Embed Size (px)
Citation preview

Bipolar Disorder in Bipolar Disorder in Women –Meeting Women –Meeting the Challengethe Challenge
Nicole Harrington Cirino M.D.Nicole Harrington Cirino M.D.
Wildwood Psychiatric Resource CenterWildwood Psychiatric Resource Center
Beaverton, OregonBeaverton, Oregon
www.wildwoodpsych.comwww.wildwoodpsych.com

DisclosureDisclosure
GlaxoSmithKlineGlaxoSmithKline Speakers BureauSpeakers Bureau
Pfizer Pharmaceuticals Inc.Pfizer Pharmaceuticals Inc. Speakers BureauSpeakers Bureau Educational GrantsEducational Grants
Off label use of products will be discussedOff label use of products will be discussed

The ChallengeThe Challenge
Women with Bipolar Disorder describe…. Women with Bipolar Disorder describe…. worse overall health and well-being worse overall health and well-being compared with mencompared with men (MCOS-SF-20) (MCOS-SF-20) despite equivalent Global Assessment of despite equivalent Global Assessment of Function (GAF) scores.Function (GAF) scores.

Reproductive Cycle
Bipolar Disorder

PrevalencePrevalence
Bipolar I with equal gender distributionBipolar I with equal gender distribution Bipolar II more common in women (3.2 to Bipolar II more common in women (3.2 to
1 ratio)1 ratio)

Age of OnsetAge of Onset
Women more commonly present with 1Women more commonly present with 1StSt episode depressionepisode depression
Women have later age of onset than menWomen have later age of onset than men First Depressive EpisodeFirst Depressive Episode
27 YEARS IN WOMEN27 YEARS IN WOMEN 22 YEARS IN MEN22 YEARS IN MEN
First Manic Episode First Manic Episode 26 YEARS IN WOMEN26 YEARS IN WOMEN 22 YEARS IN MEN22 YEARS IN MEN

Bipolar Depression in Bipolar Depression in WomenWomen
Women: MDE predominate vs Mania, Women: MDE predominate vs Mania, often precede maniaoften precede mania
DSM-IV Atypical features more common DSM-IV Atypical features more common in women, more common in Bipolar IIin women, more common in Bipolar II
Longer , treatment refractory depressive Longer , treatment refractory depressive episodes in womenepisodes in women
More commonly misdiagnosed as More commonly misdiagnosed as Unipolar depressedUnipolar depressed

Seasonal PatternSeasonal Pattern Seasonal pattern more common in Seasonal pattern more common in
womenwomen Bimodal peak of admissions in Spring Bimodal peak of admissions in Spring
and Fall for women onlyand Fall for women only

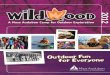
Gender Distribution of Gender Distribution of Rapid Cycling Bipolar Rapid Cycling Bipolar DisorderDisorder
0
10
20
30
40
50
60
70
80
90
100
% P
atie
nts
with R
CB
D
Male
Female
Leibenluft E . Am J Psychiatry 1996;153:163-173.

Medical Co morbidity Medical Co morbidity Higher in Women with Higher in Women with BipolarBipolar
MigraineMigraine Obesity*Obesity*
May worsen course of illnessMay worsen course of illness Thyroid DiseaseThyroid Disease
May contribute to rapid cyclingMay contribute to rapid cycling

Psychiatric Clinics of North Psychiatric Clinics of North America 26 (3) Sept 2003America 26 (3) Sept 2003
Obesity and Bipolar Obesity and Bipolar illnessillness
Obesity associated with a poorer outcome in Obesity associated with a poorer outcome in Bipolar patientsBipolar patients Increased recurrence of depressive episode in Increased recurrence of depressive episode in
obese vs. controlsobese vs. controls
LI induced weight gain more common in women, LI induced weight gain more common in women, others have not been specifically tested.others have not been specifically tested.
Obesity in Bipolar Women vs. Bipolar controls Obesity in Bipolar Women vs. Bipolar controls Overweight (44% vs. 25%)Overweight (44% vs. 25%) Obese (22% vs. 13%)Obese (22% vs. 13%)

Suicidality in Bipolar Suicidality in Bipolar WomenWomen
Higher rates of suicide attempts in Higher rates of suicide attempts in women with Bipolar D/O (and Unipolar)women with Bipolar D/O (and Unipolar)
Suicidality higher in patients with Bipolar Suicidality higher in patients with Bipolar IIII
Lithium has been associated with marked Lithium has been associated with marked reduction in suicidality in both sexesreduction in suicidality in both sexes

Reproductive Cycle Reproductive Cycle Influences on Bipolar Influences on Bipolar disorderdisorder
MensesMenses PregnancyPregnancy PostpartumPostpartum MenopauseMenopause
Reproductive Cycle
Bipolar Disorder

Estrogen – Effects on Estrogen – Effects on MoodMood
Rapid fluctuations during postpartum, Rapid fluctuations during postpartum, premenstrual and menopausal periods.premenstrual and menopausal periods.
Estrogen supports SerotoninEstrogen supports Serotonin Increases synthesis (tryptophan)Increases synthesis (tryptophan) Increased 5HT1 receptors in Dorsal RapheIncreased 5HT1 receptors in Dorsal Raphe Reduces metabolism of serotonin (Decrease Reduces metabolism of serotonin (Decrease
MAO activity)MAO activity) Estrogen potentiates Norepinephrine Estrogen potentiates Norepinephrine Antidopaminergic effectsAntidopaminergic effects

ProgesteroneProgesterone
Elevated in pregnancy with rapid drop Elevated in pregnancy with rapid drop postpartum, premenstrually, during postpartum, premenstrually, during perimenopauseperimenopause
GABA agonist propertiesGABA agonist properties Progesterone causes dysphoria, Progesterone causes dysphoria,
irritability in postmenopausal womenirritability in postmenopausal women

Menses and Effect on Menses and Effect on Mood Mood
In a retrospective interview-based study, 2/3 of In a retrospective interview-based study, 2/3 of BP women reported frequent premenstrual BP women reported frequent premenstrual mood disturbances, ¼ report depressionmood disturbances, ¼ report depression
Prospective studies have not found a specific Prospective studies have not found a specific relation between menstrual cycle and bipolar relation between menstrual cycle and bipolar disorderdisorder
Increased incidence of suicide attempts in Increased incidence of suicide attempts in premenstrual-menstrual phase from autopsies premenstrual-menstrual phase from autopsies and suicide call centerand suicide call center
Endo et al, 1978; Luggin et al, 1984; Abramowitz et al, 1982;Jacobs and Charles, 1970; Blehar et al, 1998;Wehr et al, 1988; Leibenluft et al, 1999

Impact of Reproductive Cycle: Impact of Reproductive Cycle: Childbearing YearsChildbearing Years
Most women (n=50), did not receive accurate Most women (n=50), did not receive accurate diagnosis nor treatment for BP until diagnosis nor treatment for BP until AFTERAFTER they they had childrenhad children11
Survey found health care practitioners and families Survey found health care practitioners and families are biased against women with BP becoming are biased against women with BP becoming pregnantpregnant22
45% of BP women in 1 survey were advised to not 45% of BP women in 1 survey were advised to not get pregnant get pregnant
1 Viguera AC, et al. Am J Psych 2002;159:2102-2104.2 Freeman MP, et al. J Clin Psychiatry 2002;63:264-267.3 Bouffard S et al. Presented at the American Psychiatric Association Meeting, 2001.

PregnancyPregnancy
Considered to neither protect nor worsen Considered to neither protect nor worsen symptomssymptoms
Restrospective review of 101 Bipolar women Restrospective review of 101 Bipolar women (after Li discontinuation) showed no difference (after Li discontinuation) showed no difference in pregnant vs nonpregnant controls for 40 in pregnant vs nonpregnant controls for 40 weeksweeks
Rate of recurrence for 40 weeks was 52% for Rate of recurrence for 40 weeks was 52% for both groups after Li discontinuationboth groups after Li discontinuation
Higher if discontinuation of LI<14 days.Higher if discontinuation of LI<14 days.

Pregnancy and Bipolar Pregnancy and Bipolar Disorder:Disorder:Postpartum PeriodPostpartum PeriodPostpartum period clearly destabilizes Postpartum period clearly destabilizes
moodmood BP women have 100-fold higher risk than BP women have 100-fold higher risk than
women without a psychiatric illness history of women without a psychiatric illness history of experiencing postpartum psychosis (1) (10-25%)experiencing postpartum psychosis (1) (10-25%)
40%-67% of the female BP subject population 40%-67% of the female BP subject population experienced postpartum mania or depression experienced postpartum mania or depression within 1 month of delivery (2)within 1 month of delivery (2)
70 times higher rate of suicide in the first month 70 times higher rate of suicide in the first month postpartumpostpartum
1) Pariser, Ann Clin Psychiatry 1993 2) Jefferson et al, 1987

““I killed my children….” -I killed my children….” -Andrea YatesAndrea Yates

Pregnancy
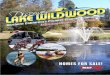
Impact of Reproductive Cycle: Impact of Reproductive Cycle: Psychiatric Admissions in the 2 Psychiatric Admissions in the 2 Years Preceding & Following Years Preceding & Following ChildbirthChildbirth
-2 Years -1 Year Childbirth +1 Year +2 Years
Ad
mis
sio
ns
/ m
on
th All admissionsn =120 (of 54,087 births)
70
60
50
40
30
20
10
Kendall RE et al. Br J Psychiatry 1987;150:662-673. Grof P et al. J of Affect Disorders 2000;61:31-39. Viguera AC, et al. Can J Psych 2002;47:426-436.

Postpartum Relapse Postpartum Relapse RatesRates
Nonacs, APA 1998Nonacs, APA 1998 Euthymic during pregnancy = Euthymic during pregnancy = 27.8%27.8% (n=18)(n=18) Illness during pregnancy = Illness during pregnancy = 68.8%68.8%(n=14)(n=14)
Cohen, Am J Psychiatry 1995Cohen, Am J Psychiatry 1995With Li prophylaxis = With Li prophylaxis = 10%10%(n=14)(n=14)Without Li prophylaxis = Without Li prophylaxis = 60%60%(n= 13)(n= 13)

Impact of Reproductive Cycle: Impact of Reproductive Cycle: MenopauseMenopause
20% of postmenopausal BPI women 20% of postmenopausal BPI women worsened (n=56)worsened (n=56)11
30% of women converted to continuous 30% of women converted to continuous cycling (no euthymia) (n=256)cycling (no euthymia) (n=256)22
Some report no changeSome report no change33
Women not using HRT more likely to report Women not using HRT more likely to report perimenopausal worsening of mood (n=50)perimenopausal worsening of mood (n=50)44
New onset Bipolar Disorder during 5New onset Bipolar Disorder during 5 thth decade decade more common in women.more common in women.
1 Blehar MC et al. Psychopharmacology Bull. 1998;34:239-243.2 Kukopulos A et al. Phamakopsychiatr Neuropsychophamakol. 1980;13:156-167.3 Wehr TA et al. Am J Psychiatry 1988;145:179-84.4 Freeman MP et al. J Clin Psychiatry 2002;63:284-287.

The Effect of Bipolar The Effect of Bipolar Disorder on the Disorder on the Reproductive cycleReproductive cycle
Menstrual irregularitiesMenstrual irregularitiesPCO, PCOSPCO, PCOSProlactin levelsProlactin levelsOCP efficacyOCP efficacyReproduction (infertility,Reproduction (infertility,
unplanned pregnancy)unplanned pregnancy)
Reproductive Cycle
Bipolar Disorder

Polycystic Ovary Polycystic Ovary Syndrome (PCOS)Syndrome (PCOS)
PCOS is among most common endocrine PCOS is among most common endocrine disorders in women of reproductive agedisorders in women of reproductive age11
Stein-Leventhal Syndrome:Stein-Leventhal Syndrome: Clinical Triad: anovulation, hirsutism, obesityClinical Triad: anovulation, hirsutism, obesity
PCOS affects 4-6% of reproductive age women PCOS affects 4-6% of reproductive age women PCOS is the leading cause of anovulatory PCOS is the leading cause of anovulatory
infertility and hirsutisminfertility and hirsutism22
PCOS is characterized by increased PCOS is characterized by increased androgens and abnormal LH/FSH ratioandrogens and abnormal LH/FSH ratio1) Franks, 1995
2) Bauer et al, 1995

Polycystic Ovarian Polycystic Ovarian Syndrome (PCOS) and Syndrome (PCOS) and Bipolar DisorderBipolar Disorder
Valproate and CarbamazepineValproate and Carbamazepine are are associated with symptoms of menstrual associated with symptoms of menstrual irregularity that may/may not lead to full irregularity that may/may not lead to full blown PCOSblown PCOS
Bipolar women prior to treatment also Bipolar women prior to treatment also show an increased risk of show an increased risk of Elevated LHElevated LH Menstrual irregularitiesMenstrual irregularities Polycystic OvariesPolycystic Ovaries

Prevalence of Menstrual Prevalence of Menstrual Disturbances in Bipolar Disturbances in Bipolar WomenWomen
Rasgon NL, Altshuler LL, Gudeman D et al. J Clin Psychiatry. 2000;61(3):173-178
Lithium Group(N = 10)
Dysmenorrhea50%
No Illness8%
Infertility8%
Miscarriages17%
OligomenorrheaIrregular Cycle
17%
Divalproex Sodium Group(N = 10)
Menorrhagia37%
OligomenorrheaIrregular Cycle
37%
Amenorrhea13%
Stillbirth13%

PCOS: Possible SequelaePCOS: Possible Sequelae
Decreased fertilityDecreased fertility MiscarriageMiscarriage Insulin ResistanceInsulin Resistance Gestational Gestational
DiabetesDiabetes Pregnancy Induced Pregnancy Induced
HTNHTN
HyperlipidemiaHyperlipidemia Cardiovascular Cardiovascular
DiseaseDisease Ovarian CancerOvarian Cancer ObesityObesity HirsutismHirsutism

Clinical Features of PCOSClinical Features of PCOSHyperandrogenismHyperandrogenism
HirsutismLobo RA et al, Ann Intern Med 2000

Effect of Mood Stabilizers (CYP3A4 Effect of Mood Stabilizers (CYP3A4 reduction) on Oral Contraceptive reduction) on Oral Contraceptive EfficacyEfficacy
Reduce Efficacy:Reduce Efficacy:
CarbamazepineCarbamazepine
TopiramateTopiramate
OxcarbazepineOxcarbazepine
No effect:No effect:
GabapentinGabapentin
LithiumLithium
Lamotrigine*Lamotrigine*
ValproateValproate
Atypical AntipsychoticsAtypical Antipsychotics*Oral Contraceptives stimulate metabolism of Lamotrigine, and reduce plasma concentrations by 40-60%-Toxicity may occur when OCP is discontinued (or pill free week)

Prolactin effectsProlactin effects
Risperidone, others increase ProlactinRisperidone, others increase Prolactin AnovulationAnovulation InfertilityInfertility Sexual dysfunctionSexual dysfunction

Women with Bipolar – The Women with Bipolar – The ChallengeChallenge
Rapid Cycling (predictor of non response for Rapid Cycling (predictor of non response for many agents)many agents)
Preponderance of Depressive episodesPreponderance of Depressive episodes Co morbid Medical conditionsCo morbid Medical conditions Increased risk of obesityIncreased risk of obesity Fertility IssuesFertility Issues Birth Control EfficacyBirth Control Efficacy Pregnancy/TeratogenesisPregnancy/Teratogenesis The Postpartum periodThe Postpartum period

Is it Worth the Is it Worth the Challenge?Challenge?

Mood Stabilizer “XX” – Mood Stabilizer “XX” – The Ideal Agent for The Ideal Agent for WomenWomen
Rapid CyclingRapid Cycling Depressive episodesDepressive episodes Co morbid Medical conditionsCo morbid Medical conditions Low risk of obesityLow risk of obesity Fertility IssuesFertility Issues Birth Control EfficacyBirth Control Efficacy Pregnancy/TeratogenesisPregnancy/Teratogenesis The Postpartum PeriodThe Postpartum Period

Bipolar Disorder in Bipolar Disorder in Women - EvaluationWomen - Evaluation
Reproductive functionReproductive function Menstrual diary: note cycle length, duration of flowMenstrual diary: note cycle length, duration of flow H/O infertilityH/O infertility
Birth Control methodBirth Control method Plans for ChildbearingPlans for Childbearing Quality of Parenting/Interpersonal relationshipsQuality of Parenting/Interpersonal relationships Metabolic StatusMetabolic Status
Weight / Ideal WeightWeight / Ideal Weight Fasting glucose and lipid profileFasting glucose and lipid profile

Treatment During Treatment During PregnancyPregnancyIntroduction to the Risk/Benefit RatioIntroduction to the Risk/Benefit Ratio

Pre-pregnancy Pre-pregnancy Consult!Consult!

FDA Categories in FDA Categories in PregnancyPregnancy
FDA categories are not necessary helpful.
Must rely on evidence based information in the literature.
A. Controlled studies fail to demonstrate risk in humans
B. No controlled studies in women, animal studies do not show risk or adverse effect in animal studies.
C Adverse effects in animals, no controlled trials in women
D Evidence of human risk exist
X Contraindicated

Pharmacologic Risks Pharmacologic Risks during Pregnancyduring Pregnancy11STST Trimester- Morphologic risk Trimester- Morphologic risk <2 weeks No maternal/ fetal exposure<2 weeks No maternal/ fetal exposure 1-5 weeks Neural Tube Development1-5 weeks Neural Tube Development 3-8 weeks Cardiac3-8 weeks Cardiac 6-9 weeks Lip and Palate6-9 weeks Lip and Palate
22ndnd-3-3rdrd Trimester Trimester Behavioral/ functional risksBehavioral/ functional risks Neonatal effects (toxicity/withdrawal)Neonatal effects (toxicity/withdrawal) Preterm laborPreterm labor Maternal side effectsMaternal side effects

= ?


VALPROIC ACID / VALPROIC ACID / PREGNANCYPREGNANCY
11stst trimester - Major congenital trimester - Major congenital anomalies(8-11%) anomalies(8-11%) 2-3% background risk2-3% background risk Neural tube defects ,open spinal defectsNeural tube defects ,open spinal defects Spina bifida most serious (1-2%)Spina bifida most serious (1-2%)
2nd-3rd trimester “Fetal valproate 2nd-3rd trimester “Fetal valproate syndrome”syndrome” 23% of children with significant 23% of children with significant
developmental delays/ low IQdevelopmental delays/ low IQ

VALPROIC ACID VALPROIC ACID RECOMMENDATIONSRECOMMENDATIONS
Reduce daily dose, 3-4 divided dosesReduce daily dose, 3-4 divided doses 4-5 mg folic acid before conception and 4-5 mg folic acid before conception and
throughout pregnancythroughout pregnancy Vitamin K (20/mg/day) first trimester and Vitamin K (20/mg/day) first trimester and
lastlast Vitamin K (IM) 1mg at birthVitamin K (IM) 1mg at birth High resolution ultrasound 16-18 High resolution ultrasound 16-18
weeks(92%)weeks(92%)

Lamotrigine Pregnancy Lamotrigine Pregnancy RegistryRegistryAs of March 2006:As of March 2006: 2232 pregnancies involving exposure to 2232 pregnancies involving exposure to
lamotrigine have been prospectively lamotrigine have been prospectively registeredregistered 332 pending delivery 332 pending delivery 488 cases lost to follow-up488 cases lost to follow-up 1412 prospectively registered pregnancies 1412 prospectively registered pregnancies
with 1440 outcomes with 1440 outcomes
Lamotrigine Pregnancy Registry. Interim Report. 1 September 1992 through 31 March 2006.

Lamotrigine Pregnancy Lamotrigine Pregnancy Registry: Risk With Registry: Risk With MonotherapyMonotherapy Estimates of malformations risk in the general Estimates of malformations risk in the general
population population 2 to 3%2 to 3% 1 1
Frequency of birth defects in women with Frequency of birth defects in women with epilepsy using AED monotherapyepilepsy using AED monotherapy 3.3 to 4.5% 3.3 to 4.5% 2,3,4,52,3,4,5
Major malformation rate associated with Major malformation rate associated with lamotrigine lamotrigine monotherapymonotherapy first trimester first trimester exposure exposure 23/831 = 2.8% (95% CI 1.8-4.2%)23/831 = 2.8% (95% CI 1.8-4.2%)66
1Honein MA et al. Teratology 1999;60:356-364. 2Holmes LB, et al. N Engl J Med 2001;344(15):1132-8.3Morrow JI, et al. Epilepsia 2001;42(Suppl 2):125. 4Morrow JI, et al. Epilepsia 2003;44(Suppl 8):60. 5Samren EB, et al. Ann Neurol 1999;46:739-46. 6Lamotrigine Pregnancy Registry. Interim Report. 1 September 1992 through 31 March 2006.

Rates of Non-Syndromic Oral Rates of Non-Syndromic Oral Clefts Associated with Clefts Associated with LamotrigineLamotrigine
NAAED reported signal of increased risk of NAAED reported signal of increased risk of non-syndromic oral clefts (cleft palate or non-syndromic oral clefts (cleft palate or cleft lip)cleft lip)1 1
8.9 per 1,000 (5/564; 3 isolated cleft 8.9 per 1,000 (5/564; 3 isolated cleft palate and 2 isolated cleft lip) associated palate and 2 isolated cleft lip) associated with lamotriginewith lamotrigine
0.37 per 1,000 in an unexposed 0.37 per 1,000 in an unexposed population grouppopulation group
24-fold increase with lamotrigine24-fold increase with lamotrigine1. Holmes LB et al (abstract). Birth Defects Research Part A: Clinical and Molecular Teratology
2006;76(5)318 2. Bille C et al. Epidemiology. 2005; 16: 311-16 3. Croen LA et al. J Med Genetics 1998;79:42-47.4. Kallen B et al. Cleft Palate Craniofacial Journal 2003;40(6):624-8.

Guidelines for Guidelines for Lamotrigine during Lamotrigine during PregnancyPregnancy
Increased lamotrigine clearance Increased lamotrigine clearance documented during pregnancydocumented during pregnancy
Higher doses may be required for clinical Higher doses may be required for clinical responseresponse
4 mg Folic Acid prior to conception and 4 mg Folic Acid prior to conception and during pregnancyduring pregnancy

Lithium in Pregnancy –Lithium in Pregnancy –Treatment of Bipolar Treatment of Bipolar DisorderDisorder Morphologic risksMorphologic risks: Epsteins’ anomaly : Epsteins’ anomaly
Incidence 1 per 1000 (.05-.1%) associated Incidence 1 per 1000 (.05-.1%) associated with Lithiumwith Lithium
4 fold increase in risk4 fold increase in risk Diagnosed by a Level II US at 16 weeks. Diagnosed by a Level II US at 16 weeks.
Often surgically correctable.Often surgically correctable. Neonatal ToxicityNeonatal Toxicity
Floppy baby syndrome, Nephrogenic Floppy baby syndrome, Nephrogenic Diabetes Insipidus in the fetus-(reversible), Diabetes Insipidus in the fetus-(reversible), Neonatal hypothyroidismNeonatal hypothyroidism

Lithium –PregnancyLithium –Pregnancy
Dose adjustmentsDose adjustments Require increase doses third trimesterRequire increase doses third trimester Prior to Delivery -dose should be cut in half Prior to Delivery -dose should be cut in half
48 hours prior to delivery (scheduled?)48 hours prior to delivery (scheduled?) Throughout pregnancy and postpartum- Throughout pregnancy and postpartum-
Lithium and thyroid levels checked Lithium and thyroid levels checked frequentlyfrequently
Doses given in three to four daily doses to Doses given in three to four daily doses to prevent nauseaprevent nausea

Typical AP agents during Typical AP agents during pregnancypregnancy
Low doses ofLow doses of High-potency High-potency agents show agents show relative safety in pregnancy-drugs of choice relative safety in pregnancy-drugs of choice haloperidol (haloperidol (HaldolHaldol)/ trifluoperazine ()/ trifluoperazine (StelazineStelazine) ) n=2900n=2900
Increase minor abnormalities with Increase minor abnormalities with ThorazineThorazine Behavioral Teratogenicity – No effect on IQBehavioral Teratogenicity – No effect on IQ Perinatal syndrome rarely reported including Perinatal syndrome rarely reported including
hypertonia, tremor, hyperreflexia-all of which hypertonia, tremor, hyperreflexia-all of which resolved without sequelaeresolved without sequelae

Atypical AP in Pregnancy-Atypical AP in Pregnancy-DataData
No national database.No national database. Case series, case reports and manufacturers data make up Case series, case reports and manufacturers data make up
a small sample size, a small sample size, Olanzapine 129, Quetiapine 39, Risperidone 61, Olanzapine 129, Quetiapine 39, Risperidone 61,
Clozapine 6Clozapine 6 Reports of gestational diabetes, obesity, seizures, Reports of gestational diabetes, obesity, seizures,
preeclampsiapreeclampsia McKenna J Clinical Psych 2006McKenna J Clinical Psych 2006 -Only Prospective study -Only Prospective study
Olanzapine (n=60)Olanzapine (n=60) Risperidone (n=49)Risperidone (n=49) Quetiapine (n=36)Quetiapine (n=36) Clozapine (n=6)Clozapine (n=6)

Atypical AP in Pregnancy Atypical AP in Pregnancy - Conclusions- Conclusions
Not enough data to establish safetyNot enough data to establish safety No association No association thus farthus far with major with major
malformations, stillbirth, prematurity, malformations, stillbirth, prematurity, neonatal complications.neonatal complications.
Olanzapine, risperidone, quetiapine with Olanzapine, risperidone, quetiapine with the most datathe most data
No data on ziprasidone (Geodon) or No data on ziprasidone (Geodon) or aripiprazole (Abilify)aripiprazole (Abilify)

The Bipolar Pregnant The Bipolar Pregnant Patient: Treatment Patient: Treatment OptionsOptions
Mild to Moderate IllnessMild to Moderate Illness Trial of safer agent/ monotherapy prior to Trial of safer agent/ monotherapy prior to
pregnancypregnancy Gradual taper of mood stabilizer before Gradual taper of mood stabilizer before
pregnancy or when pregnancy test positivepregnancy or when pregnancy test positive Maintain drug free in first trimester with low Maintain drug free in first trimester with low
threshold for reintroduction of mood stabilizerthreshold for reintroduction of mood stabilizer
Severe Bipolar illnessSevere Bipolar illness Consider continuation of mood stabilizer in first Consider continuation of mood stabilizer in first
trimester and throughout pregnancytrimester and throughout pregnancy

Treatment in Treatment in the the Postpartum Postpartum PeriodPeriod

Bipolar Disorder and Bipolar Disorder and Breastfeeding- Breastfeeding- Risk/BenefitRisk/Benefit
Due to limited and concerning lactation Due to limited and concerning lactation data, BF generally discouraged in BP data, BF generally discouraged in BP women women
Most important variable may be sleep Most important variable may be sleep deprivationdeprivation
Inform pediatrician so infant can be Inform pediatrician so infant can be monitored if infant is exposedmonitored if infant is exposed

Chaudron, Jefferson. J Clin Psych Chaudron, Jefferson. J Clin Psych 2000;61:79-90; Am J Psychiatry 2000;61:79-90; Am J Psychiatry
161:4 April 2004161:4 April 2004
Psychotropics and Psychotropics and LactationLactation
Lithium –American Academy of Lithium –American Academy of Pediatrics (AAP) -From Pediatrics (AAP) -From ContraindicatedContraindicated to to Use With CautionUse With Caution Reported cases of Li toxicity in infant.Reported cases of Li toxicity in infant. Levels 5-200% of maternal serum.Levels 5-200% of maternal serum.
Lamotrigine- AAP “may be a concern”.Lamotrigine- AAP “may be a concern”. Higher than expected levels (30-60%). Higher than expected levels (30-60%). No adverse effects reported.No adverse effects reported.

J Clinical Psychiatry 2002:63J Clinical Psychiatry 2002:63
Psychotropics and Psychotropics and LactationLactation
Valproic Acid/ Carbamazepine -AAP Valproic Acid/ Carbamazepine -AAP considers it “compatible”.considers it “compatible”. Low infant serum levels. Low infant serum levels. Reports of neonatal toxicity, hepatic failure Reports of neonatal toxicity, hepatic failure
infants <2, fetal valproate syndromeinfants <2, fetal valproate syndrome Atypical Antipsychotics – Little data Atypical Antipsychotics – Little data
(n<25)(n<25) Low infant serum levels (except clozapine).Low infant serum levels (except clozapine). Reports of jaundice, sedation, lethargy.Reports of jaundice, sedation, lethargy.

Postpartum Guidelines – Postpartum Guidelines – Do’s and Don’tsDo’s and Don’ts
Do achieve euthymia in pregnancyDo achieve euthymia in pregnancy Do consider postpartum prophylaxisDo consider postpartum prophylaxis Do discuss/”discourage” breastfeedingDo discuss/”discourage” breastfeeding Do discuss postpartum planning during Do discuss postpartum planning during
pregnancy with partner presentpregnancy with partner present Do involve all providers in care planDo involve all providers in care plan
Don’t routinely taper or change postpartumDon’t routinely taper or change postpartum Don’t wait for patient to call for PP follow upDon’t wait for patient to call for PP follow up

Reproductive Cycle
Bipolar Disorder

ResourcesResources
www.wildwoodpsych.com www.motherisk.com www.womensmentalhealth.org