Embed Size (px)
Citation preview

Basic Airway Management

Review of Important Facts and Concepts:
Airway AnatomyAirway AssessmentReview basic drugs and equipment setup for
managing airway

The Pharynx

The Glottis

While this only basic, you will become an expert in airway management and expected to communicate and document in proper anatomical terms:
Definitions
• Difficult Airway– “A conventionally trained anesthetist
experiences difficulty with mask ventilation, endotracheal intubation, or both”.
• Difficult Mask Ventilation– "It is not possible for the unassisted
anesthesiologist to maintain SaO2 >90% using 100% O2 and positive pressure mask ventilation in a patient whose SaO2 was >90% before anesthetic intervention”.

Definitions
• Difficult laryngoscopy– "It is not possible to visualize any portion of the
vocal cords with conventional laryngoscopy”.
• Difficult endotracheal intubation– "Proper insertion of the endotracheal tube with
conventional laryngoscopy requires more than three attempts or more than 10 minutes."

Airway Management • 1 in 10,000 patients have an unpredicted difficult airway
– Caplan RA et al: Anesthesiology 1993; 78:597-602
• 1% of patients will have a difficult intubation– Walls RM et al: Ann Emerg Med 1999; 34: S14
• Risk of difficult intubation in general population is 1 in 2400
• Prospective evaluation of the airway SHOULD BE DONE systematically in every patient before they become apneic

Principles in Evaluating the Upper Airway: “Concept 1)—look for things that correlate with difficult mask ventilation”“Concept 2)—this can be done in seconds
1. Size of Tongue versus Pharynx– Mallampati classification
2. Facial features that can directly compromise mask seal
– Beard, edentulous
3. Neck features associated with difficult mass ventilation
– Thyromental distance, large neck, laryngeal tongue

Understanding Upper Airway Obstruction—”cork in the bottle”

1. Size of Tongue vs Pharynx“Mallampati Classification”
Concept: Patient’s with a Class 3-4 airway have a relatively large tongue relative to the volume of their pharynx which can lead to difficulty performing positive pressure ventilation.

2. Facial features:Concept: Be wary of facial features in sedation candidates that could
make trying to obtain a mask seal very difficult (they all leak).
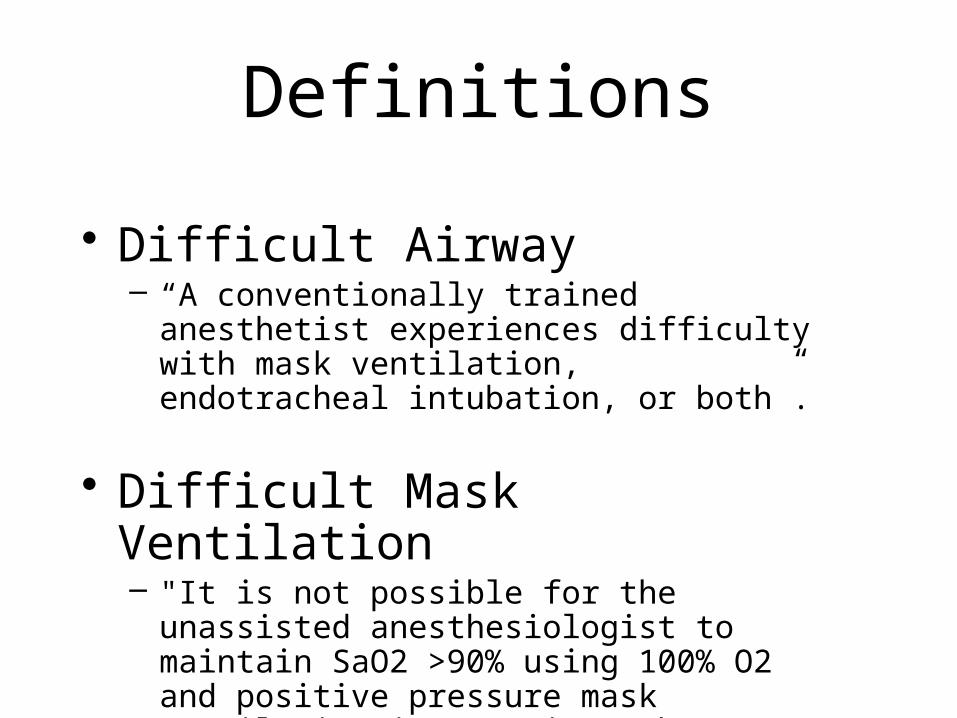
3. ↓ Anterior Mandibular Space& Large Neck
Concept: “neck features that in the presence of sedation, relaxed airway, recumbent position: a) place a patient at higher risk for obstruction and b) that if needed, could make positive pressure ventilation difficult”.

Predictors of Difficult Mask Ventilation: Summary—watch out!
• High Mallampatti score• Beard• Large neck• BMI > 26 kg/m2
• History of Snoring (??OSA)• Edentulous
Assessing for Intubation
Preoperative Evaluation of the Upper Airway for signs of difficulty with intubation:
1. Size of Tongue versus Pharynx– Mallampati classification
2. Atlanto-Occipital Joint Extension– Cervical spine mobility
3. Anterior Mandibular Space– Thyromental distance
4. Dental Examination

Size of Tongue vs Pharynx
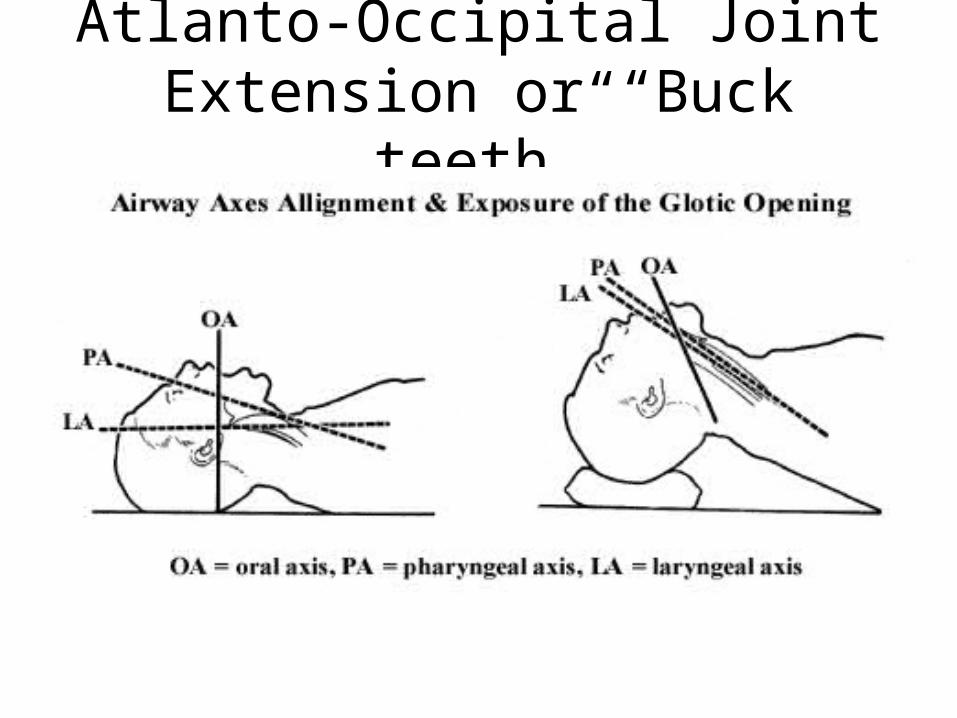
Atlanto-Occipital Joint Extension or “Buck teeth”

Anterior Mandibular Space(Thyromental distance)

Dental Examination
• Ascertain the presence of– Loose teeth– Dental Prostheses– Co-existing dental abnormalities

PREOP EXAM ACCEPTABLE ENDPOINTS SIGNIFICANCE OF ENDPOINTS
1. Length of upper incisors Qualitative/short incisors Long incisors-blade enters mouth in cephalad direction
2. Involuntary: Maxillary teeth anterior to mandibular teeth
No overriding of maxillary teeth ant. to the mandib. teeth
Overriding maxillary teeth-Blade enters mouth in a more cephalid direction.
3. Voluntary: Protrusion of mandibular teeth anterior to the maxillary teeth
Anterior protrusion of the mandibular teeth relative to the maxillary teeth
Test of TMJ function ; means good mouth opening and jaw will move anteriorly with laryngoscopy.
4. Intercisor distance > 3 cm 2-cm phlange on blade can be easily inserted between teeth.
5. Oropharyngeal class (Mallampatti exam)
< Class II Tongue is small in relation to size of oropharyngael cavity.
6. Narrowness of palate Should not appear very narrow and/or highly arched
A narrow palate decreases the oropharyngeal volume and room for both blade and ETT.
7. Mandibular space length (Thyromental Distance)
= 5 cm or = 3 ordinary - sized fingerbreadths
Larynx is relatively to other upper airway structures.
8. Mandibular space (MS) compliance Qualitative palpation of normal resilience / softness
Laryngoscopy retracts tongue into the MS. Compliance of the MS determines if tongue fits into MS.
9. Length of neck Qualitative. A quantitative index is not available.
A short neck decreases the ability to align the upper airway axes.
10. Thickness of neck Qualitative. A quantitative index is not available.
A thick neck decreases the ability to align the upper airway axes.
11. Palpation of cricoid membrane Cricoid membrane can be readily identified.
If the cricoid membrane can not be palpated readily, then the ability to perform TTJV or establish a surgical airway are not available as options in an emergency.
12. Cervical range of motion Neck flexed on chest 35 degrees + head extended on neck 35 degrees = sniff position
The sniff position aligns the oral, pharyngeal and laryngeal axes to create a favorable line of sight.

Basic Setup for intubation:
• Equipment & tubes• Drugs• Airway Emergency equipment (readily
accessible)

Equipment
1. Laryngoscope handle
2. 3 MAC blade
3. 3 Miller blade
4. 4 MAC blade
5. 6.0, 7.0, 8.0 Endotracheal Tube with stylets
6. 10cc syringe
7. Tongue blade
8. Oral/Nasal airways
9. Suction available

Drugs for airway management1. Atropine - 1 x 10cc syringe
2. Ephedrine - 1 x 10cc syringe
3. Epinephrine - 1 x 10cc syringe
4. Fentanyl - 1 x 5cc syringe
5. Lidocaine - 1 x 10cc syringe
6. Nitroglycerin - 1 x 10cc syringe
7. Propofol- 1 x 20cc syringe (2nd dose immediately available!)
8. Phenylephrine - 1 x 10cc syringe
9. Rocuronium - 1 x 5cc syringe
10. Succinylcholine - 1 x 10cc syringe (2nd dose immediately available!)

Airway Emergency equipment (readily accessible)
• Bougie (great for anterior view)• BMV (backup for machine failure)• A supraglottic airway device (LMA & or
FTLMA, range of sizes)• A subglottic technique—TTJV (hand jet
vent & 14G jelco)• Know how to quickly get help if needed
(charge person, attending pager & cell#)

Adequate Pre-oxygenation
• Purpose of pre-oxygenation– Provide the patient with maximum available
oxygen store (for “denitrogenation”)– A fully denitrogenated subject with normal lungs
can tolerate apnea for up to 8 minutes before they desaturate below 90%
– Give yourself good time to intubate

Why Pre-oxygenate?
• Discuss two methods for pre-oxygenation (3 breaths vs 5 min.)
• What can you do if the patient is claustrophobic?

Notes:
• While this is a “basic” course in airway management, you will receive training in an additional two courses covering a) difficult airway management and b) FOB