Embed Size (px)
Citation preview

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 1
BATES’ VISUAL GUIDE TO PHYSICAL EXAMINATION
Vol. 16: Musculoskeletal System
I’m Dr. Bickley, it’s very nice to meet you, Jason.
Nice to meet you.
Your learning objectives for mastering the examination of the musculoskeletal system are: to
understand the link between anatomy and functional movement for each of the major joints and to
perform the techniques and maneuvers needed for assessing the range of motion, function, and soft
tissues for each of the major joints. It is also important to recognize the changes of inflammatory and
degenerative joint disease and trauma.
Musculoskeletal disorders are the leading cause of medical office visits in the United States. Common or
concerning symptoms relating to the musculoskeletal system include: neck pain; low back pain;
monoarticular or polyarticular joint pain; inflammatory or infectious joint pain; joint pain with systemic
features such as fever, chills, rash, anorexia, weight loss, and weakness; and joint pain with symptoms
from other organ systems.
Some tips for assessing joint pain are:
Always ask the patient to “point to the pain” since not all patients explain pain well.
Clarify when the pain started and especially the mechanism of injury, or exactly how the pain began, for
example, the detail relating to trauma or from a particular exercise or movement.
Identify key features of the pain—is it localized or diffuse, acute or chronic, inflammatory or non‐
inflammatory.
With the patient’s health history in mind, and by eliciting the patient’s concerns before the examination,
you prepare for an examination that is focused, efficient, and productive.
As you examine each joint be sure to…look for joint symmetry, alignment, bony deformities, and
swelling. Assess the surrounding tissues noting skin changes, subcutaneous nodules, and muscle
atrophy. Test range of motion and perform maneuvers to demonstrate limitations. Note any swelling,
warmth, tenderness, or redness.
Anatomy Review—Mandible
Before examining the head and neck, let’s review their anatomy.
In the head, the temporomandibular joint (or TMJ) arises from the articulation between the mandible
and the skull.
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 2
A fibrocartilaginous disc cushions the action of the condyle of the mandible against the synovial
membrane and capsule of the articulating surfaces of the temporal bone.
After comprehensive hand hygiene, you are ready for the physical examination.
Examining the Mandible
Begin the examination by assessing the temporomandibular joint. Place the tips of your fingers in front
of the tragus of each ear. Then ask the patient to open and close his mouth.
Your fingertips should drop into the joint spaces as the mouth opens. Check for a smooth range of
motion. Feel for swelling, and note any tenderness or crepitus.
Palpate the muscles of mastication: the temporal muscles, the pterygoid muscles, and the masseters.
Ask the patient to demonstrate protrusion and retraction by jutting the mandible forward…and lateral
and side‐to‐ side motion.
Anatomy Review—Shoulders
When you assess the shoulders identify the following important landmarks and articulations.
The bony structures of the shoulder include the humerus, the clavicle, and the scapula. Three different
joints articulate the shoulder: the glenohumeral joint, the sternoclavicular joint, and the
acromioclavicular joint.
Three groups of muscles attach at the shoulder. The scapulohumeral group includes the important SITs
muscles or the rotator cuff—suspraspinatus, infraspinatus and teres minor, and subscapularis muscles.
The axioscapular group includes the trapezius, rhomboids, serratus anterior, and levator scapulae
muscles.
The axiohumeral group includes the pectoralis major and minor and the latissimus dorsi muscles.
Examining the Shoulders
Begin by inspecting the shoulder and shoulder girdle anteriorly.
Inspect the scapulae and related muscles posteriorly. During both inspections, note any swelling,
deformity, muscle atrophy, or fine tremors of the muscles.
Palpate for tenderness at the sternoclavicular joint, tracing the clavicle laterally with your fingers.
From behind, follow the bony spine of the scapula laterally and upward until it becomes the acromion,
the summit of the shoulder.
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 3
From there, palpate the acromioclavicular joint, and from there down to the coracoid process of the
scapula.
Palpate the greater tubercle…
…and the biceps tendon in the intertubercular groove, checking for tenderness.
Also lift the humerus posteriorly so you can palpate over the subacromial bursa…
…and subdeltoid bursa and the underlying palpable SITS muscles, which include the supraspinatus,
infraspinatus, teres minor, and subscapularis.
To evaluate the range of motion of the shoulders, ask the patient to perform the six motions of the
shoulder girdle. These include flexion…where the patient raises his arm in front and overhead…
Extension, where he moves his arms behind…
Abduction, raising his arms out to the side and overhead…
Adduction, crossing an arm in front of his body…
Internal rotation, placing a hand behind his back to touch his shoulder blade…
And external rotation, rotating an arm toward the ceiling from shoulder level. If you suspect a problem,
cup your hand over the patient’s shoulders and feel for crepitus as the patient repeats the movements.
Examination of the shoulders often calls for the patient to perform maneuvers to test specific motions
and structures.
This maneuver assesses the acromioclavicular joint and is sometimes called the “crossover test.”
The Apley scratch test, tests overall shoulder rotation.
Assess the rotator cuff, the most common source of shoulder pain. When positive, Neer’s impingement
sign suggests a rotator cuff sprain.
Hawkin’s impingement sign also indicates rotator cuff sprain or tear.
Now for direct testing of the SITs muscles. To assess the supraspinatus, do the “empty can test.”
…and don’t let me push. Any problems? Any pain?
Excellent.
Test for function and pain in the infraspinatus with this maneuver.
Keep your thumbs up and press out against my hands. Okay, any pain?
Now test for forearm supination.
Now I’d like you to turn them around like you’re holding a bowl of soup. Go ahead…and I’m pressing.
Any pain?
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 4
Test the “drop‐arm” sign by asking the patient to fully abduct the arm to shoulder level (that is, to 90
degrees), and then to lower it slowly. When positive these tests suggest rotator cuff sprain, partial tear,
or full tear, depending on the severity of loss of function.
Before examining the elbows, let’s review their basic anatomy. Assessment of the elbow joint includes
examination of the ulna, its olecranon process, the overlying olecranon bursa, and the medial
epicondyle of the humerus.
The bones of the elbow have three articulations: the humeroulnar joint, the radiohumeral joint, and the
radioulnar joint. Note also in this anterior view, the lateral epicondyle of the humerus.
Examining the Elbows
Support the patient’s forearm so that the elbow is flexed to about 70 degrees. Inspect and palpate the
elbow including the medial and lateral epicondyles, the olecranon processes in the groove between the
epicondyles, and the extensor surface of the ulna. Note any nodules or swelling that suggest olecranon
bursitis or arthritis.
Normally you cannot palpate either the synovium or the olecranon bursa.
Note any tenderness or effusion, as well as any displacement of the olecranon or the olecranon process,
particularly if there is a history of trauma.
The sensitive ulnar nerve can be felt posteriorly between the olecranon process and the medial
epicondyle.
Next, assess the range of motion of the patient’s elbows. To test flexion and extension, have the patient
bend and then straighten his elbows.
To check supination and pronation, ask the patient to flex his elbows at 90 degrees and turn his palms
up and then down.
Anatomy Review—Wrists and Hands
Before examining the patient’s wrists and hands, consider these important structures. Bones of the wrist
and hand include the distal radius and ulna, the carpal bones, the metacarpals, and the phalanges. The
joints of the hand include the metacarpophalangeal (MCPs), proximal interphalangeal (PIPs), and distal
interphalangeal (DIPs).
Related joints include the distal radioulnar joint, radiocarpal and intercarpal, and phalangeal joints.
Be familiar with the structures in the carpel tunnel. This channel contains the sheath and flexor tendons
of the forearm muscles and the median nerve. Holding the tendons and tendon sheath in place is the
transverse flexor retinaculum.
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 5
Examining the Wrists and Hands
Observe the position of the hands in motion to see if movements are smooth and natural. When fingers
are relaxed, they should be slightly flexed.
Inspect the patient’s wrists and hands, noting any swelling over the joints as well as any deformities or
angulation. Observe the contours of the palm, namely the thenar and hypothenar eminences. Note any
thickening of the tendons or fingers.
Palpate the distal radius and ulna on the lateral and medial surfaces of the wrist.
Palpate the radial styloid bone and the anatomical snuffbox, a hollowed depression just distal to the
radial styloid process. Pain when palpating the snuffbox suggests a scaphoid fracture.
Palpate over the eight carpal bones lying distal to the wrist joint, and then each metacarpophalangeal
joint.
Compress the MCP joints by squeezing the hand from each side between the thumb and fingers. Note
any tenderness, swelling, or bogginess.
Now palpate the medial and lateral aspects of each of the proximal interphalangeal joints between the
thumb and index finger noting any swelling, bogginess, bony enlargement, or tenderness. Bony nodules
at the PIP joints, or Bouchard’s nodes, are common in osteoarthritis. They are benign.
Using the same techniques, examine the DIP joints. Benign bony nodules at the DIP joints, or Heberden’s
nodes, are also common in osteoarthritis. Repeat on the other hand.
To check range of motion of the wrists and hands, begin with flexion and extension.
So turn your hands palms up. And then just bring the fingers up toward your face. Good. Palms flat…
Okay.
…and down towards your toes.
Continue to assess range of wrist movement with adduction and abduction.
With your palm down, bring your wrist into flat position and turn it away…and towards you. Very good.
If there complaints of wrist pain suggesting carpal tunnel syndrome, test sensation by assessing the
median nerve in the pulp of the index finger, the ulnar nerve in the pulp of the fifth finger, and the radial
nerve in the dorsal web space of the thumb and index finger.
Other tests include hand grip strength.
We’re going to check the strength of your fingers…your hand grip. Squeeze as hard as you can. Okay,
very good.
Loss of grip strength is seen in de Quervain’s tenosynovitis or inflammation of the thumb extensor
tendon, arthritis, and cervical radiculopathy.
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 6
Let’s check out your wrist pain. Grab your thumb in your palm…and squeeze hard…turn in this way a
little bit.
Make note of any wrist pain with extension of the wrist toward the midline in ulnar deviation, or a
positive Finkelstein’s test for de Quervain’s tenosynovitis.
Any problems?
No.
Let’s check your thumb…
Perform tests for carpal tunnel syndrome, first using thumb abduction.
So I want you to just lift your thumb out like that…and go ahead. Any problems there?
No.
Now Tinel’s sign for median nerve compression.
Any pain in your second, third, or fourth fingers?
No.
Or tingling?
No.
What I’d like you to do is put the backs of your two hands together.
And Phalen’s sign for median nerve compression.
If there’s a problem you should again feel tingling in your second, third, and fourth fingers. Any
problem?
No.
Anatomy Review—Spine
The vertebral column, or spine, is the central supporting structure of the trunk and back. The vertebral
column contains 24 vertebrae stacked on the sacrum and coccyx.
Each vertebra contains a spinous process which projects posteriorly in the midline. Transverse processes
are at the junction of the pedicle and the lamina.
The articular processes, two on each side of the vertebra, are often called articular facets. Note the
intervertebral foramen, formed by the inferior and superior articulating process of adjacent vertebrae.
Between the vertebral bodies are the intervertebral discs, which cushion movement and allow the
vertebral column to curve, flex, and bend.
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018
Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 7
Also note the vertebral foramen, which encloses the spinal cord.
The trapezius and the latissimus dorsi form the large outer layer of muscles attaching to each side of the
spine. They overlie two deeper muscle layers—a layer attaching to the head, neck, and spinous
processes, and a layer of smaller intrinsic muscles between vertebrae.
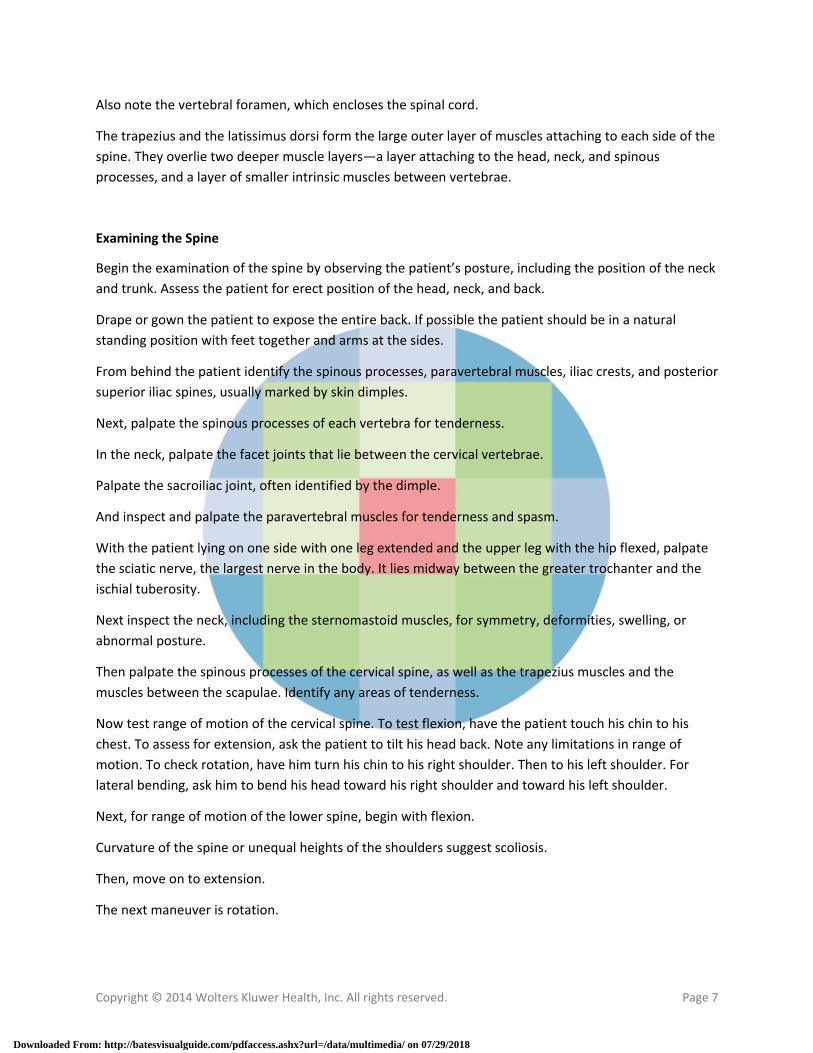
Examining the Spine
Begin the examination of the spine by observing the patient’s posture, including the position of the neck
and trunk. Assess the patient for erect position of the head, neck, and back.
Drape or gown the patient to expose the entire back. If possible the patient should be in a natural
standing position with feet together and arms at the sides.
From behind the patient identify the spinous processes, paravertebral muscles, iliac crests, and posterior
superior iliac spines, usually marked by skin dimples.
Next, palpate the spinous processes of each vertebra for tenderness.
In the neck, palpate the facet joints that lie between the cervical vertebrae.
Palpate the sacroiliac joint, often identified by the dimple.
And inspect and palpate the paravertebral muscles for tenderness and spasm.
With the patient lying on one side with one leg extended and the upper leg with the hip flexed, palpate
the sciatic nerve, the largest nerve in the body. It lies midway between the greater trochanter and the
ischial tuberosity.
Next inspect the neck, including the sternomastoid muscles, for symmetry, deformities, swelling, or
abnormal posture.
Then palpate the spinous processes of the cervical spine, as well as the trapezius muscles and the
muscles between the scapulae. Identify any areas of tenderness.
Now test range of motion of the cervical spine. To test flexion, have the patient touch his chin to his
chest. To assess for extension, ask the patient to tilt his head back. Note any limitations in range of
motion. To check rotation, have him turn his chin to his right shoulder. Then to his left shoulder. For
lateral bending, ask him to bend his head toward his right shoulder and toward his left shoulder.
Next, for range of motion of the lower spine, begin with flexion.
Curvature of the spine or unequal heights of the shoulders suggest scoliosis.
Then, move on to extension.
The next maneuver is rotation.
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 8
To assess lateral bending, have the patient bend to his right…and then to his left. Pain or tenderness
with these maneuvers warrants additional neurologic testing.
Anatomy Review—Hips
To prepare for examination of the hips, let’s review the pertinent anatomy. The hip joint lies deep to the
inguinal ligament. Because of its overlying muscles and location deep in the pelvis, the hip joint is not
readily palpable. On the anterior aspect of the hip, you can identify the iliac crest, the iliac tubercle, the
anterior superior iliac spine, the greater trochanter, and the pubic tubercle.
On the posterior aspect of the hip, note the posterior superior iliac spine, the greater trochanter, the
ischial tuberosity, and the sacroiliac joint.
Four powerful muscle groups move the hips: the flexor group, which lies anteriorly and flexes the thigh,
primarily the iliopsoas; the extensor group, primarily the gluteus maximus; the adductor group, which
swings the thigh toward the body; and the abductor group, which moves the thigh away from the body.
Examining the Hips
Inspection of the hip begins with careful observation of the two phases of the patient’s gait: stance,
when the foot is on the ground and bears weight,…
…and swing, when the foot moves forward and does not bear weight.
Normal gait has a smooth continuous rhythm. Most hip problems appear during the weight‐bearing
stance phase.
Palpate the bony landmarks, including the iliac crest at the upper margin of the pelvis at the level of L4.
From there you can follow the downward anterior curve to locate the iliac tubercle, marking the widest
point of the crest.
Tracking downward you’ll find the anterior superior iliac spine. Place your thumbs there and move your
fingers downward to find the greater trochanter of the femur. Move your thumbs medially and
obliquely to the pubic tubercle.
On the posterior aspect of the hip, palpate the posterior superior iliac spine directly underneath the
visible dimples just above the buttocks.
Next locate the greater trochanter at the level of the gluteal fold. And place your thumb medially on the
ischial tuberosity. The sacroiliac joint is not always palpable, but may be tender.
Note that an imaginary line between the posterior superior iliac spines crosses the sacroiliac joint at S2.
Then, palpate along the inguinal ligament. Here the femoral nerve, artery, and vein bisect the overlying
inguinal ligament while the lymph nodes lie medially. The mnemonic NAVEL may help you remember
the lateral to medial sequence of Nerve‐Artery‐Vein‐Empty space‐Lymph node.
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 9
If the hip is painful, with the patient lying on the side and the upper hip flexed, palpate the trochanteric
bursa, lying over the greater trochanter…
…and the ischiogluteal bursa over the ischial tuberosity, which is not palpable unless inflamed.
Now assess the mobility of the patient’s hips. First, check flexion. With the patient supine, place your
hand under the patient’s lumbar spine. Ask the patient to bend a knee up to the chest and firmly against
the abdomen. Note when the back touches your hand, indicating normal flattening of the lumbar
lordosis. Further flexion must arise from the hip joint itself.
Observe the degree of flexion at the hip and knee. Normally, the anterior portion of the thigh can almost
touch the chest wall. Note whether the opposite thigh remains fully extended, resting on the table. If
the opposite thigh flexes, there may be a flexion deformity of the hip.
Next, check extension. Have the patient hyper‐extend the thigh in a posterior direction.
Check abduction next. Stabilize the pelvis by pressing down on the opposite anterior superior iliac spine
with one hand. With the other hand, grasp the ankle and abduct the extended leg until you feel the iliac
spine move. This movement marks the limit of hip abduction.
Next, check adduction. With one hand on the patient’s opposite hip, hold one ankle, and move the leg
medially across the body and over the opposite extremity.
Test internal and external rotation of the hip; when this helpful test is normal, hip arthritis is less likely.
Flex the leg to 90 degrees at the knee. Then, stabilize the thigh with one hand and grasp the ankle with
the other.
Now swing the lower leg medially for external rotation at the hip…
…and laterally for internal rotation. Repeat each of these maneuvers on the opposite side.
Anatomy Review—Knees
To accurately assess the knee, the largest joint in the body, you must thoroughly understand the
important features of the anatomy of the knee joint. On the medial surface note the adductor tubercle,
the medial epicondyle of the femur, and the medial condyle of the tibia. On the lateral surface, note the
lateral epicondyle of the femur, the lateral condyle of the tibia, and the head of the fibula.
Seven key structures determine knee function. Four ligaments help stabilize the knee: the medial
collateral ligament (MCL), the lateral collateral ligament (LCL), the anterior cruciate ligament (ACL), and
the posterior cruciate ligament (PCL). The medial and lateral menisci cushion knee compression.
Note also the patellar tendon, necessary for lower leg extension.
On the anterior surface, note the patella, which rests on the surface of the femur midway between the
epicondyles, embedded in the tendon of the quadriceps muscle. This tendon continues as the patellar
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 10
tendon, which inserts distally on the tibial tuberosity. On the upper surface of the tibia lie the medial
meniscus and the lateral meniscus. The menisci cushion some of the stress on this weight bearing joint.
The powerful muscle groups that support the knee include the quadriceps femoris, which extends the
knee,…
…and the hamstring muscles, which flex the knee.
Examining the Knees
With the patient supine on the examining table and with his knees in flexion, inspect the knees, noting
their alignment and any deformities.
Note loss of the normal hollows around the patella or atrophy of the quadriceps muscles. Then,
straighten the patient’s leg and palpate the suprapatellar pouch on each side of the quadriceps, noting
any swelling.
Palpate the tibiofemoral joint, the edge of the tibial plateau, and the margins of the joint. Note any
irregular bony ridges.
Palpate the medial meniscus. Then palpate the lateral meniscus. Tenderness suggests a partial tear.
With the knee flexed 90 degrees, assess the medial joint compartments for any tenderness.
Palpate the medial femoral condyle, the adductor tubercle and the medial tibial plateau. Also palpate
and identify the medial collateral ligament.
Assess the lateral joint compartment and palpate the lateral femoral condyle, the lateral tibial plateau
and the lateral collateral ligament.
Assess the range of motion of each knee beginning with flexion... and extension. Be sure to provide
support as needed.
Check internal and external rotation of the knee. Instruct the sitting patient to swing the lower leg
toward the midline ... and away from the midline.
You have already palpated the menisci for tenderness, two of the seven major structures of the knee
joint. To test the medial collateral ligament (or MCL), perform the abduction or valgus stress test, where
you move the thigh about 30 degrees laterally to the side of the examination table, push medially
against the knee, and pull laterally at the ankle to open the knee joint on the medial side. Injuries from
trauma or sports to both the medial meniscus and the MCL are common.
To test the lateral collateral ligament (or LCL), perform the adduction or varus stress test, where you
push laterally against the knee and pull medially at the ankle to open the knee joint on the lateral side.
To test the anterior cruciate ligament (or ACL), check for the anterior drawer sign, where you draw the
tibia forward and observe if it slides forward (like a drawer) from under the femur.
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 11
To test the posterior cruciate ligament (or PCL), check for the posterior drawer sign, where you push the
tibia posteriorly and observe the degree of backward movement in the femur.
Now ask the patient to extend the leg to check the integrity of the patellar tendon.
Anatomy Review—Ankles and Feet
Before examining the patient’s ankles and feet, let’s review the anatomic structures that are important
to your assessment. The ankle is the hinge joint formed by the tibia, the fibula, and the talus. The
principal joints are the tibiotalar joint and the subtalar joint. The medial malleolus is the bony
prominence at the distal end of the tibia, and the lateral malleolus at the distal end of the fibula. The
heel bone is called the calcaneus. Note the strong Achilles tendon. Ligaments include the deltoid
ligament, fanning out from the medial malleolus,…
…the anterior and posterior talofibular ligaments, and the calcaneofibular ligament.
Examining the Ankles and Feet
With the patient supine, inspect the patient’s ankles and feet. Note any deformities, nodules, swelling,
corns, or calluses.
With your thumbs, palpate the anterior aspect of each ankle joint noting any bogginess, swelling, or
tenderness. Feel along the Achilles tendon for nodules and tenderness.
Palpate the heel, especially the posterior and inferior calcaneus for tenderness. Palpate the planter
fascia as well.
Palpate over the medial and lateral malleolus, especially in cases of trauma.
Compress the forefoot and the metatarsophalangeal joints for tenderness.
Palpate the heads of the five metatarsals…and the grooves between them.
To assess the range‐of‐motion of the ankle, begin with ankle (or plantar) flexion…
…and ankle extension or dorsiflexion.
Evaluate inversion of the ankle…
…and eversion of the ankle.
Stabilize the heel and invert and evert the forefoot.
Finally, move the proximal phalanx of each toe up and down. There should be no limitation of
movement or pain.
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Page 12
Recording Your Findings
A clear, well‐organized clinical record—employing language that is neutral, professional, and succinct—
is one of the most important adjuncts to patient care.
[TYPING] Full range of motion in all joints. Hands with no degenerative changes of Heberden's nodes in
the DIPs. Proximal interphalangeal joints are normal. No pain with flexion, extension, or rotation of the
hips.
After practice and further review of this video, make sure you have mastered the important learning
objectives for examining the patient’s musculoskeletal system.
Downloaded From: http://batesvisualguide.com/pdfaccess.ashx?url=/data/multimedia/ on 07/29/2018




















![Jon Bates & Tim Tompkins - Utilizare Visual C++ 6 [RO]](https://img.dokumen.tips/doc/110x75/55cf8df9550346703b8d39c6/jon-bates-tim-tompkins-utilizare-visual-c-6-ro.jpg)