Embed Size (px)
Citation preview

Bernardino Alcázar Lanagrán
GRANADA-2009

ROBERT KOCH 1834-1910
Robert KochRobert Koch
24 MARZO 188224 MARZO 1882
Physiological Society of Berlin Physiological Society of Berlin lectura:lectura:
The etiology of tuberculosisThe etiology of tuberculosis
PREMIO NOBEL Octubre de 1905

Genetic epidemiology of TB
The analysis of the epidemic wave of tuberculosis observed in Europe in the XVIII and XIX centuries, have shown mortality frequencies that reach the 2% per year. In particular, in absence of chemotherapy, a spike can be observed in the first 50-100 years, followed by a slow decline in the next 200-250 years.
These data support the hypothesis, developped by E.R.N. Grigg, that in the first phase of the epidemic wave the most susceptible portion of population has been eliminated (rappresenting up to 20% of the whole population).
Grigg ERN. Am Rev Tuberc 1958; 78: 426-53



Manabe YC, Bishai WR.. Nat Med 2000; 6:
1327–1329.

Historia Natural de Infección por MTB
Innate ImmunityExpression of
IL-1, IL-6, TNF- αααα and ΝΟΝΟΝΟΝΟ
Hipersensibilidad Retardada
Mycobacterium tuberculosisAntigenic expression
(virulance and trascriptional factors,metabolic adaptation to the host etc.)
Specific T-cellresponse
Expression ofIL-2, IFN- γγγγ and TNF-αααα
X%Resuelve la Infección
5% en 2 años puede des,
Enfermedad5% puede des. Enf. A lo largo de su vida

La carga de TB en 2005
1.6 million deaths
in 2005
– 98% of these in
developing world
219,000 deaths
due to TB/HIV
MDR-TB present
in 102 of 109
countries and
settings surveyed,
XDR-TB emerging
8.9 million new
cases in 2005 –
80% in 22 high-
burden countries
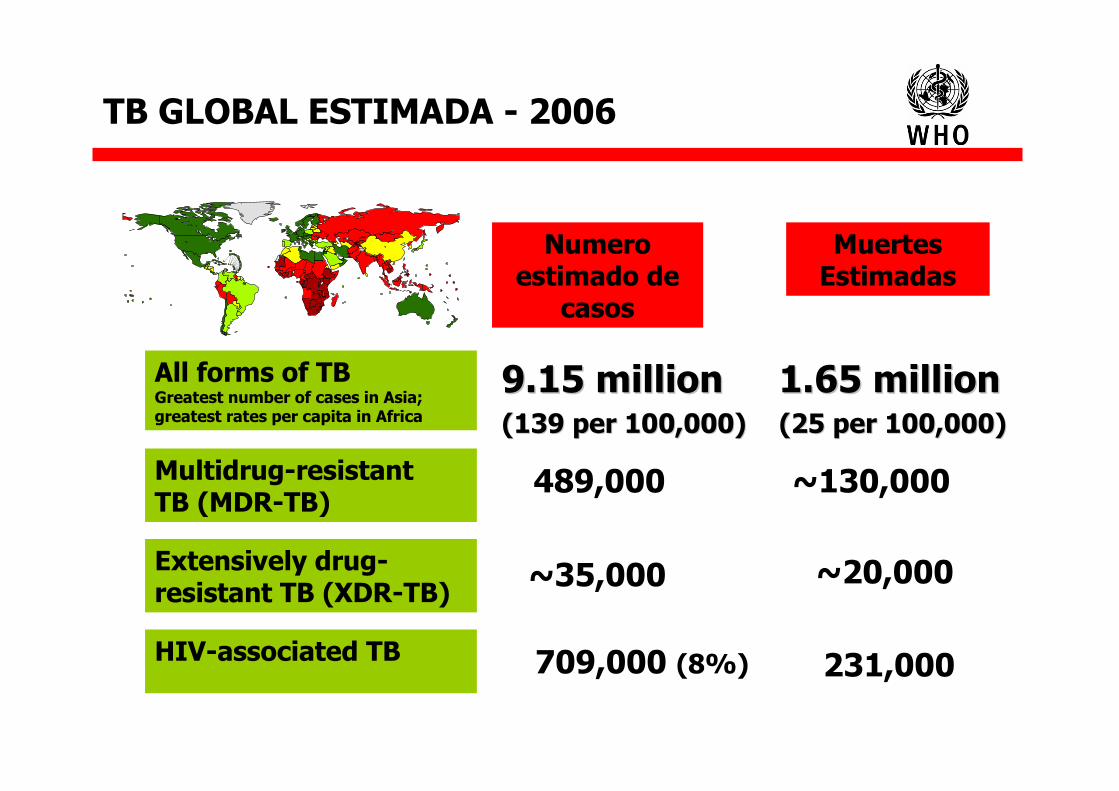
TB GLOBAL ESTIMADA - 2006
Numero estimado de
casos
Muertes Estimadas
1.65 million1.65 million(25 per 100,000)(25 per 100,000)
9.15 million9.15 million(139 per 100,000)(139 per 100,000)
~130,000489,000
All forms of TB Greatest number of cases in Asia; greatest rates per capita in Africa
Multidrug-resistant TB (MDR-TB)
Extensively drug-resistant TB (XDR-TB)
~35,000 ~20,000
HIV-associated TB 709,000 (8%) 231,000

Tuberculosis estimada 2007Tuberculosis estimada 2007Tuberculosis estimada 2007Tuberculosis estimada 2007Tuberculosis estimada 2007Tuberculosis estimada 2007Tuberculosis estimada 2007Tuberculosis estimada 2007
Se estiman 9,27 millones de nuevos casos.
Se estima 1,32 millones de muerte no VIH.
En VIH + 456.000
Pero estas cifras si se comparan con el crecimiento de población.
Asi en 2004 era 142 por 100.000.
En el 2007 son de 139 por 100.00
OMS 24- Marzo-2009

TUBERCULOSIS EN ESPAÑA
• En 1996 Proyecto Multicéntrico de Investigación para TB se situó en 38,48 casos por 100,000,
• Según las declaraciones obligatorias EDO en el año 1997 era de 26,7/100,000. Situándose por debajo de 20 casos/100,000 en el año 2001.

Alveolar macrophage kill MTB: no infection
Infection: MTB released in extra-cellular space, recruitment of mononuclear cells
LATENT INFECTIONLATENT INFECTIONStrong effective cellular responseStrong effective cellular responseContainment of MTB proliferationContainment of MTB proliferation
ACTIVE DISEASEACTIVE DISEASEPoor ineffective immune responsePoor ineffective immune response
Progressive diseaseProgressive disease
REACTIVATIONREACTIVATIONHIVHIV
DrugsDrugsSenescenceSenescence
CoCo--morbiditiesmorbidities
Granuloma formationGranuloma formationSpread to lymph nodes, blood Spread to lymph nodes, blood
and other organsand other organs
Nat Med 2000; 6: 1327-9 modified

INFECCIO
N LATENTE

PUNTOS CLAVESPUNTOS CLAVES
1. Diagnostico de infección latente es de importancia para clinica y evaluación.
2. El método de diagnóstico más utilizado no es adecuado.
3. Son ahora posibles nuevos métodos diagnosticos.

HISTORY OF TUBERCULINHISTORY OF TUBERCULIN
1890189019071907190919091909190919101910192419241926192619341934
1950ies1950ies19581958--656519651965--9595
Koch old tuberculinKoch old tuberculinvon Pirquet scratch testvon Pirquet scratch testMoro patch testMoro patch testMendel intradermal testMendel intradermal testMantoux intradermal testMantoux intradermal testHastings noHastings no--lesion, reactor cattlelesion, reactor cattleCrawford heterologous antigensCrawford heterologous antigensSeibert PPDSeibert PPD--SSWHO surveysWHO surveysUS Navy recruit studyUS Navy recruit studyKorea surveysKorea surveys
www.tbrieder.org

r
C. Mantoux. Intradermo-réaction de la tuberculine. Comptes rendus de l’Académie des sciences.Paris, 1908; 147: 355-357

MANTOUX
Lectura a las 72 horas
POSITIVO > 5 mms

INFECCION TUBERCULOSA
En España se recomienda el derivado proteico purificado (PPD) de la tuberculina PPD- RT 23 con Tween 80, a dosis de 2 UT en 0,1 ml que es bioequivalente a la dosis de 5 UT de tuberculina de patrón internacional PPD S


Tuberculin skin test
• False Positives– People who have received the BCG vaccine
will show up positive– People exposed to mycobacteria in
environment will show up positive
• False Negatives– skin reaction is a very crude measure:
• Small responses not picked up (real problem in immunosuppressed patients)
• In active disease (only 75-90% sensitivity, worse in immunosuppressed)
Berlin, October 4th, 2008

Diagnostico de Infección latente
Tuberculosis Coalition for Technical Assistance. International Standards for Tuberculosis Care (ISTC). The Hague, TuberculosisCoalition for Technical assistance, 2006.


Pai M et al. Lancet Infect Dis 2004

Lalvani, A. Chest 2007;131:1898-1906
Diagrammatic representation of TST, ELISpot, and EL ISA for diagnosing M tuberculosis infection


infección tiempo
T cells
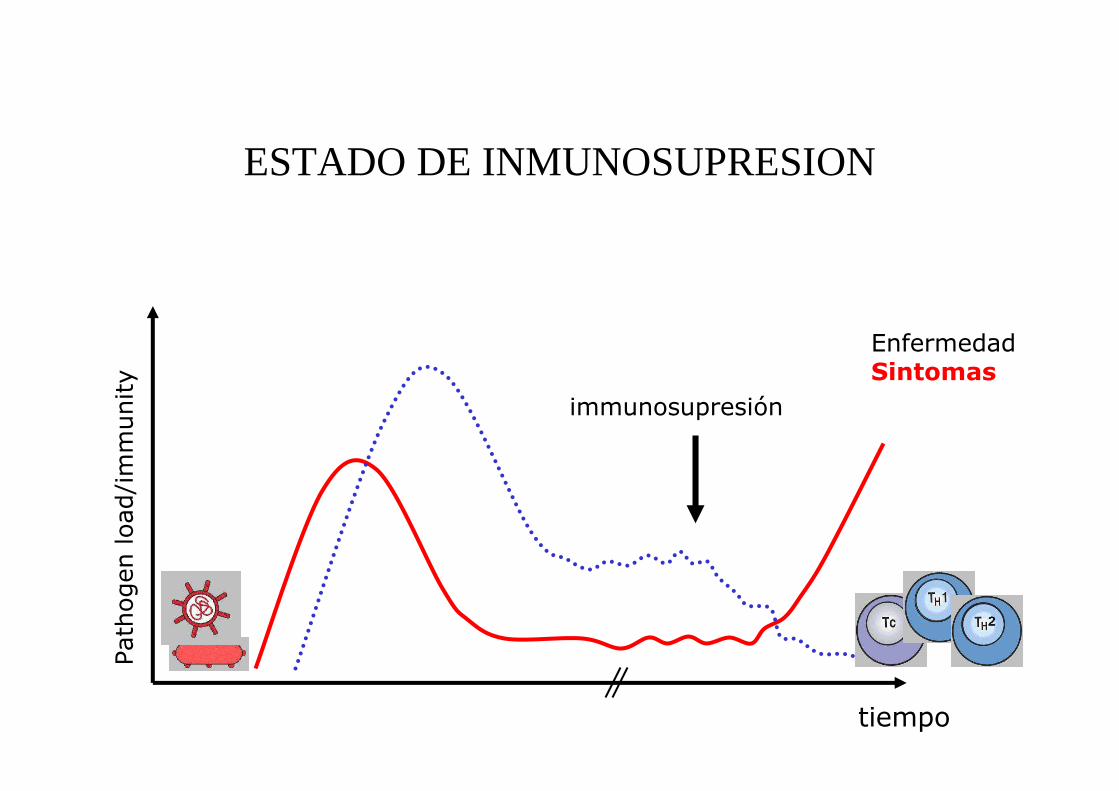
Inmunidad celular específica en infecciones persistentesPathogen load/immunity
equilibrio

immunosupresión
EnfermedadSintomas
ESTADO DE INMUNOSUPRESION
tiempo
Pathogen load/immunity

QuantiFERONQuantiFERON--TB Gold TB Gold In TubeIn Tube

TT--SPOT.SPOT.TBTB

ARE IGRA ARE IGRA DIFFERENT FROM DIFFERENT FROM
TST?TST?TT--SPOT.SPOT.TBTB QuantiFERONQuantiFERON--TBTB Tuberculin skin testTuberculin skin test
Antigens ESATESAT--6 + CFP106 + CFP10 ESATESAT--6 + CFP10 (TB7.7)6 + CFP10 (TB7.7) PPDPPD
Positive internal control YesYes YesYes NoNo
Uniformity of methods and reagents
YesYes YesYes NoNo
Potential for boosting effect in repeated tests
NoNo NoNo YesYes
Need for return visit NoNo NoNo YesYes
Time required for results 1616--20 hrs20 hrs 1616--24 hrs24 hrs 4848--72 hrs72 hrs
Test setting In vitroIn vitro In vitroIn vitro In vivoIn vivo
Test interpretationObjectiveObjective
(instrument(instrument--based)based)ObjectiveObjective
(instrument(instrument--based)based)SubjectiveSubjective
(operator(operator--based)based)
Richeldi L, AJRCCM 2006

5-10% every year
>30%lifetime
HIV+HIV+
5% first 2 years
<10%lifetime
RISK OF PROGRESSING TO ACTIVE TB ONCE LATENTLY RISK OF PROGRESSING TO ACTIVE TB ONCE LATENTLY INFECTED AND INFECTED AND NOTNOT TREATEDTREATED
Latent TB infection

Alveolar macrophage kill MTB: no infection
Infection: MTB released in extra-cellular space, recruitment of mononuclear cells
LATENT INFECTIONLATENT INFECTIONStrong effective cellular responseStrong effective cellular responseContainment of MTB proliferationContainment of MTB proliferation
ACTIVE DISEASEACTIVE DISEASEPoor ineffective immune responsePoor ineffective immune response
Progressive diseaseProgressive disease
REACTIVATIONREACTIVATIONHIVHIV
DrugsDrugsSenescenceSenescence
CoCo--morbiditiesmorbidities
Granuloma formationGranuloma formationSpread to lymph nodes, blood Spread to lymph nodes, blood
and other organsand other organs
Nat Med 2000; 6: 1327-9 modified

TUBERCULOSIS ENFERMEDAD

TUBERCULOSIS ENFERMEDAD

CURSO CLINICO.El COMIENZO
• acquired through inhalation
• engulfed by lung dendritic cells and
macrophages
• migration to lymph node and activation of T cells
• innate immune response / Th1 response result in
granuloma formation
• Th1 = delayed type hypersensitivity
• CD4 T cells act through secretion of IFN-gamma
that activates macrophages
• granuloma formation is important for infection
control and requires balances cytokine
expression
Salgame, Curr Op Immunol, 2005
immunosupresión
EnfermedadSintomas
ESTADO DE INMUNOSUPRESION
tiempo
Pathogen load/immunity

CURSO CLINICO
• development of progressive disease or latency
• MTB persists in macrophage phagosomes by
interfering with with membrane trafficing and
phagolysosome formation
• MTB kill macrophages
• Latency is supported also by specific latency
genes, under hypoxic conditions
• Reactivation• HIV / AIDS (CD4)• end stage renal disease• diabetes• lymphoma• Cortcosteroid• anti-TNF-therapy
LATENCIA
ENFERMEDAD


• « L’examen crucial est représenté par la recherche de bacilles dans l’expectoration. …on est frappé combien peu souvent on a recours à cet examen dans la pratique courante. Pourtant, il est simple... »
E. Arnold, Le diagnostic de la tuberculose, 1944
WHO targets
• ≥70% detection of infectious TB• >85% cured/completed
World Health Organization. Treatment of tuberculosis. Guidelines for National Programmes. WHO report 2003. Document WHO/CDS/TB 2003/313. Geneva, WHO, 2003

PAPEL IMPORTANTE DEL BACTERIOLOGPAPEL IMPORTANTE DEL BACTERIOLOGÍÍAA


Sputum-ZN stain
Esputo-auramina

Hoy aHoy aúún se utiliza:n se utiliza:
El numero de El numero de GaffkyGaffky --

Factores que tienen influencia al escoger el tratamiento
• Localización de la enfermedad.• Resultados Bacteriologicos • Riesgo de tratamiento anteriores para
resistencia.• Posibles efectos secundarios
interreacciones• Drogas disponibles.

La tinción de los bacilos va ligada a los ácidos micólicos de la pared micobacteriana, y éstosestán presentes en el resto de las micobacterias y no se pierden cuando el bacilo muere.

Mycobacterium tuberculosis (MTB)
24 h
DIASSemanas



Rifampicin
Ciprofloxacin
Liquefaction & decontamination in
transport medium at room temperature
MDR
SUSCEPTIBLE
Direct application of 2 drops to selective thin layer agar for incubation in room air for MDRTB testing & XDRTB screening
Color growth detection & microscopy
confirmation of morphology
MDR-XDRTB Color Test for Regional Labs*
Detection Isoniazid
Biosafety similar to sputum microscopy because sputum is smeareddirectly onto the plate which is then permanently double-sealed until autoclaving
1 2 3
*Carlton Evans, Welcome Trust, Peru

Robert KochRobert Koch
Koch RT. A further communication on a remedy for tuberculosis. BMJ
1890; 2: 1193-5
“I assume that the material will be valuable diagnostic
measure in the future. It will become possible to diagnose
questionable cases of phthisis even in those cases where
bacilli cannot be detected in the sputum.”

GenoType® MTBDR plustest procedure
1) DNAExtractionFrom NALC/NaOHProcessed sputum
2) Amplificationby PCR
3) HybridizationReverse hybridization ofamplified nucleic acidsto specific DNA probes
bound on strips
4) Evaluation



The fall of the wall, Berlin 1989The fall of the wall, Berlin 1989

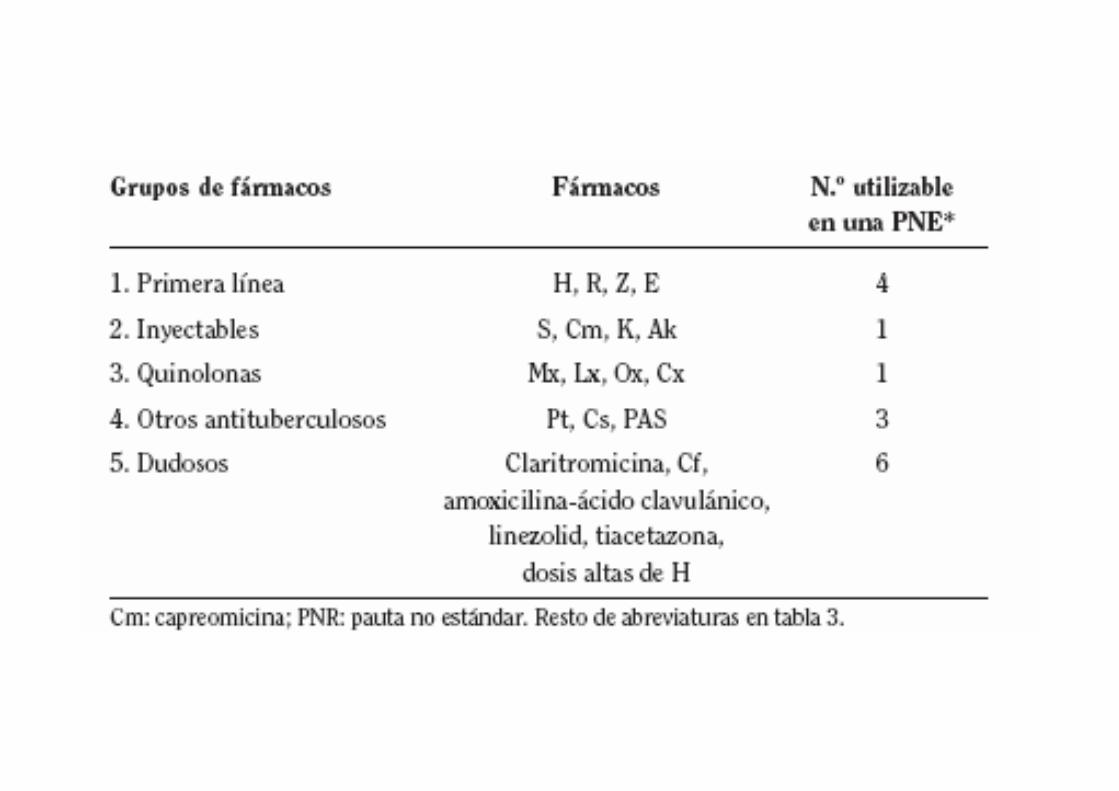
1st-line agents
•INH
•RIF
•PZA
•EMB
Injectable agents
•SM
•KM
•AMK
•CM
Fluoroquinolones
•Cipro
•Oflox
•Levo
•Moxi
•Gati
2nd-line Oral agents
"3rd-line" agents•ETA/PTA
•PASA
•CYS
Not routinely recommended, efficacy unknown, e.g., amoxacillin/clavulanic acid, clarithromycin, clofazamine,
XDR= HR + 1 FQ + 1 Injectable (KM or AMK or CM)

MDR-TB among new cases 1994-2007
< 3%3-6 %> 6 %No data
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO 2006. All rights reserved
* Sub-national coverage in India, China, Russia, Indonesia.

En España se ha producido un aumento de población, pero hemos alcanzado el 12%de población nacida fuera de nuestro país,


Czech Rep.
The boundaries and names shown and the designations used on thismap do not im
ply the expression of any opinion
whatsoever on the part o
f the WHO concerning the legal status ofany country, te
rritory, city or area or of its
authoritie
s, or concerning the delimitation of its
frontiers or boundaries. D
otted lines on maps represent approximate
border lin
es for w
hich there may not yet be full agreement.
WHO 2005. All rig
hts reserved
Ecuador
Georgia
Argentina
Bangladesh
Germany
Rep of Korea
Armenia
Russian Fed.
South Africa
Portugal
Latvia
Mexico
Peru
USA
Brazil
UK
Sweden
Thailand
Chile
Based on information provided to WHO Stop TB Department - May 2008
Spain
China, Hong Kong SAR
France
Japan
Norway
Canada
Italy
Netherlands
Estonia
Lithuania
Ireland
RomaniaIsrael
Azerbaijan
Poland
Slovenia
India
Australia
Mozambique
Vietnam
Ukraine
Moldova
Philippines
Botswana
Nepal
Islamic Rep. of Iran
Lesotho
Swaziland
Namibia
Countries with confirmed XDR-TB cases as of June 2008
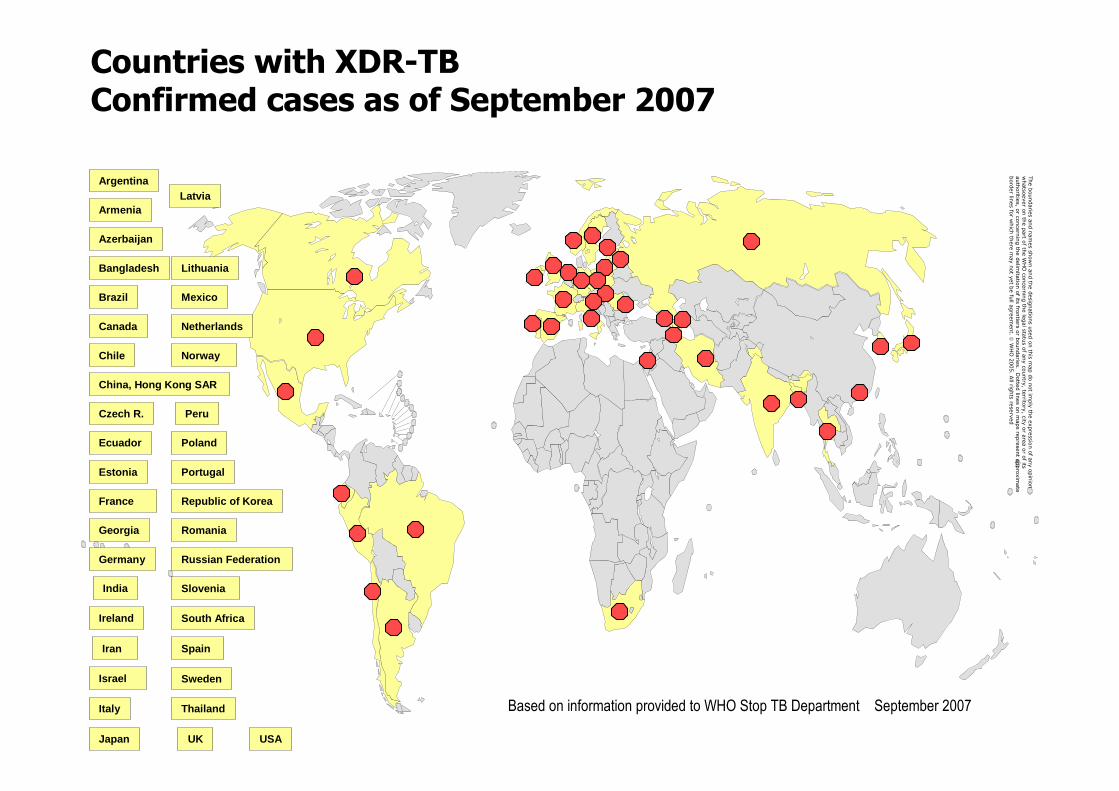
Countries with XDR-TB Confirmed cases as of September 2007
Czech R.
The boundaries and names shown and the designations used on thismap do not im
ply the expression of any opinion
whatsoever on the part o
f the WHO concerning the legal status ofany country, te
rritory, city or area or of its
authoritie
s, or concerning the delimitation of its
frontiers or boundaries. D
otted lines on maps represent approximate
border lin
es for w
hich there may not yet be full agreement.
WHO 2005. All rig
hts reserved
Ecuador
Georgia
Argentina
Bangladesh
Germany
Republic of Korea
Armenia
Russian Federation
South Africa
Portugal
Latvia
Mexico
Peru
USA
Brazil
UK
Sweden
Thailand
Chile
Based on information provided to WHO Stop TB Department September 2007
SpainIran
China, Hong Kong SAR
France
Japan
Norway
Canada
Italy
Netherlands
Estonia
Lithuania
Ireland
Romania
Israel
Azerbaijan
Poland
Slovenia India

Tuberculosis resistente a drogas
Migliori GB,. Eur Respir J 2007;29:423–427

TERAPIA EN EL TIEMPO viejas armas TERAPIA EN EL TIEMPO viejas armas
pueden ser pueden ser úútiles en XDRtiles en XDR
First sanatorium First sanatorium Germany, 1857Germany, 1857 First Dispensary, First Dispensary,
Scotland, 1897Scotland, 1897
Koch, Mtb,Koch, Mtb,18821882
Drugs, 1945Drugs, 1945--19621962
MMR,1950MMR,1950--19801980
Fox:Ambulatory treatment, 1968Fox:Ambulatory treatment, 1968
Styblo model, 1978Styblo model, 1978
DOTS, 1991DOTS, 1991
sanatoriasanatoria Outbreak Management,Outbreak Management,
Risk Group ManagementRisk Group Management
screeningscreening
BCG vaccinationBCG vaccination
drug therapydrug therapy
SocioSocio--economic improvementeconomic improvement
Pneumotorax, Italy, 1907Pneumotorax, Italy, 1907


EUROPEAN LUNG WHITE BOOK, 2003

WHO 2007
GlobalAllianceagainstchronicRespiratoryDiseases

I have called this principle, by whicheach slight variation, if useful, is preserved, by the term Natural Selection.
— Charles Darwin from "The Origin of Species"
Charles DarwinNaturalist1809 -1882

Europe
439 000 (5.0%)439 000 (5.0%)
Africa
2.4 m (26.9%)2.4 m (26.9%)
Eastern Mediterranean
634 000 (7.2%)634 000 (7.2%)South-East Asia
3.1 m (34.8%)3.1 m (34.8%)
The Americas
370 000 (4.2%)370 000 (4.2%)
The Western Pacific
1.9 m (21.9%)1.9 m (21.9%)
Estimated new TB (all) cases (2003)
Source: WHO. WHO report 2005: global tuberculosis control; surveillance, planning, financing. Geneva: WHO (WHO/HTM/TB/2005.349)
� 8.8 million new cases (80% in 22 countries, 30% in India and China)
� 1.7 million deaths (98% in developing world)
� 229 000 deaths due to TB/HIV
� > 0.4 million MDR-TB cases (in new or previously treated)

GRACIAS