Embed Size (px)
Citation preview

Basics of Continuous Basics of Continuous Subcutaneous Insulin Subcutaneous Insulin
Infusion TherapyInfusion TherapyThomas Repas D.O.Thomas Repas D.O.
Diabetes, Endocrinology and Nutrition Center, Affinity Medical Group, Neenah, WisconsinDiabetes, Endocrinology and Nutrition Center, Affinity Medical Group, Neenah, WisconsinMember, Inpatient Diabetes Management Committee, St. Elizabeth’s Hospital, Appleton, WIMember, Inpatient Diabetes Management Committee, St. Elizabeth’s Hospital, Appleton, WIMember, Diabetes Advisory Group, Wisconsin Diabetes Prevention and Control Program Member, Diabetes Advisory Group, Wisconsin Diabetes Prevention and Control Program
Website: www.endocrinology-online.comWebsite: www.endocrinology-online.com

Overview
• History of insulin pumps• Benefits of improved glycemic control• Advantages of insulin pump therapy• Indications for pump therapy• Beginning insulin pump therapy (basal and bolus dosing)• Carbohydrate Counting• Hypoglycemia and hyperglycemia prevention• Conclusions

History of PumpsHistory of Pumps

Best and BantingBest and Banting

Evolution of Diabetes Management Evolution of Diabetes Management TechnologiesTechnologies
Discovery of Insulin
Urine Test Strips
Glucose Sensors
ArtificialPancreas
1999197819211900s 1977
Urine Tasting
1776
BG Meters
Insulin Pump Therapy

First Insulin PumpFirst Insulin Pump (early 1970s)(early 1970s)

Early Insulin Pumps

AutoSyringe AS*6cAutoSyringe AS*6c1979-19801979-1980

Lilly Betatron 1983Lilly Betatron 1983

Present Day Insulin PumpsPresent Day Insulin Pumps

6,600 8,700 11,40015,000
20,00026,500
35,00043,000
60,000
81,000
120,000
157,000
200,000
0
50,000
100,000
150,000
'90 '91 '92 '93 '94 '95 '96 '97 '98 '99 2000 2001 2002
U.S. Pump UsageTotal Patients Using Insulin Pumps

60%
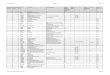
How Diabetes Specialists Treat How Diabetes Specialists Treat Their Own Type 1 DiabetesTheir Own Type 1 Diabetes
AADE Membershipn=229
•Industry estimates at time of survey (9/98); •Graff: Diabetes Educator 2000; 46:460-467
6%General Type 1General Type 1PopulationPopulation**
52%
Injections
Pump Therapy
Color Key:
n=293ADA Membership

Benefits of Improved Benefits of Improved Glycemic ControlGlycemic Control

Potential ChronicPotential ChronicComplications of Elevated HbA1cComplications of Elevated HbA1c
CONTROLCONTROL
• Foot UlcersFoot Ulcers• AnginaAngina• Heart AttackHeart Attack• Coronary BypassCoronary Bypass SurgerySurgery• StrokeStroke• BlindnessBlindness• AmputationAmputation• DialysisDialysis• Kidney Kidney TransplantTransplant
• MicroalbuminuriaMicroalbuminuria• Mild RetinopathyMild Retinopathy• Mild NeuropathyMild Neuropathy
• AlbuminuriaAlbuminuria• Macular EdemaMacular Edema• ProliferativeProliferative RetinopathyRetinopathy• Peridontal DiseasePeridontal Disease• ImpotenceImpotence• GastroparesisGastroparesis• DepressionDepression
RIS
KR
ISK
GoodGood PoorPoor

DCCTDCCT
Microvascular Risk Reduction With Microvascular Risk Reduction With Intensive TreatmentIntensive Treatment
Data from the Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329:977-986.
Reduction inReduction inComplicationComplication Relative RiskRelative Risk
RetinopathyRetinopathy 63%63%
NephropathyNephropathy 54%54%
NeuropathyNeuropathy 60%60%

Additional Benefits of Improving Glycemic Control
• Decreased macrovascular changes– Insulin is NOT atherogenic
• Improved wound healing• Decreased infections• Improved post infarct survival• Minimization of oxidative damage

Treatment Strategies for Diabetes:Treatment Strategies for Diabetes:Are Patients Achieving Good Control?Are Patients Achieving Good Control?
Controlled
Uncontrolled
Hypertension Hyperlipidemia Glycemic control
59%
41%
Harris MI et al. Diabetes Care. 2000;23:754
BP <140/90 mm Hg LDL-C <130 mg/dL A1C <7.0
59%
41%
58%
42%

A1C’s in Clinical PracticeA1C’s in Clinical Practice
~30% of type 2 insulin users have A1C <8% Harmel et al.
7.0
8.0
9.5
A1C (%)
6.0
7.5
8.5
10.0
6.5
5.5
Upper limit of normal range6
AACE/ACE: recommended target<6.5
ADA: recommended target<7
9.0
~20 to >40% have A1C > 9.5% NHANES/BRFSS; Harmel et al.; NCQA 2000
~40 to >50% have A1C > 8% NHANES/BRFSS; Harmel et al.
ADA. Diabetes Care 2003; 26(S1):S33-S50ACE Consensus Conference on Guidelines for Glycemic Control. Endocrine Practice, 2002HEDIS 2000. Washington: National Committee for Quality Assurance, 1999State of Managed Care Quality. National Committee for Quality Assurance, 2000

Advantages of CSIIAdvantages of CSII

The Goal of Insulin Therapy:Attempt to Mimic Normal Pancreatic Function
Schade, Skyler, Santiago, Rizza, “Intensive Insulin Therapy,” 1993, p. 131.
0
60
30
100
60
140
15
1930
HO URS
2330 0330 073015301130330
80
40
120
75
160
PLA SM AG LUC O SE
m g /d l
B L S HS
PLA SM A FREEIN SULIN
u/m l

Twice-daily Split-mixed RegimensTwice-daily Split-mixed Regimens
Regular
NPH
B SL HS
Insu
lin
Eff
ect
B
6-23

B SL HS B
lispro
GlargineIn
suli
n E
ffec
t
Basal Bolus Regimen with Glargine and LisproBasal Bolus Regimen with Glargine and Lispro
6-56

Continuous Subcutaneous Insulin Continuous Subcutaneous Insulin InfusionInfusion
B SL HS B
Insu
lin
Eff
ect
BolusBolus
BasalBasal

Pharmacokinetics of CSII vs MDI
• Uses only immediate acting insulin– More predictable absorption
• Uses one injection site
– Reduces variations in absorption
• Eliminates most of the subcutaneous insulin depot
• Closest match with physiologic needs
* Lauritzen: Diabetologia 1983; 24:326-9

Advantages of Pump Therapy
• Improved blood glucose control – Improved AIC’s– Decreased hypoglycemia and hyperglycemia– Delay in incidence and progression of complications
• Precise dosage delivery • Improved control for pre-conception and pregnancy• Management of dawn phenomenon• Increased flexibility in lifestyle• Improved control during exercise• Improved gastroparesis management

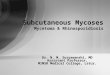
Population: Comparison of glycemic control in 58 patients while on MDI x 3yrs and subsequent CSII x 3yrs
Methods: Retrospective, observational cohort study of patients with Type 1 diabetes
Trial Evidence: CSII versus MDI use in routine clinical practice
MeanHbA1c%
10
9
8
7
6
MDI
CSII
MDI HbA1c >8.0%
Entire Cohort MDI HbA1c >9.0%
8.4
9.2
10.0
8.48.2
7.7
P=0.0006
P=0.0006
P=0.001
Bell and Ovalle, Endocr Pract 2000;6:357-60

Improved Control and Less Variability Improved Control and Less Variability With Pump TherapyWith Pump Therapy
Time (Day)12:00 a.m.12:00 a.m.6:00 a.m.6:00 a.m. 12:00 p.m.12:00 p.m.6:00 p.m.6:00 p.m. 12:00 a.m.12:00 a.m.0
50
100
150
200
250
300
350
400
Glucose (mg/dl)
Time (Day)12:00 a.m.12:00 a.m.6:00 a.m.6:00 a.m. 12:00 p.m.12:00 p.m.6:00 p.m.6:00 p.m. 12:00 a.m.12:00 a.m.0
50
100
150
200
250
300
350
400
Glucose (mg/dl)Finger StickSensor
Finger StickSensor
Pump TherapyPump Therapy Multiple Daily InjectionsMultiple Daily Injections

Improved Control:Improved Control:Decreased HypoglycemiaDecreased Hypoglycemia
138
22 2639 36
0
50
100
150
Pre CSII 1 yr 2 yr 3 yr 4 yr
------------ With CSII------------
Bode et al: Diabetes Care 1996; 19:324-7
Episodes perEpisodes per100 pt yrs100 pt yrs
N=55

Benefits of Decreased Hypoglycemia
• Reduced risk of diabetic encephalopathy
• Reduced risk of accidents and death
• Improved hypoglycemia awareness

ImprovedHypoglycemia Awareness
• Meticulous glycemic control reduced hypoglycemia events from 20 to 2 per month in this study of 21 patients
• Glycemic thresholds for hypoglycemia symptoms normalized in all groups
• Partial recovery of the counterregulatory response
Fanelli: Diabetes 1997;46: 1172-1181

15
7
0
2
4
6
8
10
12
14
16
Pre-CSII Post-CSII
Diabetic KetoacidosisDiabetic Ketoacidosis(e
pis
od
es /
100 p
t years
)
Bode, BW, Diabetes Care 19:324-7, 1996.

Improved Health Status with CSIIImproved Health Status with CSII
Worse2%
No Change16%
Improved82%
Association for Insulin Pump Therapy, Diabetes 1991:40:#1807
N=886Self-Reported Data

Advantages of Pump Therapy in Pregnancy
• Mimics normal physiology
• Decreases glucose excursions
• Reduces hypoglycemia
• Provides insulin regimen individualization
• Improves management of morning sickness
• Increase lifestyle flexibility
Jornsay, DL. CSII Therapy During Pregnancy. Diabetes Spectrum 11:1998: 26-32.

Children
• Recent studies show benefits for under 12 years of age
• Prevention and reduction of night-time hypoglycemia
• Ability to accommodate variable appetites and eating patterns
• Effective and safe with parental education/control/supervision
Buckingham, B; Kaufman, F;
ADA 61st Scientific Sessions, 2001

Pump Therapy in Type 2 diabetes
• Reduces glucose toxicity
• Decreases insulin resistance
• Restores sensitivity to oral agents and diet
• Often can result in reduced total daily insulin needs
Ilkova et al., Diabetes Care 1997, vol 20: p 1353. Glaser,1985; Garvey, 1985; Scarlett,1997
Must meet same criteria as Type 1

Challenges of Pump Therapy
• Learning curve
• Risk of DKA
• Possible weight gain
• Frequent monitoring required
• Potential site infections
• Inconvenience in wearing pump
• Education and follow-up required
• Cost

Cost and Insurance
• A pump typically lists for close to $5000.
• Pump supplies average $1,200 to $1,600 per year!
• Many insurance companies cover all or most of this cost.

Choosing a Pump . . .
• Ease of use• Clinical features• Safety features• Customer service• Cost of pump• Insurance coverage• Physician/CDE preference• Bolus options• Number of basal programs
• Training and education• Insulin delivery system• Patient age• Patient lifestyle• Cosmetic issues
Some things to consider……

Indications for Pump Indications for Pump TherapyTherapy

Criteria for Selection of a Pump Candidate
Clinical Indications:• Inadequate glucose control OR HbA1c >7.0% with MDI regimen• Hypoglycemia unawareness• Recurrent hypoglycemia• Dawn phenomenon• Preconception and pregnancy • Gastroparesis or other complications• Post-renal transplant

Patient Success Characteristics:
• Motivated• Realistic expectations• Ability to manage diabetes—MDI, frequent SMBG and
interpretation of results• Uses carbohydrate counting effectively• Family support• Financial resources• Psychological and emotional stability• Intellectual, physical, and technical ability to use the pump

Contraindications to Pump Therapy
Insufficient motivation to:
•Perform frequent (4+ daily) SBGM tests
•Learn and practice CHO counting
•Initially document activities of daily living
•Adjust to recommended medical therapy

Current Continuation RateCurrent Continuation Rate Continuous Subcutaneous Insulin Infusion (CSII)Continuous Subcutaneous Insulin Infusion (CSII)
Continued97%
Discontinued3%
N = 165N = 165Average Duration = 3.6 yearsAverage Duration = 3.6 yearsAverage Discontinuation <1%/yrAverage Discontinuation <1%/yr
Bode, et al.: Diabetes 1998; 47 (Suppl 1): 392.

Beginning Insulin Pump TherapyBeginning Insulin Pump Therapy

Basal Rate of Insulin
• Mimics fasting insulin secretion of a normal pancreas
• Continuous flow of insulin
• Replaces the intermediate or long acting insulin of MDI regimen
• Adjust to match metabolic need for insulin under fasting conditions

Bolus Insulin
• Simulates mealtime insulin secretion of normal pancreas
• Programmed for delivery by patient
• Replaces short acting insulin of MDI regimen
• Is given as needed by patient premeal or to correct for hyperglycemia

Pump Therapy Insulin Doses
Basal rate = 40 – 50% TDDBasal rate = 40 – 50% TDD
Bolus totals = 50 – 60% TDDBolus totals = 50 – 60% TDD
American Diabetes Association, Intensive Diabetes Management. 2nd ed. Alexandria, VA: 1998.Bode, BW. The Insulin Pump Therapy Book: Insights From the Experts. Sylmar, CA: MiniMed Technologies; 1995: 49-56, 85-93.
Remember: Always Individualize!

~50%
Basal*
Total Daily DoseTotal Daily Dose(~70-75% of prior insulin regimen TDD)(~70-75% of prior insulin regimen TDD)
~50%
Bolus*
Usually divided into 3 premeal dosesUsually divided into 3 premeal doses(depending on number and size of meals)(depending on number and size of meals)*Range: 40 to 60%*Range: 40 to 60%
Pre-Pump Dose
Establishing StartingEstablishing StartingBasal and Bolus DosesBasal and Bolus Doses

Total Daily Dose (75% pre-pump dose)
Example:
TDD (Total Daily Dose) = ~27 u/24 hrsTDD (Total Daily Dose) = ~27 u/24 hrs
27 u x .75 = 20.25 u TDD27 u x .75 = 20.25 u TDD
Note: If pre-pump dose of fast acting is >70% /24 hrs, may need If pre-pump dose of fast acting is >70% /24 hrs, may need
further reduction. further reduction.
Bode, BW. The Insulin Pump Therapy Book: Insights From the Experts. Sylmar, CA: MiniMed Technologies, 1995: 49-56, 85-93.

Basal Rate Calculation: 40 – 50% TDD
40 – 50 % of TDD 40 – 50 % of TDD ÷ 24 hours = u/hr÷ 24 hours = u/hr
Example:
TDD = 48 u x 0.4 = TDD = 48 u x 0.4 = 19.219.2 = = 0.8 u/hr0.8 u/hr 2424
American Diabetes Association, Intensive Diabetes Management. 2nd ed. Alexandria, VA: 1998.Bode, BW. The Insulin Pump Therapy Book: Insights From the Experts. Sylmar, CA: MiniMed Technologies; 1995: 49-56, 85-93.

Basal Rate Calculation
• May need to use 60% or higher of the TDD for insulin resistance:
Teens
Type 2
Dawn phenomenon

Which basal rate to start with??
• Most clinicians prefer to initiate a conservative basal rate.
• It’s always better if the patient’s blood glucose values run slightly higher than too low during pump initiation.
• It’s easier to increase a basal rate gradually by 0.1 u/hr.

Fine Tuning: Basal Rate
• Monitor BG pre-meal, post-meal, bedtime, 12am, and 2-4am
• We assess basal insulin by fasting and premeal BG’s• Test fasting BG with skipped meals• Adjust nighttime basal based on
2-4am and pre-breakfast BG• Usually adjust basal by 0.1 u/hr to avoid
over-correction




Bolus InsulinBolus Insulin

Bolus Dose Insulin
• Premeal boluses: – Taken before meals
– Covers mealtime carbohydrate intake
– Prevents postprandial hyperglycemia
• Correction or supplementation boluses:– Used to Correct and treat hyperglycemia
– May be given alone between meals for hyperglycemia
– May be given to supplement already scheduled insulin to cover premeal hyperglycemia

Calculation of Premeal Bolus Doses
Methods
1. Use the patient’s pre-pump insulin-to carb ratio
2. Formula: 500 Rule
3. Weight based Method
* Bode et al: Diabetes Care 1994: 19: 324-7

Determination of Insulin to Carb Ratio: Method 1
EXAMPLE: Pre-pump 1 unit of insulin: 15 gm carb
Note: 1 unit: 15 gm is often a “safe” starting pointfor most patients . . .

Determination of Insulin to Carb Ratio: Method 2
Use the 500 Rule:
Divide 500 by TDD= 1 unit insulin to ___ gm CHO as bolus
EXAMPLE: 500 ÷ 34 u= 15
Bolus ratio is 1 u insulin : 15 gm CHO

Weight (lb) Insulin u: CHO gm *
100-109 1: 16
110-129 1: 15
130-139 1: 14
140-149 1: 13
150-169 1: 12
170-179 1: 11
180-189 1: 10
190-199 1: 9
200+ 1: 8
Determination of Insulin to Carb Ratio: Method 3
*Walsh, Pumping Insulin, 2nd ed.Weight Based Method

Extended Bolus Option
• Equally divides, or “spreads” one bolus amount over a specific number of hours
• Use for: • long meals (parties or holidays)• high fat meals (pizza)• delayed digestion (gastroparesis)

Normal vs. Extended Bolus
Extended BolusNormal Bolus
Time Time
Insu
lin
Insu
lin

Split or Dual Wave Bolus Option
• Patient divides bolus into 2 separate bolus amounts
• Use for continuous snacking, high fat meals or snacks : Initial bolus: 30–50% of total bolus
Second bolus: – Set an Extended Bolus
OR – Bolus remainder 2 to 4 hours later

Split or Dual Wave Bolus
Time
Insu
lin
First Phase InsulinSecretion
Second PhaseInsulin Secretion

Dual Wave Bolus vs. Standard Bolus after High Fat Meal
050
100150200
250300350400
Standard Bolus
Dual WaveBolus

Pump Therapy Initiation Insulin: Carb Bolus Tips
• Use pre-pump MDI insulin-to-CHO ratio for boluses, if has been successful
• Try to keep CHO amount consistent at meals (consume same amount of CHO for each breakfast, each lunch, etc.)
• Avoid excessive protein, high fat content meals, alcohol, and foods not usually consumed

Carbohydrate CountingCarbohydrate Counting

Macronutrient Conversion to Blood Glucose

Glucose Elevations per Carbohydrate Glucose Elevations per Carbohydrate GramsGrams
Each gram of carbohydrate raises glucose by 3-4 mg/dlEach gram of carbohydrate raises glucose by 3-4 mg/dl
0
50
100
150
200
250
5 15 45
Blo
od
Glu
cose
Incr
ease
(m
g/d
l)
Carbohydrate grams ingested

Carbohydrate Counting
BenefitsAllows for variation in appetite
and preferences
Increases variety of food choices
Can be used to match insulin bolus doses to food intake

Carb Counting and Insulin Bolusing
Sample Meal 1 c. orange juice 30 g2 slices toast 30 g½ c. oatmeal 15 g1 soft-cooked egg1 tsp margarineCoffee & 1 T cream_____________________Total CHO: 75 gInsulin bolus: 5 units
Sample Meal2 slices wheat bread 30 g2 oz. turkey breastLettuce leaf, tomato slice1 tsp mayonnaise6-8 3-ring pretzels 15 g2 small choc cookies 15 gDiet soda, 16 oz__________Total CHO: 60 gInsulin bolus: 4 units
Insulin-to-Carb Ratio
EXAMPLE: 1 unit insulin: 15 grams CHO

Fine Tuning: Meal Bolus Doses
• Adjust bolus based on post-meal BGs
• Carbohydrate counting or pre-determined meal portion
• Individualize insulin to carbohydrate dose or insulin to premeal dose


Correction BolusesCorrection Boluses

Correction Bolus Insulin
• To be taken to correct for hyperglycemia
• Based on insulin sensitivity factor
• Goal is for correction bolus to lower blood glucose to within 30 to 50 mg/dl of target value

Insulin Sensitivity Factor
1 unit of insulin will blood glucose by: mg/dl
Regular: 1500 Rule
Humalog: 1800 Rule
1500 or 1800 divided by TDD= amount of blood glucose lowered by 1 unit insulin
Use to high blood glucose

Insulin Sensitivity Factor
EXAMPLETDD is 34 units
1500 Rule: 1500 ÷ 34 = 44 1 unit of Regular bg 44 mg/dl
1800 Rule: 1800 ÷ 34 = 53 1 unit of Humalog bg 53 mg/dl


Unused Insulin Rule
Lispro is gone in approx. 3 – 4 hrs
Decrease bolus 30% each hour:1st hour = 70% remaining2nd hour = 40% remaining3rd hour = 10% remaining4th hour = 0% remaining
Walsh. PA. Roberts. R Pumping Insulin. 3rd ed. San Diego, Calif: Torrey Pines Press; 2000

Preventing HypoglycemiaPreventing Hypoglycemia

Preventing Hypoglycemia
• Check BG 4-6 times per day
• Carry glucose tablets
• Have Glucagon Kit available

Preventing Hypoglycemia
• Test before driving and ideally 1 hour later (target: over 100 mg/dl)
• Perform two SMBG 30 minutes apart prior to bedtime (confirming rising or falling BG)
• When drinking alcohol, perform SMBG hourly
• With exercise, perform SMBG pre- and post-exercise
• If hypoglycemia episodes persist, raise target glucose levels

Hypoglycemia Treatment Guidelines
The Rule of 15• If BG is 70 mg/dl or below
– Treat with 15 grams of carbohydrates (glucose tabs)– Check BG in 15 minutes, and if not above 70 mg/dl, repeat
treatment
Glucagon• Current emergency kit readily available and knowledgeable
person trained to administer

PreventingPreventingHyperglycemia and DKAHyperglycemia and DKA

Preventing Hyperglycemia and DKA
• Monitor BG 4-6 times per day
• Use Correction Boluses when appropriate
• Change infusion set every 2-3 days

Hyperglycemia Treatment GuidelinesThe Key to Preventing DKA
1st BG over 250 mg/dl:• Take a correction bolus via pump, check again
in 1 hour
2nd BG over 250 mg/dl:• Take correction bolus by syringe and change
infusion set, review pump, check BG again in 1 hour• Call physician immediately if nausea and vomiting and/or ketones
are present

Follow-Up: The Patient’s Role
Every Day• Check BG 4-6 times a day, and
always before bed• Follow hypoglycemia guidelines• Follow hyperglycemia guidelines
Every 3 months• Visit healthcare provider - even if
feeling well• Review log book and pump
settings with physician/CDE• Get a HbA1c
Every month• Review DKA prevention• Check BG
- 3am (overnight)- 1 and/or 2-hour post-meal BG for all meals on a given day

Conclusion
• Pump Therapy is becoming widely recognized as the best way to treat insulin requiring diabetes
• It is now considered standard of care in appropriate patients
• Pump Therapy is not difficult to implement in a medical practice
• When implantable continuous glucose sensors are perfected and become readily available; pumps will become an even greater tool

Implantable Pumps: Coming Soon?
•Continuous intraperitoneal insulin delivery – provides physiologic insulin absorption
•Negative pressure insulin reservoir –special U-400 insulin refilled every 2 to 3 months
• Small, programmer communicates with the pump using RF telemetry.
In the US implantable insulin pumps are investigational only

Consider Pump Therapy…
• Poor HbA1c’s• Frequent hypoglycemia• Dawn phenomenon• Pediatrics• Pregnancy• Gastroparesis• Hectic Lifestyle
• Shift Work
• Insulin Requiring Type 2’s?