Embed Size (px)
Citation preview

Benign Prostatic Benign Prostatic Hyperplasia (BPH)Hyperplasia (BPH)
JOSE RIZALITO C. CATIPAY, M.DJOSE RIZALITO C. CATIPAY, M.DAssociate ProfessorAssociate Professor
SWU-MHAM College of MedicineSWU-MHAM College of Medicine

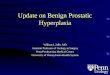
Definition of BPHDefinition of BPH
Benign enlargement of the prostate Benign enlargement of the prostate gland that results from varying degrees gland that results from varying degrees of hyperplasia of glandular and / or of hyperplasia of glandular and / or fibromuscular elementsfibromuscular elements

Natural history of BPHNatural history of BPH
Remain stable
Improved withtime
Worseningsymptoms
55%30%
15%

Prevalence. . .Prevalence. . .
40 - 49 y.o 50 - 59 y.o 60 y.o. +
14% 24%
43%

Pathophysiology. . .Pathophysiology. . .
As BPH progresses, the hyperplastic As BPH progresses, the hyperplastic tissue increasingly encroaches on the tissue increasingly encroaches on the prostatic urethraprostatic urethra
Prolonged outflow obstruction results in:Prolonged outflow obstruction results in:
-- Bladder stone formationBladder stone formation
- Deterioration of renal function- Deterioration of renal function
- Formation of bladder diverticula- Formation of bladder diverticula
- UTI & pyelonephritis- UTI & pyelonephritis





Diagnosis of BPHDiagnosis of BPHBasic evaluation of BPHBasic evaluation of BPH
- Detailed history & symptom assessment- Detailed history & symptom assessment
- P.E., Including D.R.E.- P.E., Including D.R.E.
- U/A- U/A
- Measurement of serum creatinine- Measurement of serum creatinine
- Measurement of serum PSA - optional - Measurement of serum PSA - optional

Diagnosis of BPH. . .Diagnosis of BPH. . .Obstructive SxObstructive Sx hesitancyhesitancy weak streamweak stream straining to pass urinestraining to pass urine prolonged micturitionprolonged micturition urinary retentionurinary retention feeling of incomplete feeling of incomplete
bladder emptying bladder emptying
Irritative SxIrritative Sx urgencyurgency frequencyfrequency nocturianocturia urge incontinenceurge incontinence

Diagnosis of BPH. . .Diagnosis of BPH. . .
The International Prostate Symptom Score ( I- PSS )The International Prostate Symptom Score ( I- PSS )
- - based on answers to the seven questions based on answers to the seven questions concerning urinary symptoms, designed for self concerning urinary symptoms, designed for self administrationadministration
patients can be tentatively classified as follows:patients can be tentatively classified as follows:
0 - 7 = mildly symptomatic0 - 7 = mildly symptomatic
8 - 19 = moderately symptomatic8 - 19 = moderately symptomatic
20 - 35 = severely symptomatic20 - 35 = severely symptomatic


Treatment OptionsTreatment Options
Watchful waitingWatchful waiting
Alpha-Blocker TherapyAlpha-Blocker Therapy
5 alpha-reductase Inhibitor Therapy5 alpha-reductase Inhibitor Therapy
PhytotherapyPhytotherapy
SurgerySurgery
Minimally Invasive TherapiesMinimally Invasive Therapies

Surgical management of BPHSurgical management of BPHIndications for surgery in patients with BPHIndications for surgery in patients with BPH
refractory retention refractory retention
recurrent UTI / hematuriarecurrent UTI / hematuria
bladder stones sec. to BPHbladder stones sec. to BPH
renal insufficiency due to BPHrenal insufficiency due to BPH
large bladder diverticulumlarge bladder diverticulum
patient preferencepatient preference



Minimally Invasive Treatment Minimally Invasive Treatment OptionsOptions
prostatic stents (temporary and permanent)prostatic stents (temporary and permanent) balloon dilatationballoon dilatation electrovaporizationelectrovaporization laser ablationlaser ablation
- transurethral laser incision of the prostate- transurethral laser incision of the prostate (TULIP) (TULIP) - endoscopic laser ablation of the prostate (ELAP)- endoscopic laser ablation of the prostate (ELAP) - interstitial laser therapy- interstitial laser therapy
transurethral needle ablation (TUNA)transurethral needle ablation (TUNA) transurethral microwave thermotherapy (TUMT)transurethral microwave thermotherapy (TUMT)

Prostate CancerProstate Cancer

Annual incidence*Annual incidence*
- 100/100,000 between 50-60 years old- 100/100,000 between 50-60 years old - - 200 to 300/100,000 between 60 and 70 years 200 to 300/100,000 between 60 and 70 years
- 179,500 cases in 1999 - 179,500 cases in 1999
Annual incidence*Annual incidence*
- 100/100,000 between 50-60 years old- 100/100,000 between 50-60 years old - - 200 to 300/100,000 between 60 and 70 years 200 to 300/100,000 between 60 and 70 years
- 179,500 cases in 1999 - 179,500 cases in 1999
IncidenceIncidence

Prostatic Carcinoma: Risk Factors
3 risk factors are well-established:3 risk factors are well-established:1. 1. ageage
2.family history2.family history
3. race3. race
3 risk factors are well-established:3 risk factors are well-established:1. 1. ageage
2.family history2.family history
3. race3. race

• Digital rectal examinationDigital rectal examination
• PSAPSA
• Ultrasonography (TRUS)Ultrasonography (TRUS)
Histological confirmationHistological confirmation
• Digital rectal examinationDigital rectal examination
• PSAPSA
• Ultrasonography (TRUS)Ultrasonography (TRUS)
Histological confirmationHistological confirmation
Diagnostic Methods Diagnostic Methods for Prostatic Carcinomafor Prostatic Carcinoma


Localized prostatic carcinoma
1.1. Watchful waiting onlyWatchful waiting only
2. Curative surgery: 2. Curative surgery:
radical prostatectomyradical prostatectomy
3. External beam radiation therapy3. External beam radiation therapy
4. Brachytherapy4. Brachytherapy
5. Cryotherapy5. Cryotherapy

Localized prostatic carcinoma: curative surgery
(RADICAL PROSTATECTOMY)
•• • Excision of the prostate, seminal vesiclesExcision of the prostate, seminal vesicles and the ampulla of the ductus deferens and the ampulla of the ductus deferens


The TNM classification The TNM classification for prostatic carcinoma (1997)for prostatic carcinoma (1997)• T1T1 Normal prostate on digital rectal examination, Normal prostate on digital rectal examination,
not visible on imaging not visible on imaginga: < 5% surgical specimena: < 5% surgical specimenb: > 5% surgical specimenb: > 5% surgical specimenc: detected by biopsyc: detected by biopsy
• T2T2 Tumor limited to the prostate Tumor limited to the prostatea: one lobe affecteda: one lobe affectedb: two lobes affectedb: two lobes affected
• T3T3 Tumor extended outside the capsule Tumor extended outside the capsulea: extra-capsular extensiona: extra-capsular extensionb: extension to seminal vesiclesb: extension to seminal vesicles
• T4 T4 Invasion of neighbouring organ or fixated tumor Invasion of neighbouring organ or fixated tumor (bladder neck, sphincter, rectum, pelvic wall)(bladder neck, sphincter, rectum, pelvic wall)
• T1T1 Normal prostate on digital rectal examination, Normal prostate on digital rectal examination, not visible on imaging not visible on imaging
a: < 5% surgical specimena: < 5% surgical specimenb: > 5% surgical specimenb: > 5% surgical specimenc: detected by biopsyc: detected by biopsy
• T2T2 Tumor limited to the prostate Tumor limited to the prostatea: one lobe affecteda: one lobe affectedb: two lobes affectedb: two lobes affected
• T3T3 Tumor extended outside the capsule Tumor extended outside the capsulea: extra-capsular extensiona: extra-capsular extensionb: extension to seminal vesiclesb: extension to seminal vesicles
• T4 T4 Invasion of neighbouring organ or fixated tumor Invasion of neighbouring organ or fixated tumor (bladder neck, sphincter, rectum, pelvic wall)(bladder neck, sphincter, rectum, pelvic wall)


Advanced prostatic carcinoma
Palliative treatment
Based on androgen deprivationand symptomatic measures
Castration:• surgical• pharmacologic
Anti-androgens combined or not with castration

Advanced prostatic carcinoma: Advanced prostatic carcinoma: symptomatic treatmentsymptomatic treatment
Radiation therapyRadiation therapy Pharmacological treatment of painPharmacological treatment of pain
• biphosphonates• biphosphonates
• • narcotic analgesicsnarcotic analgesics
Surgery in the event of:Surgery in the event of:
• • vertebral compressionvertebral compression• bladder outlet obstruction• bladder outlet obstruction (transurethral resection of the prostate) (transurethral resection of the prostate)

Advanced prostatic carcinoma:Advanced prostatic carcinoma:
1. Hormone resistance1. Hormone resistance
2. Immunotherapy 2. Immunotherapy (recombinant interleukin 2, (recombinant interleukin 2, -interferon)-interferon)
3. Gene therapy3. Gene therapy (immunostimulation, cytoreduction strategy) (immunostimulation, cytoreduction strategy)

Erectile DysfunctionErectile Dysfunction

Erectile Dysfunction: DefinitionErectile Dysfunction: Definition
Erectile dysfunction (ED) is the inability to Erectile dysfunction (ED) is the inability to achieve and/or maintain an erection adequate achieve and/or maintain an erection adequate for satisfactory sexual performancefor satisfactory sexual performance
Erectile difficulty and impotence are also Erectile difficulty and impotence are also referred to as EDreferred to as ED
NIH Consensus Development Panel on Impotence. JAMA 1999;270:83–90

Erectile Dysfunction:Erectile Dysfunction: Epidemiology Epidemiology
The incidence of ED is age-relatedThe incidence of ED is age-related11
1Johannes CB, et al. J Urol 2000;163:460–4632Fugl-Meyer AR, et al. Int J Impot Res 1997;9:141–148
3 NIH Consensus Development Panel on Impotence. JAMA 1999;270:83–90
ED negatively affects sexual and non-sexual domains of ED negatively affects sexual and non-sexual domains of
quality of lifequality of life22
ED is under-diagnosed and under-treatedED is under-diagnosed and under-treated33
Age Incidence
40–4950–5960–69
12.429.846.4

DEMOGRAPHICS OF EDDEMOGRAPHICS OF ED
30 million is the US between 40-70 y/o 30 million is the US between 40-70 y/o may have EDmay have ED
10.5 million or 10.5 million or 35%35% will have moderate will have moderate to severe EDto severe ED

PROJECTED RP ED PROJECTED RP ED STATISTICSSTATISTICS
8 M filipinos between 40-70 years8 M filipinos between 40-70 years
2.8 M filipinos or (2.8 M filipinos or (35%35%) may have ) may have moderate to severe EDmoderate to severe ED

Erectile DysfunctionErectile Dysfunction
More prevalent among patients w/:More prevalent among patients w/:
• Heart DiseasesHeart Diseases• HypertensionHypertension• Diabetes Mellitus Diabetes Mellitus • Cigarette smokersCigarette smokers

Etiology :Etiology :
AnteriogenicAnteriogenic
Venogenic or CavernosalVenogenic or Cavernosal
NeurogenicNeurogenic
Related to DrugsRelated to Drugs
EndocrinologicEndocrinologic
PsychogenicPsychogenic

Erectile Dysfunction: Diagnostic Erectile Dysfunction: Diagnostic TestingTesting
Mandatory or routine testsMandatory or routine tests– Focused physical examinationFocused physical examination– Comprehensive history (sexual, medical, drug Comprehensive history (sexual, medical, drug
and psychosocial)and psychosocial)
Recommended testsRecommended tests– Testosterone (total, free or bioavailable) Testosterone (total, free or bioavailable) – Fasting glucose and serum lipidsFasting glucose and serum lipids
Specialized testsSpecialized tests– Nocturnal penile tumescence or vascular studiesNocturnal penile tumescence or vascular studies
Jardin A, et al (eds). Recommendations of the 1st InternationalConsultation on Erectile Dysfunction. Erectile Dysfunction July 1999

TreatmentTreatment

I. First-line therapyI. First-line therapy• oral erectogenic agentsoral erectogenic agents• couples/sexual therapycouples/sexual therapy
KEY CONCEPTS IN SEX THERAPYKEY CONCEPTS IN SEX THERAPY
--couples communicationcouples communication
-reduction of performance anxiety-reduction of performance anxiety
-enhanced sexual stimulation-enhanced sexual stimulation
-management of concomitant sexual problems-management of concomitant sexual problems
-maintenance and follow-up-maintenance and follow-up
Therapeutic optionsTherapeutic options

C-5

CialisTM

LevitraLevitra

ContraindicationsContraindicationsAdministration of phosphodiesterase Administration of phosphodiesterase inhibitors to patients who use nitrates inhibitors to patients who use nitrates in any form is contraindicated. in any form is contraindicated. Consistent with its known effects on the Consistent with its known effects on the nitric oxide/cGMP pathway, nitric oxide/cGMP pathway, phosphodiesterase inhibitors has been phosphodiesterase inhibitors has been shown to potentiate the hypotensive shown to potentiate the hypotensive effects of nitrates.effects of nitrates.Also contraindicated in patients with Also contraindicated in patients with known hypersensitivity to any known hypersensitivity to any component of the tablet.component of the tablet.
1. Data on file, Pfizer Inc.
S-6


II.II. Consider second-line therapy Consider second-line therapy• intraurethral alprostadilintraurethral alprostadil
• intracavernosal self-injectionintracavernosal self-injection
• Vacuum devicesVacuum devices
Therapeutic optionsTherapeutic options


Intraurethral SuppositoryIntraurethral Suppository MUSE ( Alprostadil )MUSE ( Alprostadil )


Intracavernosal agentsIntracavernosal agents Prostaglandin E 1 ( Alprostadil )Prostaglandin E 1 ( Alprostadil ) PhentolaminePhentolamine MoxysyliteMoxysylite Papaverine Papaverine VIPVIP


III. If necessary, consider third-lineIII. If necessary, consider third-line
therapy therapy • surgical prosthesissurgical prosthesis
Therapeutic optionsTherapeutic options


Penile ImplantsPenile Implants
Penile Vascular surgery Penile Vascular surgery