Embed Size (px)
Citation preview

Basic Pharmacokinetics REV. 99.4.25 15-1Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
CHAPTER 15 Practice Exams: Exam 2

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-2Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.1 Nifedipine: Exam 2
Nifedipine (Procardia @) is a calcium channel blocker which specifically inhibits potential-dependent channels notreceptor-operated channels, preventing calcium influx of cardiac and vascular smooth muscle (coronary, cerebral).Calcium channel blockers reduce myocardial contractility and A-V node conduction by reducing the slow inward cal-cium current. They are indicated in angina, cardiac dysrhythmias, and hypertension among others. Nifedipineappears to be metabolized entirely into an inactive metabolite, an acid and subsequently further metabolized to a lac-tone. Both the acid and the lactone are excreted into the urine and the feces.
Hepatic blood flow in normals is 1.6 L/min
Renal blood flow in normals is 1.2 L/min
Echizen and Eichelbaum (Clin Pkin 1986; 11:425-49) and Kleinbloesem et al (Clin Pcol Therap 1986; 40: 21-8)reviewed the pharmacokinetics of Nifedipine. While the drug is not routinely given by IV bolus and does not strictlyconform to a one compartment model, let's treat the data as if those problems can be ignored. The following data isoffered for evaluation:
TABLE 1-1. Nifedipine IV Bolus Profile
Time (hr) Cp (mcg/L) Cm1 (mcg/L) Xm1f (mg) Xm1u (mg) Xm2f (mg) Xm2u (mg)
0.5 24.7
1 44.4
2 139 71.8 .14 .59
4 65.6 96.5 .44 1.83 .028 .11
6 31.1 100 .77 3.25 .073 .29
8 14.6 94.7 1.1 4.65 .135 .54
12 76.5 1.69 7.10 .291 1.15
24 34 2.77 11.63 .75 2.95
7 days 3.6 15.1 1.3 5.0
TABLE 1-2 Nifedipine Oral information
Brand Generic
Route IV Oral Capsule Oral Capsule
Dose (mg) 25 10 10
AUC (ug/L*hr) 785 236 204
AUMC (ug/L*hr2 ) 2093 866 816

Practice Exams: Exam 2 : Nifedipine: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-3Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.1.1 NIFEDIPINE QUESTIONS:
Find:
1) MRT iv (hr)
2) Ke (elimination rate constant) for Nife-dipine (hr-1 )
3) T 1/2 for Nifedipine
4) Cp0 for iv dose (ug/L)
5) Vd for Nifedipine (L)
7) Cp of Nifedipine at one hour after theIV dose
8) AUC from 0 to one hour for the IV dose
9) Total Body Clearance of Nifedipine (L/hr)
10) Renal Clearance of Nifedipine (L/hr)
11) Hepatic Clearance of Nifedipine (L/hr)
12) Renal Extraction Ratio
13) Hepatic Extraction Ratio
14) Absolute bioavailability for the brandname capsule
15) MRT (oral brand name capsule) (hr)
16) MAT (oral brand name capsule) (hr)
17) Ka, the apparent absorbtion rate con-stant, for the brand name capsule (hr-1 )
18) Peak time for the brand name capsule(hr)
19) Cpmax , the maximum concentrationof the brand name oral capsule give as asingle dose (ug/L)
20) Absolute bioavailability for the genericcapsule
21) MRT (oral generic capsule) (hr)
22) MAT (oral generic capsule) (hr)
23) Ka, the apparent absorbtion rate con-stant, for the generic capsule (hr-1 )
24) Peak time for the generic capsule (hr)
25) Cpmax , the maximum concentrationof the generic oral capsule give as a singledose (ug/L)
26) Comparative bioavailability of the oralcapsules
Your patient is controlled by 20 mg TIDof the brand name oral capsule when heis healthy.
27) What is his N for that dosing regimen?
28) Cpssmax for this patient at this dosingregimen (ug/L)
29) Cpssavg for this patient at this dosingregimen (ug/L)
30) Cpssmin for this patient at this dosingregimen (ug/L)
You want to maintain his plasma con-centrations between 110% of Cpssmaxand 90% of Cpssmin . How would youchange the dosage regimen to if yourpatient suffered from:
31) stenosis of the kidney (Fr = 0.67).
32) renal failure (Fi = 0.67).
33) stenosis of the liver (Fr = 0.67)
34) cirrhosis of the liver (Fi = 0.67)

Practice Exams: Exam 2 : Nifedipine: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-4Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
TABLE 1-3 Nifedipine Answer Pool
Small Medium Large Dosing changes:
a) 0.00 a) 1.85 a) 59 a) 10 mg once daily
b) 0.05 b) 2.67 b) 85 b) 10 mg BID
c) 0.33 c) 3.67 c) 92.5 c) 10 mg TID
d) 0.375 d) 4.0 d) 101 d) 10 mg QID
e) 0.65 e) 4.32 e) 124 e) 20 mg once daily
f) 0.75 f) 9.3 f) 147 f) 20 mg BID
g) 0.85 g) 18.5 g) 185 g) 20 mg TID (no change necessary)
h) 1.0 h) 32 h) 202 h) 20 mg QID
i) 1.33 i) 38 i) 248 i) 30 mg once daily
j) 1.57 j) 49 j) 294 j) 30 mg BID

Practice Exams: Exam 2 : Nifedipine: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-5Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.1.2 NIFEDIPINE SOLUTIONS
1.
2.
3.
4.
5.
6. skip (error in numbering)
7.
8.
9.
10.
11.
12.
13.
14. Absolute bioavailability for brandname capsule = 0.75
15. Oral brand name capsule
16. Oral brand name capsule
17. Oral brand name capsule
18. Oral brand name peak time
19. Oral brand name
20. Absolute bioavailability forgeneric = 0.65
21. Oral generic capsule
22. Oral generic capsule
23. Oral generic capsule
24. Oral generic capsule peak time
25. Oral generic capsule
26. Comparative bioavailability of theoral capsules B/A:
AUC = 0.86 (ok)
Peak time = 1.18 (ok)
Cpmax = 0.78 (not ok!)
27.
28.
29.
30.
31. No change
32. No change
33. No change
34. No change
MRT iv 2.67hr=
ke 0.375hr1–
=
T1 2⁄ 1.85hr=
Cp0 294ug L⁄=
Vd 85L=
Cp1 202ug L⁄=
AUC0 1– 248ug L⁄ hr⋅=
Cls 32L hr⁄=
Clr 0=
Clh 32L hr⁄=
Er 0=
Eh 0.33=
MRT 3.67hr=
MAT 1.0hr=
Ka 1.0hr1–
=
1.57hr
Cpmax 49ug L⁄=
MRT 4hr=
MAT 1.33hr=
Ka 0.75hr1–
=
1.85hr
Cpmax 38ug L⁄=
N 4.32=
Cpss
max 185ug L⁄=
Cpss
ave 59ug L⁄=
Cpss
min 9.3ug L⁄=

Practice Exams: Exam 2 : Valproate: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-6Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.2 Valproate: Exam 2
All questions are internally consistent. Information gained in any one can be used in all others. Note, however, thereis a change in patient status midway through.
Valproate is a carboxylic acid anticonvulsant. Its activity may be related, at least in part, to increase concentra-tions of the neurotransmitter inhibitor gamma aminobutyric acid in the brain. It is used alone or in combinationwith other anticonvulsants. in the prophylactic management of petit mal. It appears to be almost entirely clearedby liver function with negligible amounts excreted into the urine unchanged. It comes as soft gelatin capsules of 250mg and enteric coated tablets 250 and 500 mg. The therapeutic range for valproate appears to be between 20 and 100mic/ml. The volume of distribution is 0.19 L/Kg and your patient is 70 kg.
TABLE 1-4
IV bolus Brand Generic
Dose (mg) 500 250 250
AUC (mg/L*hr) 594 273 253
AUMC(mg/L*hr2 ) 9428.6 4605.5 4184.6
Tpeak (hr) 2.95
Cpmax 14.35
Bioavailability (f) 1.0 .92

Practice Exams: Exam 2 : Valproate: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-7Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.2.1 VALPROATE QUESTIONS
1) Calculate the MRTiv of Valproate (hr).
a) 11 b) 15.87 c) 16.54 d) 16.87 e) 17.08
2) Calculate the rate constant of elimination (hr-1 ) in normals ?
a) 0.091 b) 0.063 c) 0.060 d) 0.0593 e) 0.0585
3) Calculate the half life of Valproate (hr)?
a) 7.6 b) 11 c) 11.5 d) 11.7 e) 11.8
4) Calculate the hepatic clearance of valproate (L/hr).
a) 0.0084 b) 0.063 c) 0.84 d) 1.25 d) 2.5
5) Calculate the hepatic extraction ratio of valproate.
a) 0.0063 b) 0.0084 c) 0.063 d) 0.084 e) 0.84
6) What is the maximum N for multiple dosing of Valproate?
a) 0.78 b) 1.65 c) 2.12 d) 2.32 e) 2.5
7) What is the maximum acceptable dosing interval for normal patients (hr)?
a) 8 b) 12 c) 18 d) 24 e) 25.5
8) What is the N if we are going to dose TID?
a) 0.63 b) 0.727 c) 0.842 d) 1.25 e) 1.42
9) If you dosed this patient 500 mg BID with the brand name product, what would be your maximum concentration atsteady state (mg/L)?
a) 87.3 b) 70.9 c) 65.2 d) 52.8 e) 45.8
10) What would be your minimum concentration at steady state (mg/L)?
a) 52.8 b) 32.7 c) 30.1 d) 27.1 e) 22.9

Practice Exams: Exam 2 : Valproate: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-8Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
11) What would be your average concentration at steady state (mg/L)?
a) 63.8 b) 49.8 c) 47.7 d) 45.8 e) 34.4
12) What loading dose would you give to get to Cpss right away (mg)?
a) 250 b) 500 c) 750 d) 1000 e) 1500
13) If you changed the dosage regimen to 250 mg QID, what would happen to the Cpssmax, Cpssave, Cpssmin?
a) Cpssmax - up, Cpssave - up, Cpssmin - up
b) Cpssmax - down, Cpssave - down, Cpssmin - down
c) Cpssmax - same, Cpssave - same, Cpssmin - same
d) Cpssmax - up, Cpssave - same, Cpssmin - down
e) Cpssmax - down, Cpssave - same, Cpssmin - up
14) Calculate f, the absolute bioavailability of the generic product.
a) 0.67 b) 0.75 c) 0.85 d) 0.93e) 1.0
15) Calculate the comparative bioavailability of the generic product.
a) 0.67 b) 0.75 c) 0.85 d) 0.93e) 1.0
16) Calculate the MRToral of the generic product.
a) 11 b) 15.87 c) 16.54 d) 16.87 e) 17.08
17) Calculate the MAT of the generic product.
a) 0.67 b) 0.75 c) 0.85 d) 0.93e) 1.0
18) Calculate the Ka of the generic product.
a) 1.5 b) 1.33 c) 1.18 d) 1.08 e) 1.0
19) Calculate the peak time of the generic product.
a) 2.21 b) 2.45 c) 2.59 d) 2.76 e) 2.95
20) Calculate the Cpmax of the generic product.

Practice Exams: Exam 2 : Valproate: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-9Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
a) 8.1 b) 9.3 c) 10.7 d) 12.6 e) 14.4
21) Is the generic product bioequivalent?
a) Yes
b) No, because the comparative bioavailability is outside the federal guidelines.
c) No, because the ratio of the peak times is outside the federal guidlines.
d) No, because the ratio of the Cpmax s is outside the federal guidlines.
e) No, because the generic fails more than one of the required comparisons.
In patients who are also currently on phenobarbital their intrinsic clearance of valproate increases by 50% as the phe-nobarbital induces the enzymes which metabolize valproate. Further questions refer to this condition.
22) Calculate his new clearance.
a) 0.0084 b) 0.063 c) 0.84 d) 1.25 d) 2.5
23) Calculate his new K.
a) 0.095 b) 0.084 c) 0.063 d) 0.059 e) 0.042
24) Calculate his new maximum acceptable dosing interval (hr).
a) 8 b) 12 c) 17 d) 18 e) 24
25) What dosage regimen would you recommend to try to maintain his plasma concentrations within 110% of the max-imum and 90% of the minimum concentrations attained when he was normal?
a) 750 mg BID b) 500 mg TID c) 750 mg TID d) 250 mg QID e) 500 mg QID
Practice Exams: Exam 2 : Valproate: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-10Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.2.2 VALPROATE SOLUTIONS

Practice Exams: Exam 2 : Methyl phenidate
Basic Pharmacokinetics REV. 99.4.25 15-11Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.3 Methyl phenidate
Methyl phenidate (MP) (Ritalin@) is an effective stimulant in the treatment of narcolepsy in adults and attention deficitsyndrome in children. It is entirely metabolized to the inactive metabolite, Ritalinic Acid (RA), by the liver which issubsequently excreted unchanged into the urine. The following information was obtained from a 70 Kg male.
QH = 24 mL/min/Kg
QR = 19 mL/min/Kg
TABLE 1-6 Ritalin Answer Pool
TABLE 1-5 Ritalin Data
IVBrand Name Generic
Dose (mg) 10 20 20
AUC (ug/ml*hr) 0.20 0.04 0.035
AUMC (ug/ml*hr2 0.32 0.14 0.1225
Itty- Bitty Tiny Puny Small Medium Large Words
a 0 0.016 0.1 1.1 10 100 yes
b 0.00016 0.0251 0.125 1.6 20 125 no, Ratio of Tps
c 0.0005 0.035 0.25 1.75 30 225 no, Ratio of Cmaxs
d 0.00074 0.042 0.35 1.9 40 375 no, Ratio of AUCs
e 0.00084 0.05 0.42 2.6 50 435 no, Ratio of AUMCs
f 0.0016 0.067 0.53 3.5 60 550 no, more than one criterion
g 0.005 0.075 0.625 4.2 70 675 20 mg TID
h 0.0074 0.0875 0.727 5.0 80 750 20 mg BID
i 0.0084 0.091 0.875 7.27 90 875 20 mg QD
j 0.0090 0.096 0.91 8.75 96 995 20 mg QID

Practice Exams: Exam 2 : Methyl phenidate
Basic Pharmacokinetics REV. 99.4.25 15-12Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.3.1 METHYL PHENIDATE QUESTIONS:
1) MRT iv (hr)
2) Ke (elimination rate constant) forRitalin (hr-1 )
3) T 1/2 for Ritalin (hr)
4) Cp0 for iv dose (ug/mL)
5) Vd for Ritalin (L)
6) Cp of Ritalin at one hour after the IVdose
7) AUC from 0 to one hour for the IV dose
8) Total Body Clearance of Ritalin (L/hr)
9) Renal Clearance of Ritalin (L/hr)
10) Hepatic Clearance of Ritalin (L/hr)
11) Intrinsic Hepatic Clearance of Ritalin(L/hr)
12) Renal Extraction Ratio
13) Hepatic Extraction Ratio
14) Absolute bioavailability for the brandname tablet
15) MRT (oral brand name tablet) (hr)
16) MAT (oral brand name tablet) (hr)
17) Ka, the apparent absorbtion rate con-stant, for the brand name tablet (hr-1 )
18) Peak time for the brand name tablet(hr)
19) Cpmax , the maximum concentration ofthe brand name oral tablet give as a singledose (ug/mL)
20) Absolute bioavailability for the generictablet
21) MRT (oral generic tablet) (hr)
22) MAT (oral generic tablet) (hr)
23) Ka, the apparent absorbtion rate con-stant, for the generic tablet (hr-1 )
24) Peak time for the generic tablet (hr)
25) Cpmax , the maximum concentration ofthe generic oral tablet give as a single dose(ug/mL)
26) Comparative bioavailability of the oraltablets
27) Are the tablets bioequivalent?
Your patient is controlled by 20 mg TID ofthe brand name oral tablet when he ishealthy. For This patient and this dosageregimen, what is his:
28) N ?
29) Cpssmax (ug/mL)
30) Cpssavg (ug/mL)
31) Cpssmin (ug/mL)
You want to maintain his plasma concen-trations between 110% of Cpss
max and 90% of
Cpssmin . How would you change the dosage
regimen to if your patient suffered from:
(in no case was there a change in Vd)
32) stenosis of the kidney (Fr = 0.67)?
33) renal failure (Fi = 0.34)?
34) stenosis of the liver (Fr = 0.67)?
35) cirrhosis of the liver. (Fi = 0.67)?
36) treatment with phenobarbital (Fi =1.33)?

Practice Exams: Exam 2 : Methyl phenidate
Basic Pharmacokinetics REV. 99.4.25 15-13Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.3.2 METHYL PHENIDATE SOLUTIONS:
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14. Brand name -
15. Brand name -
16. Brand name -
17. Brand name -
18. Brand name -
19. Brand name -
20. Generic -
21. Generic -
22. Generic -
23. Generic -
24. Generic -
25. Generic -
26. Comparative bioavailability =0.875
27. Yes, the tablets are bioequivalent -all parameters are within federal guide-lines.
28.
29.
30.
31.
32. 20 mg TID
33. 20 mg TID
34. 20 mg BID
35. 20 mg TID
36. 20 mg QID
MRT iv 1.6hr=
k 0.625hr1–
=
T1 2⁄ 1.1hr=
Cp0 0.125ug mL⁄=
Vd 80L=
Cp1 0.067ug mL⁄=
AUC0 1– 0.096ug mL hr⋅⁄=
Cls 50L hr⁄=
Clr 0=
Clh 50L hr⁄=
Clint 100L hr⁄=
Er 0=
Eh 0.53=
f 0.1=
MRT 3.5hr=
MAT 1.9hr=
Ka 0.526hr1–
=
Tpeak 1.74hr=
Cpmax 0.0084ug mL⁄=
f 0.0875=
MRT 3.5hr=
MAT 1.9hr=
Ka 0.53hr1–
=
Tpeak 1.75hr=
Cpmax 0.0074ug mL⁄=
N 7.27=
Cpss
max 0.0251ug mL⁄=
Cpss
avg 0.005ug mL⁄=
Cpss
min 0.00016ug mL⁄=

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-14Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/

Practice Exams: Exam 2 : Verapamil
Basic Pharmacokinetics REV. 99.4.25 15-15Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.4 Verapamil
Verapamil is a calcium channel blocker with vasodilatory and antiarrhythmic effects. It is about 95% metabolized bythe liver with the metabolites showing up in the urine and feces.
Hepatic blood flow in normals is 1.6 L/min
Renal blood flow in normals is 1.2 L/min
TABLE 1-7 Verapamil Data
TABLE 1-8 Verapamil Answer Pool
Brand Generic
Route IV Oral Tablet Oral Tablet
Dose (mg) 15 80 80
AUC (ng/mL*hr) 300 480 400
AUMC (ng/mL*hr2 ) 1600 2690 2280
Tiny Small Medium Large Dosing regimens Bioavailability answers
a 0 1.06 26 116 40 mg qd Yes
b 0.063 2.15 46 267 40 mf bid No, tp ratio is not within limits
c 0.188 2.50 47.5 369 40 mg tid No, Cpmax ratio is not within limits
d 0.250 2.70 50 533 40 mg qid No, AUC ratio is not within limits
e 0.270 3.69 56 637 80 mg qd No, f ratio is not within limits
f 0.300 5.33 61.5 830 80 mg bid No, ka ratio is not within limits
g 0.370 5.60 76.5 905 80 mg tid No, ke ratio is not within limits
h 0.693 5.70 83 970 80 mg qid No, MRT ratio is not within limits
i 0.85 6.37 90.5 1160 160 mg qd No, Cl ratio is not within limits
j 0.905 8.30 97 2670 160 mg bid No, more than one of the required ratios are no within limits

Practice Exams: Exam 2 : Verapamil
Basic Pharmacokinetics REV. 99.4.25 15-16Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.4.1 VERAPAMIL QUESTIONS
1) MRT iv (hr)
2) Ke (elimination rate constant) for Vera-pamil (hr-1 )
3) T 1/2 for Verapamil
4) Cp0 for iv dose (ug/L)
5) Vd for Verapamil (L)
7) Cp of Verapamil at one hour after the IVdose
8) AUC from 0 to one hour for the IV dose
9) Total Body Clearance of Verapamil (L/hr)
10) Renal Clearance of Verapamil (L/hr)
11) Hepatic Clearance of Verapamil (L/hr)
12) Renal Extraction Ratio
13) Hepatic Extraction Ratio
14) Absolute bioavailability for the brandname tablet
15) MRT (oral brand name tablet) (hr)
16) MAT (oral brand name tablet) (hr)
17) Ka, the apparent absorbtion rate con-stant, for the brand name tablet (hr-1 )
18) Peak time for the brand name tablet(hr)
19) Cpmax , the maximum concentrationof the brand name oral tablet give as a sin-gle dose (ug/L)
20) Absolute bioavailability for the generictablet
21) MRT (oral generic tablet) (hr)
22) MAT (oral generic tablet) (hr)
23) Ka, the apparent absorbtion rate con-stant, for the generic tablet (hr-1 )
24) Peak time for the generic tablet (hr)
25) Cpmax , the maximum concentrationof the generic oral tablet give as a singledose (ug/L)
26) Comparative bioavailability of the oraltablets
27) Are the tablets bioequivalent?
Your patient is controlled by 80 mg TIDof the brand name oral tablet when he ishealthy.
28) What is his N for that dosing regimen?
29) Cpssmax for this patient at this dosingregimen (ug/L)
30) Cpssavg for this patient at this dosingregimen (ug/L)
31) Cpssmin for this patient at this dosingregimen (ug/L)
You want to maintain his plasma con-centrations between 110% of Cpssmaxand 90% of Cpssmin . How would youchange the dosage regimen to if yourpatient suffered from:
32) stenosis of the kidney (Fr = 0.67). (Nochange in volume of distribution.)
33) renal failure (Fi = 0.34).(Volume ofdistribution is reduced in this disease to50% of normal)
34) stenosis of the liver (Fr = 0.67) (Nochange in volume of distribution)
35) cirrhosis of the liver (Volume of Dis-tribution and the bioavailability are bothdoubled while the half life is quadrupled )

Practice Exams: Exam 2 : Verapamil
Basic Pharmacokinetics REV. 99.4.25 15-17Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.4.2 VERAPAMIL SOLUTIONS
1.
2.
3.
4.
5.
6. skip - error in numbering
7.
8.
9.
10.
11.
12.
13. Correction - should
be added to answer pool
14. Brand name tablet - absolute bio-availability = 0.30
15. Brand name tablet -
16. Brand name tablet -
17. Brand name tablet -
18. Brand name tablet - peak time -
19. Brand name tablet -
20. Generic - Absolute bioavailability
-
21. Generic -
22. Generic -
23. Generic -
24. Generic -
25. Generic -
26. Comparative bioavailability - 0.85
27. The tablets are not bioequivalent -peak time ratio is not within limits.
28.
29.
30. (change inanswer pool)
31.
32. No change in dosing regimen - 80mg TID
MRT iv 5.33hr=
ke 0.188hr1–
=
T1 2⁄ 3.69hr=
Cp0 56ug L⁄=
Vd 267L=
Cp1 47ug L⁄=
AUC0 1– 50ug L⁄ hr⋅=
Cl 50L hr⁄=
Clr 2.50L hr⁄=
Clh 47.5L hr⁄=
Er 0.063=
Eh 0.49=
MRT 5.60hr=
MAT 0.270hr=
Ka 3.69hr1–
=
0.85hr
Cpmax 76.5ug L⁄=
f 0.25=
MRT 5.7hr=
MAT 0.37hr=
Ka 2.70hr1–
=
Tpeak 1.06hr=
Cpmax 61.5ug L⁄=
N 2.15=
Cpss
max 116ug L⁄=
Cpss
avg 60ug L⁄=
Cpss
min 26ug L⁄=

Practice Exams: Exam 2 : Verapamil
Basic Pharmacokinetics REV. 99.4.25 15-18Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
33. 40 mg TID
34. No change in dosing regimen - 80mg TID
35. 40 mg BID
Practice Exams: Exam 2 : Hydromorphone hydrochloride
Basic Pharmacokinetics REV. 99.4.25 15-19Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
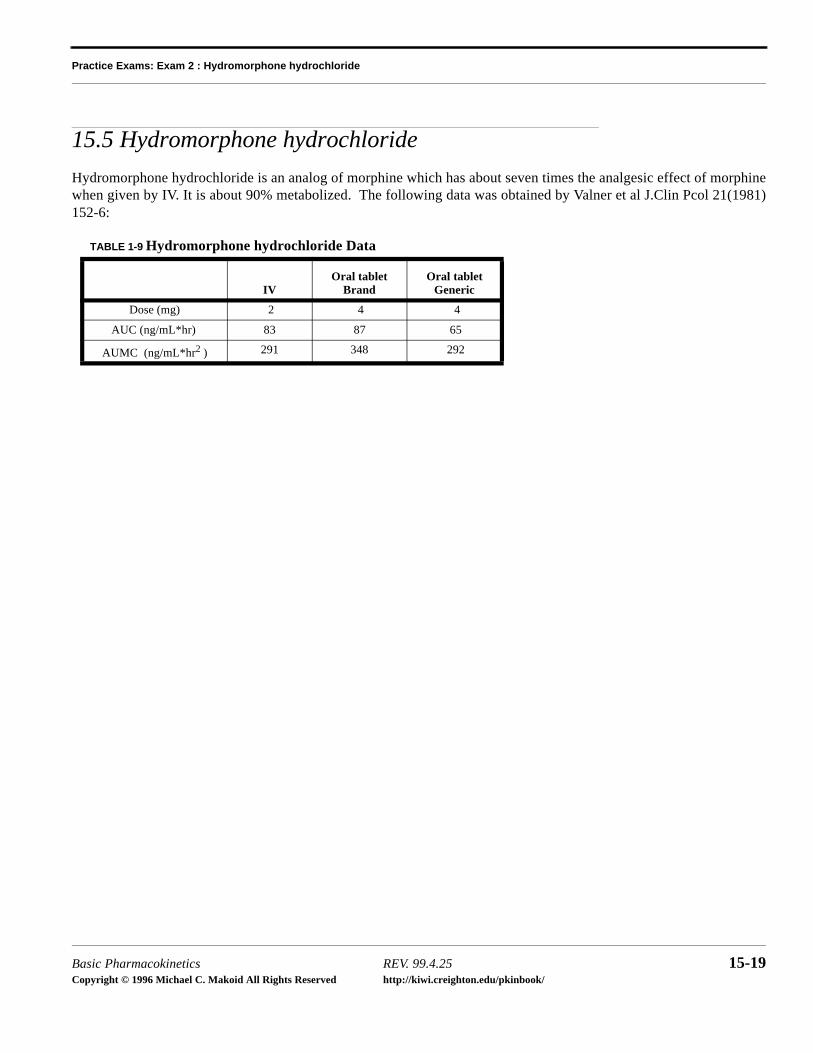
15.5 Hydromorphone hydrochloride
Hydromorphone hydrochloride is an analog of morphine which has about seven times the analgesic effect of morphinewhen given by IV. It is about 90% metabolized. The following data was obtained by Valner et al J.Clin Pcol 21(1981)152-6:
TABLE 1-9 Hydromorphone hydrochloride Data
IVOral tablet
Brand Oral tablet
Generic
Dose (mg) 2 4 4
AUC (ng/mL*hr) 83 87 65
AUMC (ng/mL*hr2 ) 291 348 292
Practice Exams: Exam 2 : Hydromorphone hydrochloride
Basic Pharmacokinetics REV. 99.4.25 15-20Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
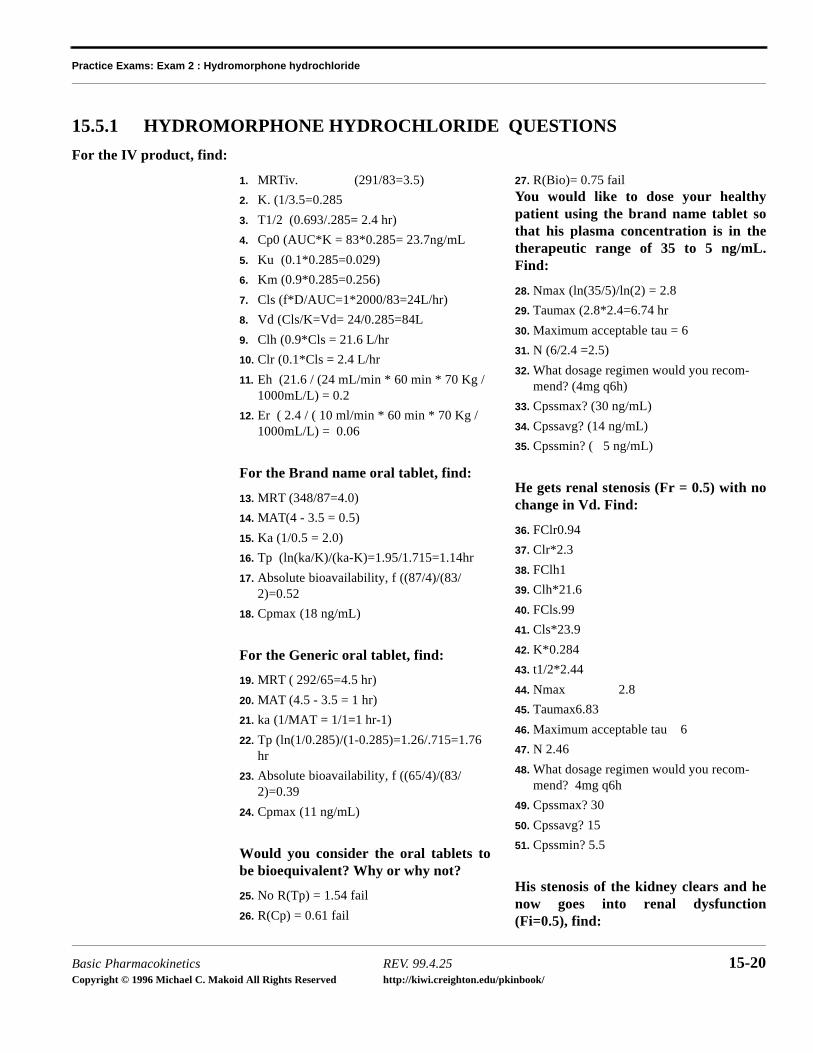
15.5.1 HYDROMORPHONE HYDROCHLORIDE QUESTIONS
For the IV product, find:
1. MRTiv. (291/83=3.5)
2. K. (1/3.5=0.285
3. T1/2 (0.693/.285= 2.4 hr)
4. Cp0 (AUC*K = 83*0.285= 23.7ng/mL
5. Ku (0.1*0.285=0.029)
6. Km (0.9*0.285=0.256)
7. Cls (f*D/AUC=1*2000/83=24L/hr)
8. Vd (Cls/K=Vd= 24/0.285=84L
9. Clh (0.9*Cls = 21.6 L/hr
10. Clr (0.1*Cls = 2.4 L/hr
11. Eh (21.6 / (24 mL/min * 60 min * 70 Kg / 1000mL/L) = 0.2
12. Er ( 2.4 / ( 10 ml/min * 60 min * 70 Kg / 1000mL/L) = 0.06
For the Brand name oral tablet, find:
13. MRT (348/87=4.0)
14. MAT(4 - 3.5 = 0.5)
15. Ka (1/0.5 = 2.0)
16. Tp (ln(ka/K)/(ka-K)=1.95/1.715=1.14hr
17. Absolute bioavailability, f ((87/4)/(83/2)=0.52
18. Cpmax (18 ng/mL)
For the Generic oral tablet, find:
19. MRT ( 292/65=4.5 hr)
20. MAT (4.5 - 3.5 = 1 hr)
21. ka (1/MAT = 1/1=1 hr-1)
22. Tp (ln(1/0.285)/(1-0.285)=1.26/.715=1.76 hr
23. Absolute bioavailability, f ((65/4)/(83/2)=0.39
24. Cpmax (11 ng/mL)
Would you consider the oral tablets tobe bioequivalent? Why or why not?
25. No R(Tp) = 1.54 fail
26. R(Cp) = 0.61 fail
27. R(Bio)= 0.75 failYou would like to dose your healthypatient using the brand name tablet sothat his plasma concentration is in thetherapeutic range of 35 to 5 ng/mL.Find:
28. Nmax (ln(35/5)/ln(2) = 2.8
29. Taumax (2.8*2.4=6.74 hr
30. Maximum acceptable tau = 6
31. N (6/2.4 =2.5)
32. What dosage regimen would you recom-mend? (4mg q6h)
33. Cpssmax? (30 ng/mL)
34. Cpssavg? (14 ng/mL)
35. Cpssmin? ( 5 ng/mL)
He gets renal stenosis (Fr = 0.5) with nochange in Vd. Find:
36. FClr0.94
37. Clr*2.3
38. FClh1
39. Clh*21.6
40. FCls.99
41. Cls*23.9
42. K*0.284
43. t1/2*2.44
44. Nmax 2.8
45. Taumax6.83
46. Maximum acceptable tau 6
47. N 2.46
48. What dosage regimen would you recom-mend? 4mg q6h
49. Cpssmax? 30
50. Cpssavg? 15
51. Cpssmin? 5.5
His stenosis of the kidney clears and henow goes into renal dysfunction(Fi=0.5), find:

Practice Exams: Exam 2 : Hydromorphone hydrochloride
Basic Pharmacokinetics REV. 99.4.25 15-21Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
52. FClr.52
53. Clr*1.23
54. FClh2
55. Clh*21.6
56. FCls.95
57. Cls*22.8
58. K*0.271
59. t1/2*2.55
60. Nmax 2.8
61. Taumax 7.13
62. Maximum acceptable tau6
63. N 2.35
64. What dosage regimen would you recom-mend? 4mg q6h
65. Cpssmax? 31
66. Cpssavg? 15
67. Cpssmin? 6.1
His renal dysfunction clears and now hesuffers from stenosis of the liver(Fr=0.5), Find:
68. FClr1
69. Clr*2.4
70. FClh.833
71. Clh*18
72. FCls.85
73. Cls*20.4
74. K*.243
75. t1/2*2.85
76. Nmax 2.8
77. Taumax8
78. Maximum acceptable tau 8
79. N 6
80. What dosage regimen would you recom-mend? 4 mg q6h
81. Cpssmax? 32
82. Cpssavg? 17
83. Cpssmin? 7.5
His stenosis of the liver clears and henow suffers from liver dysfunction(Fi=0.05), Find:
84. FClr1
85. Clr*2.4
86. FClh.56
87. Clh*12
88. FCls.6
89. Cls*14.4
90. K*.171
91. t1/2*4.04
92. Nmax 2.8
93. Taumax11.3
94. Maximum acceptable tau8
95. N 1.48
96. What dosage regimen would you recom-mend?4 mg q8h
97. Cpssmax? 33
98. Cpssavg? 18
99. Cpssmin?8.4

Practice Exams: Exam 2 : Hydromorphone hydrochloride
Basic Pharmacokinetics REV. 99.4.25 15-22Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-23Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.6 Fosinopril Sodium
Fosinopril Sodium (MW 585) is a phosphinic prodrug of the angiotensin converting enzyme (ACE) inhibitor fosinopri-lat (MW 563). After oral administration, fosinopril is slowly and incompletely absorbed, and is converted to the activefosinoprolat by esterases in the gastrointestinal mucosa and the liver. Unlike other ACE inhibitors, elimination of fosi-noprilat is divided equally between renal and hepatic pathways. With the IV dose fosinoprilat was given and mea-sured. With the oral dose fosinopril was given but fosinoprilat was measured. The following information was obtainedfrom a 70 Kg male. This information was constructed from Kostis et al “Fosinopril: Pharmacokinetics and pharmaco-dynamics in congestive heart failure” Clin Pcol Ther 58(6) 660-5 (1995); Hui et al “Pharmacokinetics of fosinopril inpatients with various degrees of renal function” Clin Pcol Ther 49(4) 457 -66 (1991)
QH = 24 mL/min/Kg Blood
QR = 19 mL/min/Kg Blood
TABLE 1-10 Fosinopril Data
IV Brand Name Tablet
Generic Tablet
Dose (mg) 7.5 10 10
AUC (ng/ml*hr) 5700 1500 1400
AUMC (ng/ml*hr2) 78000 25000 23100
TABLE 1-11 Fosinopril Answer Pool:
a 0 0.015 0.19 1.3 10 100 yes
b 0.00016 0.0251 0.21 1.6 13.7 142 no, Ratio of Tps
c 0.0005 0.035 0.25 1.75 16.6 192 no, Ratio of Cmaxs
d 0.00074 0.042 0.36 1.9 18 253 no, Ratio of AUCs
e 0.00084 0.05 0.42 2.8 50 387 no, Ratio of AUMCs
f 0.0016 0.067 0.53 3.5 67 402 no, more than one criterion
g 0.005 0.073 0.65 4.0 73 416 10 mg qid
h 0.0064 0.0875 0.72 5.6 84 750 10 mg tid
i 0.0084 0.091 0.84 7.0 93 875 10 mg bid
j 0.0090 0.096 0.93 9.5 96 995 10 mg qd
Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-24Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
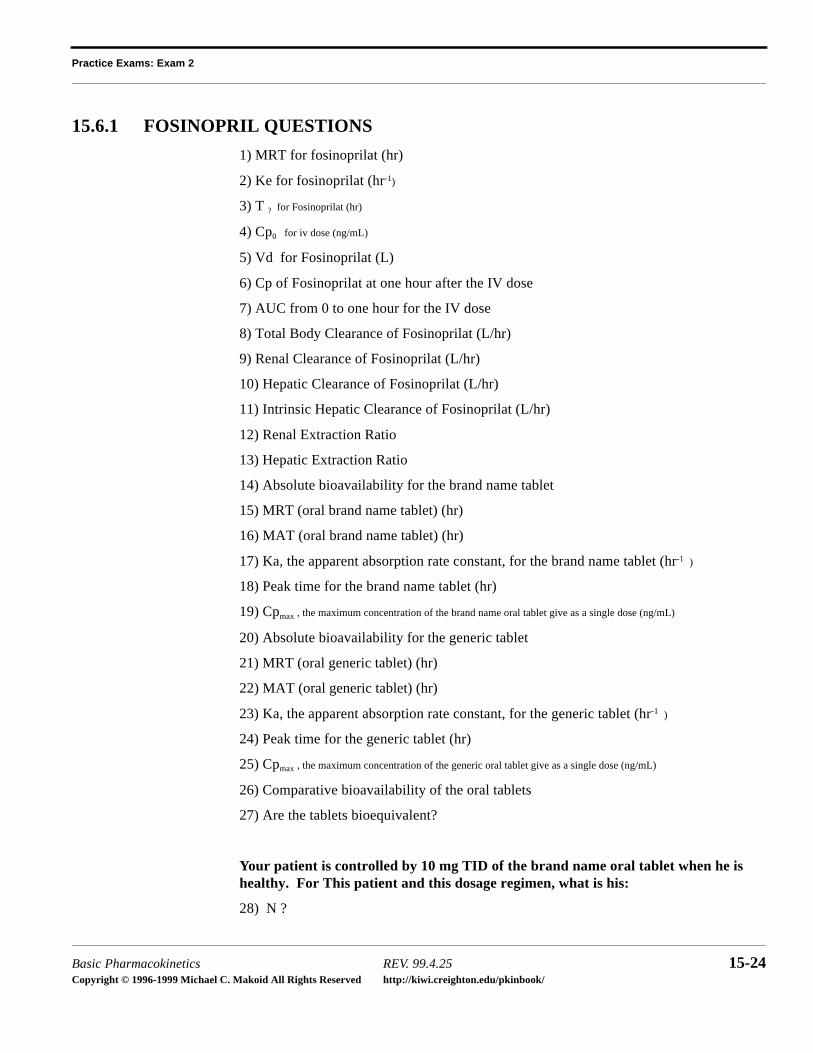
15.6.1 FOSINOPRIL QUESTIONS
1) MRT for fosinoprilat (hr)
2) Ke for fosinoprilat (hr-1)
3) T ? for Fosinoprilat (hr)
4) Cp0 for iv dose (ng/mL)
5) Vd for Fosinoprilat (L)
6) Cp of Fosinoprilat at one hour after the IV dose
7) AUC from 0 to one hour for the IV dose
8) Total Body Clearance of Fosinoprilat (L/hr)
9) Renal Clearance of Fosinoprilat (L/hr)
10) Hepatic Clearance of Fosinoprilat (L/hr)
11) Intrinsic Hepatic Clearance of Fosinoprilat (L/hr)
12) Renal Extraction Ratio
13) Hepatic Extraction Ratio
14) Absolute bioavailability for the brand name tablet
15) MRT (oral brand name tablet) (hr)
16) MAT (oral brand name tablet) (hr)
17) Ka, the apparent absorption rate constant, for the brand name tablet (hr-1 )
18) Peak time for the brand name tablet (hr)
19) Cpmax , the maximum concentration of the brand name oral tablet give as a single dose (ng/mL)
20) Absolute bioavailability for the generic tablet
21) MRT (oral generic tablet) (hr)
22) MAT (oral generic tablet) (hr)
23) Ka, the apparent absorption rate constant, for the generic tablet (hr-1 )
24) Peak time for the generic tablet (hr)
25) Cpmax , the maximum concentration of the generic oral tablet give as a single dose (ng/mL)
26) Comparative bioavailability of the oral tablets
27) Are the tablets bioequivalent?
Your patient is controlled by 10 mg TID of the brand name oral tablet when he is healthy. For This patient and this dosage regimen, what is his:
28) N ?

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-25Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
29) Cpssmax (ng/mL)
30) Cpssavg (ng/mL)
31) Cpssmin (ng/mL)
You want to maintain his plasma concentrations between 120% of Cpssmax and 80% of
Cpssmin . How would you change the dosage regimen to if your patient suffered from:
(in no case was there a change in Vd)
32) stenosis of the kidney (Fr = 0.67)?
33) renal failure (Fi = 0.34)?
34) stenosis of the liver (Fr = 0.67)?
35) cirrhosis of the liver. (Fi = 0.67)?
36) treatment with phenobarbital (Fi = 1.5)?

Practice Exams: Exam 2 : Fosinopril Sodium
Basic Pharmacokinetics REV. 99.4.25 15-26Copyright © 1996 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.6.2 FOSINOPRIL SODIUM SOLUTIONS
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11. Intrinsic Hepatic Clearance is
12.
13.
14. Oral brand name tablet absolutebioavailability is 0.21
15. Oral brand name tablet
16. Oral brand name tablet
17. Oral brand name tablet
18. Oral brand name tablet peak time
19. Oral brand name tablet
20. Oral generic tablet absolute bio-availability is 0.19
21. Oral generic tablet
22. Oral generic tablet
23. Generic tablet
24. Generic tablet peak time
25. Generic tablet
26. Comparative bioavailability of theoral tablets = 0.93
27. Yes! the tablets are bioequivalent
The AUCs, peak times, and s are
all within 20% range.
28.
29.
30.
31.
32. 10 mg TID
33. 10 mg BID
34. 10 mg TID
35. 10 mg TID
36. 10 mg QID
MRT 13.7hr=
k 0.073hr1–
=
T1 2⁄ 9.5hr=
Cp0 416ng mL⁄=
Vd 18L=
Cp1 387ng mL⁄=
AUC0 1– 402ng mL⁄=
Cls 1.3L hr⁄=
Clr 0.65L hr⁄=
Clh 0.65L hr⁄=
0.65L hr⁄
Er 0.015=
Eh 0.0064=
MRT 16.6hr=
MAT 2.8hr=
Ka 0.36hr1–
=
5.6hr
Cpmax 0.073ng mL⁄=
MRT 16.6hr=
MAT 2.8hr=
Ka 0.36hr1–
=
5.6hr
Cpmax 0.067ng mL⁄=
Cpmax
N 0.84=
Cpss
max 253ng mL⁄=
Cpss
avg 192ng mL⁄=
Cpss
min 142ng mL⁄=

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-27Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-28Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.7 Remoxipride
Remoxipride (MW 296 - Unionized Base pKa 9.4) is a new antipsychotic of the benzamide type (See figure 1). Thepharmacokinetics were studied by Movin-Osswald and Hammarlind-Udenaes (Brit. J Clin Pcol 1991 32(3) 355ff).Their results are summarized in table 1. The HCl salt of the drug was given (MW 332.5) to these patients in this studybut the drug concentration was reported as the free base in the plasma. In this study, 25% of the Remoxipride wasexcreted unchanged, 75% was metabolized. The hepatic and renal blood flow in these patients was 1.5 and 1.2 L/minrespectively. REMEMBER TO PAY ATTENTION TO UNITS.
FIGURE 4-5. Remoxipride
TABLE 1-12 Remoxipride Data
IV bolus Oral Solution Tablet A Tablet B
Dose (mg) 50 100 100
AUMC (umole/L*hr2 )
145 158.7 319.6 282.6
AUC (umole/L*hr) 20.9 19.8 37.6 31.4
Tp (hr) 3.6
Cpmax (mg/L) .8
f .75

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-29Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.7.1 REMOXIPRIDE QUESTIONS
1) Find the MRT of the IV product (hr).
2) Find the elimination rate constant of remoxipride (hr-1 ).
3) Find the Cp0 of the IV product (mg/L)
4) Find the volume of distribution of the IV product. (L)
5) Find the half life of remoxipride (hr).
6) Find the clearance of remoxipride (L/hr).
7) Find the renal clearance (L/hr).
8) Find the hepatic clearance
9) Find the renal extraction ratio.
10) Find the hepatic extraction ratio.
11) Find the MRT of remoxipride given as the oral solution (hr).
12) Find the MAT of remoxipride given as oral solution (hr).
13) Find the absorption rate constant of remoxipride given as an oral solution (hr-1 ).
14) Find the bioavailability of the oral solution (f).
15) Find the peak time of the oral solution (hr).
16) Find the MRT of remoxipride given as Tablet A, the brand name product.
17) Find the MAT of remoxipride given as Tablet A.
18) Find the apparent absorption rate constant (ka) of remoxipride given as Tablet A.
19) Find the peak time of Tablet A.
20) Find the single dose Cpmax for tablet A (mg/L)
21) Find the mean dissolution time (MDT) of Tablet A, the brand name product (hr).
22) Is Tablet B, the generic product is bioequivalent to Tablet A. Why or why not?
23) Find N for BID dosing.
24) Find Cpss max for two caps bid for the brand name product.
25) Find Cpss avg for two caps bid for the brand name product.
26) Find Cpss min for two caps bid for the brand name product.
27) Which change in physiological status would result in the most significant change inthe TBC of remoxipride?
a) Changes which effect the flow of blood to the liver.
b) Changes which effect the flow of blood to the kidney.
c) Changes which effect the function of the liver.

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-30Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
d) Changes which effect the function of the kidney.
Your patient is experiencing that change. That physiological function was up 75% abovenormal (F = 1.75).
28) Find his new renal clearance
29) Find his new hepatic clearance.
30) Find his new total body clearance.
31) Assuming now change in volume of distribution, find his new half life.
32 Assuming no change in dosage regimen, find his new N.
33 What dosing regimen would you recommend to return his plasma concentrations backto normal (within 110% of max and 90% of min)?

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-31Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.7.2 REMOXIPRIDE SOLUTIONS
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11. Oral solution
12. Oral solution
13. Oral solution
14. Oral solution bioavailability
15. Oral solution peak time
16. Tablet A
17. Tablet A
18. Tablet A
19. Tablet A peak time
20. Tablet A single dose
21. Tablet A
22. Tablet B is not bioequivalent to Tablet A because peak time and are out of
federal guidelines.
23. For dosing BID,
MRT 6.93hr=
ke 0.144hr1–
=
Cp0 0.88mg L⁄=
Vd 50L=
T1 2⁄ 4.8hr=
Cl 7.28L hr⁄=
Clr 1.8L hr⁄=
Clh 5.46L hr⁄=
Er 0.025=
Eh 0.06=
MRT 8hr=
MAT 1.07hr=
Ka 0.935hr1–
=
f 0.95=
2.4hr
MRT 8.5hr=
MAT 1.57hr=
Ka 0.637hr1–
=
3.0hr
Cpmax 1.03mg L⁄=
MDT 0.5hr=
Cpmax
N 2.5=

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-32Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
24.
25.
26.
27. The change in physiological status that would result in the most significant changein TBC of remoxipride is (C) - changeswhich effect the function of the liver.
28. New renal clearance = no change
29. New
30. New
31. New
32. New
33. The dosing regimen to recommend = 200 mg TID
Cpss
max 3.88mg L⁄=
Cpss
avg 1.85mg L⁄=
Cpss
min 0.685mg L⁄=
Clh 9.0L hr⁄=
Cls 10.8L hr⁄=
T1 2⁄ 3.2hr=
N 3.75=

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-33Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.8 Naproxen
Naprosyn@ (naproxen) is a nonsteroidal anti-inflammatory drug (NSAID) with analgesic properties. It is well absorbed (f = 0.95) and highly protein bound (98%) with a volume of distribution of about 10 L and a half-life of 13 hours in normal adults. It is almost entirely cleared by hepatic function (CLr = 1%) with about one-third being metabolized to the 6-o-desmethylnaproxen (which is further metabo-lized by conjugation) and two-thirds being conjugated directly. Both the 6-o-des-methyl metabolites as well as the conjugates are inactive.
Normal dosing is 500 mg Naproxen BID. You stock 200 and 500 mg tablets inyour HMO.
For the following conditions, new parameters are given in parentheses.
Concomitant treatment with Probenecid, a uricosuric which increases the urinaryexcretion of uric acid, while not interfering with the protein binding, effectivelyblocks the hepatic conjugation process reducing the hepatic function (Clinth ) toone-third of normal.
In chronic renal failure (Fir = 0.1) the protein binding is reduced (94%) because ofuremia. This results in a marginal increase in half-life (14 hr.)
In rheumatoid arthritis, hypoalbuminaemia results in a reduction in protein binding(97%) and increase in the volume of distribution (13 L).
Elderly patients exhibit a decrease in binding (96%), but no change in half-life orvolume of distribution.
For each of the conditions, (with Probenecid, chronic renal failure, arthritic, andelderly), please recommend a dosage regimen which would give approximately thesame plasma concentrations of free naproxen obtained in the normal case (+ 10%.)
Constants:
Extraction ratios are calculated for normals and considered to be constant through-out.
Qr 0.0191 Lmin kg⋅-------------------- renal blood perfusion 70kg 60min
hr---------⋅ ⋅ 80 L
hr-----blood≈=
QH 0.0238 Lmin kg⋅-------------------- hepatic blood perfusion 70kg 60min
hr---------⋅ ⋅ 100 L
hr-----blood≈=

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-34Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
15.8.1 NAPROXEN QUESTIONS
TABLE 1-1. Question Numbers For Exam
Patient Condition Normal Probenecid
treatment
Chronic
Renal Failure
Rheumatoid
arthritis
Elderly
Dose(mg) 1 27 51 75 99
f 2 28 52 76 100
fu 3 29 53 77 101
Vd (L) 4 30 54 78 102
k (hr-1) 5 31 55 79 103
T 1/2 (hr) 6 32 56 80 104
AUC (mg/L*hr) 7 33 57 81 105
% 8 34 58 82 106
% 9 35 59 83 107
(L/hr) 10 36 60 84 108
(L/hr) 11 37 61 85 109
(L/hr) 12 38 62 86 110
13
14
(L/hr) 15 39 63 87 111
(L/hr) 16 40 64 88 112
17 41 65 89 113
18 42 66 90 114
19 43 67 91 115
20 44 68 92 116
FCL 21 45 69 93 117
(hr) 22 46 70 94 118
N 23 47 71 95 119
24 48 72 96 120
Clh
Clr
Cltot
Clh
Clr
Eh
Er
Clhint
Clr int
FRh
FIh
FRr
FIr
τ
Cpss
maxfree
µgmL--------

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-35Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
25 49 73 97 121
26 50 74 98 122
Cpss
avgfree
µgmL--------
Cpss
minfree
µgmL--------
Answer Pool
S M L XL XXL XXXL
A 0.000067 0.0182 0.100 1.0 10.0 100
B 0.0005 0.0200 0.133 1.1 11.3 200
C 0.0050 0.0300 0.177 1.4 12.0 303
D 0.0080 0.0400 0.182 1.5 13.0 356
E 0.0089 0.0495 0.267 1.6 13.3 500
F 0.0092 0.0533 0.315 1.7 14.0 595
G 0.0095 0.0600 0.333 1.8 26.5 891
H 0.0097 0.0610 0.341 1.9 31.7 1044
I 0.0098 0.0675 0.528 2.0 38.1 2000
J 0.0099 0.0700 0.533 2.1 45.0 3000
A 0.0790 0.577 2.2 50.0
B 0.0798 0.615 2.9 53.0
C 0.0857 0.675 3.0 62.0
D 0.0923 0.700 5.3 80.0
E 0.0950 0.790 6.2 86.0
F 0.0970 0.798 8.0 92.0
G 0.0990 0.857 8.5 97.0
I 0.0999 0.923 9.0 99.0
J 0.09997 0.95 9.9 99.97
Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-36Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
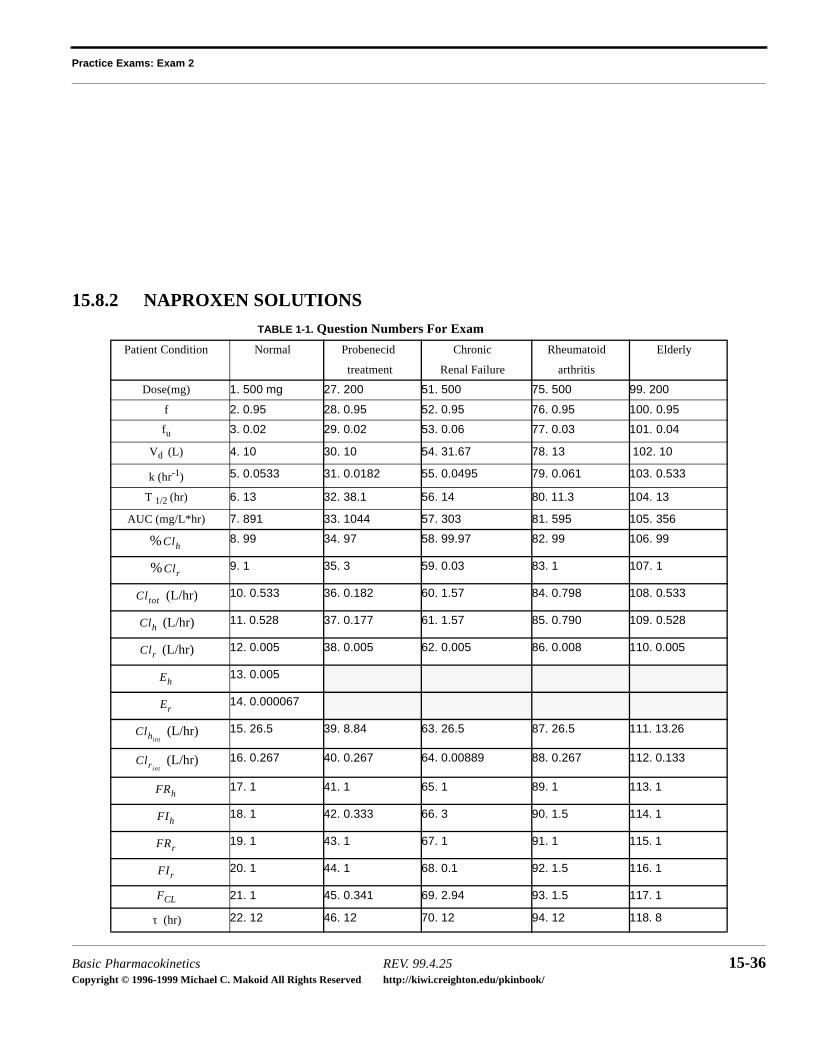
15.8.2 NAPROXEN SOLUTIONS
TABLE 1-1. Question Numbers For Exam
Patient Condition Normal Probenecid
treatment
Chronic
Renal Failure
Rheumatoid
arthritis
Elderly
Dose(mg) 1. 500 mg 27. 200 51. 500 75. 500 99. 200
f 2. 0.95 28. 0.95 52. 0.95 76. 0.95 100. 0.95
fu 3. 0.02 29. 0.02 53. 0.06 77. 0.03 101. 0.04
Vd (L) 4. 10 30. 10 54. 31.67 78. 13 102. 10
k (hr-1) 5. 0.0533 31. 0.0182 55. 0.0495 79. 0.061 103. 0.533
T 1/2 (hr) 6. 13 32. 38.1 56. 14 80. 11.3 104. 13
AUC (mg/L*hr) 7. 891 33. 1044 57. 303 81. 595 105. 356
% 8. 99 34. 97 58. 99.97 82. 99 106. 99
% 9. 1 35. 3 59. 0.03 83. 1 107. 1
(L/hr) 10. 0.533 36. 0.182 60. 1.57 84. 0.798 108. 0.533
(L/hr) 11. 0.528 37. 0.177 61. 1.57 85. 0.790 109. 0.528
(L/hr) 12. 0.005 38. 0.005 62. 0.005 86. 0.008 110. 0.005
13. 0.005
14. 0.000067
(L/hr) 15. 26.5 39. 8.84 63. 26.5 87. 26.5 111. 13.26
(L/hr) 16. 0.267 40. 0.267 64. 0.00889 88. 0.267 112. 0.133
17. 1 41. 1 65. 1 89. 1 113. 1
18. 1 42. 0.333 66. 3 90. 1.5 114. 1
19. 1 43. 1 67. 1 91. 1 115. 1
20. 1 44. 1 68. 0.1 92. 1.5 116. 1
FCL 21. 1 45. 0.341 69. 2.94 93. 1.5 117. 1
(hr) 22. 12 46. 12 70. 12 94. 12 118. 8
Clh
Clr
Cltot
Clh
Clr
Eh
Er
Clhint
Clr int
FRh
FIh
FRr
FIr
τ
Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-37Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
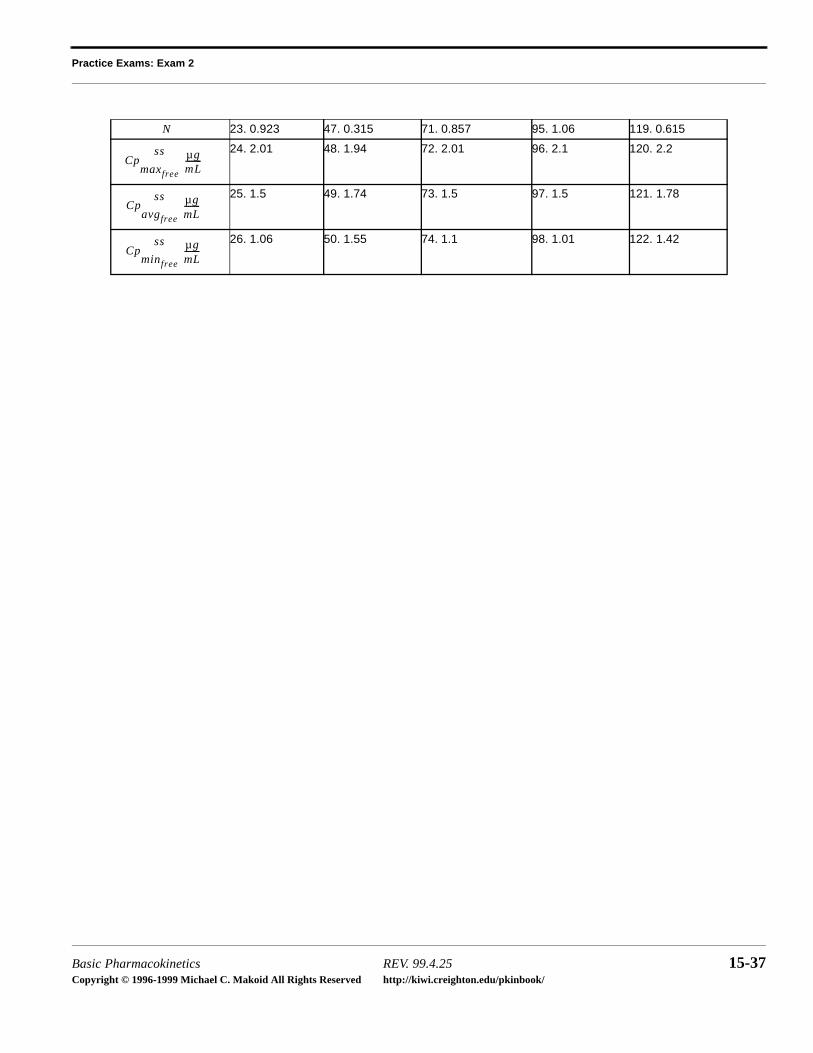
N 23. 0.923 47. 0.315 71. 0.857 95. 1.06 119. 0.615
24. 2.01 48. 1.94 72. 2.01 96. 2.1 120. 2.2
25. 1.5 49. 1.74 73. 1.5 97. 1.5 121. 1.78
26. 1.06 50. 1.55 74. 1.1 98. 1.01 122. 1.42
Cpss
maxfree
µgmL--------
Cpss
avgfree
µgmL--------
Cpss
minfree
µgmL--------
Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-38Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
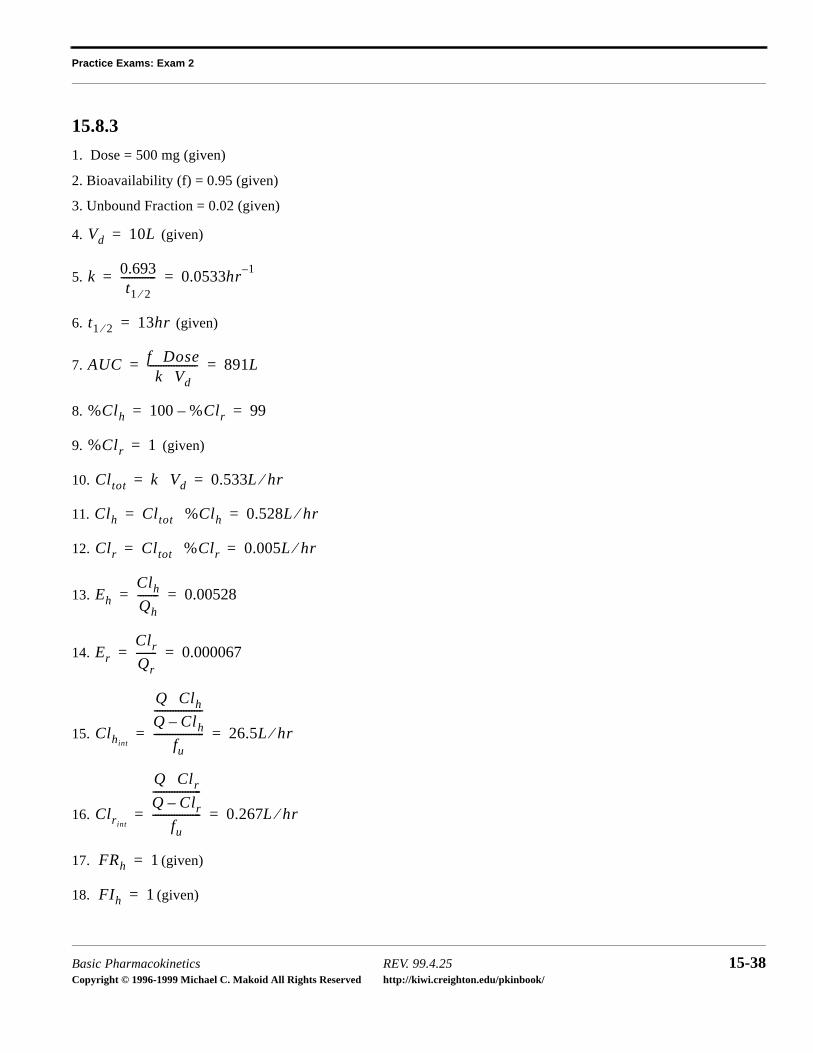
15.8.3
1. Dose = 500 mg (given)
2. Bioavailability (f) = 0.95 (given)
3. Unbound Fraction = 0.02 (given)
4. (given)
5.
6. (given)
7.
8.
9. (given)
10.
11.
12.
13.
14.
15.
16.
17. (given)
18. (given)
Vd 10L=
k 0.693t1 2⁄
------------- 0.0533hr1–
= =
t1 2⁄ 13hr=
AUC f Dose⋅k Vd⋅
------------------- 891L= =
%Clh 100 %Clr– 99= =
%Clr 1=
Cltot k Vd⋅ 0.533L hr⁄= =
Clh Cltot %Clh⋅ 0.528L hr⁄= =
Clr Cltot %Clr⋅ 0.005L hr⁄= =
Eh
Clh
Qh
-------- 0.00528= =
Er
Clr
Qr
-------- 0.000067= =
Clhint
Q Clh⋅Q Clh–------------------
fu
------------------- 26.5L hr⁄= =
Clrint
Q Clr⋅Q Clr–------------------
fu
------------------ 0.267L hr⁄= =
FRh 1=
FIh 1=

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-39Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
19. (given)
20. (given)
21. (given)
22. (given)
23.
24.
25.
26.
27. Dose = mg
28. Bioavailability (f) = 0.95 (no change)
29. Unbound Fraction = 0.02 (no change - given)
30. (given)
31.
32. (given)
33.
34.
35. (given)
36.
37.
FRr 1=
FIr 1=
FCl 1=
τ 12hr=
N τt1 2⁄--------- 0.923= =
Cpss
maxfree
fu S f D⋅ ⋅ ⋅V
-------------------------- 1
1 12---
N–
--------------------⋅ 2.0 µgmL--------= =
Cpss
avgfree
fu S f D⋅ ⋅ ⋅V K τ⋅ ⋅
--------------------------fu S f D⋅ ⋅ ⋅
V 0.693 N⋅ ⋅------------------------------= 1.5 µg
mL--------= =
Cpss
minfree
fu S f D⋅ ⋅ ⋅V
--------------------------
12---
N
1 12---
N–
--------------------⋅ 1.1 µgmL--------= =
Vd 10L=
k 0.693t1 2⁄
------------- 0.0533hr1–
= =
t1 2⁄ 13hr=
AUC f Dose⋅k Vd⋅
------------------- 891L= =
%Clh 100 %Clr– 99= =
%Clr 1=
Cltot k Vd⋅ 0.533L hr⁄= =
Clh Cltot %Clh⋅ 0.528L hr⁄= =

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-40Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
38.
39.
40.
41. (given)
42. (given)
43. (given)
44. (given)
45. (given)
46. (given)
47.
48.
49.
50.
51. Dose = mg
52. Bioavailability (f) = 0.95 (no change)
53. Unbound Fraction = 0.02 (no change - given)
54. (given)
Clr Cltot %Clr⋅ 0.005L hr⁄= =
Clhint
Q Clh⋅Q Clh–------------------
fu
------------------- 26.5L hr⁄= =
Clrint
Q Clr⋅Q Clr–------------------
fu
------------------ 0.267L hr⁄= =
FRh 1=
FIh 1=
FRr 1=
FIr 1=
FCl 1=
τ 12hr=
N τt1 2⁄--------- 0.923= =
Cpss
maxfree
fu S f D⋅ ⋅ ⋅V
-------------------------- 1
1 12---
N–
--------------------⋅ 2.0 µgmL--------= =
Cpss
avgfree
fu S f D⋅ ⋅ ⋅V K τ⋅ ⋅
--------------------------fu S f D⋅ ⋅ ⋅
V 0.693 N⋅ ⋅------------------------------= 1.5 µg
mL--------= =
Cpss
minfree
fu S f D⋅ ⋅ ⋅V
--------------------------
12---
N
1 12---
N–
--------------------⋅ 1.1 µgmL--------= =
Vd 10L=

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-41Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
55.
56. (given)
57.
58.
59. (given)
60.
61.
62.
63.
64.
65. (given)
66. (given)
67. (given)
68. (given)
69. (given)
70. (given)
71.
72.
k 0.693t1 2⁄
------------- 0.0533hr1–
= =
t1 2⁄ 13hr=
AUC f Dose⋅k Vd⋅
------------------- 891L= =
%Clh 100 %Clr– 99= =
%Clr 1=
Cltot k Vd⋅ 0.533L hr⁄= =
Clh Cltot %Clh⋅ 0.528L hr⁄= =
Clr Cltot %Clr⋅ 0.005L hr⁄= =
Clhint
Q Clh⋅Q Clh–------------------
fu
------------------- 26.5L hr⁄= =
Clrint
Q Clr⋅Q Clr–------------------
fu
------------------ 0.267L hr⁄= =
FRh 1=
FIh 1=
FRr 1=
FIr 1=
FCl 1=
τ 12hr=
N τt1 2⁄--------- 0.923= =
Cpss
maxfree
fu S f D⋅ ⋅ ⋅V
-------------------------- 1
1 12---
N–
--------------------⋅ 2.0 µgmL--------= =

Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-42Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
73.
74.
75. Dose = mg
76. Bioavailability (f) = 0.95 (no change)
77. Unbound Fraction = 0.02 (no change - given)
78. (given)
79.
80. (given)
81.
82.
83. (given)
84.
85.
86.
87.
88.
89. (given)
90. (given)
Cpss
avgfree
fu S f D⋅ ⋅ ⋅V K τ⋅ ⋅
--------------------------fu S f D⋅ ⋅ ⋅
V 0.693 N⋅ ⋅------------------------------= 1.5 µg
mL--------= =
Cpss
minfree
fu S f D⋅ ⋅ ⋅V
--------------------------
12---
N
1 12---
N–
--------------------⋅ 1.1 µgmL--------= =
Vd 10L=
k 0.693t1 2⁄
------------- 0.0533hr1–
= =
t1 2⁄ 13hr=
AUC f Dose⋅k Vd⋅
------------------- 891L= =
%Clh 100 %Clr– 99= =
%Clr 1=
Cltot k Vd⋅ 0.533L hr⁄= =
Clh Cltot %Clh⋅ 0.528L hr⁄= =
Clr Cltot %Clr⋅ 0.005L hr⁄= =
Clhint
Q Clh⋅Q Clh–------------------
fu
------------------- 26.5L hr⁄= =
Clrint
Q Clr⋅Q Clr–------------------
fu
------------------ 0.267L hr⁄= =
FRh 1=
FIh 1=
Practice Exams: Exam 2
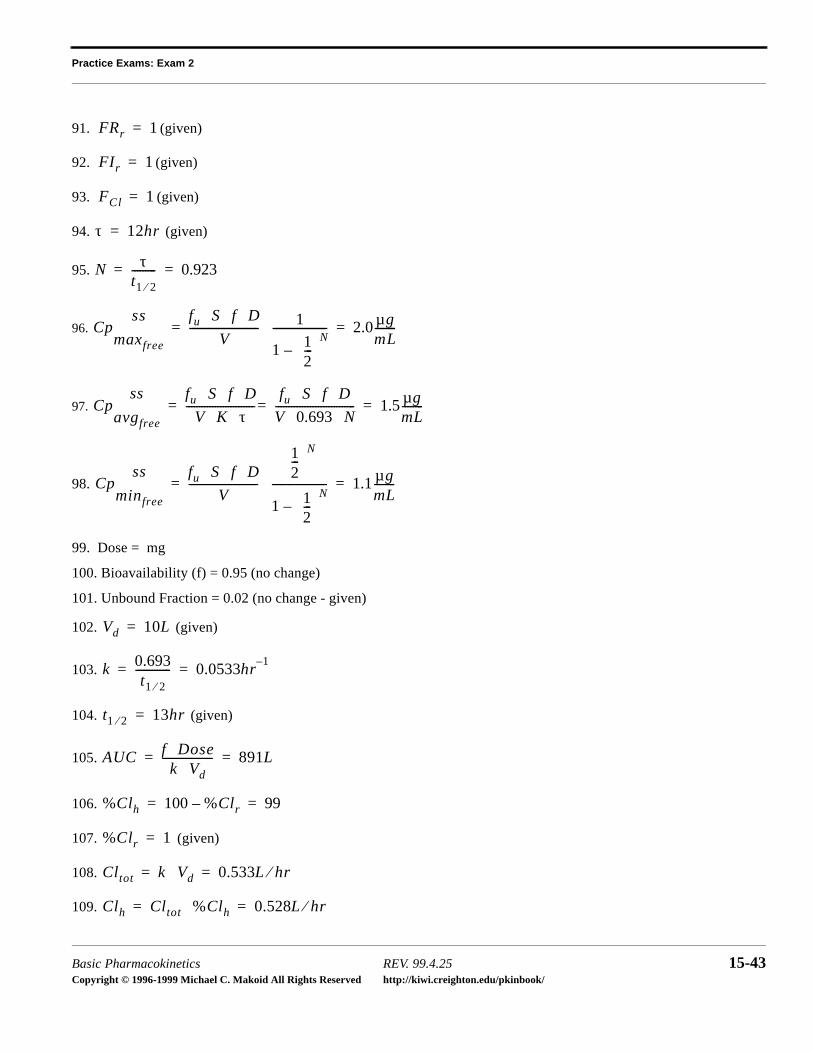
Basic Pharmacokinetics REV. 99.4.25 15-43Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
91. (given)
92. (given)
93. (given)
94. (given)
95.
96.
97.
98.
99. Dose = mg
100. Bioavailability (f) = 0.95 (no change)
101. Unbound Fraction = 0.02 (no change - given)
102. (given)
103.
104. (given)
105.
106.
107. (given)
108.
109.
FRr 1=
FIr 1=
FCl 1=
τ 12hr=
N τt1 2⁄--------- 0.923= =
Cpss
maxfree
fu S f D⋅ ⋅ ⋅V
-------------------------- 1
1 12---
N–
--------------------⋅ 2.0 µgmL--------= =
Cpss
avgfree
fu S f D⋅ ⋅ ⋅V K τ⋅ ⋅
--------------------------fu S f D⋅ ⋅ ⋅
V 0.693 N⋅ ⋅------------------------------= 1.5 µg
mL--------= =
Cpss
minfree
fu S f D⋅ ⋅ ⋅V
--------------------------
12---
N
1 12---
N–
--------------------⋅ 1.1 µgmL--------= =
Vd 10L=
k 0.693t1 2⁄
------------- 0.0533hr1–
= =
t1 2⁄ 13hr=
AUC f Dose⋅k Vd⋅
------------------- 891L= =
%Clh 100 %Clr– 99= =
%Clr 1=
Cltot k Vd⋅ 0.533L hr⁄= =
Clh Cltot %Clh⋅ 0.528L hr⁄= =
Practice Exams: Exam 2
Basic Pharmacokinetics REV. 99.4.25 15-44Copyright © 1996-1999 Michael C. Makoid All Rights Reserved http://kiwi.creighton.edu/pkinbook/
110.
111.
112.
113. (given)
114. (given)
115. (given)
116. (given)
117. (given)
118. (given)
119.
120.
121.
122.
Clr Cltot %Clr⋅ 0.005L hr⁄= =
Clh int
Q Clh⋅Q Clh–------------------
fu
------------------- 26.5L hr⁄= =
Clrint
Q Clr⋅Q Clr–------------------
fu
------------------ 0.267L hr⁄= =
FRh 1=
FIh 1=
FRr 1=
FIr 1=
FCl 1=
τ 12hr=
N τt1 2⁄--------- 0.923= =
Cpss
maxfree
fu S f D⋅ ⋅ ⋅V
-------------------------- 1
1 12---
N–
--------------------⋅ 2.0 µgmL--------= =
Cpss
avgfree
fu S f D⋅ ⋅ ⋅V K τ⋅ ⋅
--------------------------fu S f D⋅ ⋅ ⋅
V 0.693 N⋅ ⋅------------------------------= 1.5 µg
mL--------= =
Cpss
minfree
fu S f D⋅ ⋅ ⋅V
--------------------------
12---
N
1 12---
N–
--------------------⋅ 1.1 µgmL--------= =





























