-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
1/21
This article has been accepted for publication and undergone
full peer review but has not
been through the copyediting, typesetting, pagination and
proofreading process which may
lead to differences between this version and the Version of
Record. Please cite this article as
an 'Accepted Article', doi: 10.1111/iej.12018
2012 International Endodontic Journal
Received Date : 02-Aug-2012
Accepted Date : 20-Sep-2012
Article type : Review
Bisphosphonates and their clinical implications in
endodontictherapy
A.T. Moinzadeh1, H. Shemesh
1, N.A.M. Neirynck
2, C. Aubert
3, P.R. Wesselink
1
1Department of Endodontology, Academic Center for Dentistry
Amsterdam (ACTA),
Amsterdam, the Netherlands, 2Department of Internal Medicine,
Ghent University Hospital,
Gent, Belgium,3Department of Head and Neck Surgery, CHU
Charleroi, Montigny le Tilleul,
Belgium
Running title:Bisphosphonates and endodontic treatment
Keywords:Bisphosphonate, BRONJ, ONJ, endodontic treatment, root
canal, osteonecrosis.
Corresponding author
A.T. Moinzadeh
Department of Endodontology, Academisch Centrum Tandheelkunde
Amsterdam (ACTA),
Gustav Mahlerlaan 3004, 1081 LA Amsterdam, the Netherlands,
e-mail: [email protected]
tel: +31(0)205980363
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
2/21
2012 International Endodontic Journal
Abstract
This review gives an overview of the factors that may play a
role in the development of
osteonecrosis of the jaw in patients treated with
bisphosphonates (BPs) and undergoing
nonsurgical endodontic treatment as well as some recommendations
for its prevention.
BPs are a widely prescribed group of drugs for diverse bone
diseases. The occasional but
devastating adverse effect of these drugs has been described as
bisphosphonate-related
osteonecrosis of the jaw (BRONJ). Since this condition is
debilitating and difficult to treat, all
efforts should be made to prevent its occurence in patients at
risk. The main triggering event
is considered to be dental extraction. Even though nonsurgical
endodontic treatment appears
to be a relatively safe procedure, care remains essential. After
an overview of this class of
drugs, the clinical presentation, epidemiology and pathogenesis
of BRONJ, as well as the
possible risk factors associated to its development after
nonsurgical endodontic treatment will
be described. Finally, several strategies will be proposed for
the prevention of BRONJ during
nonsurgical endodontic treatment.
Introduction
Bisphosphonates (BPs) are non-metabolized analogues of
pyrophosphates that are often
prescribed to treat patients with bone disorders, such as
osteoporosis (Gateset al.2009), and
Pagets disease. Other indications for the use of BPs are the
control of symptoms and signs
(pain, fractures, hypercalcemia) due to bone invasion in
multiple myeloma or bone metastasis
in other malignancies (Zysset et al. 1992, Mhaskar et al. 2012).
Between 2005 and 2009
more than 150 million prescriptions for BPs were dispensed
worldwide for the treatment of
osteoporosis (Whitakeret al.2012).
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
3/21
2012 International Endodontic Journal
Rare systemic adverse events linked to the use of BPs include:
renal (acute renal
insufficiency, deterioration of chronic renal insufficiency),
gastrointestinal (gastrointestinal
intolerance, anorexia), and bone and joint pain (Kuhlet
al.2012). BP-related osteonecrosis of
the jaw (BRONJ) is also one of the complications associated with
the administration of these
drugs (Marxet al.2005). A positive correlation exists between
the duration and cumulative
dosage of BP treatment and the incidence of BRONJ (Kuhlet
al.2012). According to several
observational studies, dental procedures are one of the risk
factors for the development
ofBRONJ. Mavrokokki et al. (2007) found that the main trigger of
BRONJ in patients taking
BPs was dental extraction. This was confirmed by several studies
which identified dental
extractions or invasive surgical procedures as being one of the
risk factors for the
development of BRONJ (Marxet al.2005, Pazianaset al.2007, Hoffet
al.2008, Filleulet
al.2010).
In 2003 the first cases of osteonecrosis of the jaw in patients
medicated with BPs were
reported (Marx 2003) and in 2005, Marx et al. (2005) mentioned a
possible association
between root canal treatment and the development of BRONJ in a
case series. In a total of
119 patients presenting with BRONJ, the most common dental
comorbidity was considered
to be clinically and radiographically apparent marginal
periodontitis, which was present in
84% of the patients. Previous root canal treatments with
supposed evidence of failure
(presence of an apical radiolucency or an inadequate root
filling) counted for 10.9 % of the
cases. Among the inciting events leading to BRONJ, dental
extraction counted for 37.8 % of
the cases as compared to 0.8% for endodontic surgery.
As a result of these findings, nonsurgical endodontic treatment
should be favored to dental
extractions in patients at higher risk for BRONJ whenever
possible.
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
4/21
2012 International Endodontic Journal
The first part of this review describes the biochemical
mechanism of action of BPs molecules
and discusses the pathosis of BRONJ. The second part will
describe the endodontic clinical
implications for patients medicated with systemic BPs.
Review
Mechanism of action of BPs and BRONJ
BPs and their mechanism of action
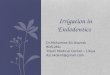
BPs are structural analogs of pyrophosphate (P-O-P), with a
carbon (P-C-P) replacing the
central oxygen (fig. 1). Molecules of BPs all have two side
chains from the central carbon,
R1 and R2, which vary in structure depending on the product. The
structure of the R1 side
chain changes the affinity of BPs for hydroxyapatite (HAP)
whereas the difference in R2
side chain determines the antiresorptive properties, and plays
to a lesser extent a role in HAP
affinity. Based on the structure of the R2 side chain, BPs can
be divided into 2 classes, the
non-nitrogencontaining, and the nitrogencontaining which
inhibits osteoclast activity to a
greater extent (Russell 2006). Examples of non-nitrogen
containing BPs are etidronate and
clodronate, and examples of nitrogen containing BPs are
pamidronate and zolendronate.
Since BPs bind to HAP, it was first hypothesized that BPs work
by preventing the dissolution
of HAP (Fleisch et al. 1966) and this theory even led to a
dental study, using BPs as an
intracanal medication to investigate if they may delay the
progressive replacement of dentine
by bone in cases of late reimplantation (Thonget al.2009).
However, it is now accepted that BPs mainly affect osteoclast
function through inhibition of
differentiation and maturation, loss of function and apoptosis.
This eventually results in a
decrease of bone resorption and an increase of mineralization
(Fleisch 1998).
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
5/21
2012 International Endodontic Journal
BRONJ
Definition
The American Association of Oral and Maxillofacial Surgeons
(2007) provided a position
paper which defines BRONJ as : the persistence of exposed bone
in the oral cavity, despite
adequate treatment for 8 weeks, without local evidence of
malignancy and no prior
radiotherapy to the affected region in patients having been
administrated BPs.
Pathophysiology
The pathophysiologic mechanism of BRONJ remains unclear and
current hypotheses are
mainly based on histopathological observations showing bone
necrosis, inflammation, the
presence of bacterial aggregates and/or areas of thickening of
trabecular bone (Favia et al.
2009, Lesclouset al.2009, Paparellaet al.2012).
A widely accepted hypothesis considers BPs toxicity and the
resulting decrease in bone
remodeling as the initial and main event in the development of
BRONJ (Sarin et al. 2008,
Chenget al.2009, Tubiana-Hulinet al.2009). Jaws are
characterized by high bone turnover
and are highly vascularized, which result in high local
concentrations of BPs. Their action
hampers normal bone turnover, resulting in acellular bone, which
can get secondarily
infected, due to (micro) trauma of the oral mucosa.
Naik & Russo (2009) stressed the importance of infection,
often caused by Actinomyces, in
the initiation of BRONJ. The adverse effects of BPs aggravate
the osteomyelitis and result in
the osteonecrosis as described above.
Other contributing factors in the pathogenesis are local
inflammation, anti-angiogenic effects
of BPs, an interplay between bone and overlying mucosa, direct
toxic effects of BPs to oral
epithelium and oral trauma (Sarinet al.2008, Naik & Russo
2009, Tubiana-Hulinet al.2009,
Landesberget al.2011).
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
6/21
2012 International Endodontic Journal
Multiple risk factors for the development of BRONJ such as the
dose of BPs, the duration of
treatment, smoking, alcohol use, diabetes, chemotherapeutic,
corticosteroid use and dental
procedures, (especially dental extraction as mentioned above)
have been described (Sarin et
al.2008, Allen & Burr 2009, Tubiana-Hulinet al.2009,
Landesberget al.2011).
Clinical presentation
Although one third of the lesions are painless, once
established, BRONJ is often debilitating
to the patient and refractory to treatment (Edwardset al.2008).
Some patients will present
with persistent jaw pain, gingival swelling and a sinus tract
(Fedele et al. 2010). When
radiographically visible, BRONJ would appear as a radiolucency
(Chiandussi et al.2006) and
could therefore be misdiagnosed as an empty socket or periapical
lesion. Estilo et al.(2008)
described tooth mobility and numbness of affected areas and
identified Actinomyces species
in all histological samples. Recently a non-exposed variant of
BRONJ, which can even be
undetected by computed tomography has been described (Fedele et
al. 2010, Patel et al.
2012). Such clinical situation could easily mislead the
clinician while establishing a
differential diagnosis with other conditions such as
non-odontogenic pain or periapical
inflammation.
Several classifications have attempted to define BRONJ (Kalmar
2012), among which the 5
stages classification adopted by the American Association of
Maxillofacial Surgeons
(AAOMS) and authored by Ruggiero et al.(2009) (Table 1).
Endodontic clinical implications of BPs administration.
BPs can be administered orally or intravenously (i.v.), the
latter being the most at risk of
developing BRONJ (Khl et al. 2012). They reviewed 47 studies
describing i.v.
administration at oncologic dosage and 9 with oral
administration at osteoporotic dosage. The
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
7/21
2012 International Endodontic Journal
mean incidence of BRONJ was 7% (mean duration of the studies 5
to 75 months) and 0.12%
(mean duration of the studies 24 to > 60 months)
respectively. Additionally, in a retrospective
study with 4019 patients treated with i.v.BPs, only patients who
received significantly higher
doses of BPs for a longer period of time related to their
underlying condition, developed
BRONJ (Hoffet al.2008). Furthermore, according to a
retrospective study on 4835 patients
treated with i.v.BPs (Estiloet al.2008), the interruption or
decrease of BP therapy did not
seem to modify the course of BRONJ.
Conflicting results are reported regarding the role of oral
health and dental procedures. The
study by Hoff et al. (2008) recognized poor oral health as a
significant risk factor for
developing BRONJ whereas the study by Estilo et al.(2008) did
not, although 51,4% of the
patients in that study had a nonhealing dental surgical
procedure in the BRONJ site. In a
cohort study of 1621 patients, dental extraction and the use of
dentures but not nonsurgical
endodontic treatment or periodontitis were associated with an
increased probability of
developing BRONJ (Vahtsevanos et al. 2009). On the contrary,
periodontal disease was a
comorbidity in the studies by Marx et al. (2005) and Hoff et al.
(2008),in84% and 41% of
the cases of BRONJ respectively.
Overall, surgical invasive procedures such as dental extraction
seem to be the main
precipitating factor associated with the development of BRONJ
(Marxet al.2005, Hoffet al.
2008, Filleul et al. 2010), and different guidelines concerning
the cessation of BPs
administration prior to invasive dental surgery have been
proposed by several scientific
societies but without consensus (Borromeo et al. 2011). The best
prevention to invasive
dental surgery may therefore be abstention and on account of
this, any surgical endodontic
procedure should also be avoided.
Nonsurgical endodontic treatment has been recommended as an
alternative to extraction in
order to minimize the risk of developing BRONJ (Edwardset
al.2008). Indeed, nonsurgical
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
8/21
2012 International Endodontic Journal
endodontic treatment aims to control and prevent the spread of
infection to the periapical
tissues. Nevertheless, there is no scientific evidence
concerning the risk/safety ratio of
endodontic therapy in patients taking BPs.
Two steps during nonsurgical endodontic treatment may be able to
trigger the
pathophysiological process of BRONJ:
- Several studies (Kyrgidis 2009 Kyrgidis & Andreadis 2009
Kyrgidis 2010) pointedout the possible role of soft tissue damage
in the initiation of BRONJ and insist on the
fact that one should try to be as cautious and atraumatic as
possible when placing a
rubber dam clamp. This was emphasized by Gallego et al.(2011)
who questioned the
role played by the rubber dam clamp as trigger of BRONJ. Nase
& Suzuki (2006)
reported a case where gingival correction without bone
involvement prior to
nonsurgical endodontic treatment led to BRONJ in a patient
medicated with oral BPs
for 5 years. It therefore appears prudent to avoid any damage to
the gingival tissues
during tooth isolation and caries excavation.
- Even though there is no clear evidence whether infection is a
primary or secondaryevent in BRONJ pathophysiology (Marxet
al.2005),Actinomyces species seem to be
ubiquitous once infection has been identified (Hellstein &
Marek 2005). It has also
been demonstrated that the microbiota of periapical lesions
refractory to endodontic
treatment is often composed of Actinomyces species (Sunde et
al.2002). In a case-
series by Sedghizadeh et al. (2008), micro-organisms that are
consistent with
pathologic conditions such as periapical, pulpal, periodontal
and mucosal (fungal)
disease were identified by scanning electron microscopy,
organized in biofilm in
osteonecrosis sites. Furthermore, even when following
guidelines, extrusion of debris
beyond the apical foramen remains unavoidable during nonsurgical
endodontic
treatment (Ferrazet al.2001). This raises the question whether
antibiotic prophylactic
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
9/21
2012 International Endodontic Journal
coverage during nonsurgical endodontic treatment of a necrotic
tooth with patients
currently or formerly treated with BPs is indicated. This
question has not yet been
answered in the relevant literature.
Since BPs affect the bone remodeling process, they could
therefore influence the dynamics of
the healing process of periapical lesions of endodontic origin.
Retrospectively, no difference
could be found between patients medicated or not with oral BPs
for more than 1 year [2-12
years] on the healing pattern of apical periodontitis (Hsiaoet
al.2009). However, the number
of patients included in this study was small and no information
was provided concerning
comorbidities. It should also be mentioned that the evaluation
of healing in this study was
done by means of conventional radiography. It is a
well-established fact that 2-dimensional
radiography fails to accurately assess the periapical status
when lesions are confined to the
cancellous bone (Bender & Seltzer 2003, Liang et al. 2011).
One can therefore speculate
wheter some of the cases of BRONJ with unknown etiology were not
be related to lesions of
endodontic origin which went undetected by conventional
radiography.
Recommendations
It is well-established that patients treated with BPs are at
higher risk of developing
osteonecrosis of the jaw (Mavrokokki et al. 2007). One of the
main triggering factors is
dental extraction. A position paper of the American Association
of Endodontists (2006)
discussed some of the endodontic implications of BRONJ.
Endodontic therapy has not been
identified as a significant risk factor in promoting BRONJ and
is therefore considered as the
favored alternative to extraction when possible (Marx et
al.2005). However, as soft tissue
damage during tooth isolation might occur as well as extrusion
of microorganisms during
root canal instrumentation, care is recommended. Since there is
scarce evidence on the
consequences of nonsurgical endodontic treatment on patients
treated with BPs, the informed
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
10/21
2012 International Endodontic Journal
consent of the patient and communication with the treating
physician are of utmost
importance.
The low incidence of BRONJ makes it difficult to conduct
clinical trials with high level of
evidence in order to allow the establishment of evidence-based
guidelines for nonsurgical
endodontic treatment in patients treated with BPs. Even though
the occurrence of BRONJ is
considered to be a rare event, its consequences for the patient
are catastrophic. Therefore,
until more evidence is available, it is necessary to be cautious
while performing nonsurgical
endodontic treatment on patients medicated with BPs and at risk
of developing BRONJ. The
following recommendations are suggested by inductive reasoning
and based on the literature:
- Some groups are particularly at risk and deserve particular
care. These includepatients treated with i.v.BPs as well as
patients taking BPs orally for more than 3
years and who concomitantly present systemic issues (such as
chronic kidney disease,
diabetes, corticosteroid therapy etc.) (Bamiaset al.2005,
Ruggieroet al.2009).
- A one minute mouth-rinse with chlorhexidine prior to the start
of the treatment wouldlower the bacterial load of the oral cavity
(Cousidoet al.2010) and aim at decreasing
the bacteremia caused by any soft tissues trauma.
- As impaired vascularization is a risk factor for osteonecrosis
in general, the use ofanaesthetic agents with vasoconstrictors
should be avoided since BPs already exert an
anti-angiogenic action (Tarassoff & Csermak 2003, Soltauet
al.2008).
- Working under aseptic conditions is mandatory. This includes
steps such as theremoval of caries and leaking restorations, the
cleaning of the tooth as well as the
placement of a rubber dam prior to the start of the intra-canal
procedures. The proper
adaptation of the dam should be checked. Disinfection of the
tooth and of the dam
should thereafter be performed by rubbing a disinfecting
solution such as 80% ethanol
for 2 minutes (Peterset al.2002).
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
11/21
2012 International Endodontic Journal
- Particular care should be given to avoid any damage to the
gingival tissues during theplacement of a rubber dam clamp
(Kyrgidis 2009). An alternative may be the use of
wedges to stabilize the rubber dam instead of using clamps.
- Patency of the apical foramen should be avoided. This could
only elevate thebacteremia (Debelianet al.1995) inherent to any
dental procedure without improving
the outcome of the treatment (Wuet al.2000).
- Techniques which lower the risk of overfilling and
overextension of the fillingmaterial are recommended since these
may impair the endodontic treatment
effectiveness (Liang et al. 2011) and exert irritation and
cytotoxicity to the
surrounding tissues (Scelzaet al.2012).
The evidence concerning the administration of a prophylactic
dose of antibiotics in patients
treated with BPs prior to nonsurgical endodontic treatment is
non-existent and there is
actually no consensus on this topic. It is important to balance
the risk of developing BRONJ
against the risk of adverse events from antibiotic prophylaxis.
There should be concerns
about the risks associated with the careless use of antibiotics
in regards to adverse events
such as allergic reactions caused by antibiotics or the
induction of antibiotic resistance.
However the risk of antibiotic resistance is considered to be
low after a single dose of
prophylactic antibiotics (Woodman et al.1985). Another point is
that cancer patients treated
with chemotherapy are immunosupressed and at risk for
neutropenia and subsequent related
serious infections. Therefore it may be expected that such
patients would be more prone to
infectious complications following procedures such as
nonsurgical endodontic treatment in
infected canals.
In cases of necrotic (infected) pulps in patients treated with
i.v. BPs, or medicated with oral
BPs for more than 3 years with concomitant risk factors, an
antibiotic single-dose prophylaxis
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
12/21
2012 International Endodontic Journal
may be advocated, since the adverse effects of the recommended
antibiotics, once allergies
have been ruled out, are minimal. Since Actinomyces species are
common in BRONJ loci,
amoxicillin would appear as the first choice (Smithet al.2005).
Whenever there is allergy or
severe intolerance to amoxicilline, clindamycin is an
appropriate alternative (Smith et al.
2005). If several teeth in the same patient need to be treated,
all treatments should be
scheduled during a single visit if possible, in order to take
place during a single antibiotic
coverage period. The benefit of antibiotic prophylaxis for
patients at risk of BRONJ is not
proven and therefore no dosage recommendations can be suggested.
Proper communication
with the patient and the treating physician is therefore
essential. In case of flare-up in a
patient at risk of BRONJ and according to the observed symptoms,
antibiotic coverage in
addition to the required dental treatment may be a safe
choice.
Finally, it should be mentioned that recently osteonecrosis of
the jaw has also been observed
in patients medicated with a new antiresorptive class of drugs,
Denosumab, a monoclonal
antibody against RANKL (Saadet al.2012). It therefore appears
important to establish and
adopt working protocols for patients undergoing nonsurgical
endodontic treatment and who
are medicated with drugs which may induce osteonecrosis of the
jaws.
Conclusion
BPs are a commonly and widely prescribed group of drugs used for
the treatment of various
bone pathologies. Nonsurgical endodontic treatment is a safe
alternative to dental extraction
which is the main trigger to BRONJ. However, caution is
mandatory during nonsurgical
endodontic treatment in these patients. More studies are needed
in order to obtain further
insight on the safety of nonsurgical endodontic treatment in
patients at risk of BRONJ.
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
13/21
2012 International Endodontic Journal
Acknowledgment
The authors would like to thank Prof. Roeland De Moor for the
stimulating initiative.
References
American Association of Endodontics position statement on the
endodontic implications of
bisphosphonate-associated osteonecrosis of the jaws (2006) [WWW
document]. URL
http://www.aae.org/ManagedFiles/pub/0/Pulp/bisphosonatesstatement.pdf
[accessed on 02
Augustus 2012].
American Association of Oral and Maxillofacial Surgeons position
paper on bisphosphonate-
related osteonecrosis of the jaws (2007) Journal of Oral and
Maxillofacial Surgery65,369-
76.
Allen MR, Burr DB (2009) The pathogenesis of
bisphosphonate-related osteonecrosis of the
jaw: so many hypotheses, so few data.Journal of Oral and
Maxillofacial Surgery67,61-70.
Bamias A, Kastritis E, Bamia C et al. (2005) Osteonecrosis of
the jaw in cancer after
treatment with bisphosphonates: incidence and risk factors.
Journal of Clinical Oncology23,
8580-7.
Bender IB, Seltzer S (2003) Roentgenographic and direct
observation of experimental lesions
in bone: I. 1961.Journal of Endodontics29,702-6.
Borromeo GL, Tsao CE, Darby IB, Ebeling PR (2011) A review of
the clinical implications
of bisphosphonates in dentistry.Australian Dental
Journal56,2-9.
Cheng A, Daly CG, Logan RM, Stein B, Goss AN (2009) Alveolar
bone and the
bisphosphonates.Australian Dental Journal54 Suppl 1,S51-61.
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
14/21
2012 International Endodontic Journal
Chiandussi S, Biasotto M, Dore F, Cavalli F, Cova MA, Di Lenarda
R(2006) Clinical and
diagnostic imaging of bisphosphonate-associated osteonecrosis of
the jaws.
Dentomaxillofacial Radiology35, 236-43.
Cousido MC, Tomas Carmona I, Garcia-Caballero L, Limeres J,
Alvarez M, Diz P (2010) In
vivo substantivity of 0.12% and 0.2% chlorhexidine mouthrinses
on salivary bacteria.
Clinical Oral Investigations14,397-402.
Debelian GJ, Olsen I, Tronstad L (1995) Bacteremia in
conjunction with endodontic therapy.
Endodontics and Dental Traumatology11,142-9.
Edwards BJ, Gounder M, McKoy JM et al. (2008) Pharmacovigilance
and reporting
oversight in US FDA fast-track process: bisphosphonates and
osteonecrosis of the jaw.
Lancet Oncology9,1166-72.
Estilo CL, Van Poznak CH, Wiliams T et al. (2008) Osteonecrosis
of the maxilla and
mandible in patients with advanced cancer treated with
bisphosphonate therapy. The
Oncologist13,911-20.
Favia G, Pilolli GP, Maiorano E (2009) Histologic and
histomorphometric features of
bisphosphonate-related osteonecrosis of the jaws: an analysis of
31 cases with confocal laser
scanning microscopy.Bone45,406-13.
Fedele S, Porter SR, D'Aiuto F et al. (2010) Nonexposed variant
of bisphosphonate-
associated osteonecrosis of the jaw: a case series.American
Journal of Medicine123,1060-4.
Ferraz CC, Gomes NV, Gomes BP, Zaia AA, Teixeira FB, Souza-Filho
FJ (2001) Apical
extrusion of debris and irrigants using two hand and three
engine-driven instrumentation
techniques.International Endodontic Journal34,354-8.
Filleul O, Crompot E, Saussez S (2010) Bisphosphonate-induced
osteonecrosis of the jaw: a
review of 2,400 patient cases.Journal of Cancer Research and
Clinical Oncology136,1117-
24.
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
15/21
2012 International Endodontic Journal
Fleisch H (1998) Bisphosphonates: mechanisms of action.Endocrine
Reviews19,80-100.
Fleisch H, Russell RG, Straumann F (1966) Effect of
pyrophosphate on hydroxyapatite and
its implications in calcium homeostasis.Nature212,901-3.
Gallego L, Junquera L, Pelaz A, Diaz-Bobes C (2011) Rubber dam
clamp trauma during
endodontic treatment: a risk factor of bisphosphonate-related
osteonecrosis of the jaw?
Journal of Oral and Maxillofacial Surgery69,e93-5.
Gates BJ, Sonnett TE, Duvall CA, Dobbins EK (2009) Review of
osteoporosis
pharmacotherapy for geriatric patients. Am Journal of Geriatric
Pharmacotherapy 7, 293-
323.
Hellstein JW, Marek CL (2005) Bisphosphonate osteochemonecrosis
(bis-phossy jaw): is this
phossy jaw of the 21st century?Journal of Oral and Maxillofacial
Surgery63,682-9.
Hoff AO, Toth BB, Altundag K et al. (2008) Frequency and risk
factors associated with
osteonecrosis of the jaw in cancer patients treated with
intravenous bisphosphonates.Journal
of Bone and Mineral Research23,826-36.
Hsiao A, Glickman G, He J (2009) A retrospective clinical and
radiographic study on healing
of periradicular lesions in patients taking oral
bisphosphonates. Journal of Endodontics35,
1525-8.
Kalmar JR (2012) Commentary on proposed new classification
system for BRONJ. Oral
Diseases doi:10.1111/j.1601-0825.2012.01936.x.
Kuhl S, Walter C, Acham S, Pfeffer R, Lambrecht JT (2012)
Bisphosphonate-related
osteonecrosis of the jaws - A review. Oral Oncology [WWW
document]. URL
http://dx.doi.org/10.1016/j.oraloncology.2012.03.028 [accessed
on 2 augustus 2012]
Kyrgidis A (2009) Novel hypotheses in the etiopathogenesis of
bisphosphonate-related
osteonecrosis of the jaws.Journal of Oral and Maxillofacial
Surgery67,2554.
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
16/21
2012 International Endodontic Journal
Kyrgidis A (2010) Bisphosphonate-related osteonecrosis of the
jaw in randomized clinical
trials.Breast Cancer Research and Treatment119,253-4.
Kyrgidis A, Andreadis C (2009) Epidemiologic studies are needed
to clarify whether dental
modalities could be predictors of bisphosphonate osteonecrosis
of the jaw in breast cancer
patients. The Oncologist14,101-2; author reply 103.
Landesberg R, Woo V, Cremers Set al.(2011) Potential
pathophysiological mechanisms in
osteonecrosis of the jaw.Annals of the New York Academy of
Sciences1218,62-79.
Lesclous P, Abi Najm S, Carrel JPet al.(2009)
Bisphosphonate-associated osteonecrosis of
the jaw: a key role of inflammation?Bone45,843-52.
Liang YH, Li G, Wesselink PR, Wu MK (2011) Endodontic outcome
predictors identified
with periapical radiographs and cone-beam computed tomography
scans. Journal of
Endodontics37,326-31.
Marx RE (2003) Pamidronate (Aredia) and zoledronate (Zometa)
induced avascular necrosis
of the jaws: a growing epidemic.Journal of Oral and
Maxillofacial Surgery61,1115-7.
Marx RE, Sawatari Y, Fortin M, Broumand V (2005)
Bisphosphonate-induced exposed bone
(osteonecrosis/osteopetrosis) of the jaws: risk factors,
recognition, prevention, and treatment.
Journal of Oral and Maxillofacial Surgery63,1567-75.
Mavrokokki T, Cheng A, Stein B, Goss A (2007) Nature and
frequency of bisphosphonate-
associated osteonecrosis of the jaws in Australia. Journal of
Oral and Maxillofacial Surgery
65,415-23.
Mhaskar R, Redzopovic J, Wheatley K et al.(2012) Bisphosphonates
in multiple myeloma: a
network meta-analysis. Cochrane Database Systematic Review5,
CD003188
Naik NH, Russo TA (2009) Bisphosphonate-related osteonecrosis of
the jaw: the role of
actinomyces. Clinical Infectious Diseases49,1729-32.
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
17/21
2012 International Endodontic Journal
Nase JB, Suzuki JB (2006) Osteonecrosis of the jaw and oral
bisphosphonate treatment.
Journal of the American Dental Association137,1115-9.
Paparella ML, Brandizzi D, Santini-Araujo E, Cabrini RL (2012)
Histopathological features
of osteonecrosis of the jaw associated with
bisphosphonates.Histopathology60,514-6.
Patel S, Choyee S, Uyanne J, Nguyen A et al.(2012) Non-exposed
bisphosphonate-related
osteonecrosis of the jaw: a critical assessmen of current
definition, staging and treatment
guidelines. Oral Diseases doi: 10.1111/j.1601-0825.2012.01911.x
[Epub]
Pazianas M, Miller P, Blumentals WA, Bernal M, Kothawala P
(2007) A review of the
literature on osteonecrosis of the jaw in patients with
osteoporosis treated with oral
bisphosphonates: prevalence, risk factors, and clinical
characteristics. Clinical Therapeutics
29,1548-58.
Peters LB, van Winkelhoff AJ, Buijs JF, Wesselink PR (2002)
Effects of instrumentation,
irrigation and dressing with calcium hydroxide on infection in
pulpless teeth with periapical
bone lesions.International Endodontic Journal35,13-21.
Ruggiero SL, Dodson TB, Assael LA, Landesberg R, Marx RE,
Mehrotra B (2009) American
Association of Oral and Maxillofacial Surgeons position paper on
bisphosphonate-related
osteonecrosis of the jaws--2009 update.Journal of Oral and
Maxillofacial Surgery67,2-12.
Russell RG (2006) Bisphosphonates: from bench to bedside. Annals
of the New York
Academy of Sciences1068,367-401.
Saad F, Brown JE, Van Poznak C et al. (2012) Incidence, risk
factors, and outcomes of
osteonecrosis of the jaw: integrated analysis from three blinded
active-controlled phase III
trials in cancer patients with bone metastases.Annals of
Oncology23,1341-7.
Sarin J, DeRossi SS, Akintoye SO (2008) Updates on
bisphosphonates and potential
pathobiology of bisphosphonate-induced jaw osteonecrosis. Oral
Diseases14,277-85.
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
18/21
2012 International Endodontic Journal
Scelza MZ, Linhares AB, da Silva LE, Granjeiro JM, Alves GG
(2012) A multiparametric
assay to compare the cytotoxicity of endodontic sealers with
primary human osteoblasts.
International Endodontic Journal45,12-8.
Sedghizadeh PP, Kumar SK, Gorur A, Schaudinn C, Shuler CF,
Costerton JW (2008)
Identification of microbial biofilms in osteonecrosis of the
jaws secondary to bisphosphonate
therapy.Journal of Oral and Maxillofacial Surgery66,767-75.
Smith AJ, Hall V, Thakker B, Gemmell CG (2005) Antimicrobial
susceptibility testing of
Actinomyces species with 12 antimicrobial agents. Journal of
Antimicrobial Chemotherapy
56,407-9.
Soltau J, Zirrgiebel U, Esser N et al. (2008) Antitumoral and
antiangiogenic efficacy of
bisphosphonates in vitro and in a murine RENCA model.Anticancer
Research28,933-41.
Sunde PT, Olsen I, Debelian GJ, Tronstad L (2002) Microbiota of
periapical lesions
refractory to endodontic therapy.Journal of
Endodontics28,304-10.
Tarassoff P, Csermak K (2003) Avascular necrosis of the jaws:
risk factors in metastatic
cancer patients.Journal of Oral and Maxillofacial
Surgery61,1238-9.
Thong YL, Messer HH, Zain RB, Saw LH, Yoong LT (2009) Intracanal
bisphosphonate does
not inhibit replacement resorption associated with delayed
replantation of monkey incisors.
Denalt Traumatology25,386-93.
Tubiana-Hulin M, Spielmann M, Roux Cet al.(2009) Physiopathology
and management of
osteonecrosis of the jaws related to bisphosphonate therapy for
malignant bone lesions. A
French expert panel analysis. Critical Reviews in
Oncology/Hematology71,12-21.
Vahtsevanos K, Kyrgidis A, Verrou Eet al.(2009) Longitudinal
cohort study of risk factors
in cancer patients of bisphosphonate-related osteonecrosis of
the jaw. Journal of Clinical
Oncology27,5356-62.
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
19/21
2012 International Endodontic Journal
Whitaker M, Guo J, Kehoe T, Benson G (2012) Bisphosphonates for
Osteoporosis - Where
Do We Go from Here?New England Journal of Medicine 366,
2048-51.
Woodman AJ, Vidic J, Newman NH, Marsh PD (1985) Effect of
repeated high dose
prophylaxis with amoxicilline on the resident oral flora on
adult volunteers. Journal of
Medical Microbiology 19, 15-23
Wu MK, Wesselink PR, Walton RE (2000) Apical terminus location
of root canal treatment
procedures. Oral Surgery, Oral Medicine, Oral Pathology, Oral
Radiology and Endodontics
89,99-103.
Zysset E, Ammann P, Jenzer Aet al.(1992) Comparison of a rapid
(2-h) versus a slow (24-h)
infusion of alendronate in the treatment of hypercalcemia of
malignancy. Bone and Mineral
18,237-49.
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
20/21
2012 International Endodontic Journal
Table 1: 5 stage classification for the diagnosis of BRONJ as
proposed by the AAOMS
(Ruggiero et al.2009)
Stage Description
At risk
category
The patient has been treated with BPs (either oral or
intravenous (i.v.)) and there
is no apparent necrotic bone
Stage 0 Presence of nonspecific clinical findings and symptoms
and no clinical evidence
of bone necrosis
Stage 1 Presence of exposed and necrotic bone in asymptomatic
patients and no evidence
of infection
Stage 2 Presence of exposed necrotic bone associated with
infection (pain and erythema,
with or without purulent drainage)
Stage 3 Presence of exposed necrotic bone, pain, infection, and
one of the following
clinical manifestations: exposed and necrotic bone extending
beyond the region
of alveolar bone, resulting in pathologic fracture, extraoral
fistula, oral antra/oral
nasal communication or osteolysis extending to the inferior
border of the
mandible or the sinus floor.
-
8/13/2019 Bisphosphonates and Their Clinical Implications in
Endodontic Therapy
21/21
Figure 1: Chemical structure of the bisphosphonate molecule