Embed Size (px)
Citation preview

American Journal of Medical Genetics 111:381–387 (2002)
Behavioral Phenotypes in Four Mental RetardationSyndromes: Fetal Alcohol Syndrome, Prader-WilliSyndrome, Fragile X Syndrome, and Tuberosis Sclerosis
Hans-Christoph Steinhausen,1* Alexander von Gontard,2 Hans-Ludwig Spohr,3 Berthold P. Hauffa,4
Urs Eiholzer,5 Margitta Backes,2 Judith Willms,3 and Zeno Malin1
1Department of Child and Adolescent Psychiatry, University of Zurich, Zurich, Switzerland2Department of Child and Adolescent Psychiatry, University of Cologne, Cologne, Germany3Children’s Hospital, German Red Cross, Berlin, Germany4Department of Pediatric Hematology, Oncology, and Endocrinology, Children’s Hospital, University of Essen,Essen, Germany5Foundation Growth Puberty Adolescence, Zurich, Switzerland
Behavioral phenotypes were studied in fourmental retardation syndromes using theDevelopmental Behavior Checklist (DBC).The four samples comprised fetal alcoholsyndrome (FAS), Prader-Willi syndrome(PWS), fragile X syndrome (FRAX), and tub-erosis sclerosis (TSC). Both on the item andthe subscale level, there were clear beha-vioral differentiations across the four syn-dromes. FAS and FRAX proved to be mostclearly differentiated from the other twosamples, with PWS and TSC showing lowerscores and less abnormal behavior profiles.Neither intelligence nor gender nor agecontributed to variations in the number ofbehavior abnormalities. It was concludedthat the DBC as a quantitative approach con-tributes significantly to the differentiationof behavioral phenotypes in various mentalretardation syndromes. � 2002 Wiley-Liss, Inc.
KEY WORDS: behavioral phenotypes; fetalalcohol syndrome; Prader-Willi syndrome; fragile X syn-drome; tuberosis sclerosis
INTRODUCTION
There is a longstanding history of psychopathologyresearch inmental retardation syndromes.Thus, various
genetic syndromes associated with mental retardationhave been studied with the aim of identifying signifi-cant relationships between genes and behavior. In therecent past, the rapid increase in knowledge gained bymolecular-biological investigations further stimulatedthis area of research. A variety of mental retardationsyndromes have been assessed in order to identifybehavioral and psychiatric phenotypes [Dykens, 2000;Dykens and Hodapp, 2001].
A behavioral phenotype has been defined as a charac-teristic pattern of motor, cognitive, linguistic, and socialabnormalities constantly associated with a biologicaldisorder [Flint and July, 1994]. There are two mainapproaches to the study of behavioral phenotypes: thegenomic and the phenomic approach.While the genomicapproach studies genetically identifiable conditions andseeks to which extent they have behavioral character-istics, the phenomic approach begins with observationsof behavior itself, with the aim of elucidating underlyinggenetic mechanisms [O’Brien and Yule, 1995]. Bothapproaches are highly relevant for the study of mentalretardation syndromes.
In the present study, behavioral phenomena wereassessed in four syndromes strongly associated withmental retardation, namely, fetal alcohol syndrome(FAS), Prader-Willi syndrome (PWS), fragile X syn-drome (FRAX), and tuberosis sclerosis (TSC). Using thesame questionnaire developed for behaviors specific tomental retardation syndromes, we aimed at a compar-ison of behavioral profiles in order to identify behaviorthat might be specific to the syndromes under study.Furthermore, wewere interested in the extent the beha-vioral profiles were moderated by shared or syndrome-specific variables in the various groups.
Children with fetal alcohol syndrome have a broadscale of both developmental hazards and psychopatho-logical symptoms not confined only to hyperkinetic dis-orders. A strong persistence over time was found bothfor cognitive functioning and psychopathology [Spohr
*Correspondence to: Dr. Hans-Christoph Steinhausen,Department of Child and Adolescent Psychiatry, Universityof Zurich, Neumunsterallee 9, Postfach, CH-8032 Zurich,Switzerland. E-mail: [email protected]
Received 13 August 2001; Accepted 17 April 2002
DOI 10.1002/ajmg.10627
� 2002 Wiley-Liss, Inc.

et al., 1993; Steinhausen et al., 1993, 1994; Spohr andSteinhausen, 1996; Steinhausen andSpohr, 1998]. PWSpatients have been shown to display a variety ofabnormal behavior, including temper tantrums, stub-bornness,manipulative and controlling behavior, obses-sive-compulsive features, and difficultieswith change inroutines [Dykens andCassidy, 1996; vanLieshout et al.,1998a, 1998b; Akefeldt andGillberg, 1999;Einfeld et al.,1999; State et al., 1999]. Psychiatric diagnoses in adultsmay include schizophrenia, bipolar disorder, and obses-sive-compulsive disorder [Gunay-Aygun et al., 1997;Clarke et al., 1998; Verhoeven et al., 1998, 2000].
In the FRAX syndrome, behavioral symptoms such asattention-deficit hyperactivity disorder (ADHD), autis-tic behavior, and speech and motor developmentaldelays predominate [Hagerman, 1996]. In TSC, intelli-gence varies from the normal range to mental retarda-tion in about 50%–60% of patients. The number andposition of brain lesions influencenot only the severity ofseizures and learning difficulties, but also the severity oftypical behavioral problems such as sleep problems,autism, and hyperactivity [Harrison and Bolton, 1997].
MATERIALS AND METHODS
Samples
Theparents of children in four syndromegroupsparti-cipated in this study concernedwith possible behavioraland emotional differences in children and adolescentswith mental retardation. The FAS sample consisted ofparents of 38 children newly diagnosed at a specializedGerman pediatric center headed by one of the authors(H.-L.S.) with extensive expertise in the assessment andtreatment of these children. There were 19 boys and19 girls in the sample. The age ranged from 4 to 12 years(mean, 6.3� 2.7). Diagnoses weremade according to thecriteria set out by the Research Society on Alcoholism[Sokol and Clarren, 1989]. These criteria require con-firmation of history of maternal alcohol abuse and eachof the following characteristics: prenatal or postnatalgrowth retardation, CNS dysfunction, and syndrome-specific craniofacial abnormalities.Due to the severity ofmental retardation and the young age, formal intelli-gence testing was possible only in 24 patients. Intelli-gencewasnormal innine (26.3%of the entire sample), inthe borderline range in another 9 (23.7%), and in therange of mental retardation in six (15.8%). Based onclinical assessment, another four patients (10.4%) wereclearly mentally retarded.
The PWS sample was taken from a larger series of 58patients who were diagnosed in two German and Swisscenters by genetic and pediatric experts (B.P.H. andU.E.) according to the consensus diagnostic criteria asdescribed by Holm et al. [1993]. From this sample, alladult patients and those with clinical diagnoses onlywere excluded. The remaining PWS sample consisted of39 patients and contained 16 male and 23 femalepatients ranging from 3 to 16 years (mean, 7.8� 4.0).The PWS sample showed paternal deletions in 25patients, maternal uniparental disomy in 9 patients,and imprinting accounted for 1 patient. Inactivation ofpaternally derived genes in the PWS region by use of the
methylation test was proven in another four patients.Mild mental retardation was present in 16 patients(41.0%) and severe retardation in 7 patients (17.9 %); 8patients (20.5%) showedborderline intelligence,whereas4 patients (10.2%) displayed normal intelligence. Datawere missing in another four patients.
A group of 49 boys with full-mutation FRAX aged 5.7to 16.10 years (mean, 8.6� 2.9) and 16 boys with TSCaged 5.0 to 17.7 years (mean, 9.5� 2.9) were recruitedthrough institutes of genetics and parental self-helpgroups. Girls were excluded from the study. Full-mutation FRAX boys are known to have higher rates ofmore severe comorbid psychiatric disorders, as they donot have a second X chromosome to compensate theeffects of themutation. Due to these differences, it is notsensible to include full-mutation boys and girls in thesame study. Only boys with TSC were examined toachieveahomogeneous control group for theFRAXboys.Furthermore, onlyboyswhowereable tounderstand theinstructions of the intelligence testswere included in thestudy. Severely affected children with TSC had thus tobe excluded [Backes et al., 2000]. In the FRAX sample,7 patients (14.3%) scored in themildmental retardationrange and 35 patients (71.4%) were severely mentallyretarded. Data were missing in another seven patients(14.3%). Clinically, these patients were severely men-tally retarded. The TSC sample comprised four patients(25.1%) with borderline intelligence, five (31.3%) withmild mental retardation, and seven (43.8%) with severemental retardation. Besides the difference in gendercomposition, there was also a significant age differenceacross the four samples (F¼ 6.114, df¼3, P¼ 001).
Procedure
Questionnaires and tests were completed when visit-ing the clinical centers, i.e., institutes of genetics,departments of pediatrics, and child and adolescentpsychiatric clinics.
Questionnaire datawere collected by using theDevel-opmental Behavior Checklist (DBC) by Einfeld andTonge [1992, 1995], with parents serving as responders.TheDBC is a standardized instrument completed by layinformants to assess behavioral and emotional distur-bance in children and adolescents with mental retarda-tion. It covers 96 behavioral items, including two openquestions that are rated on a three-point scale rangingfrom 0 (not true) to 1 (somewhat or sometimes true) to 2(very true or often true). The DBC has good psycho-metric properties [Einfeld and Tonge, 1992, 1995] andhas also been used for the assessment of populationprevalence of psychopathology of mentally retardedchildren and adolescents [Einfeld and Tonge, 1996a,1996b].
Based on the 94 items, a total score and six subscalesbased on factorial analyses can be computed. These sub-scales have been slightly revised based on more recentnew analyses by Einfeld and Tonge [1996c]. The sixsubscales are labeled disruptive, self-absorbed, com-munication disturbance, anxiety, autistic relating, andantisocial. Because of a lack of a standardized scale forthe DBC scores, we computed raw scores for the six
382 Steinhausen et al.

subscales and transformed them into weighted rawscores (total subscore divided by the number of items ofthe respective subscale). Thus, thevarious subscales canbe compared across the various samples.
Intelligence was assessed in three of the four samples(FAS, FRAX, TSC) by using the Kaufman AssessmentBattery for Children (K-ABC) [Kaufman and Kaufman,1983]. The following four subscores were computed:achievement, mental processing composite, simulta-neous processing, and sequential processing. Scoreswere based on the German standardization [Melchersand Preuss, 1992]. In the PWS sample, various tests ofintelligence and development were used so that thesedata were not included in the analyses.
RESULTS
As a test for the specificity of a behavioral phenotype,the frequencies of the 94 items of the DBC were com-pared across the four samples. In view of the limitedsample sizes, the 0 (not true) scores were contrastedwith the combined 1 and 2 (somewhat or sometimes andvery or often true) scores. Significant behavior differ-ences across the four syndromes are shown in Table I,with the items ordered according to the subscale struc-ture. Two syndromes, namely FAS and FRAX, standout with regard to their very high frequencies of be-havioral abnormalities. A smaller number of behavioralitems are marked by high frequencies in the PWSsample, whereas the TSC sample shows the smallestnumber of items with enlarged frequencies of behaviorabnormalities.
In Table I, the highest frequencies (in percentages)are underlined so that for each item the most specificallocation to one of the four syndromes becomes appa-rent. In a few items, the frequencies are rather similarfor two of the four syndromes as shown by dotted under-lining. With 49/94 items showing significant differencesacross the four syndromes, the findings in general arenot indicative of chance findings only. However, a con-servative control of type 1 error is warranted so that thefollowing description of behavioral features in the var-ious syndromes will consider differences at a P< 0.005level only.
The FAS sample is characterized by high frequencieson all items of the disruptive subscale, with most fre-quencies exceeding those of the FRAX sample, whichcomes second in this domain. The behavioral patternof the FAS sample is thus most specifically described bythe following items: abusive/swears, irritable, jealous,kicks/hits, rapid mood changes, noisy, overly attention-seeking, throws or breaks objects, and manipulative.In the self-absorbed subscale, FAS children are furthermarked by the following items: flicks/taps, overactive,and screams. There is no specific behavioral patternin the domains of communication disturbance, anxiety,autistic relating, and antisocial. Among further itemsthat are not included in one of the six subscale of theDBC, one finds further indications of a specific beha-vioral pattern that is marked by descriptions such asinability to attend, running away, being easily dis-turbed, and loss of appetite.
The PWS sample does not show any specific patternin the disruptive subscale and is characterized by a fewitems across the other subscales only. These pertain tothe following behavioral items: preference to do thingson his/her own, talking to self or imaginary people orobjects, beingupset anddistressed over small changes inroutines or environment, moving slowly/being under-active, and gorging food.
In the FRAX sample, there are similarities both interms of types and frequencies of behavioral phenomenawith the FAS samples. In the subscale measuring dis-ruptive behaviors, the following items are most charac-teristic: overexcited/impulsive and (similar to the FASsample) also abusive/swears, irritable, and attention-seeking. There are further specific abnormalities in thedomain of self-absorbed behavior as indicated by thefollowing items: chewing or mouthing objects or bodyparts, hittingorbiting self, hummingor othernonspeechnoises, whereas the very high frequencies of overactivebehavior and the high frequency of the item ‘‘flicks, taps,and twists objects’’ are shared by both the FRAX and theFAS sample.
FRAX patients are further marked by repetitivewords andphrases, unconnected thoughts in thedomainof communication disturbance, shyness, and the follow-ing features of autistic relating: avoidance of eye con-tact, laughing and giggling for no obvious reasons, andrepeated movements of various body parts. Further-more, outside the six major domains of the DBC, theyfrequently arrange objects or routines in a strictmannerand all or almost all FRAX patients are inattentive andeasily distracted. Finally, a larger proportion than in allother syndromes lacks self-confidence and self-esteem.
The fourth sample of the present study, the TSCsample, is the least abnormal in terms of behavior anddoes not show a single item that is specific to the TSCsyndromewhen compared to the other three syndromes.
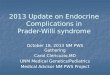
In a second step of the analyses, the total score andthe six subscales of the DBC were compared across thefour syndromes. There were significant differences(F¼11.41, df¼3, P<0.001) of the total score acrossthe four samples, as shown in Table II, with FAS andFRAX on the one hand and PWS and TSC on the otherhand, forming two homogeneous subsets. The behaviorprofilesof the fourgroupsareshowninFigure1.The fourprofilesdifferhighly significantly fromeachother (Wilkslambda¼0.545, F¼5.02, df¼18;376, P< 0.001). Thisholds true also for all six subscales (each P� 0.001).Posthoc tests indicated that FRAX and FAS on the onehandandPWSandTSCon the other hand formseparatesubgroups on the following three scales: disruptive, self-absorbed, and anxiety. The differentiation is less clearfor the subscales measuring communication distur-bance, autistic relating, andantisocial. ThePWSsampleforms homogeneous subsets with all other samples asregards the subscales measuring communication dis-turbance and antisocial, whereas the FAS sample formshomogeneous subgroups with all other groups on theautistic relating subscale.
Finally, a test was made whether or not intelligence,age, or gender had any significant association withthe various DBC scores. Computation of correlation
Behavioral Phenotypes in Mental Retardation 383

TABLE
I.Frequen
cyof
Beh
avioralAbnormalities
inFou
rSyndromes*
Item
no.
Description
FAS(n
¼38)
PWS(n
¼42)
FRAX(n
¼49)
TSC(n
¼16)
Chi-sq
uare
Pn
%n
%n
%n
%
Subscale
1:disru
ptive
4.
Abusive,
swea
rsatothers
22
57.9
10
25.6
26
53.1
318.8
14.10
0.003
7.
Becom
esov
erex
cited
25
65.8
18
46.2
35
71.4
425.0
13.95
0.003
35.
Impulsive,
actsbeforethinking
26
68.4
18
46.2
39
79.6
956.3
11.37
0.01
37.
Irritable
22
57.9
10
25.6
29
59.2
531.3
13.47
0.004
38.
Jea
lous
24
63.2
12
30.8
27
55.1
743.8
9.14
0.03
39.
Kicks,
hitsothers
10
73.7
10
25.6
26
53.1
531.3
20.12
<0.001
46.
Moo
dch
anges
rapidly
fornoapparentreason
12
68.4
14
35.9
29
59.2
318.8
16.14
0.001
48.
Noisy
orboisterou
s30
78.9
512.8
28
57.1
531.3
37.36
<0.001
52.
Overly
atten
tion
-seeking
30
78.9
15
38.5
38
77.6
10
62.5
18.87
<0.001
85.
Throwsor
breaksob
jects
25
65.8
512.8
24
49.0
318.8
27.6
<0.001
86.
Tries
tomanipulate
orprovok
eothers
24
63.2
10
25.6
20
40.8
425
13.22
0.004
Subscale
2:self-absorbed
10.
Chew
sor
mou
thsob
jects,
orbod
yparts
22
57.9
13
33.3
36
73.5
425.0
19.69
<0.001
23.
Flick
s,taps,
twirls
objectsrepea
tedly
17
44.7
410.3
21
42.9
212.5
16.98
0.001
24.
Fussyea
teror
hasfood
fads
20
52.6
820.5
14
28.6
17.98
<0.001
31.
Hitsor
bites
self
923.7
37.7
24
49.0
318.8
19.92
<0.001
32.
Hums,
whines,gru
nts,sq
uea
ks,
ormakes
other
non
spee
chnoises
12
31.6
410.3
31
63.3
16.3
34.18
<0.001
49.
Overactive,
restless,unable
tositstill
30
78.9
25.1
44
89.8
850.0
72.87
<0.001
56.
Prefers
todothingson
his/her
own;tendsto
bealoner
718.4
27
69.2
20
40.8
425.0
22.58
<0.001
63.
Smells,tastes,or
lick
sob
jects
10
26.3
14
35.9
27
55.1
425.0
9.41
0.02
65.
Screa
msalot
21
55.3
820.5
19
38.8
425.0
11.08
0.01
67.
Staresatlights
orsp
inningob
jects
615.8
410.3
17
34.7
212.5
9.74
0.02
93.
Wandersaim
lessly
14
36.8
12.6
11
22.4
9.34
<0.001
Subscale
3:communication
disturbance
61.
Rep
eats
back
whatotherssa
ylikeanecho
20
52.6
10
25.6
26
53.1
318.8
12.08
0.07
62.
Rep
eats
thesa
mewordor
phrasesov
erandov
er15
39.5
14
35.5
33
67.3
425.0
14.05
0.003
81.
Talksto
selfor
imaginary
peo
ple
orob
jects
14
36.8
24
61.5
21
42.9
18.17
<0.001
83.
Thou
ghts
are
unconnected
20
2.6
717.9
26
53.1
425.0
15.39
0.002
88.
Unrealisticallyhappyor
elated
11
28.9
819.0
19
38.8
16.3
8.38
0.04
Subscale
4:anxiety
21.
Fea
rsparticularthingsor
situation
s24
63.2
11
28.2
22
44.9
850.0
9.61
0.02
36.
Ignores
soundsor
coversea
rsto
variou
ssounds
821.1
38.1
20
40.8
637.5
13.95
0.03
74.
Shy
821.1
16
41.0
28
57.1
425.0
13.27
0.004
90.
Upsetanddistressedov
ersm
allch
anges
inroutineor
environ
men
t13
34.2
33
84.6
33
67.3
637.5
24.82
<0.001
Subscale
5:autistic
relating
2.
Avoidsey
econtact
14
36.8
11
28.2
33
67.3
743.8
15.29
0.002
22.
Facialtw
itch
esor
grimaces
11
28.9
410.3
14
28.6
16.3
7.92
0.05
41.
Laughsor
gigglesfornoob
viousreason
15
39.5
512.8
30
61.2
425.0
22.89
<0.001
47.
Mov
esslow
ly,underactive
718.4
24
61.5
19
38.8
212.5
19.97
<0.001
59.
Rep
eatedmov
emen
tsof
hands,
bod
y,hea
d,or
face
11
28.9
410.3
27
55.1
318.8
22.05
<0.001
Subscale
6:antisocial
30.
Hides
things
20
52.6
14
35.9
12
24.5
212.5
11.24
0.01
Further
item
s5.
Arranges
objectsor
routines
inastrict
order
410.5
12
30.8
21
42.9
318.8
11.90
0.008
8.
Bites
others
13
34.2
25.1
15
30.6
16.3
14.28
0.003

coefficients between the four K-ABC intelligence scoresand the six DBC subscale scores in a total of 88 subjects(excluding PWS subjects) ranged from r¼�0.10 to 0.09and did not result in any significant association betweenintelligence and behavior. Furthermore, age did not cor-relate significantly with the DBC total score (r¼�0.09)in the total sample of 142 patients and gender was alsonot significantly associated with the DBC total score(chi-square¼0.63, df¼ 1) in the PWS and FAS sample(n¼77).
DISCUSSION
The findings of the present study are relevant intwo ways, namely, with regard to the measurement ofbehavior in mental retardation syndromes and withregard to the delineation of distinct behavioral pheno-types in these syndromes. From a methodological pointof view, the dimensional approach in measuring beha-vioral phenomena as represented by the DBC provedeffective in detecting subtle behavioral differences infour different syndromes. The use of a questionnaire forcaregivers is effective, economic, and,most importantly,specific because itmeasures behaviors that are frequentin individuals with mental retardation but infrequentin normal-functioning individuals. Disadvantages mayinclude certain errors such as leniency or severity errorwhen behavior is judged too leniently or too severely.
In the delineation of distinct behavioral phenotypes,the DBC contributed to clear behavioral differentia-tions across the four syndromes. These differentiationsapplied to both type andmagnitude of behavioral abnor-malities. Both the comparison of items and aggregatedsubscales indicated that FAS and FRAX are the twosyndromes with the highest number and frequencies ofbehavioral abnormalities. In contrast, PWS is markedonly by a few specific behavioral phenomena, whereasTSC lacks any specific characteristics.
The FAS sample, both on the more molecular itemand the aggregated subscale level, shows a pattern thatis dominated by disruptive and overactive-inattentivebehavior. This pattern is very much in accordance withprevious empirical studies that have emphasized thedominance of attentiondeficits andhyperactivity inFASchildren [Steinhausen et al., 1993; Streissguth et al.,1996]. However, a variety of other behavioral pheno-mena have been particularly noted in previous studiesby some of the present authors, including disruptive be-havior in terms of a conduct disorder type [Steinhausenet al., 1993].
The findings in the PWSsample are less impressive asfar as a distinct behavioral phenotype is concerned. Thismaybepartlydue to theyoungageof thepresent sample.
9.
Cannot
atten
dto
oneactivityforanylength
oftime,poo
ratten
tion
span
31
81.6
14
35.9
49
100.0
11
68.8
47.94
<0.001
12.
Deliberately
runsaway
22
57.9
18
20.5
918.4
212.5
21.63
<0.001
17.
Easily
distracted
from
task
37
97.4
23
59.0
48
98.0
11
68.8
32.77
<0.001
25.
Gorges
food
923.7
24
61.5
9.0
18.4
16.3
26.50
<0.001
40.
Lack
sself-con
fiden
ce,poorself-estee
m18
47.2
820.5
30
61.2
850.0
14.90
0.002
44.
Lossof
appetite
17
44.7
410.3
510.2
25.17
<0.001
55.
Prefers
thecompanyof
adultsor
you
nger
children
17
44.7
24
61.5
38
77.6
850.0
10.71
0.01
64.
Scratches
orpickssk
in15
10.3
24
61.5
24
49.0
212.5
9.22
0.008
89.
Unusu
albod
ymov
emen
ts,posture,or
wayof
walking
10
26.3
14
35.9
26
53.1
212.5
11.47
0.009
*,indicatesthegroupwithhighestitem
freq
uen
cy;----indicatesthetw
ogroupswithhighestandsimilaritem
freq
uen
cies.
TABLE II. Total DBC Scores in the Four Samples
FAS(n¼ 38)
PWS(n¼ 39)
FRAX(n¼ 49)
TSC(n¼ 16)
Mean 54.1 32.7 54.2 27.3SD 31.1 15.3 22.0 19.5Range 3–133 3–66 17–105 6–64
Behavioral Phenotypes in Mental Retardation 385

In this sample, the socially withdrawn behavior of thesepatients in combination with some indication of obses-sive features in terms of being upset and distressed oversmall changes in routines or environments and theassociation with the appetite disturbance fit nicely intothe known behavioral features of the PWS [Dykens andCassidy,1996; AkefeldtandGillberg,1999;Einfeldetal.,1999; State et al., 1999]. Due to different methods andcontrast groups, it is difficult to compare the presentstudy’s findingswith those by vanLieshout et al. [1998a,1998b], who studied both behavioral and personalityphenotypes using methods that are more suitable forsubjects with normal intelligence.
The FRAX sample showed the most complex beha-vioral pattern among all four syndromes that were stu-died by us. Their disruptive and self-absorbed behaviorswere only slightly different from the FAS sample intermsof thecompositionofvarious items.FRAXpatientsshare the high load of attention deficit andhyperactivitywith FAS patients, and both can be considered as vari-ants of the common ADHD that is seen frequently inchild psychiatric patients of normal intelligence. Takingthe similarities ofFRAXandFAS into consideration, it isperhaps the autistic pattern of behavior that differsmost between the two syndromes.
As shown previously, the most common DSM-IVdiagnosis among the FRAX boys was ADHD (74%),followed by oppositional defiant disorder (29%), func-tional enuresis (27%), functional encopresis (20%), sepa-ration anxiety disorder (10%), and one child (2%) withan obsessive-compulsive disorder [Backes et al., 2000].In addition, 18% (n¼ 9) fulfilled the criteria for anautistic disorder.
This is in accordance with most other studies thathave reported hyperactivity in the majority of boyswith FRAX [Hagerman, 1996]. Even in a comparisonto IQ-matched controls, ADHD remained a signifi-
cant problem [Baumgardner et al., 1995]. In contrast,the association with autism is far more controversial.Although autistic symptoms such as avoidance gazeand bodily contact, tactile defensiveness, preservations,and hand flapping are common, childrenwith FRAX areinterested in communication and dialogue [Wolf-Scheinet al., 1987; Hagerman, 1996]. Although 15% fulfillDSM-IV criteria for an autistic disorder [Baumgardneret al., 1995], their specific communication deficits arenot due to a lack of interpersonal empathy, but rather tosocial anxiety.
While the comparison of behavioral items anddomains across the four syndromes does not indicatethat TSC does not imply some vulnerability for beha-vioral abnormality, our findings clearly show that thesepatients are the least abnormal among the four syn-dromes. In addition, the psychiatric comorbidity amongthe TSC children was lower, the types of disorderssimilar to those of the FXS boys. ADHD was the mostcommon diagnosis (44%), again followed by oppositionaldefiantdisorder(25%),separationanxietydisorder (19%),functional enuresis in two, and functional encopresis inone child. No child fulfilled the criteria for an autisticdisorder [Backes et al., 2000]. This psychiatric comor-bidity is much lower than reported in other studies with40%–60% of TSC children showing hyperactivity and50% autism [Harrison and Bolton, 1997]. This is mainlydue to selection effects, as only children who could betested psychometrically were recruited for the study.The more severely affected children were thereforeexcluded.
The study of the associations of certain mental retar-dation syndromes and behavioral phenotypes startedfrom the general assumption that there should be amajor association between either teratogenic (FAS)or genetic (PW, FRAX, TSC) syndrome and behavior.However, one has to consider both within-syndrome
Fig. 1. Mean DBC profiles in four mental retardation syndromes.
386 Steinhausen et al.

variation and individual differences in behavioral phe-notypes [Dykens and Hodapp, 2001]. This conclusion isclearly supported by the varying frequencies of beha-viors in the four syndromes, with only two items ofinattentiveness and distractibility reaching a 100% or98% in the FRAX sample.
We also looked for moderating variables other thanthe syndrome itself. There was no indication that theobserved behavior patterns in FAS, FRAX, and TSCvaried systematically with intelligence. However, it hasto be admitted that mentally more severely affectedTSC patients were not included in the study and thatthe K-ABC test findings may be suffering from a flooreffect, i.e., insufficient differentiation in the range ofmental retardation. Furthermore, our findings shouldnot be confused with the well-established association ofincreased psychopathological vulnerability in mentalretardation in general [Dykens, 2000].
The lack of a gender impact in our relatively youngFAS and PWS patients matches findings in normalfunctioning patients. There is no gender difference interms of frequency of general psychopathology also intheseindividualsbeforeadolescence[Steinhausen,1992].Furthermore, the lack of a significant association be-tween age and total score of behavioral abnormalitiesunderlines the fact that, besides gender, age duringchildhood and adolescence is also not a confounder ofbehavioral phenotypes in the four mental retardationsyndromes under study.
REFERENCES
Akefeldt A, Gillberg C. 1999. Behavior and personality characteristics ofchildren and young adults with Prader-Willi syndrome: a controlledstudy. J Am Acad Child Adolesc Psychiatry 38:761–769.
BackesM,GencB,DoerflerW,Schreck J,LehmkuhlG, vonGontardA.2000.Cognitive and behavioral profile of fragile X boys: correlations tomolecular data. Am J Med Genet 95:150–156.
Baumgardner T, Reiss AL, Freund LS, Abrams MP. 1995. Specifications ofthe neurobehavioral associations in males with fragile X syndrome.Pediatrics 95:744–752.
Clarke D, Boer H, Webb T, Scott P, Frazer S, Vogels A, Borghgraef M,Curfs LMG. 1998. Prader-Willi-syndrome and psychotic symptoms:I, case descriptions and genetic studies. J Intell Disab Res 42:440–450.
Dykens EM. 2000. Annotation: psychopathology in children with intellec-tual disability. J Child Psychol Psychiat 41:407–417.
Dykens EM, Cassidy SB. 1996. Prader-Willi syndrome: genetic, behavioral,and treatment issues. Child Adolesc Psychiatr Clin North Am 5:913–927.
Dykens EM, Hodapp RM. 2001. Research in mental retardation: toward anetiologic approach. J Child Psychol Psychiat 42:49–71.
Einfeld SL, Tonge BJ. 1992. Manual for the developmental behaviourchecklist: primary care version (DBC-P). Australia: University of NewSouth Wales and Monash University.
Einfeld SL, Tonge BJ. 1995. The developmental behavior checklist: thedevelopment and validation of an instrument to assess behavioral andemotional disturbance in children and adolescents with mentalretardation. J Aut Dev Disord 25:81–104.
Einfeld SL, Tonge BJ. 1996a. Population prevalence of psychopathology inchildren and adolescents with intellectual disability: I, rationale andmethods. J Intell Disab Res 40:91–98.
Einfeld SL, Tonge BJ. 1996b. Population prevalence of psychopathology inchildren and adolescents with intellectual disability: II, epidemiologicalfindings. J Intell Disab Res 40:99–109.
Einfeld SL, Tonge BJ. 1996c. Personal communication: amendments to themanual for the developmental behaviour checklist, primary carerversion (DBC-P). Australia: University of New South Wales andMonash University.
Einfeld SL, Smith A, Durvasula S, Florio T, Tonge BJ. 1999. Behavior andemotional disturbance in Prader-Willi-syndrome. Am J Med Genet82:123–127.
Flint J, Yule W. 1994. Behavioral phenotypes. In: Rutter M, Taylor E,Hersov L, editors. Child and adolescent psychiatry, 3rd ed. Oxford:Blackwell Scientific. p 666–687.
Gunay-Aygun M, Cassidy SB, Nicholls RD. 1997. Prader-Willi and othersyndromes associatedwith obesity andmental retardation.BehavGenet27:307–324.
Hagerman RJ. 1996. Physical and Behavioral Phenotype In: Hagerman RJ,Cronister A, editors. Fragile X syndrome: diagnosis, treatment, andresearch. Baltimore, MD: Johns Hopkins University Press. p 3–87.
Harrison JE, Bolton PF. 1997. Annotation: tuberous sclerosis. J ChildPsychol Psychiat 38:603–614.
Holm VA, Cassidy SB, Butler MG, Hanchett JM, Greenswag LR,Whitman BY, Greenberg F. 1993. Prader-Willi syndrome: consensusdiagnostic criteria. Pediatrics 91:398–402.
Kaufman AS, Kaufman NL. 1983. (K-ABC): Kaufman Assessment Batteryfor Children. Circle Pines, MN: American Guidance Service.
Melchers P, PreussU. 1992. Bearbeitung derKaufman-Assessment Batteryfor Children (K-ABC) fur den deutschsprachigen Raum. Teil 1 und 2.Zeitschrift fur Kinder und Jugendspaychiatric 20:85–93 and 223–231.
O’Brien G, YuleW. 1995. Why behavioural phenotypes? In: O’Brien G, YuleW, editors. Behavioural phenotypes. Cambridge: Cambridge UniversityPress. p 1–23.
Sokol RJ, Clarren SK. 1989.Guidelines for use of terminology describing theimpact of prenatal alcohol on the offspring. Alcoholism 13:597–598.
Spohr HL, Steinhausen H-C. editors. 1996. Alcohol, pregnancy and thedeveloping child. Cambridge: Cambridge University Press.
Spohr HL,Willms J, SteinhausenH-C. 1993. Prenatal alcohol exposure andlong-term developmental consequences: a 10-year following of 60children with fetal alcohol syndrome (FAS). Lancet 341:907–910.
State MW, Dykens EM, Rosner B, Martin A, King BH. 1999. Obsessive-compulsive symptoms in Prader-Willi and ‘‘Prader-Willi-like’’ patients.J Am Acad Child Adolesc Psychiatry 38:329–334.
Steinhausen HC. 1992. Sex differences in developmental psychopathology.In: Remschmidt H, Schmidt MH, editors. Developmental psychopathol-ogy. Lewiston, NY: Hogrefe and Huber. p 7–16.
SteinhausenHC, Spohr HL. 1998. Long-term outcome of children with fetalalcohol syndrome: psychopathology, behavior, and intelligence. Alco-holism Clin Exp Res 22:334–338.
Steinhausen HC, Willms J, Spohr HL. 1993. Long-term psychopathologicaland cognitive outcome of children with fetal alcohol syndrome. J AmAcad Child Adolesc Psychiatry 32:990–994.
Steinhausen HC, Willms J, Spohr HL. 1994. Correlates of psychopathologyand intelligence in childrenwith fetal alcohol syndrome. J Child PsycholPsychiat 35:323–331.
Streissguth AP, Bookstein FL, Barr HM. 1996. A dose-response study of theenduring effects of prenatal alcohol exposure: birth to 14 years. In: SpohrHL, Steinhausen H-C, editors. Alcohol, pregnancy and the developingchild. Cambridge: Cambridge University Press, p 141–168.
van Lieshout CFM, de Meyer RE, Curfs LM, Koot HM, Fryns JP. 1998a.Problem behaviors and personality of children and adolescents withPrader-Willi syndrome. J Pediat Psychol 23:111–120.
van Lieshout CFM, de Meyer RE, Curfs LMG, Fryns JP. 1998b. Familycontexts, parental behavior, and personality profiles of children andadolescent with Prader-Willi, fragile-X, or Williams syndrome. J ChildPsychol Psychiat 39:699–710.
Verhoeven WMA, Curfs LMA, Tunier S. 1998. Prader-Willi syndrome andcycloid psychoses. J Intell Disab Res 42:455–462.
Verhoeven WMA, Tuiniers S, Curfs LMG. 2000. Prader-Willi psychiatricsyndrome and velo-cardio-facial psychiatric syndrome. Genet Counsel11:205–213.
Wolf-Schein EG, Sudhalter V, Cohen IL, Fisch GS, Hanson D, Pfadt AG,Hagerman R, Jenkins EC, Brown WT. 1987. Speech-language and thefragile-X-syndrome: initial findings. Am Speech Hearing Assoc 29:35–38.
Behavioral Phenotypes in Mental Retardation 387