Embed Size (px)
Citation preview

REPRESENTED EMPLOYEESTHE JOHNS HOPKINS HOSPITAL
BenefitsGuide to

IMPORTANT INFORMATION
Aflac
Bright Horizons
Care.com/BackupCare
CareWorks Absence Management
Delta Dental
EHP
Employee After-Hours Clinic
Empolyee Health & Wellness Center
Employee Labor Relations
Faculty & Staff Assistance Program(FASAP)
Healthy at Hopkins
HR Solutions Center
Hyatt Legal Plans
Johns Hopkins FederalCredit Union
MetLife
Occupational Health
Transamerica
UNUM
WageWorks
Workers’ Compensation
WORKLife Programs
1-800-443-3036
410-614-4111
855-781-1303
844-263-3121
1-800-932-0783
1-800-557-6916410-424-4450410-762-5312
410-955-7374
410-614-1620
410-955-6783
443-997-7000
410-955-9538
443-997-5400
800-821-6400
410-534-4500800-543-2870
800-GET-MET8
410-955-6211
410-955-5828800-755-5801
800-227-4165800-633-7479800-421-0344800-635-5597800-635-5597
855-774-7441877-502-6272
410-955-6433
443-997-7000
www.aflacgroupinsurance.com
www.jhbrighthorizons.org
www.care.com/backupcare
http://timeoff.careworksabsence.com
www.deltadentalins.com
www.ehp.org
http://www.hopkinsmedicine.org/human_resources/benefits/healthy_at_hopkins/
http://www.hopkinsmedicine.org/human_resources/benefits/healthy_at_hopkins/
www.hopkinsmedicine.org/jhhr
www.fasap.org
www.healthyathopkins.org
www.legalplans.com access code: 1380010
www.jhfcu.org
www.metlife.com/mybenefits
www.hopkinsmedicine.org/hse/occupation_health/
www.hopkinsmedicine.org/jhhr/pensionjhm.trsretire.com
http://unuminfo.com/hopkinsmedicinewww.unum.com
www.wageworks.com
www.hopkinsmedicine.org/hse/workers_compensation/
www.hopkinsworklife.org
Johns HopkinsFamily Day Care Center
Back Up Child & Adult Care
FML/LOA
Dental Customer Service
Care Management ProgramClaims or Coverage Questions
Short Term Disability
HR Solution Center
Prepaid Legal
Auto & Homeowners InsurancePet Insurance
403(b)
Long Term CareLong Term Disability
Life InsuranceGroup AccidentGroup Whole Life
Flexible Spending QuestionsCobra Questions

Memorandum
To: JHH Represented Employees
From:
Date: Effective January 1, 2018
Re: Summary Plan Description
The Johns Hopkins Summary Plan Description of Benefit Plans (SPD) gives detailed information
contains the identity of the plan administrator, the requirements for eligibility and participation in the plan, circumstances that may result in disqualification or denial of benefits, and the identity of any insurers.
The SPD can be retrieved from the Benefits section of the Human Resources website www.hopkinsmedicine.org/human_resources. Click on the Benefits tab at the top of the page and then “Benefits Guides and Summary Plan Descriptions”.
The SPD displays specific information in reference to:
Next, click on the Summary Plan Description for Represented (Union) employees.
1974about the plan provided under Employment Retirement Income Security Act of (ERISA). It
Wellness, Benefits & Retirement Office
• Retirement & 403(b) Plans• Medical, Dental, Short Term Disability• Long Term Disability Insurance• Basic Life Insurance
If you would like a free hardcopy of any of the resources listed above, or if you have any benefitsrelated questions, contact [email protected] or 443-997-5400.

2 2018 Guide to Benefits
IntroductionBecause we value the people who work here, The Johns
Hopkins Hospital is proud of the collection of benefits made
available to you. Since the benefits provided to you are an
important part of your total compensation package as a
Hopkins employee, you are encouraged to take some time to
read this guide and become familiar with its contents. This
guide gives you a brief overview of the benefits offered and is
not intended to be a complete source of information on the
plans.

3Represented Employees
EligibilityEMPLOYEESAll employees regularly scheduled to work 20 hours or more per week and weekend option nurses are eligible formost benefits. For all benefits except Paid Time Off, Short Term Disability and Tuition Assistance, coverage fornew hires or newly eligible employees is effective the first day of the month following date of hire or eligibilitywith completion of the enrollment process. All newly hired employees have 30 days from date of hire to com-plete their enrollment. For Short Term Disability benefits, employees scheduled to work 20 or more hours perweek are eligible after completion of a 90-day probationary period.
DEPENDENTSWhen you enroll in a medical, dental, vision and/or dependent life insurance plan, you may also elect coveragefor:• Your children (with submission of birth license & social security number) up to age 26 regardless of studentor marital status
• Your legal spouse (with submission of certified marriage certificate & social security number)
If your spouse works for JHH/JHHSC, you cannot be covered as both an employee and adependent. In addition, your eligible dependents may only be covered under one plan.
FAMILY STATUS CHANGESOutside of the annual Open Enrollment period, the only time during the plan year that you can add or dropcoverage for dependents is when you have a family status change. Qualifying events include: marriage or divorce,birth or adoption of a child, death of a dependent, gain or loss of a spouse.
To make a mid-year change in benefits, you must provide written proof of your family status change to thebenefits office within 30 days of the qualifying event.
Wellness BenefitsAs a leader in health care, the Johns Hopkins Health System is committed to promoting healthy lifestyles andsupporting our employees by creating an overall culture of health and well-being within the Johns Hopkins com-munity. Johns Hopkins employees can take advantage of a wide variety of programs and resources so that younever have to manage your health without help including onsite staff who are available to answer questions tohelp you quit smoking, manage your weight, or improve your fitness and/or diet.
The Healthy at Hopkins initiative is one way we assist our staff members in taking charge of their health. Inkeeping with our decision to continually invest in our employees and the resources available that support andempower their well-being, we have created a new online portal. The Healthy at Hopkins portal will provide aone-stop shop for employee health resources and information. It gives you access to our new Healthy at HopkinsRewards Program, health/wellness coaching, integration of data with wearable devices and phone apps, trackingtools, and access to an extensive library of Johns Hopkins sponsored health information.
With our quarterly rewards program, employees will complete activities to earn points for a $20 bi-weekly reward(full time 30+ hours/week - $520 maximum annually; part time 20-29 hours/week - $25 each quarter/$100maximum annually.)
To get started go to my.jh.edu site and on the home page click the Healthy at Hopkins logo.

4
NEW TOBACCO TESTING PROCESS FOR EMPLOYEESOFFERS REWARDSA voluntary tobacco testing process takes effect this year as part of the 2018 benefit enrollment to reward em-ployees who don’t use tobacco. The benefit is being rolled out across many Johns Hopkins Health System enti-ties to promote employee health as outlined in the Strategic Plan. To find out more about the process and read alist of frequently asked questions, please go to:http://www.hopkinsmedicine.org/human_resources/benefits/tobacco-testing.html
Those who take the test and pass will receive a $11.03 per pay credit on their health insurance premium for2018. Employees enrolling in healthcare benefits who do not wish to receive the credit do not need to partici-pate in tobacco testing.
Medical BenefitsJohns Hopkins Employer Health Programs (EHP) is a frexible medical plan that offers low deductibles, and outof pocket limits that protect you from catastrophic costs. You can choose providers from one of three networks:
• Hopkins Preferred- Services covered at 90% of the allowed amount. Employees will pay 10% of the costafter all deductible and co-pays have been applied.
• EHP- Services from providers in the EHP network will be covered at 80%. Employees will pay 20% after alldeductibles and co-pays have been applied.
• Out of network- Services from providers at facilities outside of the Johns Hopkins Medicine and EHPnetwork will be covered at 70% of the reasonable and customary rate after all deductibles and copays havebeen applied. Employees may be balanced billed by the provider.
MULTIPLANMultiPlan is an extended provider network consisting of over 600,000 providers nationwide. Multiplan’s PHCSHealthy Directions Network is available for services rendered outside of the state of Maryland and is consideredthe same as EHP in-network benefits. To find a MultiPlan PHCS Healthy Directions network provider outsidethe state of Maryland, visit www.multiplan.com.
SPECIALTY APPOINTMENT LINE 1-866-206-7210The Johns Hopkins EHP Specialty appointment line helps facilitate “new” timely appointments for specialtycare with “Hopkins Preferred Providers”. It was designed to assist EHP members of Johns Hopkins CommunityPhysicians, Johns Hopkins Healthcare, The Johns Hopkins Hospital, Johns Hopkins Health System Corpora-tion, and Johns Hopkins Medicine International.
VISIONWhen you enroll in the Johns Hopkins EHP medical plan, your vision benefits are included. A full range of op-tometry and ophthalmology vision care services, administered on an annual basis, from any in-network or out-of-network provider, are available. If you receive care from a non-network provider, your benefits will be limitedand you will pay more money for certain services.
PHARMACYWhen you enroll in the Johns Hopkins EHP medical plan, the prescription drug benefit is included. This four-tier benefit structure offers savings for using EHP’s approved drug formulary listing. There is a mail order op-tion for most maintenance medications. Visit www.ehp.org and search “pharmacy” for details.
TERMS YOU SHOULD KNOWAllowed Benefit:The reimbursement amount the plan has contractually negotiated with network providers toaccept as full payment. Nonparticipating (out-of-network) providers are not obligated to accept the allowed ben-efit as payment in full and may charge more (balance bill) than the plan’s allowed benefit. For example, in the
2018 Guide to Benefits
Represented Employees 5
charts that follow, if it indicates a service is covered at 90%, you only pay 10% of the allowed benefit up to yourout of pocket maximum. If it indicates the service is covered at 70% out-of-network, it means the plan pays 70%of the allowed benefit. You are responsible for 30% of the cost of services or supplies, including any amountabove the plan’s allowed benefit, when you receive services from nonparticipating (out-of-network) providers.
Balance Billing:When a provider bills you for the difference between the out-of-network provider’s charge andthe allowed amount. For example, if the provider’s charge is $100 and the allowed amount is $70, the providermay bill you for the remaining $30. An in-network, participating provider or facility may not balance bill youfor covered services.
Coinsurance:The percentage of the cost you and the plan pay for a covered expense. Coinsurance is differentfor services received from in-network providers and out-of-network providers.
Copayment:The fixed dollar amount an employee or covered dependent pays at the time service is rendered.This money goes directly to the health care provider.
Deductible:The amount an employee or covered dependent is required to pay before your medical plan paysbenefits for care.
EHP Network Providers: Providers/facilities that have contracts with EHP and have agreed to accept certainfees for their services. These providers and facilities will submit the insurance claim to EHP on your behalf. Youare responsible for any applicable copays, deductibles and co-insurance.
Hopkins Preferred Providers: Johns Hopkins Providers/Johns Hopkins facilities that have contracts with EHPand have agreed to accept certain fees for their services. Hopkins Preferred Providers will submit the insuranceclaim to EHP on your behalf. You are responsible for any applicable copays, deductibles and co-insurance.
Out-of-Pocket Maximum:When the total amount of copayments and/or coinsurance you and/or your covereddependents reaches the out-of-pocket limits noted in the charts, the plan will pay 100% of your copays and coin-surance for the remainder of the plan year (through December 31).
Out of Network Providers: Services received from providers/facilities that do not have a contract with EHP.such services are subject to any applicable copays, deductibles and co-insurance. Because the provider/facility isnon-participating, they have the ability to balance bill the member for charges above the allowed benefit amount.
Out-of-Pocket Maximum:The most an employee and their covered dependent(s) will pay out of his or herpocket in deductible and coinsurance charges.
Preauthorization: A decision by your health insurer or plan that a health care service, treatment plan, prescrip-tion drug or durable medical equipment is medically necessary. Sometimes called prior authorization, prior ap-proval or precertification. EHP may require preauthorization for certain services before you receive them, exceptin an emergency. Preauthorization isn’t a promise EHP will cover the cost.

EHP Network Provider Out of Network Provider
Plan Year Deductible
Out-of-Pocket Maximum
Lifetime Maximum
Individual
Family
Individual
Family
$750
$1500
$3500
$7000
MEDICAL SCHEDULE OF BENEFITSHopkins Preferred Network
Provider
$150 (under $50K) / $200 ($50K to $119,999K)/ $300 ($120K and over)
$300 (under $50K) / $400 ($50K to $119,999K)/ $600 ($120K and over)
$1500 (under $50K) / $2000 ($50K to $119,999K)/ $3000 ($120K and over)
$3000 (under $50K) / $4000 ($50K to $119,999K)/ $6000 ($120K and over)
Unlimited
EHP Network Provider Out of Network ProviderHopkins Preferred NetworkProvider
Acupuncture
Allergy Tests& Procedures
Ambulance Transportation
Biofeedback
Chemo & RadiationTherapy
Chiropractic Care
Dialysis
Durable MedicalEquipment
Medically necessary services for anesthesia,
pain control, andtherapeutic purposes
Allergy test
Desensitization materialsand serum
Medically necessarytransport
Biofeedback
Physician visit
Material and treatment
Chiropractor restricted toinitial exam, x-rays, and
spinal manipulations
Chiropractor with PT privileges (physical therapy services)
Medically necessaryservices
Breast pumps(standard) and
related supplies
Contraceptive devices
Custom DME, includingcustom wheelchairs
Custom-moldedorthotics
Insulin pumps, ContinuousGlucose Monitor and
related supplies
Hearing aids
80% of allowed amount; deductibleapplies (20 visit annual maximum
for all networks combined)
80% of allowed amount; deductible applies
80% of allowed amount; deductible applies
100% of allowed amount;deductible applies
80% of allowed amount; deductible applies (pre-authorization required)
80% of allowed amount;deductible applies
80% of allowed amount;deductible applies
80% of allowed amount; deductible applies (20 visit annual maxi-
mum for all networks combined)
Refer to Therapy Section
80% of allowed amount;deductible applies
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
90% of allowed amount; deductible applies (pre-authorization required)
80% of allowed amount; deductible applies (pre-authorization required)
90% of allowed amount;deductible applies
90% of allowed amount; deductibleapplies (Covered only for dependent
children under age 26; up to $1,400 per aid; pre-authorization required; replacement aids once
every 36 monthsall networks combined)
70% of R&C; deductible applies (20 visit annual maximum for
all networks combined)
70% of R&C; deductible applies
70% of R&C; deductible applies
100% of R&C; deductible applies
70% of R&C; deductible applies(pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies (20 visit annual maximum for all
networks combined)
Refer to Therapy Section
70% of R&C; deductible applies(pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies(pre-authorization required)
70% of R&C; deductible applies(pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies (Covered only for dependent
children under age 26; up to $1,400 per aid;
pre-authorization required; replacement aids once every
36 months all networks combined)
90% of allowed amount; deductibleapplies (20 visit annual maximum
for all networks combined)
90% of allowed amount; deductible applies
90% of allowed amount; deductible applies
100% of allowed amount; deductible applies
90% of allowed amount; deductible applies (pre-authorization required)
90% of allowed amount;deductible applies
90% of allowed amount;deductible applies
90% of allowed amount; deductible applies (20 visit annual maxi-
mum for all networks combined)
Refer to Therapy Section
90% at Fresenius/DavitaDialysis Centers: deductible applies
(pre-authorization required)
100% of allowed amount for JohnsHopkins Home Care Group/Pharmaquip;
deductible waived
100% of allowed amount; deductible waived
90% of allowed amount; deductible applies (pre-authorization required)
90% of allowed amount; deductible applies (pre-authorization required)
90% of allowed amount; deductible applies
90% of allowed amount; deductibleapplies (Covered only for dependent
children under age 26; up to $1,400 per aid; pre-authorization required; replacement aids once
every 36 monthsall networks combined)
$150 (under $50K) / $200 ($50K to $119,999K)/ $300 ($120K and over)
$300 (under $50K) / $400 ($50K to $119,999K)/ $600 ($120K and over)
$1500 (under $50K) / $2000 ($50K to $119,999K)/ $3000 ($120K and over)
$3000 (under $50K) / $4000 ($50K to $119,999K)/ $6000 ($120K and over)
6 2018 Guide to Benefits
EHP Network Provider Out of Network ProviderHopkins Preferred NetworkProvider
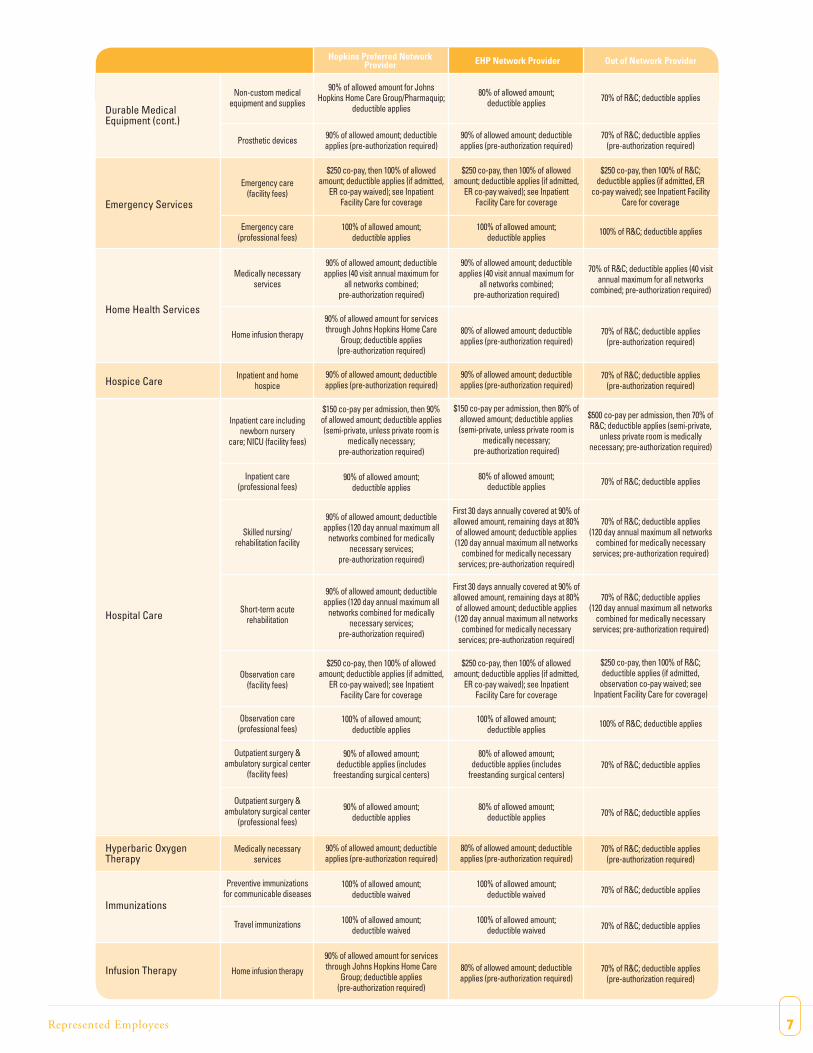
Durable MedicalEquipment (cont.)
Emergency Services
Home Health Services
Hospice Care
Hospital Care
Hyperbaric OxygenTherapy
Immunizations
Infusion Therapy
Non-custom medicalequipment and supplies
Prosthetic devices
Emergency care(facility fees)
Emergency care(professional fees)
Medically necessaryservices
Home infusion therapy
Inpatient and homehospice
Inpatient care includingnewborn nursery
care; NICU (facility fees)
Inpatient care(professional fees)
Skilled nursing/rehabilitation facility
Short-term acuterehabilitation
Observation care(facility fees)
Observation care(professional fees)
Outpatient surgery &ambulatory surgical center
(facility fees)
Outpatient surgery &ambulatory surgical center
(professional fees)
Medically necessaryservices
Preventive immunizationsfor communicable diseases
Travel immunizations
Home infusion therapy
80% of allowed amount; deductible applies
90% of allowed amount; deductibleapplies (pre-authorization required)
$250 co-pay, then 100% of allowedamount; deductible applies (if admitted,
ER co-pay waived); see InpatientFacility Care for coverage
100% of allowed amount;deductible applies
90% of allowed amount; deductibleapplies (40 visit annual maximum for
all networks combined;pre-authorization required)
80% of allowed amount; deductibleapplies (pre-authorization required)
90% of allowed amount; deductibleapplies (pre-authorization required)
$150 co-pay per admission, then 80% ofallowed amount; deductible applies(semi-private, unless private room is
medically necessary; pre-authorization required)
80% of allowed amount;deductible applies
First 30 days annually covered at 90% of allowed amount, remaining days at 80% of allowed amount; deductible applies (120 day annual maximum all networks
combined for medically necessary services; pre-authorization required)
First 30 days annually covered at 90% of allowed amount, remaining days at 80% of allowed amount; deductible applies (120 day annual maximum all networks
combined for medically necessary services; pre-authorization required)
$250 co-pay, then 100% of allowedamount; deductible applies (if admitted,
ER co-pay waived); see InpatientFacility Care for coverage
100% of allowed amount;deductible applies
80% of allowed amount;deductible applies (includes
freestanding surgical centers)
80% of allowed amount;deductible applies
80% of allowed amount; deductible applies (pre-authorization required)
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
80% of allowed amount; deductibleapplies (pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies (pre-authorization required)
$250 co-pay, then 100% of R&C;deductible applies (if admitted, ER
co-pay waived); see Inpatient FacilityCare for coverage
100% of R&C; deductible applies
70% of R&C; deductible applies (40 visitannual maximum for all networks
combined; pre-authorization required)
70% of R&C; deductible applies(pre-authorization required)
70% of R&C; deductible applies(pre-authorization required)
$500 co-pay per admission, then 70% ofR&C; deductible applies (semi-private,
unless private room is medicallynecessary; pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies(120 day annual maximum all networks
combined for medically necessaryservices; pre-authorization required)
70% of R&C; deductible applies(120 day annual maximum all networks
combined for medically necessaryservices; pre-authorization required)
$250 co-pay, then 100% of R&C; deductible applies (if admitted,
observation co-pay waived; seeInpatient Facility Care for coverage)
100% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies(pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies(pre-authorization required)
90% of allowed amount for JohnsHopkins Home Care Group/Pharmaquip;
deductible applies
90% of allowed amount; deductibleapplies (pre-authorization required)
$250 co-pay, then 100% of allowedamount; deductible applies (if admitted,
ER co-pay waived); see InpatientFacility Care for coverage
100% of allowed amount;deductible applies
90% of allowed amount; deductibleapplies (40 visit annual maximum for
all networks combined;pre-authorization required)
90% of allowed amount for servicesthrough Johns Hopkins Home Care
Group; deductible applies(pre-authorization required)
90% of allowed amount; deductibleapplies (pre-authorization required)
$150 co-pay per admission, then 90%of allowed amount; deductible applies(semi-private, unless private room is
medically necessary;pre-authorization required)
90% of allowed amount;deductible applies
90% of allowed amount; deductibleapplies (120 day annual maximum all
networks combined for medicallynecessary services;
pre-authorization required)
90% of allowed amount; deductibleapplies (120 day annual maximum all
networks combined for medicallynecessary services;
pre-authorization required)
$250 co-pay, then 100% of allowedamount; deductible applies (if admitted,
ER co-pay waived); see InpatientFacility Care for coverage
100% of allowed amount;deductible applies
90% of allowed amount;deductible applies (includes
freestanding surgical centers)
90% of allowed amount;deductible applies
90% of allowed amount; deductible applies (pre-authorization required)
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
90% of allowed amount for servicesthrough Johns Hopkins Home Care
Group; deductible applies(pre-authorization required)
7Represented Employees
EHP Network Provider Out of Network ProviderHopkins Preferred NetworkProvider
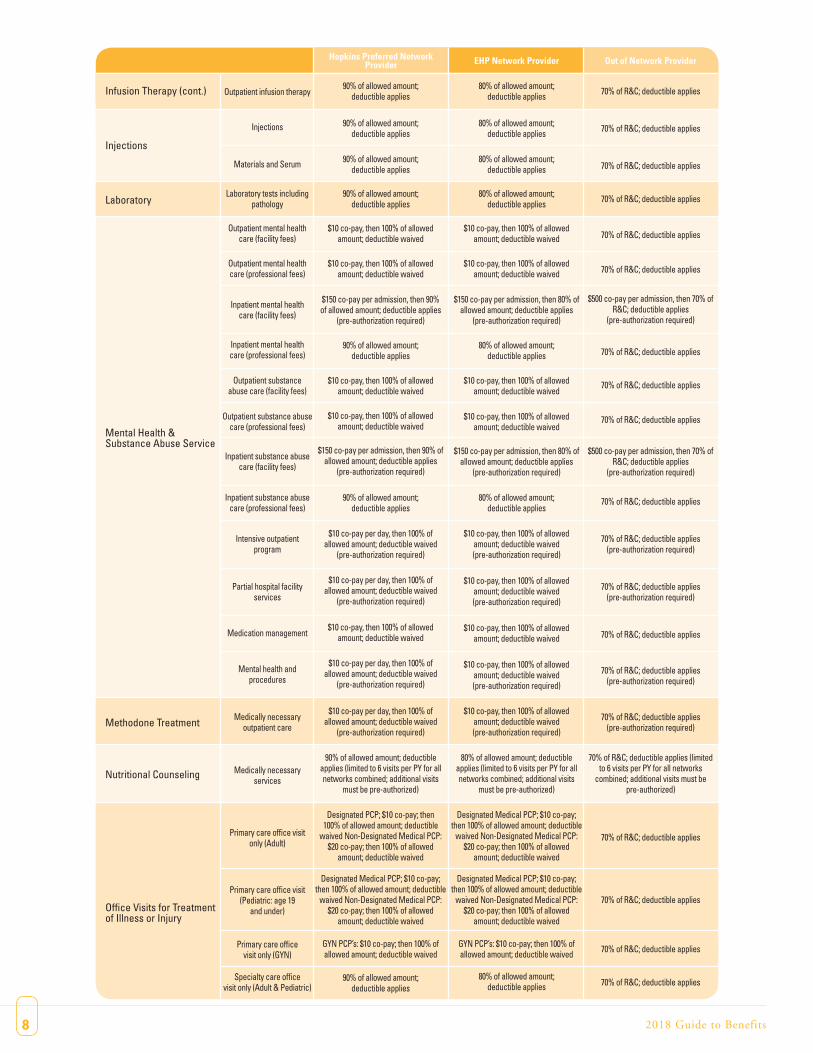
Infusion Therapy (cont.)
Injections
Laboratory
Mental Health &Substance Abuse Service
Methodone Treatment
Nutritional Counseling
Office Visits for Treatmentof Illness or Injury
Outpatient infusion therapy
Injections
Materials and Serum
Laboratory tests includingpathology
Outpatient mental healthcare (facility fees)
Outpatient mental healthcare (professional fees)
Inpatient mental healthcare (facility fees)
Inpatient mental healthcare (professional fees)
Outpatient substanceabuse care (facility fees)
Outpatient substance abusecare (professional fees)
Inpatient substance abusecare (facility fees)
Inpatient substance abusecare (professional fees)
Intensive outpatientprogram
Partial hospital facilityservices
Medication management
Mental health andprocedures
Medically necessaryoutpatient care
Medically necessaryservices
Primary care office visitonly (Adult)
Primary care office visit(Pediatric: age 19
and under)
Primary care officevisit only (GYN)
Specialty care officevisit only (Adult & Pediatric)
80% of allowed amount;deductible applies
80% of allowed amount; deductible applies
80% of allowed amount; deductible applies
80% of allowed amount; deductible applies
$10 co-pay, then 100% of allowedamount; deductible waived
$10 co-pay, then 100% of allowedamount; deductible waived
$150 co-pay per admission, then 80% ofallowed amount; deductible applies
(pre-authorization required)
80% of allowed amount; deductible applies
$10 co-pay, then 100% of allowedamount; deductible waived
$10 co-pay, then 100% of allowedamount; deductible waived
$150 co-pay per admission, then 80% ofallowed amount; deductible applies
(pre-authorization required)
80% of allowed amount; deductible applies
$10 co-pay, then 100% of allowed amount; deductible waived(pre-authorization required)
$10 co-pay, then 100% of allowed amount; deductible waived(pre-authorization required)
$10 co-pay, then 100% of allowed amount; deductible waived
$10 co-pay, then 100% of allowed amount; deductible waived(pre-authorization required)
$10 co-pay, then 100% of allowed amount; deductible waived(pre-authorization required)
80% of allowed amount; deductible applies (limited to 6 visits per PY for all networks combined; additional visits
must be pre-authorized)
Designated Medical PCP; $10 co-pay;then 100% of allowed amount; deductible
waived Non-Designated Medical PCP:$20 co-pay; then 100% of allowed
amount; deductible waived
Designated Medical PCP; $10 co-pay;then 100% of allowed amount; deductible
waived Non-Designated Medical PCP:$20 co-pay; then 100% of allowed
amount; deductible waived
GYN PCP’s: $10 co-pay; then 100% ofallowed amount; deductible waived
80% of allowed amount; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
$500 co-pay per admission, then 70% ofR&C; deductible applies
(pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
$500 co-pay per admission, then 70% ofR&C; deductible applies
(pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies(pre-authorization required)
70% of R&C; deductible applies(pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies(pre-authorization required)
70% of R&C; deductible applies(pre-authorization required)
70% of R&C; deductible applies (limitedto 6 visits per PY for all networks
combined; additional visits must be pre-authorized)
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
90% of allowed amount; deductible applies
90% of allowed amount; deductible applies
90% of allowed amount; deductible applies
90% of allowed amount; deductible applies
$10 co-pay, then 100% of allowedamount; deductible waived
$10 co-pay, then 100% of allowedamount; deductible waived
$150 co-pay per admission, then 90%of allowed amount; deductible applies
(pre-authorization required)
90% of allowed amount;deductible applies
$10 co-pay, then 100% of allowedamount; deductible waived
$10 co-pay, then 100% of allowedamount; deductible waived
$150 co-pay per admission, then 90% ofallowed amount; deductible applies
(pre-authorization required)
90% of allowed amount;deductible applies
$10 co-pay per day, then 100% ofallowed amount; deductible waived
(pre-authorization required)
$10 co-pay per day, then 100% ofallowed amount; deductible waived
(pre-authorization required)
$10 co-pay, then 100% of allowed amount; deductible waived
$10 co-pay per day, then 100% ofallowed amount; deductible waived
(pre-authorization required)
$10 co-pay per day, then 100% ofallowed amount; deductible waived
(pre-authorization required)
90% of allowed amount; deductible applies (limited to 6 visits per PY for all networks combined; additional visits
must be pre-authorized)
Designated PCP; $10 co-pay; then100% of allowed amount; deductible
waived Non-Designated Medical PCP:$20 co-pay; then 100% of allowed
amount; deductible waived
Designated Medical PCP; $10 co-pay;then 100% of allowed amount; deductible
waived Non-Designated Medical PCP:$20 co-pay; then 100% of allowed
amount; deductible waived
GYN PCP’s: $10 co-pay; then 100% ofallowed amount; deductible waived
90% of allowed amount; deductible applies
8 2018 Guide to Benefits
EHP Network Provider Out of Network ProviderHopkins Preferred NetworkProvider
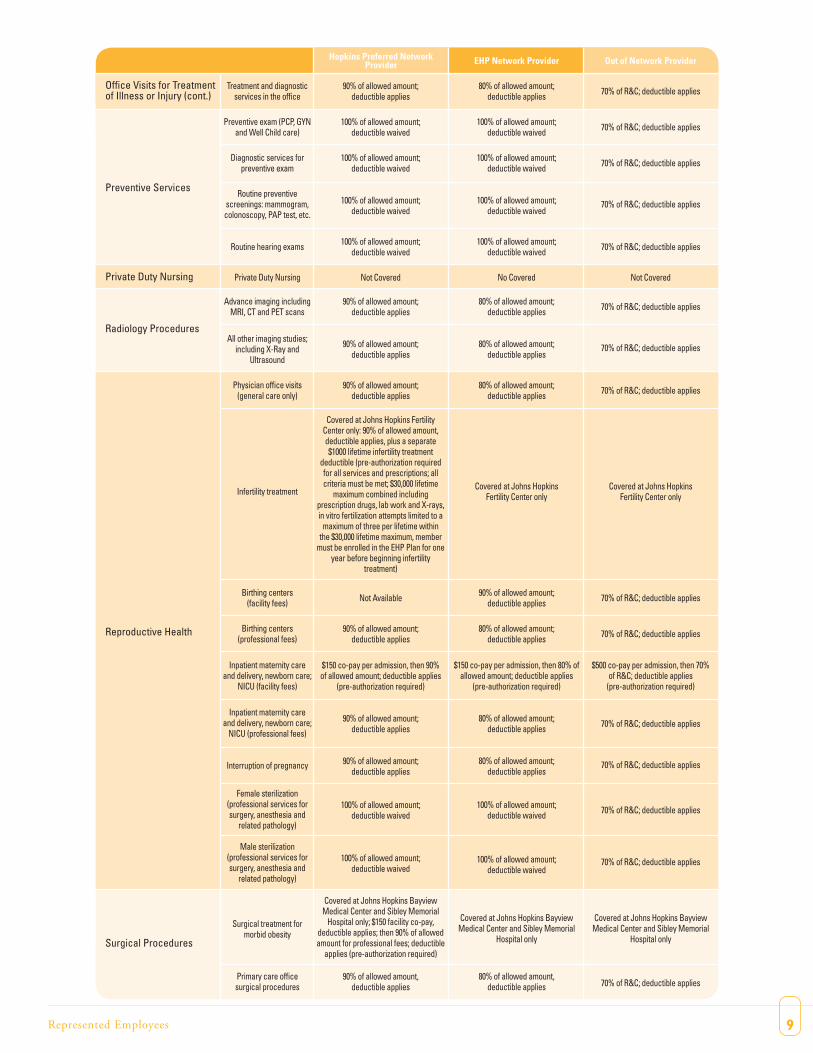
Office Visits for Treatmentof Illness or Injury (cont.)
Preventive Services
Private Duty Nursing
Radiology Procedures
Reproductive Health
Surgical Procedures
Treatment and diagnosticservices in the office
Preventive exam (PCP, GYNand Well Child care)
Diagnostic services forpreventive exam
Routine preventivescreenings: mammogram,colonoscopy, PAP test, etc.
Routine hearing exams
Private Duty Nursing
Advance imaging includingMRI, CT and PET scans
All other imaging studies;including X-Ray and
Ultrasound
Physician office visits(general care only)
Infertility treatment
Birthing centers(facility fees)
Birthing centers(professional fees)
Inpatient maternity careand delivery, newborn care;
NICU (facility fees)
Inpatient maternity careand delivery, newborn care;
NICU (professional fees)
Interruption of pregnancy
Female sterilization(professional services forsurgery, anesthesia and
related pathology)
Male sterilization(professional services forsurgery, anesthesia and
related pathology)
Surgical treatment formorbid obesity
Primary care officesurgical procedures
80% of allowed amount; deductible applies
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
No Covered
80% of allowed amount;deductible applies
80% of allowed amount;deductible applies
80% of allowed amount;deductible applies
Covered at Johns HopkinsFertility Center only
90% of allowed amount; deductible applies
80% of allowed amount; deductible applies
$150 co-pay per admission, then 80% ofallowed amount; deductible applies
(pre-authorization required)
80% of allowed amount;deductible applies
80% of allowed amount;deductible applies
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
Covered at Johns Hopkins BayviewMedical Center and Sibley Memorial
Hospital only
80% of allowed amount, deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
Not Covered
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
Covered at Johns HopkinsFertility Center only
70% of R&C; deductible applies
70% of R&C; deductible applies
$500 co-pay per admission, then 70%of R&C; deductible applies
(pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
Covered at Johns Hopkins BayviewMedical Center and Sibley Memorial
Hospital only
70% of R&C; deductible applies
90% of allowed amount; deductible applies
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
Not Covered
90% of allowed amount;deductible applies
90% of allowed amount;deductible applies
90% of allowed amount;deductible applies
Covered at Johns Hopkins FertilityCenter only: 90% of allowed amount,deductible applies, plus a separate$1000 lifetime infertility treatment
deductible (pre-authorization requiredfor all services and prescriptions; allcriteria must be met; $30,000 lifetime
maximum combined includingprescription drugs, lab work and X-rays,in vitro fertilization attempts limited to a
maximum of three per lifetime withinthe $30,000 lifetime maximum, member
must be enrolled in the EHP Plan for oneyear before beginning infertility
treatment)
Not Available
90% of allowed amount;deductible applies
$150 co-pay per admission, then 90%of allowed amount; deductible applies
(pre-authorization required)
90% of allowed amount;deductible applies
90% of allowed amount;deductible applies
100% of allowed amount;deductible waived
100% of allowed amount;deductible waived
Covered at Johns Hopkins BayviewMedical Center and Sibley Memorial
Hospital only; $150 facility co-pay, deductible applies; then 90% of allowedamount for professional fees; deductible
applies (pre-authorization required)
90% of allowed amount, deductible applies
9Represented Employees
EHP Network Provider Out of Network ProviderHopkins Preferred NetworkProvider
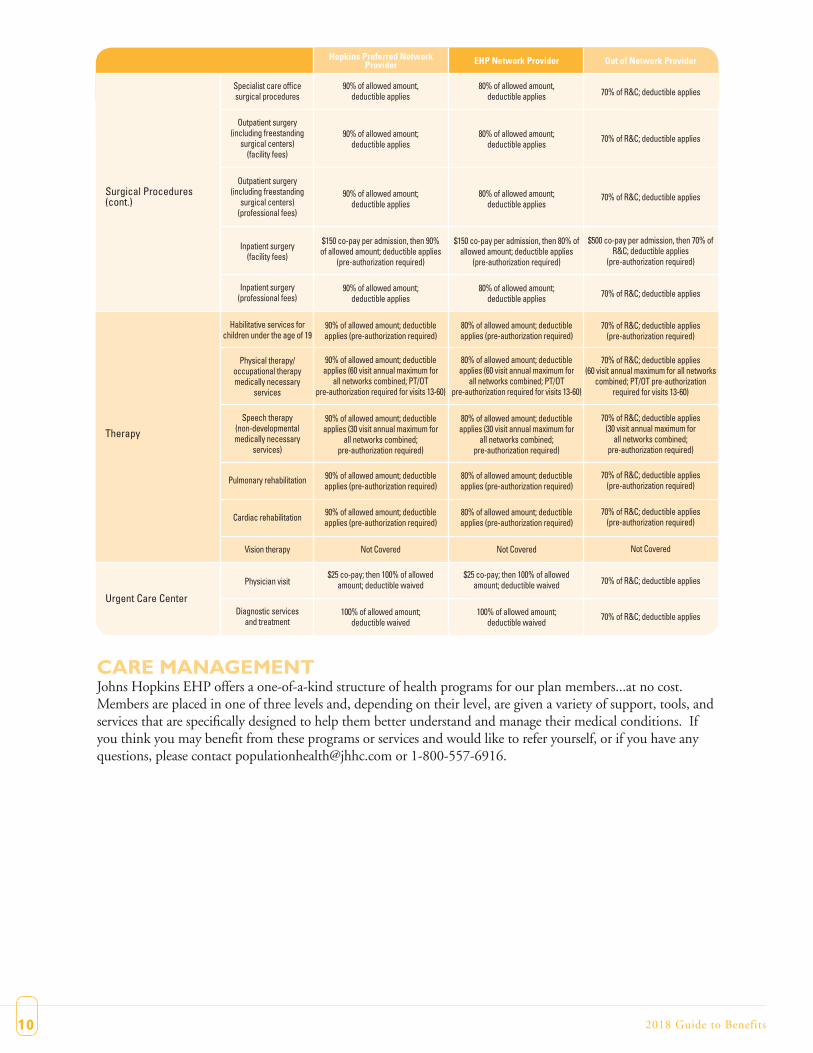
Surgical Procedures(cont.)
Therapy
Urgent Care Center
Specialist care officesurgical procedures
Outpatient surgery(including freestanding
surgical centers)(facility fees)
Outpatient surgery(including freestanding
surgical centers)(professional fees)
Inpatient surgery(facility fees)
Inpatient surgery(professional fees)
Habilitative services forchildren under the age of 19
Physical therapy/occupational therapymedically necessary
services
Speech therapy(non-developmentalmedically necessary
services)
Pulmonary rehabilitation
Cardiac rehabilitation
Vision therapy
Physician visit
Diagnostic servicesand treatment
80% of allowed amount, deductible applies
80% of allowed amount;deductible applies
80% of allowed amount;deductible applies
$150 co-pay per admission, then 80% ofallowed amount; deductible applies
(pre-authorization required)
80% of allowed amount;deductible applies
80% of allowed amount; deductible applies (pre-authorization required)
80% of allowed amount; deductibleapplies (60 visit annual maximum for
all networks combined; PT/OTpre-authorization required for visits 13-60)
80% of allowed amount; deductibleapplies (30 visit annual maximum for
all networks combined; pre-authorization required)
80% of allowed amount; deductibleapplies (pre-authorization required)
80% of allowed amount; deductibleapplies (pre-authorization required)
Not Covered
$25 co-pay; then 100% of allowedamount; deductible waived
100% of allowed amount;deductible waived
70% of R&C; deductible applies
70% of R&C; deductible applies
70% of R&C; deductible applies
$500 co-pay per admission, then 70% ofR&C; deductible applies
(pre-authorization required)
70% of R&C; deductible applies
70% of R&C; deductible applies (pre-authorization required)
70% of R&C; deductible applies(60 visit annual maximum for all networks
combined; PT/OT pre-authorization required for visits 13-60)
70% of R&C; deductible applies(30 visit annual maximum for
all networks combined; pre-authorization required)
70% of R&C; deductible applies (pre-authorization required)
70% of R&C; deductible applies (pre-authorization required)
Not Covered
70% of R&C; deductible applies
70% of R&C; deductible applies
90% of allowed amount, deductible applies
90% of allowed amount;deductible applies
90% of allowed amount;deductible applies
$150 co-pay per admission, then 90% of allowed amount; deductible applies
(pre-authorization required)
90% of allowed amount;deductible applies
90% of allowed amount; deductible applies (pre-authorization required)
90% of allowed amount; deductibleapplies (60 visit annual maximum for
all networks combined; PT/OTpre-authorization required for visits 13-60)
90% of allowed amount; deductibleapplies (30 visit annual maximum for
all networks combined; pre-authorization required)
90% of allowed amount; deductibleapplies (pre-authorization required)
90% of allowed amount; deductibleapplies (pre-authorization required)
Not Covered
$25 co-pay; then 100% of allowedamount; deductible waived
100% of allowed amount;deductible waived
10 2018 Guide to Benefits
CARE MANAGEMENTJohns Hopkins EHP offers a one-of-a-kind structure of health programs for our plan members...at no cost.Members are placed in one of three levels and, depending on their level, are given a variety of support, tools, andservices that are specifically designed to help them better understand and manage their medical conditions. Ifyou think you may benefit from these programs or services and would like to refer yourself, or if you have anyquestions, please contact [email protected] or 1-800-557-6916.

11Represented Employees
OVER-THE-COUNTER (OTC) MEDICATIONSOver the counter (OTC) drugs or medication can typically be obtained without a prescription, regardless ofwhether or not your doctor gives you a prescription for it. However, the co-pay is waived for Claritin OTC andClaritin-D OTC, but only if your doctor prescribes these drugs and you show the pharmacist your prescriptionat time of purchase. A $10 co-pay applies when you obtain a prescription for Prilosec OTC, Nexium 24H, Pre-vacid 24H and Zegerid 24H. The following chart highlights the Johns Hopkins EHP Pharmacy Plan.
COST OF MEDICAL/VISION/PHARMACY COVERAGEFor 2018, bi-weekly, pre-taxmedical contributions are as follows:
YOUR PHARMACY PLAN YEAR COSTS IN NETWORK RETAIL PHARMACY(30-DAY SUPPLY)
IN NETWORK RETAIL PHARMACY(90-DAY SUPPLY)
MAIL ORDER (90-DAY SUPPLY)
PRESCRIPTION DRUGS IN NETWORK RETAIL PHARMACY(30-DAY SUPPLY)
IN NETWORK RETAIL PHARMACY(90-DAY SUPPLY)
MAIL ORDER (90-DAY SUPPLY)
IndividualFamily
IndividualFamily
UnlimitedUnlimited
$0$0
$3600$7200
UnlimitedUnlimited
$0$0
$3600$7200
UnlimitedUnlimited
$0$0
$3600$7200
UnlimitedUnlimited
Plan Year Deductible
Out-of-Pocket Maximum
Lifetime Maximum
Oral Contraceptives
Prescription Drugs
GenericPreferred Brand
Non-Preferred BrandSpecialty Medications
GenericPreferred Brand
Non-Preferred Brand
Brand with Generic Equivalent
Specialty Medications
$0$120$195
Restricted to 30-day retail supply only$30$120$195
$195 plus the cost differential between generic and brand
Restricted to 30-day retail supply only
$0$40$65
Refer to Preferred/Non-Preferred Brand$10$40$65
$65 plus the cost differentialbetween generic and brand
Refer to Preferred/Non-Preferred Brand
$0$80$130
Restricted to 30-day retail supply only$20$80$130
$130 plus the cost differential between generic and brand
Restricted to 30-day retail supply only
Salary Tier 1: $34,999 and under Tier 2: $35,000 to $49,999 Tier 3: $50,000 and over
FULL TIME MEDICAL RATESScheduled 30 or more hours per week
or weekend option nurses
PART TIME MEDICAL RATESScheduled 20-29 hours per week
Employee
Employee & Child(ren)
Employee & Spouse
Family
Tier #1 Tier #2 Tier #3 Tier #1 Tier #2 Tier #3
$39.30
$85.25
$116.64
$125.12
$41.76
$91.70
$125.82
$135.03
$42.37
$93.31
$128.12
$137.51
$122.63
$234.23
$288.92
$311.25
$123.78
$236.57
$291.81
$314.38
$127.86
$244.70
$301.94
$325.32
Salary

12
COST OF DENTAL COVERAGEFor 2018, bi-weekly, pre-tax dental contributions are as follows:
DENTALJohns Hopkins EHP offers two dental plans (Comprehensive & High Option), whose plan administrator isDelta Dental. With each of the two plan options, you may receive care in-network or out-of-network. The fol-lowing chart provides comparison of the two Johns Hopkins Dental plans.
InsuranceSHORT TERM DISABILITYYour Short Term Disability benefits are designed to provide you with a continuing source of income during shortperiods of illness or injury. Employees who are regularly scheduled to work 20 or more hours per week, are auto-matically enrolled in this benefit. Coverage is provided by JHH at no cost to you. You are eligible for this bene-fit effective the first day of the month following date of hire and completion of any employment probationaryperiod that may apply to you. Short Term Disability benefits replace 60 percent of your bi-weekly base pay forup to 24 weeks of disability, after a 14 day elimination period. Short Term Disability benefits run concurrentlywith Family Medical Leave (FML) benefits.
Cost of STD CoverageShort Term Disability is provided by JHH at no cost to you.
2018 Guide to Benefits
COVERED SERVICES COMPREHENSIVE HIGH OPTION
In-Network Out-of-Network In-Network Out-of-Network
Calendar Year Deductible
Per individual
Per family
Combined Maximum Annual Benefit
Preventive Services
Exams Twice per year
X-rays Twice per year
Basic Service
Fillings
Oral Surgery
Major Service
Crowns, inlays and overlays
Bridges
OrthodontiaLifetime Maximum benefit of $1,500
None
None
100%
100%
80%
80%
50%
50%
Not covered
$50
$150
80% of R&C; after deductible
80% of R&C; after deductible
60% of R&C; after deductible
60% of R&C; after deductible
30% of R&C; after deductible
30% of R&C; after deductible
Not covered
None
None
100%
100%
80%
80%
60%
60%
50% up to lifetime maximum
$50
$150
80% of R&C; after deductible
80% of R&C; after deductible
60% of R&C; after deductible
60% of R&C; after deductible
40% of R&C; after deductible
40% of R&C; after deductible
Not covered
$1500 per person $3000 per person
FULL TIMEScheduled 30 or more hours
per week or weekendoption nurses
PART TIMEScheduled 20-29hours per week
Comprehensive High Option
Employee
Employee & Child(ren)
Employee & Spouse
Family
$4.72
$9.44
$12.98
$14.16
Comprehensive High Option
$6.39
$12.78
$17.57
$19.17
$7.16
$14.33
$19.70
$21.49
$9.37
$18.73
$25.76
$28.10
13Represented Employees
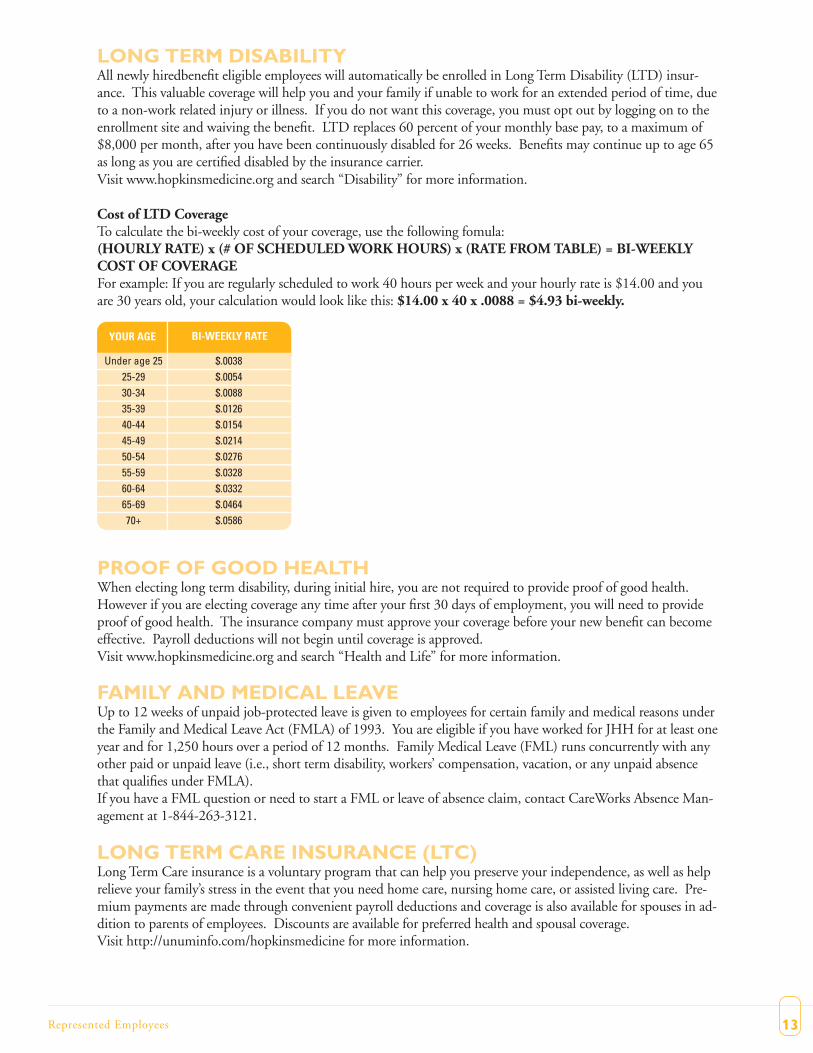
LONG TERM DISABILITYAll newly hiredbenefit eligible employees will automatically be enrolled in Long Term Disability (LTD) insur-ance. This valuable coverage will help you and your family if unable to work for an extended period of time, dueto a non-work related injury or illness. If you do not want this coverage, you must opt out by logging on to theenrollment site and waiving the benefit. LTD replaces 60 percent of your monthly base pay, to a maximum of$8,000 per month, after you have been continuously disabled for 26 weeks. Benefits may continue up to age 65as long as you are certified disabled by the insurance carrier.Visit www.hopkinsmedicine.org and search “Disability” for more information.
Cost of LTD CoverageTo calculate the bi-weekly cost of your coverage, use the following fomula:(HOURLY RATE) x (# OF SCHEDULEDWORK HOURS) x (RATE FROMTABLE) = BI-WEEKLYCOST OF COVERAGEFor example: If you are regularly scheduled to work 40 hours per week and your hourly rate is $14.00 and youare 30 years old, your calculation would look like this: $14.00 x 40 x .0088 = $4.93 bi-weekly.
PROOF OF GOOD HEALTHWhen electing long term disability, during initial hire, you are not required to provide proof of good health.However if you are electing coverage any time after your first 30 days of employment, you will need to provideproof of good health. The insurance company must approve your coverage before your new benefit can becomeeffective. Payroll deductions will not begin until coverage is approved.Visit www.hopkinsmedicine.org and search “Health and Life” for more information.
FAMILY AND MEDICAL LEAVEUp to 12 weeks of unpaid job-protected leave is given to employees for certain family and medical reasons underthe Family and Medical Leave Act (FMLA) of 1993. You are eligible if you have worked for JHH for at least oneyear and for 1,250 hours over a period of 12 months. Family Medical Leave (FML) runs concurrently with anyother paid or unpaid leave (i.e., short term disability, workers’ compensation, vacation, or any unpaid absencethat qualifies under FMLA).If you have a FML question or need to start a FML or leave of absence claim, contact CareWorks Absence Man-agement at 1-844-263-3121.
LONG TERM CARE INSURANCE (LTC)Long Term Care insurance is a voluntary program that can help you preserve your independence, as well as helprelieve your family’s stress in the event that you need home care, nursing home care, or assisted living care. Pre-mium payments are made through convenient payroll deductions and coverage is also available for spouses in ad-dition to parents of employees. Discounts are available for preferred health and spousal coverage.Visit http://unuminfo.com/hopkinsmedicine for more information.
Under age 25 $.003825-29 $.005430-34 $.008835-39 $.012640-44 $.015445-49 $.021450-54 $.027655-59 $.032860-64 $.033265-69 $.046470+ $.0586
YOUR AGE BI-WEEKLY RATE

14
LIFE INSURANCEBasic Life & Accidental Death and DismembermentAll employees regularly scheduled to work 20-29 hours per week and have completed 12 months of service areeligible for $4,000 of Basic Life Insurance in the event of their death.
All employees who are regularly scheduled to work 30-40 hours per week are eligible to receive $1,000 of BasicLife Insurance during the first 12 months of service. After 12 months, employees are eligible for one times theirannual salary, up to $50,000.
Your life insurance also includes basic accidental death & dismemberment (AD&D) insurance, which is equal tothe amount of life insurance coverage to which you are entitled. AD&Dmay pay benefits if you die or suffercertain serious injuries as a result of an accident.Visit www.hopkinsmedicine.org and search “Health and Life” for more information.
EducationTUITION ASSISTANCEAfter 60 days of employment (Courses starting 61 days after hire date and later), employees regularly scheduledto work 20 or more hours per week are eligible for tuition assistance for degree seeking studies.
Assistance is provided only if you attend an accredited college/university for studies towards an approved degree.In this educational partnership, you agree to work for JHH for a predetermined period of time as detailed withinthe JHHTuition Assistance Policy (HR332).
As an employee hired after 1/1/2007, you are eligible for assistance as follows:• $10,000 per fiscal year (July 1st to June 30th) for degree seeking studies (AA/AS, BA/BS, Masters, PhD, JD,etc.) with satisfactory completion of approved courses as detailed further within Policy (HR332).• $15,000 per fiscal year (July 1st to June 30th) for degree seeking studies (AA/AS, BA/BS, Masters, PhD, JD,etc.) at Johns Hopkins School of Nursing only with satisfactory completion of approved courses asdetailed further within Policy (HR332).• $15,000 per fiscal year (July 1st to June 30th) for approved Accelerated MBA/MHS programs only withsatisfactory completion of approved courses as detailed further within Policy (HR332).
View the full Tuition Assistance Policy online at www.hopkinsmedicine.org/jhhr (Policy HR332).Please direct tuition related inquiries to [email protected].
DEPENDENT CHILD TUITIONDependent children of regular, full-time employees* (see eligibility below) are eligible to receive tuition assistanceif the dependent is: age 26 or younger, enrolled full-time (12 credits or more) in an undergraduate program at anaccredited college or university, and in good academic standing. Assistance is available for mini-sessions and sum-mer courses only if the courses will count towards a degree and the dependent child is a full-time student alreadyparticipating in the Dependent Tuition Assistance Program for a previous fall or spring semester, and the studenthas not received the maximum benefit allowance for the fiscal year. Accredited institutions that do not offer de-grees, but instead issue diplomas or certificates, are not eligible.
Payment is for 50 percent of the tuition and eligible mandatory academic fees and when combined with grants,scholarships, awards, employers benefits, etc. (excluding loans) may not exceed 100 percent of the tuition and eli-gible mandatory fees. The benefit is available up to a maximum of 50 percent of the Johns Hopkins University’sfreshman undergraduate tuition. Payment is limited to four years of full-time, undergraduate study per depend-ent child at any accredited, degree-granting institution. Room and board, books, part-time and graduate studyare not eligible. Please note this benefit is taxable.
2018 Guide to Benefits
15Represented Employees
*Eligibility:Employees hired prior to 12/31/2017 must be in a regular, full-time position with two years of continuous full-time service to be eligible for this benefit. Employees hired after 1/1/2018 must be in a regular, full-time positionwith four years of continuous full-time service to be eligible for this benefit.
View the fullDependentChildTuitionAssistancePolicy online atwww.hopkinsmedicine.org/jhhr (PolicyHR335).
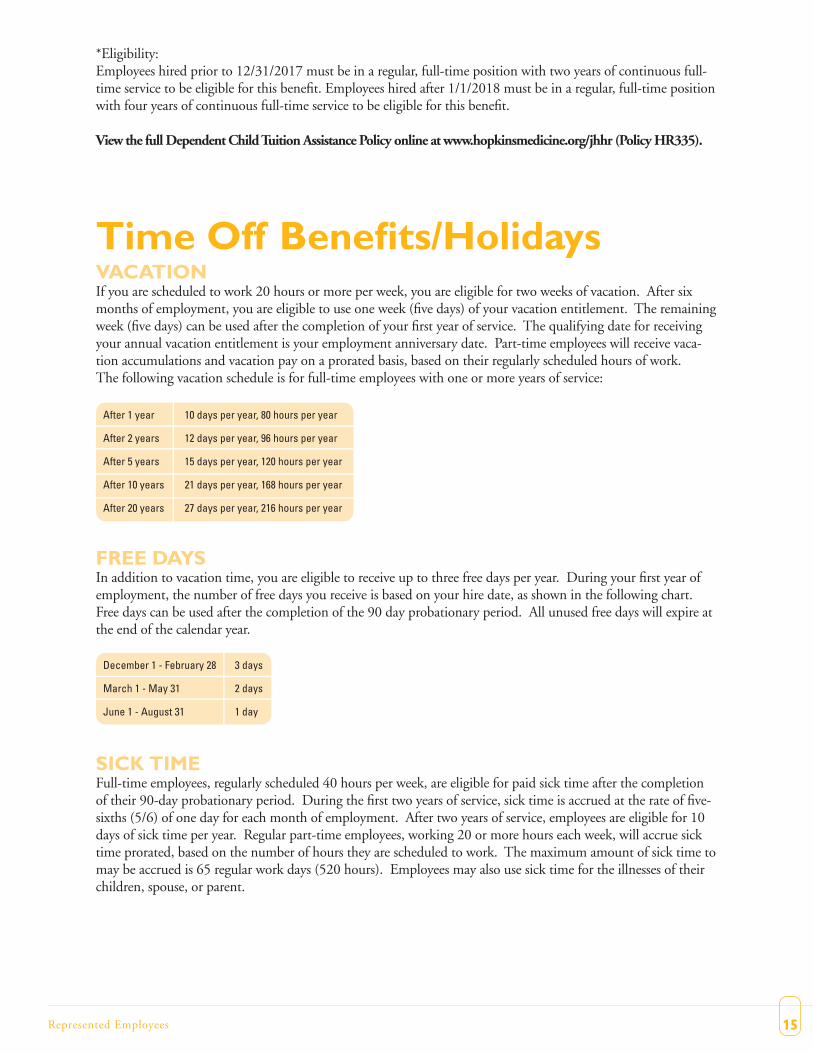
Time Off Benefits/HolidaysVACATIONIf you are scheduled to work 20 hours or more per week, you are eligible for two weeks of vacation. After sixmonths of employment, you are eligible to use one week (five days) of your vacation entitlement. The remainingweek (five days) can be used after the completion of your first year of service. The qualifying date for receivingyour annual vacation entitlement is your employment anniversary date. Part-time employees will receive vaca-tion accumulations and vacation pay on a prorated basis, based on their regularly scheduled hours of work.The following vacation schedule is for full-time employees with one or more years of service:
FREE DAYSIn addition to vacation time, you are eligible to receive up to three free days per year. During your first year ofemployment, the number of free days you receive is based on your hire date, as shown in the following chart.Free days can be used after the completion of the 90 day probationary period. All unused free days will expire atthe end of the calendar year.
SICK TIMEFull-time employees, regularly scheduled 40 hours per week, are eligible for paid sick time after the completionof their 90-day probationary period. During the first two years of service, sick time is accrued at the rate of five-sixths (5/6) of one day for each month of employment. After two years of service, employees are eligible for 10days of sick time per year. Regular part-time employees, working 20 or more hours each week, will accrue sicktime prorated, based on the number of hours they are scheduled to work. The maximum amount of sick time tomay be accrued is 65 regular work days (520 hours). Employees may also use sick time for the illnesses of theirchildren, spouse, or parent.
After 1 year 10 days per year, 80 hours per year
After 2 years 12 days per year, 96 hours per year
After 5 years 15 days per year, 120 hours per year
After 10 years 21 days per year, 168 hours per year
After 20 years 27 days per year, 216 hours per year
December 1 - February 28 3 days
March 1 - May 31 2 days
June 1 - August 31 1 day

16 2018 Guide to Benefits
REASON FOR LEAVE BENEFIT
Death of immediate family member
Jury duty
Annual military leave
Up to three days off withinone week of death(prorated for part-time employees)
Employee receives regular payup to 10 business days
The difference betweenregular pay and military payup to 10 days per year
HOLIDAYSJHH provides you with seven paid holidays each year. You are eligible for the holidays after completing the 90-day probationary period. Part-time employees are paid for holidays on a pro-rated basis according to the numberof hours they are scheduled to work. The seven observed holidays are:
• New Year’s Day• Martin Luther King, Jr. Day• Memorial Day• Independence Day• Labor Day• Thanksgiving Day• Christmas Day
OTHER PAID LEAVEJHH grants other paid leave to employees once they have completed the 90-day probationary period, as shownon the chart below:
Retirement BenefitsPENSION PLANJHH pays the full cost of this retirement benefit. You become eligible to participate in the pension plan after oneyear of employment during which you have worked 1,000 hours or more. You become eligible for a pension ben-efit once you meet the 5-year vesting requirement. The amount of your pension benefit is calculated using a for-mula based on your JHH years of service and your final average earnings.
RETIREMENT SAVINGS PLAN [403(b)]In addition to your Pension Plan benefit, you may participate in the 403(b) program. New employees will beautomatically enrolled in the 403(b) program with an initial 2% pre-tax contribution level unless you elect not toparticipate. You may also elect to have a different percentage of your salary deposited into an account each payperiod on a pre-tax or after-tax (“Roth”) basis.
RETIREE MEDICAL/DENTALRetiring employees who are at least age 62 with 15 years of service may elect to continue their EHP medical planunder COBRA until they become eligible for Medicare. This coverage can help bridge the gap in medical insur-ance for employees and their eligible dependents prior to Medicare eligibility. Retiree Dental is offered byMetLife who has two dental plans for retirees and dependents. Both plans include access to a comprehensive net-work of dentists across the country.
You may receive additional information by contacting the Retirement Office at 443-997-3789 or by [email protected]. You may also visit www.hopkinsmedicine.org and search “Pension” for more information.
17Represented Employees
Voluntary BenefitsJOHNS HOPKINS FEDERAL CREDIT UNIONAs an employee of Johns Hopkins, you are eligible to join the Johns Hopkins Federal Credit Union (JHFCU)and take advantage of their competitive, high-quality financial services. JHFCU members can use their ATM orVisa Check cards for withdrawals at over 50,000 CU24 & CO-OP Network ATMs nationwide, without sur-charges from the ATM owner! With a full range of savings and loan products and branches conveniently locatedat various locations, JHFCU is a smart and trusted banking option. To learn more about the benefits ofJHFCU, please call 410-534-4500 or visit www.jhfcu.org.
UNUM -WHOLE LIFE INSURANCEUnum’s Whole Life Insurance is designed to pay a death benefit to your beneficiaries, but it can also build cashvalue you can use while you are living. The policy accumulates cash value at a guaranteed rate of 4.5%.* Onceyour cash value builds to a certain level, you can borrow from the cash value or use it to buy a smaller “paid-up”policy with no more premiums due. If you are diagnosed with a medical condition that limits life expectancy to12 months or less, you can request up to 100% of the benefit amount, to a maximum of $150,000. Your spouseand dependents have this option as well. *The policy accumulates cash value based on a non-forfeiture interestrate of 4.5% and the 2001 CSO mortality table. The cash value will be reduced by any outstanding loans againstthe policy. For complete details of coverage and availability, please refer to policy form GA-1 or contact yourUnum representative.
UNUM - GROUP ACCIDENT INSURANCEUnum’s Accident Insurance can pay benefits based on the injury you receive and the treatment you need, includ-ing emergency-room care and related surgery. The benefit can help offset the out-of-pocket expenses that medicalinsurance does not pay, including deductibles and co-pays. Family coverage is available. Employees must belegally authorized to work in the U.S. and actively working at a U.S. location. Spouses and dependents must livein the U.S. to receive coverage. For complete details of coverage and availability, please refer to policy form GA-1or contact your Unum respresentative.
AFLAC - GROUP HOSPITAL INDEMNITY INSURANCEThe Aflac Group Hospital Indemnity plan provides cash benefits directly to you that help pay for some of thecosts–medical and non-medical–associated with a covered hospital stay due to a sickness or accidental injury. Forcomplete details of coverage and availability, please contact Aflac directly at Aflac 1-800-99-AFLAC (23422).
AFLAC - GROUP CRITICAL ILLNESS INSURANCEThe Group Critical Illness product provides a lump-sum benefit upon the diagnosis of not only one covered ill-ness, but for each covered illness. For complete details of coverage and availability, please contact Aflac directly atAflac 1-800-99-AFLAC (23522).
ADOPTION ASSISTANCEA lump sum payment of up to $5,000 to help with adoption expenses is available for eligible employees whoadopt a child. This lump sum payment can be used to assist with agency adoption fees, court costs, attorney fees,and round-trip transportation to bring the child home. Visit the web address below for more details:http://www.hopkinsmedicine.org/human_resources/benefits/health_life/voluntary.html#AdoptionCont
EMPLOYEE ASSISTANCEThe Johns Hopkins Faculty and Staff Assistance Program (FASAP) is a resource for all current Hopkins employ-ees. FASAP is a professional counseling service offered at no cost to assist employees in managing the challengesof daily living. FASAP can help identify stresses and problems and support an employee in handling those issues.The program offers short-term counseling and provides suitable resources to assist employees. Visit the websiteat www.fasap.org or call 443-997-7000.
LIVE NEAR YOURWORKThe Johns Hopkins Health System, in partnership with the City of Baltimore and the State of Maryland provides finan-cial assistance for eligible employees to purchase homes in designated areas near their place of employment via the “LiveNear Your Work Program”. Visit www.hopkinsworklife.org or call 443-997-7000.
BACK-UP CHILD AND ADULT CARECare.com/BackupCare provides emergency child or elder care services on a seven day-a-week availability. Back-up childcare providers have been screened, bonded and trained and will come to the employee’s home in those circumstanceswhere this service will enable the employee to go to work. JHH shares in the cost of this service. Pre-registration is re-quired. Visit www.hopkinsworklife.org or call 443-997-7000.
AUTO/HOMEOWNERS DISCOUNT PROGRAMMetLife offers special group rates and the opportunity to pay by payroll deduction. MetLife offers discounts from 10% to20%. Additionally, MetLife, through Veterinary Pet Insurance, provides a 5% discount for your pet, including dogs, cats,birds, etc. For more information call 1-800-GET-MET-8 or visit www.metlife.com/mybenefits. Identify yourself as aJHH employee and provide your employee badge I.D. number, as verification.
PRE-PAID LEGALHyatt Legal Plans offers a special group rate to employees who participate in their pre-paid legal plan. For a deduction ofjust $15 per month you can receive legal advice for a wide range of legal matters, including: Identity theft, defense of civillawsuits, will preparation, pre-marital agreements, real estate matters and more.Call 1-800-821-6400 or visit info.legalplans.com and enter access code “1380010” for more information.
Employee DiscountsPRESCRIPTION DRUGSHopkins employees receive a $5 co-pay discount at the Monument St. Outpatient Pharmacy, Bayview Outpatient Phar-macy, and Zayed Arcade Pharmacy when you present your badge at time of purchase.
JOHNS HOPKINS MEDICINE PERKS ATWORKYou can save on hotels, airline tickets, brand name products, and more, by registering online.Visit https://www.perksatwork.com/login and enter the company code “hopkins.” For more informationcontact the HR Solution Center at 443-997-5400.
18 2018 Guide to Benefits
19Represented Employees
NewHire Enrollment InstructionsAfter attending benefits orientation, you’ll be able to log into the enrollment system to take the required wellnesscourses, make your benefit elections and complete your wellness profile.
If you are unable to access any part of the site immediately after orientation, please wait untilWednesday and try again.
Follow the steps outlined below to gain access to the enrollment site and to enroll in benefits.
� Visit theMy Johns Hopkins Web site (https://my.jh.edu) to obtain your JHED IDand password. Instructions on obtaining your JHED ID and password are attached.
� Log into theMy Johns Hopkins Web site with your JHED ID and password. Instructions onhow to log in are attached.
� Once you’ve logged in, click the Staff tab button near the of the screen, scroll downthe JHMI Staff page until you see the JHHS Resources box on the left.
� On the Resources tab, click the “Enrollment” button and follow the instructions on each screen tomake your elections. Be sure to print a confirmation statement for your records.
Once you’ve completed the on-line enrollment portion, be sure to visit the HRWeb site to access andprint all other forms, as applicable.
http://www.hopkinsmedicine.org/human_resources/benefits/index.htmlHAVE QUESTIONS ABOUT ENROLLING? Contact the Human Resources Department at 443-997-5400.

How Do I Find My JHED ID?The first step in initiating your JHED account is to determine your JHED Login ID. You can find your LoginID by performing a lookup on yourself from any campus computer. This can be achieved by going tohttp://my.johnshopkins.edu, entering your name in the Search box at the top-right of the screen, and clickingGo.
If you find your name in the JHED Search Results screen, you may click your name to view detailed informationabout yourself. If you are logging in from a campus computer, your JHED Login ID or LID will be displayednear the top of the detail screen.
If you cannot conveniently get to a campus computer or have access but cannot find yourself in the directory you mustcall the HITS Help Desk at 410-516-HELP for assistance.
If you are not able to access the site on your day of hire, wait a day or two and try again.
20 2018 Guide to Benefits

21Represented Employees
The following chart highlights the benefits you are eligible to receive depending on the number of hoursyou are regularly scheduled to work.
Eligibility Chart
EMPLOYEES EMPLOYEESSCHEDULED TO SCHEDULED TO EMPLOYEE
BENEFIT PLAN WORK 30 OR WORK 20-29 CONTRIBUTIONMORE HOURS HOURS PER REQUIREDPER WEEK WEEK
AFLAC Yes Yes Yes
Auto/Homeowner Insurance Yes Yes Yes
Back-Up Child and Adult Care Yes Yes Yes
Child Day Care Yes Yes Yes
Credit Union Yes Yes Yes
Dependent TuitionEmployees working Yes No N/A40 hours only
Direct Deposit Yes Yes N/A
Life InsuranceBasic w/AD&D Yes Yes No
Long Term Care Yes Yes Yes
Medical-Dental-Vision- Yes Yes YesPrescription Drugs
Vacation/Sick Time Yes Yes N/A
Pension Yes Yes No
Pet Insurance Yes Yes Yes
Prepaid Legal Yes Yes Yes
Retiree Dental Yes Yes Yes
Retiree Medical Yes Yes Yes
Salary Protection
Short Term Disability Yes Yes No
Long Term Disability Yes Yes Yes
Tax-Deferred Annuity (403(b)) Yes Yes Yes
Tuition Assistance Yes Yes N/A
Wellness Rewards Yes Yes N/A
The benefits described in this booklet are for represented employees only. You may work for The Johns Hopkins Health System Corporation or for The Johns Hopkins Hospital. The Johns Hopkins Health System Corporation and The Johns Hopkins Hospital expect to continue these plans indefinitely but reserve the right to modify, amend, suspend or terminate any plan at any time and for any reason without prior notification. You will be notified of any changes to these plans and how they affect your benefits, if at all. The plans described in this booklet are governed by insurance contracts and self-insured plan documents, which are available for examination in the HR Service Center. We have attempted to make the explanation of the plans in this booklet as accurate as possible. However, should there be a discrepancy between this booklet and the provisions of the insurance contracts or plan documents, the provisions of the insurance contracts or plan documents will govern. In addition, you should not rely on any oral descriptions of the plans, since the written descriptions in the insurance contracts or plan documents will always govern.
Fall 2017 for 2018 Plan Year
The Johns Hopkins Hospital





























