-
BRIEF ARTICLE
Bisphosphonate use and gastrointestinal tract cancer risk:
Meta-analysis of observational studies
Yun Hwan Oh, Chan Yoon, Sang Min Park
World J Gastroenterol 2012 October 28; 18(40): 5779-5788 ISSN
1007-9327 (print) ISSN 2219-2840 (online)
© 2012 Baishideng. All rights reserved.
Online Submissions:
http://www.wjgnet.com/esps/[email protected]:10.3748/wjg.v18.i40.5779
5779 October 28, 2012|Volume 18|Issue 40|WJG|www.wjgnet.com
Yun Hwan Oh, Sang Min Park, Department of Family Medi-cine,
Seoul National University Hospital, Seoul National Uni-versity
College of Medicine, Seoul 110-774, South Korea Chan Yoon, Seoul
National University Hospital, Seoul Nation-al University College of
Medicine, Seoul 110-774, South Korea Author contributions: Oh YH
and Yoon C contributed equally to this work; Yoon C was responsible
for the study design, data acquisition, data extraction, data
interpretation, statistical analy-sis and conducting the study; Oh
YH was responsible for data acquisition, data extraction, data
interpretation and conducting the study; and Park SM was
responsible for the conception, study design, data interpretation,
critical revision and supervis-ing the study. Supported by The
Basic Science Research Program through the National Research
Foundation of Korea funded by the Min-istry of Education, Science
and Technology, No. 2012-0003761Correspondence to: Sang Min Park,
MD, MPH, PhD, Depart-ment of Family Medicine, Seoul National
University Hospital, Seoul National University College of Medicine,
28 Yeongeon-Dong, Jongno-Gu, Seoul 110-774, South Korea.
[email protected] Telephone: +82-2-20723331 Fax:
+82-2-20723276Received: April 5, 2012 Revised: August 23,
2012Accepted: August 25, 2012Published online: October 28, 2012
AbstractAIM: To perform a meta-analysis of observational
stud-ies to further elucidate the relationship between oral
bisphosphonate use and gastrointestinal cancer risk.
METHODS: Systematic literature search was con-ducted in MEDLINE,
EMBASE, and the Cochrane Library to identify studies through
January 2011. Search terms were “bisphosphonates” or trade names of
the drugs, and “observational studies” or “cohort studies” or
“case-control studies”. Two evaluators reviewed and se-lected
articles on the basis of predetermined selection criteria as
followed: (1) observational studies (case-control or cohort
studies) on bisphosphonate use; (2) with at least 2 years of
follow-up; and (3) reported data
on the incidence of cancer diagnosis. The DerSimonian and Laird
random effects model were used to calculate the pooled relative
risk (RR) with 95% confidence in-terval (CI). Two-by-two
contingency table was used to calculate the outcomes not suitable
for meta-analysis. Subgroup meta-analyses were conducted for the
type of cancer (esophageal, gastric and colorectal cancers).
Sensitivity analyses were performed to examine the ef-fect sizes
when only studies with long-term follow-up (mean 5 years; subgroup
3 years) were included.
RESULTS: Of 740 screened articles, 3 cohort studies and 3
case-control studies were included in the analy-ses. At first, 4
cohort studies and 3 case-control studies were selected for the
analyses but one cohort study was excluded because the cancer
outcomes were not categorized by type of gastrointestinal cancer.
More than 124 686 subjects participated in the 3 cohort stud-ies.
The mean follow-up time in all of the cohort studies combined was
approximately 3.88 years. The 3 case-control studies reported 3070
esophageal cancer cases and 15 417 controls, 2018 gastric cancer
cases and 10 007 controls, and 11 574 colorectal cancer cases and
53 955 controls. The percentage of study partici-pants who used
bisphosphonate was 2.8% among the cases and 2.9% among the
controls. The meta-analysis of all the studies found no significant
association be-tween bisphosphonate use and gastrointestinal
cancer. Also no statistically significant association was found in
a meta-analysis of long-term follow-up studies. There was no
negative association between bisphosphonate use and the incidence
of esophageal cancer in the over-all analysis (RR 0.96, 95% CI:
0.65-1.42, I 2 = 52.8%, P = 0.076) and no statistically significant
association with long-term follow-up (RR 1.74, 95% CI: 0.97-3.10, I
2 = 58.8%, P = 0.119). No negative association was found in the
studies reporting the risk of gastric cancer (RR 0.89, 95% CI:
0.71-1.13, I 2 = 0.0%, P = 0.472). In case of colorectal cancer,
there was no association between colorectal cancer and
bisphosphonate use (RR 0.62, 95% CI: 0.30-1.29, I 2 = 88.0%, P =
0.004) and
-
Oh YH et al . Bisphosphonate and gastrointestinal tract
cancer
5780 October 28, 2012|Volume 18|Issue 40|WJG|www.wjgnet.com
also in the analysis with long-term follow-up (RR 0.61, 95% CI:
0.28-1.35, I 2 = 84.6%, P = 0.011).
CONCLUSION: Oral bisphosphonate use had no sig-nificant effect
on gastrointestinal cancer risk. However, this finding should be
validated in randomized con-trolled trials with long-term
follow-up.
© 2012 Baishideng. All rights reserved.
Key words: Bisphosphonate; Gastrointestinal tract can-cer;
Esophageal cancer; Gastric cancer; Colorectal can-cer;
Meta-analysis
Peer reviewer: Dr. Kok Sun Ho, Department of Colorectal Surgery,
Singapore General Hospital, Outram Road, Singapore 169608,
Singapore
Oh YH, Yoon C, Park SM. Bisphosphonate use and gastrointes-tinal
tract cancer risk: Meta-analysis of observational studies. World J
Gastroenterol 2012; 18(40): 5779-5788 Available from: URL:
http://www.wjgnet.com/1007-9327/full/v18/i40/5779.htm DOI:
http://dx.doi.org/10.3748/wjg.v18.i40.5779
INTRODUCTIONBisphosphonates are commonly used in postmenopausal
women with osteoporosis. In vitro and in vivo studies have
suggested that bisphosphonate has anticancer proper-ties[1]:
promoting apoptosis[2], inhibiting tumor cell adhe-sion and
invasion[3], inhibiting angiogenesis[4], altering tumor-associated
macrophage function[4], and enhancing immune surveillance[1,5].
However, it was recently re-ported that the Food and Drug
Administration received reports of 23 cases of esophageal cancer in
the United States and another 31 cases in Europe and Japan, all
oc-curring from 1995 through 2008 among patients using oral
bisphosphonates[6]. Since then, there have been sev-eral cohort
studies and case-control studies to elucidate the association
between the use of bisphosphonate and the risk of gastrointestinal
tract cancer. However, results of the observational studies are
inconsistent[7,8].
As yet, there have been no randomized controlled tri-als
demonstrating a causal relationship between bisphos-phonate use and
gastrointestinal track cancer. Moreover, no meta-analysis has been
performed despite the incon-sistent results of observational
studies. Therefore, in the present study, we aimed to investigate
the association between the use of oral bisphosphonate and the risk
of gastrointestinal cancer via meta-analysis of cohort stud-ies and
case-control studies.
MATERIALS AND METHODSStudy selection We conducted a systematic
literature search of MED-LINE, 1977 April 2011; EMBASE, 1971 April
2011; and the Cochrane Database of Systematic Reviews in
the Cochrane Library, 1973 April 2011. We identified
observational studies of bisphosphonate use whose pri-mary or
secondary outcomes included gastrointestinal tract cancer. The
search terms were "bisphosphonates" or trade names of the drugs,
and "observational studies" or "cohort studies" or "case-control
studies" (Table 1). All the searches were restricted to human
studies. In ad-dition, a manual review of references from primary
and review articles was performed to locate any additional relevant
studies. All the potentially relevant articles were independently
reviewed by 2 investigators (Oh YH and Yoon C). Disagreements
between evaluators were re-solved by discussion or consultation
with a third author (Park SM).
The inclusion criteria were: (1) observational studies
(case-control or cohort studies) on bisphosphonate use; (2) with at
least 2 years of follow-up; and (3) reported data on the incidence
of cancer diagnosis.
Data synthesis To compute a pooled relative risk (RR) with 95%
con-fidence interval (CI), we used the RRs or odds ratios and 95%
CIs that were adjusted for most confounders. Because the incidence
of cancer is generally low, we did not distinguish between the
various measures of RR. If the outcome measures were unsuitable for
meta-analysis, we calculated a crude estimate using a two-by-two
con-tingency table.
We also assessed the heterogeneity for each meta-analysis by
using the I2 value which measures the per-centage of total
variation across that is attributable to heterogeneity rather than
chance. High value of I2 index suggests increased heterogeneity. We
also calculated P value of Q-test which represents heterogeneity.
If which represents heterogeneity. IfIff P value is less than 0.10,
it represents there is heterogeneity. 0.10, it represents there is
heterogeneity. it represents there is heterogeneity.
Because of the known clinical and methodological heterogeneity
of the studies we analyzed, we calculated the pooled RR with 95% CI
based on the DerSimonian and Laird random effects model. We used
Stata Version 11.0 (Stata Corp., College Station, Texas) for the
statisti-cal analysis.
Statistical analysisSubgroup meta-analyses were carried out for
the study design (cohort and case-control) and type of cancer. For
the cancer subgroup analyses, esophageal, gastric and colorectal
cancers were analyzed independently.
We also performed sensitivity analyses to examine the effect
sizes when only studies with long-term follow-up (mean 5 years;
subgroup 3 years) were included.
RESULTSIdentification of relevant studies Figure 1 is a flow
diagram of how we identified the relevant studies. Of the 740
articles identified, 4 cohort studies[7,9-11] and 3 case-control
studies[8,12,13] were selected for the analyses. Many of initial
742 articles are not in
-
5781 October 28, 2012|Volume 18|Issue 40|WJG|www.wjgnet.com
our scope. They are mainly about effect of bisphos-phonates,
effects of several types of bisphosphonate regimen, other adverse
effects of bisphosphonate, such as atrial fibrillation,
osteonecrosis of jaw syndrome, and anti-cancerous bisphosphonate
use for breast cancer and prostate cancer. We performed review of
titles and abstract of the articles, then excluded irrelevant for
our study. Thirty articles were remained after overall pro-cess,
but 23 of 30 articles included no available data for outcome
measures. One cohort study[9] was excluded be-cause the cancer
outcomes were not categorized by type of gastrointestinal
cancer.
We also contacted Dr. Chris Cardwell to ask the data for the
adjusted hazards ratio and 95% CI for gastric cancer only in
bisphosphonate users[7].
Characteristics of the studies included in the analyses More
than 124 686 subjects participated in the 3 cohort studies[7,10,11]
used in our meta-analyses. The mean follow-up time in all of the
cohort studies combined was ap-proximately 3.88 years (range:
0.5-13 years). The 3 case-control studies[8,12,13] used in our
meta-analyses reported the number of cases and controls: 3070
esophageal
cancer cases and 15 417 controls, 2018 gastric cancer cases and
10 007 controls, and 11 574 colorectal cancer0 007 controls, and 11
574 colorectal cancer 007 controls, and 11 574 colorectal cancer
cases and 53 955 controls. The percentage of study par-ticipants
who used bisphosphonate was 2.8% among the cases and 2.9% among the
controls. Tables 2 and 3 sum-marize the general characteristics of
the studies included in our analyses.
The methods of the studies we included were as-sessed on the
basis of 5 predetermined quality assess-ment items (Table 4). All
of the studies included in our analyses were based on the secure
record linkage regard-ing medication use and cancer diagnosis.
Association between bisphosphonate use and the risk of
gastrointestinal tract cancer There was no negative association
between bisphospho-nate use and the incidence of esophageal cancer
in the overall analysis (RR 0.96, 95% CI: 0.65 1.42, I2 = 52.8%,, P
= 0.076; Figure 2A). In 2 studies with long-term fol-0.076; Figure
2A). In 2 studies with long-term fol-; Figure 2A). In 2 studies
with long-term fol-low-up, there was a tendency for bisphosphonate
users to develop esophageal cancer; however, this finding was not
statistically significant (RR 1.74, 95% CI: 0.97-3.10, I2 = 58.8%,,
P = 0.119�. �o significant association was0.119�. �o significant
association was�. �o significant association was
Table 1 Search strategy
Search strategy for MEDLINE Search strategy for EMBASE Search
strategy for Cochrane reviews of the Cochrane Library
1. Diphosphonates [MH] OR diphosphonates [ALL] OR diphosphonate
[ALL]
1. Bisphosphonates/de 1. Bisphosphonates [ALL]
2. Bisphosphonates [ALL] 2. Diphosphonate/de 2. Diphosphonate
[ALL] 3. Alendronate [MH] OR alendronate [ALL] 3. Alendronate/de 3.
Alendronate [ALL] 4. Clodronic acid [MH] OR clodronic acid [ALL] OR
clodronate [ALL] 4. Clodronate/de 4. Clodronate [ALL] 5. Etidronic
acid [MH] OR etidronic acid [ALL] OR etidronate [ALL] 5.
Etidronate/de 5. Etidronate [ALL] 6. Ibandronic acid [NM] OR
ibandronic acid [ALL] OR ibandronate [ALL] 6. Ibandronate/de 6.
Ibandronate [ALL] 7. Minodronate [ALL] OR YM 529 [NM] OR YM 529
[ALL] 7. Minodronate/de 7. Minodronate [ALL] 8. Neridronate [ALL]
OR 6-amino-1-hydroxyhexane-1,1-diphosphonate [NM] OR
6-amino-1-hydroxyhexane-1,1-diphosphonate [ALL]
8. Neridronate/de 8. Neridronate [ALL]
9. Olpadronic acid [NM] OR olpadronic acid [ALL] OR olpadronate
[ALL] 9. Olpadronate/de 9. Olpadronate [ALL] 10. Pamidronate [NM]
OR pamidronate [ALL] 10. Pamidronate/de 10. Pamidronate [ALL] 11.
Risedronic acid [NM] OR risedronic acid [ALL] OR risedronate [ALL]
11. Risedronate/de 11. Risedronate [ALL] 12. Tiludronic acid [NM]
OR tiludronic acid [ALL] OR tiludronate [ALL] 12. Tiludronate/de
12. Tiludronate [ALL] 13. Zoledronic acid [NM] OR zoledronic acid
[ALL] OR zoledronate [ALL] 13. Zoledronate/de 13. Zoledronate [ALL]
14. 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10 OR 11 OR 12 OR
13 14. 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7
OR 8 OR 9 OR 10 OR 11 OR 12 OR 13 14. 1 OR 2 OR 3 OR 4 OR 5 OR 6
OR 7 OR 8 OR 9 OR 10 OR 11 OR 12 OR 13
15. Observational studies [ALL] 15. Observational studies/de 16.
CohORt studies [ALL] 16. CohORt studies/de [ALL] - in all text 17.
Case control studies [ALL] OR case-control studies [ALL] 17. Case
control studies/de OR case-
control studies/de 18. Case referent studies [ALL] OR
case-referent studies [ALL] 18. Case referent studies OR case-
referent studies 19. 15 OR 16 OR 17 OR 18 19. 15 OR 16 OR 17 OR
18 20. 14 OR 19 20. 14 OR 19 21. Humans [MH] 21. [Humans]/lim 22.
20 AND 21 22. [Embase]/lim OR [embase clas-
sic]/lim 23. 20 AND 21 AND 22
Date of search: April 29, 2011 (1973 April 2011); Result: 1709
articles found
Date of search: April 29, 2011 (1977 April 2011);Result: 2129
articles found
Limitation: cochrane database of systematic reviews;Date of
search: April 29, 2011 (1971 April 2011); Result: 47 articles
found
ALL: All fields; MH: MeSH terms; NM: Supplementary
concept/substance name; PT: Publication type; /de: Mapped terms;
/lim: Limitation.
Oh YH et al . Bisphosphonate and gastrointestinal tract
cancer
-
5782 October 28, 2012|Volume 18|Issue 40|WJG|www.wjgnet.com
foun
d in
the
stud
ies[8
,14] re
port
ing
the
risk
of g
astri
c ca
ncer
(RR
0.89
, 95%
CI:
0.71
-1.1
3, I2
= 0
.0%
,, P =
0.4
72;F
igur
e2B
).0.
472;
Figu
re2B
).; F
igur
e 2B
).Bi
spho
spho
nate
use
rs w
ere
less
like
ly to
rece
ive
a di
agno
sis o
f co
lore
ctal
can
cer;
how
ever
, thi
s find
ing
was
not
stat
istic
ally
sign
ifica
nt in
the
over
all a
naly
sis (R
R 0.
62,
95%
CI:
0.30
-1.2
9, I2
= 8
8.0%
,, P =
0.0
04)o
rin
the
anal
ysis
limite
dto
stud
iesw
ithlo
ng-te
rmfo
llow
-up
(RR
0.61
,95%
CI:
0.28
-1.3
5,0.
004)
orin
the
anal
ysis
limite
dto
stud
iesw
ithlo
ng-te
rmfo
llow
-up
(RR
0.61
,95%
CI:
0.28
-1.3
5,) o
r in
the
anal
ysis
limite
d to
stud
ies w
ith lo
ng-te
rm fo
llow
-up
(RR
0.61
, 95%
CI:
0.28
-1.3
5, I2
= 8
4.6%
,, P =
0.01
1;Fi
gure
2C).
= 0
.011
;Fig
ure
2C).
0.01
1;Fi
gure
2C).
; Fig
ure
2C).
DIS
CU
SSIO
NMa
in fi
ndin
gs
In th
e pr
esen
t stu
dy, w
e ex
amin
ed th
e as
soci
atio
n be
twee
n or
al b
ispho
spho
nate
use
and
the
inci
denc
e of
gas
troin
test
inal
trac
t can
cer b
y an
alyz
ing
the
resu
lts o
f pr
evi-
Tabl
e 2 C
hara
cter
istics
of
coho
rt s
tudi
es (n
= 3
) in
clud
ed in
met
a-an
alys
is r
egar
ding
use
of
bisp
hosp
hona
tes
and
risk
of
canc
er
Ref
.C
ount
ryC
ohor
t fo
rmat
ion
(pop
ulat
ion)
Stud
y pe
riod
Mea
n F/
U
dura
tion
, yr
(ra
nge)
Age
, yr
(m
ean±
SD)
Sex
ratio
(ref
eren
ce
grou
p)
Type
of
canc
erTy
pe o
f dr
ug
(ref
eren
ce g
roup
)R
isk
estim
ate
Adj
ustm
ent
No.
of
canc
er d
evel
opm
ent/
no
. of
stu
dy p
opul
atio
nN
o. o
f to
tal
coho
rt
Bisph
osph
onat
e us
erR
efer
ence
gro
up
Abr
aham
sen
et al
[10]
Den
mar
kPa
tient
s w
ith
frac
ture
who
had
pr
escr
iptio
n fo
r ora
l bi
spho
spho
nate
(n
atio
nal r
egis
ters
)
E:19
95-2
005;
F/
U: -
2005
2.8
(NA
)74
.3 ±
8.8
M: 1
1;
F: 8
9Es
opha
geal
ca
ncer
, ga
stri
c ca
ncer
Any
bi
spho
spho
nate
use
(n
o bi
spho
spho
nate
us
e)
Esop
hage
al o
r ga
stri
c ca
ncer
0.
78 (0
.49-
1.26
); es
opha
geal
can
cer
0.35
(0.1
4-0.
85);
gast
ric
canc
er
1.23
(0.6
8-2.
22)
Age
, sex
, fra
ctur
e ty
pe, C
harl
son
inde
x, n
umbe
r of
con
com
itant
m
edic
atio
n, ti
me
to e
vent
NA
/13
678
NA
/27
356
41 0
34
Solo
mon
et
al[1
1]U
nite
d St
ates
Patie
nts
who
had
pr
escr
iptio
n fo
r ora
l bi
spho
spho
nate
(h
ealth
car
e ut
iliza
tion
reco
rds
of m
edic
are
bene
ficia
ries
)
NA
NA
(NA
)N
AN
AEs
opha
geal
ca
ncer
Any
bi
spho
spho
nate
use
(o
ther
ost
eopo
rosi
s m
edic
atio
ns u
se)
Esop
hage
al c
ance
r 0.
55 (0
.06-
4.72
)N
AIn
cide
nce
rate
26
.7/1
00 0
00In
cide
nce
rate
48
.4/1
00 0
00N
A
Car
dwel
l et
al[7
]U
nite
d K
ingd
omPa
tient
s re
ceiv
ing
pres
crip
tion
for o
ral
bisp
hosp
hona
te
(GPR
D)
E:19
96-2
006;
F/
U: -
2008
4
.5
(0.5
-12.
9)70
.0 ±
11.
4M
: 19;
F:
81
Esop
hage
al
canc
er,
gast
ric
canc
er
Any
bi
spho
spho
nate
us
e (r
egar
dles
s of
bi
spho
spho
nate
us
e)
Gas
tric
can
cer
0.78
(0.5
0-1.
23);
esop
hage
al c
ance
r 1.
07 (0
.77-
1.49
)
Age
, sex
, ge
nera
l pra
ctic
e,
BMI,
ciga
rette
sm
okin
g, a
lcoh
ol
inta
ke, h
orm
one
ther
apy,
NSA
ID
use,
Bar
rett'
s es
opha
gus,
GER
D,
H2
rece
ptor
an
tago
nist
use
, pr
oton
pum
p in
hibi
tor u
se
Esop
hage
al o
r ga
stri
c ca
ncer
11
6/41
826
(g
astr
ic c
ance
r 37
/41
826;
es
opha
geal
can
cer
79/4
1 82
6)
Esop
hage
al o
r ga
stri
c ca
ncer
11
5/41
826
(g
astr
ic c
ance
r43
/41
826;
es
opha
geal
can
cer
72/4
1 82
6)
83 6
52
E: E
nrol
lmen
t; F/
U: F
ollo
w u
p; B
MI:
Body
mas
s in
dex;
GER
D: G
astr
oeso
phag
eal r
eflux
dis
ease
; NSA
ID: N
onst
eroi
dal a
ntiin
flam
mat
ory
drug
s; M
: Mal
e; F
: Fem
ale;
NA
: Not
ava
ilabl
e; G
PRD
:Gen
eral
Prac
tice
Rese
arch
GPR
D: G
ener
al P
ract
ice
Rese
arch
D
atab
ase..
Oh YH et al . Bisphosphonate and gastrointestinal tract
cancer
-
5783 October 28, 2012|Volume 18|Issue 40|WJG|www.wjgnet.com
ous o
bser
vatio
nal s
tudi
es. O
ur m
eta-
anal
yses
foun
d no
sign
ifica
nt a
ssoc
iatio
n be
twee
n th
e us
e of
ora
l bisp
hosp
hona
te a
nd th
e ov
eral
l gas
troin
test
inal
can
cer i
ncid
ence
. In
the
stud
y de
sign
subg
roup
met
a-an
alys
is, n
o st
atist
ical
ly si
gnifi
cant
ass
ocia
tion
was
foun
d fo
r the
coh
ort s
tudi
es o
r cas
e-co
ntro
l stu
dies
. The
can
cer t
ype
subg
roup
ana
ly-
sis id
entifi
ed n
o as
soci
atio
n be
twee
n bi
spho
spho
nate
use
and
eso
phag
eal c
ance
r or
gas
tric
canc
er. C
olor
ecta
l can
cer
was
less
like
ly to
be
diag
nose
d in
bisp
hosp
hona
te u
sers
; ho
wev
er, t
his
findi
ng w
as n
ot s
tatis
tical
ly s
igni
fican
t. T
he r
esul
ts o
f th
e se
nsiti
vity
ana
lyse
s of
the
stud
ies
with
mor
e th
an 3
yea
rs o
f or
al b
ispho
spho
nate
use
wer
e sim
ilar
to
thos
e of
the
over
all a
naly
ses.
Acc
ordi
ng to
our
ana
lyse
s, or
al b
ispho
spho
nate
seem
s to
have
littl
e as
soci
atio
n w
ith th
e in
cide
nce
of g
astro
inte
stin
al c
ance
r. It
is w
ell k
now
n th
at th
e us
e of
ora
l bisp
hosp
hona
te in
duce
s gas
troin
test
inal
pro
blem
s, su
ch a
s ero
sive
esop
hagi
tis[1
5]. T
he e
ndos
copi
c an
d hi
stol
ogic
al fi
ndin
gs o
f m
ucos
al
inju
ry o
f th
e es
opha
gus
in p
atie
nts
usin
g or
al b
ispho
spho
nate
s[15-
20] s
ugge
st th
at p
rolo
nged
use
may
incr
ease
the
risk
of e
soph
agea
l can
cer.
Gre
en et
al[8
] ana
lyze
d th
e U
nite
d
Tabl
e 3 C
ase-
cont
rol s
tudi
es (n
= 3
) in
clud
ed in
met
a-an
alys
is r
egar
ding
use
of
bisp
hosp
hona
tes
and
risk
of
canc
er
Ref
.C
ount
ry
(stu
dy t
ype)
Cas
e se
lect
ion
met
hod
Con
trol
sa
mpl
ing
met
hod
Med
icat
ion
data
col
lect
ion
met
hod
(per
iod)
Age
, yr
(m
ean±
SD)
Sex
ratio
of
case
s (r
efer
ence
gr
oup)
Site
of
canc
erTy
pe o
f dr
ug
(ref
eren
ce
grou
p)
Odd
’s r
atio
(9
5%
CI)
Adj
ustm
ent
No.
of
case
s/no
. of
con
trol
s
Expo
sed
Une
xpos
ed
Gre
en
et a
l[8]
Uni
ted
Kin
gdom
(n
este
d ca
se-
cont
rol)
Revi
ew o
f co
mpu
teri
zed
info
rmat
ion
(with
in
part
icip
ants
of
GPR
D b
etw
een
1995
-200
5)
Mat
ched
on
age
(with
in 2
yr)
, se
x, o
bser
vatio
n pe
riod
in th
e da
taba
se a
nd
gene
ral p
ract
ice
atte
nded
)
Revi
ew o
f co
mpu
teri
zed
med
ical
reco
rds
(from
199
5 un
til
canc
er d
iagn
osis
)
72 ±
11
M: 5
7;
F: 4
3G
astr
oint
estin
al
canc
er
(eso
phag
eal,
gast
ric,
co
lore
ctal
)
Any
bi
spho
spho
nate
us
e (n
o bi
spho
spho
nate
us
e)
Esop
hage
al ca
ncer
1.
30 (1
.02-
1.66
); G
astr
ic c
ance
r 0.
87 (0
.64-
1.19
); co
lore
ctal
can
cer
0.87
(0.7
7-1.
00)
Age
, sex
, obs
erva
tion
peri
od, g
ener
al p
ract
ice,
BM
I, ci
gare
tte s
mok
ing,
al
coho
l int
ake
Esop
hage
al c
ance
r 90
/345
; ga
stri
c ca
ncer
49
/270
; co
lore
ctal
can
cer
276/
1555
Esop
hage
al c
ance
r 28
64/1
4 37
6;
gast
ric
canc
er
1969
/973
7;
colo
rect
al c
ance
r 10
365
/51
467
Ngu
yen
et a
l[12]
Uni
ted
Stat
es
(nes
ted
case
-co
ntro
l)
Revi
ew o
f co
mpu
teri
zed
info
rmat
ion
(with
in p
atie
nts
with
Bar
rett’
s
esop
hagu
s in
th
e na
tiona
l ve
tera
ns a
ffair
da
taba
se b
etw
een
2000
-200
2)
Mat
ched
on
age(
inte
rval
of 5
yr
) and
Bar
rett’
s es
opha
gus
inde
x da
te
Revi
ew o
f co
mpu
teri
zed
med
ical
reco
rds
(from
Bar
rett’
s
esop
hagu
s di
agno
sis
until
3
mo
befo
re c
ance
r di
agno
sis)
65.0
± 1
0.3
M: 2
.6;
F: 9
7.4
Esop
hage
al
canc
erA
ny
bisp
hosp
hona
te
use,
mos
tly
alen
dron
ate
(no
bisp
hosp
hona
te
use)
0.81
(0.1
8-3.
72)
Age
, Bar
rett’
s es
opha
gus
inde
x da
te,
race
, non
can
cer d
isea
se
com
orbi
dity
inde
x,
NSA
ID u
se, P
PI u
se
2/13
114/
683
Renn
ert
et a
l[13]
Isra
el
(con
vent
iona
l ca
se-c
ontr
ol)
Revi
ew o
f a
com
pute
rize
d in
form
atio
n (w
ithin
po
stm
enop
ausa
l w
omen
in C
HS
data
base
bet
wee
n 20
00-2
006)
Mat
ched
on
age,
se
x, re
side
nce,
an
d et
hnic
gro
up
in C
HS
data
base
Revi
ew o
f CH
S ph
arm
acy
reco
rds
71.1
± N
AF:
100
Col
orec
tal
canc
erA
ny
bisp
hosp
hona
te
use
mor
e th
an 1
yr (
no
bisp
hosp
hona
te
use)
0.41
(0.2
5-0.
67)
BMI,
fam
ily h
isto
ry
of c
olor
ecta
l can
cer,
vege
tabl
e co
nsum
ptio
n,
spor
ts p
artic
ipat
ion,
us
e of
low
-dos
e as
piri
n,
stat
ins,
vita
min
D,
post
men
opau
sal
horm
ones
53/1
0088
0/83
3
E: E
nrol
lmen
t; F/
U: F
ollo
w u
p; C
I: C
onfid
ence
inte
rval
; M: M
ale;
F: F
emal
e; N
A: N
ot a
vaila
ble;
BM
I: Bo
dy m
ass
inde
x; N
SAID
: Non
ster
oida
l ant
iinfla
mm
ator
y dr
ugs;
PPI
: Pro
ton
pum
p in
hibi
tors
; CH
S: C
lalit
Hea
lth S
ervi
ce;
GPR
D: G
ener
al P
ract
ice
Rese
arch
Dat
abas
e.
Oh YH et al . Bisphosphonate and gastrointestinal tract
cancer
-
5784 October 28, 2012|Volume 18|Issue 40|WJG|www.wjgnet.com
Kingdom General Practice Research Database and re-ported that
bisphosphonate use increases esophageal cancer risk (RR 1.30, 95%
CI: 1.02-1.66). The cancer-promoting effect was even greater in
patients who used the drug for more than 3 years (RR 2.24, 95% CI:
1.47-3.43). We can infer from this result that bisphos-phonate
should be restricted among people with risk factors for esophageal
cancer, such as Barrettv's esopha-gus. However, according to the
study of Nguyen et al[12], the use of oral bisphosphonate does not
increase the risk of esophageal adenocarcinoma in patients with
Barrett's esophagus (incidence density ratio 0.92; 95% CI:
0.21-4.15). The risk of esophageal adenocarcinoma in patients with
Barrett's esophagus is 30- to 125-fold
greater than the risk in the general population[21]. The
carcinogenic effect of oral bisphosphonate, including damage to the
esophagus due to the toxicity of the drug itself and the effect of
contact between the pill and the esophageal mucosa[15], may
expedite the development of esophageal cancer in patients with
Barrett's esophagus. However, a correlation between the risk of
esophageal adenocarcinoma and use of oral bisphosphonate by
pa-tients with Barrett's esophagus is inconsistent with the concept
of the so-called Barrett pathway.
Several in vivo and in vitro studies suggest that
bispho-sphonate has anticancerous properties[1-5]. Clinical
stud-ies also implicate the anticancerous effect of bisphos-phonate
in breast cancer[22]. It can be inferred from these
Table 4 Assessment of study quality
Study Quality assessment items
Representativeness Ascertainment of exposure: Secure record or
structured interview
Demonstration that outcome
of interest
Assessment of outcome: Independent blind assessment or record
linkage was
not present at start of study
Study controls for age, cigarette smoking, BMI status
Cohort studies Steinbuch et al[9] - (female) + + + - (randomized
controlled trials) Abrahamsen et al[10] + + - + + (age) Solomon et
al[11] - (medicare beneficiaries) + - + - (not reported) Cardwell
et al[7] + + + + +++ (age, cigarette smoking, BMI) Case-control
studies Green et al[8] + + - + +++ (age, cigarette smoking, BMI)
Nguyen et al[12] - (Barrett’s esophagus) + + + + (age) Rennert et
al[13] - (female) + + + ++ (age, BMI)
BMI: Body mass index.
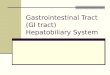
Additional studies identified from relevant articles (n = 2)
Identified articles from databases (n = 740): PubMed (n = 331),
EMBASE (n = 362), Cochrane Library (n = 47)
Total identified articles (n = 742)
Duplicates (n = 51)
Excluded articles (n = 661) After review of title and/or
abstract (not relevant for the study or follow up duration shorter
than 2 years)
Articles screened (n = 691)
Full-text articles assessed for eligibility (n = 30)
Articles included in qualitative synthesis (n = 6)
Articles included in quantitative synthesis (meta-analysis) (n =
6); cohort 3, case control 3
Excluded articles (n = 24)No available data for outcome
measures
Figure 1 Flow diagram of the identification of the relevant
cohort studies and case-control studies.
Oh YH et al . Bisphosphonate and gastrointestinal tract
cancer
-
5785 October 28, 2012|Volume 18|Issue 40|WJG|www.wjgnet.com
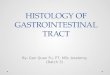
Study RR (95% CI) Weight
Overall 0.35 (0.14, 0.85) 13.47
Abrahamsen et al [10] 0.55 (0.06, 4.72) 2.97
Solomon et al [11] 1.07 (0.77, 1.49) 36.40
Cardwell et al [7] 1.30 (1.02, 1.66) 41.36
Green et al [8] (esophagus) 0.81 (0.18, 3.72) 5.80
Nguyen et al [12] 0.96 (0.65, 1.42) 100.00
Overall (I 2 = 52.8%, P = 0.076)
Long-term follow up
Cardwell et al [7] 1.23 (0.66, 2.30) 42.39
Green et al [8] (esophagus) 2.24 (1.47, 3.43) 57.61
Overall (I 2 = 58.8%, P = 0.119) 1.74 (0.97, 3.10) 100.00
NOTE: Weights are from random effects analysis
0.2 0.5 1 2 5
A
B
.. ..
Study RR (95% CI) Weight
Overall
Abrahamsen et al [10] 1.23 (0.68, 2.22) 15.71
Cardwell et al [7] (stomach) 0.78 (0.50, 1.23) 27.14
Green et al [8] (stomach) 0.87 (0.64, 1.19) 57.16
Overall (I 2 = 0.0%, P = 0.472) 0.89 (0.71, 1.13) 100.00
Long-term follow up
Green et al [8] (stomach) 0.54 (0.24, 1.18)
NOTE: Weights are from random effects analysis
0.2 0.5 1 2 5
Study RR (95% CI) Weight
Overall 0.87 (0.77, 1.00) 55.19
Green et al [8] (colorectal) 0.41 (0.25, 0.67) 44.81
Rennert et al [13] 0.62 (0.30, 1.29) 100.00
Overall (I 2 = 88.0%, P = 0.004)
Long-term follow up
Green et al [8] (colorectal) 0.88 (0.67, 1.15) 54.82
Rennert et al [13] 0.39 (0.22, 0.68) 45.18
Overall (I 2 = 84.6%, P = 0.011) 0.61 (0.28, 1.35) 100.00
NOTE: Weights are from random effects analysis
C
0.2 0.5 1 2 5
Figure 2 Association between bisphosphonate use and some cancer
risk using the meta-analysis of the random effects model. A:
Esophageal cancer risk; B: Gastric cancer risk; C: Colorectal
cancer risk.
Oh YH et al . Bisphosphonate and gastrointestinal tract
cancer
-
5786 October 28, 2012|Volume 18|Issue 40|WJG|www.wjgnet.com
studies that there is no significant association between the use
of oral bisphosphonate and the risk of esopha-geal cancer because
bisphosphonate has anticancerous effects. As for procancerous
effects, oral bisphosphonate directly irritates the esophageal
mucosa and induces erosive esophagitis. On the contrary,
bisphosphonate directly and indirectly interferes with cancer cell
growth. Our finding about the correlation between the risk of
esophageal cancer and oral bisphosphonate use sug-gests that the
procancerous and anticancerous effects of bisphosphonate may cancel
each other out.
There is also an implication about esophageal cancer within the
statistical results in our study. Two observa-tional studies that
have great significance in our meta-analyses Caldwell et al[7] and
Green et al[8], reported dis-crepant results (Figure 2A). According
to the analyses of Dixon et al[23], the time-dependent RRs of
esophageal cancer and oral bisphosphonate indicate no significant
increased risk for esophageal cancer within 3 years of oral
bisphosphonate use. However, when these inves-tigators restricted
their analyses to bisphosphonate use for more than 3 years, their
results were different[23]. The Caldwell study[7] reported a RR of
1.01 (95% CI: 0.48-2.12); Green et al[8] reported a RR of 2.24 (95%
CI: 1.47-3.43). The result of our meta-analysis was a RR of 1.74
(95% CI: 0.97-3.10) for the follow-up longer than 3 years. Our
results show no statistical correlation between the long-term oral
bisphosphonate use and the risk of esophageal cancer. However, in
the study of Caldwell et al[7], the RR increased to 1.23 (95% CI:
0.66-2.3) when the analysis was restricted to a group of patients
with a mean bisphosphonate use duration of 6.8 years. These results
indicate that there is somewhat an association between prolonged
oral bisphosphonate use and risk of esophageal cancer. Both studies
used data from the Uinted Kingdom General Practice Research
Database. Inconsistency between the 2 studies may be explained by
differences in study design and confounding that could not be
measured.
As stated previously, oral bisphosphonates induce
esophagitis[15] and esophageal cancer that can be devel-oped from
reflux esophagitis through the Barrett path-way[19,20], and this is
not a one-time process; it takes time. For this reason, recurrent
injuries and healing processes induced by prolonged oral
bisphosphonate use could be clinically meaningful factors. The
long-term effect of oral bisphosphonate could be confirmed by an
observa-tional study that focuses on much longer periods of oral
bisphosphonate use.
Regarding gastric cancer, our results show no signifi-cant
association with oral bisphosphonate use. There is only 1 study
that estimates RR dependent on duration of oral bisphosphonate use.
Although there is no sta-tistical significance, Green et al[8]
found that RR is less for those using oral bisphosphonate longer
than 3 years (RR 0.54, 95% CI: 0.24-1.18) than for those using oral
bisphosphonate shorter than 3 years (RR 1.03, 95% CI: 0.67-1.59 for
less than 1 year; RR 0.89, 95% CI: 0.52-1.53
for 1-3 years). This implies that there is no cumulative effect
of oral bisphosphonate on the risk of gastric can-cer. If
bisphosphonate has competing procancerous and anticancerous
properties, it may not affect the risk of cancer.
We performed a random-effects model analysis of the data on
colorectal cancer because of high heteroge-neity (I2 = 88.0%, P =
0.004). According to our meta-analysis, oral bisphosphonate use
demonstrates no effect on the risk of colorectal cancer (RR 0.62,
95% CI: 0.30-1.29). The analysis of the long-term use (more than 3
years) revealed that there is no statistically sig-nificant
association between oral bisphosphonate use and colorectal cancer
(RR 0.61, 95% CI: 0.28-1.35). However, the subgroup analysis shows
a significant negative association between oral bisphosphonate use
and the incidence of colorectal cancer (RR 0.87, 95% CI: 0.77-1.00;
RR 0.41, 95% CI: 0.25-0.67). Therefore, it may be hasty to conclude
on the basis of overall meta-analysis that oral bisphosphonate use
does not affect colorectal cancer. In the study by Rennert et
al[13], cases and controls were matched for age, ethnicity, family
history of colorectal cancer, sports activity, vegetable
consumption, body mass index (BMI), low-dose aspirin use, statin
use, postmenopausal hormone use, calcium supplement use, and
vitamin use, all of which can affect the risk of colorectal cancer.
However, in Green et al[8], RRs were only adjusted for smoking
status, alcohol in-take and BMI. Thus, there were important
differences in the study design and quality of methods.
The study by Rennert et al[13] implies that oral bispho-sphonate
has a protective effect against colorectal and breast cancers. The
anticancerous effects of bisphospho-nate, such as promoting
apoptosis[2], inhibiting tumor cell adhesion and invasion[3],
inhibiting angiogenesis[4], al-tering tumor-associated macrophage
function[4], and en-hancing immune surveillance, as previously
mentioned, may have a key role in such a protective effect. One
study reported that ibandronate reduces the incidence of colorectal
dysplasia in mice with induced ulcerative colitis[24]. In
colorectal cancer, different from esophageal cancer, oral
bisphosphonate does not directly injure the intestinal mucosa or
induce chronic mucosal inflamma-tion and healing processes.
Considering this background, the results of our me-ta-analyses
should be interpreted as inconclusive. A well-designed randomized
controlled study or prospective cohort study is needed to confirm
the preventive effect of oral bisphosphonate against colorectal
cancer.
Our study has a few limitations. First, the number of studies we
analyzed is small. There have been few studies about the
correlation between oral bisphosphonate use and the risk for
gastrointestinal cancer. For this reason, each study that reported
on colorectal cancer reported a negative association, but the
overall meta-analysis showed no statistical significance. Thus,
oral bisphos-phonate use is seemingly irrelevant to colorectal
cancer. Second, the quality of our study depends on data from
Oh YH et al . Bisphosphonate and gastrointestinal tract
cancer
-
5787 October 28, 2012|Volume 18|Issue 40|WJG|www.wjgnet.com
original publications. Our study inevitably inherits some
problems from the observational studies, such as selec-tion bias,
surveillance bias, and confounding. For exam-ple, more esophageal
and gastric abnormalities might be observed in bisphosphonate users
simply because they receive more endoscopic exams for abdominal
discom-fort caused by oral bisphosphonate.
We discussed the small number of studies regarding
bisphosphonate use and development of gastrointes-tinal cancer in
our article as a limitation. However, the actual number of overall
subjects in our meta-analysis is not too small. In cohort studies,
124 686 subjects with mean follow up of 3.88 years were included in
the final analysis. In case of case-control studies, there were
3070 esophageal cancer cases, 2018 gastric cancer cases and 11 574
colorectal cancer cases were included as well. Moreover, the
results of two large observational studies were inconsistent.
Caldwell et al[7] showed no significant association between
bisphosphonate use and esophageal cancer. On the other hand, Green
et al[8] had revealed the significant association. The inconsistent
results of ob-servational studies suggest the need of further
studies as well as a meta-analysis.
Despite the negative results, our study is meaningful since it
provides not an ultimate but a reasonable interim conclusion
regarding the safety of bisphosphonate use before definite
accumulation of long-term observational studies.
In summary, our meta-analyses indicate that there is no
significant association between oral bisphosphonate use and the
risk of gastrointestinal cancer. Oral bisphos-phonate use has no
significant association with the risk of esophageal cancer. There
is an increased, though not statistically significant, risk of
esophageal cancer in long-term users of oral bisphosphonate. An
observational study focused on long-term use of bisphosphonate is
needed to confirm this finding. The risk of gastric can-cer is not
associated with oral bisphosphonate use. Each study reporting on
colorectal cancer indicates a negative association between the risk
of colorectal cancer and oral bisphosphonate use, but our
meta-analysis showed no statistically significant association. The
confidence in-tervals were large (95% CI: 0.30-1.29). Thus, a
random-ized controlled trial or prospective cohort study should be
performed to confirm the preventive effect of oral
bisphosphonate.
COMMENTSBackgroundThere rises concerns about bisphosphonate use
after the reports of 23 cases of esophageal cancer in the United
States and another 31 cases in Europe and Japan, all occurring from
1995 through 2008 among patients using oral bisphosphonates.
Bisphosphonate induced esophagitis, Barrett's esophagus and gastric
ulcer can be the precancerous condition. There were observational
studies to evaluate the risk between esophageal cancer and
bisphosphonate use. But the results were inconsistent. So the
overall evaluation of the associa-tion between gastrointestinal
cancer and bisphosphonate is required. Research
frontiersMeta-analysis was used to evaluate the risk of
bisphosphonate for gastrointes-
tinal cancer (esophageal, stomach, and colorectal cancer) in
this study.Innovations and breakthroughsThis meta-analysis
systemically assessed the relation between bisphosphonate use and
gastrointestinal cancer risk, and also showed site specific,
long-term follow up results.ApplicationsThe results of
meta-analysis in this study show that use of bisphosphonate has no
significant association with gastrointestinal cancers. According to
the results, bisphosphonate can be used without charge of
carcinogen for now. But there should be a far more long-term
observational studies to guarantee the long-term safety.
TerminologyMeta-analysis is method focused on contrasting and
combining results from different studies to show the overall
conclusion. It is essential component of a systematic review
procedure. Peer reviewThis is a good descriptive study in which
authors perform a meta-analysis of observational studies to further
elucidate the relationship between oral bisphos-phonate use and
gastrointestinal cancer risk. The results are interesting and
suggest that oral bisphosphonate use had no significant effect on
gastrointesti-nal cancer risk.
REFERENCES1 Green J, Lipton A. Anticancer properties of
zoledronic acid.
Cancer Invest 2010; 28: 944-9572 Hiraga T, Williams PJ, Ueda A,
Tamura D, Yoneda T. Zole-
dronic acid inhibits visceral metastases in the 4T1/luc mouse
breast cancer model. Clin Cancer Res 2004; 10: 4559-4567
3 Boissier S, Ferreras M, Peyruchaud O, Magnetto S, Eb-etino FH,
Colombel M, Delmas P, Delaissé JM, Clézardin P. Bisphosphonates
inhibit breast and prostate carcinoma cell invasion, an early event
in the formation of bone metastases. Cancer Res 2000; 60:
2949-2954
4 Coscia M, Quaglino E, Iezzi M, Curcio C, Pantaleoni F, Riganti
C, Holen I, Mönkkönen H, Boccadoro M, Forni G, Musiani P, Bosia A,
Cavallo F, Massaia M. Zoledronic acid repolarizes tumour-associated
macrophages and inhibits mammary carcinogenesis by targeting the
mevalonate path-way. J Cell Mol Med 2010; 14: 2803-2815
5 Sato K, Kimura S, Segawa H, Yokota A, Matsumoto S, Ku-roda J,
Nogawa M, Yuasa T, Kiyono Y, Wada H, Maekawa T. Cytotoxic effects
of gammadelta T cells expanded ex vivo by a third generation
bisphosphonate for cancer immuno-therapy. Int J Cancer 2005; 116:
94-99
6 Wysowski DK. Reports of esophageal cancer with oral
bisphosphonate use. N Engl J Med 2009; 360: 89-90
7 Cardwell CR, Abnet CC, Cantwell MM, Murray LJ. Expo-sure to
oral bisphosphonates and risk of esophageal cancer. JAMA 2010; 304:
657-663
8 Green J, Czanner G, Reeves G, Watson J, Wise L, Beral V. Oral
bisphosphonates and risk of cancer of oesophagus, stomach, and
colorectum: case-control analysis within a UK primary care cohort.
BMJ 2010; 341: c4444
9 Steinbuch M, D”Agostino RB, Mandel JS, Gabrielson E, McClung
MR, Stemhagen A, Hofman A. Assessment of mortality in patients
enrolled in a risedronate clinical trial program: a retrospective
cohort study. Regul Toxicol Pharma-col 2002; 35: 320-326
10 Abrahamsen B, Eiken P, Eastell R. More on reports of
esophageal cancer with oral bisphosphonate use. N Engl J Med 2009;
360: 1789; author reply 1791-1792
11 Solomon DH, Patrick A, Brookhart MA. More on reports of
esophageal cancer with oral bisphosphonate use. N Engl J Med 2009;
360: 1789-1790; author reply 1789-1790
12 Nguyen DM, Schwartz J, Richardson P, El-Serag HB. OralOral
bisphosphonate prescriptions and the risk of esophageal
ad-enocarcinoma in patients with Barrett‘s esophagus. Dig Dis Sci
2010; 55: 3404-3407
COMMENTS
Oh YH et al . Bisphosphonate and gastrointestinal tract
cancer
-
5788 October 28, 2012|Volume 18|Issue 40|WJG|www.wjgnet.com
13 Rennert G, Pinchev M, Rennert HS, Gruber SB. Use of
bisphosphonates and reduced risk of colorectal cancer. J Clin Oncol
2011; 29: 1146-1150
14 Robins HI, Holen KD. More on reports of esophageal cancer
with oral bisphosphonate use. N Engl J Med 2009; 360: 1790; author
reply 1791-1792
15 Abraham SC, Cruz-Correa M, Lee LA, Yardley JH, Wu TT.
Alendronate-associated esophageal injury: pathologic and endoscopic
features. Mod Pathol 1999; 12: 1152-1157
16 Singh SP, Odze RD. Multinucleated epithelial giant cell
changes in esophagitis: a clinicopathologic study of 14 cases. Am J
Surg Pathol 1998; 22: 93-99
17 Graham DY, Malaty HM. Alendronate and naproxen are
synergistic for development of gastric ulcers. Arch Intern Med
2001; 161: 107-110
18 Graham DY. What the gastroenterologist should know about the
gastrointestinal safety profiles of bisphosphonates. Dig Dis Sci
2002; 47: 1665-1678
19 Chow WH, Finkle WD, McLaughlin JK, Frankl H, Ziel HK,
Fraumeni JF. The relation of gastroesophageal reflux disease and
its treatment to adenocarcinomas of the esophagus and gastric
cardia. JAMA 1995; 274: 474-477
20 Lagergren J, Bergström R, Lindgren A, Nyrén O. Symptom-atic
gastroesophageal reflux as a risk factor for esophageal
adenocarcinoma. N Engl J Med 1999; 340: 825-831
21 Pera M. Trends in incidence and prevalence of specialized
intestinal metaplasia, barrett”s esophagus, and adenocarci-noma of
the gastroesophageal junction. World J Surg 2003; 27: 999-1008;
discussion 1006-1008
22 Chlebowski RT, Col N. Bisphosphonates and breast cancer
prevention. Anticancer Agents Med Chem 2012; 12: 144-150
23 Dixon WG, Solomon DH. Bisphosphonates and esophageal
cancer--a pathway through the confusion. Nat Rev Rheumatol 2011; 7:
369-372
24 Sassa S, Okabe H, Nemoto N, Kikuchi H, Kudo H, Saka-moto S.
Ibadronate may prevent colorectal carcinogenesis in mice with
ulcerative colitis. Anticancer Res 2009; 29: 4615-4619
S- Editor Gou SX L- Editor A E- Editor Xiong L
Oh YH et al . Bisphosphonate and gastrointestinal tract
cancer