Embed Size (px)
Citation preview

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS
BENEFITS OF PHYSICAL THERAPY INTERVENTIONS IN BARIATRIC HEALTH PROMOTION AND
WELLNESS: A CASE REPORT
____________________________________________________________________________
A Case Report
Presented to
The Faculty of the College of Health Professions and Social Work
Florida Gulf Coast University
In Partial Fulfillment
of the Requirement for the Degree of
Doctor of Physical Therapy
By
Paul Brendan Kirk
2016

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS
APPROVAL SHEET
This Case Report is submitted in partial fulfillment of the requirements for the degree of
Doctor of Physical Therapy
____________________________________
Paul Brendan Kirk, SPT Approved: August 3, 2016
____________________________________
Kathy Swanick, DPT, MS, OCS Committee Chair
____________________________________
Rose Pignataro, PhD, DPT, CWS, CHES Committee Member 1
____________________________________
Ellen Donald, PhD, PT Committee Member 2
The final copy of this case report has been examined by the signatories, and we find that both
the content and the form meet acceptable presentation standards of scholarly work in the above
mentioned discipline.

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS
Acknowledgements
I would like to express gratitude to my academic committee for their continued support
and advice throughout the duration of this project. I would also like to thank the College of
Health Promotions and Social Work at Florida Gulf Coast University and Zenergy Physical
Therapy in Fort Myers for the use of their facilities, which were instrumental in allowing this
project to come to fruition. Finally, I would like to express my deep gratitude to the case patient:
I hope this project will benefit them as much as their participation benefitted me.

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 1
Table of Contents
Abstract ............................................................................................................................................ 2
Background and Purpose ................................................................................................................. 4
Case Description .............................................................................................................................. 7
Clinical Impression #1 .................................................................................................................. 8
Examination ................................................................................................................................. 9
Clinical Impression #2 ................................................................................................................ 11
Intervention ............................................................................................................................... 12
Outcomes ................................................................................................................................... 18
Discussion ...................................................................................................................................... 19
References ..................................................................................................................................... 24
Appendix A – Exercise and Strength Logs ...................................................................................... 27
Appendix B – Psychosocial Surveys ............................................................................................... 29

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 2
Abstract
Background and Purpose: The prevalence and severity of obesity among the American public is
steadily rising. It is well-recognized that increased body mass is a major preventable risk factor
for cardiovascular disease, hypertension, type 2 diabetes, stroke, osteoarthritis, certain types of
cancer, and a variety of mental health issues such as depression and anxiety. Prevention and
treatment therefore focuses on promoting a change in nutritional choices and physical activity.
As movement specialists and experts in non-invasive health management, physical therapists
have a unique opportunity to expand their impact on public wellness by promoting physical
activity and exercise, particularly among those affected by elevated body mass and its
associated risks.
Case Description: The patient was a 28-year old administrative assistant at a health care facility.
She expressed interest in receiving consultation to improve her health and learn behaviors that
would help her continue to improve her overall wellness beyond the intervention period.
Outcomes: After a 22 day intervention period, the patient made improvements in several key
areas. Weight decreased by 4 pounds, waist-to-hip ratio decreased from 0.97 to 0.89 (with a
drop in waist circumference of 13cm), BMI dropped from 40.4 to 39.5, plank time improved
from 11 to 33 seconds, and pectoral flexibility improved by 15o. In addition, the patient showed
improvements in self-efficacy, decisional balance, and process of change.
Discussion: As specialists of function and movement, physical therapists are in a unique position
to offer overweight and obese clients expertise in improving their overall wellness. Customized
wellness plans can be developed that maximize the chance of patient success through an
understanding of patient motivation and potential barriers to success, especially when taking
into account the patient’s psychosocial state of mind. By following closely with patients, plans

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 3
can be tailored so that the patient can continue to succeed in their wellness goals long after
discharge.

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 4
Background and Purpose
The prevalence and severity of obesity among the American public is rising, causing an
increase in the number of non-communicable chronic health issues (Adler & Stuart, 2009).
According to the World Health Organization, this is a global trend affecting approximately 300
million people (2009). This has led to formation of a worldwide health agenda prioritizing poor
diet, lack of physical activity, and obesity as areas in need of immediate intervention (Cecchini,
Sassi, Lauer, Lee, Guajardo-Barron, & Chisholm, 2010). It is well-recognized that increased body
mass is a major preventable risk factor for cardiovascular disease, hypertension, type 2 diabetes,
stroke, osteoarthritis, certain types of cancer, and a variety of mental health issues such as
depression and anxiety (Dixon, 2010; Adler & Stuart, 2009; Dean, 2009). Furthermore, obesity is
a major cause of premature mortality, with approximately 28 million annual deaths attributable
to the consequences of excess body weight (Bastien, et al., 2014).
In addition to chronic disease and mortality risks, there are immediate effects of
overweight and obesity that can include reduced aerobic fitness and cardiopulmonary
impairments, joint pain and other musculoskeletal pathology, and integumentary issues. From a
physical therapy perspective, these problems contribute to functional limitations and loss of
independence (Sack, Radler, Mairiella, Tougher-Decker, & Khan, 2009). Thus far, as shown by
continued increases in prevalence and severity, efforts to address overweight and obesity have
failed to demonstrate any appreciable improvements. As movement specialists and experts in
non-invasive health management, physical therapists have a unique opportunity to expand their
impact on public wellness by promoting physical activity and exercise, particularly among those
affected by elevated body mass and its associated risks (Sack, Radler, Mairiella, Tougher-Decker,
& Khan, 2009; Dean, 2009).

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 5
According to previous research, lifestyle choices and health behaviors account for
approximately 40% of the risk for premature mortality. With regard to overweight and obesity,
prevention and treatment therefore focuses on promoting a change in nutritional choices and
physical activity (Adler & Stuart, 2009). In 2008, estimated prevalence of obesity among
American adults was 33.8%, with 10-year increases noted for all age groups (Flegal, Carroll,
Ogden, & Curtin, 2010), doubling the number of people affected within the past 30 years (Hopps
& Caimi, 2010). Closely related to this, sedentary behavior is a pandemic issue within the United
States, with less than 4% of adults aged 20 to 59 currently achieving recommended levels of
physical activity: a minimum of 150 minutes of moderate activity, or 75 minutes of vigorous
activity per week (Annesi, Unruh, Marti, Gorjala & Tennant, 2011). Incidentally, physical activity
has been identified as one of the most effective strategies in preventing and reducing obesity
(Dalle Grave, Calugi, Centis, El Ghoch, & Marchesini, 2010). The use of exercise in health
promotion and wellness is two-fold: although exercise has been identified as the strongest
factor in achieving and maintaining weight loss, adequate physical activity is also an
independent predictor of reduction in disease risk (Annesi, Unruh, Marti, Gorjala & Tennant,
2011). In addition to improving overweight and obesity, enhanced physical fitness mitigates the
risk of cardiovascular disease, type2 diabetes, and premature mortality (Church, 2011).
Adherence to an exercise program, regardless of body composition, can be a significant
challenge. It has been estimated that more than half of all people who initiate a new exercise
program will drop out within the first 3 to 6 months (Annesi, Unruh, Marti, Gorjala & Tennant,
2011). Barriers to exercise may involve psychosocial and behavioral factors as well as physical
challenges (Dalle Grave, R., Calugi, S., Centis, E., El Ghoch, M., & Marchesini, G., 2010). In a
cross-sectional study, researchers found strong correlations between exercise self-efficacy and
weight loss (Linde, Rothman, Baldwin, & Jeffrey, 2006). In fact, it has been suggested that self-

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 6
efficacy is one of the most important determinants of adherence to an exercise program (Dalle
Grave, Calugi, Centis, El Ghoch, & Marchesini, 2010). According to Social Cognitive Theory, self-
efficacy can be enhanced by encouraging an individual to set a series of realistic, attainable
goals (Bandura, 2004). Monitoring physiologic improvements as a result of exercise adherence
also assists in this regard (Annesi, Unruh, Marti, Gorjala, & Tennant, 2011). One way of assessing
and monitoring an individual’s outlook with respect to physical activity is the Exercise Self-
Efficacy Scale, developed by Marcus, Selby, Niaura and Rossi (1992). This self-administered
questionnaire is used to generate a composite score based on items that ask respondents to
rate their confidence level in completing physical activity when presented with various
challenges such as time constraints and/ or lack of energy.
Clinicians can also assess a client’s readiness to engage in exercise by using the Physical
Activity Stages of Change Questionnaire, designed to assist with tailored interventions to
promote motivation and adherence (Marcus & Rossi, 1992). Strategies to promote readiness to
change might include individualized education regarding risks and benefits associated with
physical activity, opportunities for making healthy choices, and options for encouraging a
commitment to exercise (Marcus & Lewis, 2003). A non-judgmental approach is essential to
ensuring open communication between the physical therapist and the client, due to concerns
regarding stigma and personal criticism about one’s weight (Sack, Radler, Mairiella, Tougher-
Decker, & Khan, 2009).
When working with clients who are overweight or obese, clinicians should be prepared
to explore common reasons for lack of exercise adherence. These may include initial discomfort
when engaging in physical activity due to excess physiologic stresses associated with increased
body mass and low fitness levels. Selecting activities and exercise intensity that the individual
finds comfortable and enjoyable may help to offset these issues. Time constraints can be

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 7
addressed by assisting the client in identifying ways to fit short intervals of physical activity into
his or her usual daily routine. Each of these strategies should be tailored to the individual by
using a collaborative, rather than prescriptive, approach. In addition, by studying people who
have been successful in maintaining long-term adherence, researchers have concluded that
sustained physical activity is more likely with home-based programs versus on-site exercise,
which could introduce another barrier due to limited access to facilities. Additional facilitators
include social support, which can be augmented by enlisting the help of significant others such
as friends and family to provide additional motivation and encouragement (Dalle Grave, R.,
Calugi, S., Centis, E., El Ghoch, M., & Marchesini, G., 2010).
Case Description: Patient History and Systems Review
Upon initial evaluation, the case patient signed an Authorization and Consent to Treat
form, and completed a Par-Q form to identify whether it was necessary for the patient to
consult their physician before beginning an exercise program. The patient was a 28 year old
Hispanic female who works as an administrative assistant at a small private healthcare clinic in
Southwest Florida. She expressed interest in receiving physical therapy intervention after
hearing about health promotion and wellness for individuals with elevated BMI through her
clinic’s relationship with Florida Gulf Coast University’s Physical Therapy Program. The patient
was a tobacco user until 2009, but otherwise has an unremarkable history. She reported no
medical or surgical history and reported no prescription medications. Her family history is
significant for atrial fibrillation, hypertension, diabetes, lymphoma, and lung cancer.
The patient reported she was overweight, but not obese, until roughly seven years ago,
when a rapid weight increase occurred, presumably due to a combination of smoking cessation
and an increase in life stress after her mother developed cancer. In addition to stress from these
two events, the patient cited poor dietary history and a lack of exercise as reasons for her

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 8
current situation. The patient’s goals were to lose body fat and to gain knowledge on how to live
a healthier lifestyle, so that she could continue to progress her wellness plan after the
intervention period.
Clinical Impression #1
It was concluded that the patient was a good candidate for physical therapy
intervention based on several factors. First, the patient was well above the BMI threshold for
obesity. Secondly, the patient was young and had very few comorbidities, which allowed her to
participate in unrestricted exercise with minimal risk. Finally, the patient expressed a desire to
improve her overall health and wellness.
Tests and measures utilized during the initial examination included a detailed patient
history, resting vital signs, postural and gait assessment, body composition tests including BMI,
waist-to-hip ratio, and 7-site skinfold test, and fitness tests including single-leg stance test,
modified pushup, 30 second sit-to-stand, plank test, and 6-minute walk test. A general flexibility
screen was also included for the gastrocsoleus complex, hamstrings, hip flexors, iliotibial band,
and pectorals. Finally, the patient was asked to complete four psychosocial questionnaires to
determine her strengths and weaknesses when approaching health and wellness goals. These
included the Physical Activity Self-Efficacy Questionnaire, Physical Activity Decisional Balance,
Physical Activity Processes of Change Questionnaire, and Expected Outcomes and Barriers for
Habitual Physical Activity.
Tests and measures were chosen to gather as much information about the patient’s
current level of fitness and any functional limitations with the greatest efficiency. The single-leg
stance test was chosen as an overall balance screen (Jacobs, Horak, Tran, & Nutt, 2005). The
modified pushup test was chosen to assess overall upper body strength, with the ‘modified’
position chosen due to the patient’s inability to perform a standard pushup with proper form.

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 9
The 30 second sit-to-stand was chosen to assess overall lower extremity strength, and the plank
test was chosen to assess core strength. The 6-minute walk test was chosen to assess
cardiovascular function and endurance. (Enright & Sherrill, 1998) Flexibility tests were chosen to
assess the large muscle groups.
Examination
Upon initial examination, the patient’s resting vitals were all satisfactory for continuing
with an exercise program. The patient’s blood pressure was 150/88 and resting heart rate was
96; while both values were elevated, neither was cause for termination and both were stated by
the patient to be within her normal range. All resting vitals are available in Table 1. Upon
postural examination, bilateral foot and ankle pronation was noted, with the right more than
the left. In addition, mild bilateral genu valgum was also noted, as well as elevation of the right
scapula. The patient demonstrated mild forward head posture in both sitting and standing. Gait
analysis showed moderately excessive arm swing bilaterally with accompanying decreased trunk
rotation.
Body composition tests showed results consistent with an obese individual. Based upon
height and weight measurements, a BMI of 40.4 was calculated, indicating the patient is just
over the threshold for morbid obesity (BMI > 40). The Waist-to-Hip ratio was 0.97, which
indicates a very high overall health risk; the normal ratio for an adult female should fall under
0.8 (Noble, 2001). Finally, the 7-site skinfold test gave an estimated body fat percentage of 39%.
For the patient’s age group, anything over 32% is considered obese (Esmet, 2012). A specific
breakdown of body composition is given in Table 1.
There were six balance and strength tests performed. These tests were selected and
performed in order to obtain a baseline assessment of the patient’s general function. In the
single-leg stance test, the patient achieved 7 seconds with the right leg and 6 seconds with the

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 10
left. She completed 12 reps in the 30-second sit-to-stand, and 17 modified pushups in 30
seconds. She was able to hold a plank position with proper form for 11 seconds. In the 6 minute
walk test, she ambulated for 420 meters, and afterward had a blood pressure of 152/90, a heart
rate of 114 bpm, and an oxygen saturation of 98%. Flexibility tests showed decreased flexibility
of the right pectoral, both hip flexors, and both IT bands.
Table 1 Initial Examination Data
Finally, the four psychosocial questionnaires were completed and the results were
discussed with the patient. The results of the initial completion of these questionnaires were
used to help identify areas where the patient would benefit from improved motivation, self-
efficacy, and readiness to change, and what possible barriers to change were present. When
designing the intervention, the survey results were taken into account in order to produce a
plan that had a higher likelihood of succeeding given the patient’s proclivities. The same
questionnaires were given post-intervention to see if behaviors had changed over the course of
the episode of care.
Blood Pressure 150/88 Height 55.5in Single-leg Stance 7s R
Respiratory Rate 24 Weight 177lbs 6s L
O2 Sat 97% BMI 40.4 Modified Pushup 17 rep
Heart Rate 96 Waist 118.5cm 30s sit-to-stand 12 rep
Hip 122cm Plank 11s
Waist-Hip Ratio 0.97
7-site Skinfold 39%
6-minute Walk 420m Pectoral 150deg FF
BP 152/90 Hip Flexors + Thomas Bil
HR 114 TFL/ITB +Ober Bil
O2 sat 98%
Flexibility6-minute Walk
Resting Vitals Body Composition Balance and Strength

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 11
Clinical Impression #2
Based upon the results of the initial examination, it was determined that the patient
was a strong candidate for physical therapy interventions to promote weight loss and improved
fitness through a tailored program of physical activity. The patient’s history and vital signs gave
no red flags to avoid an exercise program, while at the same time, her body composition tests
showed clear indications of obesity. Balance, strength, and flexibility tests showed several
possible areas of focus that could be incorporated into a comprehensive wellness program.
Additionally, the patient interview determined that knowledge of a proper diet and healthy
eating habits were both lacking, which would indicate the need for general nutrition education.
Finally, psychosocial questionnaires provided insights into patient motivation, self-efficacy, and
readiness to change.
The psychosocial questionnaires revealed that the patient was unsure of her ability to
participate in a regular exercise program when faced with adversarial circumstances (tired, poor
mood, adverse weather, etc). However, she demonstrated awareness of the benefits of exercise
and the risks of avoiding exercise. Her readiness to become more physically active was
moderate – she was ready to make some lifestyle changes but resistant to others. Finally,
potential barriers to physical activity included self-consciousness and a perceived lack of
willpower, time, energy, equipment, knowledge, convenient location, and finances.
Based on the initial encounter, it was determined that the patient would begin the
intervention plan within a few days of the initial examination, during a follow-up visit which
would include instruction in a comprehensive health and wellness plan. The plan would be
explained to the patient, and any questions would be addressed. Modifications to the plan
would be made if necessary. After the follow-up appointment, the patient would follow the plan
independently for a period of three weeks, during which time there would be a checkup

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 12
appointment to determine if the plan was progressing well, and to make modifications as
indicated. All initial tests and measures would be repeated upon completion of the intervention
period to determine the effects of the plan.
If the health and wellness plan was to be successful, several changes might be observed
by the end of the intervention period. Reductions could be seen in resting vital signs as a result
of increased cardiovascular health. Decreases in BMI, waist-to-hip ratio, and 7-site skinfold tests
might also be present due to a combination of fat-burning exercise and nutritional changes.
Increases in performance of strength tests should occur following adherence to the strength
program, as well as improved flexibility with the stretching program. Finally, at the end of the
intervention period, the patient should demonstrate improved motivation, self-efficacy, and
readiness to change as measured by the psychosocial surveys. This should assist the patient in
continuing her lifestyle changes in the post-intervention period. Possible barriers to success
could include patient adherence, patient injury, and the brief timeframe of the intervention
period.
Intervention
To develop the intervention plan for the case patient, data from the initial examination
was analyzed to identify areas in greatest need of improvement. The intervention plan centered
on four main areas of focus: cardiovascular, strength, flexibility, and nutrition. Based upon the
initial examination data, each area was customized to produce optimal improvements in overall
wellness during the intervention period, but also to allow the patient to continue independently
after discharge. Due to the brief duration of the intervention, and the patient’s lack of previous
exercise experience, care was taken not to overwhelm the patient with exercises (Henry,
Rosemond, & Eckert, 1999), but to instead choose exercises that would give the most benefit

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 13
given the patient’s initial deficits. A breakdown of the interventions and their progressions can
be seen in Table 2.
Table 2 Breakdown of Interventions
Care was taken during the construction of the intervention plan to integrate patient
input into the final product. Data from the psychosocial questionnaires was paired with a
patient interview to determine where barriers to exercise might exist, as well as identify any
activates the patient enjoyed performing. From this information, it was determined that an
intervention plan should be developed that the patient could perform at home, could be
performed in short stages as opposed to longer sessions, and would allow the patient to choose
certain exercises to perform on a given day depending on her desires. An example can be seen
in the cardiovascular plan: the patient was instructed that she could complete as little as 5
minutes of exercise at a time, doing whatever activity raised her heart rate into the target zone,
as long as daily requirements were met. This allowed the patient the freedom to plan her own
exercise, the goal of which would be to increase the likelihood of adherence.
Results from the patient’s resting vitals and 6-minute walk test, as well as results from
the psychosocial surveys, were taken into consideration when developing the cardiovascular
Cardiovascular
Initial:
15 minutes/day,
5 days/week. 2/3
of time in Fat
Burning zone, 1/3
in cardiovascular
zone
PNF D2
Extension.
Standing.
3 sets of 6
- 10 reps
Supine hook-
lying Transverse
Abdominus
holds. 3 sets of
10 second
holds.
Seated rows
with
theraband.
3 sets of 6 -
10 reps.
Doorway "Y"
stretch. 3 sets
of 30 second
static holds.
Standing
Quadriceps
stretch. 3 sets
of 30 second
static holds.
Side-lying IT
band Table
Stretch. 3 sets of
30 second static
holds each leg.
Progression:
30 minutes/day,
5 days/week. 2/3
of time in Fat
Burning zone, 1/3
in cardiovascular
zone
N/A
Supine hook-
lying Transverse
Abdominus
holds with
stepping. 3 sets
of 5 steps each
leg, lifting foot
6in off of mat.
N/A N/A N/A
Standing IT band
stretch. 3 sets of
30 second static
holds each leg.
Strength Stretching

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 14
exercise plan. Relevant information gleaned from the patient interview included her affinity for
swimming and fitness-focused video games, which were both incorporated into her plan. To
begin, she was asked to perform 15 minutes of cardiovascular exercise 5 days a week; 10
minutes was to be in her Fat Burning zone (HR 103-141), and 5 minutes was to be in her
Cardiovascular zone (HR 141-160). After she was able to complete 15-minute sessions without
difficulty, she was progressed to 30-minute sessions (20 minutes in Fat Burn, 10 in
Cardiovascular). This allowed her to complete 150 minutes of moderate cardiovascular exercise
per week, which is in line with the recommendations of the American Heart Association for
adult activity. In order for the patient to not feel like the cardiovascular exercise was a “chore,”
she was able to choose any activity that would allow her to reach her heart rate goals for the
specified time period. A “Cardio Log” was developed for the patient to use to keep track of her
cardiovascular exercise, a copy of which is included in the Appendix.
The patient’s strength interventions were developed using results from the Tests and
Measures section. From these results, areas of identified weakness included balance (single-leg
stance test), core (plank test), and upper extremities (modified pushup). From a combination of
core weakness, postural assessment, and her job requirements of frequent prolonged sitting in
front of a computer, it was determined that postural muscles were also in need of
strengthening. In order to focus on gaining muscle strength while avoiding hypertrophy, the
patient was asked to complete 3 sets of 6-10 repetitions of each exercise, 3 days per week. Once
the patient was able to complete 3 sets of 10 reps without difficulty, the exercise would be
progressed.
As mentioned previously, a major goal of the intervention plan was to give the patient
exercises that could focus on more than one area of weakness at a time, so as not to overwhelm
her. For this reason, based upon general upper extremity weakness and postural issues, D2 PNF

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 15
extension was chosen as a strength exercise. D2 PNF extension includes shoulder flexion,
abduction and external rotation, and forearm supination. As the patient worked seated in an
office chair for a significant portion of the day, it was determined than an exercise that included
both upper extremity strengthening and an extension movement would be of significant benefit
to both strength and posture.
Figure 1. D2 PNF Extension
Based upon her plank time of 11 seconds, it was determined that the patient needed
significant core work. Improving core strength would also benefit the patient’s posture and gait.
In order to start the patient at an approachable level, it was determined that supine, hook-lying
Transverse Abdominus (TA) holds were indicated. This exercise would teach the patient both
how to properly contract her TA and to develop basic TA strength and endurance. After the
patient could complete 3 sets of 10 second holds without difficulty, the exercise was progressed
to supine, hook-lying TA steps.
Figure 2. Transverse Abdominus Steps

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 16
Finally, to further address deficits in posture, Seated Rows were added to the
intervention plan. When performed properly, seated rows work to strengthen postural muscles
of the back, and also provide an extension moment to work against the flexed posture assumed
in an office setting. The patient was instructed to keep the shoulder blades squeezed together
throughout the duration of a set of rows, since the postural muscles of the back are constantly
firing to provide postural support. Once the patient could complete 3 sets of 10 repetitions
without difficulty, the resistance would be increased. A “Strength Log” was developed for the
patient to use to keep track of her cardiovascular exercise, a copy of which is included in the
Appendix.
Figure 3. Seated Row
Developing a flexibility routine was slightly more straightforward. From the muscle-
length tests conducted in the initial evaluation, it was determined which areas of the body
required additional flexibility to increase overall function. For the case patient, these areas were
the pectorals, quadriceps, and the TFL/IT band. For all stretches, it was recommended the
patient perform them daily, and all would involve three sets of 30-second static holds (Lim,
Nam, & Jung 2014). Care was taken to instruct the patient not to ‘bounce’ at the end of the
stretch, as this would activate the quick stretch reflex and reduce effectiveness of the
intervention.

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 17
To increase the flexibility of the pectorals, it was determined that the patient should
perform a Doorway (Y) Stretch. This would address the deficit the patient presented in the initial
evaluation, where forward flexion of the shoulder was limited. For quadriceps tightness, a
Standing Quad Stretch was recommended. This would allow the patient to grade the force of
the stretch, and to increase knee flexion as flexibility progressed. Finally, for the TFL and IT band,
the Side-Lying Table Stretch was chosen. The stretch position is similar to Ober’s Test, while
allowing the superior leg to experience a passive stretch in the target areas.
Figure 4. Doorway (Y) Stretch, Standing Quad Stretch, and Side-Lying Table Stretch
Developing the patient’s nutrition plan was a slightly different process. Since it is
beyond the scope of physical therapy to offer specific nutrition and/or dietary advice, a
combination of general advice and recommendations were developed based upon the patient
interview. During the initial evaluation, the patient stated that she rarely ate breakfast, snacked
frequently, and ate a diet heavily influenced by Latino cuisine (rice, beans, chicken, pork, beef).
In addition, the patient reported she does not enjoy the majority of fruits or vegetables, with
the exception of corn.
Based upon this information, it was recommended that the patient begin having
breakfast on a regular basis. (Mekary, Giovannucci, Cahhill, Willett, Dam, & Hu, 2013) Skipping
breakfast combined with a low fruit and vegetable diet could significantly affect fiber intake, so

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 18
it was also recommended that the patient attempt to try one new fruit or vegetable per week in
the hopes of finding something she would enjoy enough to incorporate into her diet. Finally, it
was recommended that the patient attempt to reduce the amount of snacking during the day,
and replace her normal snack foods with healthier alternatives such as vegetable chips or fruits.
In addition, it was recommended that the patient set up an account on MyPlate, a website
sponsored by the United States Department of Agriculture. The website offers several tips and
instructions on how to improve diet, and has many links to other applicable resources.
During the course of the 3 week intervention period, there was a midterm appointment
that took place on intervention day 10. During this meeting, the patient was asked how the
intervention plan was progressing, and if she had any questions about any of her assigned
exercises. Several modifications and progressions were made to the intervention plan based on
this meeting. Cardiovascular exercise was progressed from 15 to 30 minute sessions, as the
patient had already progressed herself to this level. The TA exercise was progressed from a
static hold to supine marches. The patient was also corrected on proper form for the seated
rows; to this point, she had been excessively elevating her shoulders. She was instructed on a
standing variation of the TFL/IT band stretch and instructed to perform whichever version was
more convenient for her. Finally, it was suggested that the patient try to plan out meals ahead
of time to try and improve general nutrition, after she mentioned difficulty in meeting nutrition
goals.
Outcomes
The final examination was performed on intervention day 22 to determine patient
outcomes based on the intervention plan. All tests and measures relevant to the intervention
plan were re-assessed, and included baseline vital signs, body composition (height, weight,
waist-to-hip ratio, 7-site skinfold), balance and strength tests (single-leg stance, 30 second sit-to-

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 19
stand, modified pushup, plank test, 6-minute walk), flexibility screen (pectorals, hip flexors,
TFL/ITB), and the four psychosocial questionnaires. The results of the re-assessment are shown
in comparison to the initial assessment in Tables 3 and 4.
Table 3 Initial vs. Final Examination Data
Final Evaluation values are shown in shaded cells
Table 4 Psychosocial Survey Results
Discussion
Comparison of the pre- and post-intervention data leads to several promising
conclusions, as well as a few areas of concern. It can be seen in Table 3 that the patient’s
diastolic blood pressure on the day of the follow-up was markedly higher than on the initial
evaluation, both at rest and after the 6-minute walk test. This could be due in part to the
patient’s report of having consumed salty food earlier that day. However, the patient reported
no distress at any point in the follow-up. Regardless, the patient was informed of her elevated
Blood Pressure 150/88 148/98 Height 55.5in 55.5in Single-leg Stance 7s R 11s R
Respiratory Rate 24 22 Weight 177lbs 173lbs 6s L 8s L
O2 Sat 97% 98% BMI 40.4 39.5 Modified Pushup 17 rep 16 rep
Heart Rate 96 98 Waist 118.5cm 105.5cm 30s sit-to-stand 12 rep 13 rep
Hip 122cm 118.5cm Plank 11s 33s
Waist-Hip Ratio 0.97 0.89
7-site Skinfold 39% 43%
6-minute Walk 420m 424m Pectoral 150deg FF 165deg FF
BP 152/90 150/108 Hip Flexors + Thomas Bil + Thomas Bil
HR 114 112 TFL/ITB +Ober Bil +Ober Bil
O2 sat 98% 98%
6-minute Walk Flexibility
Resting Vitals Body Composition Balance and Strength
Name Scoring
Initial Exam Final Exam
Physical Activity Self-efficacy 0 - 5, 5 is better 2.20 3.20
Physical Activity Decisional Balance 1 - 5, 5 is better 4.20 4.50
1 - 5, 1 is better 1.80 1.50
Physical Activity Process of Change 1 - 5, 5 is better 2.98 3.78
Expected Outcomes and Barriers
for Habitual Physical Activity1 - 5, 5 is better 2.92
Patient Average
2.54

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 20
diastolic blood pressure, and was advised to monitor her blood pressure over the coming days
to ensure the elevation was temporary. The patient was also advised to seek medical follow-up
with her primary healthcare provider, particularly in the event of repeated or sustained
elevation of blood pressure equal or above 140/90 as per the National Institutes of Health
Guidelines for diagnosis and treatment of hypertension.
The second area of concern was in the 7-site skinfold test. A significant increase in
estimated body fat percentage was noted between the initial and final evaluations; however,
the author recommends that this number be interpreted within the context of several mitigating
factors. On the initial examination date, the patient was wearing casual fitness clothing, while
on the final evaluation they had not had time to change out of their medical scrubs. The
increased thickness of the scrubs’ material could lead to inflated skinfold measurements. In
addition, the author had minimal experience in using the skinfold calipers prior to this case
study, so the intra-rater reliability of the measurements can be called into question. It has also
been cited that variations of 2 to 3mm have been seen in repeated skinfold measurements
when comparing novice and experienced clinicians. (Burkinshaw, Jones, & Krupowicz, 1973)
Finally, since every other body composition measurement showed improvements, the results of
the 7-site skinfold test can be called into question.
As far as all other body composition measurements are concerned, the patient made
significant gains in all areas. Over the brief 22-day intervention period, the patient lost 4 pounds,
leading to a BMI decrease from 40.4 to 39.5, which moved her from Grade III or morbid obesity
to Grade II obesity. In addition, one of the greatest improvements came in the waist-to-hip ratio.
The patient’s waist circumference fell from 118.5cm to 105.5cm, while her hip circumference
fell from 122cm to 118.5cm. This significant decrease led to a waist-to-hip ratio that fell from
0.97 to 0.89. While all these numbers are laudable, the decrease in waist circumference of 13cm

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 21
(11.61%) is especially noteworthy, as increased waist circumference has been linked to
increased visceral adipose tissue and increased risk of obesity-related diseases (National
Institutes of Health, 2016; Kopelman, 2007).
The results of the balance and strength tests showed mixed, but generally positive
results. While specific balance-focused interventions were not included in the intervention plan
for reasons of manageability, the patient still improved single-leg stance time bilaterally. One
fewer pushup was recorded in the modified pushup test, but the patient did exhibit improved
form during the test. The improved form may be attributed to increased core strength in
combination with increased upper extremity muscular control. The 30 second sit-to-stand was
improved by one repetition, again despite having no specific interventions focused on lower
extremity strengthening. However, this result could be attributed to the patient’s cardiovascular
exercise plan, which included a good deal of dancing. Perhaps the greatest improvement in this
area came in the plank test, where the patient improved from an 11 second hold in the initial
evaluation to a 33 second hold in the final. This significant improvement shows the results of
one of the main areas of focus for the intervention plan. Core strength was given high
importance, as improving core strength and control could lead to benefits in posture, gait, and
functional movement.
Improvements in flexibility from initial to final examination were more nuanced. The
most significant improvement was seen in pectoral muscle length. In the initial examination, the
patient demonstrated a deficit of 30o in forward shoulder flexion of the right arm. Upon final
examination, this had been reduced to a 15o deficit. Upon initial examination, the patient also
demonstrated positive Thomas and Ober tests bilaterally, signifying reduced flexibility of the hip
flexors and the Tensor Fascia Latae/Iliotibial Band. While both tests were still positive upon final

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 22
examination, this could be due to the brief duration of the intervention period, or the binary
nature (positive or negative) of the Thomas and Ober tests.
The final test performed in both examinations was the 6-minute walk test. Upon
completion of the intervention period, the patient saw an increase in walking distance of 4
meters, while heart rate and oxygen saturation remained unchanged. As mentioned previously,
the increase in diastolic blood pressure seen at rest was also present after the 6-minute walk
test, and was discussed with the patient. While the patient’s demographic is not well
represented in study data, based upon the minimal detectable change for other patient
populations, the patient did not have a significant improvement in walk distance. (Perera, Mody,
Woodman, & Studenski, 2006; Kennedy, Stratford, Wessel, Gollish, & Penny, 2005) Since the
patient reported good adherence to the cardiovascular exercise plan, this result may be
explained either by the short duration of the study period, or possible over-reporting of the
patient.
Finally, and perhaps more to the core interest of this case study, were the results of the
psychosocial questionnaires. Table 4 shows the comparison of the questionnaire results
between the initial and final examinations. The results show obvious improvements in three out
of the four questionnaires, with only the Expected Outcomes and Barriers for Habitual Physical
Activity having a decreased score. The significant improvements in the majority of the
questionnaires show great promise for the case patient in the post-intervention period. As
mentioned in the Background and Purpose section, sticking with an exercise program is a
significant challenge to anyone, and the overweight and obese population has further barriers
to overcome. By showing improvements in self-efficacy, decisional balance, and process of
change, the case patient shows that she has put herself in the right frame of mind to continue
with her wellness plan going forward, thus increasing her chances of continued successful

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 23
outcomes. Perhaps the patient’s ability to self-motivate should not come as a revelation; as was
mentioned in the patient history, she had previously successfully quit smoking in 2009.
The results of this case study can have broad applications to the field of physical
therapy. As specialists of function and movement, physical therapists are in a unique position to
offer overweight and obese clients expertise in improving their overall wellness. Especially when
taking into account the patient’s psychosocial state of mind, customized wellness plans can be
developed in order to maximize the chance of patient success through understanding
motivation and potential barriers to success. By following closely with patients, plans can be
tailored such that the patient can continue to succeed in their wellness goals long after
discharge.

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 24
References
Adler, N. and Stuart, J. (2009). Reducing obesity: Motivating action while not blaming the victim. The Milbank Quarterly, 87(1): 49-70.
Annesi, J., Unruh, J. L., Marti, C. N., Gorjala, S., & Tennant, G. (2011). Effects of The Coach
Approach Intervention on Adherence to Exercise in Obese Women: Assessing Mediation
of Social Cognitive Theory Factors. Research Quarterly for Exercise and Sport Rqes, 82(1),
99-108.
Bandura, A. (2004). Health Promotion by Social Cognitive Means. Health Education & Behavior,
31(2), 143-164.
Bastien, M., Poirier, P., Lemieux, I., & Després, J. (2014). Overview of Epidemiology and
Contribution of Obesity to Cardiovascular Disease. Progress in Cardiovascular Diseases,
56(4), 369-381.
Burkinshaw, L., Jones, P. R. M., & Krupowicz, D. W. (1973, May). Observer error in skinfold
thickness measurements. Human Biology, 45(2), 273-279.
Cecchini, M., Sassi, F., Lauer, J., Lee, Y., Guarjardo-Barron, V., and Chisholm, D. (2010). Tackling
of unhealthy diets, physical inactivity, and obesity: health effects and cost-effectiveness.
Lancet, 376: 1775-1784.
Church, T. (2011). Exercise in obesity, metabolic syndrome, and diabetes. Progress in
Cardiovascular Diseases, 53: 412-418.
Dalle Grave, R., Calugi, S., Centis, E., El Ghoch, M., & Marchesini, G. (2010). Cognitive-behavioral
strategies to increase the adherence to exercise in the management of obesity. Journal
of Obesity, 2011 , 1-11.
Dean, E. (2009). Physical therapy in the 21st century (Part I): Toward practice informed by
epidemiology and the crisis of lifestyle conditions. Physiotherapy Theory and Practice,
25(5): 330-353.
Dixon, J. (2010). The effect of obesity on health outcomes. Molecular and Cellular Endocrinology,
316: 104-108.
Enright, P. L. and Sherrill, D. L. (1998). "Reference equations for the six-minute walk in healthy
adults." Am J Respir Crit Care Med 158(5 Pt 1): 1384-1387.
Esmat, T., Ph.D. (2012, January 11). Measuring and Evaluating Body Composition. Retrieved July
21, 2016, from http://www.acsm.org/public-
information/articles/2012/01/12/measuring-and-evaluating-body-composition
Flegal, K., Carroll, M., Ogden, C., and Curtin, L. (2010). Prevalence and trends in obesity among
US adults, 1999-2008, JAMA, 303(3): 235-241.

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 25
Henry, K. D., Rosemond, C., & Eckert, L. B. (1999). Effect of Number of Home Exercises on
Compliance and Performance in Adults Over 65 Years of Age. Physical Therapy, 79(3),
270-277.
Hopps, E. and Caimi, G. (2011). Exercise in obesity management, Journal of Sports Medicine and
Physical Fitness, 51, 275.
Jacobs, J. V., Horak, F. B., Tran, V. K., & Nutt, J. G. (2005). Multiple balance tests improve the
assessment of postural stability in subjects with Parkinson's disease. Journal of
Neurology, Neurosurgery & Psychiatry, 77(3), 322-326.
Kennedy, D. M., Stratford, P. W., Wessel, J., Gollish, J. D., & Penney, D. (2005). Assessing stability
and change of four performance measures: A longitudinal study evaluating outcome
following total hip and knee arthroplasty. BMC Musculoskeletal Disorders BMC
Musculoskelet Disord, 6(1), 1.
Kopelman, P. (2007). Health risks associated with overweight and obesity, Obesity Reviews, 8
(Suppl 1): 13-17.
Lim, K., Nam, H., & Jung, K. (2014). Effects on Hamstring Muscle Extensibility, Muscle Activity,
and Balance of Different Stretching Techniques. J Phys Ther Sci Journal of Physical
Therapy Science, 26(2), 209-213. doi:10.1589/jpts.26.209
Linde, J., Rothman, A., Baldwin, A., and Jeffrey, R. (2006). The impact of self-efficacy on behavior
change and weight change among overweight participants in a weight loss trial. Health
Psychology, 25(3): 282-291.
Marcus, B. and Lewis, B. (2003). Physical activity and the stages of motivational readiness to
change model. Research Digest: The President’s Council on Physical Fitness and Sports,
4(1): 1-8.
Marcus, B., Selby, V., Niaura, R. and Rossi, J. (1992). Self-efficacy and the stages of exercise
behavior change. Research Quarterly for Exercise and Sport, 63: 60-66.
Mekary, R. A., Giovannucci, E., Cahill, L., Willett, W. C., Dam, R. M., & Hu, F. B. (2013). Eating
patterns and type 2 diabetes risk in older women: Breakfast consumption and eating
frequency. American Journal of Clinical Nutrition, 98(2), 436-443.
National Institutes of Health. (2016). Aim for a healthy weight.
http://www.nhlbi.nih.gov/health/educational/lose_wt/menuplanner.html
Noble, R. E. (2001). Waist-to-hip ratio versus BMI as predictors of cardiac risk in obese adult
women. Western Journal of Medicine, 174(4), 777-780.
Perera, S., Mody, S. H., Woodman, R. C., & Studenski, S. A. (2006). Meaningful Change and
Responsiveness in Common Physical Performance Measures in Older Adults. Journal of
the American Geriatrics Society, 54(5), 743-749.

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 26
Sack, S., Radler, D., Mairiella, K., Tougher-Decker, R., and Khan, H. (2009). Physical therapists’
attitudes, knowledge, and practice approaches regarding people who are obese.
Physical Therapy, 89: 804-815.

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 27
Appendix A – Exercise and Strength Logs
Date Type of Cardio Performed Duration Maximum HR
Date Type of Cardio Performed Duration Maximum HR
Date Type of Cardio Performed Duration Maximum HR
Date Type of Cardio Performed Duration Maximum HR
Date Type of Cardio Performed Duration Maximum HR
Exercise Log
Notes:
Notes:
Notes:
Notes:
Notes:

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 28
Appendix A (continued)
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Date Exercise Performed Sets Reps
Strength Log

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 29
Appendix B – Psychosocial Surveys
Physical Activity Self-efficacy Questionnaire:
Please Rate the 5 components on a personal level based on the criteria below:
0=not at all confident, 5 = extremely confident
I am confident I can participate in exercise when:
1. I am tired 0 1 2 3 4 5
2. I am in a bad mood 0 1 2 3 4 5
3. I feel I don’t have the time 0 1 2 3 4 5
4. I am on vacation 0 1 2 3 4 5
5. It is raining or snowing 0 1 2 3 4 5

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 30
Appendix B (continued)
Physical Activity Decisional Balance:
Please Rate the following Pros and Cons 1-5 based on the criteria below:
1 = Not important at all
5 = very important
Pros:
1. I would have more energy for my family and friends if I exercised regularly.
1 2 3 4 5
2. Regular exercise would help me relieve tension.
1 2 3 4 5
3. I would feel more confident if I exercised regularly.
1 2 3 4 5
4. I would sleep more soundly if I exercised regularly.
1 2 3 4 5
5. I would feel good about myself if I kept my commitment to exercise regularly.
1 2 3 4 5
6. I would like my body better if I exercised regularly.
1 2 3 4 5
7. It would be easier for me to perform routine physical tasks if I exercised
regularly.
1 2 3 4 5

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 31
Appendix B (continued)
8. I would feel less stressed if I exercised regularly
1 2 3 4 5
9. I would feel more comfortable with my body if I exercised regularly.
1 2 3 4 5
10. Regular exercise would help me have a more positive outlook on life.
1 2 3 4 5
Cons:
1. I think I would be too tired to do my daily work after exercising.
1 2 3 4 5
2. I would find it difficult to find an exercise activity that I enjoy that is not affected
by bad weather.
1 2 3 4 5
3. I feel uncomfortable when I exercise because I get out of breath and my heart
beats very fast.
1 2 3 4 5
4. Regular exercise would take too much of my time.
1 2 3 4 5
5. I would have less time for my family and friends if I exercised regularly.
1 2 3 4 5

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 32
Appendix B (continued)
6. At the end of the day, I am too exhausted to exercise.
1 2 3 4 5

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 33
Physical Activity Processes of Change Questionnaire
Physical activity or exercise includes activities such as walking briskly, jogging, bicycling,
swimming, and any other activity in which the exertion is at least as intense as these activities.
The following experiences can affect the exercise habits of some people. Think of any
similar behaviors you may currently have or have had during the past. Then rate how frequently
the behavior occurs. Please circle the number that best describes your answer for each
experience.
How frequently does this occur?
1 = never
2 = seldom
3 = occasionally
4 = often
5 = repeatedly
1. Instead of remaining inactive, I engage in some physical activity. 1 2 3 4 5
2. I tell myself I am able to be physically active if I want to. 1 2 3 4 5
3. I put things around my home to remind me to by physically active. 1 2 3 4 5
4. I tell myself that if I try hard enough, I can be physically active. 1 2 3 4 5
5. I recall information people have personally given me on the benefits of 1 2 3 4 5
physical activity.
6. I make commitments to by physically active. 1 2 3 4 5
7. I reward myself when I am physically active. 1 2 3 4 5
8. I think about information from articles and advertisements on how to make 1 2 3 4 5
physical activity a regular part of my life.
9. I keep things around my place of work that remind me to be physically 1 2 3 4 5
active.
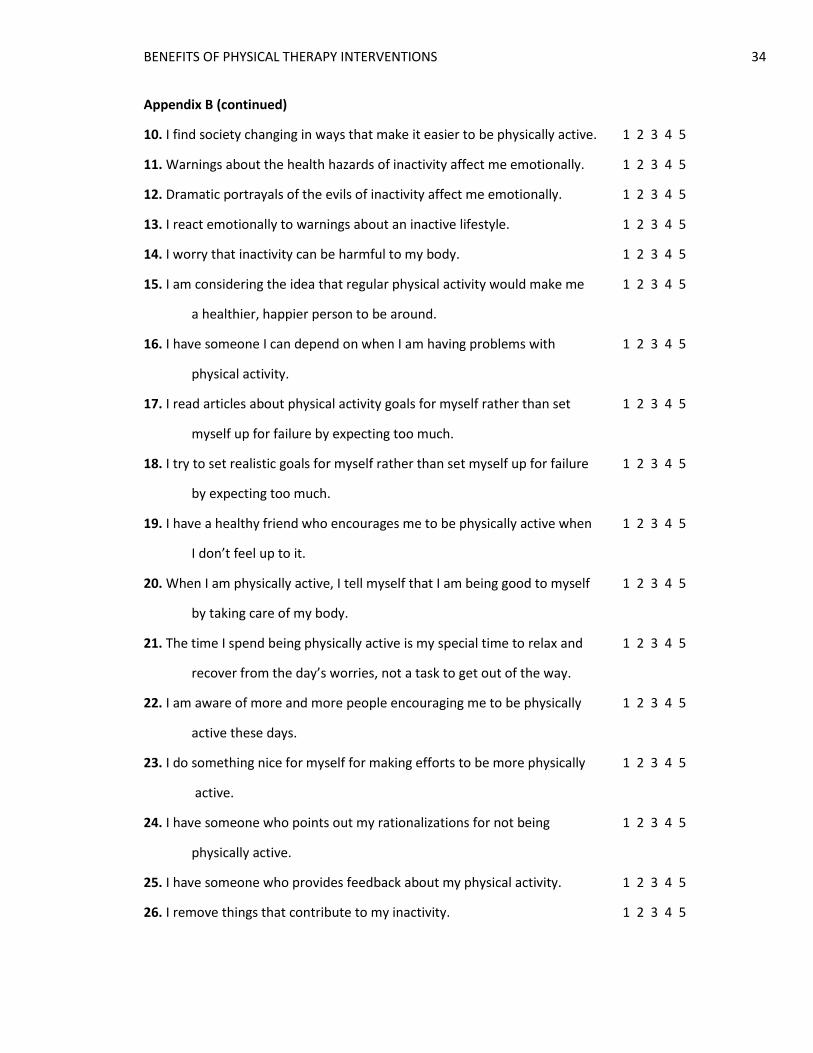
BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 34
Appendix B (continued)
10. I find society changing in ways that make it easier to be physically active. 1 2 3 4 5
11. Warnings about the health hazards of inactivity affect me emotionally. 1 2 3 4 5
12. Dramatic portrayals of the evils of inactivity affect me emotionally. 1 2 3 4 5
13. I react emotionally to warnings about an inactive lifestyle. 1 2 3 4 5
14. I worry that inactivity can be harmful to my body. 1 2 3 4 5
15. I am considering the idea that regular physical activity would make me 1 2 3 4 5
a healthier, happier person to be around.
16. I have someone I can depend on when I am having problems with 1 2 3 4 5
physical activity.
17. I read articles about physical activity goals for myself rather than set 1 2 3 4 5
myself up for failure by expecting too much.
18. I try to set realistic goals for myself rather than set myself up for failure 1 2 3 4 5
by expecting too much.
19. I have a healthy friend who encourages me to be physically active when 1 2 3 4 5
I don’t feel up to it.
20. When I am physically active, I tell myself that I am being good to myself 1 2 3 4 5
by taking care of my body.
21. The time I spend being physically active is my special time to relax and 1 2 3 4 5
recover from the day’s worries, not a task to get out of the way.
22. I am aware of more and more people encouraging me to be physically 1 2 3 4 5
active these days.
23. I do something nice for myself for making efforts to be more physically 1 2 3 4 5
active.
24. I have someone who points out my rationalizations for not being 1 2 3 4 5
physically active.
25. I have someone who provides feedback about my physical activity. 1 2 3 4 5
26. I remove things that contribute to my inactivity. 1 2 3 4 5

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 35
Appendix B (continued)
27. I am the only one responsible for my health, and only I can decide 1 2 3 4 5
whether or not I will be physically active.
28. I look for information related to physical activity. 1 2 3 4 5
29. I avoid spending long periods of time in environments that promote 1 2 3 4 5
inactivity.
30. I feel that I would be a better role model for others if I were regularly 1 2 3 4 5
physically active.
31. I think about the type of person I would be if I were physically active. 1 2 3 4 5
32. I notice that more businesses are encouraging their employees to 1 2 3 4 5
be physically active by offering fitness courses and time off to work out.
33. I wonder how my inactivity affects those people who are close to me. 1 2 3 4 5
34. I realize that I might be able to influence others to be healthier if I would 1 2 3 4 5
be more physically active.
35. I get frustrated with myself when I am not physically active. 1 2 3 4 5
36. I am aware that many health clubs now provide babysitting services to 1 2 3 4 5
their members.
37. Some of my close friends might be more physically active if I were. 1 2 3 4 5
38. I consider the fact that I would feel more confident in myself if I were 1 2 3 4 5
regularly physically active.
39. When I feel tired, I make myself be physically active anyway because I 1 2 3 4 5
know I will feel better afterward.
40. When I’m feeling tense, I find physical activity a great way to relieve 1 2 3 4 5
my worries.

BENEFITS OF PHYSICAL THERAPY INTERVENTIONS 36
Appendix B (continued)
Expected Outcomes and Barriers for Habitual Physical Activity:
Please Rate the following Pros and Cons 1-5 based on the criteria below:
1 = strongly disagree
5 = strongly agree
1. Self-conscious about my looks when I do activities 1 2 3 4 5
2. Lack of interest in physical activity 1 2 3 4 5
3. Lack of self-discipline or willpower 1 2 3 4 5
4. Lack of time 1 2 3 4 5
5. Lack of energy 1 2 3 4 5
6. I do not have anyone to do physical activities with me 1 2 3 4 5
7. I do not enjoy physical activity 1 2 3 4 5
8. I hate to fail, so I do not try 1 2 3 4 5
9. Lack of equipment 1 2 3 4 5
10. The weather is bad 1 2 3 4 5
11. Lack of skills 1 2 3 4 5
12. I am usually too tired to exercise 1 2 3 4 5
13. Lack of knowledge on how to do physical activities 1 2 3 4 5
14. Poor health 1 2 3 4 5
15. Fear of injury 1 2 3 4 5
16. Physical activity is hard work 1 2 3 4 5
17. Lack of convenient place to do physical activity 1 2 3 4 5
18. I am too overweight 1 2 3 4 5
19. Physical activity is too boring 1 2 3 4 5
20. Minor aches and pains 1 2 3 4 5
21. Work demands 1 2 3 4 5
22. Social demands 1 2 3 4 5
23. Family demands 1 2 3 4 5
24. Lack of money 1 2 3 4 5





























