Embed Size (px)
Citation preview

experimental models of DILs after subarach-noid hemorrhage will provide mechanistic insights and therapeutic targets that will guide the more challenging studies in humans. At the bedside, remarkable advances made in monitoring brain function in critically ill individuals5 will undoubtedly facilitate the interchange between experimental and clini-cal approaches needed to successfully address these key issues.
1. Bederson, J.B. et al. Stroke 40, 994–1025 (2009).2. Hijdra, A. et al. Neurology 36, 329–333 (1986).3. Stein, S.C., Browne, K.D., Chen, X.H., Smith, D.H. &
Graham, D.I. Neurosurgery 59, 781–787, discussion 787–788 (2006).
4. Macdonald, R.L., Pluta, R.M. & Zhang, J.H. Nat. Clin. Pract. Neurol. 3, 256–263 (2007).
5. Dreier, J.P. et al. Brain 132, 1866–1881 (2009).6. Somjen, G.G. Physiol. Rev. 81, 1065–1096
(2001).7. Busija, D.W., Bari, F., Domoki, F., Horiguchi, T. &
Shimizu, K. Prog. Neurobiol. 86, 379–395 (2008).8. Strong, A.J. et al. Brain 130, 995–1008 (2007).9. Minhas, P.S., et al. Neurosurgery 52, 1017–1022;
discussion 1022–1014 (2003).10. Macdonald, R.L. et al. Stroke 39, 3015–3021
(2008).11. Schlenk, F., Nagel, A., Graetz, D. & Sarrafzadeh, A.S.
Intensive Care Med. 34, 1200–1207 (2008).12. Nozari, A. et al. Ann. Neurol. published online,
doi:10.1002/ana.21871 (14 September 2009).13. Takano, T. & Nedergaard, M. J. Clin. Invest. 119,
16–19 (2009).14. Strong, A.J. Intensive Care Med. 34, 1169–1172
(2008).15. Shin, H.K. et al. Brain 130, 1631–1642 (2007).
and improve the outcome of subarachnoid hemorrhage? If CSD is an early manifesta-tion of brain dysfunction after subarachnoid hemorrhage, suppressing CSD may improve brain viability and avert DILs. An alternative scenario, however, is that CSD represents the coup de grace to brain tissue already destined to die because of terminal metabolic failure. If that is the case, preventing CSD would be futile. Clinical trials investigating the effect of CSD suppression on the incidence of DILs and on clinical outcome would address this question.
But preventing CSD may be more difficult than anticipated. N-methyl-d-aspartate recep-tor antagonists suppress CSD in the normal brain but are less effective in CSD associated with brain injury, including subarachnoid hemorrhage5,6. Hyperglycemia attenuates CSD but worsens subarachnoid hemorrhage outcome, a complication that needs to be bal-anced against the potential benefits of CSD suppression14. In contrast, hyperoxia prevents CSD-like phenomena and improves brain oxygenation in models of ischemic injury15. Therefore, administration of oxygen could be a valuable approach to suppress CSD in subarachnoid hemorrhage.
The role of CSD and its therapeutic impli-cations in subarachnoid hemorrhage need to be thoroughly explored. At the bench,
hemorrhage? CSD can be induced by intense neural activity leading to increases in extracellu-lar K+ and excitatory neurotransmitters (Fig. 1), which, in turn, induce additional depolarization and set off a vicious circle culminating in inacti-vation of neuronal excitability6. CSD-like phe-nomena occur spontaneously after experimental brain injury, and their frequency correlates with the magnitude of the brain damage8. In addi-tion, hypoxia and hypoglycemia are capable of triggering CSD6. Considering that cerebral blood flow and brain glucose concentration are already reduced in subarachnoid hemorrhage, presumably because of vasospasm9,11, it is con-ceivable that superimposed transient ischemia would further deplete the tissue of oxygen and glucose and trigger CSD. Microemboli, which have been described in subarachnoid hemor-rhage3, could act as a CSD-triggering stimulus by producing transient ischemia12.
CSD by itself, however, does not produce frank brain infarction13 and, as such, cannot be the sole cause of DIL. A probable scenario is that small ischemic lesions produced by microemboli set off recurring clusters of CSD, which promote the enlargement of the micro-infarcts into full-blown DIL (Fig. 1). The well-established role of CSD in the enlargement of infarcts after experimental cerebral ischemia supports this possibility.
Could suppressing CSD ameliorate DILs
B e t w e e n B e d s i d e a n d B e n c h
n benCH To bedsIde
Amyloid-b may keep clots awayGregory J del Zoppo
Gregory J. del Zoppo is Professor of Medicine in
Hematology and Adjunct Professor of Neurology at
the University of Washington, Harborview Medical
Center, Seattle, Washington, USA.
e-mail: [email protected]
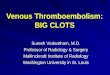
Deposition of amyloid in the parenchymal tis-sues and the blood vessels of the brain accom-panies Alzheimer’s disease. In the elderly, vascular deposition of amyloid can also have another impact: it can be associated with brain hemorrhage. Amyloid deposition increases the risk for small hemorrhages, dubbed micro-hemorrhages, and for a particular type of spontaneous hemorrhage within the gray matter of the brain, called a lobar hemor-rhage. But not all individuals who suffer from amyloid deposition are at risk for hemor-rhage (Fig. 1). One possibility is that the risk depends on the type of amyloid deposited.
Findings within the past few years have hinted that a domain that inhibits pro-teases, called a Kunitz protease inhibitor (or KPI) domain, found in several isoforms of b-amyloid (Ab), inactivates proteins in the blood that cause clotting1–5.
Does this inactivation underlie the link between amyloid and hemorrhage? Two recent studies by Xu et al.1,2 bolster this hypothesis. In one study, the authors found that mice constructed to make increased amounts of the precursor protein to Ab peptide (AbPP) had larger hemorrhages than wild-type mice in a model of artificial brain hemorrhage1. In a second study, mice that did not make AbPP experienced smaller hemorrhages in the same model2. What’s more, the isolated KPI domain could block coagulation1,2. The two studies suggest that, with aging, deposition of some isoforms of Ab in brain microvessels may
increase the chance of hemorrhage by block-ing coagulation locally.
Previous observations have suggested that the location of amyloid seems to influence the location of the hemorrhage. In blood vessels, amyloid deposits are found predominantly in the walls of arterioles and arteries in the cortex and deep brain structures. This loca-tion explains the frequent lobar distribution of the amyloid-associated hemorrhages. AbPP is found less often in capillaries and veins, but when it is, AbPP infiltrates the matrix that forms the basal lamina, as well as the sur-rounding tissue. This deposition interferes with normal vessel function and may also lead to microhemorrhages.
Another condition associated with aging, ischemic stroke, may also play into the risk of amyloid-associated hemorrhage. Hemorrhage occurs in the injury regions in up to 65% of
1132 volume 15 | number 10 | october 2009 nature medicine
©20
09 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.

B e t w e e n B e d s i d e a n d B e n c h
ischemic strokes. Deposits of Ab peptide are seen in cerebral vessels of some individu-als after ischemic stroke. Ischemia alters the adhesion of endothelial cells and astrocytes to the intervening basal lamina6,7, and it can also promote thrombosis within brain microvessels8. One possibility is that Ab pep-tides change cell-matrix interactions within brain microvessels and cause their instability, thereby promoting hemorrhage when the ves-sels are injured.
The notion that Ab peptides themselves might directly promote hemorrhage by inhib-iting thrombosis gained traction with studies of KPI domains. AbPP, the precursor of Ab, occurs in numerous isoforms, a result of alter-native splicing of a single gene. Two isoforms of AbPP have KPI domains that do not occur in other forms of the protein. Kunitz domains have a characteristic active site and a typi-cal double-loop structure that is conserved among proteins in which KPI domains are found. One or more such domains are found in biologically active proteinase inhibitors, including tissue factor pathway inhibitor, aprotinin, and the AbPP9,10. Inhibitors with Kunitz-like folds, or KPI-containing inhibi-tors, are employed by many species to regulate the initiation of clotting that prevents hemor-rhage from a vessel (hemostasis) or to block coagulation at specific steps (such as throm-bin formation). Ticks also use such domains to block blood coagulation9–11. In addition, peptides derived from the KPI domain can have antihemostatic activity.
One isoform of AbPP found in cerebral blood vessels and in brain deposits in indi-viduals with Alzheimer’s disease has a KPI domain identical to protease nexin-2 (PN-2), a protein known to regulate hemostasis12. In vitro studies have suggested that AbPP/PN-2 (the PN-2–identical isoform of AbPP) inhib-its the coagulation factors IXa and XIa10,11, which, by blocking thrombosis, could pro-mote hemorrhage. Xu et al.1,2 now flesh out this model.
The researchers examined transgenic mouse strains with either increased expression of a KPI-containing isoform of AbPP in platelets or in neurons1. They subjected the mice to a standardized experimental hemorrhage, made by injecting a fixed amount of the matrix pro-tease collagenase into the brain1. The volume of hemorrhage and hemoglobin deposition, they found, was substantially higher in the transgenic mice than in wild-type mice1,5. The authors also examined occlusion in the carotid artery in a model of laser-induced arterial thrombosis and found that occlusion
occurred more rapidly in the mice expressing the KPI-containing AbPP/PN-2 in platelets compared with wild-type mice or mice over-expressing the KPI-containing AbPP/PN-2 in neurons1. These findings suggest that the AbPP KPI insert could be responsible for enlargement of the cerebral hemorrhage in the model.
Xu et al.2 also examined mice engineered not to express AbPP and its KPI domain. They compared these mice to wild-type mice in the hemorrhage model and found substantially smaller cerebral hemorrhages with less hemo-globin deposition2. Similarly, mice lacking the amyloid precursor–like protein-2 (APLP-2), which has a KPI domain, showed a decreased volume of hemorrhage compared to wild-type mice. Experiments in the carotid artery model indicated that when AbPP or APLP-2 were absent thrombosis was enhanced2. Again, the KPI domains alone inhibited coagulation in vitro.
These findings have implications for aged individuals, but the studies are not without concerns. Models of cerebral hemorrhage are complex. The method used by the investiga-tors degrades collagen in the vascular basal lamina and surrounding tissues to produce a consistent circumscribed hemorrhage. The model is not pathophysiological partly because the collagenase stimulates its own inflamma-tory cell response and nonvascular cell injury independent of the hemorrhage—limiting the interpretation of experimental results. Models of ischemic stroke that produce hemorrhagic transformation of the injury (where ischemia causes the hemorrhage) would be of interest but are less consistent. Nonetheless, the ability of AbPP/PN-2 to increase the size of the hem-orrhage in the model used suggests that some portion of the molecule has an anticoagulant effect, and this seems to be the KPI domain. Intriguingly, mice lacking AbPP/PN-2 had decreased hemorrhage volume in this model, implying either that enhanced thrombosis limited the hemorrhage size or that there are some aspects of the artificial hemorrhage in mice that express AbPP with the KPI domain that are not understood.
Studies building on the new findings could broaden their clinical relevance. But it is important first to know how cerebral microvessels interact molecularly with AbPP and the KPI domain. The matrix barrier in the cerebral microvasculature could well be a partner in these events. Perhaps AbPP can interrupt the interaction of endothelial cells and other components of the microvessel with the basal lamina.
As hemorrhagic transformation is a com-mon accompaniment of focal ischemia, what would be the impact of varying amounts of AbPP with and without the KPI domain on the risk of hemorrhage in the setting of mouse ischemic stroke? Does AbPP/PN-2 contribute to the varying risk of hemorrhage in individu-als after ischemic stroke? Perhaps some people have one AbPP isoform with a KPI domain and others have non–KPI-containing isoforms. Perhaps the various isoforms of amyloid within the cerebral vessels promote different risks of hemorrhage. Maybe the frequency of hemor-rhage in individuals with ischemic stroke is linked to the amount of Ab deposition.
Knowing whether Ab is deposited, and which isoforms are present in people who are at risk for stroke, could help us know who might carry the risk of cerebral hemorrhage.
1. Xu, F., Previti, M.L. & Van Nostrand, W.E. Stroke 38, 2598–2601 (2007).
2. Xu, F. et al. J. Neurosci. 29, 5666–5670 (2009).3. Schmaier, A.H. et al. J. Clin. Invest. 92, 2540–2545
(1993).4. Smith, R.P., Higuchi, D.A. & Broze, G.J. Science 248,
1126–1128 (1990).5. Van Nostrand, W.E., Schmaier, A.H., Farrow, J.S. &
Cunningham, D.D. Science 248, 745–748 (1990).6. Tagaya, M. et al. J. Cereb. Blood Flow Metab. 21,
835–846 (2001).7. Milner, R. et al. Stroke 39, 191–197 (2008).8. Okada, Y., Copeland, B.R., Fitridge, R., Koziol, J.A. &
del Zoppo, G.J. Stroke 25, 1847–1853 (1994).9. Ponte, P. et al. Nature 331, 525–527 (1988).10. Broze, G.J. Jr., Girard, T.J. & Novotny, W.F.
Biochemistry 29, 7539–7546 (1990).11. Corral-Rodriguez, M.A., Macedo-Ribeiro, S., Barbosa
Periero, P.J. & Fuentes-Prior, P. Insect Biochem. Mol. Biol. 39, 1–17 (2009).
12. Van Nostrand, W.E. et al. Nature 241, 546–549 (1989).
Figure 1 Amyloid-related cerebral hemorrhages. Magnetic resonance image of the brain from a patient with amyloid deposition disease that displays microhemorrhages in gray matter (arrowheads) and a parenchymal hemorrhage (arrow).
Kyr
a B
ecke
r
nature medicine volume 15 | number 10 | october 2009 1133
©20
09 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.




![Vitiligo Acne Bleeding, Excessive Diabetes Heart Problems C] High Blood Pressure Liver Disease Mitral Valve Prolapse SCarring/Keloids Arthritis Blood Clots Eczema Hepatitis HIV/AIDS](https://img.dokumen.tips/doc/110x75/5e30a8c54b0276386f14420e/-vitiligo-acne-bleeding-excessive-diabetes-heart-problems-c-high-blood-pressure.jpg)