Embed Size (px)
Citation preview

Birth Trauma
DR. Agelebe E.
Bowen University Teaching Hospital, Ogbomoso.

Birth trauma
• The term “Birth trauma” Injuries to the infant that result from mechanical forces (i.e., compression, traction) during delivery

Epidemiology
• Even though most women give birth in modern hospitals surrounded by medical professionals, seven of every 1,000 births result in birth injuries.
• Birth injuries account for fewer than 2% of neonatal deaths.

Factors Predisposing to Birth Trauma
Maternal Factors Fetal Factors
Prolonged or rapid delivery Abnormal presentation (breech)
Cephalopelvic disproportion, Very low birth weight infant or extreme prematurity
small maternal stature, maternal Macrosomic babies
pelvic anomalies Fetal malformation
Deep transverse arrest of the fetus
Obstetric interventions Cesarean section Versions and extraction
OligohydramniosPrimiparity
Large fetal head

Classification of birth injuries
• I. Soft-tissue injuries
-Abrasions
- Erythema petechia
- Ecchymosis
- Lacerations
- Subcutaneous fat necrosis
- Retinal hemorrhage
- Subconjunctival hemorrhage
Abrasions and lacerations sometimes may occur as scalpel cuts during cesarean delivery or during instrumental delivery (i.e, vacuum, forceps). Infection remains a risk, but most uneventfully heal.
Management consists of careful cleaning, dressing , and observation. Lacerations occasionally require suturing.

Subcutaneous fat necrosis.
Irregular,hard,nonpitting,subcutaneous
induration with overlying dusky red-purple
discoloration on the extremities, face, trunk,
or buttocks may be caused by pressure
during delivery.
No treatment is necessary. Subcutaneous fat
necrosis sometimes calcifies.

Petechiae and ecchymosis
• Common manifestation of birth trauma in the newborn.
• Rule out coagulation disorders or infections etiology
• This lesions resolve spontaneously within 1 week
• Petechiae of the skin of the head and neck are common.
• If no secondary cause parents should be assured that they are temporary and they are delivery injury.

Classification of birth injuries
• II. Cranial injuries
-Caput succedaneum
- Cephalohematoma
- Subgaleal hemorrhage
- Linear fractures
- Intracranial hemorrhages

Caput succedaneum
• The most commonly observed scalp lesion
• Observed usually with vertex delivery.
• Edematous area situated over the portion of the scalp .
• The swelling is composed of blood or serum, or both
• No specific treatment is required , the swelling is usually subsided within few days.

Cephalohematoma
• A subperiosteal hemorrhage, hence always limited to the surface of one cranial bone.
• Cephalohematomas occur in 1–2% of live births. • No discoloration of the overlying scalp occurs, and
swelling is not usually visible for several hours after birth because subperiosteal bleeding is a slow process.
• The lesion becomes a firm tense mass with a palpable rim localized over 1 area of the skull.
• Most cephalohematomas are resorbed within 2 wk–3 mo, depending on their size.
• Hyperbilirubinemia may result if hematomatomaresolution due to blood lyses .


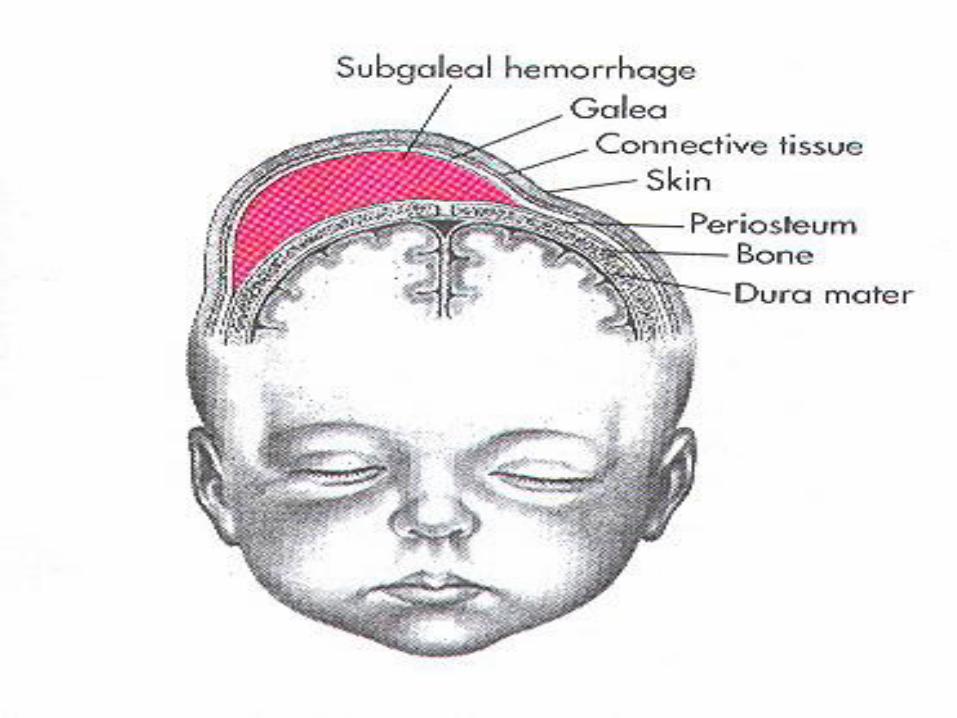
Subgaleal hemorrhage
• Subgaleal hemorrhage is bleeding into the subgaleal compartment .
• Often associated with vacuum-assisted delivery.
• The mechanism of injury is most likely secondary to a linear skull fracture, suture diastasis or fragmentation of the superior margin of the parietal bone, and/or rupture of the emissary vein

Subgaleal hemorrhage
• Serial head circumferences may detect any increase due to hemorrhage .
• The bleeding may extend to the posterior aspect of the ear and neck.
• Monitoring of the bleeding times and coagulation is important because of diff of Haemophilia A.
• Assessment to the level of consciousness.
• Assessment to the level of Hb and Hct.
• Increase in billirubin is expected due to blood lyses.
• These lesions typically resolve over a 2–3 week period.

Classification of birth injuries
• III. Intracranial hemorrhage
–subdural hemorrhage
–subarachnoid hemorrhage
– intra- and periventricular hemorrhage
–parenchyma hemorrhage

INTRACRANIAL HEMORRHAGE
• occur in 20% -40% of infants with birth weight under 1500 gm but is less common among more mature infants.
• Intracranial hemorrhage may occur in the subdural, subarachnoid, intraventricular or intracerebral regions.
• Subdural and subarachnoid hemorrhage follow head trauma e.g., in breech, difficult and prolonged labor and after forceps delivery.
• Other forms of intracranial bleeding are associated with immaturity and hypoxia.

Predisposing factors of IVH
• Prematurity
• Respiratory distress syndrome
• Hypoxic ischemic or hypotensive injuries
• Reperfusion of damaged vessels
• Hypertension
• Forceps delivery

The risk factors for IVH in low-birth-weight infants
• Impaired autoregulation
• Seizures
• Manipulative delivery
• Infusion of hyperosmotic solutions
• Rapid colloid infusion
• Asphyxia
The etiologic factors with IVH in low-birth-weight infants (Intravascular outflow factors)
• Respiratory distress
• Pneumothorax
• Continuous positive airway pressure• Relatively large blood flow to deep cerebral
structures• Hypoxic-ischemic injury to germinal matrix or
its vessels• Poor structural support of germinal matrix
vessels

Clinical manifestation IVH
• Absent Moro reflex
• Poor muscle tone
• Lethargy
• Excessive somnolence
• Pallor or cyanosis
• Respiratory distress
• DIC
• Jaundice

Clinical manifestation IVH
• Bulging anterior fontanel
• Hypotonia
• Weakness, seizures, muscular twitching
• Temperature instability
• Brain stem signs (apnea, lost extraocular movements, facial weakness, abnormal eye sing)

Laboratory correlates of blood loss
• Metabolic acidosis
• Low hematocrit
• Hypoxemia, hypercarbia
• Respiratory acidosis
• Thrombocytopenia and prolongation of protrombin time (PT) and partial thromboplastin time (PTT)
Diagnosis IVH
• Transfontanel cranial ultrasonography
• Computed tomography
• Haematocrit

Outcomes and prognosis
• Patients with massive bleeding have a poor prognosis. About 10-15% infants may develop post haemorrhagic hydrocephalus and chronic neurological pathology

Facial paralysis can be caused by pressure on the facial nerves during birth or by the use of forceps during birth. The affected side of the face droops and the infant is unable to close the eye tightly on that side. When crying the mouth is pulled across to the normal side.
Classification of birth injuries
• IV. Bone and spinal cord
– fractures of vertebra
– Erb-Duchenne paralysis
–Klumpke paralyses
–Phrenic nerve paralyses
– Facial nerves palsy– Clavicular fractures
– Fractures of long bones
– Sternocleido-mastoid injury

Duchenne-Erb paralysis
• Injury to the 5th and 6th cervical nerves
• Affected arm is adducted, internally rotated
• Forearm is in pronation
• Wrist is flexed
• Arm falls limply to the side of the body when passively adducted
• Moro, biceps and radial reflexes absent
Klumpke’s paralysis
• injury to the 7th and 8th cervical and 1st thoracic spinal nerves
• Horner syndrom (ipsilateral ptosis and miosis) if the thoraxic spinal nerve is involved
• Absent of movements of the wrist

Phrenic nerve palsy
• Injury to the C3,C4 or C5
• Brachial plexus injury
• Respiratory distress
• Paradox (upward) movement during inspiration

Clavicular fracture
• Most common
• Crepitus, palpable bony irregularity
• sternoclaidomastoid muscle spasm
• Cry during movement of upper extremities
Long bone injures
• Loss of spontaneous arm or leg movement is usually the first sign of humeral or femoral injury, followed by swelling and pain on passive motion

Classification of birth injuries
• V. Intra-abdominal injuries
- Liver hematoma
- Splenic hematoma
- Adrenal hemorrhage
- Renal hemorrhage
Intraabdominal injures – target organ
• Liver
• Spleen
• Adrenal gland (breach presentation)

Intraabdominal injures
• Sudden presentation
• Shock
• Abdominal distension
• Bluish discoloration, jaundice, pallor
• Poor feeding
• Tarchypnea, tachycardia
• History of difficult delivery

Conclusion
• Good ANC
• Planned delivery
• Incase of birth trauma patients should be closely monitored and followed up
• Exclude secondary causes




























