Embed Size (px)
Citation preview

Andrew K. Roorda, M.D., Series Editor
Practical GastroenteroloGy • december 2011 17
inFlammatory boWel disease: a Practical aPProacH, series #73
Farid Jalali, MS-IV, West Virginia University School of Medicine, Morgantown, WV. Andrew Roorda, M.D., Assistant Professor, Section of Digestive Diseases, Department of Medicine, West Virginia University School of Medicine, Morgantown, WV. Uma Sundaram, M.D., Chief, Section of Digestive Diseases; West Virginia Clinical and Translational Science Institute, West Virginia University School of Medicine, Morgantown, WV.
endoscoPy: oPeninG neW eyes, series #6
Andrew K. Roorda
Biliary Stone Extraction Techniques: Old and New
Farid Jalali Uma Sundaram
Choledocholithiasis is defined as the presence of one or more gallstones in the common bile duct. Common bile duct (CBD) stones can be divided into primary stones, which are formed within the bile ducts, and secondary stones, which originate within the gallbladder and then migrate into the common bile duct. The incidence of choledocholithiasis ranges from 5-10% in patients undergoing laparoscopic cholecystectomy for symptomatic cholelithiasis[1-4] to 18-33% in patients with acute biliary pancreatitis.[5-8] An estimated 21-34% of CBD stones spontaneously migrate[9, 10] and pose a risk of acute biliary pancreatitis or cholangitis if they obstruct the distal duct. Because of the life-threatening nature of biliary pancreatitis and cholangitis, removal of discovered common bile duct stones is generally recommended.[11] Endoscopic retrograde cholangiography (ERCP) with endoscopic sphincterotomy (ES) is currently the first-line management strategy for choledocholithiasis. Steady advancements in technology have led to creation of a myriad of devices and techniques to facilitate bile duct stone removal, ranging from the early surgical exploration of the common bile duct to newer methods of lithotripsy and novel endoscopic systems such as SpyGlass® (Boston Scientific Corporation, Natick, MA). The purpose of this publication is to provide an overview of the features, techniques, indications, clinical efficacy, safety, and potential complications of various methods of bile duct stone removal.
Surgical MethodS of coMMon Bile duct Stone reMoval
open exploration of cBd
removal of common bile duct stones prior to the introduction of endoscopic retrograde cholangiography (ERCP) and endoscopic
sphincterotomy (ES), both discussed below, in the 1970s was primarily performed by surgical open exploration of the common bile duct.
Although rarely performed today given the success of endoscopic and laparoscopic techniques of bile duct stone removal, there are still indications for performing an open common bile duct exploration. These indications include patients who are undergoing another open abdominal procedure or an open cholecystectomy because of difficulty undergoing or completing a laparoscopic cholecystectomy. Mortality rate for open elective and emergency exploration of CBD ranges from 4-20% in patients >80 years old.[12-14]
Roorda_December_11.indd 17 12/13/11 2:10 PM

18� Practical�GastroenteroloGy� •� december�2011
endoscoPy:�oPeninG�neW�eyes,�series�#6endoscoPy:�oPeninG�neW�eyes,�series�#6
Biliary Stone Extraction Techniques
Laparoscopic Common Bile Duct ExplorationIn cases of cholecystocholedocholithiasis, the simultaneous treatment of stones in both the gallbladder and the common bile duct can be achieved at the time of laparoscopic surgery. Because over 80% of gallbladders are removed laparoscopically[14], laparoscopic exploration of the common bile duct is being performed with increasing frequency in a carefully selected patient population and in the hands of skillful laparoscopic surgeons.
Two prospective, randomized European trials[15, 16] have demonstrated a significantly shorter hospital stay in patients undergoing laparoscopic cholecystectomy and common bile duct exploration compared to patients who received laparoscopic cholecystectomy followed by post-operative ERCP. Duct clearance rates and morbidity rates were found to be similar in the two treatment groups. As mentioned in these two studies, the primary obstacle to the widespread use of laparoscopic exploration of the common bile duct at the time of laparoscopic cholecystectomy is the requirement for a surgeon to have a high level of expertise and skill.
Laparoscopic common bile duct exploration (LCBDE) is generally considered to be safe and effective in skilled hands and has the advantage of being a single-stage procedure in management of bile duct stones compared to laparoscopic cholecystectomy followed by post-operative ERCP. In a meta-analysis published in 2006 that reviewed 13 randomized trials consisting of 1,351 patients, Martin et al. demonstrated that laparoscopic common bile duct stone clearance was as efficient as pre- and post-operative ERCP and with no significant difference in morbidity and mortality. The Authors noted that laparoscopic trials universally reported shorter hospital stays in surgical arms but insufficient data were available at the time of this meta-analysis for a cost analysis.[17] Given its similar efficacy and improved efficiency compared with ERCP, the American Society for Gastrointestinal Endoscopy in a 2011 publication has recommended LCBDE as an alternative to ERCP as a first-line strategy for CBD stone removal in the setting of symptomatic cholelithiasis in centers where surgical expertise is available.[18]
TechniqueTwo methods of bile duct stone removal have been used in the laparoscopic approach: transcystic and choledochotomy. A transcystic approach is easier to
perform than a direct choledochotomy as it does not require suture repair.[19] The choledochotomy approach is performed when transcystic duct exploration is not appropriate or has failed to achieve stone extraction.[20]
Whether common bile duct exploration occurs by the open or the laparoscopic method, the remainder of the procedure to achieve stone extraction is performed in a similar fashion. The first technique is to irrigate the common bile duct with normal saline while relaxing the sphincter of Oddi by administration of intravenous glucagon; success of this method is limited to very small stones <2 mm in size or sludge. Another initial method of stone removal is dislodgement using Fogarty-type, low-pressure, balloon-tipped catheters. If these maneuvers fail, basket removal, usually under direct visualization via a choledochoscope or fluoroscope, is attempted. If still unsuccessful, intracorporeal electrohydraulic lithotripsy or laser lithotripsy can be attempted under direct visualization.[19, 20]
EnDosCopiC ThErapEuTiC METhoDs
BackgroundEndoscopic retrograde cholangiography (ERCP) with endoscopic sphincterotomy (ES), first described in 1974, is considered the method of choice for clearing bile duct stones. Approximately 150,000 such procedures are performed annually in the United State, and, in experienced hands, the procedure has proven to be safe and effective.[21] Sensitivity of ERCP for detection of choledocholithiasis is 89-93%.[22, 23] Successful extraction of a stone, once identified at cholangiography, typically requires ES or other alternative techniques (discussed later). If a stone is anticipated but not identified at cholangiography (e.g., small stone in a dilated duct), an empirical ES can be performed to facilitate duct sweeping after careful risk-benefit analysis by the endoscopist. ES when combined with standard endoscopic devices such as balloon catheters and wire baskets has a 90% success rate for bile duct clearance.[24] Patients with large stones (>12 mm), multiple stones, barrel-shaped stones, or a tapering or tortuous distal common bile duct may require special treatment such as lithotripsy in addition to sphincterotomy to achieve bile duct clearance.[25] This section attempts to provide an overview of technique, safety, complications, and special circumstances encountered in the practice of ERCP with ES as it pertains to the managements of choledocholithiasis.
Roorda_December_11.indd 18 12/13/11 2:10 PM

ENDOSCOPY: OPENING NEW EYES, SERIES #6ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
Practical GastroenteroloGy • december 2011 19
Timing of ERCPThe degree of procedure urgency largely depends on the specific clinical scenario and the severity of undesirable outcomes in the patient. Truly urgent therapeutic ERCP is indicated in cases of severe acute cholangitis caused by obstructing biliary stones not responding to medical therapy; biliary drainage, rather than stone removal, is the primary goal of intervention in such severe cases of acute cholangitis. In less severe cases of acute cholangitis that exhibit clinical response to medical therapy, ERCP can be delayed generally for 72 hours.[26-28] The benefits of early (<72 hours) ERCP in patients with acute biliary pancreatitis have been a subject of controversy with some randomized trials showing reduced morbidity[29-31], yet other trials showing no benefit in the absence of concurrent acute cholangitis[32] or obstructive jaundice.[33]
The timing of ERCP for management of CBD stones in relation to a planned laparoscopic cholecystectomy has been the subject of multiple studies. No conclusive evidence exists to support superiority of outcomes in pre-, intra-, or post-operative ERCP for management of CBD stones. In a retrospective study of 67 patients, overall complication rates, hospital length of stay, and total hospital charges were not statistically different among the three groups.[34] Preoperative ERCP is typically considered for patients with a high likelihood of choledocholithiasis, whereas intraoperative and postoperative ERCP are valid and comparable approaches for patients with evidence of choledocholithiasis found during an intraoperative cholangiogram.
Delays longer than two weeks from the time of preoperative ERCP to laparoscopic cholecystectomy have been associated in multiple retrospective studies with biliary colic, recurrent choledocholithiasis, cholecystitis, gallstone pancreatitis, and a higher rate of conversion to open cholecystectomy.[35-38] Stronger evidence in support of early laparoscopic cholecystectomy after preoperative ERCP now exists through a recent randomized trial of 96 patients status post-endoscopic CBD stone clearance. This trial reported a significantly higher morbidity in patients that underwent delayed (6-8 weeks) compared to early (<72 hours) laparoscopic cholecystectomy following preoperative ERCP; a 36% incidence of recurrent biliary events, primarily acute cholecystitis and biliary colic, was reported in the delayed surgery arm compared with 2% in the early group.[39]
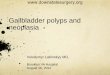
TechniqueStandard sphincterotomy requires successful retrograde cannulation of the bile duct. Access is often secured by passing a guidewire into the bile duct and confirmed by injection of radiocontrast material. After successful retrograde cannulation of the bile duct, an incision is made in the biliary sphincter by means of electrocautery through a traction-type papillotome with the cutting wire bowed against the roof of the papilla (Figure 1). ES may be performed using either pure cutting current or blended/coagulation current[18], with no difference in pancreatitis incidence but higher risk of mild bleeding associated with pure cutting current.[40] Size of the stone(s) and papillary anatomy are considered in determining an appropriate length of the sphincterotomy. The length of the sphincterotomy, however, should not extend beyond the duodenal transverse fold.[18]
Although sphincterotomy is usually performed after traditional biliary cannulation, this is not always possible (e.g. stone impaction in the ampulla). In such cases, several alternative methods are available to achieve sphincterotomy. Methods that involve dissection of the papilla to expose the bile duct are collectively known as “precut” sphincterotomy. This can be achieved in the needle-knife precut method by extending a fine cutting wire several millimeters from the catheter tip to unroof the papilla in incremental layers until the bile duct is exposed. In this method, often a small-diameter plastic stent is placed into the pancreatic duct before precutting to protect pancreatic drainage. A less common method of precutting involves wedging of a modified traction-type papillotome into the papillary orifice and using it to make incremental incisions until the bile duct is exposed. Although reported in a systematic review to increase the risk of acute pancreatitis[41], recent studies could not identify any risk factors associated with the development of post-ERCP pancreatitis in patients who underwent precut sphincterotomy by skilled endoscopists.[42, 43] Lastly, a combined percutaneous-endoscopic approach can be performed that involves transhepatic antegrade passage of a guidewire through the bile duct into the duodenum, also known as the rendezvous procedure, which ideally allows the endoscopist to perform sphincterotomy in the standard fashion either at the time of PTC[44] or after a few days of percutaneous biliary drainage.[21, 45]
Roorda_December_11.indd 19 12/13/11 2:11 PM

Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
20� Practical�GastroenteroloGy� •� december�2011
Immediate Post-Procedure ComplicationsThe incidence and type of complications after ES is primarily related to the clinical indication and context for the procedure as well as to the technical skill of the endoscopist.[21] Freeman et al. (1996) demonstrated that age or general medical condition of the patient were not associated with immediate complications.[21]
Two separate large multicenter prospective studies have been performed to investigate complications of ES. In one report, complications were observed in 6% of patients at seven academic medical centers, of which two-thirds were considered to be mild (requiring less than three days of hospital stay).[46] In a large multicenter prospective study by Freeman et al, the most frequent complications were pancreatitis (5.4%) followed by hemorrhage (2.0%), cholangitis (1.0%), acute cholecystitis (0.5%), retroperitoneal or bowel wall perforation (0.3%), and other complications (1.1%) such as cardiopulmonary complications, bile leak, intrahepatic bleeding, and ductal perforation. Independent risk factors for post-procedure complications included two patient-related factors (presence of cirrhosis, and suspected sphincter of Oddi dysfunction) and three technique-related factors (use of precut sphincterotomy, use of combined percutaneous-endoscopic procedure, and difficult bile duct cannulation). The overall risk of complications was not related to the patient’s age, the number of coexisting illnesses, or the diameter of the bile duct. Moreover, endoscopists who performed more than one sphincterotomy per week were found to have lower rates of all complications including severe complications. Rates of complications of ES in patients with bile duct stones or gallstone pancreatitis were similar (8.1% overall) regardless of whether ES was performed before, after, or without cholecystectomy. The overall complication rate was significantly lower in patients who underwent ES within thirty days before or after laparoscopic cholecystectomy.[21]
A systematic review of 15 prospective clinical trials identified risk factors for development of post-ERCP pancreatitis. Significantly higher risk of acute pancreatitis was seen in patients with suspected sphincter of Oddi dysfunction (RR 4.09), female gender (RR 2.23), and with previous pancreatitis (RR 2.46). Two endoscopy-related factors were associated with significantly higher risk of acute pancreatitis: precut sphincterotomy (RR 2.71) and pancreatic injection (RR 2.2).[41]
Long-term ComplicationsLong-term complications following ES include recurrent bile duct stones, papillary stenosis, cholangitis, cholecystitis, and liver abscess.[47] Long-term follow-up studies of ES in management of choledocholithiasis have documented a 4-24% incidence of recurrent biliary problems.[21, 47-53] Stone recurrence is attributed to several risk factors including a dilated bile duct[48, 50, 54], the presence of periampullary diverticulum[48], a gallbladder left in situ[48, 55], presence of brown pigmented stones at the initial ES[54], use of a mechanical lithotripter during treatment[51, 55], and the occurrence of pneumobilia after ES[51, 55]. Additionally, ampullary stenosis and bile duct strictures have been associated with later recurrence of bile duct stones.[56] Stone recurrence also occurs less frequently in patients with acalculous gallbladders than in patients with calculous gallbladders and in patients who have previously undergone cholecystectomy.[55] Routine follow-up is recommended to identify patients at high risk for stone recurrence. Repeat ERCP is considered an effective and safe strategy to manage recurrent CBD stones.[18, 57] Additionally, ES has been found to carry no further risk of malignancy formation (e.g. cholangiocarcinoma) in addition to the risk reported with the use of ERCP in benign disease.[58]
Safety in High-Risk PatientsSafety of ES has been studied in patients with recent acute myocardial infarction[59] as well as in patients with acute obstructive suppurative cholangitis (AOSC) and cirrhosis[60]. Although these patients are at a theoretically increased risk for complications during many invasive procedures, therapeutic ERCP with ES is not absolutely contraindicated after MI or in patients with cirrhosis. ERCP with ES for treatment of symptomatic choledocholithiasis has been safely performed in patients with recent myocardial infarction.[59] In a comparison of ES versus surgical treatment for choledocholithiasis in patients with liver cirrhosis or AOSC, Chijiiwa et al. (1995) demonstrated that ES has lower morbidity rates (24% versus 67%) in AOSC group and lower morbidity rate (22% versus 67%) in the group of patients with liver cirrhosis; however, comparisons between the two treatment approaches did not achieve statistical significance.[60]
(continued on page 22)
Roorda_December_11.indd 20 12/13/11 2:11 PM

ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
22� Practical�GastroenteroloGy� •� december�2011
Outpatient Procedure SafetySame-day discharge after outpatient ES is a common clinical practice with significant cost-savings. A review of a prospective multicenter database of complications by Freeman et al. (1999) concluded that same-day discharge is relatively safe after ES; the study further recommends observation for 6 hours or overnight for patients at higher risk of complications in order to reduce the need for readmission. Five independent risk factors predicted higher risk of complications: suspected sphincter of Oddi dysfunction, cirrhosis, difficult bile duct cannulation, precut sphincterotomy, or combined percutaneous-endoscopic procedure.[61]
Prophylactic Cholecystectomy after ERCPIn most patients with cholelithiasis who undergo ES for choledocholithiasis, prophylactic cholecystectomy is recommended after ductal clearance by ES.[18] A systematic review of multiple randomized controlled trials (662 participants) comparing the outcome of a wait-and-see approach to prophylactic cholecystectomy after ERCP reported that the wait-and-see approach carries higher rates of mortality (78% increased risk), recurrent biliary pain, jaundice or cholangitis, and a higher need for repeat ERCP or other forms of cholangiography. Thirty-five percent in the wait-and-see group eventually required cholecystectomy.[62]
EndOSCOPiC PaPillaRy BallOOn dilatiOn
Role in Current PracticeEndoscopic papillary balloon dilation (EPBD) (Figure 2) of the virgin ampulla has been promoted as an alternative to ES for treatment of bile duct stones. The primary advantage of EPBD compared to ES lies in long-term preservation of sphincter of Oddi function, as it does not permanently ablate the sphincter choledochus.[63, 64] However, because of significantly higher risk of pancreatitis and death as reported in multicenter randomized controlled trials[65] and systematic reviews[66, 67], EPBD has been abandoned in the US and avoided in Britain.[11] It is, however, relatively commonly performed in Japan[68] in treatment of bile duct stones and may be considered to have a role in patients for whom ES is contraindicated such as those with coagulopathy, periampullary diverticulum[69], liver cirrhosis[70], or those with an altered anatomy as in Billroth II gastrectomy patients.[71]
Although routine use of primary EPBD is not recommended, it has continued to garner attention and research as a potential alternative to ES. In a large randomized trial by Fujita, Yasuda, and colleagues (2003), the authors demonstrated comparable complete duct clearance rates for EPBD compared to ES, with overall complication rate of 14.5% in the EPBD group compared to 11.8% in the ES group. However, post-procedure pancreatitis rate was significantly higher in the EPBD group (10.9% versus 2.8%), whereas hemorrhage was exclusively limited to the ES group. No severe pancreatitis or death was seen in the EPBD group.[72] A more recent study by Yasuda et al. (2010) followed the patients in the initial study annually for a median of 6.7 years. This long-term follow-up study demonstrated significantly lower rate of recurrent bile duct stones in the EPBD group (17% versus 8%) and significantly lower overall morbidity in the EPBD group (25.0% versus 10.1%) compared to the ES group in management of common bile duct stones.[68] In an editorial article in the Journal of Gastrointestinal Endoscopy, while acknowledging the data presented by Yasuda et al., the author raises a serious question as to whether the initial “price” of EPBD is too high (serious pancreatitis, death) to justify the reduced long-term biliary complications of EPBD as reported in the Yasuda et al. study.[56]
StOnE ExtRaCtiOn: dORmia BaSkEtS and BallOOn CathEtERS
BackgroundFollowing an adequate sphincterotomy, most stones <10 mm in diameter will pass spontaneously.[73] However, failure to ensure stone removal carries a risk of stone impaction and cholangitis. Therefore, the current practice is to remove the bile duct stones at the time of sphincterotomy. A variety of devices, including wire baskets (Figure 3) and balloon catheters (Figure 4), are available to retrieve stones following a successful sphincterotomy.. Large stones >20 mm in size may be difficult to remove with basket and balloon extraction methods and will require stone fragmentation prior to removal.
Baskets and balloons are available in multiple shapes and sizes and have a variety of characteristics that may be preferentially suited to particular anatomic variations or stone characteristics.[74] The choice of baskets, balloons, or a combination of the two in a
(continued from page 20)
Roorda_December_11.indd 22 12/13/11 2:15 PM
ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
Practical GastroenteroloGy • december 2011 23
ENDOSCOPY: OPENING NEW EYES, SERIES #6
single procedure to retrieve biliary stones depends on the clinical judgment of the endoscopist and may hinge upon factors such as the degree of common bile duct dilation and the number, shape, and configuration of stones present. Although no data exists on the efficacy of balloons versus baskets for uncomplicated CBD stones, balloons are typically the first-line device due to their ease of use, lack of risk of entrapment in the duct, and their utility in occlusion cholangiography.[18] The extraction of bile duct stones using wire baskets and balloon catheters can be repeated in the same ERCP session to remove multiple stones. Multiple stones are recommended to be removed one at a time, starting with the distal-most stone first. Complete duct clearance is recommended to be documented by performing an occlusion cholangiogram.[74]
Wire BasketsA variety of baskets are available in different sizes and configurations that allow engagement of stones varying from 5-30 mm. However, stones >20 mm often cannot be extracted intact and require fragmentation prior to removal. A Dormia basket, shaped as a 4-wire hexagonal basket made of braided steel or nitinol wires, is the most commonly used type of basket. In basket extraction, the closed basket covered by its plastic sheath is inserted into the CBD through the therapeutic channel of the duodenoscope. Dilute contrast is then
injected through the basket to facilitate localization of the stone. Once inside the bile duct, the basket is gently opened above the stone and pulled back with caution while jiggled to engage the stone. Care must be taken to avoid opening of the basket below the stone, which may cause dislodgement of the stone further proximally into the intrahepatic biliary tracts. Once the stone is trapped, the basket is gently closed and withdrawn to the pre-ampullary level without closing the basket tightly. Tight closure of the basket at this time carries the risk of imbedding the basket wires within the stone surface, possibly causing impaction of the basket itself within the biliary ducts. Once the stone is pulled to the pre-ampullary level, traction on the basket catheter allows easy removal of small to medium-sized stones from the CBD. Potential complications of basket extraction include impaction of the basket and stone within the bile duct or at the level of the papilla due to a large stone size and/or inadequate sphincterotomy. Mechanical lithotripsy may be attempted in such cases to fragment the impacted stone and free the basket-stone apparatus.[74]
When compared to balloon catheters, wire baskets provide more effective traction and are therefore more helpful in removal of medium to large-sized stones. However, smaller stones or stone fragments may not be easily engaged by the wires. Baskets designed with smaller mesh size such as the Olympus flower basket
Figure 1. Autotome in Papilla (Courtesy of Boston Scientific). Figure 2. Papillary balloon dilation (Courtesy of George Triadafilopoulos, M.D.).
Roorda_December_11.indd 23 12/13/11 2:16 PM

Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
24� Practical�GastroenteroloGy� •� december�2011
are available that allow easier entrapment of smaller stones.[74]
Balloon CathetersIn this method, a balloon is deflated and inserted via a catheter into the CBD through the sphincterotomy site. The deflated balloon catheter is then advanced proximally in the common bile duct to assume a location “above” the targeted stones. After gently inflating the balloon to the size of the bile duct, the balloon catheter is pulled back through the duodenoscope. Once the stone is pulled to the level of ampulla, traction on the balloon catheter while exerting downward deflection on the duodenoscope tip allows extraction of the stone.[74]
When compared to wire baskets, balloon catheters are better suited for removal of small to medium-sized stones and particularly helpful in removal of intrahepatic stones as the narrow caliber of intrahepatic ducts limit the opening of the wires in the wire basket method.[74]
Technique Details: To Overcome ResistanceIn many instances, simple pulling of the basket or balloon catheter is sufficient to extract the stone. However, in some instances, high resistance is encountered as the stone reaches the ampulla particularly if the sphincterotomy size is smaller than the stone’s diameter. The endoscopist can gain a larger mechanical force by gently pushing the duodenoscope further in the stomach (the “long position”) while creating a right rotational movement by turning the small wheel of the duodenoscope to the right, thereby straightening the bile duct axis of the duodenoscope. Exertion of a traction force along a straight axis in the CBD facilitates the removal of stones while reducing the risk of injury to the papilla or periampullary area. However, straightening of the duodenoscope using the aforementioned method is not without disadvantages. This maneuver may be uncomfortable for the patient and every attempt should be made to shorten the duodenoscope when possible. Moreover, care must be taken during straightening of the duodenoscope to avoid perforation of the opposite duodenal wall by the duodenoscope as bending of the duodenoscope may push against the opposite duodenal wall.[74, 75] Use of nitroglycerin[76] or an infusion of isosorbide[77] to relax the sphincter of Oddi during this process has been studied. The benefit of giving these medications is unclear due to a small study size.
MeChaniCal liThOTRipsyBackgroundIt is estimated that over 80% of all common bile duct stones can be removed effectively with ES and conventional stone extraction methods such as wire baskets and balloon catheters.[24, 78] Large stones >20 mm in size may be difficult to remove with basket and balloon extraction methods alone and typically require stone fragmentation prior to removal.[74] Various techniques have been developed that focus on reduction of stone size to allow for easier extraction. Among these methods, mechanical lithotripsy has become the initial procedure of choice with a ductal clearance rate of 80-90%.[79-83] In cases of unsuccessful mechanical lithotripsy or when predictive factors determine that mechanical lithotripsy is unlikely to succeed, additional methods of lithotripsy are available that fall into two general categories: a) intraductal methods, which include intracorporeal electrohydraulic lithotripsy (EHL) and intracorporeal laser lithotripsy (ILL), and b) extraductal methods, which include extracorporeal shock-wave lithotripsy (ESWL). The following sections provide an overview of various lithotripsy methods.
TechniqueMechanical lithotripsy is accomplished by capturing a stone within a wire basket and crushing it by forceful traction of the basket wires and stone against a metal sheath that is advanced over the basket catheter.[74] Several mechanical lithotripters are available including out-of-the-scope lithotripters and through-the-scope lithotripters.
The out-of-the-scope lithotripters require cutting of the basket handle and removal of the endoscope prior to mechanical lithotripsy. This method is often used on an emergency basis when encountering unexpected impaction of the stone-basket apparatus. After cutting the basket handle to allow removal of the endoscope, the metal sheath of the mechanical lithotripter is inserted over the basket catheter and advanced all the way up to the stone under fluoroscopic guidance. The cut ends of the basket wires are then inserted into the shaft of the crank handle, which is in turn connected to the metal sheath by a Luer lock. Slow cranking of the handle of the lithotripter closes and draws the basket into the metal sheath, crushing the stone against the tip of the metal sheath in the process. Because this method is often used on an emergent basis with standard
(continued on page 30)
Roorda_December_11.indd 24 12/13/11 2:16 PM

ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
30� Practical�GastroenteroloGy� •� december�2011
baskets not designed for lithotripsy, this process must be done slowly to allow time for the basket wires to cut through the stone. Once the stone is fragmented, the apparatus is removed and conventional methods such as basket or balloon extraction can be used to remove the smaller fragments. Commonly used out-of-the-scope mechanical lithotripters are the Soehendra lithotripters (Cook Endoscopy, Winston-Salem, NC).[74]
By comparison, the through-the-scope (TTS) lithotripters share operative principles as described above, but are designed to be used without the need for scope removal. TTS lithotripters are used in a more elective setting to remove large, difficult stones or stones located above a stricture. Commonly used TTS mechanical lithotripters are the Olympus BML systems (Olympus Corporation, Tokyo, Japan) and the Trapezoid basket (Microvasive, Boston Scientific Corporation, Natick, MA). Some models allow contrast injection to better visualize the stone. Both reusable and disposable TTS systems are available. When using reusable TTS systems, it is recommended to remove and inspect the basket after crushing a stone. The goal is to examine the wires as they are often deformed due to stone breakage, necessitating reshaping either by hand or with a pair of hemostats to ensure subsequent success for repeat lithotripsy.[74]
Clinical EfficacySince its description by Demling et al. in 1982[84], mechanical lithotripsy (ML) has been accepted as a reliable method of crushing difficult CBD stones. This method carries a ductal clearance rate of approximately
80-90%, although 20-30% of patients require more than one treatment session.[79-83] Binmoeller et al. (1993) subjected 108 patients with difficult bile duct stones, who had failed extraction by ES and Dormia baskets, to lithotripsy. Thirty-three patients with stones that could not be extracted after entrapment in the Dormia basket underwent ML. Stone fragmentation and bile duct clearance was achieved in 100% of these patients.[24] Cipolletta et al. (1997) achieved complete duct clearance using ML in 84% of patients (136 of 162) who had failed extraction of common bile duct stones by standard techniques. Of these, 119 patients were cleared successfully during the initial attempt, whereas 17 patients required multiple sessions. Failure of ML was mostly due to inability to capture the stone within the basket. No deaths were observed after ML. Procedure-related morbidity occurred when there was inadequate biliary drainage and consisted of three cases of cholangitis (1.8%, all successfully managed with surgery) and two cases of clinical pancreatitis (1.2%, all subsided with conservative therapy).[82]
Complications Thomas et al. (2007) performed a comprehensive, retrospective review of 712 cases (643 biliary and 69 pancreatic) requiring ML of large or resistant CBD stones and/or pancreatic duct stones using a 46-point data questionnaire in 7 tertiary referral centers. Trapped and/or broken baskets was documented as the most frequent complication of biliary and pancreatic ML. Extension of ES and electrohydraulic lithotripsy were the most frequently utilized treatment options.[85]
Predictive Factors of Success and FailureSeveral studies have reported on predictive factors for failure of ML. Garg et al. concluded that the only predictive factor for failure was stone impaction. Stone size was not significant as a predictor for success or failure in the study.[86] Cipolletta et al. concluded (162 patients, retrospective) that stone size was the only outcome predictor, with high risk for lithotripsy failure in those with stones >28 mm in diameter.[82] Lee et al. concluded (retrospective, 134 patients) that stone impaction, stone size > 30 mm, and a stone size to bile duct diameter ratio >1.0 are predictors of failure of ML.[87]
Figure 3. Trapezoid wire-guided retrieval basket (Courtesy of Boston Scientific).
(continued from page 24)
Roorda_December_11.indd 30 12/13/11 2:16 PM

ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
Practical GastroenteroloGy • december 2011 31
ENDOSCOPY: OPENING NEW EYES, SERIES #6
Large Balloon Dilation Comparedto Mechanical LithotripsyIn recent studies, use of large balloon dilation (LBD) following ES has been proposed as an alternative to mechanical lithotripsy following ES in removal of large bile duct stones. Ersoz et al. first reported an 89 to 95 percent stone clearance rate and 15.5% complication rate in 58 patients who underwent ES-LBD after failing endoscopic sphincterotomy and standard basket/balloon extraction.[88]
In a head-to-head comparison between ES-LBD and ES followed by ML, Stefanidis et al. demonstrated in a prospective, randomized, controlled trial that ES followed by LBD is equally effective as ES followed by ML for the removal of large (> 12 mm) bile duct stones and is associated with fewer complications; post-procedure complications were significantly less in patients subjected to ES-LBD at 4.4% compared with 20% in ES-ML; cholangitis developed in none of the patients subjected to ES-LBD compared to 13.3% in ES-ML (p=0.026), while rates of pancreatitis and post-ERCP hemorrhage were similar between the two groups. Among the limitations of ES-LBD mentioned in this study is that dilation balloons greater than 20 mm are not available at this time and, therefore, as the author acknowledges, ES-ML remains the procedure of choice in patients with stones larger than 20 mm.[25]
ExtraCorporEaL ShoCk WavE LithotripSy
role in Current practiceExtracorporeal shock-wave lithotripsy (ESWL) is used to generate shock waves outside the body to fragment bile duct stones. Although recent advancements in ESWL technology have removed the requirement for general anesthesia or placing the patient in a water bath, ESWL continues to have many limitations hindering its widespread use. It is technically challenging and cost-intensive, several treatment sessions are often required, and even then, complete ductal clearance is not as successful as in other methods of lithotripsy.[89] In the following sections and throughout this publication, several studies are cited which provide comparison data between ESWL and other methods of lithotripsy. A dedicated discussion of ESWL is not undertaken in this publication as newer and more effective methods of lithotripsy have diminished the significance of ESWL in treatment of the majority of cases of choledocholithiasis.
LaSEr LithotripSyBackgroundSince its description by Ell et al. in 1988[90], intracorporeal laser lithotripsy (ILL) has been used as an alternative to fragment difficult bile duct stones. The fiber carrying the laser beam can be introduced by the standard peroral retrograde endoscopic route or, if necessary as in patients with Billroth II gastrectomy, the more time-consuming and invasive percutaneous transhepatic route.[91, 92] The underlying principle of intracorporeal laser lithotripsy is the generation of high-energy shock waves capable of fragmenting bile duct stones. The original devices used continuous-wave lasers and were inefficient at fragmentation of stones while unsafe due to a high risk of thermal injury in the surrounding biliary epithelium.[93] The newer generations of laser lithotripters, in contrast, use a pulsed mechanism to deliver small amounts of energy during extremely short pulse durations (microseconds to nanoseconds). Using the pulsed method, power density of the laser waves can reach extremely high levels while only lasting a fraction of a second, thereby reducing the risk of injury to the surrounding tissue.[94]
Figure 4. Extraction balloon (Permission for use granted by Cook Medical Incorporated, Bloomington, Indiana).
Roorda_December_11.indd 31 12/13/11 2:17 PM

Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
32� Practical�GastroenteroloGy� •� december�2011
LimitationsIn clinical practice, aligning the laser-induced shock waves precisely onto the stone surface remains a challenge under direct cholangioscopic and fluoroscopic visualization, and therefore, thermal injury to the surrounding biliary epithelium is a potential risk during the procedure, particularly with increasing exposure time and pulse energies. This risk has been reduced by the advent of stone tissue detection systems (STDS) that provide laser systems with a mechanism to avoid accidental shock wave delivery to the biliary epithelium during laser lithotripsy.[95-97] The optical STDS uses fluorescent reflection from the surface of the target tissue to differentiate the stone from the surrounding tissue and automatically cuts off the laser pulse if tissue other than the stone is detected. Advocates of ILL for treatment of difficult bile duct stones cite its exclusive ability to be coupled to stone tissue detection systems as an advantage over other methods of lithotripsy.
Improvements in the STDS systems, however significant, have not led to widespread use of ILL in the United States. The originally described methods are essentially performed blindly under fluoroscopic guidance only, without visual confirmation of the precise placement of laser beam perpendicular to the stone surface. Newer devices permit adjustment of the laser fiber by providing an acoustic signal, albeit not reliably, which changes as the fiber becomes in contact with the stone or surrounding tissue.[97] Use of mother-baby endoscopy ideally permits visual control during laser lithotripsy, but often necessitates presence of two dedicated and experienced endoscopists.[92, 98] Additionally, the enormous cost of ownership and the high learning curve have led to a slower adoption of this technique in the arsenal of endoscopists for management of difficult bile duct stones. Nevertheless, many European groups use ILL routinely in a safe and efficient manner, as described in the next section.
Clinical EfficacyIn a comparison between ILL and ESWL, Neuhaus et al. (1998) demonstrated in a prospective, randomized trial that ILL with STDS is more effective in the treatment of difficult bile duct stones compared to ESWL in terms of stone clearance rate and treatment duration; an equal number of complications were seen in both treatment groups.[89]
Additionally, data from three European groups who routinely use ILL in treatment of difficult bile
duct stones have demonstrated a bile duct clearance rate in excess of 80%. Ell et al. demonstrated 100% stone fragmentation with 89% of the treatment group remaining completely stone-free after completion of the treatment.[95] Neuhaus et al. showed 97% bile duct clearance rate using laser lithotripsy in patients who had failed conventional endoscopic methods of stone removal; no laser-related complications were observed.[97] Jakobs et al. reported 80% stone-free rate after sole laser therapy; when laser lithotripsy was combined with other methods, the overall success rate was 27/30 (90%); therapy-related mortality was 0%.[99]
Most patients in whom stone clearance is achieved by ILL remain free of stones during long-term follow-up. In a study on 80 patients who underwent successful ILL for difficult bile duct stones, Jakobs et al. reported that only 15 percent of patients had a symptomatic stone recurrence after successful bile duct clearance following ILL. Interestingly, the presence of a bile duct stenosis and a body-mass index below 25 were significantly associated with an increased risk for stone recurrence, whereas a gallbladder in situ, the presence of gallbladder stones, dilation of the bile duct, or a peripapillary diverticulum was not associated with stone recurrence.[100]
In a recent study by Jakobs et al. (2007), the authors called into question whether cholangioscopic guidance is necessary in all cases of endoscopic ILL with STDS for complicated bile duct stones. Between 1992 and 2002, 89 patients with difficult bile duct stones were treated with ERCP and ILL (35% had failed ESWL, 26% had failed EHL). ILL was effective in 79% of 72 patients guided by cholangioscopy and in 82% of 17 cases steered by fluoroscopy. The median number of impulses in the latter was 4,335 whereas there were 1,800 with the former technique. Two parameters influenced the manner of laser guidance. In cases of stones situated above a stricture, cholangioscopic control was more effective (64.7% vs. 31.9%). When the stones were in the distal bile duct, fluoroscopic control was more successful. The authors concluded that in cases of difficult stones in the distal bile duct, ILL under sole fluoroscopic control is very effective and easily performed, whereas cholangioscopic guidance should be recommended only in cases of intrahepatic stones or in patients with stones situated proximal to a bile duct stenosis.[101]
(continued on page 34)
Roorda_December_11.indd 32 12/13/11 2:17 PM

ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
34� Practical�GastroenteroloGy� •� december�2011
ElEctrohydraulic lithotripsy
BackgroundIntracorporeal electrohydraulic lithotripsy (EHL) is a method of stone fragmentation that works by delivering shock waves created by high voltage electric sparks between two isolated electrodes at the tip of a fiber. The electric sparks are delivered in short pulses with a high peak pressure, leading to immediate expansion of the surrounding liquid and induction of spherical shock waves. Oscillating shock waves are magnified when transmitted through a fluid medium such as saline, creating sufficient pressure to fragment the stone. Since shock waves carry a risk of injury to surrounding biliary epithelium, application of EHL is best achieved under direct choledochoscopic and fluoroscopic visualization.[74]
current useEHL is used by most endoscopists via the peroral route to fragment large bile duct stones. Additionally, it is used to fragment stones in cases of basket impaction in the bile duct. EHL can also be performed via the percutaneous route in stones located above a bile duct stricture, intrahepatic stones[102], and in post-pancreaticoduodenectomy patients who cannot undergo the peroral approach. EHL has also been used laparoscopically and intraoperatively.[19, 20] In addition to EHL of bile duct stones, EHL of stones in the gallbladder has been reported using peroral cholecystoscopy.[103]
techniqueIn recent years, an EHL probe is commonly used in the mini-endoscope system such as the single-operator SpyGlass® system (Boston Scientific Corporation, Natick, MA) which will be covered in the next section. Because the peri-fiber space is often almost nonexistent when using large EHL fibers in these mini-endoscope systems, great care must be taken to avoid bending or breaking the EHL fibers when advancing the fiber through the working channel of a choledochoscope. Lubrication of the channel in the mini-endoscope before insertion of the EHL probe, straightening of the mini-endoscope by pushing the endoscope forward to assume a “long” position before advancing the EHL fiber, as well as advancing the EHL fiber while simultaneously pushing water through the mini-endoscope channel, are
some of the methods used to avoid damage to the mini-endoscope channel and the EHL fiber.[104]
Once the EHL probe is outside the mini-endoscope in the desired area of the biliary duct and visualized endoscopically and fluoroscopically, an attempt is made to center the tip of the EHL probe against the stone and advance it as close to the stone as possible without touching the stone and while avoiding any contact with the wall. Firing of the probe tangentially against the center of the stone may allow for better accommodation of the EHL probe in the center of the stone. Touching of the stone with the tip of the EHL probe can be done if necessary but is not advised as this may reduce the life span of the EHL probe. Once the probe is positioned appropriately, EHL is delivered in a fluid medium created by continuous saline irrigation according to a preset power wattage (usually in the range of 70 to 100 watts) via 1 to 2-second pulses or continuous pulsations. Once the EHL is delivered and the stone is fragmented, a cholangiogram is obtained to document evidence of stone fragmentation. The mini-endoscope is subsequently withdrawn and the stone fragments are removed using standard endoscopic methods.[104]
clinical Efficacy and safetyBinmoeller et al. (1993) demonstrated excellent success in stone fragmentation and bile duct clearance using peroral cholangioscopic EHL in patients with stones that could not be engaged in Dormia baskets. Among 65 patients receiving EHL, 64 patients had successful bile duct clearance and only one patient failed the treatment due to inability to insert the cholangioscope into the
Figure 5. SpyGlass System EHL Probe with Biliary Stone (Courtesy of Boston Scientific).
(continued from page 32)
Roorda_December_11.indd 34 12/13/11 2:18 PM

ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
Practical GastroenteroloGy • december 2011 35
ENDOSCOPY: OPENING NEW EYES, SERIES #6
bile duct.[24]Adamek et al. (1996) performed a comparison
of EHL versus ESWL in a total of 125 patients with common bile duct stones in whom conventional endoscopic treatment had failed. EHL was 74% successful (34 of 46 patients) in bile duct clearance, compared to ESWL success rate of 78.5% (62 of 79 patients). Combined treatment including ESWL, EHL, and ILL achieved bile duct clearance in 94% of patient.[105]
Arya et al. (2004) in a retrospective review of 111 patients who underwent EHL under direct cholangioscopic control using a “mother-baby” system demonstrated a stone fragmentation rate of 96% and a final stone clearance rate of 90%; prior to EHL, 99% of patients had undergone ERCP and had failed standard stone extraction techniques. Seventy-six percent of patients required only one EHL session, while 14% required 2 sessions and 10% required 3 or more sessions. All patients with successful stone fragmentation required post-EHL balloon or basket extraction of fragments.[106]
Moon et al. (2004) assessed safety and efficacy of EHL without direct cholangioscopic visualization by using a balloon catheter in 19 patients with extrahepatic bile duct stones that could not be extracted using standard endoscopic methods (e.g., mechanical lithotripsy). An EHL probe with a 3.0F radio-opaque tip was inserted through a balloon catheter. EHL was performed under fluoroscopy until the fragmented stone could be captured in a large basket for ML. Stone fragmentation was 89% successful (17 of 19 patients), and bile duct clearance was 84% (16 of 19 patients). A mean of 1.8 endoscopic sessions was required for complete removal. Additional ML was performed in 56% of the 16 patients. There was no 30-day mortality, while minor complications were noted in 4 patients.[107]
Chen and Pleskow (2007) succeeded in bile duct clearance in 5 of 5 patients who underwent EHL under a Spyglass single-operator peroral cholangioscopy. In this method, EHL was successful in achieving bile duct clearance in three patients who had large stones and one patient who had an impacted stone, all of which had failed prior ERCP and standard methods; the last patient had an intrahepatic bile duct stone that was missed at prior ERCP.[108]
Moon et al. (2009) evaluated the efficacy and safety of treatment of difficult bile duct stones using EHL or
ILL under an ultra-slim endoscope designed to be used as a single-operator, peroral cholangioscopy (POCS) system (GIF-XP260N and GIF-N260 from Olympus, Tokyo, Japan). The following inclusion criteria were applied: failed stone removal using conventional methods (including ML), signs and symptoms of biliary obstruction, dilated common bile duct (>10 mm), and previous complete endoscopic sphincterotomy. The overall success rate of bile duct clearance by lithotripsy under direct POCS by a single endoscopist was 88.9% (16 of 18). Stone fragmentation under direct POCS was successfully performed in nine patients using EHL and in seven patients using LL. The average number of treatment sessions required to complete stone removal was 1.6. ML was performed to complete stone removal in 5 of 18 (27.8%) patients. Procedure-related complications were not observed.[109]
SpyGlaSS® Direct ViSualization SyStem
BackgroundSince its introduction in mid-1970s, peroral cholangioscopy (POCS) has proved to be an integral part of the evaluation and therapy of patients with biliary diseases by allowing a direct intraluminal view of the biliary duct system. Early models of “baby-mother” endoscopes did not achieve widespread use due to costliness, fragility, limited maneuverability, low optical resolution, and the requirement of two trained endoscopists to operate. Newer mini-endoscopes offer improved durability, steering ability, smaller size, and better optics. In 2007, Boston Scientific introduced the SpyGlass® Direct Visualization System with a goal of overcoming the limitations of prior choledochoscopes and simplifying POCS.
As a “single-use, single-operator” device, the SpyScope® catheter consists of four lumens; a) an optic channel through which a SpyGlass® fiber optic probe can pass, b) two separate irrigation channels, and c) a 1.2 mm accessory channel through which the SpyBite® forceps can pass. The SpyScope® catheter is 10 Fr in diameter and features four-way steering capabilities. The SpyGlass® fiber optic probe is a fragile “multiple-use” device that can transmit both light and intra-ductal images and measures 231 cm long and 0.77 mm in outer diameter. Finally, the SpyBite® forceps are “single-use” and have a central spike that minimizes the loss of small biopsies. Additionally, the SpyGlass® system is compatible with EHL and laser lithotripsy
Roorda_December_11.indd 35 12/13/11 2:18 PM

Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
36� Practical�GastroenteroloGy� •� december�2011
for stone fragmentation, allowing direct intra-luminal visualization of these two methods during shock-wave delivery and fragmentation of bile duct stones.
TechniqueAlthough no guidelines have been established, utilization of general anesthesia is recommended when performing ERCP and SpyGlass® as the procedure may last in excess of an hour. Routine pre-operative history and physical, operative risk assessment, laboratory evaluation, and informed consent must be obtained prior to initiation of the procedure. Use of antibiotics with SpyGlass in the form of ciprofloxacin or ampicillin/sulbactam is advocated. No significant body of data exists on additional risks from usage of the SpyGlass® procedure; ERCP with ES risks are mentioned in the previous sections. Thus, post-procedure care in SpyGlass® procedures is similar to post-ERCP care.
In the standard recommended setup, the SpyScope® access and delivery catheter is positioned just below the operating channel of the duodenoscope, which allows the endoscopist to control both the tip deflection wheels of the duodenoscope as well as the knobs of the SpyScope® catheter, using a single hand. Stabilization of both systems is performed with the physician’s other hand. The SpyGlass® system is then introduced into the therapeutic channel of the duodenoscope. The bile duct is cannulated, after a sphincterotomy if needed, and the SpyGlass® direct visualization probe is guided into the biliary tree using the SpyScope® catheter. The SpyScope® catheter and SpyGlass® probe can be maneuvered to the area of interest within the duct, allowing direct visualization of biliary tract stones while delivering shock-waves using EHL (Figure 5) or laser lithotripsy.
Clinical Efficacy and SafetyAlthough the SpyGlass® system has been used with good success rates in diagnostic and therapeutic procedures for bile duct strictures, biliary tract biopsy, stent placement, and management of cystic lesions, the following section focuses on reporting data from clinical trials as it pertains to solely bile duct stone management using the SpyGlass® system.
In a preclinical characterization of the SpyGlass® system, Chen (2007) used a bench simulator to directly compare SpyGlass® to a control fiber-optic trans-endoscopic choledochoscope with two-way deflection. The SpyGlass® system demonstrated statistically
significant higher success rates for accessing all quadrants within the simulated bile duct, both with (RR 2.00, 95% CI 1.56-2.78) and without (RR 1.71, 95% CI 1.39-2.29) biopsy forceps as well as higher success rates for accessing biopsy targets (RR 2.09, 95% CI 1.60-2.91) and performing simulated biopsies (RR 2.94, 95% CI 2.05-4.52).[110]
Chen and Pleskow (2007), in a prospective observational clinical feasibility study, evaluated the clinical utility and safety of the SpyGlass® system for diagnostic and therapeutic procedures in 35 patients. SpyGlass®-directed EHL succeeded in 5 of 5 patients (100%). Of these, three had large stones which had failed to be removed by prior ERCP and standard methods; one patient had an impacted stone, which had failed extraction by ERCP and standard methods; the last patient had an intrahepatic bile duct stone that was missed at prior ERCP. Overall, procedure-related complications occurred in 2 patients (6%) and resolved uneventfully.[108]
Stevens et al. (2007) reported on the use of the SpyGlass® system with EHL in 15 patients with stones that had at least one, and on average three, failed stone removal attempts in prior ERCPs. The mean size of the largest stone per case was 15 mm ± 10 mm. Stone locations were CBD (53% or 8 of 15), cystic duct (13% or 2 of 15), CHD (20% or 3 of 15), and IHD (13% or 2 of 15). There were no technical failures to deliver the fiber and no failures to deliver effective shocks using this single operator system. Stone clearance was achieved in 85% of cases (11 of 13). 61% (8 of 13) of cases cleared with one EHL treatment, whereas 23% (3 of 13) of cases cleared with two EHL treatments. One case was pending a second EHL treatment and one case was a failure because an excessive sludge could not be cleared for the EHL procedure. The mean number of EHL probes needed to complete the stone extraction was one (range 1-2). No complications were reported. The authors concluded that the SpyGlass® cholangioscopy technology provides a safe and effective method for biliary EHL.[111]
Loren et al. (2008) demonstrated 100% complete duct clearance using SpyGlass®-guided EHL or laser lithotripsy in 9 patients with biliary or pancreatic stones (8 biliary, 1 pancreatic). Complete duct clearance in a single session was achieved in all but one case, in which a heavy stone burden necessitated additional sessions. In regards to safety, the authors concluded that
(continued on page 38)
Roorda_December_11.indd 36 12/13/11 2:18 PM

ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
38� Practical�GastroenteroloGy� •� december�2011
the nature and frequency of complications were within the spectrum of those reported with other interventional pancreaticobiliary procedures.[112]
Fishman et al. (2009), in a multicenter retrospective analysis, evaluated the performance, feasibility, and safety of the SpyGlass® system in the management of pancreaticobiliary diseases. The SpyGlass® system was used in 41 patients for biliary stone disease (perorally in 35 patients, and percutaneously in six patients). The SpyGlass® system provided successful therapy in 87% of the patients with stone disease. EHL was used in 38 patients and holmium laser lithotripsy in three patients. Lithotripsy was successful in 90.2% of patients (37 of 41). In five patients, the EHL probe could not be advanced through the SpyScope at the exit of the duodenoscope. In seven patients, the EHL probe could not be accommodated to fully target the stone; however, it produced enough fragmentation to remove the stone. In 87.1% of cases, therapy for stones was completed by lithotripsy in one session either by EHL or holmium laser lithotripsy, with the remaining patients achieving successful ductal clearance in two sessions.[113]
Draganov et al. (2011), in a prospective cohort study, evaluated the feasibility, clinical efficacy, and safety of the SpyGlass® system. In patients with biliary stones, complete stone clearance was achieved in 92.3% of patients (24 of 26). The mean total procedure time (standard ERCP plus SpyGlass®) was 64.3 minutes. Four adverse events (4.8%) were observed; three patients had mild post-ERCP pancreatitis with uneventful recovery; one patient had a periampullary perforation caused by biliary sphincterotomy and recovered with conservative management. Stone clearance was achieved in one session in 84.6% of cases (22 of 26), while two patients required more than one SpyGlass® procedure to achieve bile duct clearance. The first patient had Mirizzi syndrome and required two SpyGlass® sessions to fragment and extract a 10-mm stone impacted in the cystic duct. In the second patient, after two EHL treatments failed to fragment the stone, holmium laser lithotripsy in the SpyGlass® system achieved complete bile duct clearance. One patient (3.9%) required mechanical lithotripsy in addition to cholangioscopy-guided lithotripsy. Of two failed cases, one had Mirizzi syndrome and required surgical removal of the stone after failing SpyGlass®-guided EHL treatment due to inability to target the stone
with the EHL probe. The second patient had successful fragmentation of 25 mm stone with EHL but was lost to follow-up before removing the stone fragments at a separate session. The authors concluded that ERCP-guided cholangioscopy with the SpyGlass® system is technically feasible while not inordinately time-consuming, and can safely achieve bile duct clearance in most patients with difficult biliary stones that have failed prior extraction methods.[114]
Baron and Saleem (2010), in a case report, demonstrated successful hepatic duct stone removal by using the SpyGlass® cholangioscope through a colonoscope to perform EHL under direct endoscopic visualization in a patient with a Roux-en-Y hepaticojejunostomy from an orthotopic liver transplantation 12 years earlier. In contrast to conventional cholangioscopes, the long catheter length of 230 cm provided by the SpyScope® catheter allowed passage of the SpyGlass® system through the therapeutic channel of a colonoscope (CF-Q160AL; Olympus Medical Systems, Center Valley, PA, USA). Prior to this attempt, an internal/external drain was placed but percutaneous stone extraction using lithotripsy was thought not possible, at least not until the percutaneous tract became mature several weeks later.[115] Mou et al. (2010) described another case of peroral cholangioscopy for biopsy in a Roux-en-Y hepaticojejunostomy achieved by using the SpyGlass® system and a standard colonoscope.[116]
Therapeutic capabilities offered by the utilization of the SpyGlass® system have quickly reached impressive levels and have even grown beyond the original applications marketed by the manufacturer. A case report has demonstrated success using the Spyglass® system to cannulate and stent the cystic duct in a surgically high-risk patients in whom decompression of the gallbladder could not be performed by percutaneous transhepatic gallbladder drainage or aspiration. In this case, entry into the cystic duct with a guidewire was not possible until the bile duct was explored using peroral cholangioscopy using the SpyGlass® system.[117] In another report, the SpyGlass® system with EHL was successfully used to fragment gallbladder stones and flush out the remaining small fragments in the gallbladder of a patient with symptomatic gallstone disease, multiple gallstones on transabdominal ultrasound, and Child’s Class C cirrhosis that precluded the possibility of cholecystectomy. Cholecystoscopy with EHL using the SpyGlass® system was offered to
(continued from page 36)
Roorda_December_11.indd 38 12/13/11 2:18 PM
ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
PRACTICAL GASTROENTEROLOGY • DECEMBER 2011 39
ENDOSCOPY: OPENING NEW EYES, SERIES #6
If Coagulopathy, orLiver cirrhosis, orAltered Anatomy, orPeriampullary diverticulum
If Severe Acute Cholangitis, andNo response to medical therapy
If Symptomatic Cholelithiasis, andPlanned LC
Evidence for Choledocholithiasis
Recommend ERCP to Remove Stone(s)
Stone diameter < 10 mm“Non-difficult” stones
Stone diameter > 10 mm “Difficult” stones
Endoscopic Sphincterotomy
Consider EPBD in lieu of ESELEVATED RISK OF SEVERE
PANCREATITIS, DEATH
LCBDE in Skilled Centers 1ST LINE ALTERNATIVE TO ERC
ERCP (pre-, intra-, or post-op)IF PRE-OP, LC RECOMMENDED TO
BE DONE WITHIN 2 WEEKS
Urgent ERCPGOAL: BILIARY DRAINAGE
If Failed Extraction orImpacted Basket
1st Line Therapy:Mechanical Lithotripsy
* EPBD AFTER ES PROMISING 1ST LINE
ALTERNATIVE
2nd Line Therapy:Electrohydraulic Lithotripsy
Laser Lithotripsy
ESWL IS NOT PREFERRED(LOWER RATES OF CLEARANCE)
If Failed Extraction
1st Line Therapy:Balloon Catheters
Wire Baskets
BILE DUCT CLEARANCEIN 85-90% CASES
ADDITIONAL CONSIDERATIONS
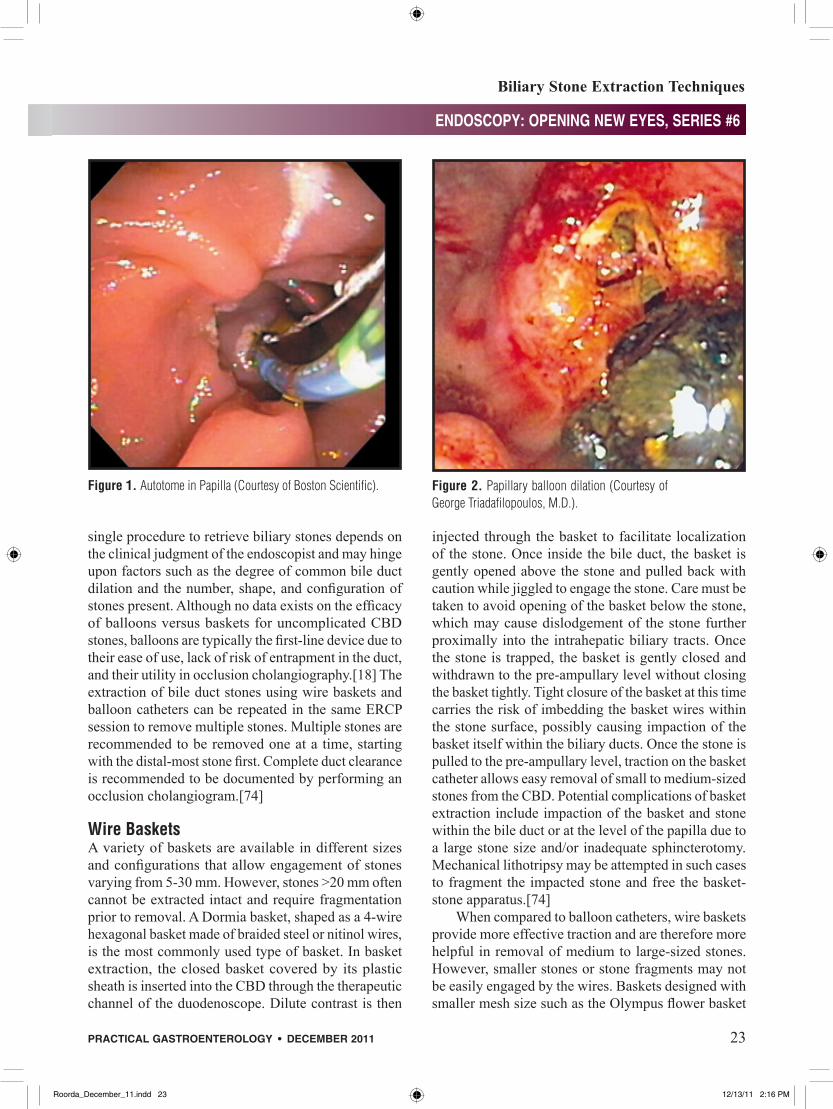
• Multiple stones can be removed in the same ERCP session.• Multiple stones should be removed one at a time, starting with distal-most stone first.• Complete duct clearance is recommended to be documented by an occlusion cholangiogram.• Prophylactic cholecystectomy is recommended in patients who underwent bile duct clearance by ERCP.
Figure 6. Management algorithm.
Roorda_December_11.indd 39 12/13/11 2:19 PM

Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
40� Practical�GastroenteroloGy� •� december�2011
(continued on page 42)
the patient while awaiting liver transplantation with the goal of achieving a gallstone-free and stent-free status. A percutaneous cholecystostomy was not performed because of concerns related to ascites, an abnormal INR, and the risks and discomfort of chronic percutaneous catheter drainage.[103]
Summary
Based on our review of the literature, a management algorithm was constructed (Figure 6). In the treatment of choledocholithiasis, endoscopic sphincterotomy serves as the standard treatment and the prerequisite for basket and balloon extraction as well as mechanical, electrohydraulic, and laser lithotripsy. While most stones <10 mm in size pass spontaneously following endoscopic sphincterotomy, it is current standard practice to attempt stone extraction and clear the bile duct to avoid stone impaction and subsequent risk of cholangitis. For extraction of stones >20 mm in size, mechanical lithotripsy is 80-90% successful, although repeated treatment sessions may be needed in 20-30% of cases to achieve complete bile duct clearance. In cases of unsuccessful mechanical lithotripsy or when predictive factors determine that mechanical lithotripsy is unlikely to succeed, additional methods of lithotripsy are available. Intracorporeal electrohydraulic lithotripsy or laser lithotripsy can be attempted under direct choledochoscopic visualization. The laser lithotripters are far too expensive to encourage widespread implementation, and therefore electrohydraulic lithotripsy has been used more frequently. Comparisons in terms of efficacy, safety, and long-term complications between various methods of lithotripsy are provided in the corresponding sections in this publication.
In the evolution of treatment options for choledocholithiasis, several techniques and devices are certainly worthy of a recap. While much of the data is preliminary, use of large balloon dilation following ES has been shown as a viable and efficient alternative with fewer complications compared to mechanical lithotripsy following ES in removal of large bile duct stones.[25] Although the recent data showed lower rate of overall morbidity and recurrent bile duct stones compared to endoscopic sphincterotomy, the jury is still out on whether endoscopic papillary balloon dilation can safely substitute for endoscopic sphincterotomy in treatment of choledocholithiasis.[56, 68] The SpyGlass® system, introduced in 2007 as a “single-operator” peroral
Practical Points
Standard of Care
• Endoscopicsphincterotomyisthestandardprocedurefortreatmentofbileductstones.
• Sphincterotomyhasan85-90%successrateforbileductclearancewhencombinedwithballoonand/orbasketextractiontechniques.
• Stones>10mminsizeand“difficult”stonesmayrequirestonefragmentationpriortoremovalwithbasketsand/orballoons.Mechanicallithotripsyisthefirstlinemethodoflithotripsy.
• Completeductclearanceisrecommendedtobedocumentedbyanocclusioncholangiogram.
• Short-termcomplicationsofsphincterotomyincludepancreatitis,hemorrhage,cholangitis,acutecholecystitis,andretroperitonealorbowelwallperforation.
• Long-termcomplicationsofsphincterotomyoccurin4-24%ofcasesandincluderecurrentbileductstones,papillarystenosis,cholangitis,cholecystitis,andliverabscessformation.
• Sphincterotomyisnotcontraindicatedandsometimespreferredtosurgeryinhigh-riskpatientssuchasthosewithrecentMI,cirrhosis,oracuteobstructivesuppurativecholangitis.
• Mechanicallithotripsyistheinitialprocedureofchoiceforstonesrequiringfragmentationwithaductalclearancerateof80-90%.
• Ifmechanicallithotripsyfailsorispredictedtofail,intracorporealelectrohydrauliclithotripsy(EHL)isacommonlyutilizedmethodtoachievestonefragmentation.
• AdvantagesofEHLincludeexcellentsuccess,safety,andlowcost.
• Othermethodsoflithotripsyincludelaserlithotripsywithstone-tissuedetectionsystemsandextracorporealshockwavelithotripsy.
Roorda_December_11.indd 40 12/13/11 2:19 PM
ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
42� Practical�GastroenteroloGy� •� december�2011
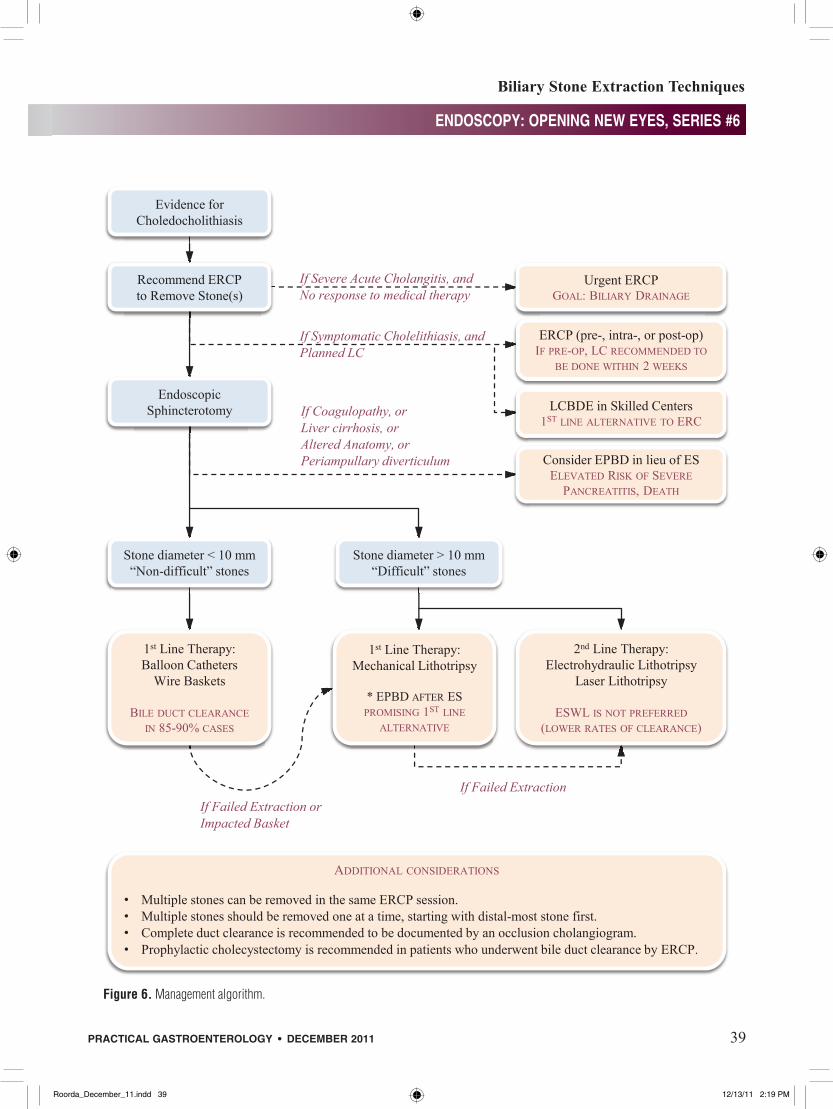
choledochoscope, provides diagnostic and therapeutic capabilities with unrivaled ease of use. Therapeutic capabilities offered by the utilization of the SpyGlass® system have rapidly reached impressive levels and continue to stretch the envelope beyond what seemed achievable only with difficulty just a few years ago with prior conventional choledochoscopes. While admittedly only a first generation device with a few disadvantages in sub-optimal image quality and fragility, SpyGlass® has become a key component in the evaluation of biliary anatomy.n
DisclosureFarid Jalali has no conflict to declare. Andrew Roorda has no conflict to declare. Dr. Sundaram serves on NIH and VA Merit Review Study Sections.
(continued from page 40)
Evolution of Treatment Options for Choledocholithiasis• Comparedtosphincterotomy,endoscopic
papillaryballoondilationhasbeenassociatedwithhigherriskofseriouspancreatitisanddeathbut,basedonpreliminarydata,loweroverallmorbidityandlowerrateofrecurrentbileductstones.
• Largeballoondilationfollowingendoscopicsphincterotomy(EST-LBD)hasbeenproposedasanalternativetomechanicallithotripsyfollowingendoscopicsphincterotomy(EST-ML)inremovaloflargebileductstones.PreliminarydatashowfewercomplicationsandequalefficacycomparedtoEST-ML.
• Laparoscopicexplorationofcommonbileductisequallyefficientinbileductstoneclearanceaspre-andpost-cholecystectomyERPC,withsimilarmortalityandmorbidity,butstatisticallysignificantshorterhospitalstays.
• TheSpyGlass®system,introducedin2007,isasingle-operatorperoralcholedochoscopesystemthathasbeenusedwithgoodsuccessandsafetyindiagnosticandtherapeuticapplicationsforbileductstonemanagement,bileductstrictures,biliarytractbiopsy,stentplacement,andmanagementofcysticlesions.
References
1. Hunter, J.G., Laparoscopic transcystic common bile duct explo-ration. Am J Surg, 1992. 163(1): p. 53-6; discussion 57-8.
2. Robinson, B.L., et al., Selective operative cholangiography. Appropriate management for laparoscopic cholecystectomy. Arch Surg, 1995. 130(6): p. 625-30; discussion 630-1.
3. Petelin, J.B., Laparoscopic common bile duct exploration. Surg Endosc, 2003. 17(11): p. 1705-15.
4. O’Neill, C.J., D.M. Gillies, and J.S. Gani, Choledocholithiasis: overdiagnosed endoscopically and undertreated laparoscopi-cally. ANZ J Surg, 2008. 78(6): p. 487-91.
5. Chang, L., et al., Gallstone pancreatitis: a prospective study on the incidence of cholangitis and clinical predictors of retained common bile duct stones. Am J Gastroenterol, 1998. 93(4): p. 527-31.
6. Chak, A., et al., Prospective assessment of the utility of EUS in the evaluation of gallstone pancreatitis. Gastrointest Endosc, 1999. 49(5): p. 599-604.
7. Liu, C.L., et al., Detection of choledocholithiasis by EUS in acute pancreatitis: a prospective evaluation in 100 consecutive patients. Gastrointest Endosc, 2001. 54(3): p. 325-30.
8. Cohen, M.E., et al., Prediction of bile duct stones and complica-tions in gallstone pancreatitis using early laboratory trends. Am J Gastroenterol, 2001. 96(12): p. 3305-11.
9. Oria, A., et al., Risk factors for acute pancreatitis in patients with migrating gallstones. Arch Surg, 1989. 124(11): p. 1295-6.
10. Frossard, J.L., et al., Choledocholithiasis: a prospective study of spontaneous common bile duct stone migration. Gastrointest Endosc, 2000. 51(2): p. 175-9.
11. Williams, E.J., et al., Guidelines on the management of common bile duct stones (CBDS). Gut, 2008. 57(7): p. 1004-1021.
12. Gonzalez, J.J., et al., Biliary lithiasis in the elderly patient: Morbidity and mortality due to biliary surgery. Hepato-Gastroenterology, 1997. 44(18): p. 1565-1568.
13. Hacker, K.A., C.C. Schultz, and T.S. Helling, Choledochotomy for calculous disease in the elderly. Am J Surg, 1990. 160(6): p. 610-613.
14. Verbesey, J.E. and D.H. Birkett, Common bile duct explora-tion for choledocholithiasis. Surgical Clinics of North America, 2008. 88(6): p. 1315-1328.
15. Rhodes, M., et al., Randomised trial of laparoscopic exploration of common bile duct versus postoperative endoscopic retrograde cholangiography for common bile duct stones. Lancet, 1998. 351(9097): p. 159-161.
16. Cuschieri, A., et al., EAES ductal stone study - Preliminary findings of multi-center prospective randomized trial comparing two-stage vs single-stage management. Surgical Endoscopy-Ultrasound and Interventional Techniques, 1996. 10(12): p. 1130-1135.
17. Martin, D.J., D.R. Vernon, and J. Toouli, Surgical versus endo-scopic treatment of bile duct stones. Cochrane Database of Systematic Reviews, 2006(2).
18. Maple, J.T., et al., The role of endoscopy in the management of choledocholithiasis. Gastrointest Endosc, 2011. 74(4): p. 731-44.
19. Cameron, J.L., Current surgical therapy. 9th ed2008, Philadelphia, PA: Mosby Elsevier. xxxii, 22 plates, 1397 p.
20. Scott-Conner, C.E.H., The SAGES manual : fundamentals of laparoscopy and GI endoscopy1999, New York: Springer. xx, 602 p.
21. Freeman, M.L., et al., Complications of endoscopic biliary sphincterotomy. New England Journal of Medicine, 1996. 335(13): p. 909-918.
22. Prat, F., et al., Prospective controlled study of endoscopic ultrasonography and endoscopic retrograde cholangiography in patients with suspected common-bileduct lithiasis. Lancet, 1996. 347(8994): p. 75-9.
23. Tseng, L.J., et al., Over-the-wire US catheter be as an adjunct to ERCP in the detection of choledocholithiasis. Gastrointest Endosc, 2001. 54(6): p. 720-3.
Roorda_December_11.indd 42 12/13/11 2:19 PM
ENDOSCOPY: OPENING NEW EYES, SERIES #6
Biliary Stone Extraction Techniques
Practical GastroenteroloGy • december 2011 43
ENDOSCOPY: OPENING NEW EYES, SERIES #6
24. Binmoeller,K.F., et al.,Treatmentofdifficult bile-duct stonesusing mechanical, electrohydraulic and extracorporeal shock-wavelithotripsy.Endoscopy,1993.25(3):p.201-206.
25. Stefanidis, G., et al., Large Balloon Dilation vs. MechanicalLithotripsy for the Management of Large Bile Duct Stones:A Prospective Randomized Study. American Journal ofGastroenterology,2011.106(2):p.278-285.
26. Mayumi, T., et al., Results of the Tokyo Consensus MeetingTokyoGuidelines.JHepatobiliaryPancreatSurg,2007.14(1):p.114-21.
27. Bornman,P.C.,J.I.vanBeljon,andJ.E.Krige,Managementofcholangitis.JHepatobiliaryPancreatSurg,2003.10(6):p.406-14.
28. Boender,J.,etal.,Endoscopicsphincterotomyandbiliarydrain-ageinpatientswithcholangitisduetocommonbileductstones.AmJGastroenterol,1995.90(2):p.233-8.
29. Acosta,J.M.,etal.,Earlyductaldecompressionversusconser-vative management for gallstone pancreatitis with ampullaryobstruction:aprospective randomizedclinical trial.AnnSurg,2006.243(1):p.33-40.
30. Neoptolemos,J.P.,etal.,Controlled trialofurgentendoscopicretrogradecholangiopancreatographyandendoscopicsphincter-otomyversusconservative treatmentforacutepancreatitisduetogallstones.Lancet,1988.2(8618):p.979-83.
31. Fan,S.T.,etal.,Earlytreatmentofacutebiliarypancreatitisbyendoscopicpapillotomy.NEnglJMed,1993.328(4):p.228-32.
32. Oria,A.,etal.,Earlyendoscopicinterventionversusearlycon-servativemanagement inpatientswith acutegallstonepancre-atitisandbiliopancreaticobstruction:arandomizedclinicaltrial.AnnSurg,2007.245(1):p.10-7.
33. Folsch, U.R., et al., Early ERCP and papillotomy comparedwith conservative treatment for acute biliary pancreatitis.TheGerman StudyGroup onAcuteBiliary Pancreatitis.NEngl JMed,1997.336(4):p.237-42.
34. Wright,B.E.,etal.,Currentmanagementofcommonbileductstones: is there a role for laparoscopic cholecystectomy andintraoperativeendoscopicretrogradecholangiopancreatographyasasingle-stageprocedure?Surgery,2002.132(4):p.729-35;discussion735-7.
35. deVries,A.,etal.,Conversionrateoflaparoscopiccholecystec-tomyafterendoscopicretrogradecholangiographyinthetreat-mentofcholedocholithiasis:doesthetimeintervalmatter?SurgEndosc,2005.19(7):p.996-1001.
36. Schiphorst, A.H., et al., Timing of cholecystectomy afterendoscopicsphincterotomyforcommonbileductstones.SurgEndosc,2008.22(9):p.2046-50.
37. Ito,K.,H.Ito,andE.E.Whang,Timingofcholecystectomyforbiliary pancreatitis: do the data support current guidelines? JGastrointestSurg,2008.12(12):p.2164-70.
38. Chiang,D.T.andG.Thompson,Managementofacutegallstonepancreatitis:sothestorycontinues.ANZJSurg,2008.78(1-2):p.52-4.
39. Reinders, J.S., et al., Early laparoscopic cholecystectomyimprovesoutcomesafterendoscopicsphincterotomyforcholed-ochocystolithiasis.Gastroenterology,2010.138(7):p.2315-20.
40. Verma, D., A. Kapadia, and D.G. Adler, Pure versus mixedelectrosurgicalcurrentforendoscopicbiliarysphincterotomy:ameta-analysisofadverseoutcomes.GastrointestEndosc,2007.66(2):p.283-90.
41. Masci,E., et al.,Risk factors for pancreatitis following endo-scopic retrograde cholangiopancreatography: a meta-analysis.Endoscopy,2003.35(10):p.830
42. Lee, J.K., et al., Risk for post-ERCP pancreatitis after needleknife precut sphincterotomy following repeated cannulationattempts.JClinGastroenterol,2007.41(4):p.427-31.
43. Testoni, P.A., et al., Precut sphterotomy, repeated cannulationandpost-ERCPpancreatitisinpatientswithbileductstonedis-ease.DigLiverDis,2011.43(:p.792-6.
44. Shorvon, P.J., et al., Percutaneous transhepatic assistance forduodenoscopicsphincterotomy.Gut,1985.26(12):p.1373-6.
45. Dowsett,J.F.,etal.,Encopicbiliarytherapyusingthecombinedpercutaneous and endoscopic technique. Gastroenterology,1989.96(4):p.1180-6.
46. Cotton, P.B., et al., Endoscopic sphincterotomy for stones byexpertsissafe,eveninyoungerpatientswithnormalducts.AnnSurg,1998.227(2):p.201-204.
47. Tanaka, M., et al., Long-term consequence of endoscopicsphincterotomyforbileductstones.GastrointestinalEndoscopy,1998.48(5):p.465-469.
48. Pereira-Lima, J.C., et al.,Long-term results (7 to10years)ofendoscopic papillotomy for choledocholithiasis. Multivariateanalysisofprognosticfactorsfortherecurrenceofbiliarysymp-toms.GastrointestinalEndoscopy,1998.48(5):p.457-464.
49. Tham,T.C.K.,D.L.CarrLocke,andJ.S.A.Collins,Endoscopicsphincterotomyintheyoungpatient:Istherecauseforconcern?Gut,1997.40(6):p.697-700.
50. Costamagna, G., et al., Long-term follow-up of patients afterendoscopic sphincterotomy for choledocholithiasis, and riskfactorsforrecurrence.Endoscopy,2002.34(4):p.273-279.
51. Saito,M.,etal.,Long-termoutcomeofendoscopicpapillotomyforcholedocholithiasiswithcholecystolithiasis.GastrointestinalEndoscopy,2000.51(5):p.540-545.
52. Fujimoto,T.,etal.,Long-termoutcomeofendoscopicpapillot-omyforcholedocholithiasiswithcholecystolithiasis.DigestiveEndoscopy,2010.22(2):p.95-100.
53. Wojtun,S.,etal.,Endoscopicsphincterotomyforcholedocholi-thiasis:Aprospectivesingle-centerstudyontheshort-termandlong-term treatment results in 483 patients. Endoscopy, 1997.29(4):p.258-265.
54. Sugiyama,M.andY.Atomi,Riskfactorspredictiveoflatecom-plicationsafterendoscopicsphincterotomyforbileductstones:Long-term (more than 10 years) follow-up study. AmericanJournalofGastroenterology,2002.97(11):p.2763-2767.
55. Ando,T.,etal.,Riskfactorsforrecurrentbileductstonesafterendoscopicpapillotomy.Gut,2003.52(1):p.116-121.
56. Al-Kawas,F.H.,Long-termoutcomesafterendoscopicmanage-mentofbileductstones:tocutortodilate?Paymenoworpayme later! Gastrointestinal Endoscopy, 2010. 72(6): p. 1192-1194.
57. Sugiyama, M., et al., Endoscopic retreatment of recurrentcholedocholithiasis after sphincterotomy. Gut, 2004. 53(12): p.1856-1859.
58. Stromberg, C., et al., Endoscopic sphincterotomy and riskof malignancy in the bile ducts, liver, and pancreas. ClinicalGastroenterologyandHepatology,2008.6(9):p.1049-1053.
59. Cappell, M.S., Endoscopic retrograde cholangiopancreatogra-phywithendoscopicsphincterotomyforsymptomaticcholedo-cholithiasisafterrecentmyocardialinfarction.AmericanJournalofGastroenterology,1996.91(9):p.1827-1831.
60. Chijiiwa,K.,etal.,Treatmentofchoiceforcholedocholithiasisin patients with acute obstructive suppurative cholangitis andliver-cirrhosis.AmJSurg,1995.170(4):p.356-360.
61. Freeman,M.L.,etal.,Same-daydischargeafterendoscopicbili-arysphincterotomy:observationsfromaprospectivemulticentercomplication study. Gastrointestinal Endoscopy, 1999. 49(5): p.580-586.
62. McAlister,V.C.,E.Davenport,andE.Renouf,Cholecystectomydeferral inpatientswithendoscopic sphincterotomy.CochraneDatabaseofSystematicReviews,2007(4).
63. Macmathuna, P., et al., Endoscopic balloon sphincteroplasty(papillary dilation) for bile-duct stones - efficacy, safety, andfollow-up in 100 patients. Gastrointestinal Endoscopy, 1995.42(5):p.468-474.
64. Komatsu,Y., et al., Endoscopic papillary balloon dilation forthemanagementofcommonbileductstones:Experienceof226cases.Endoscopy,1998.30(1):p.12-17.
65. DiSario, J.A., et al., Endoscopic balloon dilation comparedwith sphincterotomy for extraction of bile duct stones.Gastroenterology,2004.127(5):p.1291-1299.
Roorda_December_11.indd 43 12/13/11 2:19 PM
Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
44� Practical�GastroenteroloGy� •� december�2011
(continued on page 46)
66. Baron, T.H. and G.C. Harewood, Endoscopic balloon dilation of the biliary sphincter compared to endoscopic bily sphinc-terotomy for removal of common bile duct stones during ERCP: a metaanalysis of randomized, controlled trials. Am J Gastroenterol, 2004. 99(8): p. 1455-60.
67. Weinberg, B.M., W. Shindy, and S. Lo, Endoscopic balloon sphincter dilation (sphincteroplasty) versus sphincterotomy for common bile duct stones. Cochrane Database Syst Rev, 2006(4): p. CD004890.
68. Yasuda, I., et al., Long-term outcomes after endoscopic sphinc-terotomy versus endoscopic papillary balloon dilation for bile duct stones. Gastrointestinal Endoscopy, 2010. 72(6): p. 1185-1191.
69. Liao, W.C., et al., Comparison of endoscopic papillary balloon dilatation and sphincterotomy for lithotripsy in difficult sphinc-terotomy. J Clin Gastroenterol, 2008. 42(3): p. 295-9.
70. Park, D.H., et al., Endoscopic sphincterotomy vs. endoscopic papillary balloon dilation for choledocholithiasis in patients with liver cirrhosis and coagulopathy. Gastrointestinal Endoscopy, 2004. 60(2): p. 180-185.
71. Bergman, J., et al., A randomized trial of endoscopic balloon dilation and endoscopic sphincterotomy for removal of bile duct stones in patients with a prior Billroth II gastrectomy. Gastrointestinal Endoscopy, 2001. 53(1): p. 19-26.
72. Fujita, N., et al., Endoscopic sphincterotomy and endoscopic papillary balloon dilatation for bile duct stones: a prospec-tive randomized controlled multicenter trial. Gastrointestinal Endoscopy, 2003. 57(2): p. 151-155.
73. Lauri, A., et al., Endoscopic Extraction Of Bile-Duct Stones - Management Related To Stone Size. Gut, 1993. 32): p. 1718-1721.
74. Baron, T.H., R.A. Kozarek, and D.L. Carr-Locke, ERCP 2008, Philadelphia, PA.: Saunders/Elsevier. xvii, 505 p.
75. Raijman, I., Endoscopic management of bile duct stones: Standard techniques and mechanical lithotripsy, in UpToDate, D.S. Basow, Editor 2011, UpToDate: Waltham, MA.
76. Uchida, N., et al., Endoscopic lithotomy of common bile duct stones with sublingual nitroglycerin and guidewire. American Journal of Gastroenterology, 1997. 92(9): p. 1440-1443.
77. Minami, A., et al., Endoscopic papillary dilation by balloon and isosorbide dinitrate drip infusion for removing bile duct stone. Scandinavian Journal of Gastroenology, 1998. 33(7): p. 765-768.
78. Carr-Locke, D.L., Therapeutic role of ERCP in the manage-ment of suspected common bile duct stones. Gastrointestinal Endoscopy, 2002. 56(6): p. S170-S174.
79. Chung, S.C.S., et al., Mechanical Lithotripsy Of Large Common Bile-Duct Stones Using A Basket. British Journal of Surgery, 1991. 78(12): p. 1448-1450.
80. Shaw, M.J., et al., Results of a multicenter trial using a mechani-cal lithotripter for the treatment of large bile-duct stones. American Journal of Gastroenterology, 1993. 88(5): p. 730-733.
81. Hintze, R.E., A. Adler, and W. Veltzke, Outcome of mechani-cal lithotripsy of bile duct stones in an unselected series of 704 patients. Hepato-Gastroenterology, 1996. 43(9): p. 473-476.
82. Cipolletta, L., et al., Endoscopic mechanical lithotripsy of dif-ficult common bile duct stones. British Journal of Surgery, 1997. 84(10): p. 1407-1409.
83. Chang, W.H., et al., Outcome of simple use of mechani-cal lithotripsy of difficult common bile duct stones. World J Gastroenterol, 2005. 11(4): p. 593-6.
84. Demling, L., K. Seuberth, and J.F. Riemann, A mechanical litho-tripter. Endoscopy, 1982. 14(3): p. 100-101.
85. Thomas, M., et al., Mechanical lithotripsy of pancreatic and biliary stones: Complications and available treatment options collected from expert centers. American Journal of Gastroenterology, 2007. 102(9): p. 1896-1902.
86. Garg, P.K., et al., Predictors of unsuccessful mechanical litho-tripsy and endoscopic clearance of large bile duct stones. Gastrointestinal Endoscopy, 2004. 59(6): p. 601-605.
87. Lee, S.H., et al., How to predict the outcome of endoscopic mechanical lithotripsy in patients with difficult bile duct stones? Scandinavian Journal of Gastroenterology, 2007. 42(8): p. 1006-1010.
88. Ersoz, G., et al., Biliary sphincterotomy plus dilation with a large balloon for bile duct stones that are difficult to extract. Gastrointestinal Endoscopy, 2003. 57(2): p. 156-159.
89. Neuhaus, H., et al., Randomized study of intracorporeal laser lithotripsy versus extracorporeal shock-wave lithotripsy for dif-ficult bile duct stones. Gastrointestinal Endoscopy, 1998. 47(5): p. 327-334.
90. Ell, C., et al., Laserlithotry of common bile-duct stones. Gut, 1988. 29(6): p. 746-751.
91. Brambs, H.J., et al., Percutaneous transhepatic cholangioscopy and dye-laser lithotripsy of bile-duct stones. Zeitschrift Fur Gastroenterologie, 1992. 30(10): p. 748-751.
92. Neuhaus, H., et al., Laser lithotripsy of difficult bile-duct stones under direct visual control. Gut, 1993. 34(3): p. 415-421.
93. Sliney, D.H. and S.L. Trokel, Medical lasers and their safe use1993, New York: Springer-Verlag. xii, 230 p.
94. Razvi, H.A., et al., Intracorporeal lithotripsy with the holmium:YAG laser. Journal of Urology, 1996. 156(3): p. 912-914.
95. Ell, C., et al., Laser lithotripsy of difficult bile-duct stones by means of a rhodamine-6g laser and an integrated auto-matic stone-tissue detection system. Gastrointestinal Endoscopy, 1993. 39(6): p. 755-762.
96. Hochberger, J., et al., Laser lithotripsy of difficult bile duct stones: results in 60 patients using a rhodamine 6G dye laser with optical stone tissue detection system. Gut, 1998. 43(6): p. 823-829.
97. Neuhaus, H., et al., Endoscopic lithotripsy of bile-duct stones using a new laser with automatic stone recognition. Gastrointestinal endoscopy, 1994. 40(6): p. 708-715.
98. Bourke, M.J. and G.B. Haber, Transpapillary choledochoscopy. Gastrointest Endosc Clin N Am, 1996. 6(1): p. 235-52.
99. Jakobs, R., et al., Peroral laser lithotripsy of difficult intrahepatic and extrahepatic bile duct stones: Laser effectiveness using an automatic stone-tissue discrimination system. American Journal of Gastroenterology, 1996. 91(3): p. 468-473.
100. Jakobs, R., et al., Risk factors for symptomatic stone recurrence after transpapillary laser lithotripsy for difficult bile duct stones using a laser with a stone recognition system. European Journal of Gastroenterology & Hepatology, 2006. 18(5): p. 469-473.
101. Jakobs, R., et al., Endoscopic laser lithotripsy for complicated bile duct stones: is cholangioscopic dance necessary? Arquivos de Gastroenterologia, 2007. 44(2): p. 137-140.
102. Yeh, Y.H., et al., Percutaneous trans-hepatic cholangioscopy and lithotripsy in the treatment of intrahepatic stones - a study with 5-year follow-up. Gastrointestinal Endoscopy, 1995. 42(1): p. 13-18.
103. Chen, Y.K., M.T. Nichols, and M.R. Antillon, Peroral cholecys-copy with electrohydraulic lithotripsy for treatment of symp-tomatic cholelithiasis in end-stage liver disease (with videos). Gastrointestinal Endoscopy, 2008. 67(1): p. 132-135.
104. Raijman, I. and S. Escalante-Glorsky, Electrohydraulic litho-tripsy in the treatment of bile and pancreatic duct stones, in UpToDate, D.S. Basow, Editor 2011, UpToDate: Waltham, MA.
105. Adamek, H.E., et al., Management of retained bile duct stones: A prospective open trial comparing extracorporeal and intracor-poreal lithotripsy. Gastrointestinal Endoscopy, 1996. 44(1): p. 40-47.
106. Arya, N., et al., Electrohydraulic lithotripsy in 111 patients: A safe and effective therapy for difficult bile duct stones. American Journal of Gastroenterology, 2004. 99(12): p. 2330-2334.
107. Moon, J.H., et al., Endoscopic treatment of retained bile-duct stones by using a balloon catheter for electrohydraulic lithotripsy without cholangioscopy. Gastrointestinal Endoscopy, 2004. 60(4): p. 562-566.
Roorda_December_11.indd 44 12/13/11 2:20 PM
Biliary Stone Extraction Techniques
ENDOSCOPY: OPENING NEW EYES, SERIES #6
46� Practical�GastroenteroloGy� •� december�2011
(continued from page 44)
108. Chen, Y.K. and D.K. Pleskow, SpyGlass single-operator peroral cholangiopancreatoscopy system for the diagnosis and therapy of bile-duct disorders: a clinical feasibility study (with video). Gastrointestinal Endoscopy, 2007. 65(6): p. 832-841.
109. Moon, J.H., et al., Direct peroral cholangioscopy using an ultra-slim upper endoscope for the treatment of retained bile duct stones. American Journal of Gastroenterology, 2009. 104(11): p. 2729-2733.
110. Chen, Y.K., Preclinical characterization of the Spyglass peroral cholangiopancreatoscopy system for direct access, visualization, and biopsy. Gastrointestinal Endoscopy, 2007. 65(2): p. 303- 311.
111. Stevens, P.D., et al., Biliary stone extraction (BSE) guided by direct visualization using the new SpyGlass (TM) direct visualization system. Gastrointestinal Endoscopy, 2007. 65(5): p. AB96-AB96.
112. Loren, D., et al., Clinical applications of the Spyglass direct visualization system: A multicenter experience. Gastrointestinal Endoscopy, 2008. 67(5): p. AB230-AB230.
Our
36 th Year
REPRINTSSpecial rates are available for
quantities of 100 or more.
For further details email us at:[email protected]
PRACTICAL GASTROENTEROLOGY
113. Fishman, D.S., et al., Management of pancreaticobiliary disease using a new intra-ductal endoscope: The Texas experience. World Journal of Gastroenterology, 2009. 15(11): p. 1353-1358.
114. Draganov, P.V., et al., Prospective evaluation of the clinical util-ity ERCP-guided cholangiopancreatoscopy with a new direct visualization system. Gastrointestinal Endoscopy, 2011. 73(5): p. 971-979.
115. Baron, T.H. and A. Saleem, Intraductal electrohydraulic litho-tripsy by using SpyGlass cholangioscopy through a colo-noscope in a patient with Roux-en-Y hepaticojejunostomy. Gastrointestinal Endoscopy, 2010. 71(3): p. 650-651.
116. Mou, S., I. Waxman, and J. Chennat, Peroral cholangioscopy in Roux-en-Y hepaticojejunostomy anatomy by using the SpyGlass Direct Visualization System (with video). Gastrointestinal Endoscopy, 2010. 72(2): p. 458-460.
117. Barkay, O., L. Bucksot, and S. Sherman, Endoscopic transpap-illary gallbladder drainage with the SpyGlass cholangiopan-creatoscopy system. Gastrointestinal Endoscopy, 2009. 70(5): p. 1039-1040.
Roorda_December_11.indd 46 12/13/11 2:21 PM





![Choledocholithiasis, Ascending Cholangitis, and Gallstone ... · bilirubinate to form biliary sludge, which can aggregate eventually into a gallbladder stone [10]. Black pigment stones](https://img.dokumen.tips/doc/110x75/5e04b56d64882534e3400732/choledocholithiasis-ascending-cholangitis-and-gallstone-bilirubinate-to-form.jpg)