Embed Size (px)
Citation preview

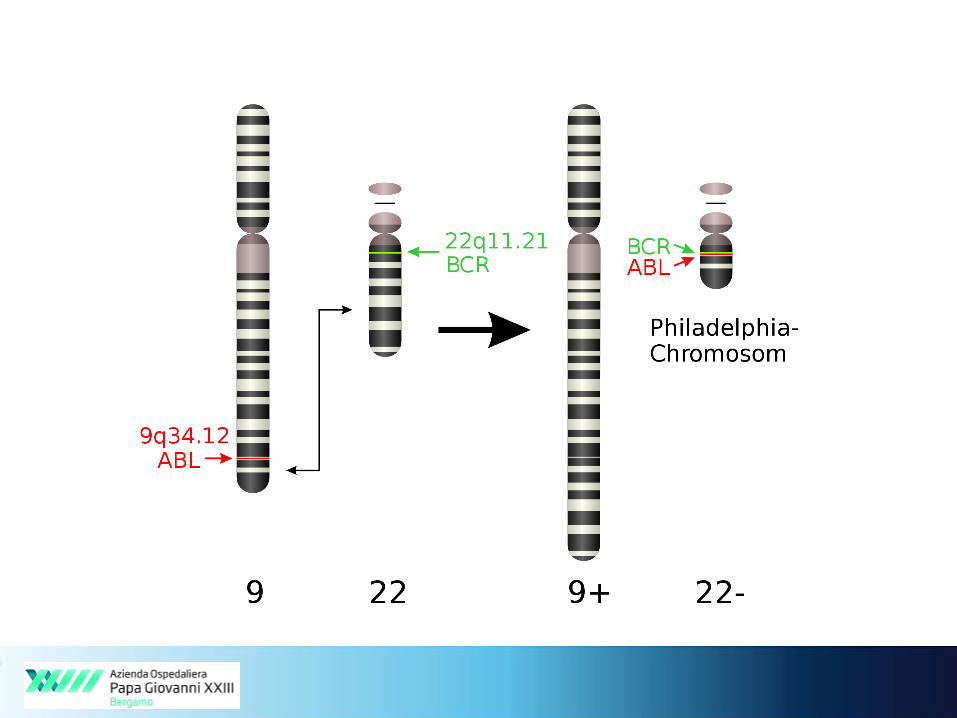
Significato clinico e applicazioni dell’analisi dei minor
BCR-ABL1 breakpoints
Orietta Spinelli
Laboratorio di Ematologia “Paolo Belli”
USC Ematologia
Ospedale Papa Giovanni XXIII
Bergamo
Milano, 13 Novembre 2014
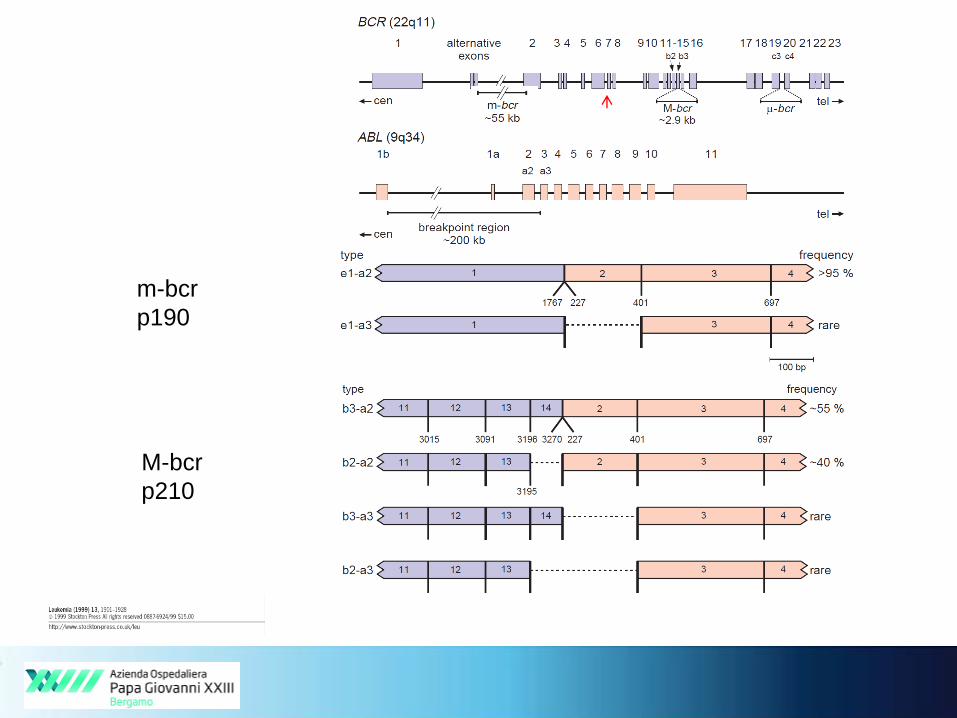
m-bcr
p190
M-bcr
p210

Usefulness of BCR-ABL identification
Diagnostic
Prognostic Therapeutic
pre and post TKI
CML within MPNs
Ph+ ALL within ALL
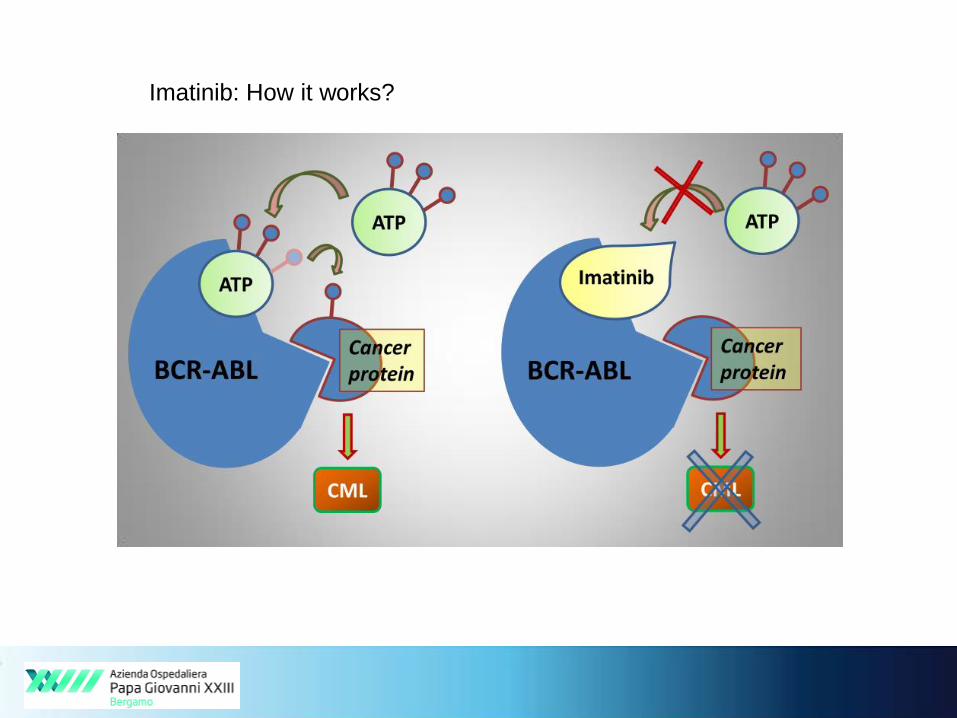
Imatinib: How it works?
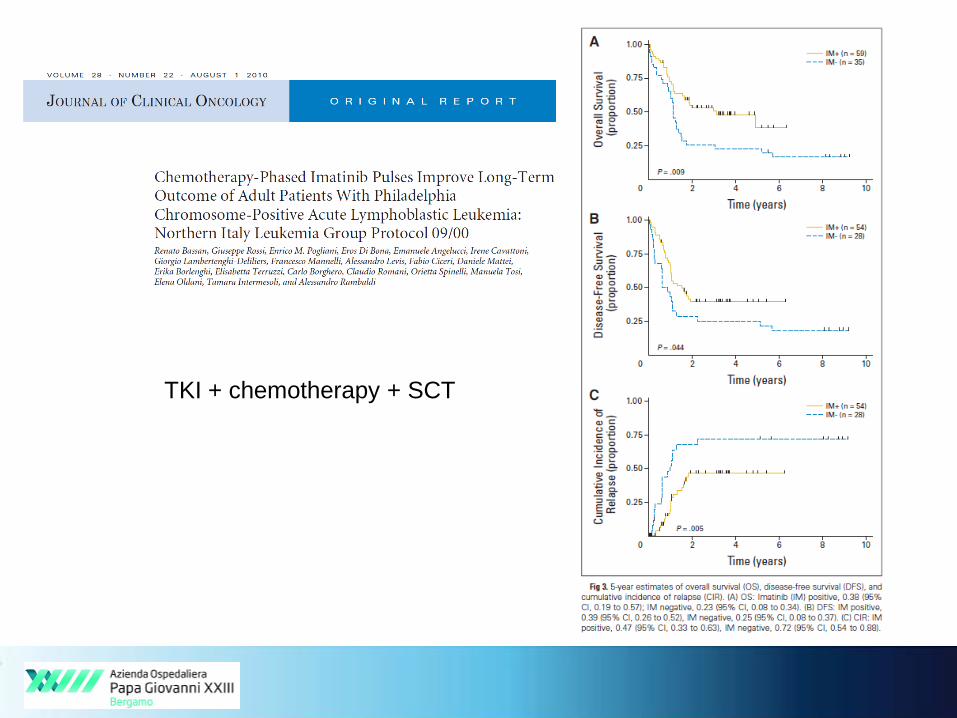
TKI + chemotherapy + SCT
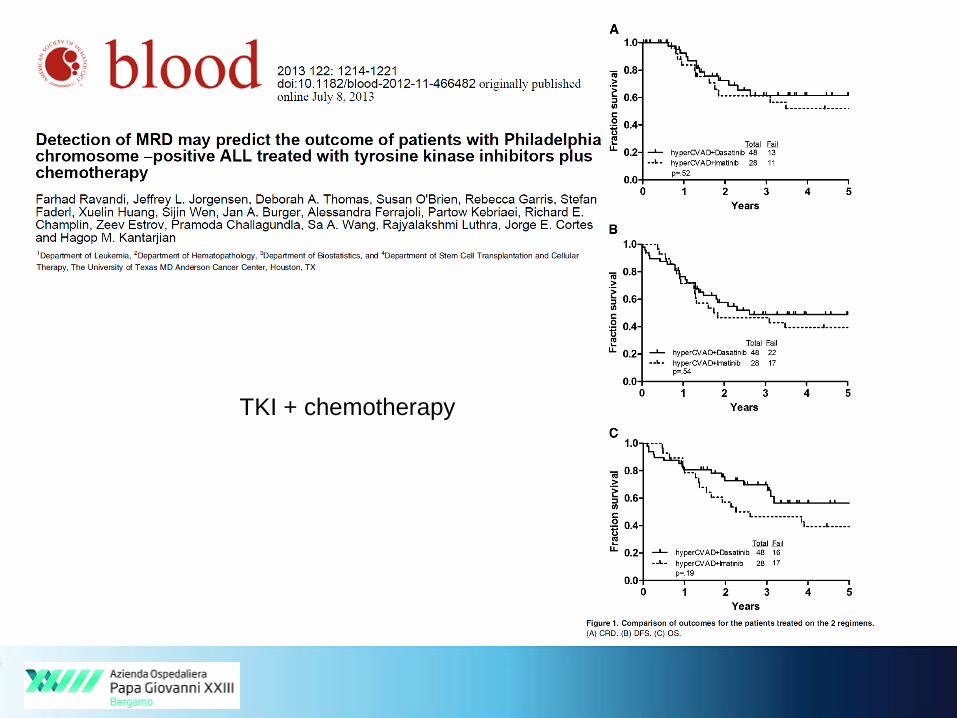
TKI + chemotherapy
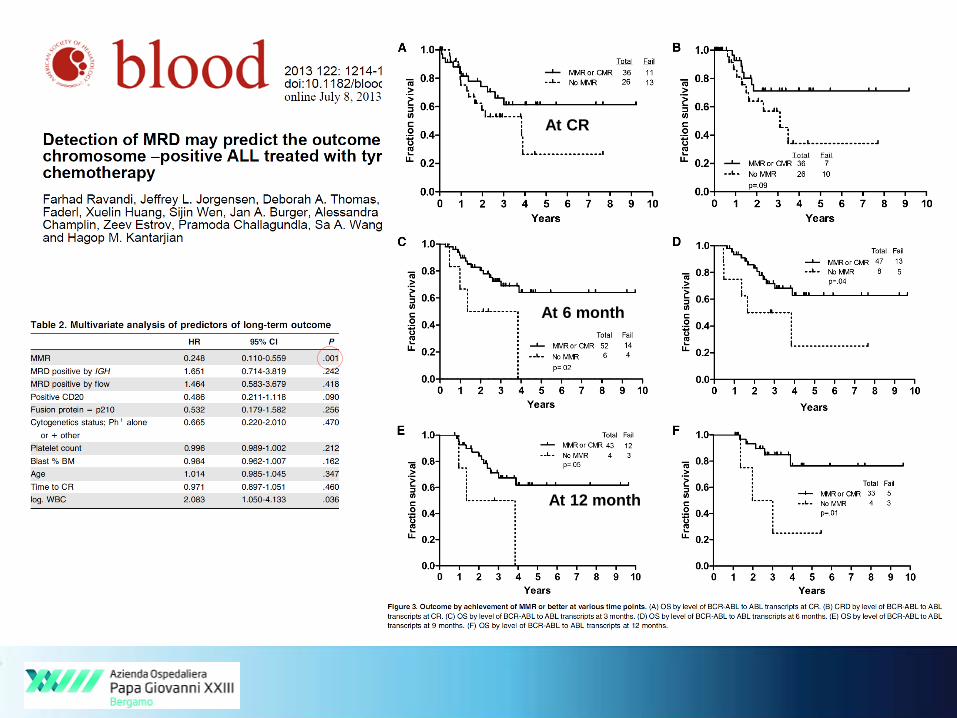
At CR
At 6 month
At 12 month
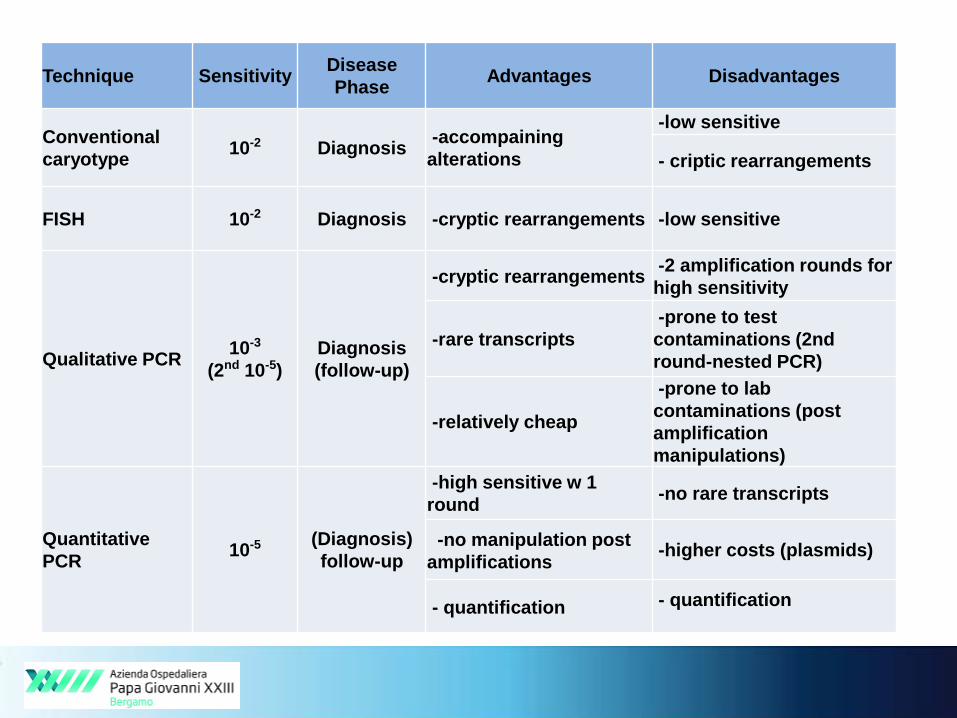
Technique SensitivityDisease
PhaseAdvantages Disadvantages
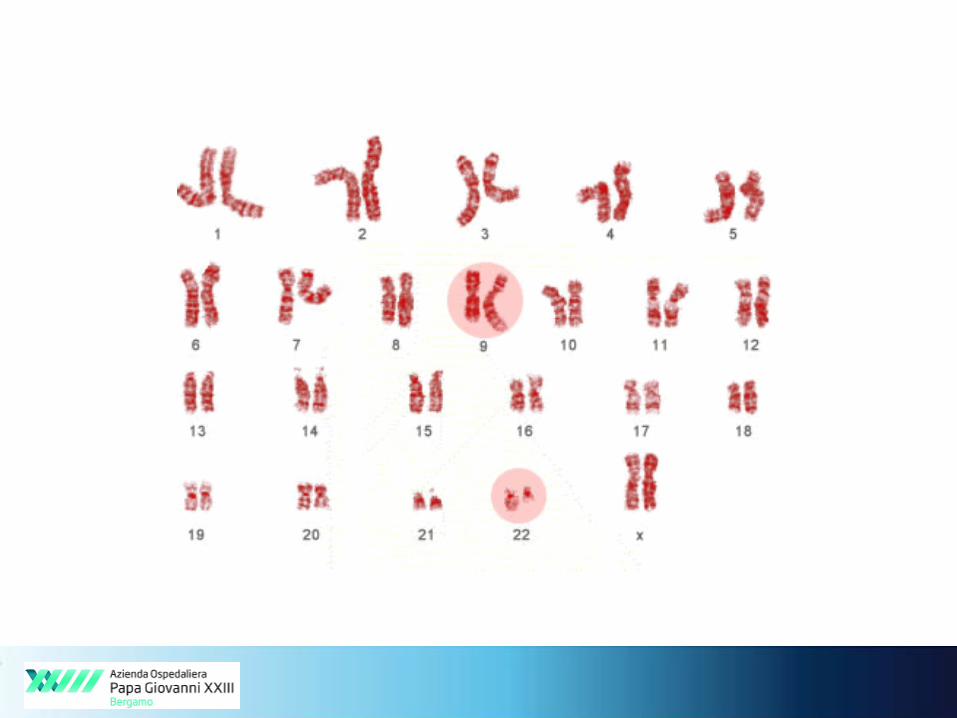
Conventional
caryotype10-2 Diagnosis
-accompaining
alterations
-low sensitive
- criptic rearrangements
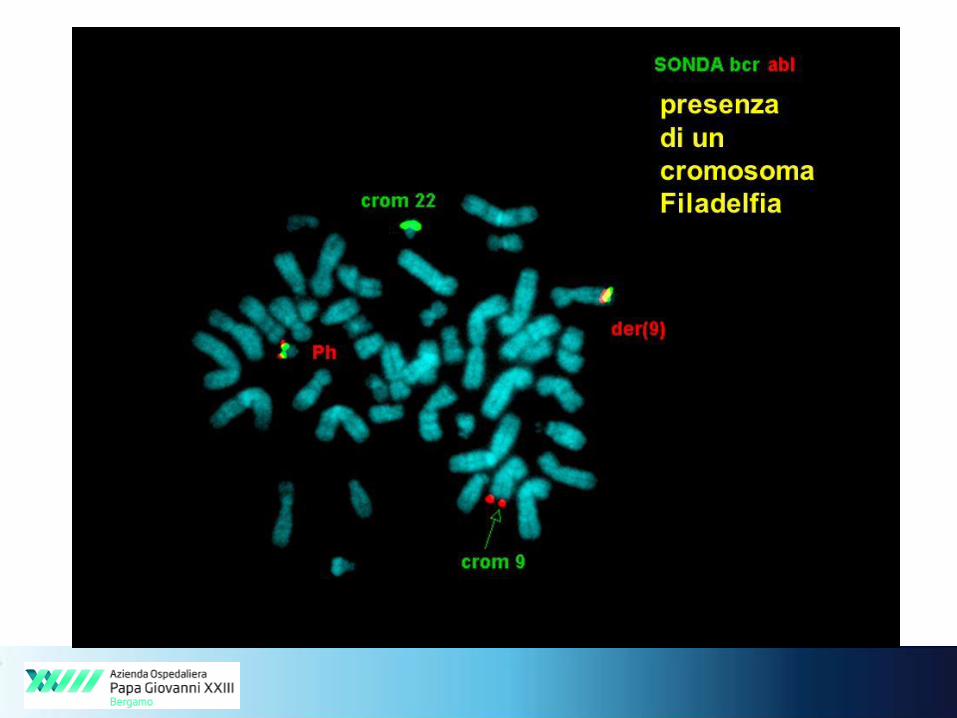
FISH 10-2 Diagnosis -cryptic rearrangements -low sensitive
Qualitative PCR10-3
(2nd 10-5)
Diagnosis
(follow-up)
-cryptic rearrangements-2 amplification rounds for
high sensitivity
-rare transcripts
-prone to test
contaminations (2nd
round-nested PCR)
-relatively cheap
-prone to lab
contaminations (post
amplification
manipulations)
Quantitative
PCR10-5 (Diagnosis)
follow-up
-high sensitive w 1
round-no rare transcripts
-no manipulation post
amplifications-higher costs (plasmids)
- quantification - quantification
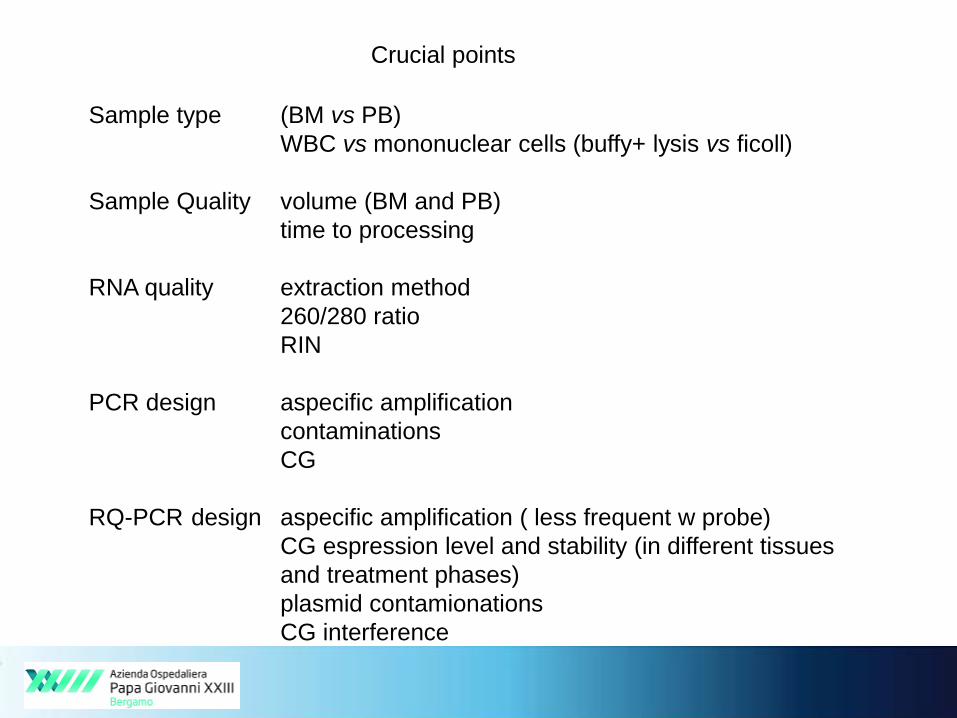
Crucial points
Sample type (BM vs PB)
WBC vs mononuclear cells (buffy+ lysis vs ficoll)
Sample Quality volume (BM and PB)
time to processing
RNA quality extraction method
260/280 ratio
RIN
PCR design aspecific amplification
contaminations
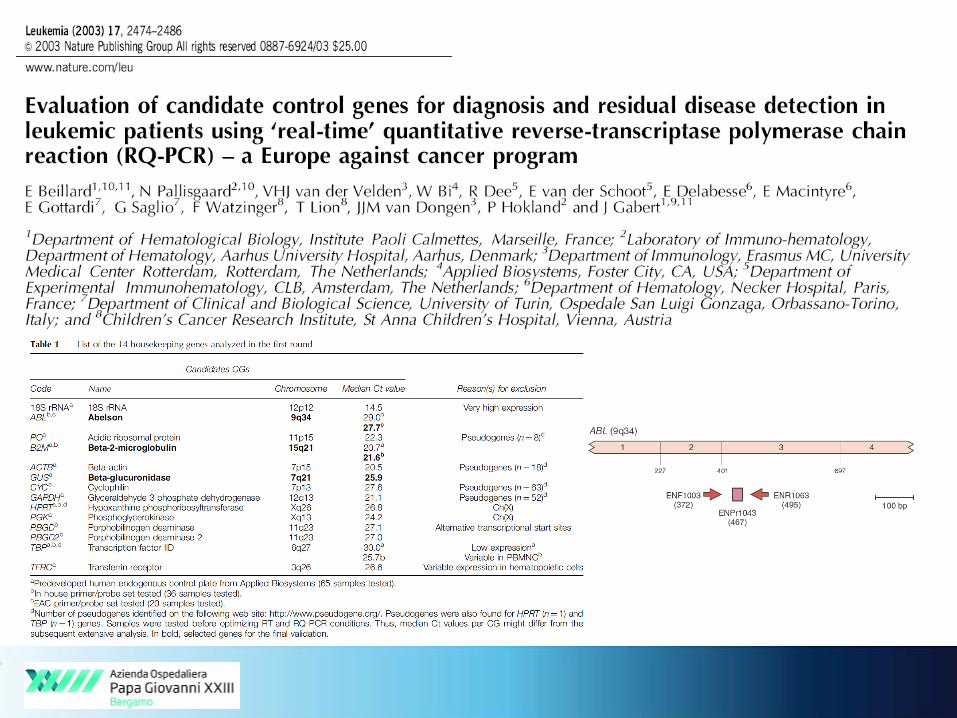
CG
RQ-PCR design aspecific amplification ( less frequent w probe)
CG espression level and stability (in different tissues
and treatment phases)
plasmid contamionations
CG interference

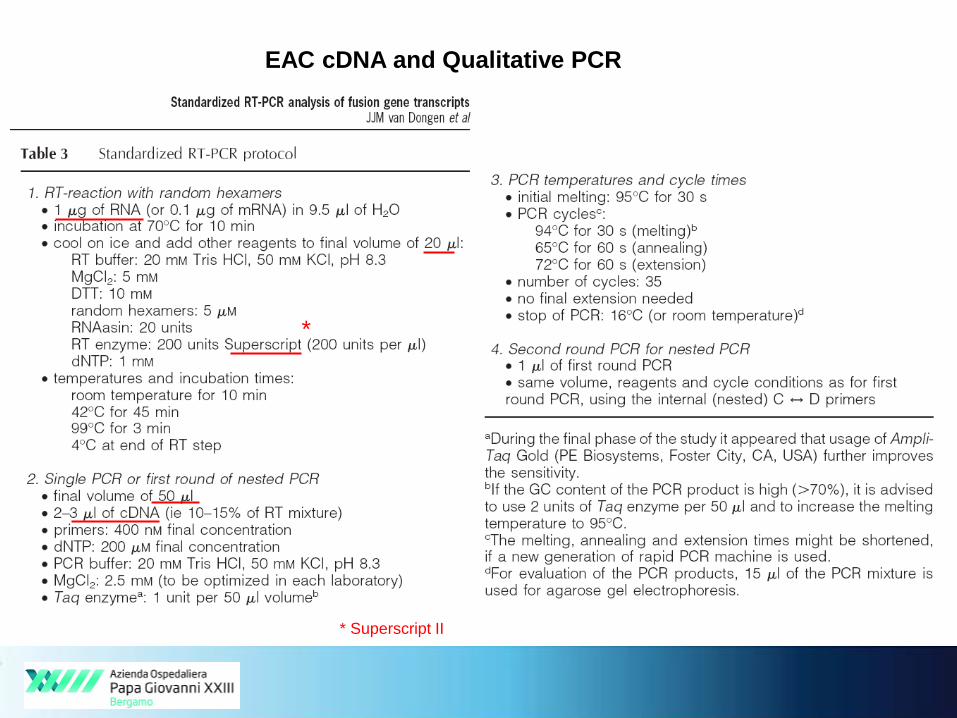
EAC cDNA and Qualitative PCR
*
* Superscript II
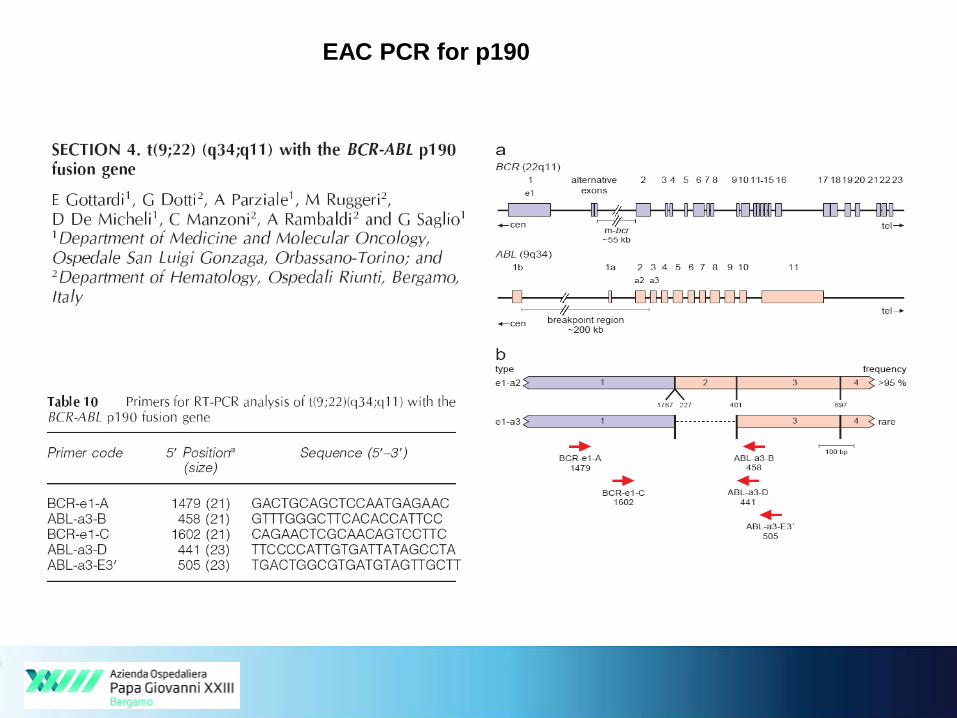
EAC PCR for p190
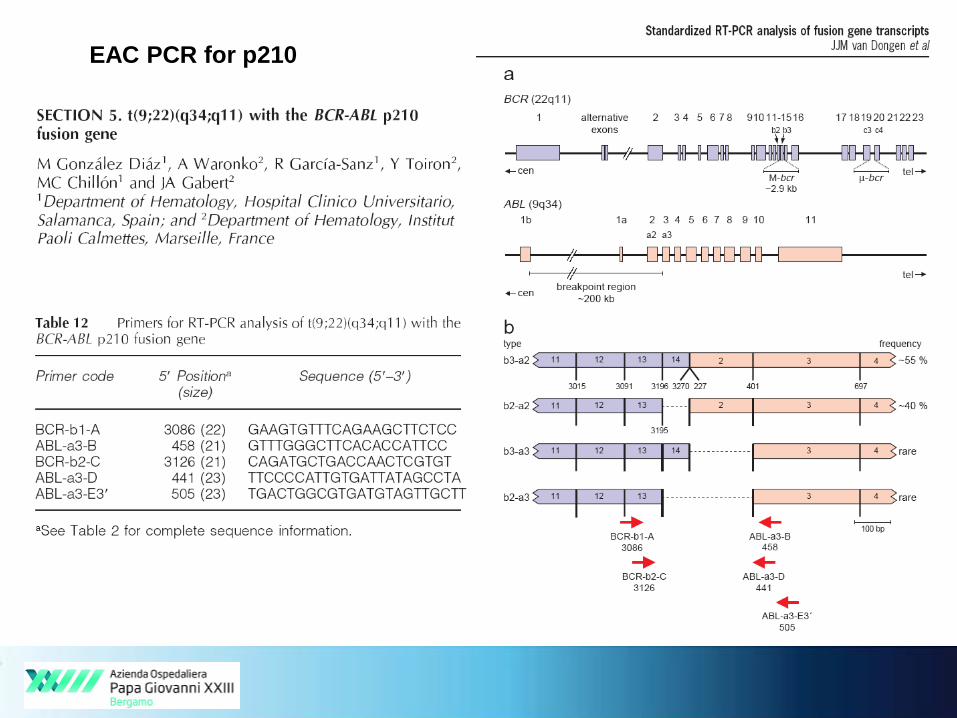
EAC PCR for p210
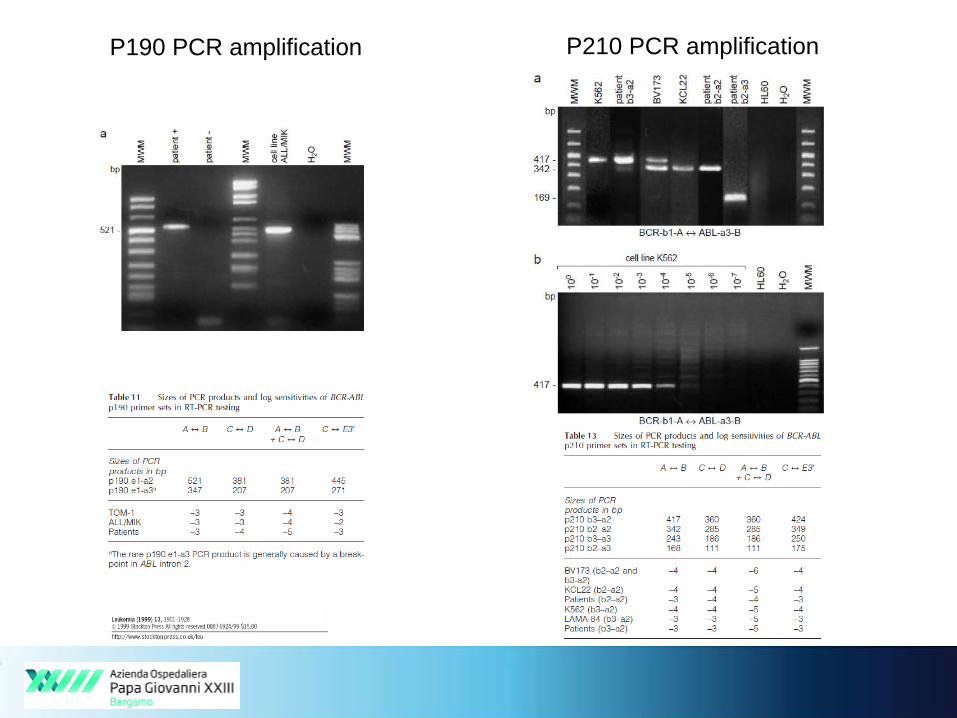
P190 PCR amplification P210 PCR amplification

Quantitative PCR
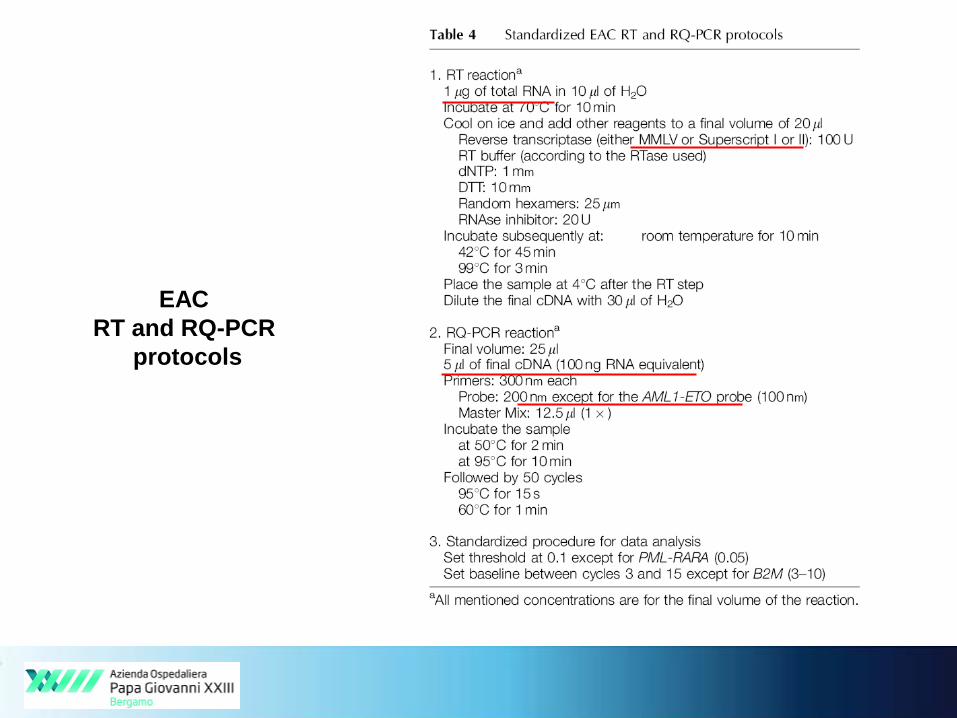
EAC
RT and RQ-PCR
protocols
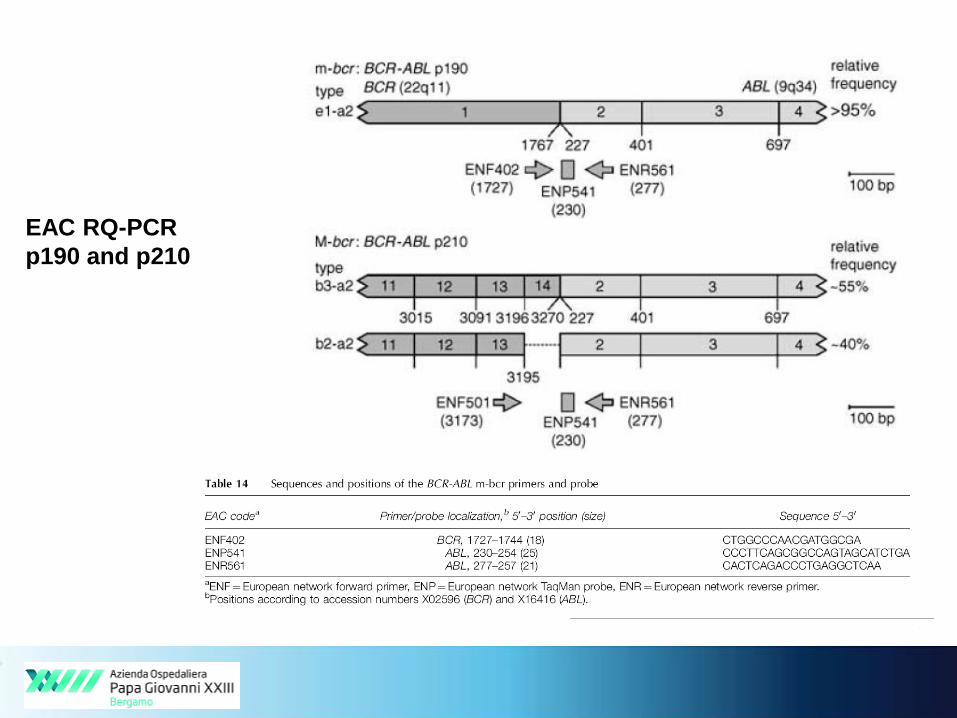
EAC RQ-PCR
p190 and p210
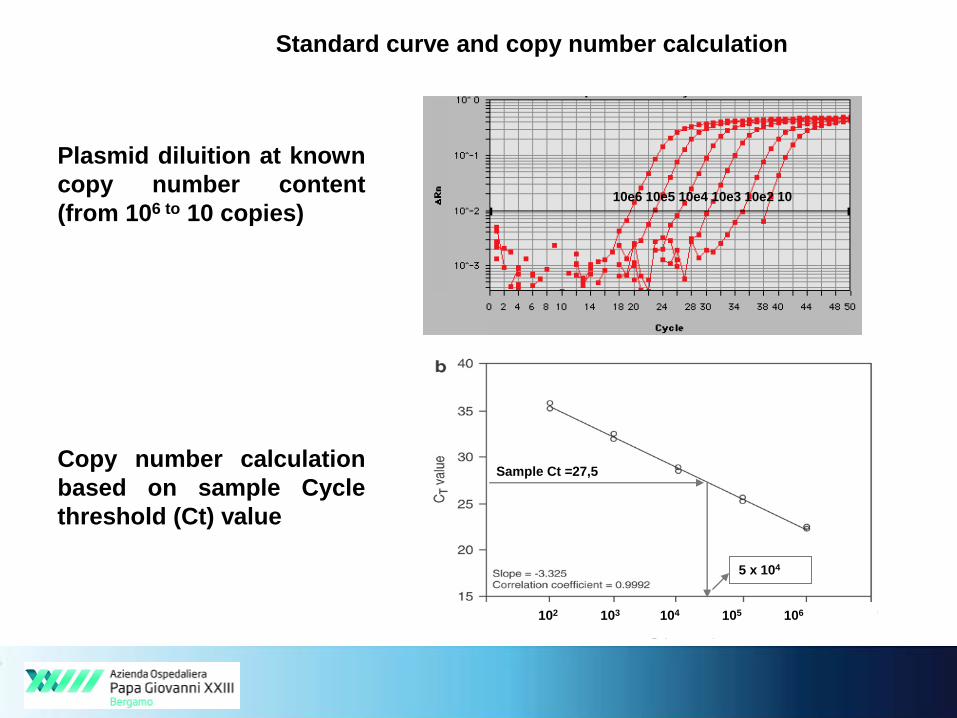
Standard curve and copy number calculation
Plasmid diluition at known
copy number content
(from 106 to 10 copies)
Copy number calculation
based on sample Cycle
threshold (Ct) value
10e6 10e5 10e4 10e3 10e2 10
Sample Ct =27,5
5 x 104
102 103 104 105 106
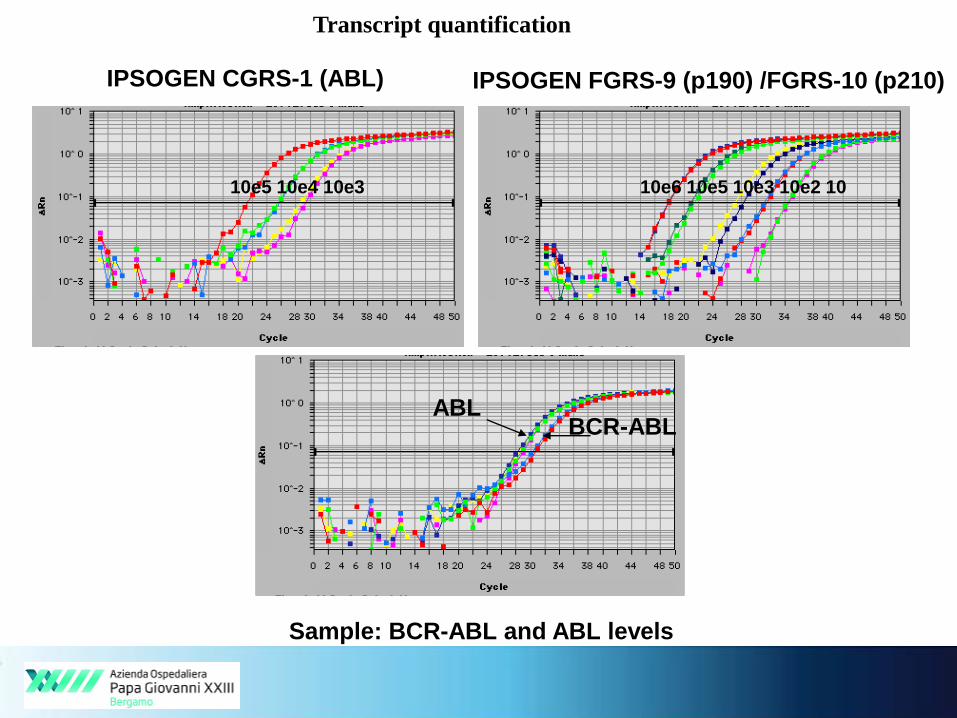
IPSOGEN FGRS-9 (p190) /FGRS-10 (p210)
10e6 10e5 10e3 10e2 10
IPSOGEN CGRS-1 (ABL)
10e5 10e4 10e3
ABLBCR-ABL
Transcript quantification
Sample: BCR-ABL and ABL levels

1- BCR-ABL Normalized Copy Number (NCN BCR-ABL)
NCN BCR-ABL = Target Copy Number x 104
CG Copy NumberAt least 10000 ABL copies
2- BCR-ABL %
BCR-ABL % = Target Copy Number x 100
CG Copy Number
3- BCR-ABL International Scale %
BCR-ABL IS % = Target Copy Number x 100 x CF*
CG Copy Number
*CF Convertion Factor experimentally calculated for Major BCR-ABL1 in
CML based on reference sample/material
Transcript quantification
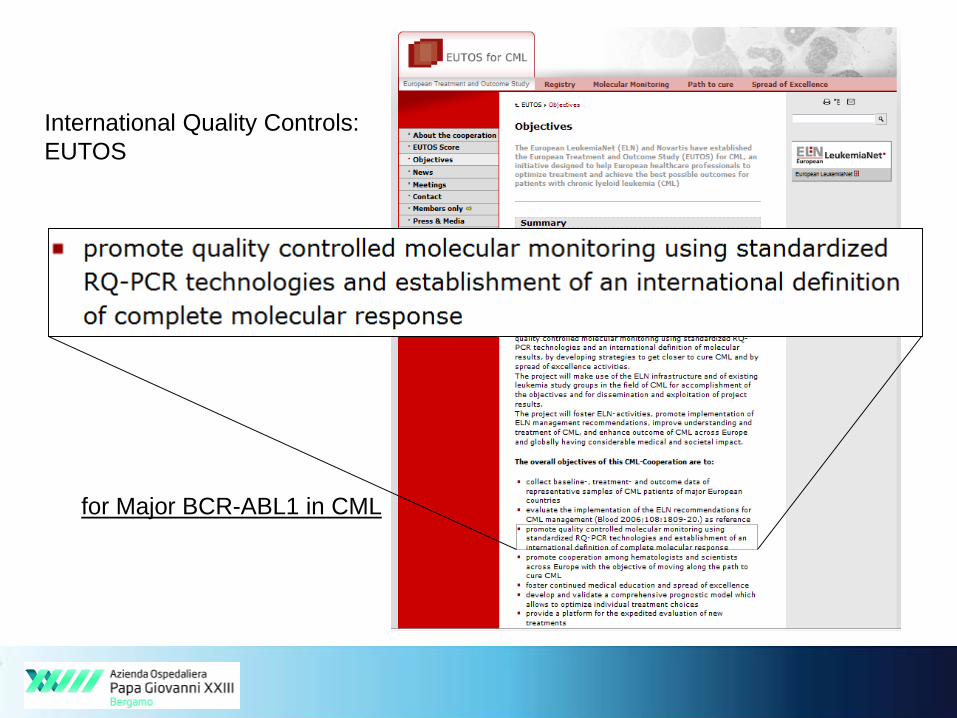
International Quality Controls:
EUTOS
for Major BCR-ABL1 in CML
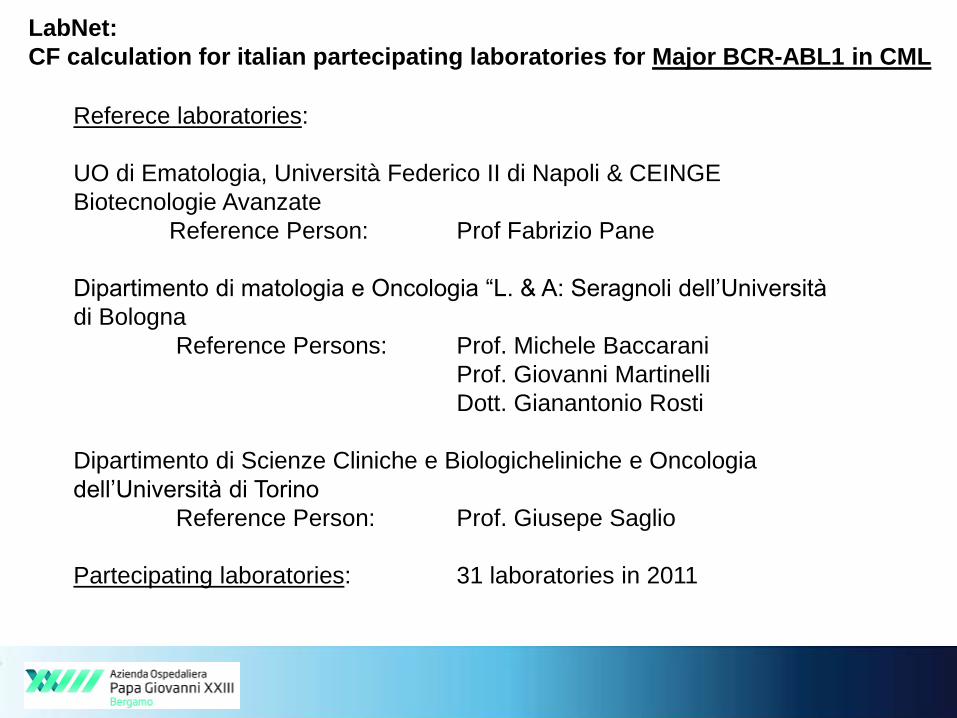
LabNet:
CF calculation for italian partecipating laboratories for Major BCR-ABL1 in CML
Referece laboratories:
UO di Ematologia, Università Federico II di Napoli & CEINGE
Biotecnologie Avanzate
Reference Person: Prof Fabrizio Pane
Dipartimento di matologia e Oncologia “L. & A: Seragnoli dell’Università
di Bologna
Reference Persons: Prof. Michele Baccarani
Prof. Giovanni Martinelli
Dott. Gianantonio Rosti
Dipartimento di Scienze Cliniche e Biologicheliniche e Oncologia
dell’Università di Torino
Reference Person: Prof. Giusepe Saglio
Partecipating laboratories: 31 laboratories in 2011
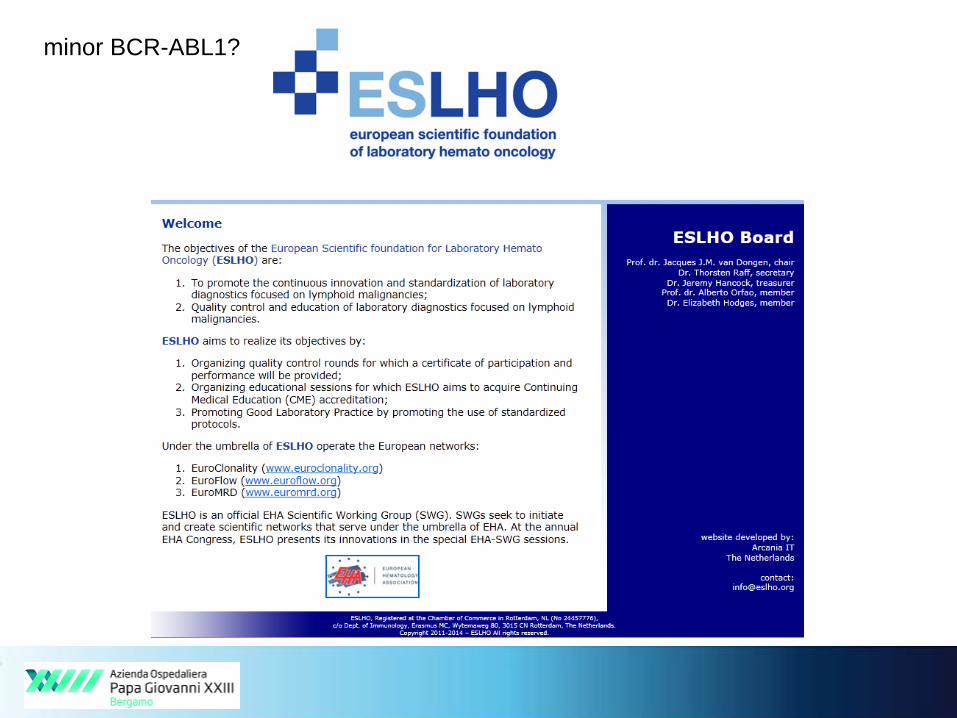
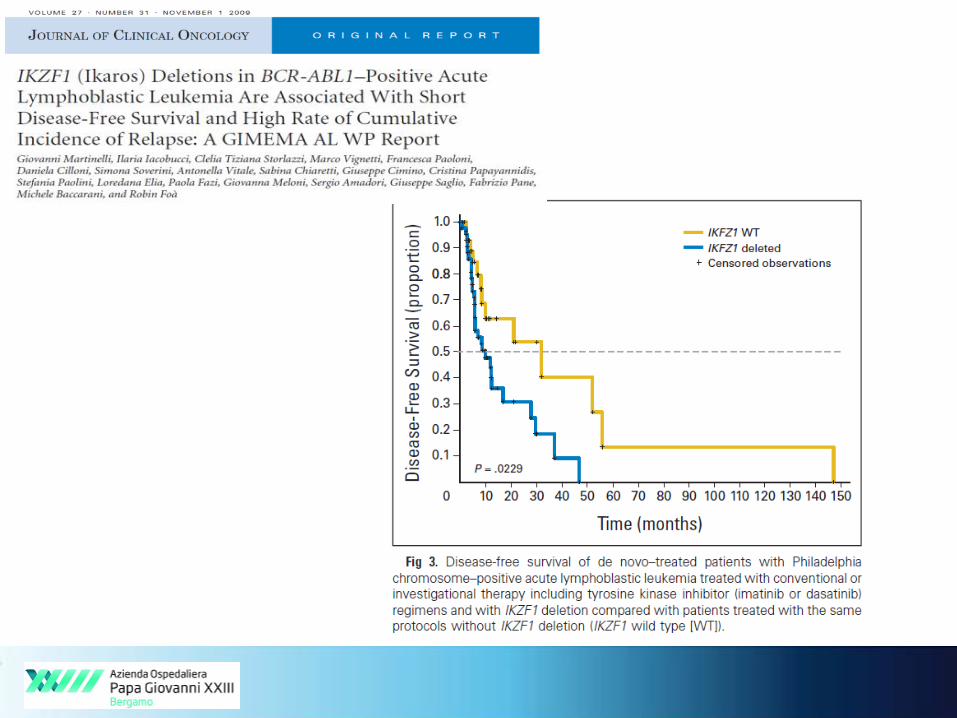
minor BCR-ABL1?
EuroMRD: European Study Group
on MRD detection
AIMS of EuroMRD (focus on PCR ananlysis of Ig/TCR genes):
1. Quality Control Program: 2 times per year: - February / March
- August / September
2. Educational meetings, including evaluation of quality control rounds:
2 times per year: - May / June
- October / November
3. Standardization of MRD techniques
- standardization techniques within each treatment protocol
- guidelines for interpretation of RQ-PCR results
- standardized diagnostics reports
4. Collaborative development and clinical evaluation of new MRD
strategies and new MRD techniquesBasis for accreditation of laboratory diagnostics
and minor-BCR-ABL (Coordinator H. Pfifer, Frankfurt)
CONCLUSIONS
- Identification of t( 9;22) (q34;q11) and BCR-ABL transcripts is
mandatory for diagnostic, prognostic and therapeutic issues in
CML and ALL.
- Qualitative PCR for BCR-ABL identification is preferable at
diagnosis to identify possible transcript variants
- Quantitative PCR is the gold standard for MRD evaluation
- Potential pitfalls in BCR-ABL evaluation are sample quality,
RNA degradation and contaminations
- Quality controls are recommended to ensure accurate and
reliable results





























