Embed Size (px)
Citation preview

SPECIAL TOPIC
Blindness following Cosmetic Injections ofthe Face
Davide Lazzeri, M.D.Tommaso Agostini, M.D.
Michele Figus, M.D., Ph.D.Marco Nardi, M.D.
Marcello Pantaloni, M.D.Stefano Lazzeri, M.D.
Pisa and Florence, Italy
Background: Complications following facial cosmetic injections have recentlyheightened awareness of the possibility of iatrogenic blindness. The authorsconducted a systematic review of the available literature to provide the bestevidence for the prevention and treatment of this serious eye injury.Methods: The authors included in the study only the cases in which blindnesswas a direct consequence of a cosmetic injection procedure of the face.Results: Twenty-nine articles describing 32 patients were identified. In 15 pa-tients, blindness occurred after injections of adipose tissue; in the other 17, itfollowed injections of various materials, including corticosteroids, paraffin, sil-icone oil, bovine collagen, polymethylmethacrylate, hyaluronic acid, and cal-cium hydroxyapatite.Conclusions: Some precautions may minimize the risk of embolization of filler intothe ophthalmic artery following facial cosmetic injections. Intravascular placementof the needle or cannula should be demonstrated by aspiration before injection andshould be further prevented by application of local vasoconstrictor. Needles, sy-ringes, and cannulas of small size should be preferred to larger ones and be replacedwith blunt flexible needles and microcannulas when possible. Low-pressure injec-tions with the release of the least amount of substance possible should be consideredsafer than bolus injections. The total volume of filler injected during the entiretreatment session should be limited, and injections into pretraumatized tissuesshould be avoided. Actually, no safe, feasible, and reliable treatment exists foriatrogenic retinal embolism. Nonetheless, therapy should theoretically be directedto lowering intraocular pressure to dislodge the embolus into more peripheralvessels of the retinal circulation, increasing retinal perfusion and oxygen deliveryto hypoxic tissues. (Plast. Reconstr. Surg. 129: 995, 2012.)CLINICAL QUESTION/LEVEL OF EVIDENCE: Risk, V.
Facial soft-tissue augmentation and rejuvena-tion procedures using various injections offiller materials are widely performed for cos-
metic enhancement because of their highly pre-dictable, convenient, and pleasing outcomes.1,2 Inrecent years, complications following facial cos-metic injections have heightened awareness of thepossibility of iatrogenic visual loss.3–31 Neverthe-less, transitory and permanent blindness has fol-lowed routine aesthetic injection of the face dur-ing which a serious injury is not expected.3–31
We reviewed and examined the influences ofinjection pressures; material type; and needle,
cannula, and syringe size in causing retrogradeflow of the substance to understand the conditionsunder which retrograde flow can lead to retinalcirculation embolism and blindness. We sought toelucidate risk factors for retinal vascular occlu-sion in addition to the cause, prevention, andtreatment options following cosmetic injectionsinto the face that resulted in blindness or severevisual disability, and we hope to provide a usefulguide for physicians who perform these cos-metic procedures.
PATIENTS AND METHODSWe reviewed the available literature regarding
the occurrence of blindness following injectionsFrom the Plastic and Reconstructive Surgery and Ophthal-mology Units, University Hospital of Pisa, and the Maxil-lofacial Surgery Unit, University of Florence.Received for publication September 12, 2011; accepted Oc-tober 5, 2011.Copyright ©2012 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e3182442363
Disclosure: There are no financial conflicts orinterests to report in association with the content ofthis article.
www.PRSJournal.com 995

of fillers of the face. Data were identified bysearches in MEDLINE, the Cochrane database,Google and Google Scholar, Current Contents,and PubMed. We used the search terms “blindnessafter steroid injection,” “blindness after fat injec-tion,” “blindness after facial injections,” “blind-ness after sclerotherapy,” “blindness after cosmeticmedicine,” “ischemic optic neuropathy after injec-tion of the face,” “emboli facial filler,” “arterial oc-clusion after soft tissue filler,” “blindness after facialfiller,” and “arterial occlusion after facial filler.” Allcases of blindness or visual impairment that were nota direct consequence of an injection procedure intothe facial skin were excluded, as were those in whichblindness was not produced by retinal or retinalbranch artery occlusion. Thus, cases of blindnessfollowing intraturbinate steroid injections,32–36 anes-thetic injections into the nasal septal mucosa,37–40
oral and palatal mucosal injections,41 and tonsillarinjections42,43 were excluded. A single case of visualimpairment subsequent to the use of nasal decon-gestant was also excluded.44 All articles that de-scribed cases in which facial injection had no purecosmetic aim, such as sclerotherapy of vascularlesions45–51 and corticosteroid injections for the treat-ment of chalazia,52,53 were excluded.
RESULTSUsing strict a priori criteria for our review, we
identified a total of 29 articles representing 32cases.3–31 We divided patients into two groups: thefirst group included patients (n � 15)3–15 diag-nosed with blindness following fat injection of theface for cosmetic reasons, and the second groupincluded patients (n � 17)16–31 diagnosed withtransitory or permanent blindness after facial aes-thetic injections of other materials. The results ofour review are summarized in Tables 1 and 2.
Fat Tissue Injection GroupA review of the literature revealed a total of 15
reports of blindness following cosmetic facial fattissue transfer3–31 (mean age, 40.0 � 8.0 years;range, 24 to 49 years), including 11 women3–7,10–15
and two men.7,8 In two cases, no demographic datawere available (Table 1).9 Three patients receivedautologous fat injections into the lower third ofthe face (nasolabial folds,6,13 lips, and chin).9 Inseven cases, the site of injection was the upperthird of the face, including the forehead,4,5,14
glabella,5,10,11 and nasal bridge,8 and in three cases,fat tissue was transferred to the mid third of theface (cheek,9 periorbita,7 and left side of the
nose15). In the remaining two cases, fat tissue wasgrafted to multiple regions of the face.9,12
Procedural details of the cannula, syringe, andneedle used were available in only three articles. A10-ml syringe was used twice: once with a 20-gauge(0.812-mm) needle and once with a 16-gauge (1.291-mm) sharp needle.9 In one case, a 20-ml syringe wasused with a 2-mm-diameter cannula.7
In all cases described,3–15 the signs and symptomsof visual adverse effects were evident immediatelyfollowing the injection, characterized by complaintof excruciating pain and a sudden blackout of theinvolved eye. Three cases5,7,10 presented with furtherneurologic complications caused by cerebral vesselembolus. Information such as history, family history,and other physical findings was not available for anycases in this group.3–15
In nine cases, no information about the treat-ment was available.3–6,8–10 In six cases, therapy (oc-ular massage,7 carbon dioxide rebreathing,7 hyper-baric oxygen therapy,7,12 oral and intravenouscorticosteroids,11–14 antiplatelet drugs,11 and fibrino-lytic agents12,15; or mechanical thrombolysis15) wasadministered without effects. Neither the treatednor the untreated patients had any return ofvision.3–15
Other Injected Materials GroupSeventeen patients16–31 (15 women and two
men; mean age, 38 � 11.5 years; range, 24 to 65years) who suffered transitory (three cases)18,26,29 orpermanent (14 cases)16,17,19–25,27,28,30,31 blindness fol-lowing the injection of materials other than adiposetissue were identified (Table 2). The injected sub-stances included corticosteroids16,18,21 and filler ma-terials such as paraffin,17 silicone oil,19,22,28 bovinecollagen,20,23,30 polymethylmethacrylate,24,25 hyal-uronic acid,26,31 and calcium hydroxyapatite.29 Thenose (root,18,22,29 dorsum,21,22,25,29 and tip30,31) and thescalp16,18 were the most frequently injected sites, withseven and three cases, respectively; whereas the re-maining seven cases involved the forehead,17,23
glabella,24,27 glabella and cheek20,26 (two cases foreach area), and temple area28 (one case). The sy-ringe and needle used were described in only onecase (25-gauge needle,21 0.455 mm).
Several different individualized treatmentswere attempted in this group of patients. Systemiccorticosteroids29,31 were administered in two patients,diuretic agents (carbonic anhydrase inhibitors19,26,28)were used in three cases, and vasodilators19 and anti-aggregant drugs (antiplatelet agents,30 aspirin31) wereused in one case each. An alternative approach such asocular massage16,19,28 was attempted in only three
Plastic and Reconstructive Surgery • April 2012
996

cases. Surgical treatment, specifically, anteriorchamber paracentesis, was attempted in just onepatient.28 Data on local and systemic treatmentswere not available in nine patients.17,18,20,22–25,27
Only three patients recovered their sight.18,26,29
One patient recovered sight 5 minutes after in-jection of corticosteroids for alopecia areata, butdetailed information about the treatment was notavailable.18 In another case,26 vision recoveredcompletely and the visual field defect improvedafter prompt administration of acetazolamide(500 mg). A healthy 25-year-old man had com-plete recovery of visual acuity, oculomotor nervepalsy, and skin necrosis after treatment with oraland topical corticosteroid tapers,29 although hisdilated pupil did not improve. Permanent visualloss without light perception persisted in all theremaining patients regardless of the type of treat-ment attempted.16,18,19,21–25,28,30,31 In three cases,outcomes were not available.17,20,27
DISCUSSIONPathophysiology
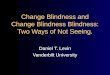
Central retinal artery embolization is relatedto the retrograde arterial displacement of the in-jected products from peripheral vessels into theophthalmic arterial system proximal to the centralretinal artery and follows the subsequent anteriormovement of the injected substance (Fig. 1). Thismay occur when the wall of a distal branch isaccidentally perforated by the injecting needle orcannula. In this case, the force of the injectionused for the product delivery exerted on theplunger of a syringe can significantly expand thesearterioles many times their normal caliber and cancause retrograde flow. Once an injection pressurehigher than systolic arterial pressure is applied,33,54
the injected material displaces the arterial bloodand travels proximally past the origin of the retinalartery. When the plunger is released, the arterialsystolic pressure then propels the resulting col-umn of material into the ophthalmic artery and itsbranches. Although larger particles can blocklarger and more consequential vessels, ophthal-mic artery and central retinal artery blockage canfollow wedging of a very small amount of materialin the retinal artery.
Just as the pressure exerted during injectionmay push a column of filler into the ophthalmicartery, a higher injection pressure may cause theretrograde migration of the column in the inter-nal carotid artery, permitting cerebrovascular em-bolization and stroke.30,50 Discoloration and ne-crosis of the facial skin and cerebral ischemia after
filler injection have the same pathophysiologicmechanism.55–64 Ocular circulation embolizationrequires the concurrent coexistence of three fac-tors, including the retrograde flow caused by highinjection pressure and a sufficient amount of ma-terial delivered into the vessel.54,65,66
The injection of the filler into an artery will causeretrograde flow if the injection pressure is greaterthan the sum of the systolic arterial pressure and thefrictional forces caused by viscous flow pressuredrops within the vessel. A mean pressure drop fromthe eyelid to the apex of the orbit is calculated to beapproximately 23 mmHg at a mean flow rate of 4ml/minute, assuming an axial distance to the medialorbit of 4.5 cm and a lumen diameter of 0.05 cm foran arteriole.54,65–67 The calculated resistance to flow68
(8L�/pr4) is less within a terminal artery than incapillaries69,70; thus, the injected material will flowpredominantly in the direction of least resistance. Asthe distance between the injection site and the ret-inal circulation increases, higher injection pressuresare required to generate retrograde flow until theophthalmic artery.
Retrograde flow caused by high injection pres-sure may lead to retinal embolism only when a suf-ficient amount of product is propelled into the ves-sel. The proximity of the injection site to the orbitalso modulates the probability of symptomatic ob-struction: injections closer to the orbit increase theprobability that a meaningful volume of injectedfiller will gain access to the ophthalmic artery prox-imal to the central retinal artery. Egbert et al. bril-liantly demonstrated this concept.54 Occlusion of anourishing arteriole of the retina proximal to thecentral retinal artery would theoretically require theminimum amount of material to occlude the lumenand, subsequently, the vessel’s blood flow. A volumeof 0.01 ml should occlude an arteriole 4.5 cm fromthe medial orbit with a diameter of 0.05 cm.54,67
However, this estimation is not realistic because itdoes not adequately address the complexity of theorbital circulation web and the many nourishingvessels branching from the ophthalmic artery67 orthe exact location of the injection site. These com-plex elements, particularly when combined with theunpredictable dispersion of the product duringtravel, preclude an accurate calculation of the exactvolume of injected material required to cause ocularembolization.
The risk of retrograde flow caused by high in-jection pressure should not be avoided by adjustingthe size of the needle and the syringe. The plungerof a 50-ml syringe has a greater cross-sectional areathan the plungers of smaller syringes and shouldtherefore theoretically allow lower pressure injec-
Volume 129, Number 4 • Blindness after Facial Cosmetic Injection
997

Table 1. Review of 15 Cases of Visual Loss after Facial Cosmetic Injection of Fat Tissue
ReferenceAge(yr) Sex
AestheticProcedure(s)
InjectingPhysician
Diameter/Size ofthe Cannula/Needle
(Gauge or mm)
Complaint of SymptomsProcedure/Symptoms
Interval
Teimourian, 19883 45 F Fat grafts to improve glabellarfrown lines
Plastic surgeon N/A Immediately: loss of visionand excruciating painin the RE
Dreizen and Framm,19894
44 F Several milliliters ofautologous fat injection intothe forehead to removefacial wrinkles
Plastic surgeon N/A Immediately: severe righthemicranial pain andtotal RE loss of vision
Egido et al., 19935 47 F Autologous fat injection intothe forehead area
N/A N/A During the injectiona sudden, severeperiocular pain withcomplete visual lossin RE
Lee et al., 19966 42 F 0.5 ml of autologous fattransplantation to hernasolabial groove
Plastic surgeon N/A During the injection:headache and dyspnea,irritability, and felt inan unconscious state
Feinendengen et al.,19987
45 M Autologous fat injection intothe nasolabial folds, lowerlip and chin
N/A 20-ml syringe and 2-mm-diameter cannula
7 hr later: global aphasiaand mild rightsensorimotorhemiparesis
CT and MRI: infarction ofthe temporoparietalregion of the left MCA
47 F Autologous fat injection intothe periorbital areas tocorrect crow’s feet
N/A N/A Immediately: LE pain andviolent headaches;complete flaccid righthemiplegia, globalaphasia and deviationof the head and eyestoward the left
Danesh-Meyer et al.,20018
43 M Autologous fat injection onthe left side of the bridge ofthe nose (0.5 ml), eachnasolabial fold (3 ml each)and the upper and lowerlips (3 ml)
N/A N/A Within 10 minutes: eyeand head pain,disorientation, andaphasic with righthemiparesis
Coleman, 20029 N/A N/A Injection of 3 ml ofautologous fat into thecheek to fill a smalldeficiency
Unspecifiedoperatingsurgeon
10-ml syringe with a 20-gauge Angiocathneedle
After recovering fromgeneral anesthesia:unilateral blindness
N/A N/A Fat injection of 0.5 ml in eachoral commissure and lateralcanthal area, 0.25 ml ineach nasojugal trough, and1.5 ml into a transverse scarand wrinkle in the forehead
Unspecifiedoperatingsurgeon
A 16-gauge sharp needlefrom a 10-ml syringewith the assistance of aDispos-a-jectmechanical gun
During the injection ofthe forehead: unilateralblindness andexcruciatinghemicranial pain
Plastic and Reconstructive Surgery • April 2012
998

Table 1. (Continued)
RiskFactors
ImmediateOcular
SituationPathogenesis/
Diagnosis
Time WhenTherapyStarted Therapy Outcomes
N/A N/A Retinal arterial occlusionprobably secondary tofat particle embolism
N/A N/A Totally and permanentlyblind in RE
N/A N/A Multiple fat emboliocclusions of distalbranches of theophthalmic artery
N/A N/A On day 75: BCVA RE: nolight perception
BCVA LE: 20/25Fundus: pale ONH and
few scattered retinalhemorrhages, nocherry-red macularspot
No cardiovascularrisk factor
BCVA RE: no light perceptionPupil: nonreactive to light, but
consensual reflex still present;complete left hemiplegiainvolving the lower face
Fundus: pale ONH and severalretinal arteries occluded
Choroidal and retinalinfarction caused by fatembolism and emboliinto the branches of theupper division of theMCA and ophthalmicarteries
N/A N/A On day 21: no lightperception
N/A Left pupil: nonreactive to directlight stimulus and reactive toindirect
Fundus: a cherry-red spot on themacula, marked retinalischemia and multiple emboliin retinal arterioles
FA: decreased caliber of the leftophthalmic artery leading toophthalmic artery insufficiencyand disappearance of theimage of ocular blush
CRAO caused byautologous fat emboli
Not specified Ocular massage, carbondioxide, oxygentherapy
After 1 wk: Recovery ofthe mental status butloss of VA
After 3 mo: No lightperception in LE witha thick fibrousmembrane on theposterior pole andoptic atrophy
Concomitantbilateral neck andface rhytidectomyand liposuction ofthe cheeks; highlevel of TG andlow level of HDL
Fundus: multiple fat emboli in theright retinal and choroidalarterioles
Multiple branch occlusionsof the retinal andchoroidal arterioles byfat emboli
Not specified Not specified On day 3:Fundus: no evidence of
multiple fat embolismsin the retinal andchoroidal arterioles
10-mo follow-up: noreport about ocularsituation
Excision of a Baker’scyst, removal offemoral varices,cosmeticcorrection of theinframammaryfolds, andliposuction of thethighs 4 daysprior; patentforamen ovale
Pupils: symmetricalLeft pupil: weakly reactive to
direct light stimulationFew hours later, areactive and
mydriatic pupilFundus: papilledema and
ischemia of the retina
Multiple branch occlusionsof the retinal artery byfat emboli
Selective angiography:occlusion of left carotidartery with cerebralinfarction
Not specified Not specified On day 1, CT: largehypodensities in theleft frontotemporalarea the next day
After several weeks: norestoration of LE vision
N/A BCVA LE: no light perceptionPupil: amauroticFundus: pale ONH and
widespread retinal whiteningwith visible emboli in severalretinal arterioles; preretinaland intraretinal hemorrhages
Fat embolism to branchesof the left MCA and theophthalmic artery
N/A N/A Over the ensuing 5 days,the LE remained blind;no longer follow-uphas been described
N/A Fundus: an embolus in the centralretinal artery
CRAO Not specified Not specified Follow-up not specified:permanent unilateralblindness
N/A N/A CRAO N/A N/A N/A
(Continued)
Volume 129, Number 4 • Blindness after Facial Cosmetic Injection
999

Table 1. (Continued)
ReferenceAge(yr) Sex
AestheticProcedure(s)
InjectingPhysician
Diameter/Size ofthe Cannula/Needle
(Gauge or mm)
Complaint of SymptomsProcedure/Symptoms
Interval
Yoon et al., 200310 39 F 5 ml of autologous fatinjection into the glabella tocorrect frown lines
N/A N/A 1 minute later: mentalchange, aphasia, andright hemiplegia
Allali et al., 200611 49 F Autologous fat injection intothe glabellar area to treatwrinkles
N/A N/A 24 hr after the aestheticprocedure: a sudden,severe ocular pain withcomplete visual lossin RE
Mori et al., 200712 30 F Cosmetic fat injection intobreasts, nose, and glabellararea
N/A N/A Immediately: nausea,pain, and visual lossin RE
Park et al., 200813 27 F Autologous fat injection intothe right nasolabial fold
Unspecifiedsurgeonoperating ina plasticsurgery clinic
N/A Within 10 minutes:sudden visual loss
Lee et al., 201014 24 F Autologous fat transplantationto her forehead for soft-tissue augmentation in theface
N/A N/A On the day of theprocedure: impossibleto open both eyesbecause of the swellingof her eyelids
Park et al., 201115 39 F Autologous fat injection intothe left side of the nose(dosage not specified)
Plastic surgeon N/A Immediately: sudden painand vision loss in herLE
F, female; RE, right eye; N/A, not available; BCVA, best corrected visual acuity; ONH, optic nerve head; MCA, middle cerebral artery; LE, left eye; FA,fluorescein angiography; CRAO, central retinal artery occlusion; VA, visual acuity; M, male; CT, computed tomography; MRI, magnetic resonance imaging;TG, triglyceride; HDL, high-density lipoprotein; VEP, visual evoked potentials; OAO, ophthalmic artery occlusion; IOP, intraocular pressure.
Plastic and Reconstructive Surgery • April 2012
1000

Table 1. (Continued)
RiskFactors
ImmediateOcular
SituationPathogenesis/
Diagnosis
Time WhenTherapyStarted Therapy Outcomes
None 30 minutes later:LE: midline fixedPupil: dilated and unresponsive to
direct light stimulationCorneal opacityIOP: 0 mmHg
Occlusion of the ocularand facial vessels andbranches of the externalcarotid arteries
— None After 2 days: necrosis ofthe LE
After 4 days: patient died
None Pupil: fixed mid dilatedFundus: retinal ischemic edema with
segmentary occlusions of multiplebranches of the central retinalartery by yellow emboli, serousmacular detachment, absence ofcherry-red macular spot
ONH: pale and edematousPtosis. FA: choroidal and retinal
unilateral occlusion
Multiple BRAOs by fatemboli with posteriorciliary arteriesinvolvement
After morethan 24 hr
Intravenouscorticosteroids andantiplatelet therapy
No visual recovery
N/A BCVA RE: no light perceptionFunduscopy: widespread retinal
whitening and obstruction of theretinal vessels of the fundus withremarkable edema of the entireretina
FA: no filling of the retinal arterioles
OAO Not specified Drip infusion ofurokinase andhyperbaric oxygentherapy
Subsequentadministration ofcorticosteroid
No improvement
None BCVA RE: hand motionRight upper eyelid: slight ptosisPupil: fixed and mid-dilatedFA: multiple whitish patchy lesions
with macular and ONH edemaand deterioration of choroidalcirculation with patchy choroidalfilling
Fundus: absence of a cherry-red spotFlash VEP: no response
Choroidal infarctionscaused by multipleocclusions of the shortposterior ciliary artery
On day 5 Methylprednisolone 1g/day intravenouslyfor 3 days and dosetapering with oraladministration
After 6 mo: no change invision
None Swelling and redness of theeyelids
OAO with infarction of theONH and retina
Not specified(at least 24hr later)
1 g/day intravenousmethylprednisolonefor 3 consecutive days
On the first postoperativeday: visual loss in the LE,decreased sensation onthe forehead and scalp
3 days after BCVA: no lightperception; ptosis;restricted extraocularmotility in all directions
LE: afferent pupillary defectFundus: LE ONH swelling
and widespread retinalwhitening
5 months later:BCVA: no light perceptionFundus: severe retinal
fibrosisNone BCVA LE: no light perception
Corneal edemaNo pupillary reflex, total
ophthalmoplegia, and large-angle(45 prism diopters) exotropia ofthe LE
Fundus: ischemic retina with multipleintraarterial yellowish emboli inthe LE
FA: minimal choroidal perfusion withthe absence of central retinalarterial filling
After 1 day: Corneal edemaFA: complete recanalization of the
ophthalmic artery withvisualization of the choroidal blush
OAO from the proximalsegment with thrombusand flow stagnation inthe distal segment
Some hourslater
Pharmacomechanicalthrombolysis with amicrowire and500,000 IU ofurokinase and 500 �gof tirofiban
6 days later:BCVA: no light perception;
no corneal edema andimproved choroidal andretinal perfusion
17 mo later BCVA: no lightperception
Fundus LE: fibrousmembrane on theposterior pole with alarge region of necrosisin the nasal retina
Complete recovery of ocularmovement
Nasal sectorial iris atrophy
Volume 129, Number 4 • Blindness after Facial Cosmetic Injection
1001

Table 2. Review of 17 Cases of Visual Loss after Facial Cosmetic Injection of Various Substances
ReferenceAge(yr) Sex Aesthetic Procedure(s)
InjectingPhysician
Diameter/Size of theCannula/Needle (Gauge
or mm)
Complaint of SymptomsProcedure/Symptoms
Interval
von Bahr, 196316 25 F 8-ml injection of a suspension ofhydrocortisone into the barespots on the scalp (leftanterior part of the crown, afew centimeters within thefrontal limit of the hair)
Dermatologist N/A During the procedure:pain in the head andin the LE
Lee et al., 196917 50 F Subcutaneous injection ofparaffin on the forehead
N/A N/A Immediately: loss of vision
Baran, 1964* 24 F Injection of hydrocortisonesuspension for alopecia areata
N/A N/A N/A
Baran, 1965* 31 F Injection of methylprednisoloneacetate suspension foralopecia areata
N/A N/A Immediately: transitoryblindness
Shin et al., 198819 30 F Injection of silicone oilsubcutaneously at the root ofher nose
N/A N/A Sudden loss of vision andpain RE of 24-hrduration
Castillo, 198920 34 F Injection of Zyderm collagenimplant into glabellar linesand acne scars in the cheeks
N/A N/A Few minutes: suddenamaurosis
Shafir et al., 199921 37 F Long-acting steroid tosubcutaneous scarring of thedorsum of the nose
Unspecifiedsurgeon
25-gauge needle Within seconds of the lastinjection: no lightperception; nopupillary reflex couldbe elicited
Jee and Lee, 200222 44 F Augmentation rhinoplasty usingliquid silicone
N/A N/A 1 day after injection:acute visual loss in LEand RE hemiplegia
Apte et al., 200323 48 F Intradermal injection of 0.5 mlof Cymetra to improve thecontour of a depressedforehead scar
N/A N/A 10 minutes later: nausea,diaphoresis, and leftside periocular pain
After 30 minutes: blurredvision
Silva and Curi,200424
52 F Aesthetic PMMA injection intothe glabellar area
Plastic surgeon N/A Immediately afterinjection: severe REpain and visual loss
Plastic and Reconstructive Surgery • April 2012
1002

Table 2. (Continued)
Risk Factors Immediate Ocular SituationPathogenesis/
Diagnosis
Time WhenTherapyStarted Therapy Outcomes
Three previoustreatments with thesame substance
Immediately: no light perception;direct pupillary reactionabolished
Fundus: block of several arterialbranches of the retina andchoroid by small deposits of alight substance
On day 1:LE BCVA: “hand motions”LE pupil: relatively wide and very
slightly reactive to direct lightONH: normal; marked ischemic
turbidity on the macula andinterruption of the bloodcolumn in some parts
CRAO Few minuteslater
Massage of the eye On day 9, BCVA:perception of “handmovements” in thetemporal VF only
LE pupil: moderatelyreactive
ONH: slightly paleRetina: white and opaque
in the macular regionFovea: brownish and
surrounded by a yellowzone
4 mo later: unchanged
N/A Immediately: loss of vision CRAO and thrombosisof the ophthalmicvein
N/A N/A N/A
N/A N/A N/A N/A N/A Persistent impairment ofsight
N/A N/A N/A N/A N/A After 5 minutes: return ofvision
N/A BCVA RE: “counting fingers,” REafferent papillary defect
Fundus: pale, partially opacified,edematous retina extendingfrom the ONH toward thefovea; in the center of thiszone a white retinal vessel;edema of RNFL in the inferiornasal margin
CRAO and PCAOs Immediately Digital massage,vasodilators, andacetazolamide
On day 9, BCVA: noimprovement
Fundus: retinal hemorrhageFA: no dye filling of the
white vessel, ONH dyeleakage, zones of retinalischemia
VF examination: inferioraltitudinal defect, centralscotoma, RNFL defect inthe superior temporalregion
N/A N/A N/A N/A N/A N/A
N/A N/A Central retinalembolus andchoroidal occlusion
Immediately Routine treatment forvascular occlusionof the bulb
After 4 yr: no recovery ofvision
N/A N/A CRAO N/A N/A On day 30: development ofright carotid cavernousfistula with right ocularpain
Concomitant injection of1.0 ml of Cymetra tothe bilateral nasolabialregions and 0.5 ml ofCymetra to thebilateral oralcommissure regionsunder a localanesthetic withoutincident
After several hours: BCVA of“hand motions,” papillaryafferent defect, mild ptosis,and exotropia
CRAO and PCAOs N/A N/A 2 mo later,BCVA: light perception;
marked afferent pupillarydefect; mild lefthypertropia andexotropia, without ptosis,large areas of RPEatrophy
FA: large areas of choroidalnonperfusion in theposterior pole andtemporal peripheralretina
None BCVA RE: no light perception;white opacity in the rightcornea and iris atrophy; totalophthalmoplegia
CRAO and PCAOs N/A N/A 10 mo later,BCVA: no light perception;
total rightophthalmoplegia
(Continued)
Volume 129, Number 4 • Blindness after Facial Cosmetic Injection
1003

Table 2. (Continued)
ReferenceAge(yr) Sex Aesthetic Procedure(s)
InjectingPhysician
Diameter/Size of theCannula/Needle (Gauge
or mm)
Complaint of SymptomsProcedure/Symptoms
Interval
Kubota and Hirose,200525
29 F Injection of 0.7 ml of MetaCrillinto the dorsum of the nosewithout local anesthetics
Cosmeticsurgeon
N/A After 15 minutes: ocularpain and a decrease ofvision in RE to “handmotion”
Peter and Mennel,200626
48 M Injection of hyaluronic acid inthe glabellar area and in thecheeks for wrinkles
N/A N/A 1 minute after: partialvisual loss in theinferior half of the VFof his RE
Kang et al., 200727 65 F Injection of a filler into theglabellar area
N/A N/A Sudden visual loss
Tangsirichaipong,200928
36 F Silicone injection in the templearea
N/A N/A Immediately: RE suddenpainful visual loss andheadache
Sung et al., 201029 25 M Calcium hydroxyapatite fillerinjection for noseaugmentation
Dermatologist N/A Immediately:blepharoptosis andorbital pain on theright side
Some hours later: centralnecrosis andsurrounding reddishreticular patternaffecting the righteyelid
Kwon et al., 201030 39 F Injection of collagenous fillermaterial into the left anteriornasal septum for a nasal tip-plasty
An acquaintanceperformedthisprocedureillegally at abeauty salon
A self-manufacturedsyringe
Immediately: completeloss of vision in her lefteye and a headache
Kim et al., 201131 30 F Injection of 0.8 ml of hyaluronicacid in the nasal tip andbridge as an augmentationand contouring
N/A N/A Immediately: visual loss inthe LE
F, female; LE, left eye; N/A, not available; BCVA, best corrected visual acuity; ONH, optic nerve head; CRAO, central retinal artery occlusion;VF, visual field; RE, right eye; RNFL, retinal nerve fiber layer; PCAO, posterior ciliary artery occlusion; FA, fluorescein angiography; RPE, retinalpigment epithelium; PMMA, polymethylmethacrylate; AC, anterior chamber; MRI, magnetic resonance imaging; M, male; BRAO, branchretinal artery occlusion.*Selmanowitz VJ, Orentreich N. Cutaneous corticosteroid injection and amaurosis: Analysis for cause and prevention. Arch Dermatol. 1974;110:729–734.
Plastic and Reconstructive Surgery • April 2012
1004

Table 2. (Continued)
Risk Factors Immediate Ocular SituationPathogenesis/
Diagnosis
Time WhenTherapyStarted Therapy Outcomes
N/A Pupil: dilated but still reactiveOcular motility: restricted on
upward and leftward gaze withtemporary displacement of theeyeball
Blepharoptosis; on day 1, BCVARE: light perception
Biomicroscopy: corneal edema and2� cells in the AC
MRI: orbital inflammation
Direct toxic effectbecause of aforeign bodyreaction andvasculitis secondaryto BRAO
N/A N/A 4-mo follow-up,BCVA RE: no light
perception; full ocularmotility and noblepharoptosis; clearcornea
Fundus: ONH atrophy
Tobacco abuse; nopreviously systemicembolic episodes
BCVA RE: 6/7.5After 24 hr, BCVA RE: 6/6Funduscopy: evidence of an
embolus in the peripheralretinal associated with retinaledema
BRAO of the superiortemporal artery
Immediately 500 mg ofacetazolamide
BVCA: complete recovery;visual field defectimproved
N/A Necrosis of the glabellar area Retinal branch arteryocclusion
N/A N/A N/A
No medical problem BCVA RE: No light perceptionRelative afferent pupillary defectDiffuse retinal whitening, a
cherry-red spot in the macula,vascular attenuation, andboxcar flow in arteries andveins
CRAO for siliconeembolism into thecentral retinalartery
After 2 hr Ocular massage, ACparacentesis, andoral acetazolamide
On day 30: no lightperception
None 8 hr hours later:BCVA RE: hand movementPupil: fully dilated without
reverse afferent pupillarydefect
Right exotropiaSevere AC reaction, including
hyphema, hypopyon, andcorneal edema
PCAOs, choroidalischemia limited inthe nasal area andocclusion of thebranch to theoculomotor nerve
After 8 hr Topical andintravenousantibiotics andtopical steroids,followed by lowdose of taperingoral corticosteroids
After 3 moBCVA RE: 20/20 with
pinholeNo intraocular
inflammation oroculomotor nerve palsy;still fixed dilated pupil
None LE: no light perception, withcomplete opacification of thecornea and iris, completeophthalmoplegia, and ptosis ofthe LE
Fundus photography: multipleBRAOs
MRI: acute cerebral infarction ofthe superior frontal subcortexand subarachnoid hemorrhageof another part of the distalbranch of the middle cerebralartery
Multiple BRAOs On day 3 Low-dose antiplateletagent and a calciumchannel blocker
Blindness
N/A Immediately: strong pain in the leftupper face
BCVA LE: no light perceptionFunduscopy: retina pale and
swollen with a cherry-red spotOn day 2, slit lamp examination:
severe chemosis, edematouscornea, Descemet folds, and irisatrophy
Ultrasonography: severechorioretinal swelling withoutdetachment
Left eyeball movement restricted atall gazes
CRAO On day 2 Intravenousmethylprednisoloneat 1 g/day for 3days and taperedhigh-dose oralprednisolone andaspirin at 100 mg;daily Comfeeldressing
At 6 mo:Complete recovery of the
eyeball movementProgressive exudative and
tractional retinaldetachment at theinferonasal retina causedphthisis bulbi
Volume 129, Number 4 • Blindness after Facial Cosmetic Injection
1005

tions (Pascal’s law71). However, beyond the fact thatthe surgeon’s control over the volume injected isseverely impaired by the use of a large syringe forfine injection of filler materials and fat, injection
with large syringes can result anyway in pressuresgreater than the systolic blood pressure.54 Even theuse of a small-gauge needle does not seem to preventretrograde flow. The decreased pressure resulting
Fig. 1. Schematic drawing that shows the anatomy, distribution, and connectionsbetween the ophthalmic and the facial arterial systems. The supratrochlear arteryis the terminal branch of the ophthalmic artery and exits at the superior and medialcorner of the bony orbit by piercing the orbital septum with the supratrochlearnerve. It runs superiorly into the forehead, where it supplies the integument, mus-cles, and pericranium and maintains numerous anastomoses with the supraorbitalartery and with the contralateral vessels. This is the vessel most likely to be involvedwhen intraarterial injection of fat and foreign material of the glabella and foreheadis responsible for embolization. The supraorbital artery may occasionally be theroute of embolization of injected material. It arises from the ophthalmic artery anddivides into superficial and deep branches that nourish the integument, muscles,and pericranium of the forehead. Its terminal branches anastomose with the su-pratrochlear artery, the frontal branch of the superficial temporal artery, and thecontralateral supraorbital artery. The second terminal branch of the ophthalmicartery, the dorsal nasal artery, may be responsible for transmission of emboli fol-lowing injections low in the glabella or proximal to the nasal root. It anastomoseswith the angular artery, the dorsal nasal artery of the opposite side, and the lateralnasal branch of the facial artery. The facial artery arises from the external carotidartery that supplies the structures of the face. The facial artery passes forward andupward across the cheek to the angle of the mouth, where it arborizes and gives riseto the labial systems and, more distally, to the lateral nasal artery that supplies theala and dorsum of the nose. It further forms anastomoses with its contralateralcounterpart, with the septal and alar branches, with the dorsal nasal branch of theophthalmic artery, and with the infraorbital branch of the internal maxillary. Thefacial artery then ascends along the side of the nose, ending at the medial canthus,where it is named the angular artery. After supplying the lacrimal sac and orbicu-laris oculi, it ends by anastomosing with the dorsal nasal branch of the ophthalmicartery. The angular artery on the cheek distributes branches that anastomose alsowith the infraorbital artery. The facial artery should be considered for embolizationfollowing injections of the cheek, nasolabial folds, and lips.
Plastic and Reconstructive Surgery • April 2012
1006

from the use of a small-gauge needle or cannula doesnot decrease the injection pressure below the sys-temic arterial pressure.54 Furthermore, the initiationof an injection requires an order of magnitude morepressure than does maintenance of flow. Smallerneedle sizes require greater initial pressure to over-come resistance to flow and thus result in higherinitial pressures transmitted to surrounding tissues.54
Obviously, in daily clinical practice, the most com-monly used devices for injecting cosmetic substancesinto the face are 1-, 3-, and 10-ml syringes, in whichthe plunger has a manyfold smaller cross-sectionalarea than the plungers of a 50-ml syringe and shouldtherefore allow higher pressure injections to occur.The use of a smaller syringe even with a small needlewill increase the risk for the physician to exceed thesystolic arterial pressure. Thus, the force with whichthe product is delivered becomes a really importantvariable to control.
TreatmentTo optimize the possibility of fully or partially
regaining normal vision, early recognition and treat-ment are essential for treating ocular circulationemboli. The goal of treatment is rapid restoration ofperfusion to the retina and optic nerve head.48,54,72,73
After 90 minutes, the damage caused by retinal isch-emia becomes irreversible and retinal necrosis oc-curs. Thus, limiting the length of ischemia may allowvarious degrees of recovery.54,74–77 Although currentstandard therapies have not been shown to alter thenatural course of the disease, it should be assumed thatshortening the ischemic period increases the proba-bility of residual visual function.54,74 The recovery pat-tern after branch retinal artery occlusion should besimilar, but remaining visual function is more likely.
Nonsurgical ManagementCurrent treatments may not satisfactorily treat
arterial retinal occlusions caused by fat graft em-boli or foreign materials that are widely used asfacial cosmetic fillers or rejuvenating procedures.The currently available recommendations for retinalembolism54,78 attempt to rapidly reduce intraocularpressure to dislodge the embolus to a downstreamlocation to improve retinal perfusion. Because ourreview identified only two cases with improvementfollowing known treatments,26,29 we cannot recom-mend any treatments as safe or effective.
Anterior chamber decompression with a needleor sharp cutting blade paracentesis results in an in-stantaneous decrease of intraocular pressure.79,80
However, this treatment failed in the case28 includedin the present review. Ocular massage may lower
intraocular pressure and increase arteriolar flow, po-tentially dislodging the embolus, but it has beenineffective in all four of the cases included in thisstudy.6,16,19,28 Intravenous administration of diureticssuch as acetazolamide81 may both increase retinalblood flow and immediately reduce intraocular pres-sure. This approach failed in two patients19,28 but wassuccessful in one case.26 Retinal arteriolar dilationand oxygen delivery to ischemic tissues from oph-thalmic vessels may be encouraged by carbogen (5percent carbon dioxide and 95 percent oxygen)inhalation.82 The only patient6 who underwent car-bogen rebreathing had no substantial recovery of hissight. Although hyperbaric oxygen therapy may the-oretically be beneficial, transportation to thenearest chamber may usurp precious time. Neitherpatient6,12 treated with oxygen therapy improved.Systemic and topical corticosteroids were success-fully administrated in one case, with full recovery ofsight but with a persistently dilated pupil.29 Systemicand local intraarterial fibrinolyses have failed to dis-solve cholesterol or heterologous materials83 as re-ported in four cases.11,12,15,30
In the European Assessment Group for Lysis inthe Eye study,77 a significant improvement in bestcorrected visual acuity in patients with an acute cen-tral retinal artery occlusion was obtained in 60 per-cent of patients at 1 month after a six-step therapyadministered within 20 hours after the ischemicevent. In the present review, improvement after ther-apy was achieved in only two cases (14 percent), bothof which suffered ocular embolism following injec-tion of heterologous material (hyaluronic acid26 andcalcium hydroxyapatite,29 respectively). In the firstcase, partial visual loss in the inferior visual fieldimproved to a best corrected visual acuity of 6/6within 24 hours after immediate administration of500 mg of acetazolamide,26 and in the second case,a best corrected visual acuity of “hand movement”improved to 20/20 at 3 months after topical antibi-otics and steroids, including intravenous antibiotics,were initiated 8 hours after the occlusive event andfollowed by a low-dose oral corticosteroid taper.29 Inthe first case,26 the recovery was attributable to boththe natural history of a branch retinal arteryocclusion82 and to the therapy that could have dis-lodged the embolus peripherally relative to the ret-inal edema. Both effects would have allowed reso-lution of the retinal edema and thus explained thevisual improvement. In the second case,29 the injurywas a posterior ciliary artery occlusion, and the cho-roidal ischemia was limited to the nasal area; thus,the recovery was likely determined by resolution ofthe corneal edema and the severe anterior chamberreaction, which included hyphema and hypopyon,
Volume 129, Number 4 • Blindness after Facial Cosmetic Injection
1007

Table 3. Tips and Techniques to Diminish the Risk of Intravascular Injection
1. Aspiration before injection. As mentioned previously, the small size and collapsibility of facial vessels limits the efficacyof preinjection aspiration for avoiding arteriolar injection*. Some authors* consider this precaution useless because,in several reported cases, aspiration did not identify intraarterial needle placement. It is our opinion, however, thataspiration will at least occasionally demonstrate intravascular placement of the needle and should thus be used. Theneedle should be withdrawn and repositioned if blood appears in the syringe during the aspiration. This precautionmay not be applied easily during fat injection procedures because of the high viscosity of the product and thepossible presence of residual blood within centrifuged fat.
2. Injections should be performed slowly and with the least amount of pressure possible. Thus, even if the tip of theneedle has perforated the arterial wall, the column of filler will not be propelled retrograde in the artery. This may bethe most important precaution for practitioners and has already been generally accepted by several authors†‡§.
3. The tip of the needle should be moved slightly to deliver the filler at different points along a line rather than as asingle deposit. This precaution minimizes the chance of depositing a critical amount of material into an artery even ifthe needle has perforated the arterial wall by limiting the time during which the needle remains within the arteriole.
4. Incremental injections should be fractionated so that any filler injected into the artery can be flushed peripherallybefore the next incremental injection is performed. The surgeon should limit therefore to 0.1 ml of filler regardlessof the filler type†‡§. This stepwise procedure minimizes the risk that a column of filler will extend proximally into theophthalmic arterial system.
5. Although high injection pressures cannot be controlled by the size of the syringe or needle used during injection,small syringes should be preferred to larger ones. As already mentioned previously, a bolus injection technique ismore likely to transmit a column of filler to the ophthalmic artery or the internal carotid system. The use of a high-volume syringe (�10 ml) may increase the probability of this complication because the surgeon cannot easily controlthe volume of the filler delivered.
6. Small needles should be preferred to larger ones. Although their initial pressure is higher and their drop pressure isinsufficient, smaller needles slow injection speed and are less likely to occlude the vessel or block peripheral flow.
7. Repeated treatments with smaller volumes may be preferred to single-stage high-volume injections. Pretreatment withbotulinum toxin type A may help reduce the volume of filler required for cosmesis�.
8. When indicated, the use of recently introduced tools such as blunt, flexible microcannulas and nontraumatic flexibleblunt tip needles should be preferred for filler injection¶. Both the microcannula and the blunt tip needle areinserted into the skin through a hole previously made with a sharp tip needle having the same diameter. Thesetechniques allow facial injection with a limited number of insertion points for the whole face, thus reducing the riskof arterial entry.
9. Either the perforation of an arterial wall or the cannulation of an artery lumen will occur more frequently in avasodilated artery. Thus, procedural risks should be reduced by application of a topical vasoconstrictor prior to fillerdelivery. Some authors†#** recommend local anesthesia with epinephrine to promote vasoconstriction. It can becombined with topical anesthesia or regional nerve block before injection to avoid excessive tissue distortion.
10. When performing autologous fat tissue transfer, sharp cannulas and small cannulas are much more likely to perforatethe wall of an artery and cannulate the artery lumen than are larger, blunt cannulas†.
11. Extensive gentle pretunneling (e.g., moving of the cannula without applying vacuum or pressure) is usuallyadvocated because the delivery of small fat parcels into multiple soft-tissue tunnels allows better revascularizationand results in more predictable and more persistent results. This method may cause a hidden vascular lesion.Thus, it becomes extremely important to allow a low-pressure microdroplet injection technique with bluntcannulas to avoid a dramatically high injection pressure for a highly viscous substance such as fat tissue. Theinjection should be accomplished by delivering very small, noncontinuous amounts of 0.1 ml per pass†. Someauthors emphasize the use of 0.025 to 0.05 ml per tunnel or even less for the periorbital region††.
12. When surgical procedures of the head and neck, such as face lifts and liposuction, are combined with localautologous fat grafting, the risk of ocular arterial system embolism increases, because intravascular delivery of fattissue is easier in pretraumatized soft tissue.‡‡ This condition should be prevented.
*McCleve DE, Goldstein JC. Blindness secondary to injections in the nose, mouth, and face: Cause and prevention. Ear Nose Throat J.1995;74:182–188.†Coleman SR. Avoidance of arterial occlusion from injection of soft tissue fillers. Aesthet Surg J. 2002;22:555–557.‡Matsuo T, Fujiwara H, Gobara H, Mimura H, Kanazawa S. Central retinal and posterior ciliary artery occlusion after intralesional injectionof sclerosant to glabellar subcutaneous hemangioma. Cardiovasc Intervent Radiol. 2009;32:341–346.§Egbert JE, Paul S, Engel WK, Summers CG. High injection pressure during intralesional injection of corticosteroids into capillary heman-giomas. Arch Ophthalmol. 2001;119:677–683.�Thomas EL, Laborde RP. Retinal and choroidal vascular occlusion following intralesional corticosteroid injection of a chalazion. Ophthalmology1986;93:405–407.¶Niamtu J III. Filler injection with micro-cannula instead of needles. Dermatol Surg. 2009;35:2005–2008.#Coleman SR. Structural fat grafting: More than a permanent filler. Plast Reconstr Surg. 2006;118(Suppl):108S–120S.**Berlin A, Cohen JL, Goldberg DJ. Calcium hydroxylapatite for facial rejuvenation. Semin Cutan Med Surg. 2006;25:132–137.††Tzikas TL. Facial fat injection. In: Thomas JR, ed. Advanced Therapy in Facial Plastic and Reconstructive Surgery. Shelton, Conn: People’s MedicalPublishing House; 2010:573–580.‡‡Feinendegen DL, Baumgartner RW, Vuadens P, et al. Autologous fat injection for soft tissue augmentation in the face: A safe procedure?Aesthetic Plast Surg. 1998;22:163–167.
Plastic and Reconstructive Surgery • April 2012
1008

rather than by the resolution of the choroidal isch-emia. In the other 12 cases in which the therapy wasadministered, no improvement was achieved regard-less of the nature of the embolus (fat6,11–15 or heter-ologous material16,19,21,28,30,31). The time between theocclusive event and the onset of the therapy couldhave contributed to these failures, however. In theEuropean Assessment Group for Lysis in the Eyestudy,77 the authors suggested that the visual prog-nosis in patients with acute central retinal arteryocclusion depends in part on the duration of symp-toms, with a shorter duration associated with bettervisual outcome. In five cases described in this review,the therapy was administered after more than 20hours11,13,14,30,31; in two cases,6,12 the timing was notspecified; and in five cases, it was administeredwithin 20 hours.15,16,19,21,28
Incomplete treatment could also have contrib-uted to failure. In the European Assessment Groupfor Lysis in the Eye study,77 the standard treatmentof central retinal artery occlusion included a six-step
therapy: topical (a single eye drop of timolol 0.5%)and systemic (intravenous injection of 500 mg ofacetazolamide) lowering of intraocular pressure, iso-volemic hemodilution in patients with a hematocritgreater than 40 percent (500 ml of blood was with-drawn and 500 ml of 10% hydroxyethyl starch wassimultaneously infused within 15 to 30 minutes),globe massage (repeated increased pressure was ap-plied to the globe for 10 to 15 seconds, followed bya sudden release with an in-and-out movement usinga three-mirror contact lens for 3 to 5 minutes), andanticoagulation with heparin and acetylsalicylicacid. In our review, all of the treated patientsunderwent at most a three-step therapy, whichincluded other treatment options, such as carbondioxide,6 oxygen therapy,6,12 oral or intravenouscorticosteroids,11–14,31 pharmacologic or pharma-comechanical thrombolysis,12,15 vasodilators,19 an-terior chamber paracentesis,28 and calcium chan-nel blockers.30 Monotherapy was administeredin four cases,13–16 dual therapy was administered in
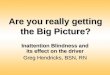
Fig. 2. A useful algorithm approach is presented to minimize the occurrence of ophthalmic arterial system embolization duringfacial cosmetic injections.
Volume 129, Number 4 • Blindness after Facial Cosmetic Injection
1009

two cases,11,30 and triple therapy was administeredin five cases6,12,19,28,31; in one case, an unspecifiedroutine treatment for vascular occlusion of thebulb was administered.21
Surgical ManagementContrasting opinions about the feasibility and
efficacy of reperfusion of the occluded retinal arterythrough surgical removal of the emboli have beenexpressed.84,85 No data support the assumption thatsurgical embolectomy of the iatrogenically injectedmaterials within the retinal circulation is a safemethod for restoring ophthalmic system circulationafter embolization from cosmetic facial injections.The same caution applies to transluminal neodym-ium:yttrium-aluminum-garnet laser embolysis.86 Sur-gical treatment has not been used or proposed byany of the articles reviewed.
Tips and Techniques to Diminish the Risk ofIntravascular Injection
Although no rule can completely prevent theoccurrence of ocular circulation embolization, somereasonable precautions that may decrease the risk ofvascular occlusion during facial cosmetic injectionsare discussed in Table 3.2,7,9,51,52,54,78,87–89 A useful al-gorithm approach is also presented in Figure 2.
CONCLUSIONSSome steps may minimize the risk of emboliza-
tion of filler into the ophthalmic artery followingfacial cosmetic injections. Intravascular placementof the needle or cannula should be demonstrated byaspiration before injection and should be furtherprevented by application of local vasoconstrictor.Needles, syringes, and cannulas of small size shouldbe preferred to larger ones and be replaced withblunt flexible needles and microcannulas when pos-sible. Low-pressure injections with the release of theleast amount of substance possible should be con-sidered safer than bolus injections. The total volumeof filler injected during the entire treatment sessionshould be limited, and injections into pretrauma-tized tissues should be avoided. Actually, no safe,feasible, and reliable treatment exists for iatrogenicretinal embolism. Nonetheless, therapy should the-oretically be directed to lowering intraocular pres-sure to dislodge the embolus into more peripheralvessels of the retinal circulation, increasing retinalperfusion and oxygen delivery to hypoxic tissues.
Davide Lazzeri, M.D.Plastic and Reconstructive Surgery Unit
Hospital of PisaVia Paradisa 2
Cisanello, 56100 Pisa, [email protected]
ACKNOWLEDGMENTSThe authors thank Dr.ssa Ilaria Bondi (MEDICAL
ILLUSTRATOR, Via Carlo Lugli, Carpi, Modena,Italy) for help with Figure 1.
REFERENCES1. Eppley BL, Dadvand B. Injectable soft-tissue fillers: Clinical
overview. Plast Reconstr Surg. 2006;118:98e–106e.2. Coleman SR. Structural fat grafting: More than a permanent
filler. Plast Reconstr Surg. 2006;118(Suppl):108S–120S.3. Teimourian B. Blindness following fat injections. Plast Re-
constr Surg. 1988;82:361.4. Dreizen NG, Framm L. Sudden unilateral visual loss after
autologous fat injection into the glabellar area. Am J Oph-thalmol. 1989;107:85–87.
5. Egido JA, Arroyo R, Marcos A, Jimenez-Alfaro I. Middle ce-rebral artery embolism and unilateral visual loss after autol-ogous fat injection into the glabellar area. Stroke 1993;24:615–616.
6. Lee DH, Yang HN, Kim JC, Shyn KH. Sudden unilateral visualloss and brain infarction after autologous fat injection intonasolabial groove. Br J Ophthalmol. 1996;80:1026–1027.
7. Feinendegen DL, Baumgartner RW, Vuadens P, et al. Au-tologous fat injection for soft tissue augmentation in the face:A safe procedure? Aesthetic Plast Surg. 1998;22:163–167.
8. Danesh-Meyer HV, Savino PJ, Sergott RC. Case reports andsmall case series: Ocular and cerebral ischemia followingfacial injection of autologous fat. Arch Ophthalmol. 2001;119:777–778.
9. Coleman SR. Avoidance of arterial occlusion from injectionof soft tissue fillers. Aesthet Surg J. 2002;22:555–557.
10. Yoon SS, Chang DI, Chung KC. Acute fatal stroke immedi-ately following autologous fat injection into the face.Neurology 2003;61:1151–1152.
11. Allali J, Bernard A, Assaraf E, Bourges JL, Renard G. Multipleembolizations of the branches of the ophthalmic artery: Anunknown serious complication of facial surgeries (inFrench). J Fr Ophtalmol. 2006;29:51–57.
12. Mori K, Ohta K, Nagano S, Toshinori M, Yago T, Ichinose Y.A case of ophthalmic artery obstruction following autologousfat injection in the glabellar area (in Japanese). Nippon GankaGakkai Zasshi 2007;111:22–25.
13. Park SH, Sun HJ, Choi KS. Sudden unilateral visual loss afterautologous fat injection into the nasolabial fold. Clin Oph-thalmol. 2008;2:679–683.
14. Lee YJ, Kim HJ, Choi KD, Choi HY. MRI restricted diffusionin optic nerve infarction after autologous fat transplantation.J Neuroophthalmol. 2010;30:216–218.
15. Park SJ, Woo SJ, Park KH, et al. Partial recovery after in-traarterial pharmacomechanical thrombolysis in ophthalmicartery occlusion following nasal autologous fat injection.J Vasc Interv Radiol. 2011;22:251–254.
16. von Bahr G. Multiple embolisms in the fundus of an eye afteran injection in the scalp. Acta Ophthalmol (Copenh.) 1963;41:85–91.
17. Lee JH, Lee KH, Moon HJ. A case of unilateral blindness afterparaffin injection on the forehead. J Korean Ophthalmol Soc.1969;10:49–51.
Plastic and Reconstructive Surgery • April 2012
1010

18. Selmanowitz VJ, Orentreich N. Cutaneous corticosteroid in-jection and amaurosis: Analysis for cause and prevention.Arch Dermatol. 1974;110:729–734.
19. Shin H, Lemke BN, Stevens TS, Lim MJ. Posterior ciliary-artery occlusion after subcutaneous silicone-oil injection.Ann Ophthalmol. 1988;20:342–344.
20. Castillo GD. Management of blindness in the practice ofcosmetic surgery. Otolaryngol Head Neck Surg. 1989;100:559–562.
21. Shafir R, Cohen M, Gur E. Blindness as a complication ofsubcutaneous nasal steroid injection. Plast Reconstr Surg.1999;104:1180–1182; discussion 1183–1184.
22. Jee DH, Lee KI. A case of left ophthalmic artery occlusionand right carotid cavernous fistula after illegal rhinoplasty.J Korean Ophthalmol Soc. 2002;43:898–904.
23. Apte RS, Solomon SD, Gehlbach P. Acute choroidal infarc-tion following subcutaneous injection of micronized dermalmatrix in the forehead region. Retina 2003;23:552–554.
24. Silva MT, Curi AL. Blindness and total ophthalmoplegia afteraesthetic polymethylmethacrylate injection: Case report. ArqNeuropsiquiatr. 2004;62:873–874.
25. Kubota T, Hirose H. Permanent loss of vision following cos-metic rhinoplastic surgery. Jpn J Ophthalmol. 2005;49:535–536.
26. Peter S, Mennel S. Retinal branch artery occlusion followinginjection of hyaluronic acid (Restylane). Clin Experiment Oph-thalmol. 2006;34:363–364.
27. Kang YS, Kim JW, Choi WS, Park HS, Jang SJ, Chio JC. A caseof sudden unilateral visual loss following injection of fillerinto the glabella. Korean J Dermatol. 2007;45:381–383.
28. Tangsirichaipong A. Blindness after facial contour augmen-tation with injectable silicone. J Med Assoc Thai. 2009;92(Suppl 3):S85–S87.
29. Sung MS, Kim HG, Woo KI, Kim YD. Ocular ischemia andischemic oculomotor nerve palsy after vascular embolizationof injectable calcium hydroxyapatite filler. Ophthal Plast Re-constr Surg. 2010;26:289–291.
30. Kwon DY, Park MH, Koh SB, et al. Multiple arterial embolismafter illicit intranasal injection of collagenous material. Der-matol Surg. 2010;36:1196–1199.
31. Kim YJ, Kim SS, Song WK, Lee SY, Yoon JS. Ocular ischemiawith hypotony after injection of hyaluronic acid gel. OphthalPlast Reconstr Surg. 2011;27:e152–e155.
32. Byers B. Blindness secondary to steroid injections into thenasal turbinates. Arch Ophthalmol. 1979;97:79–80.
33. Mabry RL. Visual loss after intranasal corticosteroid injec-tion: Incidence, causes, and prevention. Arch Otolaryngol.1981;107:484–486.
34. Mabry RL. Intranasal corticosteroid injection: Indications,technique, and complications. Otolaryngol Head Neck Surg.1979;87:207–211.
35. Whiteman DW, Rosen DA, Pinkerton RM. Retinal and cho-roidal microvascular embolism after intranasal corticoste-roid injection. Am J Ophthalmol. 1980;89:851–853.
36. Wilkinson WS, Morgan CM, Baruh E, Gitter KA. Retinal andchoroidal vascular occlusion secondary to corticosteroid em-bolisation. Br J Ophthalmol. 1989;73:32–34.
37. Savino PJ, Burde RM, Mills RP. Visual loss following intra-nasal anesthetic injection. J Clin Neuroophthalmol. 1990;10:140–144.
38. Cheney ML, Blair PA. Blindness as a complication of rhino-plasty. Arch Otolaryngol Head Neck Surg. 1987;113:768–769.
39. Rettinger G, Christ P, Meythaler FH. Blindness caused bycentral artery occlusion following nasal septum correction(in German). HNO. 1990;38:105–109.
40. Meythaler FH, Naumann GO. Intraocular ischemic infarctsin injections into the lid and parabulbar region (withoutperforation of the eye) (in German). Klin Monbl Augenheilkd.1987;190:474–477.
41. Rishiraj B, Epstein JB, Fine D, Nabi S, Wade NK. Permanentvision loss in one eye following administration of local an-esthesia for a dental extraction. Int J Oral Maxillofac Surg.2005;34:220–223.
42. Ellis PP. Visual loss following tonsillectomy; possible associ-ation with injections in tonsillar fossae. Arch Otolaryngol. 1968;87:436–438.
43. McGrew RN, Wilson RS, Havener WH. Sudden blindnesssecondary to injections of common drugs in the head andneck: I. Clinical experiences. Otolaryngology 1978;86:147–151.
44. Fivgas GD, Newman NJ. Anterior ischemic optic neuropathyfollowing the use of a nasal decongestant. Am J Ophthalmol.1999;127:104–106.
45. Chamot L, Zografos L, Micheli JL. Ocular and orbital com-plications after sclerosing injections in a case of a frontalcutaneous angioma. Ophthalmologica 1981;182:193–198.
46. Shorr N, Seiff SR. Central retinal artery occlusion associatedwith periocular corticosteroid injection for juvenile heman-gioma. Ophthalmic Surg. 1986;17:229–231.
47. Ruttum MS, Abrams GW, Harris GJ, Ellis MK. Bilateral retinalembolization associated with intralesional corticosteroid in-jection for capillary hemangioma of infancy. J Pediatr Oph-thalmol Strabismus 1993;30:4–7.
48. Egbert JE, Schwartz GS, Walsh AW. Diagnosis and treatmentof an ophthalmic artery occlusion during an intralesionalinjection of corticosteroid into an eyelid capillary hemangi-oma. Am J Ophthalmol. 1996;121:638–642.
49. Gupta V, Sharma SC, Gupta A, Dogra MR. Retinal and cho-roidal microvascular embolization with methylprednisolone.Retina 2002;22:382–386.
50. Edwards AO. Central retinal artery occlusion following fore-head injection with a corticosteroid suspension. Pediatr Der-matol. 2008;25:460–461.
51. Matsuo T, Fujiwara H, Gobara H, Mimura H, Kanazawa S.Central retinal and posterior ciliary artery occlusion after in-tralesional injection of sclerosant to glabellar subcutaneoushemangioma. Cardiovasc Intervent Radiol. 2009;32:341–346.
52. Thomas EL, Laborde RP. Retinal and choroidal vascularocclusion following intralesional corticosteroid injection ofa chalazion. Ophthalmology 1986;93:405–407.
53. Yagci A, Palamar M, Egrilmez S, Sahbazov C, Ozbek SS.Anterior segment ischemia and retinochoroidal vascular oc-clusion after intralesional steroid injection. Ophthal Plast Re-constr Surg. 2008;24:55–57.
54. Egbert JE, Paul S, Engel WK, Summers CG. High injectionpressure during intralesional injection of corticosteroidsinto capillary hemangiomas. Arch Ophthalmol. 2001;119:677–683.
55. Bachmann F, Erdmann R, Hartmann V, Wiest L, Rzany B.The spectrum of adverse reactions after treatment with in-jectable fillers in the glabellar region: Results from the In-jectable Filler Safety Study. Dermatol Surg. 2009;35(Suppl 2):1629–1634.
56. Bellman B. Complication following suspected intra-arterialinjection of Restylane. Aesthet Surg J. 2006;26:304–305.
57. Georgescu D, Jones Y, McCann JD, Anderson RL. Skin ne-crosis after calcium hydroxyapatite injection into the glabel-lar and nasolabial folds. Ophthal Plast Reconstr Surg. 2009;25:498–499.
Volume 129, Number 4 • Blindness after Facial Cosmetic Injection
1011

58. Glaich AS, Cohen JL, Goldberg LH. Injection necrosis of theglabella: Protocol for prevention and treatment after use ofdermal fillers. Dermatol Surg. 2006;32:276–281.
59. Hanke CW, Higley HR, Jolivette DM, Swanson NA, StegmanSJ. Abscess formation and local necrosis after treatment withZyderm or Zyplast collagen implant. J Am Acad Dermatol.1991;25:319–326.
60. Inoue K, Sato K, Matsumoto D, Gonda K, Yoshimura K.Arterial embolization and skin necrosis of the nasal ala fol-lowing injection of dermal fillers. Plast Reconstr Surg. 2008;21:127e–128e.
61. Hirsch RJ, Lupo M, Cohen JL, Duffy D. Delayed presentationof impending necrosis following soft tissue augmentationwith hyaluronic acid and successful management with hyal-uronidase. J Drugs Dermatol. 2007;6:325–328.
62. Park TH, Seo SW, Kim JK, Chang CH. Clinical experiencewith hyaluronic acid-filler complications. J Plast Reconstr Aes-thet Surg. 2011;64:892–896.
63. Schanz S, Schippert W, Ulmer A, Rassner G, Fierlbeck G.Arterial embolization caused by injection of hyaluronic acid(Restylane). Br J Dermatol. 2002;146:928–929.
64. Lowe NJ. Arterial embolization caused by injection of hyal-uronic acid (Restylane). Br J Dermatol. 2003;148:379; authorreply 379–380.
65. Paul S, Egbert JE, Walsh AW, Hoey MF. Pressure measure-ments during injection of corticosteroids. Med Biol Eng Com-put. 1998;36:729–733.
66. Paul S, Hoey MF, Egbert JE. Pressure measurements duringinjection of corticosteroids: In vivo studies. Med Biol EngComput. 1999;37:645–651.
67. Dutton JJ. Arterial supply to the orbit. In: Clinical and SurgicalOrbital Anatomy. Philadelphia, Pa: Saunders; 1994:68–71.
68. Badeer H. Hemodynamics for medical students. Adv PhysiolEduc. 2001;25:44–52.
69. Zweifach BW. Quantitative studies of microcirculatory struc-ture and function: I. Analysis of pressure distribution in theterminal vascular bed in cat mesentery. Circ Res. 1974;34:843–857.
70. Zweifach BW. Quantitative studies of microcirculatory struc-ture and function: II. Direct measurement of capillary pres-sure in splanchnic mesenteric vessels. Circ Res. 1974;34:858–866.
71. Bullock JD, Warwar RE, Green WR. Ocular explosion duringcataract surgery: A clinical, histopathological, experimental,and biophysical study. Trans Am Ophthalmol Soc. 1998;96:243–276; discussion 276–281.
72. Hayreh SS. Vascular disorders in neuro-ophthalmology. CurrOpin Neurol. 2011;24:6–11.
73. Chen CS, Lee AW. Management of acute central retinalartery occlusion. Nat Clin Pract Neurol. 2008;4:376–383.
74. Hayreh SS, Weingeist TA. Experimental occlusion of thecentral artery of the retina: IV. Retinal tolerance time toacute ischaemia. Br J Ophthalmol. 1980;64:818–825.
75. Selles-Navarro I, Villegas-Perez MP, Salvador-Silva M, Ruiz-Gomez JM, Vidal-Sanz M. Retinal ganglion cell death afterdifferent transient periods of pressure-induced ischemia andsurvival intervals: A quantitative in vivo study. Invest Ophthal-mol Vis Sci. 1996;37:2002–2014.
76. Roth S, Li B, Rosenbaum PS, et al. Preconditioning providescomplete protection against retinal ischemic injury in rats.Invest Ophthalmol Vis Sci. 1998;39:775–785.
77. Schumacher M, Schmidt D, Jurklies B, et al. Central retinalartery occlusion: Local intra-arterial fibrinolysis versus con-servative treatment, a multicenter randomized trial. Ophthal-mology 2010;117:1367–1375.e1.
78. McCleve DE, Goldstein JC. Blindness secondary to injectionsin the nose, mouth, and face: Cause and prevention. Ear NoseThroat J. 1995;74:182–188.
79. Ffytche TJ. A rationalization of treatment of central retinalartery occlusion. Trans Ophthalmol Soc UK. 1974;94:468–479.
80. Augsburger JJ, Magargal LE. Visual prognosis following treat-ment of acute central retinal artery obstruction. Br J Oph-thalmol. 1980;64:913–917.
81. McGrew RN, Wilson RS, Havener WH. Sudden blindnesssecondary to injections of common drugs in the head andneck: II. Animal studies. Otolaryngology 1978;86:152–157.
82. Alm A, Bill A. Ocular circulation. In: Alder FH, Moses RA,Hart WM, eds. Adler’s Physiology of the Eye. 8th ed. St. Louis:Mosby; 1987:183–203.
83. Hayreh SS. Prevalent misconceptions about acute retinalvascular occlusive disorders. Prog Retin Eye Res. 2005;24:493–519.
84. Garcıa-Arumı J, Martinez-Castillo V, Boixadera A, FonollosaA, Corcostegui B. Surgical embolus removal in retinal arteryocclusion. Br J Ophthalmol. 2006;90:1252–1255.
85. Hayreh SS. Surgical embolus removal in retinal artery oc-clusion. Br J Ophthalmol. 2007;91:1096–1097.
86. Opremcak EM, Benner JD. Translumenal Nd:YAG laser em-bolysis for branch retinal artery occlusion. Retina 2002;22:213–216.
87. Tzikas TL. Facial fat injection. In: Thomas JR, ed. AdvancedTherapy in Facial Plastic and Reconstructive Surgery. Shelton,Conn: People’s Medical Publishing House; 2010:573–580.
88. Niamtu J III. Filler injection with micro-cannula instead ofneedles. Dermatol Surg. 2009;35:2005–2008.
89. Berlin A, Cohen JL, Goldberg DJ. Calcium hydroxylapatite forfacial rejuvenation. Semin Cutan Med Surg. 2006;25:132–137.
Plastic and Reconstructive Surgery • April 2012
1012