Embed Size (px)
Citation preview

E L S E V I E R
Journal i~fPsvcho.somatic Research, Vol. 4I , No. 2, pp. 115 128, 1996 Copyright Lc 1996 Elsevier Science lnc,
All rights reserved. 0022-3999/96 $15.00 . .(h9
S0022-3999(96)00119-5
BELIEFS ABOUT MOOD MODERATE THE RELATIONSHIP OF STRESS TO ILLNESS AND
SYMPTOM REPORTING
S U S A N LEE G O L D M A N , D E B O R A H T. K R A E M E R and P E T E R S A L O V E Y
(Received 4 April 1995; accepted 19 February 1996)
Abstract-The current prospective study examined how characteristic beliefs about mood affect illness and symptom reporting. Using the Trait Meta-Mood Scale, 134 undergraduates (76 females and 58 males) reported their beliefs about attention to, clarity, and reparability of mood. Self-reported stress, illness, and symptoms were collected at three times following assessment of trait meta-mood, during times of general stress, and immediately prior to a class examination. Results indicate that, at increasing levels of distress, those who believe in greater attention to mood were more likely to report physical symptoms. In addition, those individuals who said that they generally make efforts to maintain positive mood were less likely to report illness than those less likely to engage in mood repair. The findings suggest that a person's general manner of evaluating or appraising mood is an important moderator of the relation between distress and symptom and illness reporting.
Kevwords: Illness; Mood; Stress; Symptoms.
INTRODUCTION
M a n y theor ies abou t the re la t ion be tween stress and illness have focused on expl icat ing the m o d e r a t i n g role o f people ' s appra i sa l s and eva lua t ions . F o r example , Lazarus [1] has asser ted tha t negat ive appra i sa l and eva lua t ion o f events, s i tuat ions , and avai lable resources resul t in "stress" and its concomi t an t phys io logica l a rousa l . Sufficiently high or chronic a rousa l , in turn , has consequences for illness behav io r and ac tua l physical
heal th [2]. S imi lar ly , Carver and Scheier [3] have p r o p o s e d a model o f behaviora l se l f - regula t ion in which se l f - focused a t ten t ion , s i tua t ion appra i sa l , and ou tcome ex- pectancies p l ay a p r o m i n e n t role in whether and how a person chooses to respond to a pa r t i cu l a r encounter . Med ia t ed by the behav io ra l or coping response, this model suggests tha t negat ive assessments o f a s i tua t ion and its ou t c ome have impl ica t ions for heal th behaviors and physical well-being. Cons is ten t with this theory , many studies have conf i rmed the mode ra t i ng role o f the eva lua t ion process in the re la t ion o f stress and different heal th ou tcomes , ranging f rom the repor t ing o f general physical symp- toms [4] to recovery f rom co rona ry bypass surgery [5].
A l though much l i t e ra ture has focused on how people cons t rue external or extra- pe r sona leven t s in re la t ion to themselves , a c o m p a r a b l e evaluat ive process also occurs
Yale University, New Haven, CT, USA. Address correspondence to: Susan L. Goldman, The Family Planning Council, 260 South Broad Street,
Suite 1000, Philadelphia, PA 19102-3865. Tel: (215)-985-6768; e-mail: [email protected]
115

116 S.L. GOLDMAN et al.
for internal or intra-personal events that could have similar implications for health and illness. Recent work has shown wide variation in individuals' beliefs and attitudes about the experience of emotions [6-8]. People clearly differ in their beliefs about whether and how much one should attend to these experiences, the clarity with which they can discriminate among the emotions they experience, and whether and how they can repair their emotional responses [8, 9]. Moreover, a person's characteristic way of evaluating emotions predicts recovery from a negative mood following an experimental stressor [10]. Those individuals who report that they experience their feelings clearly, for example, were less likely to engage in negative rumination follow- ing an anxiety-producing event [10]. Because persistent negative mood under stressful conditions is associated with chronic autonomic arousal [11], greater symptom and illness reporting [12-14], and poorer health-related outcomes [15], differences in people's beliefs about their moods and ability to manage it could play an important moderating role in the relationship between stress and health behavior. Thus, the present study examined how individual differences in beliefs about mood moderate the relationship between stress and symptom and illness reporting.
Predicting symptom reports
Self-directed attention has often been related to increased symptom reporting [16- 19]. Focusing attention on to the self is said to increase the relative salience of private internal events, including somatic or physiological information [3, 20, 21]. Extant measures of self-directed attention (or awareness) are often operationalized as a tendency to focus on both emotions and bodily sensations. However, attending to emotional rather than bodily sensations has different outcomes for continued psycho- logical distress and performance toward some goal. Field experiments that examined distress over aversive medical procedures and childbirth have shown that given infor- mation about the anticipated event, attention to bodily sensations decreases emotional distress more than focusing on the emotional experiences or distracting images [22- 25]. For example, women who monitored their labor contractions, rather than their emotional responses, were better able to push during the final stage of delivery and were less angry, frightened, and tense at that time [24].
The bulk of the literature suggests that under nonstressful conditions, people who attend to internal states report a greater number of symptoms than those who are not so internally focused [26, 27]. However, it may be that, under stressful conditions, a tendency to focus on emotional rather than bodily responses might heighten and/ or prolong negative mood states. If so, attention to mood may lessen a person's ability to reduce the distress associated with poor health outcomes and behaviors, thus making them more prone to its negative consequences. Therefore, it was hypothesized that individuals who believe it is important to attend to mood would report greater symptomatology, particularly as perceived distress increased.
Predicting illness reports
Research on illness behaviors has often examined either symptom reporting or a combined measure of illness and symptom reporting. However, illness reporting differs from symptom reporting, in that it requires an additional evaluative s t e p - that people interpret some constellation of physiological signs and sensations as illness. Symptom reporting merely requires an awareness of some change in the internal

Mood, stress and illness behavior.~ 117
physical condition; illness reporting necessitates a further interpretation as to the underlying cause of the perceived physiological signal.
Many factors affect this interpretative process. Certainly severity, duration, num- ber, and coherency of symptoms are strong determinants of an illness report. However, situational factors have also been shown to be influential. Illness reports are more likely when people feel that their interpersonal environments are stressful [28-30] and/or uncontrollable [31-34]. Additionally, in the face of stressful events, the mere belief that one is unable to repair one's emotional responses may also lead to feelings of uncontrollable distress. Thus, it was expected that under conditions of stress, people who report efforts to repair their moods to maintain a positive outlook would be less likely to report illness than those individuals who make few or no efforts to repair mood.
Finally, there is some suggestion that people who can clearly identify their moods are less likely to mistakenly interpret the physiological changes that accompany emotional arousal as an illness episode [10]. This led to the hypothesis that greater clarity in the experience of mood would be associated with fewer illness reports.
In summary, the current study examined whether individual differences in beliefs about: (a) attention to moods; (b) ability to discriminate among moods and experience them clearly; and (c) one's efforts to repair mood, differentially predict illness and symptom reporting in a stressed but healthy undergraduate sample. Consistent with prior research, attention to mood was expected to predict greater symptom reporting, particularly as perceived distress increased. The relation between emotional distress and illness reports was expected to be moderated by individual differences in clarity in discriminating among moods and beliefs about efforts to repair mood. We hypothe- sized that those people who report efforts toward the maintenance of positive moods in the face of negative events would be less likely to report an illness under situations of increasing distress. Illness reporting was also expected to be moderated by the degree to which people are clear in discriminating their mood states. People who are able to identify their moods or emotions should be less likely to label as illness the physiological sensations associated with affect.
M E T H O D
Design A prospective repeated measures design was used to examine the moderating role of beliefs about
mood on symptom and illness reporting during periods of general distress. Assessments of how one characteristically views mood were made prior to the collection of any health-relevant information. Self- reports of stress, illness, and symptoms were collected at three subsequent data collection times that occurred during periods of stress for the subject and immediately prior to a class examination. Repeated measurement allowed us to assess more accurately, not only the subjects' typical response to stress, but also their tendency to report both symptoms and illness.
SllbjccIs Subjects were recruited from 152 students enrolled in an undergraduate psychology course at a large
northeastern university. Of these students, 148 consented to participate in a four-phase prospective study of psychological stress and health/il lness behavior.~ Participation in the study was not a course requirement, no extra credit incentives were offered for experimental participation, and subjects who chose to participate
~Because information collected in this sample was designed to answer multiple research questions, only variables relevant to the present study are presented.

118 S . L . GOL DM AN et al.
did not receive financial compensat ion. Among those who consented to participate, 14 were excluded from the analyses because they reported some type of chronic health conditions (e.g., diabetes, asthma). The remaining 134 participants (76 females and 58 males) had a mean age of 20 years.
Measures
Life Events Scale (LES). The LES is a measure that tabulates the number of life change events an individual experiences over a given period of time [35]. Several studies have demonstrated a relationship between the cumulative number of life change events and physical symptoms [36-38]. Thus , the LES was included in the present study to control for any differential effects of life change experiences on the dependent variables. Subjects were asked to indicate which of 57 events listed they had experienced within the last 12 months . They were also asked to rate the impact of the event along a seven-point cont inuum from extremely negative to extremely positive ( - 3 to 3). An individual's LES score is the summed impact ratings.
Trait Meta-Mood Scale (TMMS). The TMMS is a 48-item self-report measure that was designed to assess a person's general beliefs about attention to mood, the clarity of their own experiences of mood, and their efforts to repair mood states [10]. It is comprised of three subscales (see Appendix). The first subscale, Attent ion to Mood (ATTENTION), indexes the amount of attention individuals feel they allot to experienced emotions and the importance of attending to mood. It consists of items like "1 pay a lot of attention to how 1 feel," and in the negative direction, "I don't think its worth paying attention to your emotions or moods ." Clarity in the Discrimination of Feelings (CLARITY) measures how clearly and distinctly individuals feel they experience their emotions. Items include "1 am usually very clear about my feelings," and "1 can't make sense out of my feelings." The final subscale, Mood Repair (REPM~) reflects an individual's efforts to repair negative mood in a way that maintains a generally positive outlook. This subscale is characterized by items like: "When I become upset, 1 remind myself of all the pleasures in life" and "I try to have good thoughts no matter how bad I feel."
The psychometric properties of the TMMS were evaluated in several recent studies involving three independent samples [10]. The Cronbach alphas for the ATTENTION subscale ranged from 0.78 to 0.86, the CLARITY subscale ranged f rom 0.80 to 0.87, and the REPAIR subscale ranged from 0.62 to 0.82, but was under 0.70 in only one of the samples. Thus , the internal consistency of these subscales is adequate. At the same time, the intercorrelations among the three factors were rather low, rarely exceeding 0.3 and usually in the 0.1-0.2 range.
The convergent validity of the TMMS was established by correlating it with constructs with which it should share some variance. A number of mood measures have been described in the literature and were used in assessments of convergent validity: Ambivalence over Emotional Expression Questionnaire [39], which taps dissatisfaction with one's emotional expression; expectancies for Negative Mood Regulation [40], which is concerned with beliefs about the changeability of negative moods; the Life Orientation Test [41], developed to measure opt imism or the tendency to have optimistic expectancies about future events; the Public and Private Self-Consciousness Scale [42], which measures the tendency to attend to aspects of ongoing consciousness, including mood; and the Center for Epidemiologic Studies Depression Scale [43], which measures depression.
In a sample of 86 young adults, the ATTENTION subscale was significantly associated with private and public self-consciousness (r values in the 0.4 range for both), but not with ambivalence over emotional expression, depression, opt imism, or beliefs about negative mood regulation. The CLARITY subscale corre- lated only with ambivalence ( r= -0 .25 ) and depression ( r= -0 .27) . REPAIR showed somewhat higher correlations with depression ( r= -0 .37) , opt imism (r= 0.57), and negative mood regulation ( r= 0.53). This pattern of correlations suggests that the subscales of the TMMS measure the constructs purported and, to varying degrees, capture significant variance not already accounted for by these existing measures.
Prior to the collection of any heaith-related measures, subjects were asked to complete the TMMS. Subjects were asked to read each statement and rate how well it described them using a five-point scale that ranged f rom strongly disagree (l) to strongly agree (5).
Spielberger State Anxiety Inventory (SSAI). The SSAI is a 20-item, self-report scale that measures state anxiety, a transitory negative emotional state or condition [44]. The SSAI is internally consistent and correlates highly with other measures of anxiety. The scale was administered at each of the three data collection occasions and a mean was calculated to describe an individual's characteristic reaction to stress over the course of the semester. 2
Self-reported stress (SRS). SRS is a single indicator that asks subjects to described how "stressed" they
2Preliminary analyses yielded correlation coefficients greater than 0.60 (p's<.001). This suggests the tendency for people to maintain their relative ranking across time with regard to their SSAI score. A one-way repeated measures A N O V A yielded no effect of time suggesting that scores did not show systematic increases or decreases over time. Therefore, we felt that an averaged score accurately captured the subject's tendency for anxiety in response to a personally relevant stressor, namely academic performance.

Mood, stress and illness behaviors 119
"feel today," on a five-point scale anchored at "not at all stressed" (1), to "'extremely stressed" (5). SRS was obtained at the at the beginning of each health data collection period with a mean calculated to indicate the subjects typical stress response)
Somatic awareness scale (SAS). The SAS is a 21-item, self-report scale which asks subjects to indicate the degree to which they were aware of various bodily states and somatic events [45]. Subjects used a five-point Likert scale to make responses to items such as "I am often aware of how full or empty my stomach feels," and "1 am often not aware of how my body feels after I have caffeine." The SAS has shown significant correlations with other measures of bodily focus and good internal consistency.
Symptom checklist. Our measure of symptom reporting was an abbreviated version of the Pennebaker Inventory of Limbic Languidness [17]. Subjects are presented with a list of symptoms such as "congested nose," "lump in throat," or "nausea." For each symptom, subjects reported on whether "it didn't happen at all this week," scored 0; "it happened a couple of times this week," scored 1; or "it happened a lot this week," scored 2. A summed symptom measure was calculated at each time period.
Illness report form. A self-report measure of illness was designed for use in this stud:,. Subjects listed any illness they experienced in the last week, the type of illness, the number of days they were ill, whether they went to the student health center, why they did or did not go to the health center, and the overall severity of their illness? The present study focused on the sum of reported illnesses across all three data collection periods.
Procedure
The study was conducted during the course of an academic semester (spring term) and consisted of four data collection periods. The LES and TMMS were administered at the first data collection time (Time 1), early in the semester. Each of the three health data collection phases that followed was timed to coincide with a class examination, an event that is particularly stressful for students. At those times, subjects completed the SSAI, SRS, symptom checklist, and illness report form prior to the first class exam (Time 2), the midterm (Time 3), and the final exam (Time 4). In addition, subjects were asked to complete a trait measure of bodily awareness (SAS) at Time 3.
RESULTS
Preliminary analyses
State anxiety~stress. The mean state anxiety level reported by students in this sample ( M = 45.96; SD = 11.03) was similar to the scores of this measure's standardization sample for undergraduates under similar test-taking situations (M=43.35; SD = 12.24) [44]. The means in the current sample indicated that students were some- what anxious, but, on average, their anxiety levels were subclinical.
Self-reports of stress were moderate on each of the data collection days (M = 2.94; range= 1-5; SD=0.83) . In addition, those individuals who said they were "very stressed" also reported high levels of state anxiety (r[2, 132] = 0.70, p = 0.0001). Be- cause we were interested in beliefs about mood and its moderating effect on negative emotions rather than on anxiety or stress per se, we formed the composite variable, distress, by taking the mean of standard scores for anxiety and stress. This composite
~As wit h the anxiety measures, preliminary correlational analyses showed a tendency for people to maimain their relative stress ranking across time (R's ranged from 0.45 to 0.53, p's<0.001. Furthermore, a one-way repeated measures ANOVA yielded no effect of time. Thus, an averaged score was used to represent the subject's tendency to report stress under academic pressure.
%lthough we had initially planned to use health center visits as a convergent indicator of illness episodes, the data indicated that very few of the subjects actually visited the university health center when ill I 13.5% at Time 2, 8.3°7o at Time 3, and 14.4070 at Time 4). The most widely cited reasons for not going to the health center was that the illness was not severe enough (87°7o), followed by lack of time (64%). As a result, the number of health visits could not be used to confirm illness reports. The data we describe focus only on symptom and illness reporting. Perceived severity of illness ratings and number of sick days were not included in these analyses due to incomplete data. Moreover, the responses that we were able to obtain failed to show adequate variance.

120 S .L . GOLDMAN et al.
score was used in subsequent analyses and the summary statistics for distress as well as its intercorrelations with other variables are presented in Table I.
Illness and symptom reporting. On average, subjects reported about one illness during the course of the academic semester and an average of six symptoms at each of the data collection days. There was a trend toward declining symptom reporting across time (F [2, 132] = 7.08, p<0.08; Time 2 M = 7.35, SD = 4.70; Time 3 M = 5.61, SD = 4.16; Time 4 M = 5.31, SD--4.79). 5 The average of these means was used in subsequent analyses and is meant to represent the subject's tendency to report symp- toms during the course of the semester.
Symptom and illness reporting were significantly correlated (r [2, 132]=0.42, p=0.0001) . Given that symptoms typically accompany illness, this finding is not surprising. However, the correlation is not perfect, indicating that symptom reporting is not completely redundant with illness reporting.
The Pearson product-moment correlations, means, and standard deviations for all variables are presented in Table 1.
Hypothesis Testing
Hierarchical regression analyses were used to test the central hypotheses concerning distress, beliefs about mood, illness and symptom reporting. 6 Although analyses proceeded separately for symptom and illness reporting, the regression procedures used were similar for both outcome variables. Our basic analytic strategy was a five-step, hierarchical regression. Gender was entered first to evaluate any differential or interactive effects of gender. Life events were entered next to control for any possible influence of these events on symptom and /o r illness reports. The effect of distress was entered in the third step, followed by the simultaneous inclusion of the three TMMS subscales in the fourth step. This accounted for all possible main effects. However, because we expected beliefs about mood to moderate the relation of stress to illness and symptoms reporting, it was also necessary to examine the interaction effects. Thus, three interaction terms, distress * ATTENTION, distress * CLARITY, and distress * REPAIR, were simultaneously entered in the fifth block. This main effects and first level interactions model tested the moderator hypotheses. In an effort to determine whether any of the preceding effects needed to be further qualified, higher order interactions were also tested by allowing them to enter the model at the sixth step based on the statistical criterion that p<0.15. None met criterion for either symptom or illness reporting.
Symptom reporting, distress and beliefs about mood. Because we were interested in whether attention to mood could predict symptom reporting over and above atten- tion to bodily sensations, we included scores on the SAS into the model after the distress measure and before any of the beliefs about mood subscales. The final model for symptom reporting was significant (R =- 0.42; F [10, 124] = 2.65, p<0.01) with the
5There were no significant gender differences in illness and symptom reporting. 6Prior to analyses, the dependent variables were subjected to square root transformation to stabilize the
variance of event count data. Square-root transformations are appropriate whenever the dependent variable is one that arises in conformity with a "Poisson process." Event count data, such as number of symptoms or illness, are examples of Poisson variables. The square-root transformation used was one suggested as optimal for stabilizing the variance of Poisson-distributed variables [46] and involves the square root of y + 3 / 8 .

Table 1 . - S u m m a r y statistics and inter-correlations for all predictor and criterion variables (N = 134)
Variable 1 2 3 4 5 6 7 8 9 10 M SD Range b
1. Illness a 1.00 0.75 0.94 0-4 2. Avg.
symptoms 0.42*** 1.00 5.80 4.06 0-24
3. LES - 0 . 1 3 - 0 . 1 1 1.00 0.29 9.05 - 2 7 - 3 6 4. Anxiety 0.10 0.33*** -0 .22** 1.00 45.96 11.03 21-73 5. Stress 0.06 0.22* -0 .20** 0.70*** 1.00 2.94 0.83 1-5
6. Distress 0.09 0.30*** - 0 . 2 2 * * * 0.92*** 0.90*** 1.00 1.07 0.97 - 1.20-3.72
7. SAS 0.08 0.14 - 0 . 0 5 0.19" 0.05 0.15 1.00 69.88 8.85 42-91 8. Attention 0.08 0.05 0.14 - 0 . 0 1 0.07 - 0 . 0 2 0.15 1.00 38.73 5.81 22-50 9. Clarity - 0 . 0 8 - 0 . 2 3 * * 0.17" -0 .28*** - 0 . 1 2 - 0 . 2 3 * - 0 . 1 4 0.12 1.00 34.21 6.81 17-50
10. Repair - 0 . 2 1 " - 0 . 2 3 * * 0.27** -0 .30*** -0 .11 - 0 . 2 1 " * - 0 . 0 9 0.17" 0.39*** 1.00 15.13 3.32 5-20
0 0
, . . .
_<.
a Represent the total number of illness episodes summed across time. b Actual range in the data. *p = 0.05; **p = .01; ***p = .001.

122 S.L. GOLDMAN et al.
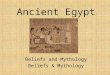
HIGH ATTENTION
AVG. ATTENTION
increasing decreasing DISTRESS LEVELS +
Fig. 1. Interaction of distress and attention to mood in predicting symptom reporting.
i n t e r a c t i o n t e r m dis t ress * ATTENTION m a k i n g the on ly s igni f icant c o n t r i b u t i o n . In
o t h e r w o r d s , the s lope desc r ib ing the r e l a t i on b e t w e e n dis t ress and s y m p t o m r e p o r t i n g
d e p e n d e d o n an i nd iv idua l ' s score o n the ATTENTION subsca le . W e had h y p o t h e s i z e d
tha t , c o m p a r e d to t h o s e w h o e n d o r s e less a t t e n t i o n to m o o d s , i nd iv idua l s wi th h ighe r
scores o n ATTENTION w o u l d r e p o r t m o r e s y m p t o m s u n d e r g rea te r levels o f dis t ress .
T o d e m o n s t r a t e t ha t t h e i n t e r a c t i o n c o n f i r m e d the h y p o t h e s i s , we c o m p u t e d and
g r a p h e d a set o f s lopes and the i r c o r r e s p o n d i n g r eg re s s ion l ines. Th i s p r o c e d u r e
a l l o w e d us to v i sua l i ze the effect o f dis t ress on s y m p t o m r e p o r t i n g at inc reas ing
ATTENTION s c o r e s / F i g u r e 1 i l lus t ra tes t ha t t he i n t e r a c t i o n was in the h y p o t h e s i z e d
7The regression equation that describes the interaction of distress (X3) and attention (X4) is given by the equation:
Y = ct + 13 IXl q- 132X2 q- 133X3 q- [~4Xd, q- [~5X5 q- 136X6 -{~ 137X7 q- 138X3X5 ~- 139X3X6 q- 1310X3X7
which can also be expressed as
Y = (135 q- ~sX3)X5 q- ([~IX1 q- g2X2 d- ~3X 3 -b ~4X 4 -~- 136X6 q- 137X7 q- ~9X3X6 a¢_ 1310X3X7 q_ (1)
to demonstrate more clearly the conditional nature of the relationship. The slope is given by the first term in the parentheses and the y-intercept is determined by the quantity in the second set of parentheses. The significant interaction indicates that each different value we assign to )(4 (attention) defines a different line. This contingency can be demonstrated by calculating the regression equation for three representative members of this family of lines. We chose to show the regression lines for low attention scores (2 SD below the mean), average attention scores (at the mean), and high attention scores (2 SD above the mean) at increasing levels of )(3 (distress). All other terms in the regression equation were held constant at their means.

Mood, stress and illness behaviors
Table 2 . - S u m m a r y o f heirarchical regress ion predict ing s y m p t o m repor t ing
123
Step Source Multi R F (eqn) df p-value [3 in Final [3
1 Gende r 0.11 1.64 1, 132 0.203 - 0 . 1 1 - 0 . 0 6 2 LES 0.15 1.48 2, 131 0.232 - 0 . 1 0 - 0 . 0 1 3 Distress 0.30 4.17 3, 130 0.007 0.26 0.12 4 SAS 0.31 3.34 4, 129 0.012 0.08 0.06 5 T M M S 0.37 2.89 7, 126 0.008
Attent ion - 0.13 0.07 Clari ty 0.09 - 0.03 Repair - 0.14 0.02
6 Distress * T M M S 0.42 2.65 10, 123 0.006 Distress * At ten t ion 1.81" 1.27" Distress * Clari ty - 0 . 7 9 - 0 . 3 9 D i s t r e s s , Repair - 1.57 0.76
p = 0.06.
direction, s Under conditions of general distress, greater ATTENTION scores were associ- ated with a greater tendency to report physical symptoms. These results support our hypothesis that attention to m o o d can moderate the relation between distress and symptoms.
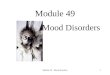
Illness reporting, distress, and beliefs about mood. The results of the final regres- sion model for illness reporting yielded a statistically significant model ( R = 0.36; F [9, 124] = 2.00, p<0.05) . Furthermore, when we considered the interaction terms individually, we found that the interaction o f distress and REPAIR predicted illness reporting. Recall our hypothesis that individuals who report greater efforts to maintain a positive out look in the face o f negative effect would be less likely to report an illness under situations o f increasing distress, when compared to those who make less of an effort to repair mood. To understand the moderating effect of REPAIR on illness reporting at increasing levels o f distress, we again computed and graphed a set o f slopes and their corresponding regression lines.9 Fig. 2 illustrates that the interaction was in the hypothesized direction. ~0 As the level o f perceived distress increased, individ- uals with low REPAIR scores reported more illness episodes than individuals with high REPAIR scores. Thus, it appears that, under conditions o f increasing distress, the number of illnesses reported depends on an individual's efforts at m o o d repair. The interaction o f distress and CLARITY was not a significant predictor of either symptom or illness reporting.
Although this graph simplifies cont inuous relationships into seemingly discontinuous high, average, and low attention slopes, the graph represents conceptually relevant instantiations from a family of regression lines that describe the changing slopes across three levels of attention. Therefore, these lines should not be interpreted as representing separate group mean differences.
9Calculations used to obtain representative regression lines were identical to those used in calculating the family of equations for attention to mood. We chose to show the regression lines for low, average, and high repair scores. All other terms in the regression equation were held constant at their means.
~Although these three lines simplify cont inuous relationships into seemingly discontinuous high, average, and low repair slopes, the graph represents conceptually relevant instantiations from a family of regression lines that describe the changing slopes across three levels of repair. Therefore, these lines should not be interpreted as representing separate group mean differences.

124 S.L. GOLDMAN et al.
LOW REPAIR
AVG. REPAIR
HIGH REPAIR
decresslng - DISTRESS L E V E L S + iacreasing
Fig. 2. Interaction of distress and mood repair in predicting illness reporting.
DISCUSSION
H o w peop le evalua te extra-personal events and s i tua t ions has been shown to influ- ence illness behav io r [47] and ac tua l heal th [48]. The cur ren t s tudy has ex tended these
f inding by d e m o n s t r a t i n g tha t the ways in which people eva lua te intra-personalevents, such as m o o d s and e m o t i o n a l s ta tes , also m o d e r a t e the effect o f stress on illness behaviors . A t increas ing levels o f dis tress , the t endency to a t t end to one 's m o o d s p red ic ted a grea te r l i ke l ihood o f r epor t ing s y m p t o m s . I l lness repor t ing , however , was no t p red ic t ed by a t t en t ion to m o o d , but by a person ' s efforts to recover posi t ive m o o d . C o m p a r e d to those who repor t no t being able to repai r negat ive m o o d , those who
m a d e efforts to move thei r affective states t o w a r d greater pos i t iv i ty r epo r t ed fewer
Table 3. - Summary of heirarchical regression predicting illness reporting
Step Source Multi R F (eqn) df p-value 13 in Final 13
1 Gender 0.06 0.54 1, 132 0.464 - 0.06 0.00 2 LES 0.15 1.48 2, 131 0.238 -0.13 0.10 3 Distress 0.16 1.09 3, 130 0.354 0.06 0.28 4 TMMS 0.25 1.37 7, 127 0.231
Attention 0.09 0.03 Clarity - 0.04 - 0.04 Repair -0 .19 0.15
5 Distress • TMMS 0.42 2.00 9, 124 0.045 Distress • Attention 0.83 0.83 Distress * Clarity 0.52 0.46 Distress * Repair - 1.15 - 1.52
p < 0.001.

Mood, stress and illness behaviors 125
illnesses in the face of increasing levels of distress. These differential effects serve to reinforce the point that symptom and illness reporting are separable, although overlapping, illness behaviors. As a result, factors that influence symptom reporting are not necessarily the same factors that influence illness reporting.
With regard to symptom reporting, the results highlight a potentially important distinction in inward focused attention. When evaluating introspective attention, it may be important to assess attention to mood separately from somatic awareness. This is because attention to bodily sensations may overlap with measurement of symptom reporting, thereby leading to spurious associations between somatic aware- ness and illness behaviors. Although an inward focus of attention has been associated with more symptom reporting [22-25], there was some question about whether atten- tion to mood, specifically, could predict symptom reporting. Our findings showed that, at progressively higher levels of distress, the number of symptoms reported rose more rapidly in people who endorsed behaviors and attitudes for attention to mood than in people who did not, even after we considered their tendency for somatic awareness.
Recall, however, that people who reported symptoms did not always report illness. This was evidenced by the imperfect correlation between these two outcome variables (r-- 0.42). Moreover, the moderators of symptom reporting were different from those of illness reporting. Under stress conditions, people who generally attend to mood reported more symptoms, but they did not necessarily report more episodes of illness. Rather, people who tended not to repair negative moods showed a greater rise in illness reports under increasing levels of distress. Thus, it appeared that, in a relatively healthy population, distressed individuals who reported greater perceived control over negative mood were less likely to report illness, despite the presence of symptoms, when compared to individuals who did not feel that they could repair their moods. It may be that relative to those who were high in perceived control over emotional responses, individuals who did not believe they could repair mood experienced more physiological arousal and compromise and therefore were more likely to be, or have been, ill. Unfortunately, the present data cannot address the processes that underlie this relationship, and it is yet unclear whether this finding is due to a general sense of loss of control or one that is specific to mood. Because the process of illness labeling has important implications for medical utilization and appropriate health care, ongo- ing research will need to clarify this question.
The predicted interactive effect of distress and mood clarity on illness reporting was not confirmed. Under increasing levels of distress, the general ability of people to label their feelings was not related to whether they reported themselves as ill. In retrospect, the arousing conditions of the examination may have made it easy for people low in clarity to label their emotions as distinct from illness, thereby preventing clarity as emerging as an effective moderator in this situation. Clarity in discriminating emotions may be a more important moderator of illness reporting under conditions of relatively mild or ambiguous states of emotional arousal. This interpretation is supported by Katkin [49], who demonstrated that people could not accurately estimate their heartbeat under conditions of low stress, but could do so under conditions of high stress.
Taken as a whole, the findings of the present study suggest that a person's general manner of evaluating or appraising mood is an important moderator of the relation

126 S.L. GOLDMAN et al.
between distress and symptom and illness reporting. Caution should be used, however, in generalizing these results beyond a population of healthy young adults. The moder- ating effects of trait recta-mood may operate differently in individuals with chronic illness or who differ significantly in demographics from the population studied. Caveats stated, it does appear that, in relatively healthy young adults, differences in self- reported attention to mood and efforts to repair mood may be useful in predicting certain illness behaviors. How these differences arise, are sustained, and might be modified are important issues for future research.
A c k n o w l e d g m e n t s - W e extend our thanks to Micheala Kiernan, Susan Ortega, and William Sieber for their help in data collection. Appreciation is also extended to John D. Mayer, David M. Bersoff, and two anonymous reviewers for their comments on earlier versions of this article. P. S. is supported by grants from the Presidential Young Investigator Program of the National Science Foundation and the American Cancer Society.
REFERENCES
1. Lazarus RS. Stress, coping, and illness. In: Friedman HS, ed. Personality and disease. New York: Wiley, 1990:97-120.
2. Kranz DS, Manuck SB. Acute psychophysiologic reactivity and risk of cardiovascular disease: A review and methodologic critique. Psychol Bull 1984;96:435-464.
3. Carver CS, Scheier MF. Control theory: A useful conceptual framework for personality-social, clinical, and health psychology. Psychol Bull 1982;92:111-135.
4. Reker GT, Wong PT. Psychological and physical well-being in the elderly: The Perceived Well-Being Scale. Can J Aging 1983;3:23-32.
5. Scheier MF, Matthews KA, Owens JF, Magovern GJ Sr, Lebfevre RC, Abbott RA, et al. Dispositional optimism and recovery from coronary artery bypass surgery: The beneficial effects on physical and psychological well-being. J Per Soc Psychol 1989;57:1024-1040.
6. Apfel R J, Sifneos PE. Alexithymia: Concept and measurement. Psychother Psychosomat 1979;32: 180-190.
7. King LA, Emmons RA. Conflict over emotional expression: Psychological and physical correlates. J Pers Soc Psychol 1990;58:864-877.
8. Salovey P, Mayer JD. Emotional intelligence. Imagin Cognit Pets 1990;9:185-211. 9. Mayer JD, Gaschke YN. The experience and recta-experience of mood. J Per Soc Psychol 1988;55:
102-111. 10. Salovey P, Mayer JD, Goldman SL, Turvey C, Palfai T. Emotional attention, clarity, and repair:
Exploring emotional intelligence using the trait meta-mood scale. In: Pennebaker JW, ed. Emotion, Disclosure and Health. Washington, DC: American Psychological Association 1995:125-154.
11. Watson D, Pennebaker J. Health complaints, stress, and distress: Exploring the centrol role of negative affectivity. Psychol Rev 1989;96:234-254.
12. Katon W. Depression: Relation to somatization and chronic medical illness. J Clin Psychiat 1984;45: 4-11.
13. Persson L, Sjoberg L. Mood and somatic symptoms. J Psychosomat Res 1987;31:499-511. 14. Tessler R, Mechanic D. Psychological distress and perceived health status. J Health Soc Behav 1978;
19:254-262. 15. Salovey P, O'Leary A, Stretton MS, Fishkin SA, Drake CA. Influence of mood on judgements about
health and illness. In: Forgas JP, ed. Emotion and social judgements. London: Pergamon 1991: 241-262.
16. Hansell S, Mechanic D. Introspectiveness and adolescent symptom reporting. J Hum Stress 1984 11: 165-176.
17. Pennebaker JW. The psychology of physical symptoms. New York: Springer-Verlag, 1982. 18. Salovey P, Birnbaum D. Influence of mood on health-relevant cognitions. J Pers Soc Psychol 1989;
57:539-551. 19. Ward SE, Leventhal H, Love R. Repression revisited: Tactics used in coping with a severe health
threat. Pets Soc Psychol Bull 1988;14:735-746. 20. Buss AH. Self-consciousness and social anxiety. San Francisco: Freeman 1980. 21. Duval S, Wickland RA. A theory of objective self-awareness. New York: Academic Press 1972.

Mood, stress and illness behaviors 127
22. Johnson J, Morrissey J, Leventhal H. Psychological preparation for an endoscopic examination. Gastrointest Endosc 1973;19:180-182.
23. Johnson J, Rice VH, Fuller SS, Endress MP. Sensory information, instruction in a coping strategy and recovery from surgery. Res Nurs Health 1978;1:4-17.
24. Leventhal E, Leventhal H, Shacham S, Easterling DV. Active coping reduces reports of pain from childbirth. J Consult Clin Psychol 1989;57:365-371.
25. Philips, H. Avoidance behavior and its rolein sustaining chronic pain. Behav Res Yher 1987;25:273-279. 26. Scheier MF, Carver CS, Gibbons FX. Self-directed attention, awareness o f bodily states and suggestibil-
ity. J Pers Soc Psychol 1979;37:1576-1588. 27. Stretton MS, Salovey P, Mayer J. Assessing health concerns. Imagin Cognit Pers 1992-1993;12:
115-137. 28. Gortmaker SL, Eckenrode J, Gore S. Stress and the utilization of health services: A time series and
cross-sectional analysis. J Health Soc Behav 1982;23:25-38. 29. Shuval JT. Social functions of medical practice. San Francisco: Jossey-Bass 1970. 30. Tessler R, Mechanic D, Diamond M. The effect of psychological distress on physician utilization: A
prospective study. J Health Soc Behav 1976;17:353-364. 3l. Luborsky L, Docherty JP, Penick S. Onset conditions for psychosomatic symptoms: A comparative
review of immediate observation with retrospective research. Psychosomat Med 1973 ;35:187-204. 32. Rodin J. Managing the stress of aging: The role of control and coping. In: Levine S, Ursin H, eds.
Coping and health. New York: Plenum 1980:171-202. 33. Wolf S. Reactions in the nasal mucosae: Relations of life stress to chronic rhinitis and "sinus" headache.
AMA Arch Otolaryngol 1954;66:297-333. 34. Wolff HG. Stress and Disease. Springfield, IL: CC Thomas 1968. 35. Sarason IG, Johnson JH, Siegel JM. Assessing the impact of life changes: Development of the Life
Experiences Survey. J Consult Clin Psychol 1978;46:932-946. 36. Dohrenwend BS, Dohrenwend BP. Stressfullife events: Their nature and effects. New Yor k: Wiley 1974. 37. Rahe RH. Life-change measurement as a predictor of illness. Proc R Soc Med 1968;61:1124-1126. 38. Rahe RH. Subjects' recent life changes and their near future illness reports. Ann Clin Res 1972;4:
250-265. 39. King LA, Emmons RA. Conflict over emotional expression: Psychological and physical correlates. J
Pets Soc Psychol 1990;58:864-877. 41). Catanzaro S J, Mearns J. Measuring generalized expectancies for negative mood regulation: Initial
scale development and implications. J Pers Soc Psychol 1990;54:546-563. 41. Scheier MF, Carver CS. Optimism, coping, and health: Assessment and implications of generalized
outcome expectancies. J Res Pers 198115:1-15. 42. Fenigstein A, Scheier MF, Buss AH. Public and private self-consciousness: Assessment and theory.
J Consult Clin Psychol 1975;43:522-527. 43. Radloff LS. The CES-D scale: A self-report depression scale for research in the general population.
Appl Psycholog Meas 1977; 1:385-401. 44. Spielberger CD, Gorsuch RL, Lushene RE. Manual for the State-Trait Anxiety Inventory. Palo Alto,
CA: Consulting Psychologist's Press 1970. 45. Stretton MS. Predicting helath concerns [dissertation]. New Haven, CT: Yale University 1990. 46. Haight F. Handbook of the Poisson distribution. New York: John Wiley & Sons 1967. 47. Leventhal H, Nerenz DR, STRAUSS A. Self-regulation and the mechanisms for symptom appraisal.
In: Mechanic D, edr. Psychosocial epidemiology. New York: Neal Watson Academic Publications 1980:55-86.
48. Lazarus RS, Folkman S. Stress, appraisal, and coping. New York: Springer 1984. 49. Kat kin ES. Blood, sweat, and tears: Individual differences in autonomic self-perception. Psychophysiol-
ogy 1984;22:125-137.

128 S . L . G O L D M A N et al.
A P P E N D I X
TRAIT META-MOOD SCALE
Please read each statement and decide whether or not you agree with it. Place a number in the blank line next to each statement using the following scale:
5 4 3 2 1 Strongly agree Somewhat agree Neither agree nor disagree Somewhat disagree Strongly disagree
1. The variety of human feelings makes life more interesting. 2. I try to think good thoughts no matter how badly 1 feel. [REPAIR] 3. 1 don't have much energy when I am happy. 4. People would be better off if they felt less and thought more. [ATTENTION (R)] 5. I usually don' t have much energy when I 'm sad. 6. When I'm angry, I usually let myself feel that way. 7. I don't thaink it's worth paying attention to your emotions or moods. [ATTENTION (R)] 8. I don't usually care much about what I 'm feeling. [ATTENTION (R)] 9. Sometimes I can't tell what my feelings are. [CLARITY (R)]
10. If I find myself getting mad, I try to calm myself down. 11. I have lots of energy when I feel sad. 12. I am rarely confused about how I feel. [CLARITY] 13. I think about my mood constantly. 14. I don't let my feelings interfere with what I am thinking. 15. Feelings give direction to life. [ATTENTION] 16. Although I am sometimes sad, I have a mostly optimistic outlook. [REPAIR] 17. When I am upset I realize that the "good things in life" are illusions. [REPAIR] 18. I believe in acting from the heart. [ATTENTION] 19. 1 can never tell how l feel. [CLARITY] 20. When I am happy I realize how foolish most of my worries are. 21. I believe it's healthy to feel whatever emotion you feel. 22. The best way for me to handle my feelings is to experience them to the fullest. [ATTENTION] 23. When I become upset I remind myself of all the pleasures in life. [REPAIR] 24. My belief and opinions always seem to change depending on how 1 feel. [CLARITY (R)] 25. I usually have lots of energy when I 'm happy. 26. I am often aware of my feelings on a matter. [CLARITY] 27. When I'm depressed, I can't help but think of bad thoughts. 28. 1 am usually confused about how I feel. [CLARXTY (R)] 29. One should never be guided by emotions. [ATTENTION (R)] 30. If I 'm in too good a mood, I remind myself of reality to bring myself down. 31. I never give in to my emotions. [ATTENTION (R)] 32. Although I am sometimes happy, I have a mostly pessimistic outlook. [REPAIR (R)] 33. I feel at ease about my emotions. [CLARITY] 34. It's important to block out some feelings in order to preserve your sanity. 35. I pay a lot of at tention to how I feel. [ATTENTION] 36. When I 'm in a good mood, I'm optimistic about the future. [ATTENTION] 37. I can't make sense out of my feelings. [CLARITY] 38. I don't pay much attention to my feelings. [ATTENTION (R)] 39. Whenever I 'm in a bad mood, I'm pessimistic about the future. 40. I never worry about being in too good a mood. 41. I often think about my feelings. [ATTENTION] 42. I am usually very clear about my feelings. [CLARITY] 43. NO matter how badly I feel, I try to think about pleasant things. [REPAIR] 44. Feelings are a weakness humans have. [ATTENTION (R)] 45. I usually know my feelings about a matter. [CLARITY] 46. It is usually a waste of t ime to think about your emotions. [ATTENTION (R)] 47. When I am happy 1 sometimes remind myself of everythink that could go wrong. 48. 1 almost always know exactly how I am feeling. [CLARITY]
Statements in boldface numbers indicate those items used to calculate subscale scores. The subscales on which these items are assigned are indicated after them. (R) indicates a reverse-scored item.