-
8/11/2019 Beer 2006 Impact of Enzyme Replacement Therapy on
Cardiac Morphology and Function and Late Enhancement i
1/4
Impact of Enzyme Replacement Therapy on Cardiac Morphology and
Functionand Late Enhancement in Fabrys Cardiomyopathy
Meinrad Beer, MD a, *, Frank Weidemann, MD b , Frank Breunig, MD
b , Anita Knoll, MD b ,Sabrina Koeppe, MD a , Wolfram Machann, MD a
, Dietbert Hahn, MD a ,
Christoph Wanner, MD b , Jrg Strotmann, MD b , and Jrn
Sandstede, MD a
The present study evaluated the evolution of cardiac morphology,
function, and lateenhancement as a noninvasive marker of myocardial
brosis, and their inter-relationduring enzyme replacement therapy
in patients with Fabrys disease using magneticresonance imaging and
color Doppler myocardial imaging. Late enhancement, whichwas
present in up to 50% of patients, was associated with increased
left ventricularmass, the failure of a signicant regression of
hypertrophy during enzyme replace-ment therapy, and worse segmental
myocardial function. Late enhancement maypredict the effect of
enzyme replacement therapy on left ventricular mass and
cardiacfunction. 2006 Elsevier Inc. All rights reserved. (Am J
Cardiol 2006;97:15151518)
Fabrys disease is an X-linked lysosomal storage disordercaused
by a deciency of the enzyme -galactosidase and is
1 cause of unexplained left ventricular hypertrophy in
mid-dle-aged men. 1 Left ventricular hypertrophy is associatedwith
progressive myocardial brosis and followed by deathfrom heart
failure. 2 Besides hypertrophy, intramural myo-cardial contrast
enhancement (late enhancement [LE]), as amarker of increased
myocardial collagen content, 3 can bedemonstrated in patients with
Fabrys disease by gadolini-um-enhanced magnetic resonance imaging
(MRI). 4 Since2001, specic enzyme replacement therapy (ERT) for
-ga-lactosidase has become available, improving clinical symp-toms
as well as the capillary clearance of globotriaosylceramide. 5,6
Moreover, a decrease in left ventricular mass
and a reduction in left ventricular dysfunction have
beendemonstrated. 7 Whether those with evidence of LE respondto ERT
is unknown. Therefore, we performed a prospectivestudy to analyze
changes in LE under ERT and to determinethe impact of LE on
regional myocardial function in patientswith Fabrys disease.
Thirty-ve patients (mean age 39 10 years; 20 men)
withgenetically proved Fabrys disease were consecutively in-cluded
in the study. Seventeen patients were scheduled toreceive ERT (mean
age 41 8 years) because of theseverity of disease (male gender;
symptoms such as severeacroparesthesia and myalgia; and/or signs of
vital organ
involvement such as left ventricular hypertrophy, impairedkidney
function, central nervous system involvement; and
history of stroke).8
-Galactosidase (agalsidase ; Fabra-zyme, Genzyme Corporation,
Cambridge, Massachusetts)was given at a dose of 1 mg/kg body weight
intravenouslyevery 2 weeks for 12 months in an open-labeled study.
Theinvestigation conformed to the principles of the Declarationof
Helsinki. Written informed consent was obtained from allpatients,
and the study was approved by the local ethicscommittee.
MRI was performed with a 1.5-T scanner (MagnetomVISION, Siemens
Medical Systems, Erlangen, Germany).Short- and long-axis cine MRI
was performed using a seg-mented 2-dimensional spoiled-gradient
echo sequence (eld of
view 240 320 mm2
, matrix 126 256, repetition time 9.9ms, echo time 4.8 ms, ip
angle 30, slice thickness 8 mm).The same sequence was consistently
used for baseline andfollow-up examinations. Left ventricular mass,
volume, andfunction were analyzed as previously described. 9
Regionalwall motion was assessed visually by 2 experienced
observ-ers using the standard 17-segment model. 10 LE was ob-tained
10 to 15 minutes after the injection of gadopentetatedimeglumine
0.2 mmol/kg (Magnevist, Schering AG, Ber-lin, Germany) using an
inversion recovery 2-dimensionalturbo-gradient echo sequence (eld
of view 240 320mm2 , matrix 165 256, repetition time 7.5 ms, echo
time
3.4 ms, ip angle 25, inversion time determined individu-ally).
The quantitative evaluation of contrast enhancementwas performed as
previously described. 9 The mass of theenhanced area was obtained
by summing the volume foreach section and is expressed as a
percentage of total leftventricular muscle mass.
Real-time 2-dimensional color Doppler myocardial im-aging data
were recorded from the interventricular septumand the left
ventricular lateral and inferior walls using stan-dard apical 4-
and 2-chamber views to evaluate longitudinalfunction (Vivid V, GE
Vingmed Ultrasound AS, Horten,
a Institut fr Rntgendiagnostik and bMedizinische Klinik der
Univer-sitt Wrzburg, Wrzburg, Germany. Manuscript received June 29,
2005;revised manuscript received and accepted November 28,
2005.
Drs. Breunig, Strotmann, Wanner, and Weidemann received
speakershonoraria or grant support from Genzyme CEE GmbH, Konstanz,
Ger-many.
* Corresponding author: Tel: 49-931-201-34884; fax:
49-931-201-34857.
E-mail address: [email protected] (M. Beer).
0002-9149/06/$ see front matter 2006 Elsevier Inc. All rights
reserved. www.AJConline.orgdoi:10.1016/j.amjcard.2005.11.087
-
8/11/2019 Beer 2006 Impact of Enzyme Replacement Therapy on
Cardiac Morphology and Function and Late Enhancement i
2/4
Norway; 3.5 MHz). Color Doppler myocardial imaging datawere
analyzed using dedicated software (TVI, GE VingmedUltrasound AS) as
described previously. 7 Briey, the regionof interest was
continuously positioned within the segmentbeing interrogated using
a semi-automatic tracking algo-rithm to derive strain-rate proles
from the at-risk seg-ments. From the resulting strain rate and
strain curves, peak systolic strain rate and systolic strain were
measured. Usingthe apical 4- and 2-chamber views, myocardial
function in12 segments in every patient was assessed. After
analyzingmyocardial function in these segments, every segment
wasassigned to be LE positive or LE negative. Matching
thesegmentation between MRI and echocardiography was doneusing the
standard 17-segment model. 10
All data are presented as mean SD. The Mann-Whit-ney U test was
used to determine differences between pa-tients with and without
LE. The nonparametric Wilcoxonsmatched-pairs test was used to
evaluate differences betweenbaseline and follow-up examination
results. Pearsons cor-relation coefcient was used for the
comparison of MRIdata (LE vs left ventricular mass). A p value of
0.05 wasconsidered statistically signicant. The interpreters of
theMRI data were blinded to the echocardiographic data, andthe
interpreters of the echocardiographic data were blindedto the MRI
data.
The baseline examinations of all 35 included patientsrevealed LE
(0.5 1.0% of left ventricular mass) in 11patients (31%). Two of the
15 female patients displayed LE(1.1% and 2.3% of left ventricular
mass). Left ventricularmass (mean 158 60 g) was correlated with the
extentof LE (r 0.54, p 0.0001). The baseline examinations of the 17
patients scheduled for ERT detected LE in 47% of patients (8 of
17), with restriction to the inferior or lateralwall of the left
ventricle in 6 patients and the anterior orseptal parts in 2
patients. Within these regions, LE wasdistributed intramurally (6
of 8 patients) and subepicardially(2 of 8 patients). No patient
showed involvement of thesubendocardial layer. Quantitative
analysis showed LE tobe 1.3 1.1% or 2.5 2.0 ml (range 0.5 to 3.8%
or 0.8 to
6.8 ml) of total left ventricular mass. Patients with LE
hadlarger left ventricular masses (211 58 vs 160 23 g, p0.046). No
signicant differences were found for all otherleft ventricular
morphologic parameters ( Table 1 ). Regionalfunction in the
segments displaying LE was signicantlyless compared with the
patients without LE (strain rate 1.00.3 vs 1.3 0.4 1/s, p 0.0001;
strain 8.6 5% vs 18.37.8%, p 0.001). Moreover, nonenhanced segments
of patients with 1 segment positive for LE also showedsevere
restriction of regional function in comparison withthe data of
patients without LE (strain rate 1.1 0.5 vs 1.30.4 1/s, p 0.01;
strain 10.5 8% vs 18.3 7.8%, p 0.001).
The follow-up examinations of patients with ERT showedno
regression of LE. In contrast, the amount of LE increasedfrom 1.3
1.1% to 2.6 2.1% or 2.5 2.0 to 4.9 3.1 ml(range 0.5 to 7.1% or 0.8
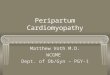
to 9.6 ml, p 0.028), as outlinedfor 1 patient in Figure 1. In
contrast, no patients without LEdeveloped LE during ERT. Signicant
regressions of leftventricular mass and volume occurred during ERT
( Table1). Separating patients according to the occurrence of
LE,
Figure 1. A 54-year-old man at baseline (upper panel) and after
1 year of ERT (lower panel) . The increase of LE (white arrows) is
clearly seen on3 contiguous short-axis views.
Table 1Baseline and follow-up data from patients scheduled for
enzyme replacement therapy
Parameter All Patients LE (positive) LE (negative) p Value for
LEPositive vs LE
Negative
Baseline(n 17)
Follow-up(n 17)
pValue
Baseline(n 8)
Follow-up(n 8)
pValue
Baseline(n 9)
Follow-up(n 9)
pValue
Baseline Follow-up
Left ventricular mass (g) 184 49* 168 53 0.003 211 58 195 64
0.161 160 23 145 27 0.008 0.046 0.074End-diastolic volume (ml) 141
29 121 47 0.039 144 27 120 50 0.123 138 31 122 47 0.214 0.481
0.888End-systolic volume (ml) 54 18 44 19 0.028 53 13 43 15 0.123
54 23 46 22 0.110 0.743 0.815Stroke volume (ml) 87 16 77 30 0.076
91 18 77 37 0.161 84 16 78 25 0.441 0.606 0.963Cardiac output
(l/min) 6.3 1.2 5.0 1.5 0.003 6.6 1.4 5.0 1.8 0.030 6.0 0.9 5.0 1.3
0.050 0.481 0.673Ejection fraction (%) 63 7 64 7 0.149 63 5 65 5
0.263 62 9 63 8 0.595 0.743 0.743LE (% left ventricular
mass)0.6 1.0* 1.2 1.9 0.028 1.3 1.1 2.6 2.1 0.028 0.0 0.0 0.0
0.0 1.000 0.000 0.000
* Correlating r 0.55; p 0.0017.
1516 The American Journal of Cardiology (www.AJConline.org)
-
8/11/2019 Beer 2006 Impact of Enzyme Replacement Therapy on
Cardiac Morphology and Function and Late Enhancement i
3/4
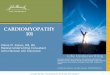
only patients without LE had signicant regressions of
leftventricular mass (p 0.008), whereas patients with LEshowed a
tendency toward the regression of left ventricularmass that did not
reach statistical signicance (p 0.161;Figure 2 ). Echocardiography
revealed an improvement of regional function in patients without LE
(strain rate 1.3 0.4 to 1.5 0.5 1/s, p 0.0001; strain 18.3 7.8%
to
20.5 6.8%, p 0.047). In addition, patients with LEshowed an
improvement of regional function, but it wasrestricted to
myocardial segments without LE (strain rate1.1 0.5 to 1.3 0.5 1/s,
p 0.003; strain 10.5 8% to14.2 8%, p 0.008). Segments with LE
showed nosignicant improvement (strain rate 1.0 0.3 to 1.2 0.41/s,
p 0.05; strain 8.6 5% to 12.5 5%, p 0.05).
The incidence and distribution resembled the pattern of
LEobserved in other forms of cardiomyopathy. 1113 The
greaterpercentage of hyperenhanced myocardium and the
bettercorrelation of hyperenhancement related to the left
ventric-ular mass index in a previous study of patients with
Fabrysdisease 4 can be explained by the greater degree of
leftventricular hypertrophy in this previous study (left
ventric-ular mass 188 vs 100 g/m 2 [LE positive vs LE
negative]compared with 115 vs 85 g/m 2 in our study). LE did
in-crease during follow-up. Compared with the small magni-tude of
LE (percentage left ventricular mass), the follow-upincrease in LE
was large, a doubling over 1 year. There areseveral possible
explanations. First of all, one must becautious to rule out
artifactual reasons. However, the ap-plied technique of manual
planimetry (for the quanticationof LE) has high reproducibility, as
recently shown 14,15 ; allinvestigators were already experienced
analyzers of cardiac
magnetic resonance images including LE; and all examina-tions
were performed using the same magnetic resonancescanner and the
same acquisition protocol. Nevertheless,one cannot rule out that
ERT has a disproportionate effecton background interstitial brosis
rather than focal brosis,so that a reduction in background
paradoxically makes focalbrosis more prominent. The impaired
ability of LE imag-
ing to discriminate diffuse brosis has already been dis-cussed
for subgroups of patients with dilated cardiomyop-athy. 12
LE was associated with impaired cardiovascular im-provement
during ERT according to changes in left ventric-ular mass and
regional function, as shown for other forms of cardiomyopathy. 13
Only patients without LE had signicantreductions in left
ventricular mass during ERT, as well asimprovements in regional
myocardial function. Patientswith LE in 1 part of the left
ventricle also showed restric-tions in myocardial function in all
other parts of the leftventricle.
The limitations of this study include a lack of
follow-upexaminations of equally ill patients without ERT because
of the limited number of patients with Fabrys disease andethical
concerns about postponing ERT in patients for theadvantage of
follow-up magnetic resonance examinations.Therefore, we do not know
the natural course of LE devel-opment in Fabrys disease, and thus
we do not knowwhether the fact that none of the patients who did
not haveLE at baseline developed LE during ERT was a success dueto
ERT. Second, none of the patients had clinical historiesof coronary
artery disease, elevated plasma creatine kinaselevels, or
electrocardiographic signs of coronary artery dis-ease. However,
coronary angiography had not been per-
Figure 2. Changes in left ventricular mass during ERT. Only
patients without LE showed signicant regressions of left
ventricular mass. (A) Patients withLE; (B) patients without LE. *p
0.01 baseline versus 12 months; # p 0.05 baseline, patients without
LE versus patients with LE.
1517Cardiomyopathy/Late Enhancement in Fabrys Disease
-
8/11/2019 Beer 2006 Impact of Enzyme Replacement Therapy on
Cardiac Morphology and Function and Late Enhancement i
4/4
formed. Nevertheless, the preferential intramural pattern of LE
observed in our patients resembled that described forother forms of
cardiomyopathy 1113 and is completely dif-ferent from the
subendocardial or transmural pattern ob-served in coronary artery
disease. 16 Moreover, a previousstudy by Moon et al 4 excluded
coronary artery disease in
patients with Fabrys disease despite the presence of LE.
Acknowledgment: We thank Bettina Borst for her excel-lent
technical assistance in our MRI studies.
1. Sachdev B, Takenaka T, Teraguchi H, Tei C, Lee P, McKenna
WJ,Elliott PM. Prevalence of Anderson-Fabry disease in male
patientswith late onset hypertrophic cardiomyopathy. Circulation
2002;105:14071411.
2. Desnick RJ, Ioannou YA, Eng CM. -Galactosidase A
deciency:Fabry disease. In: Scriver CR, Beaudet AL, Sly WS, Valle
D, eds. TheMetabolic and Molecular Bases of Inherited Disease, Vol.
3. 8th Ed.
New York, New York: McGraw-Hill, 2001:37333774.3. Moon JC, Reed
E, Sheppard MN, Elkington AG, Ho SY, Burke M,Petrou M, Pennell DJ.
The histologic basis of late gadolinium enhance-ment cardiovascular
magnetic resonance in hypertrophic cardiomyop-athy. J Am Coll
Cardiol 2004;43:22602264.
4. Moon JCC, Sachdev B, Elkington AG, McKenna WJ, Mehta
A,Pennell DJ, Leed PJ, Elliott PM. Gadolinium enhanced
cardiovascularmagnetic resonance in Anderson-Fabry disease.
Evidence for a diseasespecic abnormality of the myocardial
interstitium. Eur Heart J 2003;24:21512155.
5. Eng CM, Guffon N, Wilcox WR, Germain DP, Lee P, Waldek
S,Caplan L, Linthorst GE, Desnick RJ, International Collaborative
FabryDisease Study Group. Safety and efcacy of recombinant
humanalpha-galactosidase A-replacement therapy in Fabrys disease. N
Engl
J Med 2001;345:916.6. Schiffmann R, Kopp JB, Austin HA III,
Sabnis S, Moore DF, Weibel
T, Balow JE, Brady RO. Enzyme replacement therapy in Fabry
dis-ease: a randomized controlled trial. JAMA
2001;285:27432749.
7. Weidemann F, Breunig F, Beer M, Sandstede J, Turschner O,
VoelkerW, Ertl G, Knoll A, Wanner C, Strotmann JM. Improvement of
cardiacfunction during enzyme replacement therapy in patients with
Fabry
disease: a prospective strain rate imaging study.
Circulation2003;108:12991301.
8. Desnick RJ, Brady R, Barranger J, Collins AJ, Germain DP,
GoldmanM, Grabowski G, Packman S, Wilcox WR. Fabry disease, an
under-recognized multisystemic disorder: expert recommendations for
diag-nosis, management, and enzyme replacement therapy. Ann Intern
Med 2003;138:338346.
9. Sandstede JJ, Pabst T, Beer M, Lipke C, Baurle K, Butter F,
Harre K,
Kenn W, Voelker W, Neubauer S, Hahn D. Assessment of
myocardialinfarction in humans with (23) Na MR imaging: comparison
with cineMR imaging and delayed contrast enhancement. Radiology
2001;221:222228.
10. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S,
LaskeyWK, Pennell DJ, Rumberger JA, Ryan T, Verani MS, American
HeartAssociation Writing Group on Myocardial Segmentation and
Regis-tration for Cardiac Imaging. Standardized myocardial
segmentationand nomenclature for tomographic imaging of the heart:
a statementfor healthcare professionals from the Cardiac Imaging
Committee of the Council on Clinical Cardiology of the American
Heart Association.Circulation 2002;105:539542.
11. Bogaert J, Goldstein M, Tannouri F, Golzarian J, Dymarkowski
S.Original report. Late myocardial enhancement in hypertrophic
cardio-
myopathy with contrast-enhanced MR imaging. Am J
Roentgenol2003;180:981985.12. McCrohon JA, Moon JC, Prasad SK,
McKenna WJ, Lorenz CH, Coats
AJ, Pennell DJ. Differentiation of heart failure related to
dilated cardio-myopathy and coronary artery disease using
gadolinium-enhanced car-diovascular magnetic resonance. Circulation
2003;108:5459.
13. Teraoka K, Hirano M, Ookubo H, Sasaki K, Katsuyama H, Amino
M,Abe Y, Yamashina A. Delayed contrast enhancement of MRI
inhypertrophic cardiomyopathy. Mag Reson Med 2004;22:155161.
14. Bulow H, Klein C, Kuehn I, Hollweck R, Nekolla SG, Schreiber
K,Haas F, Bhm J, Schnackenburg B, Lange R, Schwaiger M.
Cardiacmagnetic resonance imaging: long term reproducibility of the
lateenhancement signal in patients with chronic coronary artery
disease. Heart 2005;91:11581163.
15. Mahrholdt H, Wagner A, Holly TA, Elliott MD, Bonow RO, Kim
RJ,Judd RM. Reproducibility of chronic infarct size measurement
bycontrast-enhanced magnetic resonance imaging. Circulation
2002;106:23222327.
16. Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O,
KlockeFJ, Bonow RO, Judd RM. The use of contrast-enhanced
magneticresonance imaging to identify reversible myocardial
dysfunction. N Engl J Med 2000;343:14451453.
1518 The American Journal of Cardiology (www.AJConline.org)