Embed Size (px)
Citation preview

B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
ava i l ab l e a t www.sc i enced i r ec t . com
www.e l sev i e r. com/ loca te /b ra in res rev
Review
Bipolar disorder and mechanisms of action of mood stabilizers
Stanley I. Rapoport⁎, Mireille Basselin, Hyung-Wook Kim, Jagadeesh S. RaoBrain Physiology and Metabolism Section, National Institute on Aging, National Institutes of Health, Bldg. 9, Rm. 1S128; 9000 Rockville Pike,Bethesda, MD 20892, USA
A R T I C L E I N F O
⁎ Corresponding author. Fax: +1 301 402 0074.E-mail address: [email protected] (S.I. RapAbbreviations:AA, arachidonic acid; Acsl, lo
acid; AP, activator protein;BD, bipolar disordeCREB, cAMP response element binding prodimethoxy-4-iodophenyl)-2-aminopropane hprotein receptor kinase; GSK, glycogen synthainterleukin; LOX, lipoxygenase; LTB4, leukotrieB; NR, NMDA receptor; PEA, polyoma enhancsynthase; PLA2, phospholipase A2; cPLA2, cytfatty acid; sn, stereospecifically numbered; SS
0165-0173/$ – see front matter. Published bydoi:10.1016/j.brainresrev.2009.06.003
A B S T R A C T
Article history:Accepted 15 June 2009Available online 23 June 2009
Bipolar disorder (BD) is a major medical and social burden, whose cause, pathophysiologyand treatment are not agreed on. It is characterized by recurrent periods of mania anddepression (Bipolar I) or of hypomania and depression (Bipolar II). Its inheritance ispolygenic, with evidence of a neurotransmission imbalance and disease progression.Patients often take multiple agents concurrently, with incomplete therapeutic success,particularly with regard to depression. Suicide is common. Of the hypotheses regarding theaction ofmood stabilizers in BD, the “arachidonic acid (AA) cascade” hypothesis is presentedin detail in this review. It is based on evidence that chronic administration of lithium,carbamazepine, sodium valproate, or lamotrigine to rats downregulated AA turnover inbrain phospholipids, formation of prostaglandin E2, and/or expression of AA cascadeenzymes, including cytosolic phospholipase A2, cyclooxygenase-2 and/or acyl-CoAsynthetase. The changes were selective for AA, since brain docosahexaenoic or palmiticacid metabolism, when measured, was unaffected, and topiramate, ineffective in BD, didnot modify the rat brain AA cascade. Downregulation of the cascade by themood stabilizerscorresponded to inhibition of AA neurotransmission via dopaminergic D2-like andglutamatergic NMDA receptors. Unlike the mood stabilizers, antidepressants that increaseswitching of bipolar depression to mania upregulated the rat brain AA cascade. Theseobservations suggest that the brain AA cascade is a common target of mood stabilizers, andthat bipolar symptoms, particularly mania, are associated with an upregulated cascade andexcess AA signaling via D2-like and NMDA receptors. This review presents ways to test thesesuggestions.
Published by Elsevier B.V.
Keywords:Bipolar disorderBrainLithiumValproicCarbamazepineLamotrigineArachidonic acidPhospholipase A2
Mood stabilizerAntidepressantAntipsychoticManiaDepressionRatKinetic
oport).ng-chain acyl-CoA synthetase; AMPA, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionicr; BDNF, brain derived neurotrophic factor; Bcl-2, B-cell lymphoma-2; COX, cyclooxygenase;tein; DAT, dopamine reuptake transporter; DHA, docosahexaenoic acid; DOI, (+/−)-1-(2,5-ydrochloride; FABP, fatty acid binding protein; GRE, glucocorticoid response element; GRK, G-se kinase; 5-HT, 5-hydroxytryptamine (serotonin); 5-HTT, serotonin reuptake transporter; IL,ne B4; MR, magnetic resonance; NMDA, N-methyl-D-aspartic acid; NF-κB, nuclear factor kappaer activator; PGE2, prostaglandin E2; PK, protein kinase; mPGES, microsomal prostaglandin Eosolic PLA2; iPLA2, calcium-independent PLA2; sPLA2, secretory PLA2; PUFA, polyunsaturatedRI, selective serotonin reuptake inhibitor; TX, thromboxane
Elsevier B.V.

186 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1861.1. General background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1861.2. Heritability and genetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 187
2. Proposed mechanisms of bipolar disorder. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1872.1. Neurotransmission imbalance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1872.2. Disease progression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 187
2.2.1. Neuroinflammation and excitotoxicity. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1883. Treatment of bipolar disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 188
3.1. Mood stabilizers and atypical antipsychotics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1883.2. Antidepressants and switching to mania . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1893.3. Treatment side effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 189
3.3.1. Lithium in healthy volunteers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1893.3.2. Boxed warnings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1893.3.3. Potential neurotoxicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 189
4. The brain arachidonic acid cascade . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1894.1. Roles of arachidonic acid in the brain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1904.2. Receptors coupled to phospholipase A2 enzymes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1904.3. Quantifying brain fatty acid turnover . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 190
5. Mood stabilizers downregulate global brain arachidonic acid cascade . . . . . . . . . . . . . . . . . . . . . . . . . . 1915.1. Global turnover rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1915.2. Effects on cascade enzymes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192
5.2.1. Phospholipases A2 and acyl-CoA synthetase . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1925.2.2. Downstream oxidative enzymes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192
6. Mood stabilizers may correct a neurotransmission imbalance involving arachidonic acid . . . . . . . . . . . . . . . 1936.1. Neuroreceptor specificity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 193
6.1.1. Reconciling neurotransmitter-specific effects with global brain effects . . . . . . . . . . . . . . . . . . 1956.2. Targeting neuroreceptors and their coupling machinery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 196
7. Arachidonic acid cascade and neuroprotection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1968. Antidepressants, switching and the arachidonic acid cascade. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1979. Animal models with an upregulated AA cascade . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 197
10. The arachidonic acid cascade in bipolar disorder patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19811. Other proposed mechanisms of action of mood stabilizers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19912. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 199Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 200References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 200
1. Introduction
1.1. General background
Bipolar disorder (BD) is a major medical, social and economicburden worldwide, and its treatment represents a critical as yetunfulfilled challenge for psychiatry. The estimated lifetime costof BD in the United States ranges from $11,720 for patients witha single manic episode, to $624,785 for patients with non-responsive/chronic episodes (Begley et al., 2001). Symptomsappear on average at 22 years of age (Goodwin and Jamison,2007), but the disease often is not diagnosed until 10 years later,with treatment delayed for an additional 10 years (Ghaemi,2001). Even with intensive treatment in academic centers, BDtherapy is inadequate and patients remain symptomatic forhalf of the year on average (Post et al., 1996).
BD is characterized by recurrent changes in mood. Bipolar Iconsists of cycles of mania and depression, Bipolar II of cycles
of hypomania and depression. With rapid cycling (four or moreepisodes of depression ormania/hypomania ormixed episodeswithin a year), the disease has a poorer prognosis (Belmaker,2004; DSM-IV, 1994). In Bipolar I, which afflicts 1.2 to 1.5% of theadult US population (Narrow et al., 2002), depression is 3-timesmore common than mania (Judd et al., 2002).
BD patients frequently have multiple medical illnesses inaddition to their profound mood disturbances (Evans et al.,2005). Smoking and substance abuse are common (Begley etal., 2001). Obesity and diabetes often are caused by therapy.Sleep apnea and obsessive compulsive disorder can confoundthe presentation. The suicide rate is 5–17 fold higher than inthe general population, attaining a lifetime risk of 10% to 20%(Bostwick and Pankratz, 2000).
There is no agreed upon neuropathology or pathophysiologyof BD, and a generally accepted behavioral animalmodel for thediseasedoesnot exist (CryanandSlattery, 2007;Katoet al., 2007).Some consider BD and unipolar major depressive disorder as

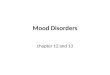
Fig. 1 – Prevalence ratio of bipolar disorder increases withrisk allele burden. A combination of more than any 15 of riskalleles significantly increases the risk for BD above the risk(1.0) in the general population, whereas a combination of any19 increases the risk 3.8 fold. From Baum et al. (2008).
187B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
part of an overlapping spectrum (Judd and Akiskal, 2003).However, in this review theywill be treated as separate entities.BD and unipolar depression differ in their responsiveness toantidepressants (Ghaemi et al., 2004; Sachs et al., 2000), theirclinical history including the presence of manic or hypomanicepisodes in BD, clinical characteristics of depression (Benazzi,2007), and family history. BD has a heritability of 86–90%, whilemajor depression has a heritability of 48–75% (McGuffin et al.,2003). Over an 11-year follow-upperiod, however, 9%of unipolardepressed patients were diagnosed as Bipolar II and 4% asBipolar I because of the later appearance of hypomanic ormanicepisodes (Akiskal et al., 1995).
1.2. Heritability and genetics
More than two-thirds of BD probands have at least one closeaffected relative or a relative with unipolar major depression.Concordance rates in monozygotic and dizygotic twins are 40%and <10%, respectively (Cardno et al., 1999; Kieseppa et al.,2004). Familial factors can determine responsiveness to lithium,the drug of choice for the disease (Alda, 1999; Grof et al., 2002).
A recent genome-wide association study with replication,involving 550,000 single nucleotide polymorphisms, impli-cated 88 different risk alleles in BD (Baum et al., 2008) (Fig. 1),consistent with a polygenic threshold inheritance (Falconer,1967). A combination of more than 15 of any of these allelessignificantly increased the risk for BD above the risk in thegeneral population, whereas a combination of any 19 increasedthe risk 3.8-fold. Multiple risk alleles also were identified inother whole genome scans (Schumacher et al., 2005; Sklar et al.,2008; Wellcome Trust, 2007; Wigg et al., 2009; Willour et al.,2003). Comparisons showed, however, that the studies hadpoor replication of positive findings, typical of measurementshaving multiple poor sensitivity items and suggesting addi-tional artifacts (Crow, 2007; Sklar et al., 2008). This limitation ofthis “bottom-up” approach makes it difficult to identifydysfunctional brain metabolic cascades characteristic of BD.
Gene linkage and candidate gene association studies alsohave identified risk alleles for BD, but such studies compared towhole genome scans are consideredunderpowered and capableof revealing only part of the genetic disturbance (Baum et al.,
2008). Many identified alleles are related to neurotransmission(Kato, 2007). They include the serotonergic (5-hydroxytrypta-mine, 5-HT) 5-HT2A receptor (Bonnier et al., 2002), the serotoninreuptake transporter (5-HTT) (Lasky-Su et al., 2005), thedopamine D2 receptor (Massat et al., 2002), the dopaminereuptake transporter (DAT) (Greenwood et al., 2006; Horschitz etal., 2005), N-methyl-D-aspartate (NMDA) receptor subunits(Martucci et al., 2006), G-protein receptor kinase-3 (GRK-3)(Barrett et al., 2003), the L-type voltage-dependent calciumchannel alpha 1C subunit (CACNA1C) (Sklar et al., 2008), and theγ-aminobutyric acid receptor (Craddock et al., 2008).
2. Proposed mechanisms of bipolar disorder
2.1. Neurotransmission imbalance
Clinical responses of BD patients to different centrally actingdrugs have suggested that BD symptoms arise from animbalance of neurotransmission, consisting of excessivedopaminergic and glutamatergic transmission and reducedcholinergic muscarinic transmission (Bunney and Garland-Bunney, 1987; Bymaster and Felder, 2002; Janowsky andOverstreet, 1995; Post et al., 1980). Thus, drugs that inhibitdopaminergic transmission, such as olanzapine and haloper-idol, have an antimanic action in the disease (Bhana and Perry,2001; Bymaster and Felder, 2002). In contrast, drugs thatstimulate dopamine synthesis (levodopa), bind to dopaminereceptors (bromocriptine), or reduce dopamine reuptake(amphetamine), can precipitate mania (Fisher et al., 1991;Peet and Peters, 1995; Sultzer and Cummings, 1989). Thecholinesterase inhibitor, physostigmine, and the cholinergicagonist, RS86, have mood-depressing effects in bipolar mania,as well as in schizophrenic and healthy subjects (Berger et al.,1989). Consistent with increased glutamate signaling in BD,memantine (1-amino-3,5-dimethyl-adamantane), an NMDAreceptor antagonist approved for treating moderate to severeAlzheimer disease (FDA, 2009), was found beneficial in bipolardepression (Davis et al., 1978; Janowsky and Overstreet, 1995;Teng and Demetrio, 2006), and Riluzole (2-amino-6-trifluor-omethoxybenzothiazole), an inhibitor of glutamate release,was reported effective in combination with lithium in an openlabel trial in BD patients (Zarate et al., 2005).
2.2. Disease progression
Symptom worsening, cognitive decline and progressive brainatrophy have been reported in BD patients, suggesting diseaseprogression. Cycles of mania and depression are reported toincrease in frequency with disease duration, and to haveshorter inter-episode intervals (Goodwin and Jamison, 2007;Kessing, 1999; Post, 1990). One study found that cognitivedeficits were present regardless of mood state, with executivefunctioning, episodic memory, and sustained concentrationmost consistently impaired (Osuji and Cullum, 2005). Structuralmagnetic resonance (MR) imaging demonstrated significantthinning of the cortical mantle, widening of cortical sulci anddilatation of the lateral cerebral ventricles in BD patients, withevidence of atrophy progression depending on symptomrecurrence (Coyle et al., 2006; Lyoo et al., 2006; Strakowski

188 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
et al., 2002). Whether atrophy is a trait marker is not certain,since BD relatives, unlike relatives of schizophrenic patients,did not demonstrate brain atrophy in one study (McDonald etal., 2006). Atrophy, cognitive decline and symptom worseningalso have been noted in schizophrenic patients (DeLisi, 2008;Nesvag et al., 2008).
2.2.1. Neuroinflammation and excitotoxicityNeuroinflammation and excitotoxicity may contribute to pro-gressive atrophy and disease worsening in BD. High levels of C-reactive protein and of pro-inflammatory cytokines have beenidentified in plasma from BD patients, suggesting a generalizedinflammatory process. Postmortem frontal cortex from BDpatients demonstrated elevated protein and mRNA levels of anumber of inflammatory markers, interleukin (IL)-1β, the IL-1receptor, inducible nitric oxide synthase, glial fibrillary acidicprotein, and myeloid differentiation primary response gene 88(Rao et al., 2009b), as well as apoptotic markers (Kim et al.,unpublished observations). MR spectroscopy demonstrated anelevated brain glutamate/glutamine ratio in adults with BD(Michael et al., 2003). Fewer NMDA receptors and reducedmRNAlevels of NMDA receptor subunits NR1, NR2A and NR3A werereported on postmortem (Kim et al., 2007), and densities ofNMDA receptor-associated post-synaptic proteins, PSD-95 andSAP102, were reduced (Rao et al., 2009b). These differences implyexcess NMDA receptor function associated with excitotoxicity(Gascon et al., 2005).
3. Treatment of bipolar disorder
There is a clear need for improved treatment of BD. Currentlyapproved agents used as monotherapy do not produce long-term responses in the majority of patients, and patientcompliance is difficult to achieve (Post et al., 1996). For example,in a collated analysis of 2300 patients with acute mania whowere given a placebo or any of 8 recognized “effective” agents asmonotherapy, patients treatedwith only one agent experienced45–60% positive symptom responses, compared with a 30%
Fig. 2 – Chemical structures of FDA-approved moodstabilizers.
positive response to placebo (Bowden et al., 2005b). Withoutfactoring in inadequate dosage and noncompliance in thisstudy, only half of the already low fraction of drug respondersmay have had a “veritable” drug response.
BD patients often are treated with more than one agent invarious doses and for various times, using combinations ofmood stabilizers, antipsychotics, antidepressants and hypno-tic benzodiazepines (Bowden, 2003). This approach is called“rational polypharmacy” (Post et al., 1996; Sachs, 1996), butoften reduces to adding a drug for a specific symptom as itappears.
3.1. Mood stabilizers and atypical antipsychotics
FDA-approved agents (Fig. 2) for treating Bipolar I include the“mood stabilizers”1 lithium (as carbonate or citrate salt,approved for mania and maintenance therapy), divalproex(Depakote®or Depakene®, containing sodium valproate andvalproic acid (2-propylpentanoic acid) in 1:1 molar ratio;approved for mania), carbamazepine (Tegretol®, 5-carba-moyl-5H-dibenz[b,f]azepine, approved for mania), and lamo-trigine (Lamictal®, 6-(2,3-dichlorophenyl)-1,2,4-triazine-3,5-diamine, approved as prophylactic treatment of Bipolar I todelay time to occurrence of the different mood episodes)(Bowden et al., 2005b; FDA, 2009; Fountoulakis et al., 2008; Ketteret al., 2005). Topiramate (Topomax®, 2,3:4,5-Di-O-isopropyli-dene-β-D-fructopyranose sulfamate), an anticonvulsant sug-gested from initial observations to be effective in BD, was laterfound ineffective in fourdoubleblind trials (Kushner et al., 2006);it is discussed below in comparative rat studies with approvedmood stabilizers.
Outcome comparisons among FDA-approved mood stabi-lizers as monotherapy have been reported (Bowden, 2003;Fountoulakis et al., 2008). For example, patients with maniaaccompanied by two or more depressive symptoms hadgreater improvement with divalproex than with lithium,whereas patients with mania alone had equivalent responsesof the order of 30–40% (Bowden, 1995; Swann et al., 1997).Divalproex or lithium in acute mania and in maintenancestudies was more effective than carbamazepine, with whichrecurrence occurred 50% more often (Kleindienst and Greil,2000; Lerer et al., 1987; Vasudev et al., 2000).
Atypical antipsychotic agents that are FDA-approved foracute mania in BD are olanzapine (Zyprexia®), aripiprazole(Abilify®), chlorpromazine (Clozaril®), risperidone (Risperdal®),quetiapine (Seroquel®), and ziprasidone (Geodon®) (Bowden et
1 This term was introduced into the psychiatric vocabularysome 20 years ago, based on observations that lithium offeredantimanic as well as antidepressant action. It was extended to theanticonvulsants, divalproex, carbamazepine and lamotrigine, yetthe first two have little efficacy against depression and lamo-trigine shows little efficacy against mania (Sobo, S., 1999. Moodstabilizers and mood swings: in search of a definition. PsychiatricTimes. 16). The term “mood stabilizer” has since been modified toidentify medication that decreases vulnerability to subsequentepisodes of mania or depression and does not exacerbate thecurrent episode or maintenance phase of treatment. (Sachs, G.S.,1996. Bipolar mood disorder: practical strategies for acute andmaintenance phase treatment. J Clin Psychopharmacol. 16, 32S–47S).

189B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
al., 2005b; FDA, 2009; Ketter et al., 2005). In addition, quetiapineis approved for bipolar depression and maintenance therapyadjunctive to lithium or divalproex, and aripiprazole andolanzapine are approved for maintenance monotherapy inBipolar I.
The atypical antipsychotics have a high affinity as antago-nists for dopamine D2 receptors, and many also have highaffinities as antagonists for serotonergic 5-HT2 receptors.Some also have affinities for adrenergic, histamine H1 andmuscarinic M1 receptors (Kapur and Remington, 2001). No onedrug has a clear advantage over the others for treating mania,but as a group they are less likely than conventionalantipsychotics to cause troubling extrapyramidal symptoms(Bowden et al., 2005b; Ketter et al., 2005; Simpson, 2005;Yatham, 2005). The atypical antipsychotics are especiallyuseful for rapidly dampening hyperactive motoric symptomsin bipolarmania, before lithium's effects are expressed (Bhanaand Perry, 2001; Lieberman and Goodwin, 2004; Post andCalabrese, 2004).
3.2. Antidepressants and switching to mania
The treatment of bipolar mania with mood stabilizers hasachieved some success, but treating the three-times morecommon bipolar depression remains problematic (Fountou-lakis et al., 2005). Lamotrigine is of some help, as is fluo-xetine (a selective serotonin reuptake inhibitor, SSRI) witholanzapine added, and quetiapine recently was approved asmonotherapy (Section 3.1). Paroxetine and bupropion werenot found useful as adjunctive therapy with mood stabilizersin bipolar depression (Bowden et al., 2005b; Sachs et al.,2007).
Some antidepressants increase the likelihood of “switching”to mania in depressed bipolar patients, when used as mono-therapy or with mood stabilizers (Calabrese et al., 1999a; Post etal., 2006). Elevated switch rates are reportedwith broad spectrumtricyclic antidepressants that inhibit reuptake of norepinephrineand serotonin (Kleindienst and Greil, 2000), SSRIs and mono-amine oxidase inhibitors, but not with bupropion, a norepi-nephrine and dopamine reuptake inhibitor and nicotinicantagonist (Leverich et al., 2006; Post et al., 2006). Switch ratesare reduced if an antimanic mood stabilizer is given with theantidepressant (31.6% versus 84.2%) (Ghaemi et al., 2004).
3.3. Treatment side effects
3.3.1. Lithium in healthy volunteersWhen administered to healthy volunteers, lithium causedlethargy, dysphoria, a loss of interest in interacting withothers, mental confusion (Judd et al., 1977a), slowed perfor-mance on cognitive and motor tests (Judd et al., 1977b), andaltered circadian rhythm, the most common effect being adelay in the phase of measured rhythms relative to anentraining light–dark cycle (Klemfuss, 1992). Lithium alsoincreased auditory and visual evoked responses in healthyvolunteers (Hegerl et al., 1990; Ulrich et al., 1990).
3.3.2. Boxed warningsLithium, divalproex and carbamazepine have boxed warningsbecause of safety concerns. Lithium can be nephrotoxic and
neurotoxic, whereas divalproex can produce hepatic andteratogenic effects and contribute to pancreatitis. Carbama-zepine may produce adverse hematological effects. As a class,atypical antipsychotics have a boxed warning for suddendeath in elderly patients. They increase risk for hyperglyce-mia, diabetes, and cardiovascular dysfunction, and oftenproduce severe weight gain and sedation (Bowden et al.,2005b; Ketter et al., 2005; Simpson, 2005).
3.3.3. Potential neurotoxicityIn animal and cell models, mood stabilizers and antipsycho-tic agents used in BD were shown to be neuroprotectivethrough a number of processes, including the reduction ofapoptosis and stimulation of brain neurotrophic and growthfactors (Section 7) (Chang et al., 2009; Chen et al., 1999;Chuang, 2005; Gould et al., 2004b; Lieberman et al., 2008; Lu etal., 2004). Thus, neuroprotection may underlie some of theiraction, especially in view of evidence for apoptosis, neuroin-flammation and excitotoxicity in the postmortem BD brain(Rao et al., 2009b).
On the other hand, as long-term therapy, antipsychoticsmay have neurotoxic effects. For example, chronic exposureto atypical antipsychotics produced oxidative brain damage(Martins et al., 2008; Terry et al., 2003), and 12 to 27 monthsof exposure of macaque monkeys to haloperidol or olanza-pine at therapeutically equivalent plasma concentrationscaused widespread brain shrinkage and reduced astrocytenumbers in parietal gray matter (Dorph-Petersen et al., 2005;Konopaske et al., 2008).
4. The brain arachidonic acid cascade
“How can we argue that we are treating […bipolardisorder…] at a fundamental, etiological level of the illnesswhen we don't know what the chemical problem is, whenour best guesses about how various mood stabilizers workare that they work differently from each other, and whenwe don't know how these proposed mechanisms might ormight not be related?” S. Sobo (1999)
We have yet to convert the disparate data about BDand the agents approved to treat it into a coherent under-standing of disease mechanisms and drug targets. Thelimited efficacy of each of the approved mood stabilizers asmonotherapy in bipolar mania (Bowden et al., 2005a; Ketteret al., 2001), the limited treatment of bipolar depression(Sachs et al., 2007), the many untoward side effects ofapproved agents, and the high morbidity, suicide rate andcost to society of BD, render understanding the disease anddesigning more appropriate treatments for it of the highestpriority.
Many hypotheses have been proposed for the mechanismsof action of agents approved for treating BD, particularly themood stabilizers. One, the “arachidonic acid (AA, 20:4n−6)cascade hypothesis,” asserts that these agents commonlyalleviate BD symptoms, particularly bipolar mania, by down-regulating brain AA metabolism (Chang et al., 1996, 1999; Raoet al., 2008; Rapoport and Bosetti, 2002). This hypothesis is

Table 1 – Receptors coupled to PLA2 activation andarachidonic acid signaling.
Neuroreceptors Subtypea
Coupled via G-proteinsCholinergic muscarinic M1,3,5 (Bayon et al.,1997; DeGeorge et al., 1991)Dopaminergic D2-like (Bhattacharjee et al.,2005; Vial and Piomelli, 1995)Serotonergic 5-HT2A/2C (Felder et al., 1990;Qu et al., 2003)Adrenergic β2 (Pavoine et al., 1999)Bradykinin β2 (Prado et al., 2002)Metabotropic glutamatergic mGlur1α(Nitsch et al., 1997)
Ionotropic, coupled via Ca2+
NMDA (Basselin et al., 2006a;Weichel et al., 1999)AMPA (Gaudreault et al., 2004)
Astrocytic receptors Subtypeb
TNFα (Luschen et al., 2000)IL-1β (Dinarello, 1988)Purigenic 2Y2 (Sun et al., 2005)
a References mainly for cPLA2.b Activation of both cPLA2 and sPLA2.
190 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
elaborated in this review. Other hypotheses are consideredbriefly in Section 11.
4.1. Roles of arachidonic acid in the brain
AA is an n−6 (omega-6) polyunsaturated fatty acid (PUFA) thatis esterified predominantly in the stereospecifically numbered(sn)-2 position of brain membrane phospholipids, as is the n−3PUFA, docosahexaenoic acid (DHA, 22:6n−3). Both PUFAs arederived from the diet, directly or by hepatic elongation oftheir nutritionally essential precursors, linoleic acid (18:2n−6)or α-linolenic acid (18:3n−3), respectively. Vertebrates cannotsynthesize them or their precursors de novo from 2-carbonfragments, and the brain's elongation capacity is inconse-quential (Demar et al., 2005; Holman, 1986; Igarashi et al.,2007).
When released by a phospholipase A2 (PLA2) from aphospholipid, AA and its eicosanoid metabolites have multi-ple biological effects, many of which are modulated byreleased DHA and its metabolites (Bazan, 2007; Contrerasand Rapoport, 2002; Farooqui et al., 2007; Fitzpatrick andSoberman, 2001; Serhan, 2006; Shimizu and Wolfe, 1990). AAand its metabolites can influence multiple processes withinthe brain (Piomelli, 1995), including neurotransmission (Axel-rod, 1990; DeGeorge et al., 1991; Rapoport, 2003), membraneexcitability (Xiao and Li, 1999), long-term potentiation (McGa-hon et al., 1997), gene transcription (Sellmayer et al., 1997),membrane fluidity (Bazan, 2005), neurite outgrowth (Ikemotoet al., 1997), cerebral blood flow (Stefanovic et al., 2006), sleep,memory and behavior (Chen and Bazan, 2005; Fitzpatrick andSoberman, 2001; Huang et al., 2007). Many AA metabolites areconsidered to be pro-inflammatory, whereas DHA and itsmetabolites are considered anti-inflammatory (Bazan, 2007;Farooqui et al., 2007; Serhan, 2006). AA is released fromsynaptic membrane phospholipids during normal neuro-transmission (Jones et al., 1996), whereas higher quantitiesare released, together with other fatty acids, during patholo-gical processes such as neuroinflammation, excitotoxicity,ischemia, and convulsions. These high quantities of AA andof concurrently formed lysophospholipids can cause neuro-nal damage by multiple mechanisms (Bazan et al., 1981;Chang et al., 2009; Contreras and Rapoport, 2002; Farooqui etal., 2007; Rabin et al., 1998; Rao et al., 2007c,d; Rosenberger etal., 2004).
4.2. Receptors coupled to phospholipase A2 enzymes
Three major PLA2 enzyme classes in the mammalian brainmediate receptor-initiated release of AA or DHA as secondmessengers (Burke and Dennis, 2009): (1) AA-selectivecytosolic cPLA2 (85 kDa, Type IVA), which requires <1 mMCa2+ and phosphatidylinositol-4,5-biphosphate for translo-cation to the membrane plus phosphorylation for its activa-tion (Clark et al., 1991); (2) secretory sPLA2 (14 kDa, Type IIA),which requires a much higher Ca2+ concentration (20 mM) foractivation; and (3) DHA-selective “Ca2+-independent” iPLA2
(88 kDa, Type VIA), which is considered “Ca2+-independent”from in vitro studies (Strokin et al., 2003), but can be activatedby Ca2+ derived from intracellular stores such as theendoplasmic reticulum (Nowatzke et al., 1998; Rosa and
Rapoport, 2009). cPLA2, which co-localizes with and iscoupled to cyclooxygenase (COX)-2 at post-synaptic sites,co-evolved with COX-2. iPLA2 also is found at post-synapticsites, as well as in astrocytes (Kaufmann et al., 1996; Ong etal., 1999, 2005; Sun et al., 2005; Tay et al., 1995). sPLA2
participates in neurotransmitter release from axonal term-inals (Matsuzawa et al., 1996).
Table 1 identifies receptors that are coupled to activa-tion of cPLA2 and/or sPLA2, so as to release AA frommembrane phospholipids. Coupling occurs by complexmechanisms as yet incompletely understood, and caninvolve a G-protein, entry of extracellular Ca2+ into thecell (to activate cPLA2), or release of Ca2+ from intracellularstores (Balsinde et al., 1998; Clark et al., 1991; Ertley et al.,2007; Nowatzke et al., 1998; Rosa and Rapoport, 2009;Takano et al., 2000). Post-synaptic neuroreceptors mediateAA release during neurotransmission or, with excessglutamate availability, during excitotoxicity, whereas astro-cytic cytokine receptors mediate AA release during neu-roinflammation (Axelrod, 1990; Basselin et al., 2006a;DeGeorge et al., 1991; Rao et al., 2007e; Rapoport, 2003;Rosenberger et al., 2004).
4.3. Quantifying brain fatty acid turnover
Fig. 3 illustrates the brain AA cascade, when initiated byneuroreceptor-mediated activation of PLA2 at the post-synap-tic membrane (Fitzpatrick and Soberman, 2001; Jones et al.,1996; Rapoport, 2001; Robinson et al., 1992; Shimizu andWolfe,1990). Comparable DHA and palmitic acid cascades have beendescribed (Rapoport et al., 2007; Robinson et al., 1992; Sun and

2 A fatty acid incorporation coefficient k⁎ is calculated asradioactivity in brain phospholipid at time of death T, c⁎brain(T),divided by integrated plasma radioactivity c⁎plasma to T, where t istime after beginning labeled fatty acid infusion,
(1)k =cbrain Tð Þ
R T0 cplasmadt
The rate of incorporation of the unlabeled fatty acid from plasmainto brain phospholipid equals,
Jin = kcplasma
and the turnover rate equals
(3)Turnover = Jin=cbraink
where λ is the steady-state ratio of brain fatty acid-CoA specificactivity to plasma fatty acid specific activity. λ represents the fluxof the fatty acid released from phospholipid into brain fatty acid-CoA, compared with the flux of plasma derived-AA (Fig. 3).
Fig. 3 – Model of brain arachidonic acid cascade initiatedat the synapse. AA is liberated from the stereospecificallynumbered (sn)-2 position of a phospholipid by activation(star) of phospholipase A2 (PLA2). A fraction is converted tobioactive eicosanoid, while the remainder diffuses to theendoplasmic reticulum bound to a fatty acid binding protein(FABP). There, it is converted to arachidonoyl-CoA byacyl-CoA synthetase with the consumption of 2 ATPs,then re-esterified into an available lysophospholipid byacyltransferase, or β-oxidized in mitochondria. AA in theendoplasmic reticulum exchanges freely with unesterifiedunboundAA in plasma, intowhich labeled AA (AA*) has beeninfused. Other metabolic pathways are not shown.Jin, the rate of incorporation of unesterified unlabeled AA intobrain, equals the net rate of loss by metabolism, since AAcannot be synthesized de novo in the brain. Adapted fromRapoport and Bosetti (2002).
(2)
191B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
MacQuarrie, 1989). In unanesthetized rats, it has been shownthat after AA is released from synaptic membrane phospho-lipid, a small fraction (about 4%) is rapidly metabolized to n−6eicosanoids by COX, lipoxygenase (LOX) or cytochrome P450epoxygenase enzymes. The remainder is recycled into mem-brane phospholipid via the brain arachidonoyl-CoA pool, withthe help of acyl-CoA synthetase and acyltransferase enzymesand the consumption of 2 ATPs, or is lost by β-oxidation andother pathways. Since AA cannot be synthesized de novo invertebrates, and its circulating precursor, linoleic acid, isalmost entirely oxidized after entering the brain, the AA lostbymetabolism is replaced by unesterified plasma AA, at a rateJin (Eq. (2), Footnote 2) (DeMar et al., 2006a; Rapoport et al.,2001).
The kinetics of the brain AA, DHA and palmitic acidcascades have been quantified in unanesthetized rodents byinfusing the respective radiolabel intravenously for 5 min, soas to rapidly produce a constant plasma specific activity. At5 min, the brain is exposed to high energy microwaveradiation to stop enzyme activity, and then is subjected tochemical and radiotracer analyses. The resultant data areused to calculate coefficients of incorporation k⁎, rates ofincorporation Jin, half-lives and turnover rates of the unlabeledfatty acid in whole brain and in individual brain phospholi-pids, by operational equations obtained from a kinetic model
(Robinson et al., 1992).2 Regional values of k⁎ and Jin also can beimaged by freezing rather than microwaving the brain,sectioning it in a cryostat, and subjecting the sections toquantitative autoradiography to determine regional radio-activity (Eqs. (1) and (2) in Footnote 2).
5. Mood stabilizers downregulate global brainarachidonic acid cascade
5.1. Global turnover rates
To compare central drug effects in rodents and humans,appropriate dose regiments should be chosen so as to produceclinically relevant plasma concentrations, since peripheralpharmacokinetics often differ between species. Table 2summarizes reported clinical plasma therapeutic concentra-tions of the four FDA-approved mood stabilizers and topir-amate, and experimental plasma concentrations that havebeen used in rodent studies.
Turnover rates of AA, DHA and palmitic acid in brainphospholipids, as well as values of λ (Footnote 2) weremeasured in unanesthetized rats that had been fed alithium-free diet for 6 weeks, or a LiCl-containing diet thatproduced a therapeutically relevant plasma lithium concen-tration (Table 2). As shown in Table 3, each of the three fattyacids had high turnover rates in rats on the control diet,consistent with fatty acid participation in active signalingprocesses that consume ATP (Purdon and Rapoport, 1998).Chronic lithium reduced AA turnover in brain phospholipidsby about 80%, without significantly affecting DHA or palmitateturnover (Chang et al., 1996, 1999; Rapoport and Bosetti, 2002).In later studies, chronic sodium valproate and carbamazepinealso were shown to reduce AA turnover without altering DHAturnover. In contrast, neither lamotrigine nor topiramateaffected turnover of either fatty acid (Table 4), althoughlamotrigine did reduce AA incorporation coefficients k⁎ in therat brain (Table 5) (Lee et al., 2008a).

Table 2 – Therapeutic concentration ranges of approved mood stabilizers and of topiramate, and concentrations used inexperimental rat studies.
Drug Therapeutic plasma concentrations in patients Plasma concentrations achieved in ratinfusion studies
mM
Lithium 0.6–1.2 (Camus et al., 2003; Eilers, 1995) 0.73 (Bosetti et al., 2002b; Chang et al., 1996)Carbamazepine 0.017–0.051 (Bialer et al., 1998; Eilers, 1995) 0.053 (Ghelardoni et al., 2005)Valproate 0.20–1.5 (Bowden et al., 1994; Eilers, 1995; Jacobsen, 1993) 0.21 (Chang et al., 2001)Lamotrigine 0.02–0.03 (Doose et al., 2003) 0.04 (Hassel et al., 2001; Lee et al., 2007a)Topiramatea 0.010–0.050 (Doose and Streeter, 2002) 0.018 (Ghelardoni et al., 2005)
a Failed phase III trials (Kushner et al., 2006).
192 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
5.2. Effects on cascade enzymes
5.2.1. Phospholipases A2 and acyl-CoA synthetaseConsistent with their reducing AA but not DHA turnover in ratbrain phospholipids, chronic lithium and carbamazepinedownregulated brain mRNA, protein and activity levels ofAA-selective cPLA2, without altering expression of sPLA2 orDHA-selective iPLA2 (Table 4). Reduced expression of cPLA2
was associated with a reduced brain AA-CoA concentration,the sequential product of AA hydrolysis from phospholipid bythe enzyme (Fig. 3). Lithium's downregulation of cPLA2 wasaccompanied by reduced binding activity of subunits of acPLA2 transcription factor, activator protein (AP)-2, which wasattributed to decreased brain protein kinase (PK)Cα, PKCɛ andAA-dependent PKC activities (Rao et al., 2005). Chroniccarbamazepine decreased AP-2 DNA-binding and cAMP-dependent PKA activity, as well as AP-2 phosphorylation(Rao et al., 2007b). Chronic sodium valproate did not alterexpression of any of the three PLA2 enzymes or of AP-2 (Bosettiet al., 2003; Chang et al., 2001; Rao et al., 2005), but non-
Table 3 – Chronic lithium administration selectivelyreduces arachidonic acid turnover in rat brainphospholipids.
Fatty acid λ Turnover rate (%/h)
PtdIns PtdCho PtdEtn
Arachidonic acid (20:4n−6)Control 0.04±0.00 15.3±0.4 18.3±0.6 1.1±0.1Lithium 0.18±0.02a,⁎⁎ 2.6±0.1⁎⁎ 5.0±0.3⁎⁎ 0.2±0.0⁎⁎
Docosahexaenoic acid (22:6n−3)Control 0.03±0.00 17.7±1.7 3.1±0.4 1.2±0.1Lithium 0.03±0.00 31.0±9.0 4.5±1.2 1.6±0.4
Palmitic acid (16:0)Control 0.02±00 29.1±2.6 7.0±0.4 4.1±0.4Lithium 0.02±00 26.0±1.2 5.1±0.3⁎ 3.5±0.1
After Chang et al. (1996, 1999), Rapoport and Bosetti (2002).Differs from control mean±SEM (n=5–6),⁎p<0.05, ⁎⁎p<0.01. LiCl orcontrol diet was fed for 6 weeks, giving brain lithium concentrationof 0.73 ± 0.03 mM. PtdIns, phosphatidylinositol; PtdCho,cholineglycerophospholipid; PtdEtn, ethanolamineglycerophospholipid.a An elevation in λ (Footnote 2) indicates that less AA is being providedby release fromphospholipid thanentry fromplasma.SeeFootnote2 fordefinitions of λ and turnover rate.
competitively inhibited a microsomal acyl-CoA synthetasethat is selective for AA conversion to arachidonoyl-CoA (Fig. 3)(Bazinet et al., 2006b). Chronic lamotrigine and topiramate didnot change brain expression of cPLA2, sPLA2 or iPLA2
(Ghelardoni et al., 2005; Lee et al., 2008a).
5.2.2. Downstream oxidative enzymesOnce released frombrain phospholipid, unesterified AA can beoxidized to bioactive eicosanoids (Fig. 3) (Fitzpatrick andSoberman, 2001). Prostaglandin (PG)G2 is formed in the firststep in this oxidation, and then is converted to PGH2 by COXenzymes. PGD2, PGE2, PGF2α and PGI2 may be produced fromPGH2 via PG synthases, thromboxanes (TX) (e.g. TXB2) via TXsynthases. In normal brain, PGE2 is produced preferentially viaCOX-2, TXB2 via COX-1 (Basselin et al., 2007c; Bosetti et al.,2004). Epoxyeicosatrienoic acids and hydroxyeicosatetraenoicacids also are formed via cytochrome P450 epoxygenase,whereas hydroxyperoxyeicosatetraenoic acids, leading toleukotrienes, hydroxyeicosatetraenoic acids, lipoxins andhepoxilins are produced via LOXs and other enzymes (Bosetti,2007).
The mood stabilizers approved for BD target many down-stream AA metabolic process in rat brain. In unanesthetizedrats, chronic lithium significantly reduced brain protein andactivity of COX-2, as well as PGE2 concentration (Bosetti et al.,2002a), without changing expression of COX-1, 5-LOX, cyto-chrome P450 epoxygenase or microsomal PGE synthase-1(mPGES-1) (Weerasinghe et al., 2004) (Table 4). Chronic lithiumalso elevated brain 17-OH-DHA, a precursor of anti-inflam-matory resolvins and neuroprotectins derived from DHA via15-LOX, in a rat model of neuroinflammation (Serhan, 2006).Chronic carbamazepine reduced COX activity without chan-ging the COX-1 or COX-2 protein level, and reduced brainconcentrations of PGE2 and TXB2. Protein levels of 5-LOX andcytochrome P450 epoxygenase, and the concentration of the 5-LOX product, leukotriene B4 (LTB4), also were unaltered(Basselin et al., 2007a; Ghelardoni et al., 2004). Chronic sodiumvalproate reduced brain mRNA, protein and activity levels ofboth COX-1 and COX-2, and brain concentrations of TXB2 andPGE2, their respective preferred metabolites (Basselin et al.,2008a; Bosetti et al., 2003). Protein levels of 5-LOX and ofcytochrome P450 epoxygenase and the concentration of LTB4
were unchanged. DNA-binding activity of nuclear factor (NF)-κB, a COX-2 transcription factor, was decreased in relation to adecreased level of its p50 subunit (Rao et al., 2007a). Chroniclamotrigine decreased COX-2 protein and mRNA (Lee et al.,

Table 4 – Baseline changes in whole brain arachidonic acid cascade markers after chronic administration of each of fourmood stabilizers to rats.
Target Lithium Carbamazepine Sodium valproate Lamotrigine
Fatty acid kineticsAA turnover in phospholipids ↓ (Chang et al., 1996;
Rapoport and Bosetti, 2002)↓ (Bazinet et al., 2006a) ↓ (Chang et al., 2001) Nc (Lee et al., 2007a)
AA-CoA concentration ↓ (Chang et al., 1999) ↓ (Bazinet et al., 2006a) Nc (Chang et al., 2001) Nc (Lee et al., 2007a)AA incorporation coefficient k⁎ Nc (Basselin et al., 2005b) Nc (Bazinet et al., 2006a) ↑ (Chang et al., 2001) ↓ (Lee et al., 2007a)DHA turnover in phospholipids Nc (Chang et al., 1999) Nc (Bazinet et al., 2006a) Nc (Bazinet et al., 2005) ?17-OH-DHA concentration ↑ ? ? ?Palmitate turnover inphospholipids
Nc (Chang et al., 1999) ? ? ?
EnzymescPLA2 IVA ↓ (Rintala et al., 1999;
Weerasinghe et al., 2004)↓ (Ghelardoni et al., 2004) Nc (Bosetti et al., 2003;
Chang et al., 2001)Nc (Lee et al., 2008a)
sPLA2 IIA Nc (Weerasinghe et al.,2004)
Nc (Ghelardoni et al., 2004) Nc (Bosetti et al., 2003) Nc (Lee et al., 2008a)
iPLA2 VIA Nc (Bosetti et al., 2002a;Rintala et al., 1999)
Nc (Ghelardoni et al., 2004) Nc (Bosetti et al., 2003) Nc (Lee et al., 2008a)
Acyl-CoA synthetase ? ? ↓ (Bazinet et al., 2006b) ?COX-1 Nc (Bosetti et al., 2002a) Nc (Ghelardoni et al., 2004) ↓ (Bosetti et al., 2003) Nc (Lee et al., 2008a)COX-2 ↓ (Bosetti et al., 2002a) ↓ (Ghelardoni et al., 2004) ↓ (Bosetti et al., 2003;
Rao et al., 2007a)↓ (Lee et al., 2008a)
5-LOX Nc (Weerasinghe et al.,2004)
Nc (Ghelardoni et al., 2004) Nc (Bosetti et al., 2003) ?
Cytochrome P450 epoxygenase Nc (Weerasinghe et al.,2004)
Nc (Ghelardoni et al., 2004) Nc (Bosetti et al., 2003) ?
mPGES-1 Nc (Weerasinghe et al.,2004)
? ? ?
EicosanoidsPGE2 ↓ (Basselin et al., 2007b;
Bosetti et al., 2002a)↓ (Basselin et al., 2007a;Ghelardoni et al., 2004)
↓ (Basselin et al., 2008a;Bosetti et al., 2003)
?
TXB2 Nc (Basselin et al., 2007b) Nc or ↓ (Basselin et al., 2007a;Ghelardoni et al., 2004)
Nc (Bosetti et al., 2003) ?
Leukotriene B4 ? Nc (Ghelardoni et al., 2004) Nc (Bosetti et al., 2003) ?
Transcription factorsAP-2 ↓ (Rao et al., 2005) ↓ (Rao et al., 2007b) Nc (Rao et al., 2007a) ?AP-1 ↑ (Ozaki and Chuang, 1997;
Rao et al., 2005)Nc (Rao et al., 2007b) ↑ (Chen et al., 1997;
Rao et al., 2007a)?
GRE Nc (Rao et al., 2005) Nc (Rao et al., 2007b) Nc (Rao et al., 2007a) ?PEA3 Nc (Rao et al., 2005) Nc (Rao et al., 2007b) Nc (Rao et al., 2007a) ?NF-κB Nc (Rao et al., 2005) Nc (Rao et al., 2007b) ↓ (Rao et al., 2007a) ?
Abbreviations: AP, activator protein; GRE, glucocorticoid response element; Nc, no significant change; NF-κB, nuclear factor kappa B; PEA,polyoma enhancer activator; cPLA2, cytosolic phospholipase A2; sPLA2, secretory PLA2; iPLA2, Ca2+-independent PLA2; COX, cyclooxygenase; LOX,lipoxygenase; mPGES, microsomal prostaglandin E synthase.
193B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
2008a), consistent with a reduction in k⁎ for AA (Table 5) (Lee etal., 2007a), whereas chronic topiramate did not significantlychange any measured marker (Ghelardoni et al., 2004, 2005).
6. Mood stabilizers may correct aneurotransmission imbalance involvingarachidonic acid
6.1. Neuroreceptor specificity
The fundamental assumption of neuropsychopharmacology isthat cognition and behavior depend on neurotransmission
involving different neurotransmitters, neurotransmitter trans-porters, neuroreceptors and second messengers (Cooper et al.,2003). Responses of BD patients to drugs other than moodstabilizers that act at specific neuroreceptors have suggestedthat bipolar symptoms arise from excessive dopaminergic andglutamatergic transmission, reduced cholinergic transmission,and disturbed serotonergic transmission (Section 2.1). If thisproposedneurotransmission imbalance involvesAA, thenmoodstabilizers might be effective in BD by correcting the imbalance.This possibility was tested by using quantitative autoradiogra-phy to image regional brain AA signaling in unanesthetized ratsthat had been treated chronically with a clinically relevant doseof mood stabilizer and then acutely administered an agonist to

Table 5 –Mood stabilizers modulate neuroreceptor signaling via arachidonic acid in unanesthetized rats.
Baseline effect Receptor subtype
NMDA D2-like M1,3,5 5-HT2A/C
Agonist used NMDA Quinpirole Arecoline DOIAntagonist used MK-801 Raclopride or butaclamol Atropine Mianserin
Mood stabilizer Effect on response to acute agonist, k⁎ for AA
Lithium ↑ in auditory andvisual areas(Basselin et al., 2005b)
↓ (Basselin et al., 2006a) ↓ (Basselin et al., 2005a) ↑ (Basselin et al., 2003) ↓ in auditory andvisual areas(Basselin et al., 2005b)
Carbamazepine Nc (Basselin et al., 2008b) ↓ (Basselin et al., 2007a) ↓ (Basselin et al., 2008b) ? ?Sodium valproate Nc (Basselin et al., 2008a) ↓ (Basselin et al., 2008a) ? ? ?Lamotrigine ↓ (Lee et al., 2007a) ? ? ? ?
Eachmood stabilizer was administered chronically to produce a plasma concentration therapeutically relevant to bipolar disorder (Table 1), andcompared with chronic vehicle. Baseline effect on k⁎ for AA (AA incorporation) was measured compared to chronic vehicle. Effect on responsesto agonists shown was also measured and compared to response in saline injected animals. In saline-treated animals, responses to agonistscould be blocked by antagonists shown in the table. Nc, no significant change; DOI, (+/−)-1-(2,5-dimethoxy-4-iodophenyl)-2-aminopropanehydrochloride.All but the lamotrigine k⁎ measurements were obtained using quantitative autoradiographic imaging.k⁎ defined by Eq. (1) in Footnote 2.
194 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
relevant cPLA2-coupled neuroreceptors (Table 1), includingcholinergic muscarinic M1,3,5, serotonergic 5-HT2A/2C, dopami-nergic D2-like (D2, D3, D4) and glutamatergic NMDA receptors.
Results of one such study are illustrated in Fig. 4, whichpresents color-coded autoradiographs of coronal brain sec-
Fig. 4 – MK-801 and chronic lithium block NMDA stimulation ofcoefficients k* in autoradiographs of coronal brain sections. Twowith saline or 50 mg/kg NMDA. Two central columns: rats on a ctwo right columns: rats on a LiCl diet injectedwith saline or NMDApretreated with MK-801 or in rats fed the LiCl diet. Fr 8 and 10, fcortex; Acg, anterior cingulate cortex; CPu, caudate putamen; Hi
tions from rats that had been injected i.p. acutely with NMDA(50 mg/kg) or vehicle, after being fed a LiCl-containing orcontrol diet for 6 weeks (Basselin et al., 2006a). NMDA widelyincreased AA incorporation coefficients k⁎ (Footnote 2, Eq. (1))in rats fed the control diet, but not in rats pretreated with the
arachidonic acid signal in the rat brain. AA incorporationleft columns: rats on a control diet, that had been injected i.p.ontrol diet injected with MK-801 or NMDA following MK-801;. NMDA increased k* in rats on the control diet, but not in rats
rontal cortex 8 and 10; Mot, Som, motor and somatosensorypp, hippocampus. From Basselin et al. (2006a).

195B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
NMDA receptor antagonist, MK-801, or fed LiCl. MK-801 itselfreduced k⁎ for AA by 30% on average.
Results from such imaging studies, summarized in Table5, indicate that chronic mood stabilizers could correct theproposed neurotransmission imbalance of BD, if the imbal-ance involved AA as a second messenger. Chronic lithium,carbamazepine and valproate each blocked the k⁎ incre-ments caused by acute NMDA (Basselin et al., 2006a, 2007a,2008b), and chronic lithium and carbamazepine blocked k⁎increments to the D2-like receptor agonist, quinpirole (Basselinet al., 2005a, 2008b). These common actions on D2-like andNMDA receptor signaling may be related to colocalization ofthe receptors in prefrontal cortex, striatum, and nucleusaccumbens (Ikeda et al., 2003; Liu et al., 2006; Tarazi andBaldessarini, 1999; Tseng and O'Donnell, 2004). In addition,chronic lithium blocked responses to the 5-HT2A/2C receptoragonist (+/−)-1-(2,5-dimethoxy-4-iodophenyl)-2-aminopropanehydrochloride (DOI) in auditory and visual rat brain regions(Basselin et al., 2005b). Consistentwith the imbalance hypothesisandwith evidence that lithium reduces the convulsive thresholdto cholinomimetics (Ormandy et al., 1991), chronic lithiumaugmented k⁎ responses to the nonspecific muscarinic agonist,arecoline (Basselin et al., 2003). Whenmeasured, the direction ofthe changes in brain PGE2 and/or TXB2 concentrations followingan agonist corresponded to the direction of the changes in k⁎ forAA.
Neither chronic carbamazepine nor valproate producedconsistent changes in baseline (resting) k⁎ for AA. On theother hand, chronic lithium increased baseline k⁎ in rat auditory
Fig. 5 – Mood stabilizers downregulate the rat brain arachidonic afirst level is the neuroreceptor itself, the second its coupling mecdownregulated by drug action on its transcription factor, AP-2 (lithbe slowed by drug inhibition of an AA-selective acyl-CoA syntheturnover of AA in membrane phospholipids. Drugs also can inhiand/or transcription of COX-2 (and expression of NF-κB) and COXArrows on left denote different levels of drug targeting. Adapted
and visual cortical cortices, inferior and superior colliculi, andgeniculate bodies (Basselin et al., 2003, 2006b) (Table 5), as it didglucosemetabolism in these areas (Basselin et al., 2006c). Theseeffects may be related to lithium's ability to potentiate auditoryand visual evoked responses in humans (Hegerl et al., 1990).Lithium's potentiation of M1,3,5 receptor signaling and suppres-sion of D2-like receptor signaling involving AA in the rat brain(Table 5) may explain the tremors and occasional extrapyrami-dal symptoms that it causes in patients (Ghadirian et al., 1996).
When measured by whole brain analysis rather than withquantitative autoradiography, chronic lamotrigine signifi-cantly decreased k⁎ for AA into brain phospholipids by about15% (Lee et al., 2007a) (Table 5).
6.1.1. Reconciling neurotransmitter-specific effects with globalbrain effectsDownregulation of the global brain AA cascade by the moodstabilizers (Section 5) may largely represent downregulation ofthe cPLA2 activation and AA turnover associated with glutama-tergic (e.g. NMDA) receptor signaling, sincemost brain synapsesare excitatory and glutamatergic (Attwell and Laughlin, 2001;Raichle and Gusnard, 2002). Consistent with this interpretation,the NMDA receptor antagonist MK-801 reduced global AAincorporation by 30% in unanesthetized rats (Fig. 4), whereasacutely administered antagonists to M1,3,5 receptors (atropine),D2-like receptors (butaclamol, raclopride) or 5-HT2A/2C receptors(mianserin) did not markedly decrease baseline AA incorpora-tion into the rat brain (Bhattacharjee et al., 2008; DeGeorge et al.,1991; Hayakawa et al., 2001; Qu et al., 2003).
cid cascade during neurotransmission at different levels. Thehanism with cPLA2. cPLA2 also can be transcriptionallyium and carbamazepine), whereas reincorporation of AA cantase (valproate). These effects are correlated with reducedbit formation of PGE2 and/or TXB2 by downregulating activity-1 respectively. See text and Table 4 for detailed effects.from Rao et al. (2008).

Table 6 – Therapeutic plasma concentrations of anti-depressants, and concentrations used in experimental ratstudies.
Antidepressant Clinical plasmaconcentrations
Plasma concentrationsin rat infusion studies
mg/L
Fluoxetinea 150–500(Wille et al., 2008)
314 (Durand et al., 1999;Lee et al., 2007b)
Imipramineb 45–150(Wille et al., 2008)
100–600 (Daniel et al., 1981;Lee et al., 2007b)
Bupropionc 25–100(Wille et al., 2008)
289 (max) (Lee et al., 2008c;Suckow et al., 1986)
a N-Methyl-g-[4-(trifluoromethyl)phenoxy]benzenepropanamine.b (5-[3-(dimethylamino) propyl]-10,11-dihydro-5H-dibenz [b,f]-azepinemonohydrochloride).c (±)-2-(tert-butylamino)-1-(3-chlorophenyl)propan-1-one.
196 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
6.2. Targeting neuroreceptors and their couplingmachinery
Suppression of the AA cascade bymood stabilizers may occur atmultiple levels: neuroreceptors, their coupling to cPLA2, AAcascade enzyme activities, or gene transcription (Fig. 5). Thus, inaddition to reducing expression of cPLA2 and activity of COX-2,mood stabilizers can directly modify NMDA receptor mechan-isms. Lithium reducedNMDA receptor-mediated Ca2+ influx intocells by inhibiting NR2 phosphorylation (Hashimoto et al., 2003).Sodium valproate inhibited PKA and PKC, which phosphorylatethe NMDA receptor (Du et al., 2004). It also reduced rat brainexpression ofNMDA receptor-interactingproteins, post-synapticdensity protein PSD-95 and type II Ca2+/calmodulin-dependentprotein kinase beta subunit (Bosetti et al., 2005), and inhibitedmicrosomal acyl-CoA synthetase (Acsl) (Bazinet et al., 2005)
Table 7 – Brain arachidonic acid cascade markers following chro
Target Fluoxetine
Fatty acid kineticsArachidonic acid turnoverin brain phospholipid
↑ (Lee et al., 2007b)
EnzymescPLA2 IVA ↑ (Lee et al., 2007b; Rao et al., 2006)sPLA2 IIA Nc (Lee et al., 2007b; Rao et al., 2006)iPLA2 VIA Nc (Lee et al., 2007b; Rao et al., 2006)COX-1 Nc (Lee et al., 2007b)COX-2 Nc (Lee et al., 2007b)
EicosanoidsPGE2 Nc (Lee et al., 2007b)
Transcription factorsAP-2 Nc (Rao et al., 2006)
AP-1 Nc (Rao et al., 2006)GRE Nc (Rao et al., 2006)PEA3 Nc (Frechilla et al., 1998; Rao et al., 2NF-κB Nc (Rao et al., 2006)RNA stabilizing protein ↑ (Rao et al., 2006)
andhistone deacetylase, which can deacetylate histones on thegene for the NMDA receptor transcription factor, specificityprotein-1 (Sp1) (Bai and Kusiak, 1995; Phiel et al., 2001). Sodiumvalproate blocked induction of Fos and binding activity of AP-1DNA, whichmodulates transcription of NMDA receptor subunit,NR2B (QiangandTicku, 2005), and it alteredNMDAreceptor levelsin hippocampal neurons (Caldeira et al., 2007).
With regard to G-protein coupled receptors, chroniclithium reduced brain levels of the Gαi1 and Gαi2 subunits ofthe inhibitory Gα protein that couples D2-like receptors tocPLA2 (Sidhu and Niznik, 2000), and guanosine-5′-tripho-sphate (GTP) binding to these subunits (Wang and Friedman,1999). Chronic carbamazepine reduced D2 receptor density,D2-like receptor coupled Gαo/i, and D2-like receptor phosphor-ylation (Beutler et al., 2005; Montezinho et al., 2006). Chroniclithium and carbamazepine but not valproate increased levelsin the rat brain of GRK3, which is involved in homologousdesensitization of agonist-activated G-protein coupled recep-tors (Ertley et al., 2007). GRK3 but not GRK4 is reduced in thepostmortem BD brain (Rao et al., 2009a).
7. Arachidonic acid cascadeandneuroprotection
Mood stabilizers have been shown to be neuroprotective inanimal and cellularmodels of neurodegeneration, excitotoxicity,stroke–ischemia–hypoxia, stress-inducedneuronal loss,neuroin-flammation, and immunological damage (Section3.3.3) (Changetal., 2009; Chen et al., 1999; Chuang, 2004; Lee et al., 2000). Part ofthis neuroprotection might be due to suppression of anupregulated brain AA cascade, which can cause cell damageandbehavioral changes (Basselin et al., 2007a,b; Bazanet al., 1995;Bosetti, 2007), or to formation of anti-inflammatory DHAmetabolites (Section 5.2.2). Chronic lithium attenuated
nic administration of each of three antidepressants to rats.
Imipramine Bupropion
↑ (Lee et al., 2008c) Nc (Lee et al., 2008c)
↑ (Lee et al., 2008c) Nc (Lee et al., 2008c)Nc (Lee et al., 2008c) Nc (Lee et al., 2008c)Nc (Lee et al., 2008c) Nc (Lee et al., 2008c)Nc (Lee et al., 2008c) Nc (Lee et al., 2008c)Nc (Lee et al., 2008c) Nc (Lee et al., 2008c)
Nc (Lee et al., 2008c) Nc (Lee et al., 2008c)
↑ (AP-2α but not AP-2β)(Lee et al., 2008c)
Nc (Lee et al., 2008c)
↓ (Damberg et al., 2000)Nc (Tamura et al., 2002) ?? ?
006) ? ?Nc (Lee et al., 2008c) Nc (Rao et al., 2007a)? ?

197B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
upregulated AA metabolism in a rat model of neuroinflamma-tion, as did chronic lithium, valproate and carbamazepine in amodel of acute NMDA-induced excitotoxicity (Table 5) (Basselinet al., 2006a, 2007a, 2007b, 2008a). The ability of each of the fourapproved mood stabilizers to increase rat brain expression ofbrain derived neurotrophic factor (BDNF) and of the anti-apoptotic factor, B-cell lymphoma-2 (Bcl-2), which are reducedin the BD brain (Dean et al., 2006), also may contribute to theirneuroprotective action (Chang et al., 2009; Garrido et al., 2003; Raoet al., 2007d). These effects may bemediated by AA (Chang et al.,2009; Rao et al., 2007d).
8. Antidepressants, switching and thearachidonic acid cascade
Certain antidepressants, when given to BD depressed patients,increase the tendency to “switch” to mania (Section 3.1). Thislimits therapy for bipolar depression, perhaps unduly in viewof the controversy concerning “switching.” Increased switchrates are reported for imipramine and fluoxetine, but not forbupropion (Calabrese et al., 1999b; Leverich et al., 2006; Post etal., 2006).
These differences in switch rates correlate with theantidepressant effects on the rat brain AA cascade. Thus,chronic fluoxetine and imipramine, which increase switching,when given to rats to produce a therapeutically relevantplasma concentration (Table 6), increased AA turnover inbrain phospholipids; brain cPLA2 expression (activity, protein,
Table 8 – Rodent models with an upregulated brain arachidonic
Parameter
Chronic i.p.NMDA in rat
6-day cerebroventricularlow-dose lipopolysaccharidea
infusion in rat
AA turnoverb ↑ ↑AA incorporation(k⁎ or Jin)d
↑ ↑
cPLA2 IVA ↑ ↑iPLA2 VIA Nc NcsPLA2 IIA Nc ↑COX-1 NcCOX-2 NcTotal COX5-LOXmPGES-2AP-2 ↑PGE2 ↑TXB2 ↑Altered behavior Yese
References Lee et al. (2008b),Rao et al. (2007e)
Basselin et al. (2007b), Lee et al.(2004), Richardson et al. (2005),Rosenberger et al. (2004)
Empty boxes indicate that measurement was not performed. +/–, heterozya 0.5–1.0 ng/h.b Measured by direct chemical analysis.c Turnover of AA elongation product, 22:5n−6, is increased.d Measured by direct chemical analysis and/or quantitative autoradiograe Measured after 1 month of infusion.
mRNA, and phosphorylation), and expression of the cPLA2
transcription factor subunit, AP-2α (Lee et al., 2007b, 2008c;Rao et al., 2006). Chronic bupropion, which doesn't increaseswitching, did not alter any of these markers (Table 7).
9. Animal models with an upregulatedAA cascade
There is no generally accepted behavioral animal model for BD(Cryan andSlattery, 2007; Kato et al., 2007). Nevertheless, as FDA-approved mood stabilizers have been shown to downregulateparameters of the brain AA cascade in normal rats, animalmodels having a pathologically upregulated brain AA cascademay help in drug discovery and in considering mechanismsrelevant to BD. Table 8 characterizes five such models.
In one rat model, chronic administration of a subconvul-sive dose (25 mg/kg i.p. daily for 21 days) of NMDA increasedbrain markers of excitotoxicity and neuroinflammation(Chang et al., 2008; Rao et al., 2007e), selectively upregulatedAA turnover in brain phospholipid, and elevated expression ofcPLA2 and AP-2. In a second rat model, 6 days of intracer-ebroventricular infusion of low-dose lipopolysaccharide (0.5–1.0 ng/h) (Basselin et al., 2007b; Lee et al., 2004; Rosenberger etal., 2004) increased AA turnover and cPLA2 and sPLA2 activitiesin the brain, whereas behavior was disturbed when measuredafter 1 month of infusion (Richardson et al., 2005). The brainAA cascade also was upregulated by feeding rats an n−3 PUFAdeficient diet for 15 weeks. This dietary regimen decreased
acid cascade.
Model
15 weeks dietaryn−3 PUFA deprivation
in 20 day old rat
COX-2−/−
knockoutmouse
5-HTT+/− or 5-HTT−/−
knockout mouse
↑ c
↑ c ↑ ↑
↑ ↑ ↑↓ Nc↑ ↑↓ ↑↑ Absent
↑ ↓Nc↓
↓ ↓↓
Yes Yes(DeMar et al. (2006b),Igarashi (2009), Rao et al.(2007c)
Basselin et al.(2006c), Bosettiet al. (2004)
Basselin et al. (2009),Murphy and Lesch(2008)
gous; –/–, homoxygous.
phy.

198 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
brain DHA by 30% and increased brain docosapentaenoic acid(DPA, 22:5n−6), an AA elongation product, by an equivalentamount. AA turnover was unaffected, whereas DPA turnoverwas increased (Contreras et al., 2001; Igarashi, 2009; Rao et al.,2007c). BDNF, cAMP response element binding protein (CREB)transcription factor activity, phosphorylated CREB (importantin learning and memory) and p38 mitogen-activated proteinkinase were reduced in the brain (Rao et al., 2007d), and therats showed aggression, depression and increased locomotionon behavioral tests (DeMar et al., 2006b).
Two genetic mouse models also show upregulated AAincorporation into brain phospholipid. The COX-2 knockoutmouse, which lacks the COX-2 gene from birth, also hasincreased cPLA2, sPLA2, and COX-1 expression in the brain.The 5-HTT knockout mouse demonstrates BD-like behavioraldisturbances (Murphy and Lesch, 2008) and increased braincPLA2 activity (Basselin et al., 2009). Regional AA incorporationinto brain is elevated by 20–70% in both heterozygous andhomozygous knockouts (Fig. 6), due to tonic activation of cPLA2-coupled 5-HT2A/2C receptors by elevated synaptic 5-HT concen-trations. The heterozygous 5-HTT+/− mouse is considered amodel for humans having a short (S) compared with long (L)allele of the 5-HTT promoter, who are at increased risk for BDand other psychiatric diseases (Murphy and Lesch, 2008).
10. The arachidonic acid cascade in bipolardisorder patients
A small case-control trial reported increased serum PLA2
activity in BD patients (Noponen et al., 1993). Genetic mapping
Fig. 6 – Coronal autoradiographs of the brain showing effects ofcoefficients k* inmice. First row,wild type; second row, heterozygoauditory cortex; CPu, caudate putamen; Hipp, hippocampus; IPC,nigra; Thal, thalamus; Vis, visual cortex; +/+, wild type; +/–, heteroz
identified involvement of the sPLA2 gene (Jacobsen et al., 1999),but this was not replicated (Meira-Lima et al., 2003), cPLA2 wasnot implicated in other analyses (Dikeos et al., 2006; Pae et al.,2004). One study reported decreased cytosolic PGES in post-mortem frontal and temporal cortices fromBD patients, but notin patients medicated prior to death (Maida et al., 2006).
The postmortem BD compared with control frontal cortexis reported to have increased mRNA and protein levels ofcPLA2, sPLA2 and COX-2 (but not of iPLA2), and increased AP-2and NF-κB levels (Rao et al., 2007b), changes opposite indirection to those produced by mood stabilizers in the ratbrain (Table 4). These changes are accompanied by elevatedexpression of markers of apoptosis, neuroinflammation andexcitotoxicity (Kim et al., unpublished observations; Rao et al.,2009b), and may be caused by or related to these pathologicalprocesses (Chang et al., 2008; Dinarello, 1988; Rao et al., 2007e;Rosenberger et al., 2004) (Section 2.2).
Dietary n−3 PUFA deprivation in rats can upregulate brainAA metabolic markers and disturb AA–DHA interactions(Table 8) (Contreras and Rapoport, 2002; Igarashi, 2009; Raoet al., 2007c). Thus, reports that subjects on a diet low in DHA-containing marine products had an increased prevalence ofBD (Noaghiul and Hibbeln, 2003), that dietary n−3 PUFAsupplementation ameliorated BD symptoms (Frangou et al.,2006; Ross et al., 2007; Stoll et al., 1999), and that the DHAconcentration in the postmortem BD brain was reduced by30% (McNamara et al., 2008; Schwarz et al., 2008), would beconsistent with an association between BD and an upregu-lated or otherwise dysfunctional brain AA cascade. However,other reports have not confirmed a positive effect of dietary n−3 PUFA supplementation or a decreased brain DHA in the
5-HTT genotype on regional arachidonic acid incorporationus; third row, homozygous.Acg, anterior cingulate cortex; Aud,interpeduncular nucleus; Mot, motor cortex; SN, substantiaygous; –/–, homozygous; Adapted from Basselin et al. (2009).

199B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
postmortem brain from BD patients (Igarashi et al., unpub-lished observations; Keck et al., 2006) or suicide victims(Lalovic et al., 2007). The issue is far from settled.
11. Other proposed mechanisms of action ofmood stabilizers
Many brain targets other than the AA cascade have beenproposed for mood stabilizers. These include enzymes inwhich lithium competes for a magnesium binding site (e.g.,inositol monophosphatase, inositol polyphosphate 1-phos-phatase, glycogen synthase kinase-3 (GSK-3), fructose 1,6-bisphosphatase, bisphosphate nucleotidase, phosphogluco-mutase); valproate-inhibitable enzymes (succinate semialde-hyde dehydrogenase, succinate semialdehyde reductase,histone deacetylase); specific targets of carbamazepine(sodium channels, adenosine receptors, adenylate cyclase);signaling pathways involving PKC, cyclic AMP, ormyo-inositol;synaptic mechanisms involving glutamate, GABA, G-proteinsand GRKs (Du et al., 2007; Ertley et al., 2007; Li et al., 2002; Manjiand Lenox, 2000); processes modulating apoptosis and neuro-protection, including the expression of brain growth andneurotrophic factors (Chen et al., 1999; Chuang, 2005; Gould etal., 2004b); and calcium currents and voltage gated sodiumchannels (Farber et al., 2002; Stefani et al., 1996). When givenchronically to rodents, mood stabilizers altered brain mRNAlevels of genes related to ion channel formation and transport,G-protein signaling, lipid, glucose and amino acidmetabolism,transcription and translation, the phosphatidylinositide cycle,protein kinases, phosphatases, and apoptosis (Bosetti et al.,2002b, 2005; Chetcuti et al., 2006; McQuillin et al., 2007).
Among hypotheses regarding the action of mood stabili-zers, the “myo-inositol depletion hypothesis” and the “GSK-3inhibition hypothesis” continue to be explored experimentallyand tested in the clinic (Eden Evins et al., 2006; Rowe et al.,2007). Ultimately, of course, which hypothesis if any is validand could be used for drug discovery in BD will be determinedempirically. Compared to the “AA cascade hypothesis,”however, neither the myo-inositol nor the GSK-3 inhibitionhypothesis identifies one common action of each of the fourFDA-approved mood stabilizers.
The “myo-inositol depletion hypothesis” is that the phos-phatidylinositide cycle, which participates in neurotransmis-sion and is initiated by the activation of phospholipase C, isthe target of lithium (Berridge et al., 1982, 1989; Hokin andDixon, 1993; Lenox and Hahn, 2000). To maintain a normalcycle, the brain must resynthesize myo-inositol, which doesnot readily cross the blood–brain barrier (Barchas et al., 1994).In the cycle, inositol-1,4,5-trisphosphate is serially depho-sphorylated to form myo-inositol, the last dephosphorylationstep being mediated by inositol monophosphatase. Lithium ispostulated to reduce myo-inositol formation within the cycleby inhibiting inositol monophosphatase, thereby interferingwith phospholipase C-mediated neurotransmission events(Berridge et al., 1982, 1989; Hokin and Dixon, 1993; Lenox andHahn, 2000). Limitations to the “myo-inositol depletionhypothesis” have been thoroughly summarized (Atack, 1996).The hypothesis does not appear to apply to carbamazepine orvalproate. While lithium inhibited partially purified inositol
monophosphatase activity in the low millimolar range,carbamazepine stimulated the enzyme starting in the lowmicromolar range, and valproate neither stimulated norinhibited the enzyme over a wide concentration range (Vadnaland Parthasarathy, 1995) (see Table 2).
GSK-3 also is considered a target of mood stabilizers (Gouldand Manji, 2005; Schloesser et al., 2008). GSK-3 modulates theWnt and insulin signaling pathways, as well as neurotrophicsignaling involving phosphoinositide-3 kinase, generallythrough downregulation (Jope, 2003). While data indicate alithium action on GSK-3 at a therapeutically relevant concen-tration, this is not the case for valproate or carbamazepine.Thus, in primary neocortical neurons, GSK-3 was inhibited by1 mM lithium but not by valproate up to a concentration>100mM, or by carbamazepine even at 0.5mM (Di Daniel et al.,2006; Ryves et al., 2005),muchhigher concentrations than theirrespective therapeutic concentrations (Table 2). Nevertheless,chronic sodiumvalproate and lithium, but not carbamazepine,increased rat frontal cortex β-catenin, indirectly suggestingGSK-3 pathway modulating activity (Gould et al., 2004a).
12. Discussion
Following the discovery in 1949 of lithium's efficacy in BD(Cade, 1949), divalproex and carbamazepine were approved bythe FDA for bipolar mania, and lamotrigine was approved fordelaying the appearance of the different mood states. Lithiumand divalproex also are recommended for maintenancetherapy. Atypical antipsychotics are especially useful foracute mania. One, quetiapine, is approved for bipolar depres-sion and maintenance therapy adjunctive to lithium ordivalproex, and aripiprazole and olanzapine are approved formaintenance monotherapy in Bipolar I. Depression is 3 timesmore common than mania in BD, but depression is generallyinadequately treated. Some antidepressants if administeredasmonotherapy or withmood stabilizers increase “switching”to mania.
Multiple risk alleles, each with a small individual contribu-tion, are consistent with a polygenic threshold inheritance ofBD. To date, however, genetic findings have shown poorreplication and have not consistently identified defectivebrain cascades as likely therapeutic targets. A “top down”approach based on identifying a common mechanism ofaction in rat brain of agents that have been shown incontrolled clinical trials to work or not to work in BD hasbeen more informative, and is the focus of this review. Twohypotheses that have been generated by this approach are the“myo-inositol depletion” and “GSK-3 targeting” hypotheses.While each might explain lithium's mechanism of action,neither convincingly accounts for the actions of the othermood stabilizers or, moreover, why some antidepressantsenhance switching from bipolar depression to mania.
The “AA cascade hypothesis,” which is closely consideredin this review, identifies a common target of the four approvedmood stabilizers as the brain AA cascade, and tentativelyexplains why some antidepressants increase switching ofbipolar depression to mania. This hypothesis was derivedlargely from studies in unanesthetized rats chronicallyadministered FDA-approved mood stabilizers, as well as the

200 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
clinically-proven ineffective topiramate for comparison.Lithium, carbamazepine and sodium valproate downregu-lated AA turnover in rat brain phospholipids, without chan-ging DHA or palmitic acid turnover. Lamotrigine reduced AAincorporation coefficients k⁎ in brain phospholipids. The effecton AA turnover of lithium and carbamazepine was ascribed toreduced expression of AA-selective cPLA2 and of its AP-2transcription factor, whereas valproate's effect was ascribedto its inhibition of an AA-selective microsomal acyl-CoAsynthetase. Each of the four agents depressed rat brain COX-2 expression and, when measured, the concentration of theCOX-2-derived AA metabolite, PGE2. Topiramate, which hadbeen proposed as a mood stabilizer based on initial trials, butlater failed Phase III trials, did not alter any brain AA cascademarker. Thus, the AA cascade hypothesis corresponds toproven clinical efficacy of the tested drugs.
The AA cascade hypothesis is consistent with evidencethat BD symptoms arise from excessive dopaminergic andglutamatergic but reduced cholinergic signaling, provided thatthe signaling uses AA as a second messenger. Thus, imagingin unanesthetized rats showed that lithium upregulatedmuscarinic cholinergic M1,3,5 receptor signaling involving AA;lithium and carbamazepine blocked D2-like receptor-initiatedAA signaling; and lithium, valproate and carbamazepine eachblocked NMDA receptor-initiated AA signaling (Table 5). TheNMDA effects may explain much of the global effects of themood stabilizers on the AA cascade, since most brainsynapses are excitatory and glutamatergic (Attwell andLaughlin, 2001; Raichle and Gusnard, 2002).
More research is needed to examine disease progressionand deterioration in BD, which only recently is beingaddressed. Progression may be a trait feature, but it alsomay be determined by factors such as diet, substance abuse,obesity, and bipolar disorder drugs. Postmortem studiesindicate the presence of neuroinflammation, excitotoxicityand apoptosis in the BD brain, processes that can underlieprogression (Kim et al., unpublished observations; Rao et al.,2009b). Chronic administration of atypical antipsychoticshas been shown to cause atrophy and astrocyte loss inmonkey brain, and chronic lithium produced neuronal deathin the rat brain (Section 3.3). On the other hand, moodstabilizers and antipsychotics have been reported to beneuroprotective in animal models of neuroinflammationand excitotoxicity, in some cases by downregulating thebrain AA cascade.
Observations that mood stabilizers selectivity downregu-late the rat brain AA cascade at therapeutically relevantplasma concentrations, and that antidepressants thatincrease switching of bipolar depression to mania upregulatethe cascade, suggest that an upregulated brain AA cascadecontributes to BD symptoms, particularly bipolar mania.Cascade-suppressing drugs, as well as dietary n−3 PUFAsupplementation (Section 10) might be used to test therelation between disturbed behavior and disturbed AAmetabolism in animal models with disturbances of bothbehavior and AA metabolism (Table 8). Additionally, cascadeparameters can be measured in such pathological models, aswell as in the normal rat, to screen for new and potentiallyclinically relevant therapeutic agents for BD. Based on thisreview and prior suggestions (Chang et al., 1996, 1999;
Rapoport and Bosetti, 2002), one would predict efficacy inBD fromNMDA transmissionmodifiers, inhibitors of cPLA2 orof COX-2 (such as non-steroidal anti-inflammatory agentsincluding COX inhibitors and aspirin (which can acetylateCOX-2 to form specific anti-inflammatory derivatives of AAand DHA) (Breitner, 2003; Farooqui et al., 2006; Ketterer et al.,1996; Rapoport and Bosetti, 2002; Serhan, 2006), otherpromoters of brain DHA conversion to resolvins and neuro-protectins (Serhan, 2006) including dietary n−3 PUFA supple-mentation, and inhibitors of AA-selective acyl-CoAsynthetase, including valproate-like compounds (Bazinet etal., 2006b; Bialer and Yagen, 2007). These predictions could betested by direct clinical trials or by analyzing relevantdatabases.
In addition, the presence of an upregulated brain AAcascade in BD patients could be tested for directly by imagingregional brain AA incorporation parameters (k⁎ and Jin)during manic, euthymic and depressive phases of thedisease, with the help of positron emission tomography.Increased AA incorporation associated with neuroinflamma-tion has been measured in this way in patients withAlzheimer disease (Esposito et al., 2007; Esposito et al.,2008; Giovacchini et al., 2004).
Acknowledgments
This work was entirely supported by the Intramural ResearchProgram of the National Institute on Aging, National Institutesof Health. We thank Professor Donald S. Klein and Dr. JakobShimshoni for their helpful comments on this paper.
R E F E R E N C E S
Akiskal, H.S., Maser, J.D., Zeller, P.J., Endicott, J., Coryell, W., Keller,M.,Warshaw, M., Clayton, P., Goodwin, F., 1995. Switching from‘unipolar’ to bipolar II. An 11-year prospective study of clinicaland temperamental predictors in 559 patients. Arch. Gen.Psychiatry 52, 114–123.
Alda, M., 1999. Pharmacogenetics of lithium response in bipolardisorder. J. Psychiatry Neurosci. 24, 154–158.
Atack, J.R., 1996. Inositol monophosphatase, the putativetherapeutic target for lithium. Brain Res. Brain Res. Rev. 22,183–190.
Attwell, D., Laughlin, S.B., 2001. An energy budget for signaling inthe grey matter of the brain. J. Cereb. Blood Flow Metab. 21,1133–1145.
Axelrod, J., 1990. Receptor-mediated activation of phospholipaseA2 and arachidonic acid release in signal transduction.Biochem. Soc. Trans. 18, 503–507.
Bai, G., Kusiak, J.W., 1995. Functional analysis of the proximal5′-flanking region of the N-methyl-D-aspartate receptorsubunit gene, NMDAR1. J. Biol. Chem. 270, 7737–7744.
Balsinde, J., Balboa, M.A., Dennis, E.A., 1998. Functional couplingbetween secretory phospholipase A2 and cyclooxygenase-2and its regulation by cytosolic group IV phospholipase A2. Proc.Natl. Acad. Sci. U. S. A. 95, 7951–7956.
Barchas, J.D., Hamblin, M.W., Malenka, R.C., 1994. Biochemicalhypotheses of mood and anxiety disorders, In: Siegel, G.J.,Agranoff, B.W., Albers, R.W., Molinoff, P.B. (Eds.), BasicNeurochemistry, Fifth Edition. Raven Press, New York,pp. 979–1001. Vol.

201B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
Barrett, T.B., Hauger, R.L., Kennedy, J.L., Sadovnick, A.D., Remick,R.A., Keck, P.E., McElroy, S.L., Alexander, M., Shaw, S.H., Kelsoe,J.R., 2003. Evidence that a single nucleotide polymorphism inthe promoter of the G protein receptor kinase 3 gene isassociated with bipolar disorder. Mol. Psychiatry 8, 546–557.
Basselin, M., Chang, L., Seemann, R., Bell, J.M., Rapoport, S.I., 2003.Chronic lithium administration potentiates brain arachidonicacid signaling at rest and during cholinergic activation inawake rats. J. Neurochem. 85, 1553–1562.
Basselin, M., Chang, L., Bell, J.M., Rapoport, S.I., 2005a. Chroniclithium chloride administration to unanesthetized ratsattenuates brain dopamine D2-like receptor-initiated signalingvia arachidonic acid. Neuropsychopharmacology 30,1064–1075.
Basselin, M., Chang, L., Seemann, R., Bell, J.M., Rapoport, S.I., 2005b.Chronic lithium administration to rats selectively modifies5-HT2A/2C receptor-mediated brain signaling via arachidonicacid. Neuropsychopharmacology 30, 461–472.
Basselin, M., Chang, L., Bell, J.M., Rapoport, S.I., 2006a. Chroniclithium chloride administration attenuates brain NMDAreceptor-initiated signaling via arachidonic acid inunanesthetized rats. Neuropsychopharmacology 31,1659–1674.
Basselin, M., Chang, L., Rapoport, S.I., 2006b. Chronic lithiumchloride administration to rats elevates glucose metabolism inwide areas of brain, while potentiating negative effects onmetabolism of dopamine D(2)-like receptor stimulation.Psychopharmacology (Berl) 187, 303–311.
Basselin, M., Villacreses, N.E., Langenbach, R., Ma, K., Bell, J.M.,Rapoport, S.I., 2006c. Resting and arecoline-stimulatedbrain metabolism and signaling involving arachidonic acidare altered in the cyclooxygenase-2 knockout mouse.J. Neurochem. 96, 669–679.
Basselin, M., Villacreses, N.E., Chen, M., Bell, J.M., Rapoport, S.I.,2007a. Chronic carbamazepine administration reducesN-methyl-D-aspartate receptor-initiated signaling viaarachidonic acid in rat brain. Biol. Psychiatry 62, 934–943.
Basselin, M., Villacreses, N.E., Lee, H.J., Bell, J.M., Rapoport, S.I.,2007b. Chronic lithium administration attenuatesup-regulated brain arachidonic acid metabolism in a ratmodel of neuroinflammation. J. Neurochem. 102, 761–772.
Basselin, M., Villacreses, N.E., Lee, H.J., Bell, J.M., Rapoport, S.I.,2007c. Flurbiprofen, a cyclooxygenase inhibitor, reduces thebrain arachidonic acid signal in response to the cholinergicmuscarinic agonist, arecoline, in awake rats. Neurochem. Res.32, 1857–1867.
Basselin, M., Chang, L., Chen, M., Bell, J.M., Rapoport, S.I., 2008a.Chronic administration of valproic acid reduces brain NMDAsignaling via arachidonic acid in unanesthetized rats.Neurochem. Res. 33, 2229–2240.
Basselin, M., Chang, L., Chen, M., Bell, J.M., Rapoport, S.I., 2008b.Chronic carbamazepine administration attenuates dopamineD2-like receptor-initiated signaling via arachidonic acid in ratbrain. Neurochem. Res. 33, 1373–1383.
Basselin, M., Fox, M.A., Chang, L., Bell, J.M., Greenstein, D., Chen,M., Murphy, D.L., Rapoport, S.I., 2009. Imaging elevated brainarachidonic acid signaling in unanesthetized serotonintransporter (5-HTT)-deficient mice. Neuropsychopharmacology34, 1695–1709.
Baum, A.E., Akula, N., Cabanero, M., Cardona, I., Corona, W.,Klemens, B., Schulze, T.G., Cichon, S., Rietschel, M., Nothen,M.M., Georgi, A., Schumacher, J., Schwarz, M., Abou Jamra, R.,Hofels, S., Propping, P., Satagopan, J., Detera-Wadleigh, S.D.,Hardy, J., McMahon, F.J., 2008. A genome-wide associationstudy implicates diacylglycerol kinase eta (DGKH) and severalother genes in the etiology of bipolar disorder. Mol. Psychiatry13, 197–207.
Bayon, Y., Hernandez, M., Alonso, A., Nunez, L., Garcia-Sancho, J.,Leslie, C., Sanchez Crespo, M., Nieto, M.L., 1997. Cytosolic
phospholipase A2 is coupled to muscarinic receptors in thehuman astrocytoma cell line 1321N1: characterization of thetransducing mechanism. Biochem. J. 323, 281–287.
Bazan, N.G., 2005. Lipid signaling in neural plasticity, brain repair,and neuroprotection. Mol. Neurobiol. 32, 89–103.
Bazan, N.G., 2007. Omega-3 fatty acids, pro-inflammatory signalingand neuroprotection. Curr. Opin. Clin. Nutr. Metab. Care 10,136–141.
Bazan, N.G., Aveldano de Caldironi, M.I., Rodriguez de Turco, E.B.,1981. Rapid release of free arachidonic acid in the centralnervous system due to stimulation. Prog. Lipid Res. 20,523–529.
Bazan, N.G., Rodriguez de Turco, E.B., Allan, G., 1995. Mediators ofinjury in neurotrauma: intracellular signal transduction andgene expression. J. Neurotrauma 12, 791–814.
Bazinet, R.P., Rao, J.S., Chang, L., Rapoport, S.I., Lee, H.J., 2005.Chronic valproate does not alter the kinetics of docosahexaenoicacid within brain phospholipids of the unanesthetized rat.Psychopharmacology (Berl) 182, 180–185.
Bazinet, R.P., Rao, J.S., Chang, L., Rapoport, S.I., Lee, H.J., 2006a.Chronic carbamazepine decreases the incorporation rate andturnover of arachidonic Acid but not docosahexaenoic acid inbrain phospholipids of the unanesthetized rat: relevance tobipolar disorder. Biol. Psychiatry 59, 401–407.
Bazinet, R.P., Weis, M.T., Rapoport, S.I., Rosenberger, T.A., 2006b.Valproic acid selectively inhibits conversion of arachidonicacid to arachidonoyl-CoA by brain microsomal long-chainfatty acyl-CoA synthetases: relevance to bipolar disorder.Psychopharmacology (Berl) 184, 122–129.
Begley, C.E., Annegers, J.F., Swann, A.C., Lewis, C., Coan, S.,Schnapp, W.B., Bryant-Comstock, L., 2001. The lifetime cost ofbipolar disorder in the US: an estimate for new cases in 1998.Pharmacoeconomics 19, 483–495.
Belmaker, R.H., 2004. Bipolar disorder. N. Engl. J. Med. 351, 476–486.Benazzi, F., 2007. Bipolar II disorder: epidemiology, diagnosis and
management. CNS Drugs 21, 727–740.Berger, M., Riemann, D., Hochli, D., Spiegel, R., 1989. The
cholinergic rapid eye movement sleep induction test withRS-86. State or trait marker of depression? Arch. Gen.Psychiatry 46, 421–428.
Berridge, M.J., Downes, C.P., Hanley, M.R., 1982. Lithium amplifiesagonist-dependent phosphatidylinositol responses in brainand salivary glands. Biochem. J. 206, 587–595.
Berridge, M.J., Downes, C.P., Hanley, M.R., 1989. Neural anddevelopmental actions of lithium: a unifying hypothesis. Cell59, 411–419.
Beutler, A.S., Li, S., Nicol, R.,Walsh, M.J., 2005. Carbamazepine is aninhibitor of histone deacetylases. Life Sci. 76, 3107–3115.
Bhana, N., Perry, C.M., 2001. Olanzapine: a review of its use in thetreatment of bipolar I disorder. CNS Drugs 15, 871–904.
Bhattacharjee, A.K., Chang, L., Lee, H.J., Bazinet, R.P., Seemann,R., Rapoport, S.I., 2005. D2 but not D1 dopamine receptorstimulation augments brain signaling involving arachidonicacid in unanesthetized rats. Psychopharmacology (Berl) 180,735–742.
Bhattacharjee, A.K., Chang, L., White, L., Bazinet, R.P., Rapoport,S.I., 2008. Imagingapomorphinestimulationof brainarachidonicacid signaling via D2-like receptors in unanesthetized rats.Psychopharmacology (Berl) 197, 557–566.
Bialer, M., Yagen, B., 2007. Valproic acid: second generation.Neurotherapeutics 4, 130–137.
Bialer, M., Levy, R.H., Perucca, E., 1998. Does carbamazepine have anarrow therapeutic plasma concentration range? Ther. DrugMonit. 20, 56–59.
Bonnier, B., Gorwood, P., Hamon, M., Sarfati, Y., Boni, C.,Hardy-Bayle, M.C., 2002. Association of 5-HT(2A) receptorgene polymorphism with major affective disorders: the caseof a subgroup of bipolar disorder with low suicide risk.Biol. Psychiatry 51, 762–765.

202 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
Bosetti, F., 2007. Arachidonic acid metabolism in brain physiologyand pathology: lessons from genetically alteredmousemodels.J. Neurochem. 102, 577–586.
Bosetti, F., Rintala, J., Seemann, R., Rosenberger, T.A., Con-treras, M.A., Rapoport, S.I., Chang, M.C., 2002a. Chroniclithium downregulates cyclooxygenase-2 activity and pros-taglandin E(2) concentration in rat brain. Mol. Psychiatry 7,845–850.
Bosetti, F., Seemann, R., Bell, J.M., Zahorchak, R., Friedman, E.,Rapoport, S.I., Manickam, P., 2002b. Analysis of gene expressionwith cDNA microarrays in rat brain after 7 and 42 days of orallithium administration. Brain Res. Bull. 57, 205–209.
Bosetti, F., Weerasinghe, G.R., Rosenberger, T.A., Rapoport, S.I.,2003. Valproic acid down-regulates the conversion of arachidonicacid to eicosanoids via cyclooxygenase-1 and -2 in rat brain.J. Neurochem. 85, 690–696.
Bosetti, F., Langenbach, R., Weerasinghe, G.R., 2004. ProstaglandinE2 and microsomal prostaglandin E synthase-2 expression aredecreased in the cyclooxygenase-2-deficient mouse braindespite compensatory induction of cyclooxygenase-1 andCa2+-dependent phospholipase A2. J. Neurochem. 91,1389–1397.
Bosetti, F., Bell, J.M., Manickam, P., 2005. Microarray analysis of ratbrain gene expression after chronic administration of sodiumvalproate. Brain Res. Bull. 65, 331–338.
Bostwick, J.M., Pankratz, V.S., 2000. Affective disorders and suiciderisk: a reexamination. Am. J. Psychiatry 157, 1925–1932.
Bowden, C.L., 1995. Predictors of response to divalproex andlithium. J. Clin. Psychiatry 56 (Suppl. 3), 25–30.
Bowden, C.L., 2003. Acute and maintenance treatment with moodstabilizers. Int. J. Neuropsychopharmacol. 6, 269–275.
Bowden, C.L., Brugger, A.M., Swann, A.C., Calabrese, J.R., Janicak,P.G., Petty, F., Dilsaver, S.C., Davis, J.M., Rush, A.J., Small, J.G.,et al., 1994. Efficacy of divalproex vs lithium and placebo inthe treatment of mania. The Depakote Mania Study Group.JAMA 271, 918–924.
Bowden, C.L., Grunze, H., Mullen, J., Brecher, M., Paulsson, B.,Jones, M., Vagero, M., Svensson, K., 2005a. A randomized,double-blind, placebo-controlled efficacy and safety study ofquetiapine or lithium as monotherapy for mania in bipolardisorder. J. Clin. Psychiatry 66, 111–121.
Bowden, C.L., Ketter, T.A., Sachs, G.S., Thase, M.E., 2005b. Focus onbipolar disorder treatment. J. Clin. Psychiatry 66, 1598–1609.
Breitner, J.C., 2003. NSAIDs and Alzheimer's disease: how far togeneralise from trials? Lancet Neurol. 2, 527.
Bunney, W.E.J., Garland-Bunney, B.L., 1987. Mechanisms of actionof lithium in affective illness: basic and clinical implications.In: Meltzer, H.Y. (Ed.), Psychopharmacology: The ThirdGeneration of Progress. Raven, New York, pp. 553–565. Vol.
Burke, J.E., Dennis, E.A., 2009. Phospholipase A2 structure/function, mechanism, and signaling. J. Lipid Res. 50 Suppl,S237–S242.
Bymaster, F.P., Felder, C.C., 2002. Role of the cholinergicmuscarinicsystem in bipolar disorder and related mechanism of action ofantipsychotic agents. Mol. Psychiatry 7 (Suppl. 1), S57–63.
Cade, J.F., 1949. Lithium salts in the treatment of psychoticexcitement. Med. J. Aust. 2, 349–352.
Calabrese, J.R., Bowden, C.L., Sachs, G.S., Ascher, J.A., Monaghan,E., Rudd, G.D., 1999a. A double-blind placebo-controlled studyof lamotrigine monotherapy in outpatients with bipolar Idepression. Lamictal 602 Study Group. J. Clin. Psychiatry 60,79–88.
Calabrese, J.R., Rapport, D.J., Kimmel, S.E., Shelton, M.D., 1999b.Controlled trials inbipolar I depression: focuson switch ratesandefficacy. Eur. Neuropsychopharmacol. 9 (Suppl. 4), S109–S112.
Caldeira, M.V., Melo, C.V., Pereira, D.B., Carvalho, R.F., Carvalho, A.L., Duarte, C.B., 2007. BDNF regulates the expression and trafficof NMDA receptors in cultured hippocampal neurons. Mol. Cell.Neurosci. 35, 208–219.
Camus, M., Hennere, G., Baron, G., Peytavin, G., Massias, L.,Mentre, F., Farinotti, R., 2003. Comparison of lithiumconcentrations in red blood cells and plasma in samplescollected for TDM, acute toxicity, or acute-on-chronic toxicity.Eur. J. Clin. Pharmacol. 59, 583–587.
Cardno, A.G., Marshall, E.J., Coid, B., Macdonald, A.M., Ribchester,T.R., Davies, N.J., Venturi, P., Jones, L.A., Lewis, S.W., Sham, P.C.,Gottesman, I.I., Farmer, A.E., McGuffin, P., Reveley, A.M.,Murray, R.M., 1999. Heritability estimates for psychoticdisorders: the Maudsley twin psychosis series. Arch. Gen.Psychiatry 56, 162–168.
Chang, M.C., Grange, E., Rabin, O., Bell, J.M., Allen, D.D., Rapoport,S.I., 1996. Lithium decreases turnover of arachidonate inseveral brain phospholipids. Neurosci. Lett. 220, 171–174.
Chang, M.C., Bell, J.M., Purdon, A.D., Chikhale, E.G., Grange, E.,1999. Dynamics of docosahexaenoic acid metabolism in thecentral nervous system: lack of effect of chronic lithiumtreatment. Neurochem. Res. 24, 399–406.
Chang, M.C., Contreras, M.A., Rosenberger, T.A., Rintala, J.J., Bell,J.M., Rapoport, S.I., 2001. Chronic valproate treatmentdecreases the in vivo turnover of arachidonic acid in brainphospholipids: a possible common effect of mood stabilizers.J. Neurochem. 77, 796–803.
Chang, Y.C., Kim, H.W., Rapoport, S.I., Rao, J.S., 2008. ChronicNMDA administration increases neuroinflammatory markersin rat frontal cortex: cross-talk between excitotoxicity andneuroinflammation. Neurochem. Res. 33, 2318–2323.
Chang, Y.C., Rapoport, S.I., Rao, J.S., 2009. Chronic administrationof mood stabilizers upregulates BDNF and bcl-2 expressionlevels in rat frontal cortex. Neurochem. Res. 34, 536–541.
Chen, C., Bazan, N.G., 2005. Lipid signaling: sleep, synapticplasticity, and neuroprotection. Prostaglandins Other LipidMediat. 77, 65–76.
Chen, G., Yuan, P., Hawver, D.B., Potter, W.Z., Manji, H.K., 1997.Increase in AP-1 transcription factor DNA binding activity byvalproic acid. Neuropsychopharmacology 16, 238–245.
Chen, G., Huang, L.D., Jiang, Y.M., Manji, H.K., 1999. Themood-stabilizing agent valproate inhibits the activity ofglycogen synthase kinase-3. J. Neurochem. 72, 1327–1330.
Chetcuti, A., Adams, L.J., Mitchell, P.B., Schofield, P.R., 2006.Altered gene expression in mice treated with the moodstabilizer sodium valproate. Int. J. Neuropsychopharmacol. 9,267–276.
Chuang, D.M., 2004. Neuroprotective and neurotrophic actionsof the mood stabilizer lithium: can it be used to treatneurodegenerative diseases? Crit. Rev. Neurobiol. 16, 83–90.
Chuang, D.M., 2005. The antiapoptotic actions of mood stabilizers:molecular mechanisms and therapeutic potentials. Ann. N.Y.Acad. Sci. 1053, 195–204.
Clark, J.D., Lin, L.L., Kriz, R.W., Ramesha, C.S., Sultzman, L.A., Lin,A.Y., Milona, N., Knopf, J.L., 1991. A novel arachidonicacid-selective cytosolic PLA2 contains a Ca2+-dependenttranslocation domain with homology to PKC and GAP. Cell 65,1043–1051.
Contreras, M.A., Rapoport, S.I., 2002. Recent studies on interactionsbetween n−3 and n−6 polyunsaturated fatty acids in brain andother tissues. Curr. Opin. Lipidol. 13, 267–272.
Contreras, M.A., Chang, M.C., Rosenberger, T.A., Greiner, R.S.,Myers, C.S., Salem Jr., N., Rapoport, S.I., 2001. Chronic nutritionaldeprivation of n−3 alpha-linolenic acid does not affect n−6arachidonic acid recycling within brain phospholipids of awakerats. J. Neurochem. 79, 1090–1099.
Cooper, J.R., Bloom, F.E., Roth, R.H., 2003. The BiochemicalBasis of Neuropharmacology. Oxford University Press,Oxford. Vol.
Coyle, T.R., Kochunov, P., Patel, R.D., Nery, F.G., Lancaster, J.L.,Mangin, J.F., Riviere, D., Pillow, D.R., Davis, G.J., Nicoletti, M.A.,Serap Monkul, E., Fox, P.T., Soares, J.C., 2006. Cortical sulci andbipolar disorder. NeuroReport 17, 1739–1742.

203B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
Craddock, N., Jones, L., Jones, I.R., Kirov, G., Green, E.K., Grozeva, D.,Moskvina, V., Nikolov, I., Hamshere,M.L., Vukcevic, D., Caesar, S.,Gordon-Smith, K., Fraser, C., Russell, E., Norton, N., Breen, G., StClair, D., Collier, D.A., Young, A.H., Ferrier, I.N., Farmer, A.,McGuffin, P., Holmans, P.A., Donnelly, P., Owen, M.J., O'Donovan,M.C., 2008. Strong genetic evidence for a selective influence ofGABA(A) receptors on a component of the bipolar disorderphenotype. Mol. Psychiatry (Electronic Publication).
Crow, T.J., 2007. How and why genetic linkage has not solved theproblem of psychosis: review and hypothesis. Am. J. Psychiatry164, 13–21.
Cryan, J.F., Slattery, D.A., 2007. Animal models of mood disorders:recent developments. Curr. Opin. Psychiatry 20, 1–7.
Damberg, M., Ekblom, J., Oreland, L., 2000. Chronic pharmacologicaltreatment with certain antidepressants alters the expressionand DNA-binding activity of transcription factor AP-2. Life Sci.68, 669–678.
Daniel, W., Adamus, A., Melzacka, M., Szymura, J., Vetulani, J.,1981. Cerebral pharmacokinetics of imipramine in rats aftersingle and multiple dosages. Naunyn-Schmiedebergs Arch.Pharmacol. 317, 209–213.
Davis, K.L., Berger, P.A., Hollister, L.E., Defraites, E., 1978.Physostigmine in mania. Arch. Gen. Psychiatry 35, 119–122.
Dean, B., Gray, L., Scarr, E., 2006. Regionally specific changes inlevels of cortical S100beta in bipolar 1 disorder but notschizophrenia. Aust. N. Z. J. Psychiatry 40, 217–224.
DeGeorge, J.J., Nariai, T., Yamazaki, S., Williams, W.M., Rapoport,S.I., 1991. Arecoline-stimulated brain incorporation ofintravenously administered fatty acids in unanesthetized rats.J. Neurochem. 56, 352–355.
DeLisi, L.E., 2008. The concept of progressive brain change inschizophrenia: implications for understanding schizophrenia.Schizophr. Bull. 34, 312–321.
Demar Jr., J.C., Ma, K., Chang, L., Bell, J.M., Rapoport, S.I., 2005.alpha-Linolenic acid does not contribute appreciably todocosahexaenoic acid within brain phospholipids of adult ratsfed a diet enriched in docosahexaenoic acid. J. Neurochem. 94,1063–1076.
DeMar Jr., J.C., Lee, H.J., Ma, K., Chang, L., Bell, J.M., Rapoport, S.I.,Bazinet, R.P., 2006a. Brain elongation of linoleic acid is anegligible source of the arachidonate in brain phospholipids ofadult rats. Biochim. Biophys. Acta 1761, 1050–1059.
DeMar Jr., J.C., Ma, K., Bell, J.M., Igarashi, M., Greenstein, D.,Rapoport, S.I., 2006b. One generation of n−3 polyunsaturatedfatty acid deprivation increases depression and aggression testscores in rats. J. Lipid Res. 47, 172–180.
Di Daniel, E., Cheng, L., Maycox, P.R., Mudge, A.W., 2006. Thecommon inositol-reversible effect ofmoodstabilizersonneuronsdoes not involve GSK3 inhibition, myo-inositol-1-phosphatesynthase or the sodium-dependent myo-inositol transporters.Mol. Cell. Neurosci. 27–36.
Dikeos, D.G., Papadimitriou, G.N., Souery, D., Del-Favero, J.,Massat, I., Blackwood, D., Cichon, S., Daskalopoulou, E., Ivezic,S., Kaneva, R., Karadima, G., Lorenzi, C., Milanova, V., Muir, W.,Nothen, M., Oruc, L., Rietschel, M., Serretti, A., Van Broeckhoven,C., Soldatos, C.R., Stefanis, C.N., Mendlewicz, J., 2006. Lack ofgenetic association between the phospholipase A2 gene andbipolar mood disorder in a European multicentre case-controlstudy. Psychiatr. Genet. 16, 169–171.
Dinarello, C.A., 1988. Interleukin-1. Ann. N.Y. Acad. Sci. 546,122–132.
Doose, D.R., Streeter, A.J., 2002. Topiramate — chemistry,biotransformation and pharmacokinetics. In: Levy, R.H.,Mattson, R.H., Meldrum, B.S., Perucca, E. (Eds.), Antiepilepticdrugs. Lippincott, Williams and Wilkins, Philadelphia,pp. 727–734. Vol.
Doose, D.R., Brodie, M.J., Wilson, E.A., Chadwick, D., Oxbury, J.,Berry, D.J., Schwabe, S., Bialer, M., 2003. Topiramate andlamotrigine pharmacokinetics during repetitive monotherapy
and combination therapy in epilepsy patients. Epilepsia 44,917–922.
Dorph-Petersen, K.A., Pierri, J.N., Perel, J.M., Sun, Z., Sampson, A.R.,Lewis, D.A., 2005. The influence of chronic exposure toantipsychotic medications on brain size before and after tissuefixation: a comparison of haloperidol and olanzapine inmacaque monkeys. Neuropsychopharmacology 30, 1649–1661.
DSM-IV, 1994. Diagnostic and Statistical Manual of MentalDisorders. American Psychiatric Association, Washington, D.C.Vol.
Du, J., Gray, N.A., Falke, C.A., Chen, W., Yuan, P., Szabo, S.T., Einat,H., Manji, H.K., 2004. Modulation of synaptic plasticity byantimanic agents: the role of AMPA glutamate receptor subunit1 synaptic expression. J. Neurosci. 24, 6578–6589.
Du, J., Suzuki, K., Wei, Y., Wang, Y., Blumenthal, R., Chen, Z., Falke,C., Zarate Jr., C.A., Manji, H.K., 2007. The anticonvulsantslamotrigine, riluzole, and valproate differentially regulateAMPA receptor membrane localization: relationship to clinicaleffects in mood disorders. Neuropsychopharmacology 32,793–802.
Durand, M., Berton, O., Aguerre, S., Edno, L., Combourieu, I.,Mormede, P., Chaouloff, F., 1999. Effects of repeated fluoxetineonanxiety-related behaviours, central serotonergic systems, andthe corticotropic axis in SHR andWKY rats. Neuropharmacology38, 893–907.
Eden Evins, A., Demopulos, C., Yovel, I., Culhane, M., Ogutha, J.,Grandin, L.D., Nierenberg, A.A., Sachs, G.S., 2006. Inositolaugmentation of lithium or valproate for bipolar depression.Bipolar Disord. 8, 168–174.
Eilers, R., 1995. Therapeutic drug monitoring for the treatment ofpsychiatric disorders. Clinical use and cost effectiveness.Clin. Pharmacokinet. 29, 442–450.
Ertley, R.N., Bazinet, R.P., Lee, H.J., Rapoport, S.I., Rao, J.S., 2007.Chronic treatment with mood stabilizers increases membraneGRK3 in rat frontal cortex. Biol. Psychiatry 61, 246–249.
Esposito, G., Giovacchini, G., Der, M., Liow, J.S., Bhattacharjee, A.K.,Ma, K., Herscovitch, P., Channing, M., Eckelman, W.C., Hallett,M., Carson, R.E., Rapoport, S.I., 2007. Imaging signal transductionvia arachidonic acid in the human brain during visualstimulation, by means of positron emission tomography.NeuroImage 34, 1342–1351.
Esposito, G., Giovacchini, G., Liow, J.S., Bhattacharjee, A.K.,Greenstein, D., Schapiro, M., Hallett, M., Herscovitch, P.,Eckelman, W.C., Carson, R.E., Rapoport, S.I., 2008. Imagingneuroinflammation in Alzheimer's disease with radiolabeledarachidonic acid and PET. J. Nucl. Med. 49, 1414–1421.
Evans, D.L., Charney, D.S., Lewis, L., Golden, R.N., Gorman, J.M.,Krishnan, K.R., Nemeroff, C.B., Bremner, J.D., Carney, R.M.,Coyne, J.C., Delong, M.R., Frasure-Smith, N., Glassman, A.H.,Gold, P.W., Grant, I., Gwyther, L., Ironson, G., Johnson, R.L.,Kanner, A.M., Katon, W.J., Kaufmann, P.G., Keefe, F.J., Ketter, T.,Laughren, T.P., Leserman, J., Lyketsos, C.G., McDonald, W.M.,McEwen, B.S., Miller, A.H., Musselman, D., O'Connor, C., Petitto,J.M., Pollock, B.G., Robinson, R.G., Roose, S.P., Rowland, J.,Sheline, Y., Sheps, D.S., Simon, G., Spiegel, D., Stunkard, A.,Sunderland, T., Tibbits Jr., P., Valvo, W.J., 2005. Mood disordersin the medically ill: scientific review and recommendations.Biol. Psychiatry 58, 175–189.
Falconer, D.S., 1967. The inheritance of liability to diseases withvariable age of onset, with particular reference to diabetesmellitus. Ann. Hum. Genet. 31, 1–20.
Farber, N.B., Jiang, X.P., Heinkel, C., Nemmers, B., 2002. Antiepilepticdrugs and agents that inhibit voltage-gated sodium channelsprevent NMDA antagonist neurotoxicity. Mol. Psychiatry 7,726–733.
Farooqui, A.A., Ong, W.Y., Horrocks, L.A., 2006. Inhibitors of brainphospholipase A2 activity: their neuropharmacological effectsand therapeutic importance for the treatment of neurologicdisorders. Pharmacol. Rev. 58, 591–620.

204 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
Farooqui, A.A., Horrocks, L.A., Farooqui, T., 2007. Modulation ofinflammation in brain: a matter of fat. J. Neurochem. 101,577–599.
FDA, 2009. FDA approved drug products. In: http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm, Accessed May 27.
Felder, C.C., Kanterman, R.Y., Ma, A.L., Axelrod, J., 1990. Serotoninstimulates phospholipase A2 and the release of arachidonicacid in hippocampal neurons by a type 2 serotonin receptorthat is independent of inositolphospholipid hydrolysis. Proc.Natl. Acad. Sci. U. S. A. 87, 2187–2191.
Fisher, G., Pelonero, A.L., Ferguson, C., 1991. Mania precipitated byprednisone and bromocriptine. Gen. Hosp. Psychiatry 13,345–346.
Fitzpatrick, F., Soberman, R., 2001. Regulated formation ofeicosanoids. J. Clin. Invest. 107, 1347–1351.
Fountoulakis, K.N., Vieta, E., Sanchez-Moreno, J., Kaprinis, S.G., Goikolea, J.M., Kaprinis, G.S., 2005. Treatment guidelinesfor bipolar disorder: a critical review. J. Affect. Disord. 86,1–10.
Fountoulakis, K.N., Grunze, H., Panagiotidis, P., Kaprinis, G., 2008.Treatment of bipolar depression: an update. J. Affect. Disord.109, 21–34.
Frangou, S., Lewis, M., McCrone, P., 2006. Efficacy of ethyl-eicosapentaenoic acid in bipolar depression: randomiseddouble-blind placebo-controlled study. Br. J. Psychiatry. 188,46–50.
Frechilla, D., Otano, A., Del Rio, J., 1998. Effect of chronicantidepressant treatment on transcription factor bindingactivity in rat hippocampus and frontal cortex. Prog.Neuro-psychopharmacol. Biol. Psychiatry 22, 787–802.
Garrido, R., Springer, J.E., Hennig, B., Toborek, M., 2003. Apoptosisof spinal cord neurons by preventing depletion nicotineattenuates arachidonic acid-induced of neurotrophic factors.J. Neurotrauma 20, 1201–1213.
Gascon, S., Deogracias, R., Sobrado, M., Roda, J.M., Renart, J.,Rodriguez-Pena, A., Diaz-Guerra, M., 2005. Transcription ofthe NR1 subunit of the N-methyl-D-aspartate receptor isdown-regulated by excitotoxic stimulation and cerebralischemia. J. Biol. Chem. 280, 35018–35027.
Gaudreault, S.B., Chabot, C., Gratton, J.P., Poirier, J., 2004.The caveolin scaffolding domain modifies2-amino-3-hydroxy-5-methyl-4-isoxazole propionatereceptor binding properties by inhibiting phospholipase A2
activity. J. Biol. Chem. 279, 356–362.Ghadirian, A.M., Annable, L., Belanger, M.C., Chouinard, G., 1996. A
cross-sectional study of parkinsonism and tardive dyskinesia inlithium-treated affective disordered patients. J. Clin. Psychiatry57, 22–28.
Ghaemi, N., 2001. Bipolar Disorder. http://www.familyaware.org/expertprofiles/drghaemi4.asp#diagnosed.
Ghaemi, S.N., Rosenquist, K.J., Ko, J.Y., Baldassano, C.F., Kontos,N.J., Baldessarini, R.J., 2004. Antidepressant treatment in bipolarversus unipolar depression. Am. J. Psychiatry 161, 163–165.
Ghelardoni, S., Tomita, Y.A., Bell, J.M., Rapoport, S.I., Bosetti, F.,2004. Chronic carbamazepine selectively downregulatescytosolic phospholipase A2 expression and cyclooxygenaseactivity in rat brain. Biol. Psychiatry 56, 248–254.
Ghelardoni, S., Bazinet, R.P., Rapoport, S.I., Bosetti, F., 2005.Topiramate does not alter expression in rat brain of enzymes ofarachidonic acid metabolism. Psychopharmacology (Berl) 180,523–529.
Giovacchini, G., Lerner, A., Toczek, M.T., Fraser, C., Ma, K., DeMar,J.C., Herscovitch, P., Eckelman, W.C., Rapoport, S.I., Carson,R.E., 2004. Brain incorporation of [11C]arachidonic acid, bloodvolume, and blood flow in healthy aging: a study withpartial-volume correction. J. Nucl. Med. 45, 1471–1479.
Goodwin, F.K., Jamison, K.R., 2007. Manic-depressive Illness:Bipolar Disorders and Recurrent Depression. Oxford UniversityPress, New York. Vol.
Gould, T.D., Manji, H.K., 2005. Glycogen synthase kinase-3: aputative molecular target for lithium mimetic drugs.Neuropsychopharmacology 30, 1223–1237.
Gould, T.D., Chen, G., Manji, H.K., 2004a. In vivo evidence in thebrain for lithium inhibition of glycogen synthase kinase-3.Neuropsychopharmacology 29, 32–38.
Gould, T.D., Quiroz, J.A., Singh, J., Zarate, C.A., Manji, H.K., 2004b.Emerging experimental therapeutics for bipolar disorder:insights from the molecular and cellular actions of currentmood stabilizers. Mol. Psychiatry 9, 734–755.
Greenwood, T.A., Schork, N.J., Eskin, E., Kelsoe, J.R., 2006.Identification of additional variants within the humandopamine transporter gene provides further evidence for anassociation with bipolar disorder in two independent samples.Mol. Psychiatry 11, 125–133, 115.
Grof, P., Duffy, A., Cavazzoni, P., Grof, E., Garnham, J., MacDougall,M., O'Donovan, C., Alda, M., 2002. Is response to prophylacticlithium a familial trait? J. Clin. Psychiatry 63, 942–947.
Hashimoto, R., Fujimaki, K., Jeong, M.R., Christ, L., Chuang de, M.,2003. Lithium-induced inhibition of Src tyrosine kinase in ratcerebral cortical neurons: a role in neuroprotection againstN-methyl-D-aspartate receptor-mediated excitotoxicity. FEBSLett. 538, 145–148.
Hassel, B., Tauboll, E., Gjerstad, L., 2001. Chronic lamotriginetreatment increases rat hippocampal GABA shunt activity andelevates cerebral taurine levels. Epilepsy Res. 43, 153–163.
Hayakawa, T., Chang, M.C., Rapoport, S.I., Appel, N.M., 2001.Selective dopamine receptor stimulation differentially affects[3H]arachidonic acid incorporation, a surrogate marker forphospholipase A2-mediated neurotransmitter signaltransduction, in a rodent model of Parkinson's disease.J. Pharmacol. Exp. Ther. 296, 1074–1084.
Hegerl, U., Herrmann, W.M., Ulrich, G., Muller-Oerlinghausen, B.,1990. Effects of lithium on auditory evoked potentials inhealthy subjects. Biol. Psychiatry 27, 555–560.
Hokin, L.E., Dixon, J.F., 1993. The phosphoinositide signaling system.I. Historicalbackground. II. Effects of lithiumon theaccumulationof secondmessenger inositol 1,4,5-trisphosphate in brain cortexslices. Prog. Brain Res. 98, 309–315.
Holman, R.T., 1986. Control of polyunsaturated acids in tissuelipids. J. Am. Coll. Nutr. 5, 183–211.
Horschitz, S., Hummerich, R., Lau, T., Rietschel, M., Schloss, P.,2005. A dopamine transporter mutation associated withbipolar affective disorder causes inhibition of transporter cellsurface expression. Mol. Psychiatry 10, 1104–1109.
Huang, Z.L., Urade, Y., Hayaishi, O., 2007. Prostaglandins andadenosine in the regulation of sleep and wakefulness. Curr.Opin. Pharmacol. 7, 33–38.
Igarashi, M., Ma, K., Chang, L., Bell, J.M., Rapoport, S.I., 2007.Dietary n−3 PUFA deprivation for 15 weeks upregulateselongase and desaturase expression in rat liver but not brain.J. Lipid Res. 48, 2463–2470.
Ikeda, H., Akiyama, G., Fujii, Y., Minowa, R., Koshikawa, N.,Cools, A.R., 2003. Role of AMPA and NMDA receptors in thenucleus accumbens shell in turning behaviour of rats:interaction with dopamine receptors. Neuropharmacology 44,81–87.
Ikemoto, A., Kobayashi, T., Watanabe, S., Okuyama, H., 1997.Membrane fatty acid modifications of PC12 cells byarachidonate or docosahexaenoate affect neurite outgrowthbut not norepinephrine release. Neurochem. Res. 22,671–678.
Jacobsen, F.M., 1993. Low-dose valproate: a new treatment forcyclothymia, mild rapid cycling disorders, and premenstrualsyndrome. J. Clin. Psychiatry 54, 229–234.
Jacobsen, N.J., Franks, E.K., Owen, M.J., Craddock, N.J., 1999.Mutational analysis of phospholipase A2A: a positionalcandidate susceptibility gene for bipolar disorder. Mol.Psychiatry 4, 274–279.

205B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
Janowsky, D.S., Overstreet, D.H., 1995. The role of acetylcholinemechanisms in mood disorders. In: FE, Bloom., Kupfer, DJ(Eds.), Psychopharmacology. The Fourth Generation ofProgress. Raven, New York, pp. 945–956.
Jones, C.R., Arai, T., Bell, J.M., Rapoport, S.I., 1996. Preferential invivo incorporation of [3H]arachidonic acid from blood into ratbrain synaptosomal fractions before and after cholinergicstimulation. J. Neurochem. 67, 822–829.
Jope, R.S., 2003. Lithium and GSK-3: one inhibitor, two inhibitoryactions, multiple outcomes. Trends Pharmacol. Sci. 24,441–443.
Judd, L.L., Hubbard, B., Janowsky, D.S., Huey, L.Y., Attewell, P.A.,1977a. The effect of lithium carbonate on affect, mood, andpersonality of normal subjects. Arch. Gen. Psychiatry 34,346–351.
Judd, L.L., Hubbard, B., Janowsky, D.S., Huey, L.Y., Takahashi, K.I.,1977b. The effect of lithium carbonate on the cognitivefunctions of normal subjects. Arch. Gen. Psychiatry 34,355–357.
Judd, L.L., Akiskal, H.S., Schettler, P.J., Endicott, J., Maser, J.,Solomon, D.A., Leon, A.C., Rice, J.A., Keller, M.B., 2002. Thelong-term natural history of the weekly symptomaticstatus of bipolar I disorder. Arch. Gen. Psychiatry 59,530–537.
Judd, L.L., Akiskal, H.S., 2003. The prevalence and disability ofbipolar spectrum disorders in the US population: re-analysis ofthe ECA database taking into account subthreshold cases.J. Affect. Disord. 73, 123–131.
Kapur, S., Remington, G., 2001. Atypical antipsychotics: newdirectionsandnewchallenges in the treatmentof schizophrenia.Annu. Rev. Med. 52, 503–517.
Kato, T., 2007. Moleculargeneticsofbipolardisorderanddepression.Psychiatry Clin. Neurosci. 61, 3–19.
Kato, T., Kubota, M., Kasahara, T., 2007. Animal models of bipolardisorder. Neurosci. Biobehav. Rev. 31, 832–842.
Kaufmann,W.E., Worley, P.F., Pegg, J., Bremer, M., Isakson, P., 1996.COX-2, a synaptically induced enzyme, is expressed byexcitatory neurons at postsynaptic sites in rat cerebral cortex.Proc. Natl. Acad. Sci. U. S. A. 93, 2317–2321.
Keck Jr., P.E., Mintz, J., McElroy, S.L., Freeman, M.P., Suppes, T.,Frye, M.A., Altshuler, L.L., Kupka, R., Nolen, W.A., Leverich,G.S., Denicoff, K.D., Grunze, H., Duan, N., Post, R.M., 2006.Double-blind, randomized, placebo-controlled trials ofethyl-eicosapentanoate in the treatment of bipolar depressionand rapid cycling bipolar disorder. Biol. Psychiatry 60,1020–1022.
Kessing, L.V., 1999. The effect of the first manic episode inaffective disorder: a case register study of hospitalisedepisodes. J. Affect. Disord. 53, 233–239.
Ketter, T.A., Kimbrell, T.A., George, M.S., Dunn, R.T., Speer, A.M.,Benson, B.E., Willis, M.W., Danielson, A., Frye, M.A., Herscovitch,P., Post, R.M., 2001. Effects of mood and subtype on cerebralglucosemetabolism in treatment-resistant bipolar disorder. Biol.Psychiatry 49, 97–109.
Ketter, T.A., Wang, P.W., Nowakowska, C. (Eds.), 2005. Treatmentof acute mania in bipolar disorder. American PsychiatricPublishing, Washington, DC.
Ketterer, M.W., Brymer, J., Rhoads, K., Kraft, P., Lovallo, W.R., 1996.Is aspirin, as used for antithrombosis, an emotion-modulatingagent? J. Psychosom. Res. 40, 53–58.
Kieseppa, T., Partonen, T., Haukka, J., Kaprio, J., Lonnqvist, J., 2004.High concordance of bipolar I disorder in a nationwide sampleof twins. Am. J. Psychiatry 161, 1814–1821.
Kim, Y.K., Jung, H.G., Myint, A.M., Kim, H., Park, S.H., 2007.Imbalance between pro-inflammatory and anti-inflammatorycytokines in bipolar disorder. J. Affect. Disord. 104, 91–95.
Kleindienst, N., Greil, W., 2000. Differential efficacy of lithium andcarbamazepine in the prophylaxis of bipolar disorder: resultsof the MAP study. Neuropsychobiology 42 (Suppl. 1), 2–10.
Klemfuss, H., 1992. Rhythms and the pharmacology of lithium.Pharmacol. Ther. 56, 53–78.
Konopaske, G.T., Dorph-Petersen, K.A., Sweet, R.A., Pierri, J.N.,Zhang, W., Sampson, A.R., Lewis, D.A., 2008. Effect of chronicantipsychotic exposure on astrocyte and oligodendrocytenumbers in macaque monkeys. Biol. Psychiatry 63, 759–765.
Kushner, S.F., Khan, A., Lane, R., Olson, W.H., 2006. Topiramatemonotherapy in the management of acute mania: results offour double-blind placebo-controlled trials. Bipolar Disord. 8,15–27.
Lalovic, A., Levy, E., Canetti, L., Sequeira, A., Montoudis, A.,Turecki, G., 2007. Fatty acid composition in postmortem brainsof people who completed suicide. J. Psychiatry Neurosci. 32,363–370.
Lasky-Su, J.A., Faraone, S.V., Glatt, S.J., Tsuang, M.T., 2005.Meta-analysis of the association between two polymorphismsin the serotonin transporter gene and affective disorders. Am.J. Med. Genet., B Neuropsychiatr. Genet. 133, 110–115.
Lee, J.M., Grabb, M.C., Zipfel, G.J., Choi, D.W., 2000. Brain tissueresponses to ischemia. J. Clin. Invest. 106, 723–731.
Lee, H., Villacreses, N.E., Rapoport, S.I., Rosenberger, T.A., 2004.In vivo imaging detects a transient increase in brainarachidonic acid metabolism: a potential marker ofneuroinflammation. J. Neurochem. 91, 936–945.
Lee, H.J., Rao, J.S., Chang, L., Rapoport, S.I., Bazinet, R.P., 2007a.Chronic lamotrigine does not alter the turnover of arachidonicacid within brain phospholipids of the unanesthetized rat:implications for the treatment of bipolar disorder.Psychopharmacology (Berl) 193, 467–474.
Lee, H.J., Rao, J.S., Ertley, R.N., Chang, L., Rapoport, S.I., Bazinet,R.P., 2007b. Chronic fluoxetine increases cytosolicphospholipase A(2) activity and arachidonic acid turnover in brainphospholipids of the unanesthetized rat.Psychopharmacology (Berl) 190, 103–115.
Lee, H.J., Ertley, R.N., Rapoport, S.I., Bazinet, R.P., Rao, J.S., 2008a.Chronic administration of lamotrigine downregulates COX-2mRNA and protein in rat frontal cortex. Neurochem. Res. 33,861–866.
Lee, H.J., Rao, J.S., Chang, L., Rapoport, S.I., Bazinet, R.P., 2008b.Chronic N-methyl-D-aspartate administration increases theturnover of arachidonic acid within brain phospholipids of theunanesthetized rat. J. Lipid Res. 49, 162–168.
Lee, H.J., Rao, J.S., Chang, L., Rapoport, S.I., Kim, H.W., 2008c. Chronicimipramine but not bupropion increases arachidonic acidsignaling in rat brain: is this related to ‘switching’ in bipolardisorder?Mol. Psychiatry. (Electronic publication ahead of print).
Lenox, R.H., Hahn, C.G., 2000. Overview of the mechanism of actionof lithium in the brain. J. Clin. Psychiatry 61 (Suppl. 9), 5–15.
Lerer, B., Moore, N., Meyendorff, E., Cho, S.R., Gershon, S., 1987.Carbamazepine versus lithium in mania: a double-blind study.J. Clin. Psychiatry 48, 89–93.
Leverich, G.S., Altshuler, L.L., Frye, M.A., Suppes, T., McElroy, S.L.,Keck Jr., P.E., Kupka, R.W., Denicoff, K.D., Nolen, W.A., Grunze,H., Martinez, M.I., Post, R.M., 2006. Risk of switch in moodpolarity to hypomania or mania in patients with bipolardepression during acute and continuation trials of venlafaxine,sertraline, and bupropion as adjuncts to mood stabilizers. Am.J. Psychiatry 163, 232–239.
Li, X., Ketter, T.A., Frye, M.A., 2002. Synaptic, intracellular, andneuroprotective mechanisms of anticonvulsants: are theyrelevant for the treatment and course of bipolar disorders?J. Affect. Disord. 69, 1–14.
Lieberman, D.Z., Goodwin, F.K., 2004. Use of olanzapine in thetreatment of bipolar I disorder. Expert Rev. Neurotherapeutics4, 759–767.
Lieberman, J.A., Bymaster, F.P., Meltzer, H.Y., Deutch, A.Y.,Duncan, G.E., Marx, C.E., Aprille, J.R., Dwyer, D.S., Li, X.M.,Mahadik, S.P., Duman, R.S., Porter, J.H., Modica-Napolitano, J.S.,Newton, S.S., Csernansky, J.G., 2008. Antipsychotic drugs:

206 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
comparison in animal models of efficacy, neurotransmitterregulation, and neuroprotection. Pharmacol. Rev. 60, 358–403.
Liu, X.Y., Chu, X.P., Mao, L.M., Wang, M., Lan, H.X., Li, M.H., Zhang,G.C., Parelkar, N., Fibuch, E., Haines, M., Neve, K., Liu, F., Xiong,Z., Wang, J., 2006. Modulation of D2R-NR2B interactions inresponse to cocaine. Neuron 52, 897–909.
Lu, X.H., Bradley, R.J., Dwyer, D.S., 2004. Olanzapine producestrophic effects in vitro and stimulates phosphorylation ofAkt/PKB, ERK1/2, and the mitogen-activated protein kinasep38. Brain Res. 1011, 58–68.
Luschen, S., Adam, D., Ussat, S., Kreder, D., Schneider-Brachert,W., Kronke, M., Adam-Klages, S., 2000. Activation of ERK1/2 andcPLA(2) by the p55 TNF receptor occurs independently of FAN.Biochem. Biophys. Res. Commun. 274, 506–512.
Lyoo, I.K., Sung, Y.H., Dager, S.R., Friedman, S.D., Lee, J.Y., Kim, S.J.,Kim, N., Dunner, D.L., Renshaw, P.F., 2006. Regional cerebralcortical thinning in bipolar disorder. Bipolar Disord. 8, 65–74.
Maida, M.E., Hurley, S.D., Daeschner, J.A., Moore, A.H., KerryO'banion, M., 2006. Cytosolic prostaglandin E(2) synthase(cPGES) expression is decreased in discrete cortical regions inpsychiatric disease. Brain Res. 1103, 169–172.
Manji, H.K., Lenox, R.H., 2000. Signaling: cellular insights into thepathophysiology of bipolar disorder. Biol. Psychiatry 48,518–530.
Martins, M.R., Petronilho, F.C., Gomes, K.M., Dal-Pizzol, F., Streck,E.L., Quevedo, J., 2008. Antipsychotic-induced oxidative stressin rat brain. Neurotox. Res. 13, 63–69.
Martucci, L., Wong, A.H., De Luca, V., Likhodi, O., Wong, G.W.,King, N., Kennedy, J.L., 2006. N-methyl-D-aspartate receptorNR2B subunit gene GRIN2B in schizophrenia and bipolardisorder: polymorphisms and mRNA levels. Schizophr. Res.84, 214–221.
Massat, I., Souery, D., Del-Favero, J., Van Gestel, S., Serretti, A.,Macciardi, F., Smeraldi, E., Kaneva, R., Adolfsson, R., Nylander,P.O., Blackwood, D., Muir, W., Papadimitriou, G.N., Dikeos, D.,Oruc, L., Segman, R.H., Ivezic, S., Aschauer, H., Ackenheil, M.,Fuchshuber, S., Dam, H., Jakovljevic, M., Peltonen, L., Hilger, C.,Hentges, F., Staner, L., Milanova, V., Jazin, E., Lerer, B., VanBroeckhoven, C., Mendlewicz, J., 2002. Positive association ofdopamine D2 receptor polymorphism with bipolar affectivedisorder in a European Multicenter Association Study ofaffective disorders. Am. J. Med. Genet. 114, 177–185.
Matsuzawa, A., Murakami, M., Atsumi, G., Imai, K., Prados, P.,Inoue, K., Kudo, I., 1996. Release of secretory phospholipaseA2 from rat neuronal cells and its possible function in theregulation of catecholamine secretion. Biochem. J. 318 (Pt. 2),701–709.
McDonald, C., Marshall, N., Sham, P.C., Bullmore, E.T., Schulze, K.,Chapple, B., Bramon, E., Filbey, F., Quraishi, S., Walshe, M.,Murray, R.M., 2006. Regional brain morphometry in patientswith schizophrenia or bipolar disorder and their unaffectedrelatives. Am. J. Psychiatry 163, 478–487.
McGahon, B., Clements, M.P., Lynch, M.A., 1997. The ability of agedrats to sustain long-term potentiation is restored whenthe age-related decrease in membrane arachidonic acidconcentration is reversed. Neuroscience 81, 9–16.
McGuffin, P., Rijsdijk, F., Andrew, M., Sham, P., Katz, R., Cardno, A.,2003. The heritability of bipolar affective disorder and thegenetic relationship to unipolar depression. Arch. Gen.Psychiatry 60, 497–502.
McNamara, R.K., Jandacek, R., Rider, T., Tso, P., Stanford, K.E.,Hahn, C.G., Richtand, N.M., 2008. Deficits in docosahexaenoicacid and associated elevations in themetabolism of arachidonicacid and saturated fatty acids in the postmortem orbitofrontalcortex of patients with bipolar disorder. Psychiatry Res. 160,285–299.
McQuillin, A., Rizig, M., Gurling, H.M., 2007. A microarray geneexpression study of the molecular pharmacology of lithiumcarbonate on mouse brain mRNA to understand the
neurobiology of mood stabilization and treatment of bipolaraffective disorder. Pharmacogenet. Genomics 17, 605–617.
Meira-Lima, I., Jardim, D., Junqueira, R., Ikenaga, E., Vallada, H.,2003. Allelic association study between phospholipase A2
genes and bipolar affective disorder. Bipolar Disord. 5, 295–299.Michael, N., Erfurth, A., Ohrmann, P., Gossling, M., Arolt, V.,
Heindel, W., Pfleiderer, B., 2003. Acute mania is accompaniedby elevated glutamate/glutamine levels within the leftdorsolateral prefrontal cortex. Psychopharmacology (Berl) 168,344–346.
Montezinho, L.P., Castro, M.M., Duarte, C.B., Penschuck, S.,Geraldes, C.F., Mork, A., 2006. The interaction betweendopamine D2-like and beta-adrenergic receptors in theprefrontal cortex is altered by mood-stabilizing agents.J. Neurochem. 96, 1336–1348.
Murphy, D.L., Lesch, K.P., 2008. Targeting the murine serotonintransporter: insights into human neurobiology. Nat. Rev.Neurosci. 9, 85–96.
Narrow, W.E., Rae, D.S., Robins, L.N., Regier, D.A., 2002. Revisedprevalence estimates of mental disorders in the United States:using a clinical significance criterion to reconcile 2 surveys'estimates. Arch. Gen. Psychiatry 59, 115–123.
Nesvag, R., Lawyer, G., Varnas, K., Fjell, A.M., Walhovd, K.B.,Frigessi, A., Jonsson, E.G., Agartz, I., 2008. Regional thinning ofthe cerebral cortex in schizophrenia: effects of diagnosis, ageand antipsychotic medication. Schizophr. Res. 98, 16–28.
Nitsch, R.M., Deng, A., Wurtman, R.J., Growdon, J.H., 1997.Metabotropic glutamate receptor subtype mGluR1αstimulates the secretion of the amyloid beta-protein precursorectodomain. J. Neurochem. 69, 704–712.
Noaghiul, S., Hibbeln, J.R., 2003. Cross-national comparisons ofseafood consumption and rates of bipolar disorders. Am. J.Psychiatry 160, 2222–2227.
Noponen, M., Sanfilipo, M., Samanich, K., Ryer, H., Ko, G., Angrist,B., Wolkin, A., Duncan, E., Rotrosen, J., 1993. Elevated PLA2
activity in schizophrenics and other psychiatric patients. Biol.Psychiatry 34, 641–649.
Nowatzke, W., Ramanadham, S., Ma, Z., Hsu, F.F., Bohrer, A., Turk,J., 1998. Mass spectrometric evidence that agents that causeloss of Ca2+ from intracellular compartments inducehydrolysis of arachidonic acid from pancreatic islet membranephospholipids by a mechanism that does not require a rise incytosolic Ca2+ concentration. Endocrinology 139, 4073–4085.
Ong, W.Y., Sandhya, T.L., Horrocks, L.A., Farooqui, A.A., 1999.Distribution of cytoplasmic phospholipase A2 in the normal ratbrain. J. Hirnforsch. 39, 391–400.
Ong, W.Y., Yeo, J.F., Ling, S.F., Farooqui, A.A., 2005. Distribution ofcalcium-independent phospholipase A2 (iPLA2) in monkeybrain. J. Neurocytol. 34, 447–458.
Ormandy, G.C., Song, L., Jope, R.S., 1991. Analysis of theconvulsant-potentiating effects of lithium in rats. Exp. Neurol.111, 356–361.
Osuji, I.J., Cullum, C.M., 2005. Cognition in bipolar disorder.Psychiatr. Clin. North Am. 28, 427–441.
Ozaki, N., Chuang, D.-M., 1997. Lithium increases transcriptionfactor binding to AP-1 and cyclic AMP-responsive element incultured neurons and rat brain. J. Neurochem. 69, 2336–2344.
Pae, C.U., Yu, H.S., Kim, J.J., Lee, C.U., Lee, S.J., Lee, K.U., Jun, T.Y.,Paik, I.H., Serretti, A., Lee, C., 2004. BanI polymorphism of thecytosolic phospholipase A2 gene and mood disorders in theKorean population. Neuropsychobiology 49, 185–188.
Pavoine, C., Magne, S., Sauvadet, A., Pecker, F., 1999. Evidence for abeta2-adrenergic/arachidonic acid pathway in ventricular car-diomyocytes. Regulation by the beta1-adrenergic/camp path-way. J. Biol. Chem. 274, 628–637.
Peet, M., Peters, S., 1995. Drug-induced mania. Drug Safety 12,146–153.
Phiel, C.J., Zhang, F., Huang, E.Y., Guenther, M.G., Lazar, M.A.,Klein, P.S., 2001. Histone deacetylase is a direct target of

207B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
valproic acid, a potent anticonvulsant, mood stabilizer, andteratogen. J. Biol. Chem. 276, 36734–36741.
Piomelli, D., 1995. Arachidonic acid. In: Bloom, F.E., Kupfer, D.E.(Eds.), Psychopharmacology: The Fourth Generation ofProgress. Raven, New York, pp. 595–607. Vol.
Post, R.M., 1990. Sensitization and kindling perspectives for thecourse of affective illness: toward a new treatment with theanticonvulsant carbamazepine. Pharmacopsychiatry 23, 3–17.
Post, R.M., Calabrese, J.R., 2004. Bipolar depression: the role ofatypical antipsychotics. Expert Rev. Neurotherapeutics 4,S27–S33.
Post, R.M., Jimerson, D.C., Bunney Jr., W.E., Goodwin, F.K., 1980.Dopamine and mania: behavioral and biochemical effects ofthe dopamine receptor blocker pimozide. Psychopharmacology(Berl) 67, 297–305.
Post, R.M., Ketter, T.A., Pazzaglia, P.J., Denicoff, K., George, M.S.,Callahan, A., Leverich, G., Frye, M., 1996. Rational polypharmacyin the bipolar affective disorders. Epilepsy Res. (Suppl. 11),153–180.
Post, R.M., Altshuler, L.L., Leverich, G.S., Frye, M.A., Nolen, W.A.,Kupka, R.W., Suppes, T., McElroy, S., Keck, P.E., Denicoff, K.D.,Grunze, H., Walden, J., Kitchen, C.M., Mintz, J., 2006. Moodswitch in bipolar depression: comparison of adjunctivevenlafaxine, bupropion and sertraline. Br. J. Psychiatry 189,124–131.
Prado, G.N., Taylor, L., Zhou, X., Ricupero, D., Mierke, D.F., Polgar, P.,2002. Mechanisms regulating the expression, self-maintenance,and signaling-function of the bradykinin B2 and B1 receptors.J. Cell. Physiol. 193, 275–286.
Purdon, A.D., Rapoport, S.I., 1998. Energy requirements for twoaspects of phospholipid metabolism in mammalian brain.Biochem. J. 335 (Pt. 2), 313–318.
Qiang, M., Ticku, M.K., 2005. Role of AP-1 in ethanol-inducedN-methyl-D-aspartate receptor 2B subunit gene up-regulationin mouse cortical neurons. J. Neurochem. 95, 1332–1341.
Qu, Y., Chang, L., Klaff, J., Balbo, A., Rapoport, S.I., 2003. ImagingbrainphospholipaseA2activation inawake rat in response to5-HT2A/2C
agonist, (+/−)-2,5-dimethoxy-4-iodophenyl-2-aminopropane(DOI). Neuropsychopharmacology 28, 244–252.
Rabin, O., Chang, M.C., Grange, E., Bell, J., Rapoport, S.I., Deutsch, J.,Purdon, A.D., 1998. Selective acceleration of arachidonic acidreincorporation into brain membrane phospholipid followingtransient ischemia in awake gerbil. J. Neurochem. 70, 325–334.
Raichle, M.E., Gusnard, D.A., 2002. Appraising the brain's energybudget. Proc. Natl. Acad. Sci. U. S. A. 99, 10237–10239.
Rao, J.S., Rapoport, S.I., Bosetti, F., 2005. Decrease in the AP-2DNA-binding activity and in the protein expression of AP-2alpha and AP-2 beta in frontal cortex of rats treated withlithium for 6 weeks. Neuropsychopharmacology 30,2006–2013.
Rao, J.S., Ertley, R.N., Lee, H.J., Rapoport, S.I., Bazinet, R.P., 2006.Chronic fluoxetine upregulates activity, protein and mRNAlevels of cytosolic phospholipase A2 in rat frontal cortex.Pharmacogenomics J. 6, 413–420.
Rao, J.S., Bazinet, R.P., Rapoport, S.I., Lee, H.J., 2007a. Chronictreatment of rats with sodium valproate downregulates frontalcortex NF-kappaB DNA binding activity and COX-2 mRNA.Bipolar Disord. 9, 513–520.
Rao, J.S., Bazinet, R.P., Rapoport, S.I., Lee, H.J., 2007b. Chronicadministration of carbamazepine down-regulates AP-2DNA-binding activity and AP-2α protein expression in ratfrontal cortex. Biol. Psychiatry 61, 154–161.
Rao, J.S., Ertley, R.N., DeMar Jr., J.C., Rapoport, S.I., Bazinet,R.P., Lee, H.J., 2007c. Dietary n−3 PUFA deprivation altersexpression of enzymes of the arachidonic anddocosahexaenoic acid cascades in rat frontal cortex. Mol.Psychiatry 12, 151–157.
Rao, J.S., Ertley, R.N., Lee, H.J., DeMar Jr., J.C., Arnold, J.T.,Rapoport, S.I., Bazinet, R.P., 2007d. n−3 polyunsaturated
fatty acid deprivation in rats decreases frontal cortex BDNFvia a p38 MAPK-dependent mechanism. Mol. Psychiatry 12,36–46.
Rao, J.S., Ertley, R.N., Rapoport, S.I., Bazinet, R.P., Lee, H.J., 2007e.Chronic NMDA administration to rats up-regulates frontalcortex cytosolic phospholipase A2 and its transcription factor,activator protein-2. J. Neurochem. 102, 1918–1927.
Rao, J.S., Lee, H.J., Rapoport, S.I., Bazinet, R.P., 2008. Mode of actionof mood stabilizers: is the arachidonic acid cascade a commontarget? Mol. Psychiatry 13, 585–596.
Rao, J.S., Rapoport, S.I., Kim, H.W., 2009a. Decreased GRK3 but notGRK2 expression in frontal cortex from bipolar disorderpatients. Int. J. Neuropsychopharmacol. 12, 851–860.
Rao, J.S., Rapoport, S.I., Kim, H.W., 2009b. Increased excitotoxicityand neuroinflammatory markers in postmortem frontal cortexfrom bipolar disorder patients. Mol Psychiatry. (Electronicpublication ahead of print).
Rapoport, S.I., 2001. In vivo fatty acid incorporation into brainphospholipids in relation to plasma availability, signaltransduction and membrane remodeling. J. Mol. Neurosci. 16,243–261.
Rapoport, S.I., 2003. In vivo approaches to quantifying and imagingbrain arachidonic and docosahexaenoic acid metabolism.J. Pediatr. 143, S26–S34.
Rapoport, S.I., Bosetti, F., 2002. Do lithium and anticonvulsantstarget the brain arachidonic acid cascade in bipolar disorder?Arch. Gen. Psychiatry 59, 592–596.
Rapoport, S.I., Chang, M.C.J., Spector, A.A., 2001. Delivery andturnover of plasma-derived essential PUFAs in mammalianbrain. J. Lipid Res. 42, 678–685.
Rapoport, S.I., Rao, J.S., Igarashi, M., 2007. Brain metabolism ofnutritionally essential polyunsaturated fatty acids depends onboth the diet and the liver. Prostaglandins Leukot. Essent. Fat.Acids 77, 251–261.
Richardson, R.L., Kim, E.M., Gardiner, T., O'Hare, E., 2005. Chronicintracerebroventricular infusion of lipopolysaccharide: effectsof ibuprofen treatment and behavioural and histopathologicalcorrelates. Behav. Pharmacol. 16, 531–541.
Rintala, J., Seemann, R., Chandrasekaran, K., Rosenberger, T.A.,Chang, L., Contreras, M.A., Rapoport, S.I., Chang, M.C., 1999.85 kDa cytosolic phospholipase A2 is a target for chroniclithium in rat brain. NeuroReport 10, 3887–3890.
Robinson, P.J., Noronha, J., DeGeorge, J.J., Freed, L.M., Nariai, T.,Rapoport, S.I., 1992. A quantitative method for measuringregional in vivo fatty-acid incorporation into and turnoverwithin brain phospholipids: review and critical analysis. BrainRes. Brain Res. Rev. 17, 187–214.
Rosa,A.O., Rapoport, S.I., 2009. Intracellular- andextracellular-derivedCa2+ influence phospholipase A(2)-mediated fatty acid releasefrom brain phospholipids. Biochim. Biophys. Acta (Electronicpublication ahead of print).
Rosenberger, T.A., Villacreses, N.E., Hovda, J.T., Bosetti, F.,Weerasinghe, G., Wine, R.N., Harry, G.J., Rapoport, S.I., 2004. Ratbrain arachidonic acid metabolism is increased by a 6-dayintracerebral ventricular infusionof bacterial lipopolysaccharide.J. Neurochem. 88, 1168–1178.
Ross, B.M., Seguin, J., Sieswerda, L.E., 2007. Omega-3 fatty acids astreatments for mental illness: which disorder and which fattyacid? Lipids Health Dis. 6, 21.
Rowe, M.K., Wiest, C., Chuang, D.M., 2007. GSK-3 is a viablepotential target for therapeutic intervention in bipolardisorder. Neurosci. Biobehav. Rev. 31, 920–931.
Ryves, W.J., Dalton, E.C., Harwood, A.J., Williams, R.S., 2005.GSK-3 activity in neocortical cells is inhibited by lithiumbut not carbamazepine or valproic acid. Bipolar Disord. 7,260–265.
Sachs, G.S., 1996. Bipolarmooddisorder: practical strategies for acuteandmaintenance phase treatment. J. Clin. Psychopharmacol. 16,32S–47S.

208 B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
Sachs, G.S., Koslow, C.L., Ghaemi, S.N., 2000. The treatment ofbipolar depression. Bipolar Disord. 2, 256–260.
Sachs, G.S., Nierenberg, A.A., Calabrese, J.R., Marangell, L.B.,Wisniewski, S.R., Gyulai, L., Friedman, E.S., Bowden, C.L.,Fossey, M.D., Ostacher, M.J., Ketter, T.A., Patel, J., Hauser, P.,Rapport, D., Martinez, J.M., Allen, M.H., Miklowitz, D.J., Otto,M.W., Dennehy, E.B., Thase, M.E., 2007. Effectiveness ofadjunctive antidepressant treatment for bipolar depression.N. Engl. J. Med. 356, 1711–1722.
Schloesser, R.J., Huang, J., Klein, P.S., Manji, H.K., 2008. Cellularplasticity cascades in the pathophysiology and treatmentof bipolar disorder. Neuropsychopharmacology 33,110–133.
Schumacher, J., Kaneva, R., Jamra, R.A., Diaz, G.O., Ohlraun, S.,Milanova, V., Lee, Y.A., Rivas, F., Mayoral, F., Fuerst, R., Flaquer,A., Windemuth, C., Gay, E., Sanz, S., Gonzalez, M.J., Gil, S.,Cabaleiro, F., del Rio, F., Perez, F., Haro, J., Kostov, C., Chorbov,V., Nikolova-Hill, A., Stoyanova, V., Onchev, G., Kremensky, I.,Strauch, K., Schulze, T.G., Nurnberg, P., Gaebel, W., Klimke, A.,Auburger, G., Wienker, T.F., Kalaydjieva, L., Propping, P.,Cichon, S., Jablensky, A., Rietschel, M., Nothen, M.M., 2005.Genomewide scan and fine-mapping linkage studies in fourEuropean samples with bipolar affective disorder suggest anew susceptibility locus on chromosome 1p35–p36 andprovides further evidence of loci on chromosome 4q31 and6q24. Am. J. Hum. Genet. 77, 1102–1111.
Schwarz, E., Prabakaran, S., Whitfield, P., Major, H., Leweke, F.M.,Koethe, D., McKenna, P., Bahn, S., 2008. High throughputlipidomic profiling of schizophrenia and bipolar disorder braintissue reveals alterations of free fatty acids, phosphatidylcholines,and ceramides. J. Proteome Res. 7, 4266–4277.
Sellmayer, A., Danesch, U., Weber, P.C., 1997. Modulation of theexpression of early genes by polyunsaturated fatty acids.Prostaglandins Leukot. Essent. Fat. Acids 57, 353–357.
Serhan, C.N., 2006. Novel chemical mediators in the resolution ofinflammation: resolvins and protectins. Anesthesiol. Clin. 24,341–364.
Shimizu, T., Wolfe, L.S., 1990. Arachidonic acid cascade and signaltransduction. J. Neurochem. 55, 1–15.
Sidhu, A., Niznik, H.B., 2000. Coupling of dopamine receptorsubtypes to multiple and diverse G proteins. Int. J. Dev.Neurosci. 18, 669–677.
Simpson, G.M., 2005. Atypical antipsychotics and the burden ofdisease. Am. J. Manag. Care 11, S235–S241.
Sklar, P., Smoller, J.W., Fan, J., Ferreira, M.A., Perlis, R.H., Chambert,K., Nimgaonkar, V.L., McQueen, M.B., Faraone, S.V., Kirby, A.,de Bakker, P.I., Ogdie, M.N., Thase, M.E., Sachs, G.S.,Todd-Brown, K., Gabriel, S.B., Sougnez, C., Gates, C.,Blumenstiel, B., Defelice, M., Ardlie, K.G., Franklin, J., Muir, W.J.,McGhee, K.A., Macintyre, D.J., McLean, A., Vanbeck, M.,McQuillin, A., Bass, N.J., Robinson, M., Lawrence, J., Anjorin, A.,Curtis, D., Scolnick, E.M., Daly, M.J., Blackwood, D.H., Gurling,H.M., Purcell, S.M., 2008. Whole-genome association study ofbipolar disorder. Mol. Psychiatry 3, 558–569.
Sobo, S., 1999. Mood stabilizers and mood swings: in search of adefinition. Psychiatric Times 16.
Stefani, A., Spadoni, F., Siniscalchi, A., Bernardi, G., 1996.Lamotrigine inhibits Ca2+ currents in cortical neurons:functional implications. Eur. J. Pharmacol. 307, 113–116.
Stefanovic, B., Bosetti, F., Silva, A.C., 2006. Modulatory role ofcyclooxygenase-2 in cerebrovascular coupling. NeuroImage 32,23–32.
Stoll, A.L., Severus, W.E., Freeman, M.P., Rueter, S., Zboyan, H.A.,Diamond, E., Cress, K.K., Marangell, L.B., 1999. Omega 3 fattyacids in bipolar disorder: a preliminary double-blind,placebo-controlled trial. Arch. Gen. Psychiatry 56, 407–412.
Strakowski, S.M., DelBello, M.P., Zimmerman, M.E., Getz, G.E.,Mills, N.P., Ret, J., Shear, P., Adler, C.M., 2002. Ventricularand periventricular structural volumes in first- versus
multiple-episode bipolar disorder. Am. J. Psychiatry 159,1841–1847.
Strokin, M., Sergeeva, M., Reiser, G., 2003. Docosahexaenoic acidand arachidonic acid release in rat brain astrocytes is mediatedby two separate isoforms of phospholipase A2 and is differentlyregulated by cyclic AMP and Ca2+. Br. J. Pharmacol. 139,1014–1022.
Suckow, R.F., Smith, T.M., Perumal, A.S., Cooper, T.B., 1986.Pharmacokinetics of bupropion andmetabolites in plasma andbrain of rats, mice, and guinea pigs. Drug Metab. Dispos. 14,692–697.
Sultzer, D.L., Cummings, J.L., 1989. Drug-induced mania—causativeagents, clinical characteristics andmanagement. A retrospectiveanalysis of the literature. Med. Toxicol. Adverse Drug Exp. 4,127–143.
Sun, G.Y., MacQuarrie, R.A., 1989. Deacylation–reacylation ofarachidonoyl groups in cerebral phospholipids. Ann. N.Y.Acad. Sci. 559, 37–55.
Sun, G.Y., Xu, J., Jensen, M.D., Yu, S., Wood, W.G., Gonzalez, F.A.,Simonyi, A., Sun, A.Y., Weisman, G.A., 2005. PhospholipaseA2 in astrocytes: responses to oxidative stress, inflammation,and G protein-coupled receptor agonists. Mol. Neurobiol. 31,27–41.
Swann, A.C., Bowden, C.L., Morris, D., Calabrese, J.R., Petty, F.,Small, J., Dilsaver, S.C., Davis, J.M., 1997. Depression duringmania. Treatment response to lithium or divalproex. Arch.Gen. Psychiatry 54, 37–42.
Takano, T., Panesar, M., Papillon, J., Cybulsky, A.V., 2000.Cyclooxygenases-1 and 2 couple to cytosolic but not group IIAphospholipase A2 in COS-1 cells. Prostaglandins Other LipidMediat. 60, 15–26.
Tamura, T., Morinobu, S., Okamoto, Y., Kagaya, A., Yamawaki, S.,2002. The effects of antidepressant drug treatments onactivator protein-1 binding activity in the rat brain. Prog.Neuro-psychopharmacol. Biol. Psychiatry 26, 375–381.
Tarazi, F.I., Baldessarini, R.J., 1999. Regional localization ofdopamine and ionotropic glutamate receptor subtypes instriatolimbic brain regions. J. Neurosci. Res. 55, 401–410.
Tay, A., Simon, J.S., Squire, J., Hamel, K., Jacob, H.J., Skorecki, K.,1995. Cytosolic phospholipase A2 gene in human and rat:chromosomal localization and polymorphic markers.Genomics 26, 138–141.
Teng, C.T., Demetrio, F.N., 2006. Memantine may acutelyimprove cognition and have a mood stabilizing effect intreatment-resistant bipolar disorder. Rev. Bras. Psiquiatr. 28,252–254.
Terry Jr., A.V., Hill,W.D., Parikh, V.,Waller, J.L., Evans, D.R., Mahadik,S.P., 2003. Differential effects of haloperidol, risperidone, andclozapine exposure on cholinergic markers and spatiallearning performance in rats. Neuropsychopharmacology 28,300–309.
Tseng, K.Y., O'Donnell, P., 2004. Dopamine–glutamate interactionscontrolling prefrontal cortical pyramidal cell excitabilityinvolve multiple signaling mechanisms. J. Neurosci. 24,5131–5139.
Ulrich,G.,Herrmann,W.M.,Hegerl,U.,Muller-Oerlinghausen,B., 1990.Effect of lithium on the dynamics of electroencephalographicvigilance in healthy subjects. J. Affect. Disord. 20, 19–25.
Vadnal, R., Parthasarathy, R., 1995. Myo-inositol monophosphatase:diverse effects of lithium, carbamazepine, and valproate.Neuropsychopharmacology 12, 277–285.
Vasudev, K., Goswami, U., Kohli, K., 2000. Carbamazepine andvalproatemonotherapy: feasibility, relative safety and efficacy,and therapeutic drug monitoring in manic disorderPsychopharmacology (Berl) 150, 15–23.
Vial, D., Piomelli, D., 1995. Dopamine D2 receptors potentiatearachidonate release via activation of cytosolic,arachidonate-specific phospholipase A2. J. Neurochem. 64,2765–2772.

209B R A I N R E S E A R C H R E V I E W S 6 1 ( 2 0 0 9 ) 1 8 5 – 2 0 9
Wang, H.-Y., Friedman, E., 1999. Effects of lithium onreceptor-mediated activation of G proteins in rat braincortical membranes. Neuropharmacology 38, 403–414.
Weerasinghe,G.R., Rapoport, S.I., Bosetti, F., 2004. Theeffect of chroniclithium on arachidonic acid release and metabolism in rat braindoes not involve secretory phospholipase A2 or lipoxygenase/cytochrome P450 pathways. Brain Res. Bull. 63, 485–489.
Weichel, O., Hilgert, M., Chatterjee, S.S., Lehr, M., Klein, J., 1999.Bilobalide, a constituent of Ginkgo biloba, inhibitsNMDA-induced phospholipase A2 activation and phospholipidbreakdown in rat hippocampus. Naunyn-Schmiedebergs Arch.Pharmacol. 360, 609–615.
Wellcome Trust, 2007. Genome-wide association study of 14,000cases of seven common diseases and 3,000 shared controls.Nature 447, 661–678.
Wigg, K., Feng, Y., Gomez, L., Kiss, E., Kapornai, K., Tamas, Z.,Mayer, L., Baji, I., Daroczi, G., Benak, I., Osvath, V.K., Dombovari,E., Kaczvinszk, E., Besnyo, M., Gadoros, J., King, N., Szekely, J.,Kovacs, M., Vetro, A., Kennedy, J.L., Barr, C.L., 2009. Genomescan in sibling pairs with juvenile-onset mood disorders:evidence for linkage to 13q and Xq. Am. J. Med. Genet., BNeuropsychiatr. Genet. 150B, 638–646.
Wille, S.M., Cooreman, S.G., Neels, H.M., Lambert, W.E., 2008.Relevant issues in the monitoring and the toxicology ofantidepressants. Crit. Rev. Clin. Lab. Sci. 45, 25–89.
Willour, V.L., Zandi, P.P., Huo, Y., Diggs, T.L., Chellis, J.L.,MacKinnon, D.F., Simpson, S.G., McMahon, F.J., Potash, J.B.,Gershon, E.S., Reich, T., Foroud, T., Nurnberger Jr., J.I., DePauloJr., J.R., McInnis, M.G., 2003. Genome scan of the fifty-sixbipolar pedigrees from the NIMH genetics initiativereplicationsample: chromosomes 4, 7, 9, 18, 19, 20, and 21. Am. J. Med.Genet., B Neuropsychiatr. Genet. 121B, 21–27.
Xiao, Y., Li, X., 1999. Polyunsaturated fatty acids modify mousehippocampal neuronal excitability during excitotoxic orconvulsant stimulation. Brain Res. 846, 112–121.
Yatham, L.N., 2005. Translating knowledge of genetics andpharmacology into improving everyday practice. BipolarDisord. 7 (Suppl. 4), 13–20.
Zarate Jr., C.A., Quiroz, J.A., Singh, J.B., Denicoff, K.D., De Jesus, G.,Luckenbaugh, D.A., Charney, D.S., Manji, H.K., 2005. Anopen-label trial of the glutamate-modulating agent riluzolein combination with lithium for the treatment of bipolardepression. Biol. Psychiatry 57, 430–432.