Embed Size (px)
DESCRIPTION
The Economics of Public Healthcare Reform in Advanced and Emerging Economies
Citation preview

1
The Economics of Public Health Care Reform in Advanced and
Emerging Economies
Benedict ClementsFiscal Affairs Department, IMF
March 2013
This presentation represents the views of the author and should not be attributed to the IMF, its Executive Board, or its management.

2
This presentation is based on the book, The Economics of Public Health Care Reform in Advanced and Emerging Economies, which
draws on contributions from leading scholars in health economics from both advanced and
emerging economies

3
I. Fiscal context of health care reform
II. Trends and outlook for public health spending
III. Health care reform in advanced economies
IV. Health care reform in emerging economies
V. Summary
Outline

4
I. The fiscal context of health
care reform

5
18
80
18
83
18
86
18
89
18
92
18
95
18
98
19
01
19
04
19
07
19
10
19
13
19
16
19
19
19
22
19
25
19
28
19
31
19
34
19
37
19
40
19
43
19
46
19
49
19
52
19
55
19
58
19
61
19
64
19
67
19
70
19
73
19
76
19
79
19
82
19
85
19
88
19
91
19
94
19
97
20
00
20
03
20
06
20
090
20
40
60
80
100
120
140
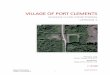
I. Debt ratios remain at historic levels in advanced economies---providing little room to accommodate higher spending on health
Public Debt, percent of GDP
World War II
Great Recession
Advanced
Emerging

6
II. Trends and outlook of public health spending

7
0
2
4
6
8
10
12
14
Private
Public
II. Led by public sector, large spending increases in advanced economies over past 40 years
Periods of Acceleration
Health spending in 27 advanced economies (percent of GDP)

8
0
1
2
3
4
5
6
Private
Public
II. Increases in public health spending were much smaller in emerging economies
Health spending in 23 emerging economies (percent of GDP)

9
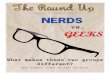
II. Higher health expenditure, however, does not necessarily lead to better health outcomes
Australia
Belgium
Canada
Czech Republic
DenmarkFinland
France
Germany
Iceland
Ireland
Italy
Japan
Korea
LuxembourgNetherlandsNorway
Portugal
Slovakia
Slovenia
SpainSweden
Switzerland
United Kingdom United States
74
76
78
80
82
84
7 8 9 10 11 12 13 14 15 16 17 18
Lif
e e
xpe
cta
ncy
at b
irth
Total health expenditure as a percent of GDP (2010)
Advanced Economies

10
Population aging—explains about one fourth of the increase in spending-to-GDP ratios
Excess Cost Growth (ECG) —the difference between real health expenditure growth and real GDP growth—explains the rest
Technology Health policies and institutions Other factors
II. Main drivers of public health spending

11
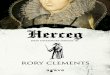
II. Public spending pressures in advanced countries are substantial
USALUX
CHEPRT
GBRAUT
KORGRC IS
LNZL
NEDFIN
AUSBEL
CANNOR
ESPFRA
SLKJP
NDEU
DENSLV
IRL
ITA
CZESW
E0
1
2
3
4
5
6Aging
Excess cost growth
Weighted average=3.0
Unweighted average=2.2
Projected increases in public health spending (percent of GDP), 2011-2030

12
II. Excess cost growth accounts for most of the increases in public health spending in advanced Europe and the US
19
80
19
82
19
84
19
86
19
88
19
90
19
92
19
94
19
96
19
98
20
00
20
02
20
04
20
06
20
08
20
10
20
12
20
14
20
16
20
18
20
20
20
22
20
24
20
26
20
28
20
30
0
1
2
3
4
5
6
7
8
9United States
IMF advanced EU estimate
European Commission advanced EU estimate 2012

13
POLHUN
BRACHL
ARG LITBGR
TURROM
UKRTHA
RUSZAF
ESTMEX
SAULVA
CHNMYS
IDN
PHLIN
DPAK
0.0
0.5
1.0
1.5
2.0
2.5
Aging
Excess cost growth
Weighted average=1.0
Unweighted average=1.1
II. Projected increases lower for emerging economies
Projected increases in public health spending (percent of GDP), 2011-2030

14
III. Health care reform in advanced economies

15
Case studies
Event analysis
Econometric analysis linking indicators of health care systems and excess cost growth (ECG)
III. Three Methodologies

16
Budget caps (Italy, Sweden)
Greater sub-national government involvement (Canada and Sweden), gate-keeping and case-based payment (Germany and Italy) – grouped under public management and coordination
III. Our results suggest five viable options to contain public health spending growth

17
Competition and choice (Germany)
Greater reliance on private financing, especially of complementary health care outside public package (Australia, Canada, and France)
Restricting the supply of health inputs and outputs (Canada)
III. Our results suggest five viable options to contain public health spending growth …

18
III. …which have the potential to contain projected increases in public spending …
Compe
tition
and
choi
ce
Contra
cting
and
pub
lic m
anag
emen
t
Budge
t cap
s
Deman
d sid
e
Suppl
y con
strai
nts
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.49
0.37
0.26
0.080.05
Average Reform Impacts on Public Health Spending (percent of GDP), 2030(Decrease Relative to Benchmark Projections)

19
Simulated reform impacts need to be interpreted with caution
Savings may not be large enough to avoid sizeable increases in spending some countries
Therefore, deeper health reforms or cuts in other spending may be required to support required fiscal adjustment
Reforms should ensure that health outcomes and access to care by the poor are not adversely affected
III. … but subject to some caveats

20
Price controls
Deregulation of insurers
Greater availability of information on the quality and price of health services to patients
III. Some reforms don’t work in containing spending growth

21
For countries that rely more heavily on competition and choice:
III. Reform options depend on country characteristics and projected growth
Low Excess Cost Growth (0-0.6): Canada, Czech Republic, France, Germany, Japan, and Slovakia
Staying the course with marginal reforms
Moderate Excess Cost Growth (0.6-1.0): Australia, Austria, Belgium, and Netherlands
Tightening budget constraintsStrengthening gate-keeping Increasing cost-sharing

22
III. Reform options depend on country characteristics and projected growth
High Excess Cost Growth (greater than 1.0): Greece, Korea, Luxembourg, Switzerland, and United States
Tightening budget constraintsIncreasing central oversightStrengthening regulations of the
workforce and equipment Strengthening gate-keeping

23
For countries that rely more heavily on public insurance and provision:
III. Reform options depend on country characteristics and projected growth
Low Excess Cost Growth (0-0.6): Denmark, Ireland, Italy, and Sweden
Enhancing efficiencyTightening budget capsImproving priority setting
Moderate Excess Cost Growth (0.6-1.0): Norway and Spain
Tightening macro-controls (including increasing central oversight)
Broadening insurance for over-the-basic health care (increasing the share of health expenditures financed out of private insurance)
Improving priority setting

24
III. Reform options depend on country characteristics and projected growth
High Excess Cost Growth (Greater than 1.0): Iceland, Finland, Portugal, New Zealand, and the United Kingdom
Strengthening supply constraints on workforce and equipment
Extending the role of private health insurance for over-the-basic health care
Increasing choice among providers

25
Improved health information technology (HIT) could help improve efficiency
Greater emphasis on primary and preventive care could also contribute to expenditure containment
III. Potential reforms not included in the analysis

26
IV. Health care reform in emerging
economies

27
IV. Emerging economies lag behind in health outcomes and coverage
0
1
2
3
4
5
6
7
8
9
10
(% of GDP)Out-Of-Pocket
Private Insurance
Public Insurance
60
65
70
75
80
85
0
5
10
15
20
25
30
35 Life Expectancy
Infant Mortality

28
In emerging Europe, coverage is almost complete; disease patterns mirror those in advanced economies; fiscal space is limited; must focus on efficiency-enhancing reforms
In emerging Latin America and emerging Asia, disease patterns are transitioning from CDs to NCDs; these countries have greater fiscal space and need to expand coverage in a fiscally sustainable manner
IV. Reform challenges differ between emerging Europe and emerging Latin America and Asia

29
Cost containment is one of the biggest challenges following a successful coverage expansion (Korea, Taiwan Province of China)
The private sector can play an important role
Improving efficiency is the key to long-term system performance
IV. Emerging economies should learn from the experiences of advanced economies

30
This is suggested by reform experiences in both advanced and emerging economies (Estonia, Korea, Taiwan Province of China)
It allows for more extensive risk pooling, and can help improve efficiency and control cost
It provides a better platform to achieve equity
It can also perform well in terms of promoting choice when combined with private provision
IV. A single payer system has several advantages

31
Many countries have successfully contained spending through reforms (Estonia, Hungary, Latvia, Russia and Ukraine)
There is scope for additional micro-level reforms to improve efficiency
Promoting healthy behaviors is also important
IV. Health reform in emerging Europe

32
Benefit packages should be restricted to most essential services as coverage expands (China, India and Mexico)
Expansion should be tax-financed if labor market informality is high
Improvements in the composition of spending can lead to better health outcomes without incurring additional costs
IV. Health reform in emerging Latin America and Asia

33
V. Summary

34
For advanced economies:
Fiscal adjustment needs are large and the projected increases in health spending account for a large share
Health reforms can help contain projected spending increases
The most effective strategy involves a mix of macro-level controls and micro-level reforms to improve spending efficiency
V. Summary

35
For emerging economies:
Fiscal adjustments needs are less pressing, but some economies are vulnerable
Efficiency-enhancing reforms should be a priority, especially for emerging Europe
Coverage expansion in emerging Latin America and Asia should not jeopardize fiscal sustainability
V. Summary

36
Thank you!
Available at IMF Bookstore and Amazon.com
There is also an accompanying video