Embed Size (px)
Citation preview
1
Benign Prostate DisordersBenign Prostate Disorders
Frank P. Begun, M.D.Associate Professor, Urology
Medical Director Urological Services at OSUMedical Director, Urological Services at OSU East Hospital
The Ohio State University
Objectives/GoalsObjectives/GoalsTo understand the causes of BPHT i th t l t d tTo review the symptoms related to BPHTo gain knowledge of the different forms of treatment for bladder outlet obstruction due to BPHobstruction due to BPH
Medical managementSurgical optionsOther treatments
2
ObjectivesObjectivesTo review the causes andTo review the causes and symptoms of prostatitisTo understand the diagnosis and management of prostatitis and Pelvic Pain Syndrome
Benign Prostate DisordersBenign Prostate Disorders
Benign Prostatic Hyperplasia (BPH)ProstatitisPelvic Pain Syndrome (PPS)
3
EpidemiologyBPH/BPEBPH/BPE
EtiologySymptomsObjective DataNonsurgical/Medical ManagementSurgical Management
BPHBPHExact molecular etiology is unknownunknownAndrogens and estrogensGrowth factorsCell-cell interactionsImpaired programmed cell death (apoptosis)Neurotransmitters
4
BPHRole of Androgens
BPHRole of Androgens
Post natal androgen surges are criticalg gImprinting of prostate cellsAffects maturation process and cell deathNecessary during puberty and agingNecessary during puberty and aging Prostatic levels of dihydrotestosterone (DHT) and androgen receptors play a key role
BPH Role of Androgens
BPH Role of Androgens
Prostate retains ability to respond to androgens throughout ones lifeConcentration of androgens does not increase with ageStromal cell – 5 alpha reductase Type 2 p ypinteraction seems to be key event in the development of BPHRole of estrogens is unclear
5
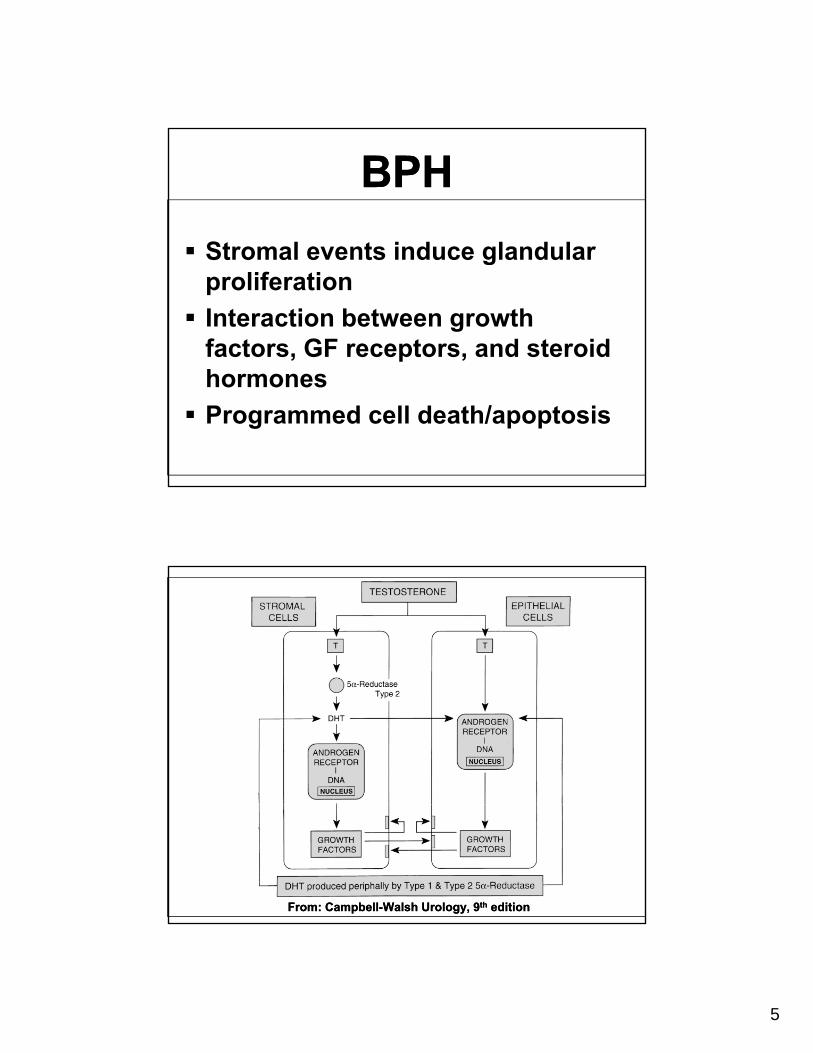
BPHBPHStromal events induce glandularStromal events induce glandular proliferationInteraction between growth factors, GF receptors, and steroid hormonesProgrammed cell death/apoptosis
From: Campbell-Walsh Urology, 9th editionFrom: Campbell-Walsh Urology, 9th edition

6
BPHOther Factors
BPHOther Factors
Inheritable component: earlier ponset, larger gland size, autosomal dominant Sympathetic nerve pathwaysInflammationInflammationRefluxEnvironmental
Pathophysiology of Obstruction
Pathophysiology of Obstruction
BPH develops in the Transition and Periurethral Zones : central prostateProstate Cancer develops in the Peripheral Zone : posterior prostateStatic component of obstructionDynamic component of obstruction
7
BPHBPHObstructive uropathy/Urinary obstructionobstructionBladder outlet obstruction (BOO)Lower Urinary Tract Sx (LUTS)Prostatism
BPH ≠ Urinary obstructionUrinary obstruction ≠ BPH
BPEBPE
E l ti f i d th lExplanation of increased urethral resistance due to BPE is too simplisticMust factor in age related detrussor and bladder neck dysfunctionStatic and dynamic factors
8
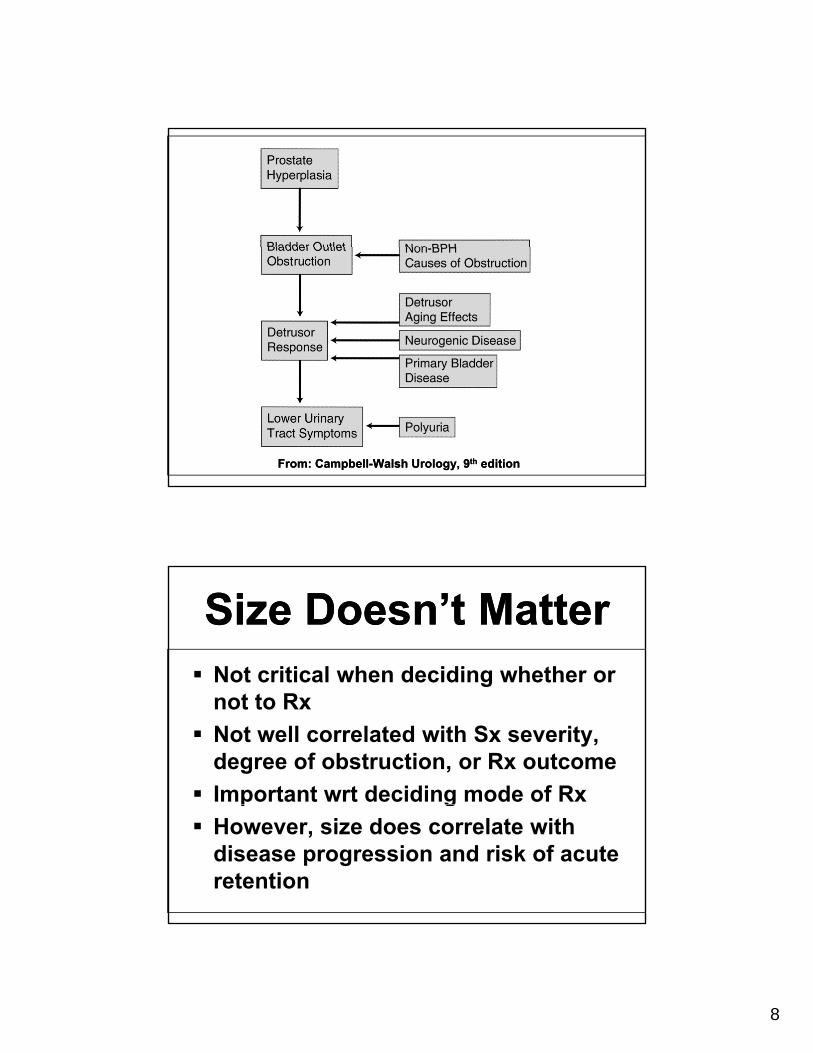
From: Campbell-Walsh Urology, 9th editionFrom: Campbell-Walsh Urology, 9th edition
Size Doesn’t MatterSize Doesn’t MatterNot critical when deciding whether or gnot to RxNot well correlated with Sx severity, degree of obstruction, or Rx outcomeImportant wrt deciding mode of Rxp gHowever, size does correlate with disease progression and risk of acute retention
9
BPHBPHMicroscopic BPH: stromal and epithelial cellular proliferationMacroscopic BPH: increase in the size of the prostate as a result of microscopic BPH (BPE)Clinical BPH: signs and Sx of obstruction due to BPE (LUTS, BOO, Prostatism)
Clinical Manifestations of BPH
Clinical Manifestations of BPH
HematuriaMicroscopicGrossLUTSUTIUTIUrinary retentionHydronephrosisRenal Insufficiency

10
EvaluationEvaluationHistoryAUA/IPSS Symptom ScoreAUA/IPSS Symptom ScoreDREUrinalysis (r/o UTI)Uroflow and Post Void Residual (PVR)(PVR)Imaging : Transrectal U/S (TRUS) with volume measurementUrodynamic Testing
International Prostate Symptom Score (IPSS)
International Prostate Symptom Score (IPSS)
7 questions + QOL assessment7 questions QOL assessmentConsidered “Gold Standard”Not intended to establish the Dx of BPEInitial assessment of severity of SxDeterminant of Rx responseDeterminant of Sx progression
11
IPSSIPSS0-7 Mild Sx8-19 Moderate Sx20-35 Severe SxDegree of “bothersomeness”Need to consider patient’s lifestyle, performance status
UroflowUroflowNon invasiveInaccurate for voided volumes <150mLMax flow rate (Qmax)No definite cutoff as a determinant for RxNo age or voided volume adjustmentLow flow does not differentiate BOO from detrussor hypocontractility
12
Post Void Residual (PVR)Post Void Residual (PVR)
High intra-individual variabilityHigh intra individual variabilityPoor correlation with other signs and SxMeasured by U/S or catheterization? P di t f R t? Predictor of Rx outcomeIncreasing PVRs may be an indicator of the need for intervention
CystoscopyCystoscopyNot indicated to determine the need for treatmentPoor correlation between visual appearance and treatment outcomeIndicated to determine the mostIndicated to determine the most appropriate type of treatment for those who have opted for surgical management
13
Surgical Rx: IndicationsSurgical Rx: IndicationsPatient preferencepRecurrent urinary retentionRecurrent UTI’s Recurrent gross hematuriaBladder calculusLarge bladder diverticulaRenal insufficiency due to BPE
Medical ManagementMedical Management
Preferred treatment for those menPreferred treatment for those men lacking absolute indications for surgical intervention.US Medicare Database:
250,000 prostate surgeries in 1987116,000 in 1996
88,000 in 2000
14
Urinary ObstructionUrinary ObstructionSt ti C tStatic Component: BPH/mechanical obstructionDynamic Component: smooth muscle function at bladder outlet
Nonsurgical Management of BPH
Nonsurgical Management of BPH
Alpha Adrenergic BlockersAlpha Adrenergic BlockersAndrogen Suppression/AblationCombination TherapyAromatase InhibitorsAromatase InhibitorsPhytotherapy
15
Alpha Adrenergic Receptors
Alpha Adrenergic Receptors
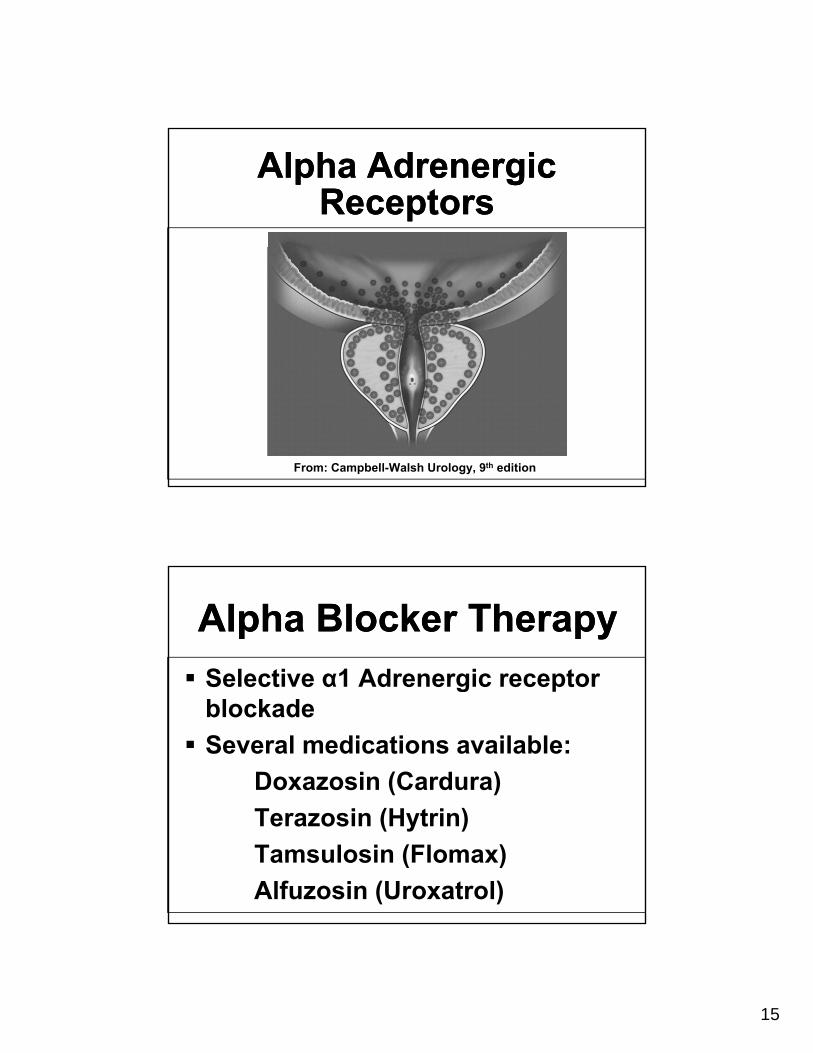
From: Campbell-Walsh Urology, 9th edition
Alpha Blocker TherapyAlpha Blocker TherapySelective α1 Adrenergic receptorSelective α1 Adrenergic receptor blockadeSeveral medications available:
Doxazosin (Cardura)Terazosin (Hytrin)Tamsulosin (Flomax)Alfuzosin (Uroxatrol)

16
Alpha Blocker TherapySide Effects
Alpha Blocker TherapySide Effects
DizzinessOrthostatic hypotensionFatigue/somnolenceHeadacheRhinitisNauseaRetrograde ejaculation
Androgen AblationAndrogen AblationAgents causing a loss of Testosterone or DHT action result in aTestosterone or DHT action result in a decrease in the volume of the prostate.Primarily an epithelial regression.Maximum results occur within 6Maximum results occur within 6 monthsTreats static component of BPH5 alpha reductase inhibitors

17
Androgen AblationAndrogen Ablation5 alpha reductase converts T DHTDHT is predominant intraprostatic androgenFinasteride (Proscar) Type 1Finasteride (Proscar) Type 1Dutasteride (Avodart) Type 1 and 2~30% volume reduction
From: Campbell-Walsh Urology, 9th editionFrom: Campbell-Walsh Urology, 9th edition

18
Androgen AblationAndrogen AblationDecreased risk of urinary retentionDecreased risk of urinary retentionDecreased need for prostate surgeryVolume reduction of prostateCan lower PSA – effect on cancer detectionSide effects : impotence
Combination TherapyCombination TherapyTheory: synergistic effects ofTheory: synergistic effects of alpha blocker and antiandrogenTreats both components of prostate obstruction: static and pdynamicVA Coop Study
19
PhytotherapyPhytotherapySerenoa repens Saw palmetto berrySabal serrulata American dwarf palmSabal serrulata American dwarf palmHypoxis rooperi South African star grassPygeum africanum African plum treeUrtica dioica Stinging nettleSecale cereale Rye pollenCucurbita pepo Pumpkin seedOpuntia Cactus flowerPinus Pine flowerPicea Spruce
PhytotherapyDosages of Common Phytotherapeutic
Preparations
PhytotherapyDosages of Common Phytotherapeutic
Preparations
Serenoa repens (Permixon)160 mg bid Pygeum africanum (Tadenan)50 mg bid Secale cereale (Cernilton)6 capsules β-Sitosterol (Harzol)20 mg tid β-Sitosterol (Azuprostat)65 mg tid
20
PhytotherapyPhytotherapyLittle is know about active compoundsLittle is know about dosageLittle is know about mechanism of actionPaucity of double blinded prospective comparative studiesAlmost all data is anecdotal.
Surgical Treatment Options
Surgical Treatment Options
Intraprostatic StentspTransurethral Needle Ablation (TUNA)Transurethral Microwave (TUMT)Transurethral Laser TherapyTURP : Gold StandardTURP : Gold StandardTransurethral Incision (TUIP)Transurethral VaporizationOpen Prostatectomy
21
Intraprostatic StentsIntraprostatic StentsPrimary indication is in patientsPrimary indication is in patients who are unfit for surgeryTemporary vs. PermanentComplications: migration, painMay be useful as a temporary measure after Laser Rx or TUMT
TUNATUNAHeats prostate tissue to >60°CHeats prostate tissue to >60 CUses radiofrequency (RF) energyResults in deep tissue necrosisSpares the prostatic urethraDoesn’t require anesthesia, therefore, office procedure

22
TUNATUNA
From: Campbell-Walsh Urology, 9th edition
Transurethral Laser Therapy
Transurethral Laser Therapy
G li ht LGreenlight Laser
Holmium Laser (HoLEP)
23
TURPTURP
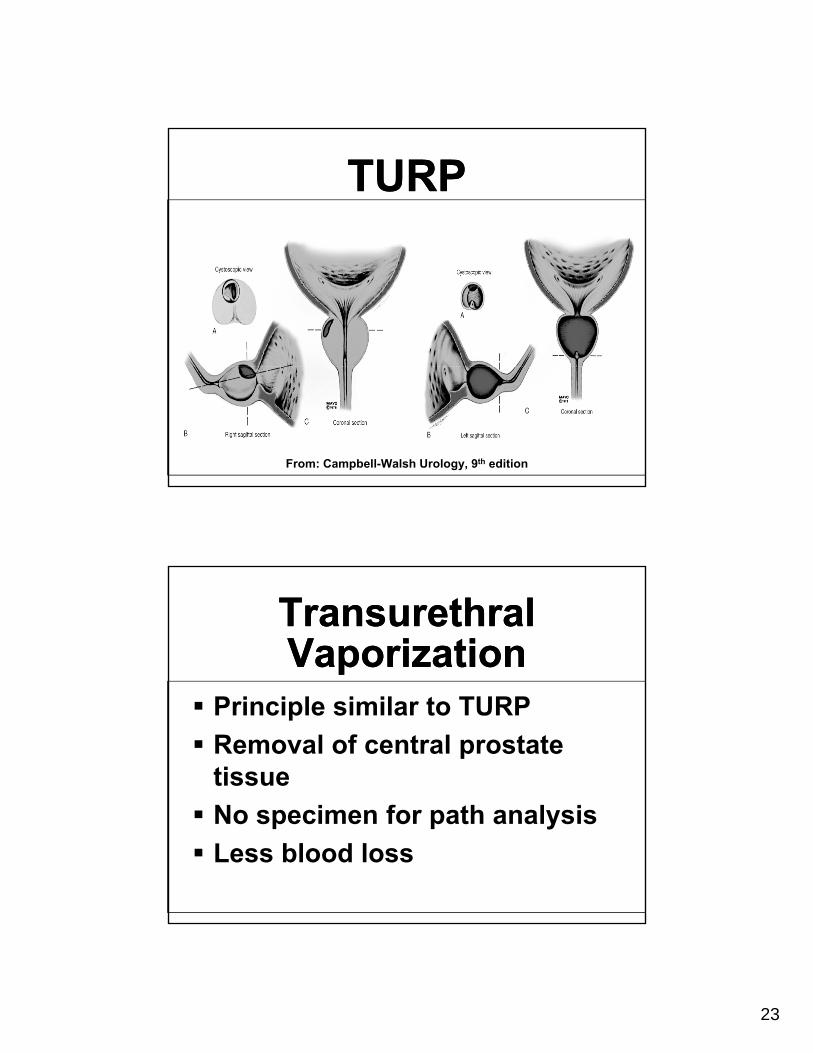
From: Campbell-Walsh Urology, 9th edition
Transurethral VaporizationTransurethral Vaporization
Principle similar to TURPRemoval of central prostate tissue
fNo specimen for path analysisLess blood loss
24
Benign Prostate Disorders
Benign Prostate Disorders
ProstatitisChronic Pelvic Pain Syndrome (CPPS)Syndrome (CPPS)
ProstatitisProstatitisMost common GU Dx in men <50 yrs old3rd most common GU Dx in men >50 yrs
(BPH, prostate cancer)2-10% of men have prostatitis-like Sx2-10% of men have prostatitis-like Sx9-16% have had the Dx of prostatitisAccounts for 3-12% of male GU office visits
25
ProstatitisClassification
ProstatitisClassification
Acute BacterialChronic BacterialNon-bacterialP d iProstatodynia
Prostatitis ClassificationNIH System
Prostatitis ClassificationNIH System
Category I : Acute bacterialCategory I : Acute bacterialCategory II : Chronic bacterialCategory III : Chronic Pelvic Pain Syndrome (CPPS)
IIIA : Inflammatory CPPSIIIB : Non-inflammatory CPPS
Category IV : Asymptomatic
26
Bacterial ProstatitisBacterial ProstatitisG S fGold Standard for Dx is the Meares Stamey “4 Glass” collection technique1st described in 1968Can use pre and post massage “2 Glass” collection
Acute Bacterial Prostatitis/UTIAcute Bacterial Prostatitis/UTI
E coli accounts for 65-80% of infectionsP d Kl b i ll S tiPseudomonas, Klebsiella, Serratia, Enterobacter account for another 10-15%Enterococci 5-10%
Urovirulence : p-fimbri, biofilmsReflux of urine into the intraprostatic ducts
27
Bacterial ProstatitisEtiologies
Bacterial ProstatitisEtiologies
UTITransurethral surgeryIndwelling catheterDysfunctional voiding/neurogenic bladderbladderPhimosisAltered host immune response Idiopathic
ProstatitisOther Organisms
ProstatitisOther Organisms
CorynebacteriumChlamydiaUreaplasmaCandidaTrichamonas

28
Bacterial Prostatitis TreatmentBacterial Prostatitis TreatmentMost antibiotics achieve poor intraprostaticconcentrations and yet antibiotics are the mainstay of treatment Fluoroquinolones Trimethoprim-sulfaMacrolides : erythromycin, azithromycinTetracycline/doxycyclineNo standard treatment durations
Chronic Bacterial ProstatitisTreatment
Chronic Bacterial ProstatitisTreatment
Duration of optimal Rx is unknownDuration of optimal Rx is unknownSulfa-trimethoprim remains primary agent30-50% efficacy ratesFl oroq inolones also sef lFluoroquinolones also useful1 month vs. 3 month RxDifferential Dx = CPPS
29
CPPSCPPSAbsence of bacteria in prostatic secretionssecretionsCommon presenting Sx is painPerineal, suprapubic, penileCan also be groin, testicular, low backPain during and after ejaculation (50%)Irritative or obstructive voiding Sx
CPPSCPPS
>3 months Sx = CPPSSx tend to wax and waneUp to 33% will resolve over 1 year’s timeyear s time
30
CPPSCPPSIntraductile reflux
Chemical prostatitisImmunological AlterationsNeurologicalPelvic floor muscle dysfunctionPsychological factors
CPPS TreatmentCPPS Treatment40% achieve benefit from antibiotic RxRxLong duration Rx not recommendedAlpha blocker RxAnti-inflammatory RxBiofeedbackBiofeedbackPelvic muscle relaxationAntidepressantsPsych