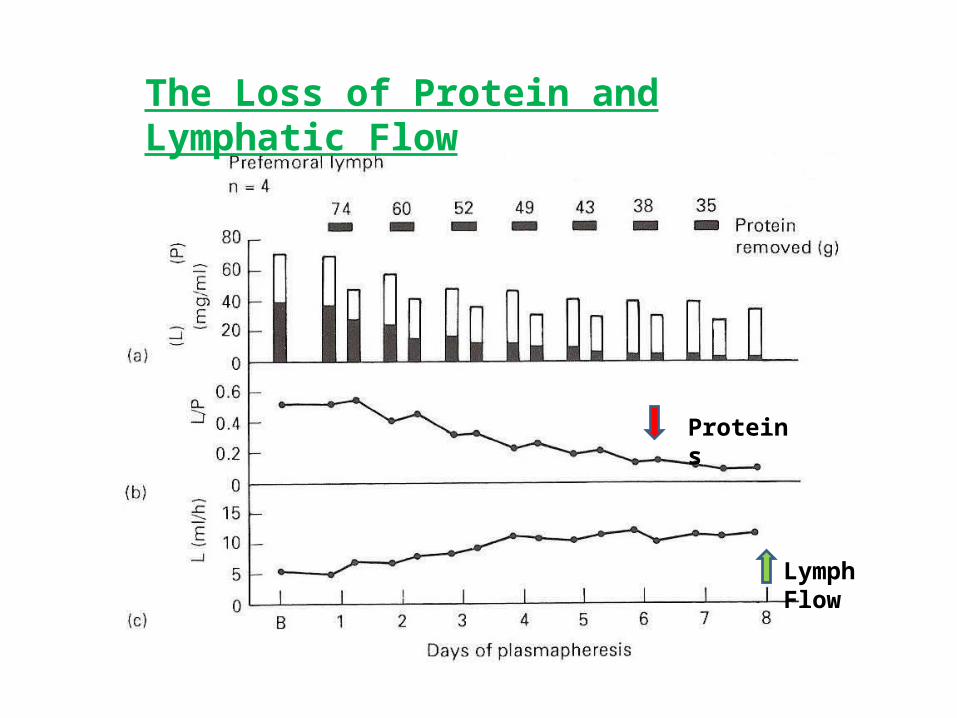
The Loss of Protein and Lymphatic Flow
Proteins
Lymph Flow
Edema:Edema: Most common clinical manifestation of an Imbalance of forces at the capillary wall
Excess accumulation of fluid in the interstitial space that has not been readsorbed into capillaries or taken up by the lymphatics
Causes include• Obstruction • Permeability or change in reflection coefficient
Increased protein permeability results in an imbalance – Occurs in trauma, thermal injury, inflammation– Life threatening manifestations - endotoxic shock, ARDS
• Plasma Protein– Reduction in circulating plasma proteins,
especially albumin!– Liver dysfunction, malnutrition, or acute alteration of fluid status
• Albumin attenuates extravasation of fluid out of intravascular space to interstitial space
• Capillary pressure62
Albumin – Physiological role• Major functions
– Most abundant protein in plasma (69 kDa)– +/- 80% of plasma colloid osmotic pressure Normal COP is 18-22 mmHg (Hemodilution really drops it)– Transport and sequestration of bilirubin– Transport of fatty acids, hormones, vitamins, enzymes, drugs
(Warfarin, Diazepam, Digoxin, NSAIDS, Midazolam, Thiopental and others)
– Antioxidant and Free Radical Scavenger effect– Inhibit Endothelial Cell Apoptosis and may influence the
Microcirculation by modifying the capillary permeability – Buffer in Acid Base Balance (fixes to H+ ions)– No Maximal Dose and No Effect on Hemostasis
78
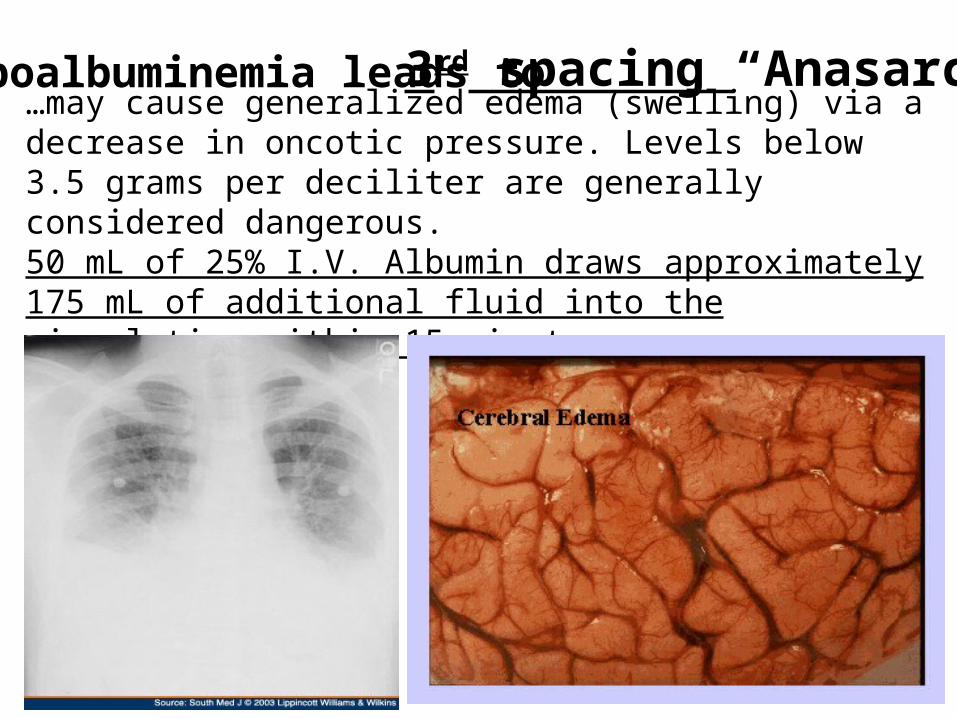
…may cause generalized edema (swelling) via a decrease in oncotic pressure. Levels below 3.5 grams per deciliter are generally considered dangerous.50 mL of 25% I.V. Albumin draws approximately 175 mL of additional fluid into the circulation within 15 minutes
Hypoalbuminemia leads to 3rd spacing “Anasarca”
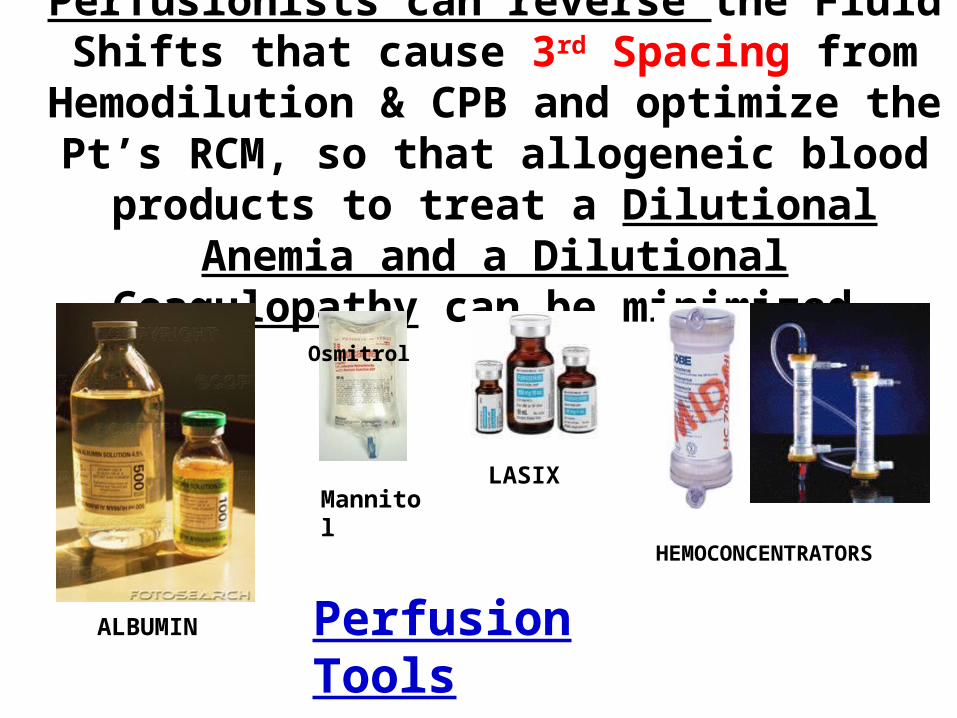
Perfusionists can reverse the Fluid Shifts that cause 3rd Spacing from Hemodilution & CPB and optimize the Pt’s RCM, so that allogeneic blood
products to treat a Dilutional Anemia and a Dilutional Coagulopathy can be minimized.
ALBUMIN
Osmitrol
LASIXMannitol
HEMOCONCENTRATORS
Perfusion Tools

Nurses & The ICU Care Team
Maintain NormothermiaMicro-sampling as little as possible
Rely on Oximetry instead of draws
Careful and judicious use of volume as neededPressors instead of volumeAlbumin instead of crystalloidsDiuretics if necessaryExtubate ASAP !No “Drive-by Transfusions” from on-call staff !
Back to the players! ------
POST-OP

Hospital AdministratorsGet to know them on a personal basisSuggest the benefits of a Blood Mgmt PrgmGet them involved in Blood Management!Look at using Consultants: Infonale’, HemoConcepts, Strategic Blood Mgmt.Encourage trials of New Equipment / DrugsFind a Champion for Blood Management !Show them the facts in $$$ savings for all!

Other Things You can Do!
Join AmSECT & get involved with the PBM Taskforce !Take the PBMS exam & be a leader in your Hospital.Join the AABB, SABM, NATA or PNBC
These are finely tuned international organizations solely focused on better blood management and improved care!
Surf the web & read current articles and share them with other members of the cardiac team (leave around).Get on your Hospital’s Transfusion Practices committee and make a difference (Go to the monthly meetings).Find and support a Champion MD who wants to change the paradigms of tx’s in your hospital’s Cardiac team.Work as a team that’s focused on improvement of care!

More Things You can Do!
Visit these sites and learn more!NoBlood.org
Bloodless Medicine Research (Univ of Pisa)
SABM (Society for the Advancement of Blood Mngmt)
NATA (Network for Advancement of Tx Alternatives)
PNBC (Physicians & Nurses for Blood Conservation)
Medical Society for Blood Management
Strategic Blood Management
Mybloodfirst.com (Excellent site for Perfusionists)
Get Involved and Change the Paradigm of Blood Use!
Take Home Message of …….Blood Management Principles
• Multidisciplinary Communication is Jugular• Find or become a champion in this effort!• Maximize Preoperative Red Cell Mass• Correct any Coag disorder prior to Sx• Minimize blood loss in Sx (this is essential !)• Avoid Allogeneic Tx (balance need vs risk)• Salvage Autologous Whole Blood first then use alternatives
if necessary• If a Transfusion is necessary: use safest, freshest and most
effective product available (wash it !)• Remember you can’t start saving blood until you actually start saving blood!

But most Importantly remember! “If its not yours its an Organ Transplant” with consequences, so
try and do your best to avoid it!Your decisions effect the patient for the rest of their life!

Thank you for your time!
Questions?