Embed Size (px)
Citation preview
(AQA A) AS Psychology
Unit 2: PSYA2 – Biological Psychology, Social Psychology
and Individual Differences
Key Study Title Relates to:
Brady (1959) Stress-related illness and the immune system
Kiecolt-Glaser (1984) Stress-related illness and the immune system
Cohen (1993) Stress-related illness and the immune system
Rahe et al (1970) Life changes
DeLongis et al (1982) Daily Hassles
Marmot et al (1997) Workplace stress
Friedman and Rosenman (1959) Personality Factors, including Type A behaviour.
Key Study Title Relates to:
Sherif (1935) Types of conformity
Asch (1951) Explanations of why people conform
Milgram (1974) Obedience
Variations on Milgram (1974) Explanations of why people obey
Bickman (1974) Obedience and pressures to obey authority.
Zimbardo (1973) Implications for social change of research into social influence
Clark (1998) Internalisation
Gamson, Fireman & Rytina (1982) Explanations of independent behaviour
Key Study Title: Relates to:
Rosenhan and Seligman (1989) Definitions of abnormality: Failure to function
Jahoda (1958) Definitions of abnormality: deviation from ideal mental health.
Watson and Rayner (1920) Key features of the behavioural approach to psychopathology
Elkin et al (1989) Psychological and Biological therapies
Davidson et al (2004) Psychological and Biological therapies
Stress-related illness and the immune system
Brady (1958)
A classic study by Joseph Brady linked high levels of stress to
increased hormone production and the development of ulcers. In
an early study he placed monkeys in “restraining chairs” and
conditioned them to press a lever. They were given shocks every
20 seconds unless the lever was pressed in the same time period.
This investigation came to an abrupt halt when many of the
monkeys suddenly died. Post-mortem examination showed that
the monkeys had raised gastro-intestinal hormone levels and that
ulcers were the cause of death. The ulcers were not due to the
restraint because other monkeys had been kept in restraining
chairs for up to 6 months with no deaths occurring. The question was, were the ulcers due the
electric shocks or the stress?
To test this Brady and his colleagues used yoked controls. One monkey, called the “executive”, was
responsible for controlling the lever while a second monkey received the shocks but had no control
over the lever. Therefore only the “executive” monkey received the psychological stress of having to
press the lever but both monkeys received the shocks.
After 23 days of 6 hours on, 6 hours off schedule the executive monkey died due to a perforated
ulcer. Initially Brady thought that the stress might be related to the reinforcement schedule. He tried
various routines, such as 18 hours on and 6 hours off, or 30 minutes on, 30 minutes off. However, no
monkeys died from ulcers. He then tested the stomachs of executive monkeys on a 6 hour on, 6
hour off schedule, and found that stomach acidity was greatest during the rest period.
Brady concluded that it was clearly stress, not the shocks, that created the ulcers, and that the
greatest danger occurred when the sympathetic arousal stopped and the stomach was flooded with
digestive hormones, a parasympathetic rebound.
Task: Re-write this key study in less than 30 words – using a cue card to restrict you. On the reverse of the cue card, find two strengths and two weaknesses of the study. Remember to State, Explain and Apply each point.
Evaluation of Brady (1959)
This study became very well known and for a long time confirmed a common belief that too
much stress at work led to ulcers. The findings were supported in a study by Weiner et al
(1957) using army recruits. Prior to basic training, the soldiers were tested and classed as
oversecretors or undersecretors of digestive enzymes. After 4 months of stressful training,
14 % of the oversecretors had developed ulcers whereas none of the undersecretors had.
This suggests not only that the same principles do apply to humans but also that individual
differences may be important because not all of the oversecretors developed ulcers
One criticism made of Brady’s study in general was that the monkeys were not randomly
selected, the “executive” was chosen because it was faster at learning an avoidance
response. This may of course have parallels with the human world.
A more serious problem was raised in the
research by Marshall et al (1985). They found
strong evidence of another cause of stomach
ulcers, a bacterium called Helicobacter pylori. It
might be that stress has some influence on the
development of ulcers but the danger was that
people assumed this was the only cause. Marshall
was so convinced that the bacterium was at fault
that he deliberately gave himself the infection –
and developed ulcers.
To what extent do you think it is
reasonable to generalise from
research on monkeys to human
behaviour?
What ethical objections could be
raised in connection with this
study?
Stress-related illness and the immune system
Kiecolt-Glaser (1984)
Kiecolt-Glaser (1984) studied human responses to stress by using a naturally occurring situation –
examinations. The researchers took blood samples from 75 1st-year medical students (49 males and
26 females), all of whom were volunteers. The samples were taken one month before their final
examination (the baseline sample) and again on the first day of their final examinations, after the
students had completed two of the examinations. This was the “stress samples” taken when the
students’ stress levels should be at their highest.
Kiecolt-Glaser et al found that natural killer cell
activity declined between the two samples,
confirming other research findings that stress is
associated with a reduced immune response.
The volunteers were also assessed using
behavioural measures. On both occasions they
were given questionnaires to assess psychiatric
symptoms, loneliness and life events. This was
because there are theories which suggest that all
3 are associated with increased levels of stress.
Kiecolt-Glaser et al found that immune responses
were especially weak in those students who
reported feeling most lonely, as well as those
who were experiencing other stressful life events
and psychiatric symptoms such as depression or
anxiety.
This means that there were 2 key findings from
this study. One was that stress was associated with a lowered immune response in humans. The
second was that there were a number of different sources of stress and factors that moderate it.
Evaluation of Kiecolt-Glaser (1984)
There are many strengths to this study. First of all, it was a natural experiment which means
that there can be fewer ethical objections but, at the same time, it does mean it was not a
true experiment. At best we can say that stress and immune response are negatively
correlated (as one increases, the other decreases), we cannot say that one caused the other.
The advantage of this study, again related to the choice of independent variable (exam
stress), is that it was a long-term form of stress. In previous studies with human participants,
stress had been artificially induced, for example by restricting sleep for several days
(Palmblad et al, 1979). This is likely to produce a different kind of stress to that experienced
naturally.

Stress-related illness and the immune system
Cohen (1993)
Cohen et al investigated the role of general life stress on vulnerability to the common cold virus.
Three hundred and ninety-four participants completed questionnaires on the number of stressful life
events they had experienced in the previous year. They also rated their degree of stress and their
level of negative emotions such as depression. The three scores were combined into what Cohen et
al called a stress index.
The participants were then exposed to the common cold virus, leading to 82% becoming infected
with the virus. After seven days the number whose infection developed into clinical colds were
recorded. The findings were that the chance of developing a cold, i.e. failing to fight off the viral
infection, was significantly correlated with stress index scores.
Cohen et al concluded that life stress and negative emotions reduce the effectiveness of our immune
system, leaving participants less able to resist viral infections.
Evaluation of Cohen (1993)
Methodological issues
This was an indirect study in that there were no direct measures of immune function.
However it is supported by Evans and Edgington (1991) who found that the probability of
developing a cold was significantly correlated with negative events in the preceding days.
It did measure health outcomes (development of clinical colds), showing a relationship
between life stress and illness. This can be compared with studies that use measures of
immune function rather than illness outcomes.
There was no direct manipulation of the independent variable (the stress index), and so a
cause and effect relationship cannot be confirmed.
This study does not tell us which element of the stress index is most important.
Ethical issues
Clinical studies in psychology and medicine are always
covered by rigorous ethical considerations. All applications
are reviewed by professional committees, who consider a
variety of issues.
Participants should be in good health with no illnesses or
infections prior to the study.
Participants should be able to give fully informed consent,
with debriefing afterwards.
During the study participants should be constantly
monitored to check for any reactions to the viral challenge.
The scientific value of the study should be balanced against
any psychological or physical distress to participants.
Life changes as a source of stress
Rahe (1970)
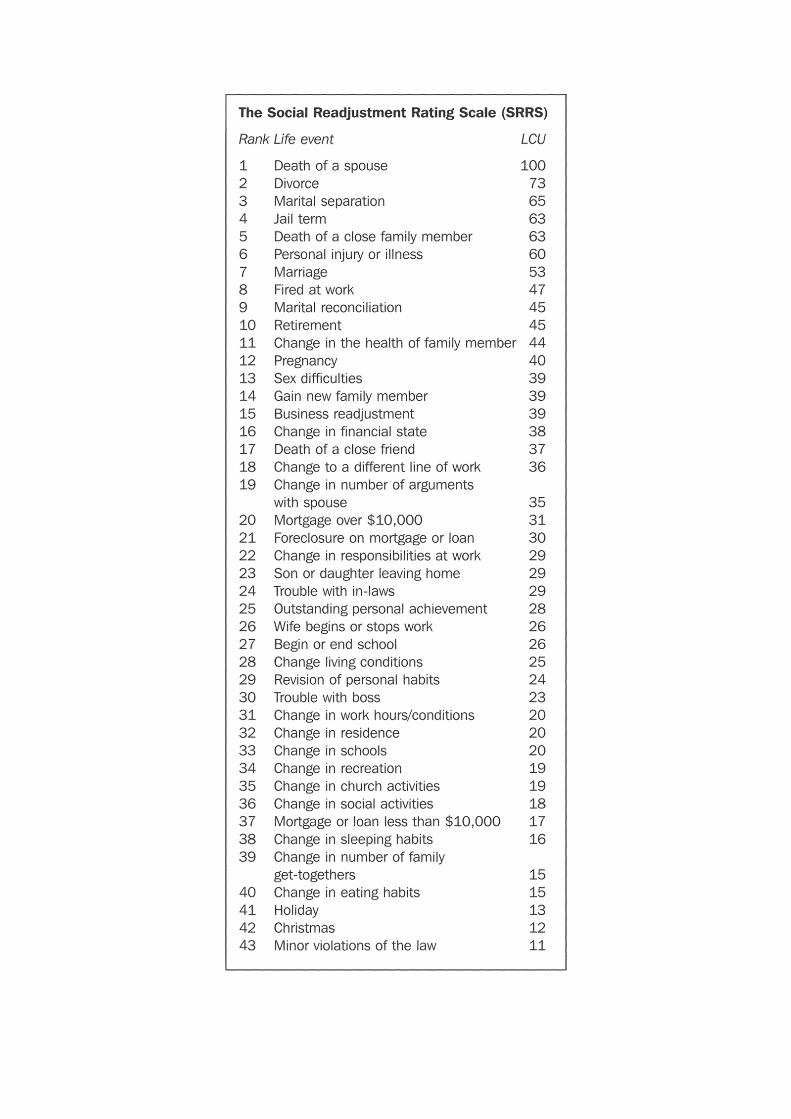
The aim of this study was to investigate whether scores on the Holmes and Rahe Social
Readjustment Rating Scale (SRRS) were correlated with the subsequent onset of illness.
2,500 male American sailors were given the SRRS to assess how many life events they had
experienced in the previous 6 months. The total score on the SRRS was recorded for each
participant. Then over the following six-month tour of duty, detailed records were kept of each
sailor’s health status. The recorded number of Life Change Units were correlated with the sailors’
illness scores.
There was a positive correlation of +0.0118 between Life Change scores and illness scores. Although
the positive correlation was small (a perfect positive correlation would be +1.00), it did indicate that
there was a meaningful relationship between Life Change Units and health (this is often referred to
as a statistically significant correlation). As Life Change Units increased, so did the frequency of
illness.
The researchers concluded that as Life Change Units were positively correlated with illness scores,
experiencing life events increased the chances of stress-related health breakdown. As the
correlation was not perfect, life events cannot be the only factor in contributing to illness.
The study does not take into account individual differences in reactions to stress.
A correlation does not imply causality nor the direction of any effect; depression or anxiety may not be caused
by life events, since depressed or anxious people may bring about life events such as separation or divorce
The sample was restricted to male US Navy personnel; therefore it was ethnocentric (Americans only) and
androcentric (males only). This reduces the validity of the study and makes it difficult to generalise to other
populations.

Daily Hassles
DeLongis et al (1982)
Most people experience major life events very infrequently. Therefore a better measure of stress
might look at the stresses and strains of daily life. These are called “hassles”. DeLongis et al (1982)
compared the two measures: a life events scale and their own hassles scale, to see which was a
better predictor of later health problems. They also considered the effects of “uplifts”. Uplifts are
events that make you feel good. How does that affect health?
Participants were asked to complete four questionnaires once a month for a period of a year:
Hassles scale (117 hassles, such as: concerns about weight, rising prices, home maintenance,
losing things, crime and physical appearance).
Uplifts scale (135 uplifts, such as: recreation, relations with friends, good weather, job
promotion).
Life events questionnaire (24 major events).
A health status questionnaire consisting of questions on overall health status, bodily
symptoms, and energy levels.
There were 100 participants from around San Francisco area, aged between 45 and 64. They were
predominantly well educated and had high income. The findings were that both the frequency and
intensity of hassles were significantly correlated with overall health status and bodily symptoms.
Daily uplifts had little effect on health. They also found no relationship between life events and
health during the study, although there was a relationship for life events recorded for the 2 ½ years
before the study.
Task: With a learning partner, try to find 3 strengths
of this study and 3 weaknesses of this study. Write
the points using the State, Explain and Apply
framework. When you are ready write your point on
the whiteboard.
How might the sample of respondents have biased the results obtained in the study? Why might daily hassles be a better measure of stress than life events?

Evaluation of DeLongis et al (1982)
This approach managed to avoid the problem of the relevance of major life events but it still
overlooked many chronic “ongoing” sources of stress, such as poor housing, low incomes, strains of
family life, unsatisfying work and so on. Health is probably affected by all three: hassles, chronic
situations, and life changes.
One problem with the scales used in this study was that the same hassle can be experienced in
different ways by different people or by the same person on different occasions. The same factors
that are a hassle to one person may actually be uplift to another, or the same factor might mean
different things to the same person on different occasions. For example, a traffic jam may
sometimes give you time to relax, whereas at other times it seems highly stressful. For this reason
DeLongis, Folkman and Lazarus (1988) later produced a single “Hassles and Uplifts Scale” where
respondents could indicate the strength of a factor either as a hassle or an uplift. In other words,
when asked to indicate how they felt about “sex” they could rate it as a 0 1 2 3 as a hassle or 0 1 2 3
as an uplift.
A further problem concerns the original sample which was of people aged over 45, this sample bias
may have affected the results. Khan and Patel (1996) found that older people tended to have less
severe, and fewer, hassles than younger people.
Workplace Stress
Marmot et al (1997)
Most people would agree that work is a source of considerable stress, and some would agree that
this stress may lead to illness. The question for researchers is to find out what aspects of the
workplace are the most important sources of stress.
Marmot et al sought to test the job-strain model. This model proposes that the workplace creates
stress and illness in two ways: (1) high demand and (2) low control. Marmot et al suggested that this
could be tested in context of civil service employees where the higher grades would experience high
job demand, and low-grade civil servants would experience low job control.
Civil service employees (men and women) working in London were invited to take part in this study.
A total of 7,372 people agreed to answer a questionnaire and be checked for signs of cardiovascular
disease. About 5 years later each participant was reassessed. For each participant the following
information was recorded: signs of cardiovascular disease (e.g. ischemia or chest pains), presence of
coronary risk factors (e.g. smoking), employment grade (a measure of the amount of job demand
an individual experienced), sense of job control (measured by questionnaire) and amount of social
support (also measured by a questionnaire).
At the end of the study it was found that participants in the higher grades of the civil service had
developed the fewest cardiovascular problems. Participants in the lower grades expressed a weaker
sense of job control and also had poorest social support. It was also found that cardiovascular
disease could in part be explained in terms of risk factors such as smoking (i.e. people who
developed cardiovascular disease were more likely to be smokers and be overweight).
The main conclusion is that low control appears to be linked to cardiovascular disorder, whereas
high job demand is not linked to stress and illness. This does not fully support the job-strain model
because it does not show that high demand is linked to illness, but lack of control does appear to be
linked to stress and illness.
Can the findings be explained in terms of socio-
economic status?
We can classify individuals in terms of their socio-
economic status (SES) – a measure of the kind of job
they do (skilled or unskilled), how much money they
have, the kind of house they live in and so on. People
who are of low SES are more likely to smoke, live in
more stressful environments and have poorer diets –
all factors linked to cardiovascular problems. This
means that low-grade civil servants may have more
cardiovascular problems than high-grade civil servants
because of factors related to low SES rather than
because they lack job control.
However, Marmot et al argue that other studies have demonstrated that lack of control
does increase stress. If low control is generally a source of stress, it may well be an
important factor of stress in the workplace in addition to other SES factors.
Biased sample
The conclusions of this study are biased on the sample studied- civil servants. The
response s of such individuals may not be typical of all adults as they are urban
dwellers who are probably quite job oriented and ambitious, in contrast with rural
inhabitants whose jobs may play a less significant role in their lives. One study found
that ambitious individuals were more affected by workplace stressors (Caplan et al
1975). Therefore, we might conclude that not everyone will be affected by low control
in the way that these individuals were.
Personality factors, including Type A behaviour
Friedman and Rosenman (1974)
The Western Collaborative Group Study was set up in the 1960’s to test Friedman and Rosenman’s
hypothesis that type A individual were more likely to develop heart disease than type B. The type A
behaviour pattern was initially assessed by means of the structured interview. This assessment
procedure makes use of two kinds of information: (1) the answers given to questions asked during
the interview, and (2) the individual’s behaviour, including aspects of his or her way of speaking (e.g.
loudness and speed of talking). The individual’s tendencies towards impatience and hostility are
assessed by the interviewer deliberately interrupting the person being interviewed from time to
time. The type A behaviour pattern has also been assessed by various self-report questionnaires
(e.g. Jenkins Activity Survey).
On the basis of these measures the participants were classed as A1 (Type A), A2 (not fully type A),
X (equal amounts of A and B), and B (fully type B). Nearly 3,200 healthy men aged between 39 and
59 living around San Francisco were assessed in 1960. Eight and half years later 257 of the men in
the original sample had developed coronary heart disease (CHD).
The findings were striking – 70% of those with CHD had been assessed as Type A, nearly twice as
many as Type Bs. This remained so, even when account was taken of various other factors (e.g.
blood pressure, smoking, obesity) which are known to be associated with heart disease.
One of the limitations of the Western Collaborative Group Study was that it was not clear which
aspect of the Type A behaviour pattern was most closely associated with heart disease. This issue
was addressed by Matthews et al (1977). They re-analysed the data from the Western Collaborative
Group Study, and found that coronary heart disease was most associated with the hostility
component of Type A.

Why is type A (or its hostility component) associated with heart disease? As Ganster et al (1991)
pointed out, it has often been assumed that “chronic elevations of the sympathetic nervous system
(in type As) lead to deterioration of the cardiovascular system”. Ganster et al put their participants
into stressful situations and recorded various physiological measures, including blood pressure and
heart rate. Only the hostility component of Type A was associated with high levels of physiological
reactivity. These findings, when combined with those of Matthews et al (1977), suggest that high
levels of hostility produce increased activity within the sympathetic nervous system, and this plays a
role in the development of coronary heart disease.
Evaluation of Friedman and Rosenman (1974) These findings were confirmed in another large-scale longitudinal study which involved both men and women, the Framingham Heart study (Haynes et al, 1980). However, some researchers have failed to find any relationship between type A and coronary heart disease. This has led a number of psychologists to doubt the importance of the Type A behaviour pattern as a factor in causing heart disease. However, Miller et al (1991) reviewed the literature, and found that many of the negative findings were obtained in studies using self-report measure of type A behaviour. Studies using the Structured Interview with initially healthy populations reported a mean correlation of +0.33 between type A behaviour and coronary heart disease, supporting the initial finding of a moderate relationship between the two variables. One problem for any study is that as soon as an individual knows they are at risk of CHD they may engage in behaviours which modify that risk, such as giving up smoking or taking more exercise. This may create lower long-term correlations between Type A and CHD. The evidence has been applied successfully, for example Friedmand, Tordoff and Ramirez (1986) reported on the Recurrent Coronary Prevention Project which aimed to modify type A behaviour and so reduce CHD in participants who had experienced a heart attack. At a five year follow-up, those participants who had taken part in a behaviour modification did have fewer second heart attacks than those who received counselling or no treatment.
Types of conformity
Sherif (1935)
The first major study of conformity was carried out by
Muzafer Sherif. He made use of what is known as the
autokinetic effect. If we look at a stationary spot of light in
a darkened room, then very small movements of the eyes
make the light seem to move. In Sherif’s key condition, the
participants were first of all tested one at a time, and then
in small groups of three. They were asked to say how much
the light seemed to move, and in what direction. Each
participant rapidly developed his or her own personal norm.
This norm was stable, but it varied considerably between
individuals. When three individuals with very different
personal norms were then put together into a group, they
tended to make judgements that were very close to each
other. The fact that a group norm rapidly replaced the
personal norms of the members of the group indicates the
influence of social influence.
Sherif (1935) also used a condition in which individuals
started the experiment in groups of three, and then were
tested on their own. Once again, a group norm tended to
develop within the group. When the members of the group
were then tested on their own, their judgements
concerning the movement of the light continued to reflect
the influence of the group.
Evaluation of Sherif (1935)
There are three major
limitations with Sherif’s
research. First, he used a
very artificial situation, and
it is not clear how relevant
his findings are for most
everyday situations.
Second, there was no
“correct” answer in his
situation. It is not very
surprising that individuals
rely on the judgment of
others when they have no
clear way of deciding what
judgments to make. Third,
conformity effects can be
assessed more directly by
arranging for all but one of
the participants in an
experiment to give the
same judgement, and then
seeing what effect this has
on the remaining
participant. This was done
by Jacobs and Campbell
(1961) using the
autokinetic effect and they
found strong evidence of
conformity.

Explanations of why people conform
Asch (1951)
Asch’s aim was to see if participants would yield to majority social influence and give incorrect
answers in a situation when the correct answers were always obvious.
Seven male, student participants looked at two cards: the test card showed one vertical line; the
other card showed three vertical lines of different length. The participants’ task was to call out, in
turn, which of these three lines was the same length as the test line. The correct answer was always
obvious. All participants, except one, were accomplices of the experimenter. The genuine
participants called out his answer last but one. Accomplices gave unanimous wrong answers on 12 of
the 18 trials. These 12 trials were called the critical trials. In total, Asch used 50 male college
students as naïve, genuine participants in this first study.
Participants conformed to the unanimous incorrect answer on 32% of the critical trials. This might
not strike you as a very high figure but remember the correct answer was always obvious. 74% of
participants conformed at least once. 26% of participants never conformed. Some of these
‘independent’ participants were confident in their judgements. More often, however, they
experienced tension and doubt but managed to resist the pressure exerted by the unanimous
majority. During post-experimental interviews, some conforming participants claimed to have
actually seen the line identified by the majority as the correct answer. Others yielded because they
could not bear to be in a minority of one and risk being ridiculed or excluded by the group. Most
participants who had conformed, however, experienced a distortion of judgement: they thought
that their perception of the lines must be inaccurate and for that reason they yielded to the majority
view.
Even in unambiguous situations, there may be a strong group pressure to conform, especially if the
group is a unanimous majority. However, after interviewing the participants, Asch concluded that
people go along with the views of other for different reasons. Some people experience normative
social influence and feel compelled to accept the mistaken majority’s norms or standards of
behaviour to avoid being rejected. Others experience informational social influence and doubt their
own judgements – they want to be seen as correct.
Evaluation of Asch (1951)
All the participants were male college students and so a very limited sample.
The time and place when the research was carried out might have affected the
findings. In the 1950s the USA was very conservative, involved in an anticommunist
witch-hunt against anyone who was thought to hold left-wing views (this became
known as ‘McCarthyism’, named after the senator who spearheaded the witch-
hunt) and its educational institutions were more hierarchal than they are today.
Since all the participants were male and college students, it might not be valid to
generalise the findings to a wider population. The way to check this is to rerun the
study using different types of participants. Do you think that male college students
are typical, or more or less conformist than the general population?
TASK:
With a learning partner, find two strengths and two limitations of Asch’s method.
State, explain and apply every point (say why it is good or bad). Furthermore,
explain in your limitations how Asch’s experiment could have been improved.
Obedience
Milgram (1974)
Stanley Milgram (1974) advertised in a local paper for men to take part in an experiment concerning
memory and learning, to be conducted at the prestigious Yale University in America. 40 men, aged
between 20 and 50 volunteered. They were paid $4.50 simply for turning up; payment did not
depend on staying the study. When participants arrived they were told that there would be two
participants, a “learner” and a “teacher”. The experimenter drew lots to see which participant would
take which part. At this point you should know that this experiment was “single blind”. The
participant was not told the true details of the research. The truth was that the other participant was
in fact a confederate of the experimenter, and the “experimenter” was also a confederate. The true
participant always ended up being given the role of the “teacher”.
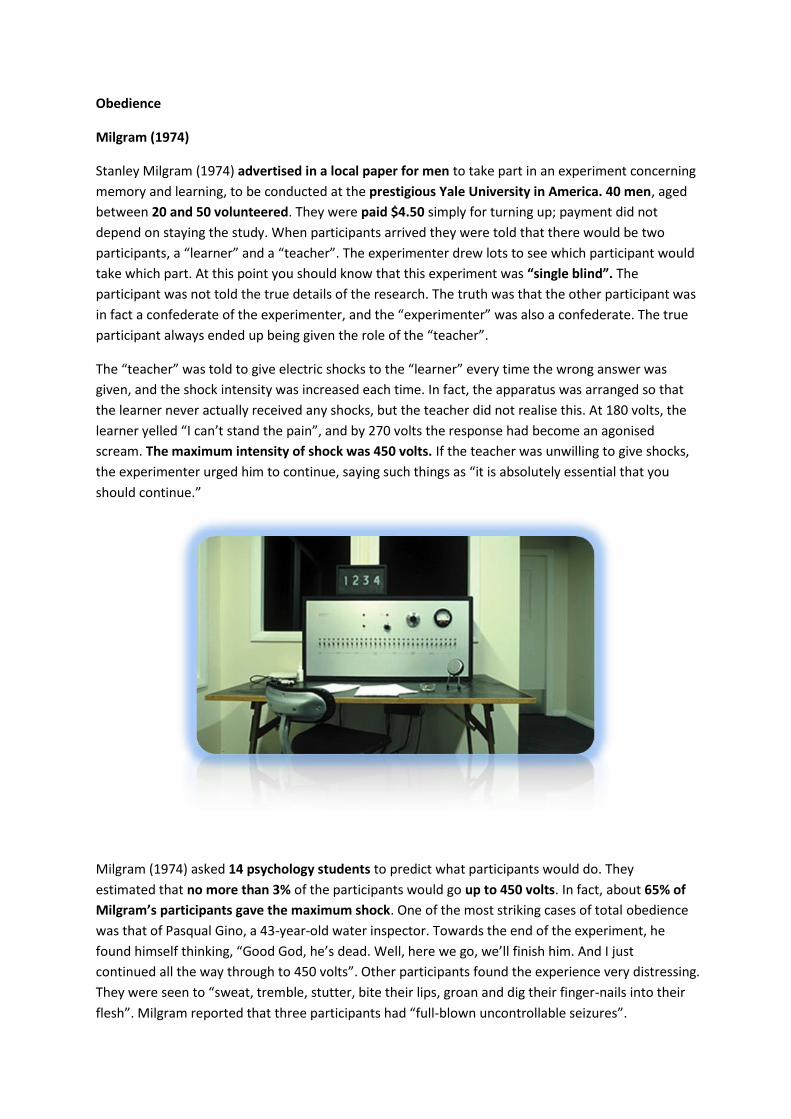
The “teacher” was told to give electric shocks to the “learner” every time the wrong answer was
given, and the shock intensity was increased each time. In fact, the apparatus was arranged so that
the learner never actually received any shocks, but the teacher did not realise this. At 180 volts, the
learner yelled “I can’t stand the pain”, and by 270 volts the response had become an agonised
scream. The maximum intensity of shock was 450 volts. If the teacher was unwilling to give shocks,
the experimenter urged him to continue, saying such things as “it is absolutely essential that you
should continue.”
Milgram (1974) asked 14 psychology students to predict what participants would do. They
estimated that no more than 3% of the participants would go up to 450 volts. In fact, about 65% of
Milgram’s participants gave the maximum shock. One of the most striking cases of total obedience
was that of Pasqual Gino, a 43-year-old water inspector. Towards the end of the experiment, he
found himself thinking, “Good God, he’s dead. Well, here we go, we’ll finish him. And I just
continued all the way through to 450 volts”. Other participants found the experience very distressing.
They were seen to “sweat, tremble, stutter, bite their lips, groan and dig their finger-nails into their
flesh”. Milgram reported that three participants had “full-blown uncontrollable seizures”.
At the end of the experiment all participants were debriefed by being told the actual nature of the
study. They were introduced to the “learner” and assured they he had experienced no actual shocks.
They were told that their behaviour was entirely normal and, when interviewed later by
questionnaire, 74% said they had learned something of personal importance. Only one person
expressed regret about having taken part.
Evaluation of Milgram (1974)
The main text offers a discussion of some of the key criticisms made of this study. The main issues
relate to experimental and ecological validity, and the ethical concerns raised by the study. Criticism
can also be positive, and the findings of this research have had a powerful influence on subsequent
empirical research and psychological theory.
A key feature of the experiment was that the authority, in this case, was “unjust”. The fact that
participants obeyed during the initial stages is neither surprising nor objectionable. The fact that they
continued to obey is surprising. Milgram (1974) said that authority-agent relations are the simple
machinery of social routine. What is significant about some situations, such as his experiment, is that
sometimes authority makes unreasonable requests and then people ought not to obey.
Explanations of why people obey
Variations on Milgram (1974)
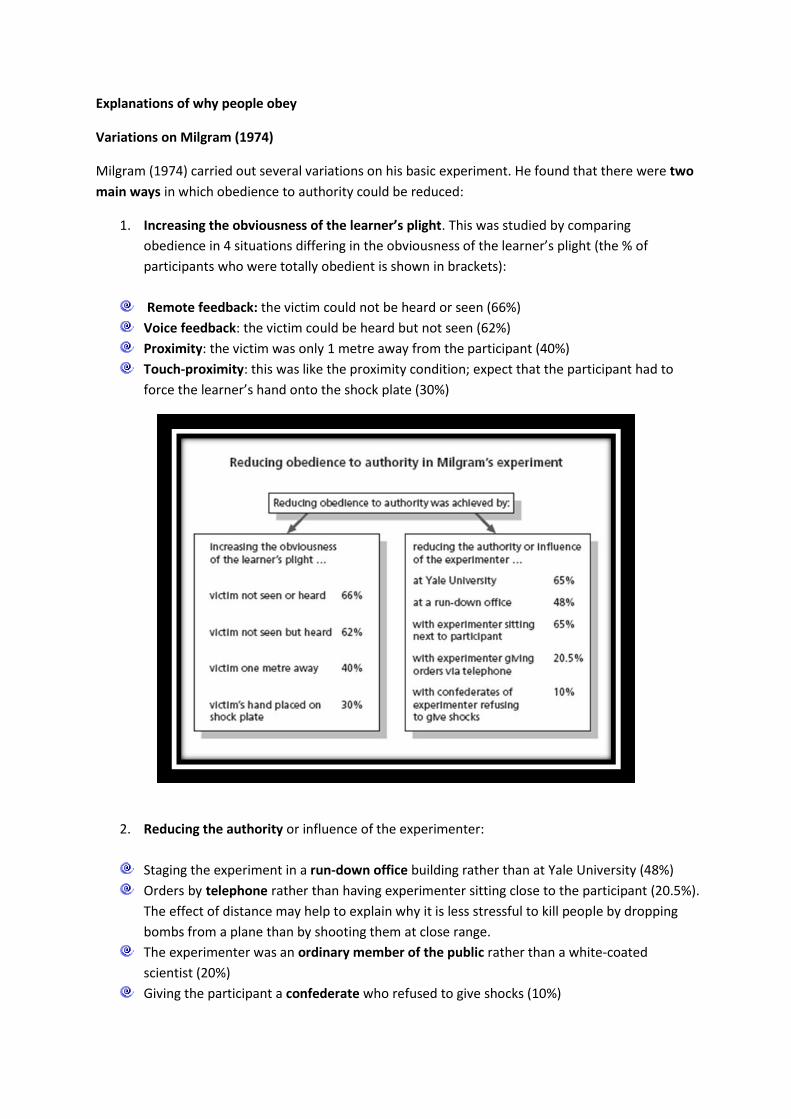
Milgram (1974) carried out several variations on his basic experiment. He found that there were two
main ways in which obedience to authority could be reduced:
1. Increasing the obviousness of the learner’s plight. This was studied by comparing
obedience in 4 situations differing in the obviousness of the learner’s plight (the % of
participants who were totally obedient is shown in brackets):
Remote feedback: the victim could not be heard or seen (66%)
Voice feedback: the victim could be heard but not seen (62%)
Proximity: the victim was only 1 metre away from the participant (40%)
Touch-proximity: this was like the proximity condition; expect that the participant had to
force the learner’s hand onto the shock plate (30%)
2. Reducing the authority or influence of the experimenter:
Staging the experiment in a run-down office building rather than at Yale University (48%)
Orders by telephone rather than having experimenter sitting close to the participant (20.5%).
The effect of distance may help to explain why it is less stressful to kill people by dropping
bombs from a plane than by shooting them at close range.
The experimenter was an ordinary member of the public rather than a white-coated
scientist (20%)
Giving the participant a confederate who refused to give shocks (10%)

Evaluation of Milgram’s variations
These variations give use greater insight into the
conditions under which people will obey unjust
requests. They also show us something about
independent behaviour because in many situations the
majority of participants behaved independently.
There were ethical criticisms made of the original study
by Milgram. One of Milgram’s defences was that he
could not anticipate how many participants would obey
and therefore suffer the stress associated with knowing
what they did. In these later variations Milgram could
not use this defence
Obedience and pressures to obey authority
Bickman (1974)
Leonard Bickman (1974) tested the ecological validity of Milgram’s work by conducting an
experiment in a more realistic setting. In this study three male experimenters gave orders to 153
randomly selected pedestrians in Brooklyn, New York. The experimenters were dressed in one of
three ways: a sports coat and tie, a milkman’s uniform, or guard’s uniform that made them look like
a police officer. The experimenter gave 1 of 3 orders:
Pointing to a bag on the street, “Pick up this bag for me.”
Nodding in the direction of a confederate “This fellow is over parked at the meter but
doesn’t have any change. Give him a dime.”
Approaching the participant at a bus stop, “Don’t you know you have to stand on the other
side of the pole? This signs says ‘No standing’”.
Bickman found that participants were most likely to obey the experimenter dressed as a guard than
the milkman or civilian. This supports one of the variations of Milgram’s findings, that obedience can
be related to the amount of perceived authority.
Who would you obey?
Evaluation of Bickman
Field experiments may have increased ecological validity and mundane realism but the cost is
decreased control. They also raise more ethical concerns because informed consent cannot be
sought and it is difficult to debrief participants without alerting others to the experiment. Bickman’s
study differs from Milgram’s in one important way. The orders were not quite so unreasonable;
therefore obedience was more understandable.

Implications for social change of research into social influence
Zimbardo (1973)
This study is relevant to understanding obedience as well as conformity. It also demonstrates the
power of social situations on people’s behaviour. Specifically, Zimbardo was testing (and trying to
find evidence against) the dispositional hypothesis. According to this, the dehumanising effects of
the prison system are due to prisoners’ antisocial attitudes and behaviour, and guards’ sadism and
insensitivity. Participants were carefully selected for not displaying any of these characteristics. They
were randomly assigned to the role of prisoner or guard. This meant that any antisocial behaviour or
sadism they showed was caused by the prison conditions, not by participants’ personal
characteristics. A mock (simulated) prison was deliberately created (in the basement of the Stanford
University psychology department). Hence, the study is often called the ‘prison simulation
experiment’ (or the ‘Stanford prison study’). Zimbardo wished to create a prison-like environment,
which was as psychologically real as possible.
Participants were recruited though newspaper advertisements asking for male student volunteers
for a two-week study of prison life. From 75 volunteers, 24 were selected. They were judged to be
emotionally stable, physically healthy, and of ‘normal to average’ personality. They also had no
history of psychiatric problems, and had never been in trouble with police. They were all white,
middle-class students from across the US. Those allocated to the prisoner role were arrested by local

police. They were charged with a felony, read their rights, searched, handcuffed, and taken to the
police station to be ‘booked’. After being fingerprinted, each prisoner was taken blindfold to the
basement prison. On arrival, they were stripped naked and issued with a loose-fitting smock. Their
ID number was printed on the front and back, and they had a chain bolted around one ankle. They
wore a nylon stocking to cover their hair, were referred to by number only, and were allocated to
6 x 9ft ‘cells’ (three to a cell). The guards wore military-style khaki uniforms and silver reflector
sunglasses (making eye contact impossible). They carried clubs, whistles, handcuffs, and keys to the
cells. There were guards on duty 24 hours a day, each working eight hour shifts. They had complete
control over the prisoners, who were confined to their cells around the clock – except for meals,
toilet privileges, head counts and work.
An initial ‘rebellion’ by the prisoners was crushed. After this, they began to react passively as the
guards stepped up their aggression. They began to feel helpless and no longer in control of their lives.
Every guard at some time or another behaved in an abusive, authoritarian way. Many seemed to
really enjoy the new-found power and control that went with the uniform. After less than 36 hours,
one prisoner had to be released because of uncontrolled crying, fits of rage, disorganised thinking,
and severe depression. Three others developed the same symptoms, and were released on
successive days. Another prisoner developed a rash over his whole body. They became demoralised
and apathetic, and started to refer to themselves (and others) by their numbers. Zimbardo intended
the experiment to run for two weeks. But it was abandoned after just six days, because of the
prisoners’ pathological reactions.
Zimbardo rejected the dispositional hypothesis. They argued that their findings supported the
situational hypothesis. This claims that it’s the conditions of prisons (physical, social and
psychological) that are ‘to blame’, not the characteristics of prisoners and guards. So, anyone given
the role of guard or prisoner would probably behave as Zimbardo’s participants did. A brutalising
atmosphere, like the mock prison, produces brutality. If the roles had been reversed, the prisoners
would have abused their power in just the same way. It’s the prison environment that makes people
act in ‘typical guard’ or ‘typical prisoner’ ways.
Evaluation of Zimbardo (1973)
High ecological validity. Both the environment and the behaviour (of guards and prisoners)
were ‘realistic’, and the findings can be applied to real prisons.
Mere role-playing. Participants were acting out their prior expectations about how guards
and prisoners should behave (based on TV, movies etc). In other words, they were
conforming, but this wasn’t so much yielding to group pressure as trying to be a ‘typical’
guard or prisoner.
The reality of roles. They may have been role-playing at the start. But participants were
soon taking their roles very seriously indeed – they became ‘real’.
Relevant to social influence. The experiment relates to various forms of social influence.
These include both conformity and obedience.
Informed consent. Participants signed an informed consent form before the experiment
began. They were told a great deal about the experiment – its purpose, what was likely to
happen and so on. But they weren’t told about how they’d be arrested.
Zimbardo’s loss of objectivity. Zimbardo should have stopped the experiment long before
6 days. Zimbardo admitted that he became too involved in his role as prison supervisor. An
outsider had to remind him that he was also the psychologist in charge of the study!
Practical consequences. The experiment had practical implications for the welfare of
prisoners.
Internalisation
Clark (1998)
Clark carried out a series of studies using the 1954 film 12 Angry Men in which a single juror (the
actor Henry Fonda) believes that a defendant is innocent of killing his father and sets out to convince
the rest of the jury that the young man is innocent. Participants were asked to play the role of jurors
and to make up their minds about the guilt or innocence of the young man.
Clark wanted to test two different predictions in these studies:
That the minority could exert its influence through the information presented and the
persuasive nature of the minority’s arguments
That the minority could influence the majority through changes in behaviour or ‘defections’.
Seeing other people change their view can have a powerful effect on the individual’s own
beliefs.
In the first study, Clark used 220 psychology students, 129 women and 91 men. The participants
were given a four-page booklet with a summary of the plot of 12 angry men. This booklet contained
evidence for the defendant’s guilt:
That he had purchased and used a rare knife from a local store.
That he had been seen by two eyewitnesses, one an old man who claimed he had heard the
defendant say ‘I am going to kill you’, and the other a woman who had been in the
apartment opposite, who identified the defendant as the murderer.
Clark varied whether or not the students were given information about Henry Fonda’s defence and
the counter arguments. He found that a minority juror only led people to change their minds when
they could provide counter-evidence to the charge. If they did not provide evidence, people did not
move from the majority position. This supports his claim that the information given by the minority
is important.
In another study, Clark focused on the impact of behaviour, or people defecting to the minority
position. Student participants were given a three-page summary of the jury’s discussion in the film.
This contained the main counter arguments presented by the minority juror played by Henry Fonda.
These were:
That he (Henry Fonda) had been able to produce in court an identical ‘rare’ knife, which he
had bought from a nearby junk shop.
That the man could not have seen or heard the murder as his old age and disabilities meant
it took him too long to get to the window in the apartment
That the old woman could not have seen the defendant as she had very bad eyesight and
was not wearing glasses.
Clark presented different scenarios to the students in which he showed varying numbers of
defectors (people changing their behaviour to adopt the ‘not guilty’ position) from one to six. Clark
asked the students to use a nine-point scale to give their opinion of whether or not the man was
guilty. He found that participants were influenced by the number of defectors to the ‘not guilty’
position. When they heard that four or seven jurors had changed their mind to agree with Henry
Fonda they were more likely to adopt the ‘not guilty’ position themselves. Seven defectors had no
more influence than four. Clark argued that after four people had changed their minds; a ‘ceiling of
influence’ is reached, meaning that more defectors do not produce more influence. The findings of
this study support Clark’s view that minorities can influence people to change their views through
changing their own behaviour.
Evaluation of Clark (1998) Methodological issues
Clark’s study provides a very good example of how research into social psychology has changed over the last 30 years. In contrast to Asch and Moscovici, who used laboratory experiments to investigate conformity, Clark’s participants were asked to play the role of jurors. The task was a simulation of a realistic situation in which social influence takes place – that of jury decision making.
The costs of making an error for participants in this research study were much lower
than in real-life jury service, where it is likely that decisions would be accompanied by much more soul searching. It is questionable how far the results of this role-play can be generalised to real-life jury service.
Ethical issues
In this study, participants were not misled as to the nature of the task and were subjected to little by way of stress or discomfort during the role play. This means that the role play is much more ethically acceptable than previous experimental studies, which have involved stress and deception.
Explanations of independent behaviour
Gamson, Fireman and Rytina (1982)
Gamson et al wished to set up a situation in which participants were encouraged to rebel against an
unjust authority. The researchers placed an advert in the local papers in a town in Michigan, US,
asking for volunteers to take part in a paid group discussion on ‘standards of behaviour in the
community’. Those who responded were asked to attend a group discussion at a local Holiday Inn.
When they arrived they were put into groups of nine and met by a consultant from a fictional human
relations company called Manufacturers Human Relations Consultants (MHRC). The young man
explained that MHRC was conducting research for an oil company, which was taking legal action
against a petrol station manager. They argued that the manager had been sacked because his
lifestyle was offensive to the local community. In contrast, the manager argued that he had been
sacked for speaking out on local television against high petrol prices.
Participants were asked to take part in a group discussion about the sacking, and this was filmed. As
the discussion unfolded, it became apparent that the participants’ own views were irrelevant and
that the HR Company wanted them to argue in favour of the sacking. At a number of points during
the discussion, the cameraman stopped filming and instructed different members of the group to
argue in favour of the oil company’s decision to sack the manager. Finally, the participants were
asked to sign a consent form allowing the film to be shown in a court case.
Of the 33 groups tested by Gamson, 32 rebelled in some way during the group discussion. In 25 out
of the 33 groups the majority of group members refused to sign the consent form allowing the film
to be used in court. Nine groups even threatened legal action against MHRC. Rebellion against
authority in this context involved challenging two well-established social norms in the situation, the
norm of obedience and the norm of commitment, both of which participants had engaged in by
agreeing to take part in the study.
Evaluation of Gamson, Fireman and Rytina (1982)
Methodological issues
Gamson’s research had a high level of realism. While the situation itself was
rather unusual, participants’’ behaviour was likely to be free from demand
characteristics as they were unaware they were participating in a research
study.
It was difficult to separate the many factors that may have led to disobedience
in this study. Rebellion could have been influenced by a number of factors
including the high costs involved of being seen to lie on film in court as well as
the group nature of the decision. Both of these are likely to have contributed
to the high level of disobedience shown.
Ethical issues
A number of ethical issues were involved in this study. Participants were
deceived as to the nature of the exercise and did not give their fully informed
consent. In addition, the experience was exceedingly stressful for those who
took part.
7 features of abnormality
Rosenhan and Seligman (1989) suggest that the most suitable approach to defining mental
abnormality may be to identify a set of abnormal characteristics. Each of these on its own may not
be sufficient to cause a problem but, when several are present, then they are symptomatic of
abnormality. The fewer of the seven features of abnormality displayed by individuals in their
everyday lives, the more they can be regarded as normal. This approach allows us to think in degrees
of normality and abnormality, rather than simply making judgements about whether a behaviour or
a person is abnormal or not.
SUFFERING – Most abnormal individuals report that they are suffering, and so the presence
of suffering is a key feature of abnormality. However, it is not adequate on its own because,
for example, nearly all normal individuals grieve and suffer when a loved one dies. In
addition, some abnormal individuals (e.g. psychopaths or those with anti-social personality
disorder) treat other people very badly but do not seem to suffer themselves.
MALADAPTIVENESS – Maladaptive behaviour is behaviour that prevents an individual from
achieving major life goals such as enjoying good relationships with other people or working
effectively. Most abnormal behaviour is maladaptive in this sense. However, maladaptive
behaviour can occur because of an absence of relevant knowledge or skills as well as
because of abnormality.
VIVIDNESS & UNCONVENTIALITY OF BEHAVIOUR – Vivid and unconventional behaviour is
behaviour that is relatively unusual. The ways in which abnormal individuals behave in
various situations differ substantially from the ways in which we would expect most people
to behave in those situations. However, the same is true of non-conformists.
UNPREDICTABLITY AND LOSS OF CONTROL – Most people behave in a fairly predictable and
controlled way. In contrast, the behaviour of abnormal individuals is often very variable and
uncontrolled, and is inappropriate. However, most people can sometimes behave in
unpredictable and uncontrolled ways. IRRATIONALITY AND INCOMPREHENSIBILITY – A common feature of abnormal behaviour is
that it is not clear why anyone would choose to behave in that way. In other words, the
behaviour is irrational and incomprehensible. However, behaviour can seem
incomprehensible simply because we do not know the reasons for it. For example, a
migraine may cause someone to behave in ways that are incomprehensible to other people. OBSERVER DISCOMFORT – Our social behaviour is governed by a number of unspoken rules
of behaviour. These include maintaining reasonable eye contact with other people and not
standing too close to other people. Those who see these rules being broken often
experience some discomfort. Observer discomfort may reflect cultural differences in
behaviour and style rather than abnormality. For example, Arabs like to stand very close to
other people, and this can be disturbing to Europeans. VIOLATION OF MORAL AND IDEAL STANDARDS – Behaviour may be judged to be abnormal
when it violates moral standards, even when many or most people fail to maintain those
standards. For example, religious leaders have sometimes claimed that masturbation is
wicked and abnormal, in spite of the fact that it is widespread.
Evaluation of Rosenhan and Seligman (1989)
One of the greatest problems with the seven features of abnormality proposed by
Rosenhan and Seligman is that most of them involve making subjective judgements.
Behaviour that causes severe discomfort to one observer may have no effect on
another observer, and behaviour that violates one person’s moral standards may be
consistent with another person’s moral standards. (an example might be
vegetarianism).
Another problem with some of the proposed features of abnormality is that they
can also apply to people who are non-conformists or who simply have their own
idiosyncratic style.
This issue was addressed in the introduction to the 3rd revised version of the
Diagnostic and Statistical Manual of Mental Disorders (DSM III-R), published in 1987.
“Neither deviant behaviour, e.g. political, religious, or sexual, nor conflicts
that are primarily between the individual and society are mental disorders
unless the deviance or condition is a symptom of a dysfunction
(i.e. impairment of function) in the person.”
This does support the concept of “dysfunction”
that is subjective but in a way that allows us to
view the experience of mental disorder from the
point of view of the person experiencing it.
TASK:
With a learning partner, search for
two strengths and two weaknesses
of this definition of abnormality.
Allow time for you to state your
point, explain what the point means
and then for you to apply your point
(say WHY it is a strength or a
weakness).
You can also suggest a way in which
this definition of abnormality could
be improved.
The characteristics of mental health
We define physical health in terms of the presence of healthy behaviours, such as normal body
temperature and normal skin colour. Why not do the same for mental illness? We can consider
abnormality as the absence of normality. In fact, Marie Jahoda (1958) argued that the concepts of
abnormality and normality were useless because they rely on the identification of a reference
population. She suggested that it was preferable to identify the criteria for positive mental health
and then look at the frequency of their distribution in any population.
Jahoda wrote a report for the Joint Commission on Mental Illness and Health. She drew on the views
of others and tried to identify common concepts that were used when describing mental health. In
her report she proposed that there were six categories that clinicians typically related to mental
health.
SELF-ATTITUDES – High self-esteem and a strong sense of identity are related to mental
health.
PERSONAL GROWTH – The extent of an individual’s growth, development or self-
actualisation is important. These criteria are not concerned with one’s self perception but
more with what a person does over a period of time.
INTERGRATION – This is a “Synthesising psychological function”, the extent to which the
above two concepts are integrated. It can be assessed in terms of the individual’s ability to
cope with stressful situations.
AUTONOMY –The degree to which an individual is independent of social influences and able
to regulate his or herself.
PERCEPTION OF REALITY – Many clinicians identify the link with reality as a prime factor in
mental healthiness. This includes being free from “need-distortion” (an individual’s need to
distort their perception of reality) and demonstrating empathy and social sensitivity.
ENVIRONMENTAL MASTERY – The extent to which an individual is successful and well-
adapted. This includes the ability to love, adequacy at work and play, adequacy in
interpersonal relations, efficiency in meeting situational requirements, capacity for
adaptation and adjustment, and efficient problem solving.
TASK:
Which of the above categories might be affected
by cultural bias? In what way might they be
affected? With a learning partner, give an
example of a cultural bias for each category.
How might the “environmental mastery”
category be criticised?
Evaluation of Jahoda (1958)
This approach has the benefit of being positive. It seeks to identify the characteristics that
people need to be mentally healthy rather than identifying the problems (i.e. ill health). As
such it could be translated into useful therapeutic aims – goals to set during treatment.
However, it may not provide useful criteria for identifying what constitutes abnormality.
When we use signs of physical health to identify physical ill health, we rely on fairly objective
measurements, such as blood pressure. The same is not true when we are using
psychological concepts. A psychological scale that measures a person’s self-esteem can
never be an objective measurement.
A further problem is that any set of values is inevitably culture-bound; related to the specific
historic period and the views of a particular society. Nobles (1976) wrote about the
extended concept of self in African people. He claimed that they have a sense of “we”
instead of the Western “me”. This means that they value co-operation whereas Westerners
value independence and autonomy, as reflected in Jahoda’s list of mentally healthy
behaviours.
Different cultures may view the themes of The Simpsons in different ways.
TASK: In what way does the above article make Marie Jahoda a more credible source?
Key features of the behavioural approach to psychopathology
Watson and Rayner (1920)
In one of the most celebrated if unethical studies in psychology, Watson and Rayner (1920)
classically conditioned an 11-month old child, since known as Little Albert, to fear fluffy animals.
They did this by pairing presentation of a tame white rat with a sudden loud noise. The noise caused
fear, an unconditional reflex equivalent to salivation in Pavlov’s experiment, while the rat was the
equivalent of the bell. Eventually Albert was conditioned to associate the rat with fear. Little Albert
also became afraid of other fluffy objects similar to the white rat such as a rabbit and white dog; this
is known as stimulus generalisation.
Methodological issues
We should also note that this was a single case study and there was no systematic and objective
measure of any signs of ‘fear’; instead Watson and Rayner relied on general verbal descriptions.
Ethical issues
Besides the serious ethical issue of scaring a young child and causing psychological harm,
Watson and Rayner did not de-condition Little Albert as his mother, with Watson and Rayner’s
knowledge, removed him from the research programme.

Biological and psychological therapies
Elkin et al (1989)
This was a study across several treatment centres. In all 240 patients with depression were treated
with either CBT, psychotherapy or anti-depressant drugs. There was also a placebo control group.
Treatment lasted for 16 weeks. The findings were:
There was a large placebo effect of 35-40%.
All therapies were significantly more effective than placebo, and overall had similar levels of
effectiveness
Drugs tended to be the most effective therapy for severe depression.
The individual therapist was a significant factor in the effectiveness of psychotherapy.
Across all treatment groups, 30-40% of patients did not respond to therapy. It is a common
finding in studies of effectiveness that no treatment is ever 100% effective.
The conclusions were that drugs, CBT and psychotherapy are all more effective that placebo in
treating depression. Also note that the follow-up was only 16 weeks. Ideally patients should be
followed up for 6-12 months, as there is evidence that the therapeutic effect of CBT in anxiety
conditions is longer lasting than the effect of drugs (Bechdolf et al 2006)
Biological and psychological therapies
Davidson et al (2004)
295 patients with generalised social anxiety (fear of social situations) were treated either with CBT,
with the SSRI antidepressant fluoxetine, or with combined CBT + fluoxetine.
The findings were:
The overall placebo effect was 19%
All therapies were effective over and above the placebo effect, and after 14 weeks there
were no differences between the therapy groups. The combined therapy was not superior to
either therapy alone.
40-50% of patients did not respond to therapy.
The conclusions were that drugs and CBT are equally effective in treating social anxiety, and
combining them does not improve their effectiveness. However many patients do not respond to
either treatment.
Studies comparing treatments – methodological issues
Elkin and Davidson are not conventional experiments. They do have an independent
variable (the different treatments) and a dependent variable (the effect of the
treatment, measured by improvement).
The separate patient groups to be given the different treatments should be
matched in terms of severity of the disorder. It would also be desirable if they
were matched on other characteristics, such as age, gender, socioeconomic
status. This is rarely possible, but these factors have been shown to influence,
for instance, depression.
The length of the study should be sufficient for treatment effects to be
observable. Even with drugs effects can take weeks to develop. Ideally
observation should continue for at least a year to check that any improvement
is sustained and not temporary.
There should be a non-treated group to control for the specific effects of
treatment. With drugs this is a placebo group given a non-active substance they
think is the drug. For psychological therapies it is more difficult. Often an
‘interaction’ condition is used where participants talk to the therapist but there
is no attempt to apply scientific techniques such as CBT or free association. This
controls for the effects of being given attention by a therapist.
Measurement of improvement should be consistent and thorough across the
groups. Questionnaires can be given to participants, and there should also be
ratings of clinical improvement by qualified staff; these staff should not know
what treatment group the participants is in to prevent bias and investigator
effects.
Studies comparing treatments – ethical issues
These studies should be subject to the same ethical criteria as psychological
experiments. For instance, a major issue in the study of psychological disorders is
informed consent; people with disorders may be less able to understand the full
consequences of a treatment. Avoidance of psychological harm is also important,
and debriefing should be carried out.
An issue specific to studies evaluating treatments is that a non-treated control
group is used. If treatments are effective, the control group is denied help. As a
control group is essential to measure improvement this is unavoidable, and is
justified by the hope of identifying the most effective treatment.
The picture that emerges is that in terms of general effectiveness, no one
therapy if consistently the best and this is particularly the case for
depression and general anxiety. However there are other considerations
that can help decide the most appropriate treatment.
For accessibility and speed of action, i.e. how easy is it to provide
treatment and how quickly it works, drug therapy stands out. Drugs are
readily available for most disorders, and although it usually takes a few
days for the therapeutic effect to appear, this is faster than for CBT,
behavioural and psychodynamic therapies.





























