Embed Size (px)
Citation preview
Benefitsof three-dimensionalimaging
Olivier SOREL, Annie OLLIVIER, Marie-Charlotte MANO
Address for correspondence:
O. SOREL,2, place Pasteur,CSD - CHU Rennes,35000 [email protected]
ABSTRACT
Three dimensional images derived from X-Rays, scans or Digital Cone BeamComputed Tomography (CBCT) are components of supplementary diagnosticprocedures. Using them, practitioners can visualize the anatomic relationships ofteeth with each other and with adjacent structures and can discern the presenceor absence of root resorption.
These radiographic films can assist in the diagnostic evaluation of impacted,transposed, or duplicated teeth or those situated on the edges of facial clefts.They are indispensable in helping diagnosticians to rule out contraindications asthey establish treatment plans and continue to be useful as guides whenmechano- therapy starts.
Recently, CBCT has become accessible for use in dental offices even thoughit has been an expensive and bulky instrument with a relatively high radiationoutput. Today, with a more acceptable radiation dosage, it is well accepted as analternative diagnostic procedure in the field of oro-facial implants, but overall, itcannot yet be considered as a technique that should be systematically employedin every supplementary examination.
KEYWORDS
Cone Beam Computed Tomography
Computerized Tomography
Orthodontics
Radiographic exposure guidelines
Embedded Canines.
J Dentofacial Anom Orthod 2010;13:75-90© RODF / EDP Sciences
DOI: 10.1051/odfen/2010107
75
Article available at http://www.jdao-journal.org or http://dx.doi.org/10.1051/odfen/2010107

OLIVIER SOREL, ANNIE OLLIVIER, MARIE-CHARLOTTE MANO
The canines, particularly the maxil-lary ones, are the teeth which are mostfrequently over-retained or impacted.The objective of this study is to demon-strate the benefits of modern three-dimensional imaging in evaluating thespatial position of these teeth and theirrelationship with neighbouring struc-tures. This evaluation is particularlyimportant in making decisions for treat-ment. Uncovering and moving animpacted tooth into its proper positionin the arch may be impossible or partic-ularly risky. Because of its importanceas a strongly rooted and powerfultooth, dentists are justifiably reluctantnot to make the effort to bring it into
place, so the decision to extract it orleave it untouched in its original positionshould only be made after an exhaus-tive and well-reasoned diagnosis. If aplan to uncover and move it17 is indi-cated, three-dimensional imaging canbe a most helpful tool to, first, help oralsurgeons choose their approach and,next, for orthodontists to determine thedirection in which to apply traction. Wediscuss this subject from a clinical notan exhaustive academic point of view,pointing out in addition other indica-tions1 for this type of imaging. In con-clusion, we discuss the benefits ofcone-beam imaging compared with theclassic scanner.
1 - INTRODUCTION
2 - INDICATIONS AND BENEFITS OF IMAGING IN LOCATING EMBEDDED TEETH
Today dentists extract canine teethonly as a last resort only when noother treatment is possible. Therewas a time when the “saber“ toothwas often removed for cosmetic rea-sons and even if its importance as akey to a balanced occlusion is a mat-ter of dispute, and even if the impor-tance of the canines in occlusalbalance is questionable; the cessationof their promiscuous extraction marksa forward step for dentistry.
Sometimes the problems posed tothe movement of impacted cuspidsinto place are almost insurmountable.So in making the decision to electsuch a course of treatment dentistsmust always weigh the risk/benefitratio against the therapeutic benefitsthat might be obtained. To evaluatethose therapeutic risks the practi -tioner must determine the precise
location of the impacted tooth, itsrelationship with its anatomical envi-ronment, and the path it must take tomove into position.
How can practitioners view theinvisible? Since Rontgen, X-rays havegiven them a means to observe mostof the internal structures of the body.Conventional imaging by projectionprovides excellent service in medicineand odontology. This type of examina-tion has become a routine componentof our clinical practice. Orthodontistsuse it, for example, to take diagnosticcephalometric films. But this tech-nique provides information that isincomplete and sometimes inaccu-rate in locating impacted teeeth7, 9, 13.
From profile and frontal cephalomet-ric films, the examiner can gain a roughidea of an impacted tooth’s positionthat might be confirmed by palpation of
76 Sorel O, Ollivier A, Mano MC. Benefits of three-dimensional imaging

J Dentofacial Anom Orthod 2010;13:75-90. 77
BENEFITS OF THREE-DIMENSIONAL IMAGING
a bulge. In such cases it is not neces-sary for the patient to endure furthercostly and irradiating supplementaryradiographic imaging 20.
Clinical examination by direct pal-pation is a reliable way of evaluatingposition3 when it is positive.
The treating dentist can use thepanoramic X-Ray to obtain an over-allbut not anatomically precise view ofthe dentition. The curving movementof the cone head taking a panoramicfilm makes the perceived axial inclina-tion of teeth, particularly the canines,unreliable. When a tooth is not locatedin the thicker portion of a sector, itsimage is blurred and it is impossible todetermine accurately whether thetooth is in front of or behind the planeof the section (fig. 1). A canine that isthought to be missing may go unper-ceived on first inspection. And even if
it is remarked, its blurred image cannot give an accurate idea of its location. Unless a clinical exami -nation provides the required informa-tion, further radiological investigationis essential. The examination of choice is three-dimensional scanningor for defining the indications and
Figure 1Panoramique dentaire montrant un nombreimportant de dents absentes. Au premierexamen l’image floue de la canine dans lasymphyse peut passer inaperçue.
Chronology
Technique/definition
Protocol, patient comfortDosimetric estimatein µSvDosimetric estimatein equivalent days ofnatural irradiation
Cost
Panoramic
1950
Analogical sagittal andfrontal sections
Standing, seated
6 to 15 µSv
1 to 3 days
Low
X-ray scan
1972
The X-ray beam is collimatedto the thickness of the sec-tion and recorded on emer-gence by a ring of detectors
Supine, immobile
50 to 120 µSv
8 to 20 days
High
Cone beam
1988
The pulsed, open, conicalsection X-ray beam makesa single rotation around thedental-maxillary structures
Standing, seated
10 to 65 µSv
2 to 11 days
Intermediate
Table ISummary of the different imagers (Panoramic, X-ray scanner and Cone beam). The doses given depend on themachines and the accuracy of the examination, i.e. the thickness of the section for the scanner and size of voxel forthe cone beam. A wide field cone beam examination with high definition may involve more radiation than a simplescan.
Sorel O, Ollivier A, Mano MC. Benefits of three-dimensional imaging78
OLIVIER SOREL, ANNIE OLLIVIER, MARIE-CHARLOTTE MANO
contraindications for uncovering animpacted tooth, the surgical approach,and the orthodontic mechanics to beimplemented, notably the orientationof traction.
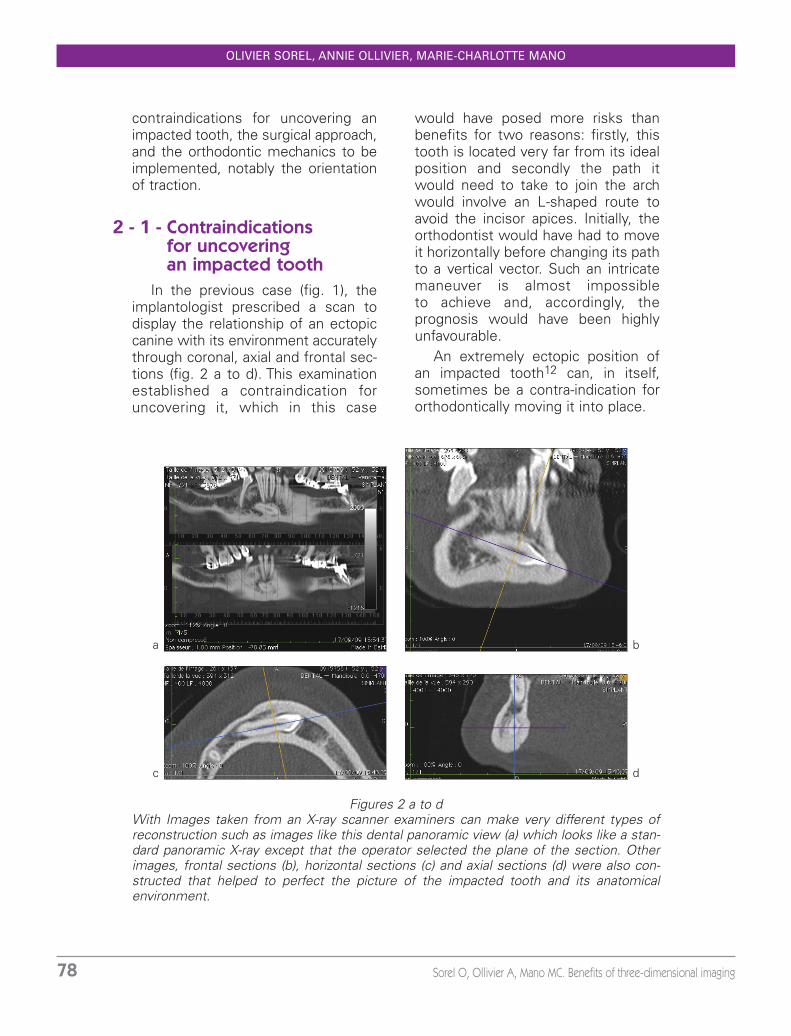
would have posed more risks thanbenefits for two reasons: firstly, thistooth is located very far from its idealposition and secondly the path itwould need to take to join the archwould involve an L-shaped route toavoid the incisor apices. Initially, theorthodontist would have had to moveit horizontally before changing its pathto a vertical vector. Such an intricatemaneuver is almost impossible to achieve and, accordingly, the prognosis would have been highlyunfavourable.
An extremely ectopic position ofan impacted tooth12 can, in itself,sometimes be a contra-indication fororthodontically moving it into place.
2 - 1 - Contraindications for uncovering an impacted tooth
In the previous case (fig. 1), theimplantologist prescribed a scan todisplay the relationship of an ectopiccanine with its environment accuratelythrough coronal, axial and frontal sec-tions (fig. 2 a to d). This examinationestablished a contraindication foruncovering it, which in this case
Figures 2 a to dWith Images taken from an X-ray scanner examiners can make very different types ofreconstruction such as images like this dental panoramic view (a) which looks like a stan-dard panoramic X-ray except that the operator selected the plane of the section. Otherimages, frontal sections (b), horizontal sections (c) and axial sections (d) were also con-structed that helped to perfect the picture of the impacted tooth and its anatomical environment.
a b
c d
J Dentofacial Anom Orthod 2010;13:75-90. 79
BENEFITS OF THREE-DIMENSIONAL IMAGING
In this case, transplantation, depend -ing upon the suitability of the locationof the tooth as well as the site intowhich it will be placed, may be anacceptable alternative treatment. Theprognosis for transplantation dependson how effectively it can be removedfrom its original site, with excellentpreservation of its periodontal mem-brane, the tissue that will have thepotential to re-establish a bond withenveloping alveolar bone. But theanatomical situation of the impactedtooth could be such that removing itwould inevitably damage neighbouringstructures.
Finally, the practitioner may decidethat doing nothing at all would be thebest treatment, providing leaving theimpacted tooth in place would not poseany risks of infection or to planned
orthodontic or implant therapy. Thiswas the decision we made for thepatient depicted in (fig. 2 a to d) wherewe had, in a pre-implant scanning filmfound, to our surprise, an ectopicallyplaced canine.
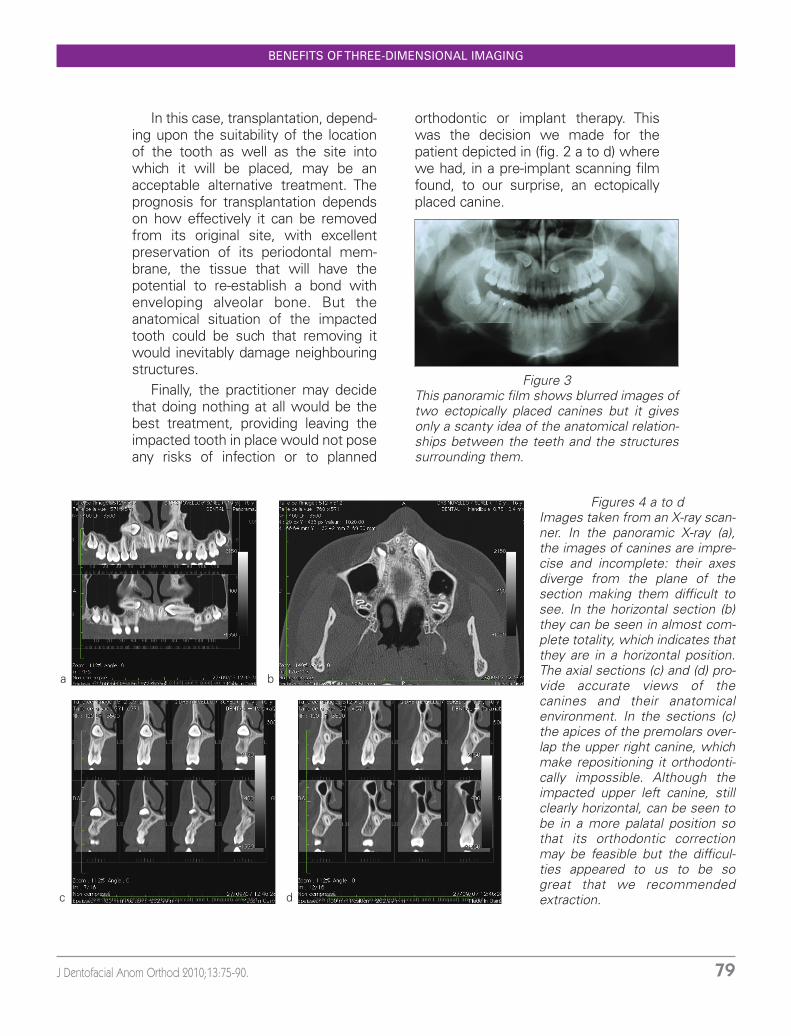
Figure 3This panoramic film shows blurred images oftwo ectopically placed canines but it givesonly a scanty idea of the anatomical relation-ships between the teeth and the structuressurrounding them.
Figures 4 a to dImages taken from an X-ray scan-ner. In the panoramic X-ray (a),the images of canines are impre-cise and incomplete: their axesdiverge from the plane of thesection making them difficult tosee. In the horizontal section (b)they can be seen in almost com-plete totality, which indicates thatthey are in a horizontal position.The axial sections (c) and (d) pro-vide accurate views of thecanines and their anatomicalenvironment. In the sections (c)the apices of the premolars over-lap the upper right canine, whichmake repositioning it orthodonti-cally impossible. Although theimpacted upper left canine, stillclearly horizontal, can be seen tobe in a more palatal position sothat its orthodontic correctionmay be feasible but the difficul-ties appeared to us to be so great that we recommendedextraction.
a b
c d
Sorel O, Ollivier A, Mano MC. Benefits of three-dimensional imaging80
OLIVIER SOREL, ANNIE OLLIVIER, MARIE-CHARLOTTE MANO
Extraction is justified to preventdevelopment of infectious problemslike pericoronitis, for the same rea-sons that extractions of wisdom teethare sometimes prescribed. Extrac -tions of impacted teeth may also be justified when they might be locatedin a posture that could interfere with the orthodontic movement ofother teeth or cause iatrogenic api cal resorption their root apices.Extraction is then the best way ofavoiding highly predictable collateraldamage.
We made the same decision toextract for another patient, whosetwo maxillary canines were impacted
in a high position. The panoramic X-Ray (fig. 3) showed their positionbut gave only a vague, blurred imageof their anatomical relationship toadjacent teeth, cavities, and bonestructures. But with a 3D image thatdid reveal these details15 (fig. 4 a tod), we were able to make a reasonedrecommendation for extraction.
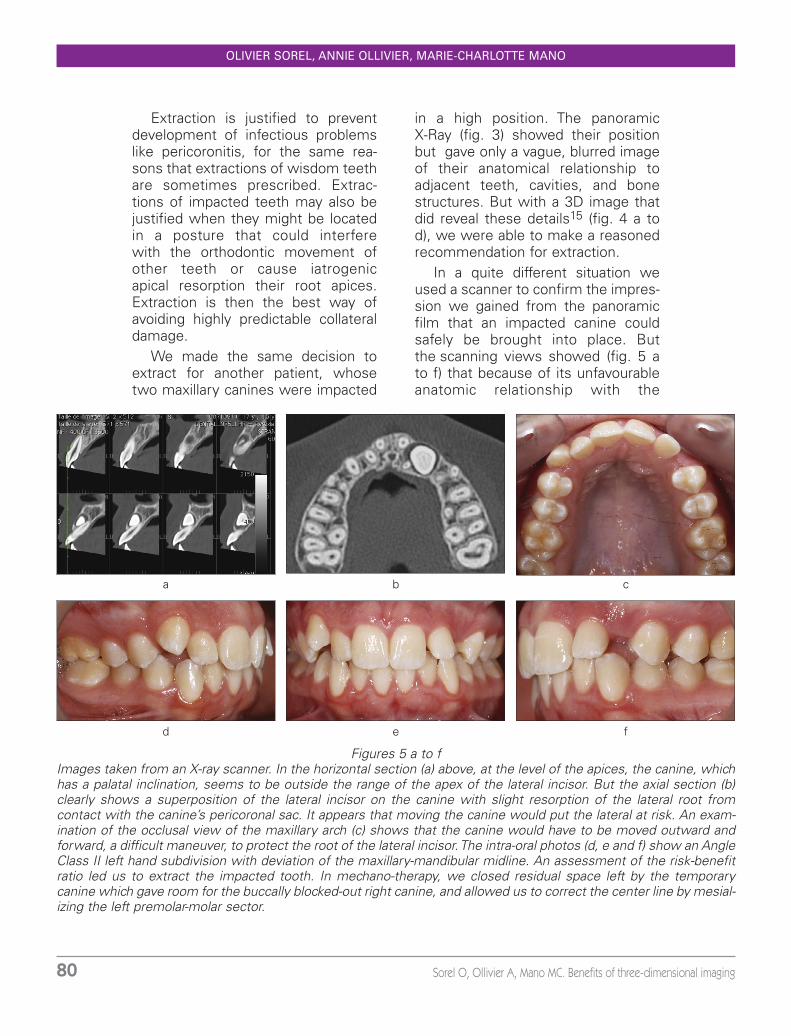
In a quite different situation weused a scanner to confirm the impres-sion we gained from the panoramicfilm that an impacted canine couldsafely be brought into place. Butthe scanning views showed (fig. 5 ato f) that because of its unfavourableanatomic relationship with the
Figures 5 a to fImages taken from an X-ray scanner. In the horizontal section (a) above, at the level of the apices, the canine, whichhas a palatal inclination, seems to be outside the range of the apex of the lateral incisor. But the axial section (b)clearly shows a superposition of the lateral incisor on the canine with slight resorption of the lateral root from contact with the canine’s pericoronal sac. It appears that moving the canine would put the lateral at risk. An exam-ination of the occlusal view of the maxillary arch (c) shows that the canine would have to be moved outward andforward, a difficult maneuver, to protect the root of the lateral incisor. The intra-oral photos (d, e and f) show an AngleClass II left hand subdivision with deviation of the maxillary-mandibular midline. An assessment of the risk-benefitratio led us to extract the impacted tooth. In mechano-therapy, we closed residual space left by the temporarycanine which gave room for the buccally blocked-out right canine, and allowed us to correct the center line by mesial-izing the left premolar-molar sector.
a
d e f
b c
J Dentofacial Anom Orthod 2010;13:75-90. 81
BENEFITS OF THREE-DIMENSIONAL IMAGING
adjacent lateral incisor orthodonticmechano-therapy would be accompa-nied by a high risk of iatrogenic dam-age to the root of the lateral. Therisk-benefit ratio appeared to us to beunfavourable and after discussionwith the patient, we decided toextract the impacted tooth.
more than determine the way toapproach them surgically. We alsoestablish, by scrupulously examiningthe X-ray images, sections and recon-stitutions, the best path to place it onto avoid obstacles as it moves to itscorrect position in the arch. Whenimpacted canines lie in buccal posi-tions, they are usually easy to uncov-er and can be moved into arch with nomajor technical problems16.
However, sometimes 3D imagingis a great help in protecting practition-ers from making faulty assessmentson the basis of information providedby routine X-rays. The crown of theimpacted canine of the young patient
2 - 2 - Indications for uncovering an impacted tooth
In establishing accurate anatomicalrelationships between impacted teethand neighbouring structures we do
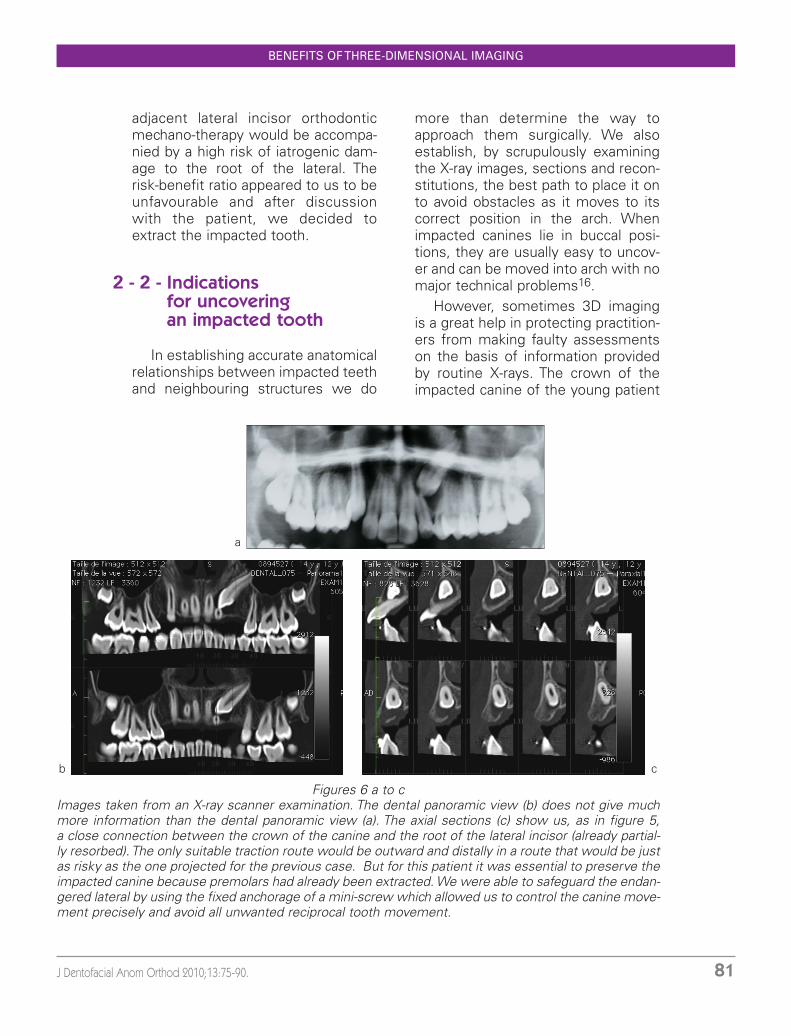
Figures 6 a to cImages taken from an X-ray scanner examination. The dental panoramic view (b) does not give muchmore information than the dental panoramic view (a). The axial sections (c) show us, as in figure 5, a close connection between the crown of the canine and the root of the lateral incisor (already partial-ly resorbed). The only suitable traction route would be outward and distally in a route that would be justas risky as the one projected for the previous case. But for this patient it was essential to preserve theimpacted canine because premolars had already been extracted. We were able to safeguard the endan-gered lateral by using the fixed anchorage of a mini-screw which allowed us to control the canine move-ment precisely and avoid all unwanted reciprocal tooth movement.
a
b c
Sorel O, Ollivier A, Mano MC. Benefits of three-dimensional imaging82
OLIVIER SOREL, ANNIE OLLIVIER, MARIE-CHARLOTTE MANO
depicted in (fig. 6 a to c) lay in a buc-cal position but its root was morepalatal.
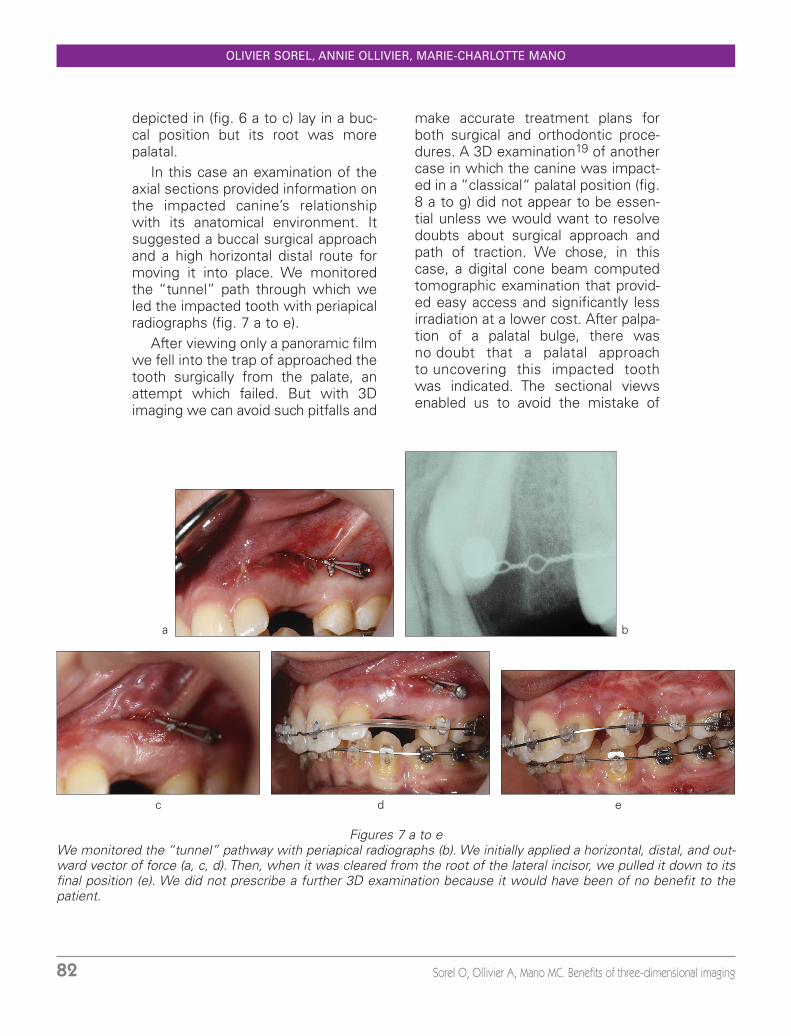
In this case an examination of theaxial sections provided information onthe impacted canine’s relationshipwith its anatomical environment. Itsuggested a buccal surgical approachand a high horizontal distal route formoving it into place. We monitoredthe “tunnel” path through which weled the impacted tooth with periapicalradiographs (fig. 7 a to e).
After viewing only a panoramic filmwe fell into the trap of approached thetooth surgically from the palate, anattempt which failed. But with 3Dimaging we can avoid such pitfalls and
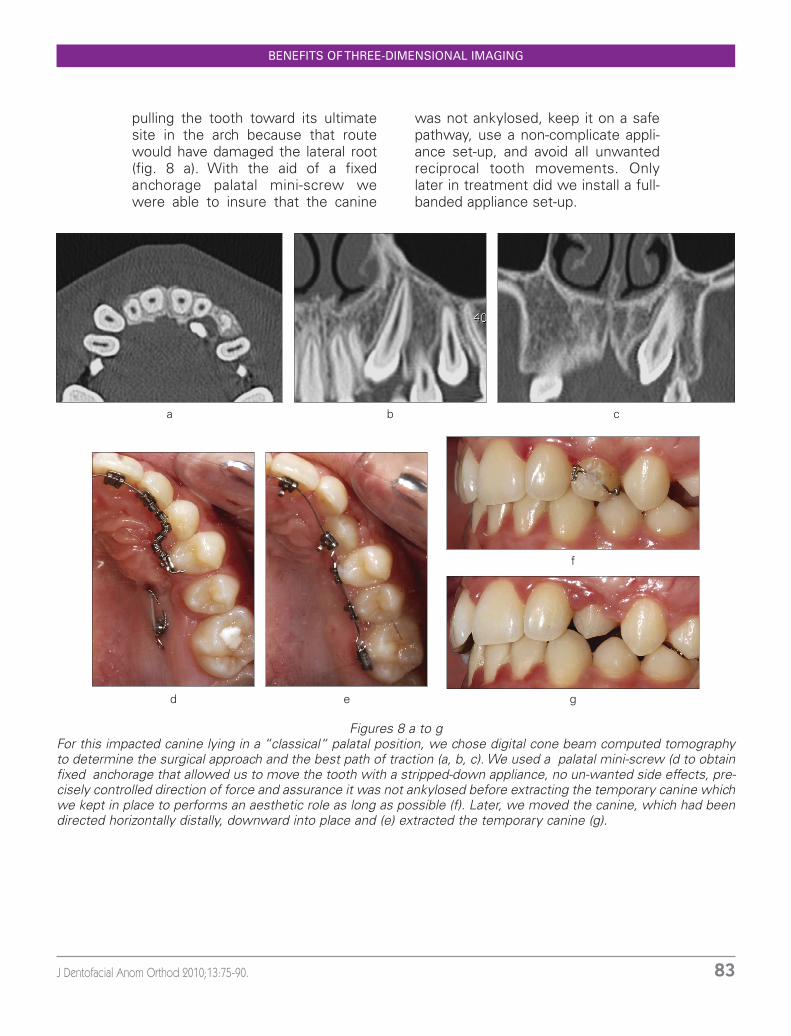
make accurate treatment plans forboth surgical and orthodontic proce-dures. A 3D examination19 of anothercase in which the canine was impact-ed in a “classical“ palatal position (fig.8 a to g) did not appear to be essen-tial unless we would want to resolvedoubts about surgical approach andpath of traction. We chose, in thiscase, a digital cone beam computedtomographic examination that provid-ed easy access and significantly lessirradiation at a lower cost. After palpa-tion of a palatal bulge, there wasno doubt that a palatal approachto uncovering this impacted toothwas indicated. The sectional viewsenabled us to avoid the mistake of
Figures 7 a to eWe monitored the “tunnel” pathway with periapical radiographs (b). We initially applied a horizontal, distal, and out-ward vector of force (a, c, d). Then, when it was cleared from the root of the lateral incisor, we pulled it down to itsfinal position (e). We did not prescribe a further 3D examination because it would have been of no benefit to thepatient.
c d e
a b
J Dentofacial Anom Orthod 2010;13:75-90. 83
BENEFITS OF THREE-DIMENSIONAL IMAGING
pulling the tooth toward its ultimatesite in the arch because that routewould have damaged the lateral root(fig. 8 a). With the aid of a fixedanchorage palatal mini-screw wewere able to insure that the canine
was not ankylosed, keep it on a safepathway, use a non-complicate appli-ance set-up, and avoid all unwantedreciprocal tooth movements. Onlylater in treatment did we install a full-banded appliance set-up.
Figures 8 a to gFor this impacted canine lying in a “classical“ palatal position, we chose digital cone beam computed tomographyto determine the surgical approach and the best path of traction (a, b, c). We used a palatal mini-screw (d to obtainfixed anchorage that allowed us to move the tooth with a stripped-down appliance, no un-wanted side effects, pre-cisely controlled direction of force and assurance it was not ankylosed before extracting the temporary canine whichwe kept in place to performs an aesthetic role as long as possible (f). Later, we moved the canine, which had beendirected horizontally distally, downward into place and (e) extracted the temporary canine (g).
a b c
d e g
f

Sorel O, Ollivier A, Mano MC. Benefits of three-dimensional imaging84
OLIVIER SOREL, ANNIE OLLIVIER, MARIE-CHARLOTTE MANO
Three-dimensional scanning or dig-ital cone beam computed tomogra-phy10, 18 is also indicated for manyother cases, either as a diagnostictool or to elucidate specific atypicalanatomical situations such as transpo-sitions and to assist practitioners inmaking therapeutic decisions.
The lack of image of the alveolarbone means that it is not denseenough to make an appearanceon the X-ray film. Surgeons oftenreport fenestrations in thistype of case when orthodontistsexpand the maxilla;
– a non-calcified inter-maxillarysuture.
By providing a view of the weak-ness of the alveolar rampart, thisexamination influences the choice oftreatment to expand the maxilla thusreducing the burden buccal alveolarbone would have to bear.
After completion of expansiontherapy, the 3D examination againprovided a wealth of information:
– the frontal sections show thatthe axial inclination of the molarsremains upright, allowing themto serve as stress-breaking sup-ports and that the premolars arenow leaning more buccally thanlingually;
– the fenestrations persist but donot seem to have worsened. Onthe 3D surface reconstruction(fig. 9 k) we have images show-ing major improvement in theosseous support for all the buccalteeth except the upper right sec-ond bicuspid. But this view of 15is not confirmed in the frontalsections; where, on the otherhand, 14 seems to be lackingalveolar bone support. The imageprovided by the horizontal sectionshows the roots in the alveolarbone more accurately, recordingthe positions of their roots out-side the cortical area but with no great change from the initialsituation;
3 - OTHER INDICATIONS
3 - 1 - Usefulness in diagnosis
In cases of narrow maxillary arches,for example, it is often difficult to deter-mine what part is played by a problemof basic bone insufficiency and whatcontribution is made by a narrowdento-alveolar arch. Orthodontists willwant to make therapeutic choices thatwill have no deleterious iatrogeniceffects. For the intense debatesorthodontists have with themselvesand with their colleagues about suc-cessful expansion therapy, 3D imagingprovides useful information on a num-ber of points, both before and duringtreatment11, 21.
Three-dimensional investigationusing digital cone beam computertomography provides worthwhile diag-nostic data about teeth and theiranatomical relationships with alveolarbone at an irradiation cost to the patientfar less than that demanded by a scan-ner, the equivalent of 2 to 11 days ofnatural irradiation compared to 8 to 20.
The initial examination of a patientdisplaying transverse maxillary insuffi-ciency depicted in fig. 9a to k shows:
– in frontal sections, molar axial incli-nations that are quite vertical pre-molars that are inclined palatally;
– natural fenestrations especially inthe premolars regions as seen infrontal and horizontal sections.

J Dentofacial Anom Orthod 2010;13:75-90. 85
Figures 9 a to kThe frontal sections (b, c, d, e)show upright molars andpalatally inclined premolars.The inter-maxillary suture is notcalcified (a). By providing a viewof the weakness of the alveolarrampart, this examination indi-cates that palatal expansionwould fulfill treatment objec-tives. After expansion treat-ment, a 3D examination showsin frontal sections that themolar axes have remained ver-tical and still serve as stress-breaking supports and that thepremolars have been uprighted(g, h, i, j). The fenestrations per-sist but do not seem to haveworsened. The 3D surfacereconstruction (k) images showmajor root relief. The horizontalsection shows the relationshipof roots with alveolar bonemore accurately and their posi-tions outside the cortical boneareal but with no great changefrom the initial situation (f).
a
h
f
b g
k
d
e
i
j
c

Sorel O, Ollivier A, Mano MC. Benefits of three-dimensional imaging86
OLIVIER SOREL, ANNIE OLLIVIER, MARIE-CHARLOTTE MANO
– the inter-maxillary suture is clear-ly open in the anterior zone.
With this kind of imaging, practi-tioners can gain an accurate visualiza-tion of the effects of treatment andmake the kind of pertinent and criticalanalyses that are impossible to formsolely on the basis of unreliable, sub-jective clinical impressions.
of the canines. Bone grafts can solvethis problem.
Orthodontists often fail to assessthese situations accurately when theexuberant tissue caused by the scarsof healing makes it difficult to distin-guish supernumerary teeth from permanent teeth erupting normally.A panoramic film may add to the con-fusion with its often misleading andpartial depiction of multiple more orless normal tooth buds in ectopicpositions. 3D imaging provides anaccurate view of all the teeth and theircrowns and roots (fig. 10 a to f) thusenabling the orthodontist to make areasoned judgment on which teeth toextract.
3 - 2 - Usefulness for cases of facial clefts and twinned teeth
Labio-maxillary clefts are oftenaccompanied by impacted or over-retained teeth because the cleft initself is an obstacle to natural eruption
Figures 10 a to fThe examiner cannot get anaccurate view of the exactposition of the teeth or theiranatomy from a panoramic X-ray film. But 3D imagingdoes provide a clear pictureof all the teeth, their crownsand roots. From it, theorthodontist can evaluate allthe available see anatomicstructures and relationshipsof teeth to them. It is hard toshow, with a few pictures ona page, how valuable thesetypes of examination can be.But these six sections (a, b,c, d, e, f), which illustrate a case of a right unilateralcleft, give some idea of their clarity. In them, we can fol-low this cleft from the high-est section (a) to the lowest(f). Similarly, we can readilyidentify the position and sizeand shape of impacted teethas well as assess the size oftheir roots and their relation-ships to neighbouring struc-tures, including the cleft.
a
c d
e f
b
J Dentofacial Anom Orthod 2010;13:75-90. 87
BENEFITS OF THREE-DIMENSIONAL IMAGING
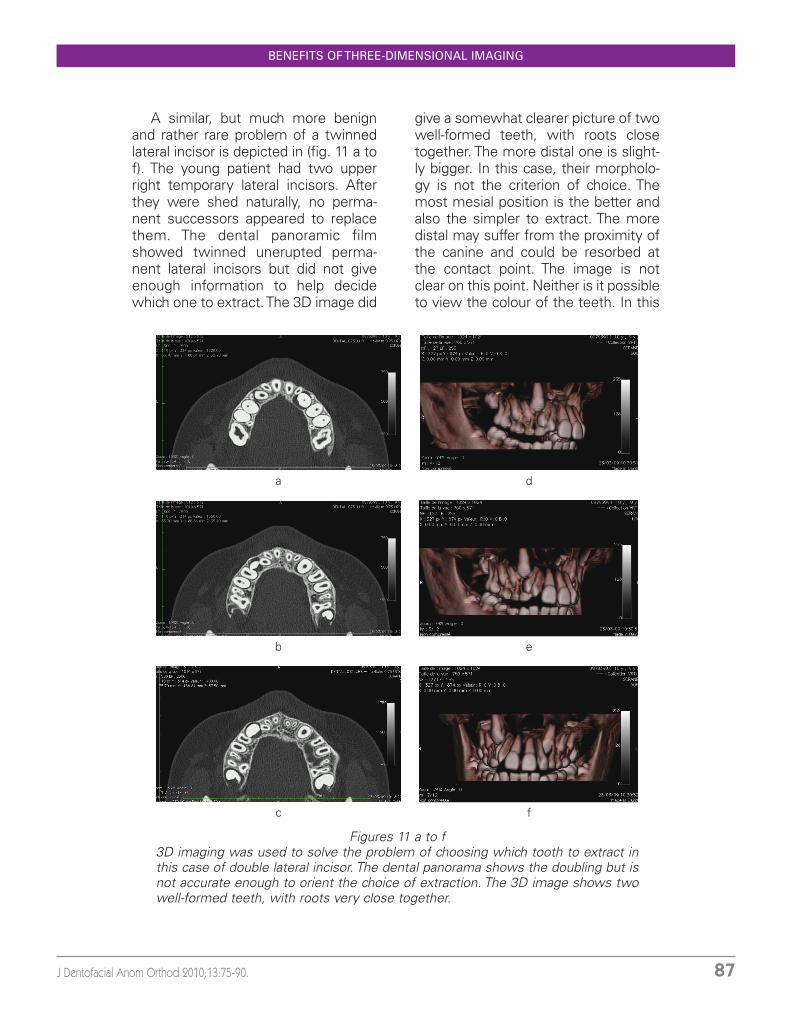
A similar, but much more benignand rather rare problem of a twinnedlateral incisor is depicted in (fig. 11 a tof). The young patient had two upperright temporary lateral incisors. Afterthey were shed naturally, no perma-nent successors appeared to replacethem. The dental panoramic filmshowed twinned unerupted perma-nent lateral incisors but did not giveenough information to help decidewhich one to extract. The 3D image did
give a somewhat clearer picture of twowell-formed teeth, with roots closetogether. The more distal one is slight-ly bigger. In this case, their morpholo-gy is not the criterion of choice. Themost mesial position is the better andalso the simpler to extract. The moredistal may suffer from the proximity ofthe canine and could be resorbed atthe contact point. The image is notclear on this point. Neither is it possibleto view the colour of the teeth. In this
Figures 11 a to f3D imaging was used to solve the problem of choosing which tooth to extract inthis case of double lateral incisor. The dental panorama shows the doubling but isnot accurate enough to orient the choice of extraction. The 3D image shows twowell-formed teeth, with roots very close together.
a
c
eb
d
f

Sorel O, Ollivier A, Mano MC. Benefits of three-dimensional imaging88
OLIVIER SOREL, ANNIE OLLIVIER, MARIE-CHARLOTTE MANO
case, extracting one of the two teethpromotes eruption of the other; doingnothing compromises the more distalincisor. We had no clear choice andsince we had to make some kind ofdecision, we asked the oral surgeon toextract the more distal tooth, if, andonly if he was sure that the moremesial tooth would not be damaged inthe process. If he was not sure, in viewof the over-all surgical difficultiesinvolved, extraction of the more mesialtooth seemed to us to be preferable.
tioned here. But L. Delsol will presentit in greater detail in the next issue.The difficulty in treating transpositionslies mainly in the anatomical relation-ships these teeth have with otherstructures and dental units. 3D imag-ing becomes an invaluable tool inassessing these cases because it pro-vides a view of the roots and enablesthe examiner to envisage the paththey will have to take to move intoposition. This case of transposition ofcanine and first premolar is a goodexample. (fig. 12). After explaining therisks of root resorption and the bene-fits of correction to the patient and hisparents, we all agreed to treat thisproblem. The images show that theavailable space left some margin ofmaneuverability for the requiredorthodontic movement.
3 - 3 - Usefulness in cases of transpositionde transpositions
Figure 123D imaging is also highlyuseful in viewing the rela-tionships of roots in casesof transposed teeth. Theseimages (Pasquet andCavezian) show transposi-tion of the left maxillarycanine and first premolar.3D reconstruction of theentire dentition, from allthe sections gives a goodview of the relationships ofthe roots of the teeth witheach other and with neigh-bouring anatomical struc-tures. Taken together withthe details of the clinicalexamination they give the treating orthodontistenough information todecide whether correctionof the transposition is indi-cated or contraindicated.
The case of dental transposition8
deserves to be at least to be men-

J Dentofacial Anom Orthod 2010;13:75-90. 89
BENEFITS OF THREE-DIMENSIONAL IMAGING
Scanner imaging can provide X-rayfilms that are invaluable in the diag-nosis of impacted teeth, the positionof roots of transposed teeth, or ofteeth in complicated situations likethose located on the edges of facialclefts, and of duplicated teeth. Thistype of imaging has become moreaccessible but it still requires theemployment of bulky equipment andexposes patients to significantamounts of radiation. At present, dig-ital cone beam computed tomogra-phy is an appropriate alternative forthe orofacial sphere, emitting, as itdoes, far less radiation and providingeven higher quality images. This diagnostic tool widely extends therange of information gathering thathas traditionally been available in
orthodontics22 or implantology, Andpromises to be immensely useful toendodontists searching out foci ofperiapical infections. Pinpointing theindications7, 13 and the limitations ofthese supplementary examinationsis essential, as specified in article R. 1333-56 of the Public Health Codewhich requires practitioners to makesure that no other technique of com-parable efficacy but with “less risk”are available...
CBCT10 meets the need for provid-ing accurate investigation of a widerange but demanding minimal irradia-tion, which optimises the risk-benefitratio. We share the opinion ofCavézia5 who anticipates a brightfuture for this type of exploration.
4 - CONCLUSION
1. American Academy of Oral and Maxillofacial Radiology. Executive opinion statement onperforming and interpreting diagnostic cone-beam computed tomographiy. Oral SurgOral Med Oral Path Oral Radiol Endod 2008;106:561-62.
2. Angelopoulos C. Cone beam tomographic Imaging anatomy of the maxillofacial région.Dent Clin North Am 2008 Oct;52(4):731-52, vi.
3. Autorité de sureté Nucléaire. Présentation des principales dispositions réglementairesde radioprotection applicables en radiologie médicale et dentaire.
4. Cavezian R, Pasquet G. L’imagerie médicale en odontologie. Paris : Édition CdP, 2005.5. Cavezian R, Pasquet G. Imagerie et orthopédiedento-faciale : évolution, présentet ave-
nir. Orthod Fr 2008;79:3-12.6. Cavezian R, Pasquet G, Batard J. Imagerie sectionnelle en odontostomatologie : de la
tomographie au scanner RX et au cone beam. Réalités cliniques 2008;19(2):151-65.7. Code de la Santé Publique. Guide des indications et des procédures des examens
radiologiques en odontostomatologie. Paris : Dalloz, 2006.8. Delsol L, Orti V, Chouvin M, Canal P. Canines et incisives maxillaires incluses : dia-
gnostic et thérapeutique. EMC (Elsevier SAS, Paris) Odontologie : Orthopédie dento-faciale 23-492-A-11, 2006.
9. Foucart JM. La radioprotection en odontologie. Paris : Édition CdP, 2004.10. Foucart JM, Felizardo R, Bourriau J, Bidange G. La tomographie volumique à faisceau
conique (CBCT) : du mythe à la réalité. Clinic 2009;Oct;30:483-91.
BIBLIOGRAPHY
Sorel O, Ollivier A, Mano MC. Benefits of three-dimensional imaging90
OLIVIER SOREL, ANNIE OLLIVIER, MARIE-CHARLOTTE MANO
11. Garrett BJ, Caruso JM, Rungcharassaeng K, Farrage JR, Kim JS. Skeletal effects to themaxilla after maxillary expansion with cone-beam computed tomography. Eur J Radiol2008;Jul:23.
12. Guiral H, Medina L, Cavezian R, Pasquet G. Localisation des canines incluses : mise aupoint. AOS 2009;245:63-70.
13. Has. Guide des indications et des procédures des examens radiologiques en odonto-stomatologie, 2006.
14. Hauret L, Hodez C. Nouveauté en radiologie dento-maxillofaciale : la tomographie volu-métrique à faisceau conique. J Radiol 2009;90:604-17.
15. Horner K, Islam M, Flygare L, Tsiklakis K, Whaites E. Basic principles for use of dentalcone beam computed tomography: consensus guidelines of the European Academy ofDental and Maxillofacial Radiology. Dentomaxillofac Radiol 2009 May;35(3):152-7.
16. Korbendau JM, Guyomard F. Chirurgie muco-gingivale chez l’enfant et l’adolescent.Paris : CdP, 1992:212.
17. Korbendau JM, Patti A. Le traitement orthodontique et chirurgical des dents incluses.Quintessence international, 2005. Réussir, 135 p.
18. Ludlow JB, Davies-Ludlow LE, Brooks SL, Howerton WB. Dosimetry of 3 CBCTdevices for oral and maxillofacial radiology: CB MercurRay, NewTom 3G, and i-Cat.Dentomaxillofacial Radiology 2006;35:219-26.
19. Noble J, Hechter FJ, Karaiskos NE, Lekic N, Wiltshire XA. Future practice plans of ortho-dontic résidents in thr United States. Am J Orthod Dentofacial Orthop 2009Mar;135(3):357-60.
20. Nrdstrom D. Radiographic exposure guidelines. Am J Orthod Dentofacial Orthop 2009Mar;135 (3):272.
21. Rungcharassaeng K, Caruso J, Kan J, Kim J, Taylor G, Factors affecting buccal bonechanges of maxillary posterior teeth after rapid maxillary expansion. Am J of OrthodDentofacial Orthop 2007 Oct;132-4:428.e1-428.e8.
22. Treil J, Bracia J, Aïat Ameur A. Modélisation 3D du viscéro-crâne. Applications enorthodontie et clinique orthognatique. J Radiol 2009;90:634-41.
23. Walker L, Enciso R, Mah J. Three-dimensional localization of maxillary canines withcone-beam computed tomography. Am J Orthod Dentofacial Orthop 2005;128(4):418-23.





























