Embed Size (px)
DESCRIPTION
Blok Elektif prognostik.pptx
Citation preview

PrognosisEpidemiologi Klinik

• Answers questions about a patient's future health, life span and quality of life in the event one chooses a particular treatment option
- Example: find how would the quality of life change for a patient who undergoes surgery for prostate cancer
Prognosis

Prognosis studies
• Prediction• Cohort studies of “risk” (patient)• What are the consequences of having
disease• Prognostic factor → predictor • Affect of illnes
– Die– Pain– Ability– Work– Actifities

Prognosis Importance
• Secondary Prevention• Life Expectancy• Patient Comfortable• Disease management:
predictor test, treatment, rehabilitation+Wallahu a’lam bishowab

Disease prognosis type
• Course disease – Medical treatment
• History of natural disease– Without treatment

Zero time
• Beginning Observation• Inception cohort • “Simillar” for all subject
Inception cohort
• Cohorts should be observed starting from a point in time called zero time.
This point should be described clearly and be at a well-defined point in the course of disease - for example the onset of symptoms, time of diagnosis, beginning of treatment - for each patient.

Inception cohort
• For studies of prognosis the term inception cohort is used to describe a group of people who are assembled near the onset (“inception”) of disease.

• If observation is begun at different points in the course of disease for the various patients in the cohort, description of their subsequent course will lack precision and the relative timing of such events as recurrence or death would be difficult to interpret or would be misleading.
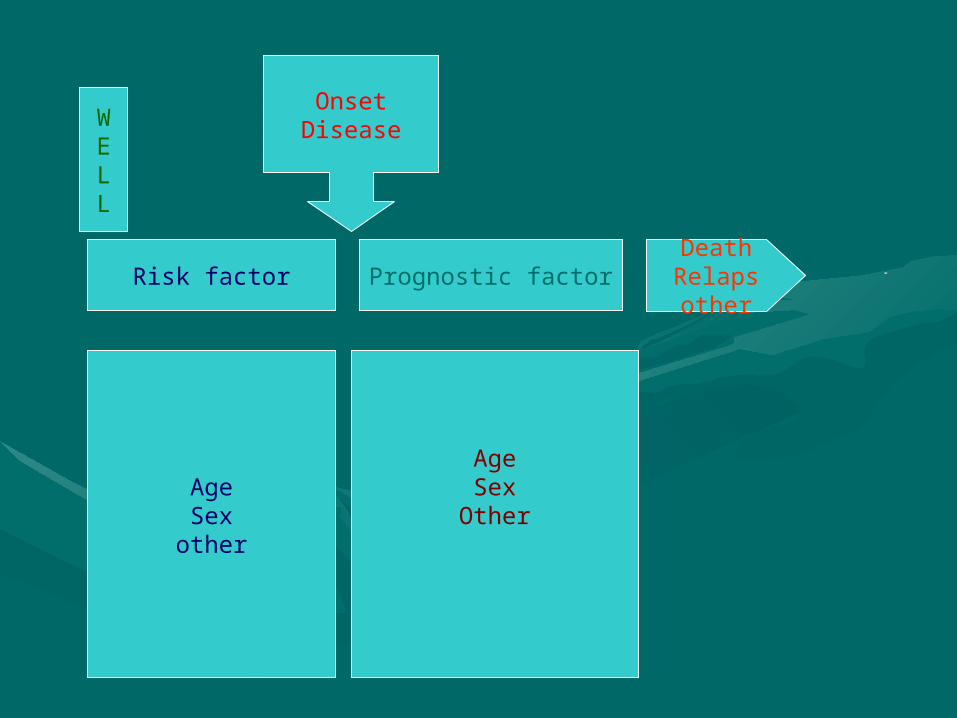
Risk factor Prognostic factor
AgeSex
other
AgeSex
Other
WELL
OnsetDisease
DeathRelapsother

Differences between risk and prognosis
• A distinction should be made between factors associated with an increased risk of developing a disease (risk factor) and those that predict a worse prognosis once the disease is present (prognostic factors).

Myocardial infarction
• Risk factors– Age– Male– Cigarette smoking– Hypertension– LDL/HDL
→ to become AMI

Myocardial infarction
• Prognostic factors– Age– Male– Anterior infarction– Hypotension– Ventricular arrhythmia– CKMB level
→ to become sudden death

Out come
• Death• Disease• Discomfort• Disability• Dissatisfaction

Outcome• Sebaiknya berorientasi pd pasien
– Harapan hidup– Rasa nyeri– Kecemasan– Aktifitas harian
• Pengamatan yang “ilmiah” meski terkait dengan klinis namun tidak dirasakan secara langsung oleh pasien :– Ukuran tumor– Perubahan biokimia– Perubahan serologi
Out come
• Quality of life• Health status• Functional status

Rates commonly used to describe prognosis
• 5 years survival• Case fatality• Disease spesific mortality• Response• Remission• Reccurence
Some end points in the course of disease
• Cure• 5 years survival• Death• Response (Percent of patients showing
some evidence of improvement following an intervention).
• Remission (Percent of patients entering a phase in which disease is no longer detectable)
• Recurrence (Percent of patients who have return of disease after a disease free interval)

Approaches used to describe the prognosis
of disease• Case Fatality - Percent of patients
with a disease who die of it.
Approaches used to describe the prognosis
of disease• Five-year survival - Percent of
patients surviving 5 years from some point in the course of the disease.
Approaches used to describe the prognosis
of disease• Median survival time - Time at which
50% of patients still alive.

Approaches used to describe the prognosis
of disease• Person years - The sum of the
number of years of observation in each individual in the study
Approaches used to describe the prognosis
of disease• Observed survival - Life tables or
Kaplan Meier plots.

Survival curves
0102030405060708090
100
Time (years)
Probability of survival (%)
Line 1

Interpretasi kurva survival rate
• Sumbu vertikal mrp kemungkinan survival• Sumbu horisontal mrp periode waktu
pengamatan• Prosentase: masih hidup dibagi total
penderita• Sampel DO dikeluarkan dari
kohort→perhitungan prosentase, jmlh penyebut dikurangi yg DO
• Amati kecuraman/kelandaian kurva


The next step would be to determine the best study design
needed to answer the clinical question.

1. Cohort study• Answers prognosis, etiology, prevention
questions• Cohorts are defined populations that, as a
whole, are followed in an attempt to determine distinguishing subgroup characteristics.
• Researchers identify and compare two groups over a period of time.

At the start of the study, one of the groups has a particular condition or receives a particular treatment, and the other does not.
At the end of a certain amount of time, researchers compare the two groups to see how they did.
Cohort study
2. Case Control study
• Answers prognosis, etiology, prevention questions
• Identifies patients who already have the outcome of interest and control patients without that outcome, and look back to see if they had the exposure of interest or not.

3. Case series & Case Reports
• Answers prognosis, etiology, prevention questions
• Consist either of collections of reports on the treatment of individual patients, or of reports on a single patient.

• The best design of study to answer a prognosis question is a prospective cohort study.

Bias penelitian kohort• Adakah kemungkinan bias• Apakah benar terjadi bias• Berapa besar pengaruh bias• Assembly bias
– Terdapat perbedaan karakteristik sejak awal selain faktor prognosis yang diamati
– Bias kepekaan: perbedaan kepekaan antara kelompok yang dibandingkan
• Bias Migrasi– Subyek meninggalkan kohort– DO

Important sources of selection bias include:
• Non random sample selected e.g.. volunteers, workers, hospital patients
• Hard to trace people are omitted• Large number of refusals in selected
population• Large number of people dropping
out of the study

Diagnostic (measurement or information) bias can be introduced because of:
• Subject variation - physiological, psychological or induced
• Observer variation - intra and inter observer variation, lack of independence in the observer (blinding) or error in the administration of the test
• Limitations of the method - I.e. the test may be inappropriate, the method may be intrinsically unreliable or there may be an error in the administration of the test.

• Many reports on prognosis in the medical literature come from hospitals and academic centres and patients seen in these centres are not a representative sample of patients who are seen in the community.
• For example they may be referred if they are not responding to treatment or they have a troublesome complication of their diseases.

Minimalisasi Bias
• Blind– Pengamat tidak mengetahui kelompok
subyek/pasien– Penetapan outcome scr cermat dan
blind• Upaya memberi perlakuan yg sama
pd msg2 kelompok

Methods of controlling bias
• Randomization• Restriction• Matching• Stratification• Simple adjustment• Multiple regression

Randomization
• Assign patients to groups in a way that gives each patient an equal chance of falling into one or the other group.

Restriction
• Limit the range of characteristics of patients in the study
Matching
• For each patient in one group select one or more patients with the same characteristics (except for the one under study) for a comparison group.

Stratification
• Compares rates within subgroups (strata) with otherwise similar probability of the outcome.

Simple adjustment
• Mathematically adjust crude rates for one or a few characteristics so that equal weight is given to strata of similar risk.

Multiple regression
• Adjust for differences in a large number of factors related to outcome using mathematical modelling techniques.
Insidensi prognosis hrs disertai komponen
• Zero time• Definisi kejadian• Jumlah Populasi yang berisiko• Waktu pengamatan

Critically appraising a prognosis paper

Validity• There was a representative and
well defined sample of patients at a similar point in the course of the disease
• There was follow-up sufficiently long and complete?
• the objective and unbiased outcome criteria were used
• There was the adjusment for important prognostic factor

the results• How large is the likelihood of
outcome events in a specific period of time?
• How precise are the estimates of likelihood?

• Will the results help me in caring for my patients
– Were the study patients similar to my own
– Will the results lead directly to selecting or avoiding therapy
– Are the results useful for reassuring or counselling patients