Embed Size (px)
Citation preview

Official Journal of
Association for the Study of Liver Diseases Bangladesh(National Association of Hepatologists of Bangladesh)
ASSOCIATION FOR THESTUDY OF LIVER
DISEASESBANGLADESH
Volume 3 Naumber 1 March 2016 ISSN 2071-2324
BANGLADESH Jounrnal of
HEPATOLOGY


Bangladesh Journal of Hepatology
Vol. 3 No. 1 01
Room # 506, 4th floorBlock # D
Bangabandhu Sheikh Mujib Medical UniversityShahbag, Dhaka-1000
Email: [email protected], [email protected]
Bangladesh Journal of HepatologyOfficial Journal of
Association for the Study of Liver Diseases Bangladesh(National body of Hepatologists of Bangladesh)
Correspondence

02
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Bangladesh Journal of HepatologyEditorial Board
Editor in Chief Professor Salimur Rahman
Associate Editor Dr. Ayub Al Mamun Dr. Chitto Ranjan Debnath Dr. Faroque Ahmed Dr. K. M. J. Zaki Dr. Mamun-Al-Mahtab Dr. Md. Jasmshed Alam Khan
Assistant Editor Dr. Harun Or Rashid Dr. Md. Fazal Karim Dr. Md. Izazul Haque Dr. Muhammad Mahbub Hossain
Editorial Board Dr. Abu Saleh Md. Sadequl Islam Dr. Abul Barkat Muhammad Adnan Dr. Ahmed Lutful Moben Dr. Amalendu Bhattacharyya Dr. Arun Jyoti Tarafder Dr. Forhad Hossain Md. Shahed Dr. Golam Mashud Dr. Kutub Uddin Mollick Dr. Md. Abdur Rahim Dr. Md. Ashraful Alam Dr. Md. Dalil Uddin Dr. Md. Jahangir Alam Sarker Dr. Md. Zia Hayder Bosunia Dr. Mohammad Faiz Ahmad Khondaker Dr. Provat Kumar Podder Dr. Shamsul Kabir Dr. Sheikh Mohammad Noor-E-Alam Dr. Syed Abul Foez

Bangladesh Journal of Hepatology
Vol. 3 No. 1 03
Volume 3 Number 1
ContentEditorial Page
Original Articles
Review Articles
Causes of jaundice in clinical practice: An observation at BrahmanbariaForhad Hossain Mohammad Shahed, Mamun Al Mahtab, Mohammad Fakhrul Islam Khaled, Mohammad Abul Fayaz, Ashiqur Rahman Khan
Prevalence of Hepatitis B and Hepatitis C in Rural Population of BangladeshMohammad Izazul Hoque, Mohammad Belalul Islam, Mostafa Kamal Azad
Socio-demographic profile of non alcoholic fatty liver disease of 100 patients attended SBMCH BarisalGolam Mashud, Jamsed Alom, Swapon Kumar Sarkar, Anwar Hossain, Amolendu Bhattacharia, Al Mamun Hossain
Upper gastrointestinal endoscopic findings in adults at Comilla Medical College & Hospital, BangladeshMohammad Forhad Abedin, Mohammad Asaduzzaman Lashkar, Mohammad Shah Jamal, Mohammad Belalul Islam, Mohammad Izazul Haque, Mohammad Abdur Rob Sarkar
Bangladesh Journal of Hepatology: Blown in the winds of heterogeneity and pluralitySheikh Mohammad Fazle Akbar, Mamun Al Mahtab
Hepatic hydrothorax: Challenge for HepatologistSyed Abul Foez, Mohammad Abdur Rahim, Sheikh Mohammad Noor-E-Alam, Mohammad Ashraful Alam, AKM Shoab, Swapan Kumar Singha, Joy Vargese, Chandan Kumar, Mamun-Al-Mahtab, Salimur Rahman, Ziaur Rahman Chowdhury
Brief Review
Current strategies in the management of hepatocellular carcinomaPremashish Kar
Case Reports
A case of occult hepatitis B virus infection and hepatocellular carcinoma from Bangladesh Ponkaj Kumar Naha, Mamun-Al-Mahtab, Sarkar Mohammad Shahadat Hossain, Rokshana Begum, Abul Hayet Manik, Debraj Malakar, Partho Pratic Roy, Ayub Al Mamun, Salimur Rahman
07
10
15
20
25
31
34
05

04
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Abstracts of LIVERCON 2016
Association of portal vein tumor thrombus in hepatitis B related hepatocellular carcinomaAbu Saleh Mohammad Sadequl Islam, Mamun Al Mahtab, Ayub Al Mamun, Sheikh Mohammad Fazle Akbar, Mohammad Kamal Hossain, Zia Hayder Bosunia, Salimur Rahman
Metabolic syndrome is a good predictor for diagnosing non-alcoholic steatohepatitis.Sheikh Mohammad Noor-E-Alam, Ahmed Lutful Moben, Zia Hayder Basunia, Amalendu Bhattacharyya, Abdur Rahim, Syed Abul Foez, Mohammad Shahed Ashraf, Faiz Ahmad Khandoker, Md. Jahangir Alam Sarker, Abu Saleh Mohammad Sadequl Islam, Mohammad Forhad Abedin, Utpal Das Gupta, Mohammad Jahangir Kabir, Mamun-Al-Mahtab, Salimur Rahman
Upper gastrointestinal endoscopic findings in adults at Comilla Medical College & Hospital, BangladeshMohammad Forhad Abedin, Mohammad Asaduzzaman Lashkar, Mohammad Shah Jamal, Mohammad Belalul Islam, Mohammad Izazul Haque, Mohammad Abdur Rob Sarkar
Causes of jaundice in clinical practice: An observation at BrahmanbariaForhad Hossain Mohammad Shahed, Mamun Al Mahtab, Mohammad Fakhrul Islam Khaled, Mohammad Abul Fayaz, Ashiqur Rahman Khan
Non favorable genotype is predominant at IL28B rs12979860 polymorphism in hepatitis B related hepatocellular carcinomaAbu Saleh Mohammad Sadequl Islam, Mamun Al Mahtab, Ayub Al Mamun, Sheikh Mohammad Fazle Akbar, Mohammad Eunus Ali, Zia Hayder Bosunia, Salimur Rahman
Life Sketch of Professor Baruch Samuel Blumberg
Email from Professor Baruch Samuel Blumberg
Brief Introduction of Dr. Nagaraja Rao Padaki: Blumberg Orator 2016
List of Blumberg Orators
36
37
38
39
40
41
43
44
45

Bangladesh Journal of Hepatology
Vol. 3 No. 1 05
Editorial
Bangladesh Journal of Hepatology: Blown in the winds of heterogeneity and plurality
Sheikh Mohammad Fazle Akbar1, Mamun Al Mahtab2
1Department of Medical Sciences, Toshiba General Hospital, Tokyo, Japan, 2Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
Correspondence toDr. Sheikh Mohammad Fazle Akbar
Principal Investigator, Department of Medical Sciences, Toshiba General Hospital, Tokyo, Japan.Email <[email protected]>
Transmission of knowledge, acceptance of new and novel ideas and discarding false but tempting concepts constitute the backbone of social and scientific developments of modern-day society. This is especially relevant in the context of liver and its pathologies as more than one halves of world population represent the causality of different hepatotrophic viruses that infects the liver, disrupt its microenvironments, and induce long-term complications like the deadly term of liver cirrhosis and liver cancer. The impacts and implications of these diseases are more pronounced in developing countries, like Bangladesh with limited resources. The primary responsibility of tackling liver and its diseases in Bangladesh has been shouldered by Association for the Study of Liver Diseases Bangladesh (ASLDB) with the assistance of its members and patrons. However, another major responsibility remains regarding the means of transmitting evolving knowledges about liver diseases to the members of ASLDB and also to other allied physicians and medical service delivery personnel. This noble responsibility has mainly been accomplished by a publication named “Bangladesh Journal of Hepatology”.
Bangladesh Journal of Hepatology has dedicated its presence to compile the specific features of liver diseases in Bangladesh. In addition, it has been acting as a bridge to connect knowledge and information
about liver and allied disciplines of the world and Asia-Pacific region with Bangladesh; thus it is acting as media to translate all new information palatable to Bangladeshi hepatologists and physicians of multidisciplinary positions. A journal is judged by its longevity and also persistent improvement of its qualitative inceptions. Bangladesh Journal of Hepatology has entered the stage of adolescence after crossing the steps of new born, infant and child. The future is waiting to accept it as an “ADULT” in the world of modern publication.
The uninterrupted publication of this journal has been possible due enormous efforts of its leadership because most of the journal of developing countries undergo spontaneous apoptosis soon after their sailings. Now, it is the time to make qualitative improvement of the journal in global perspective. Various clinical researches and case-control studies have been accomplished in Bangladesh. Also, new and novel therapeutic approaches have been tested in Bangladesh in last one decade. ASLDB is also credited for being the sole sponsor of Single Topic Conference of The Asian Pacific Association for the Study of the Liver (APASL) in 2012, an act that has not been accomplished in most of the countries of Asia with better economical capabilities. Now, it is time for ASLDB to assess and act to induce qualitative improvement of their inherent heart,

06
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Bangladesh Journal of Hepatology. Although the ensuing task is not an easy one, but ASLDB is capable of taking this challenge to move forward.
At present, the hepatologists have been facing a major challenge about treatment of HCV infection as drugs with potent capacities are now present in market. However, both aspirations and confusions have been prevailing about these drugs. In Bangladesh, the drugs are cheap and concerns remain if these are efficacious or not? Bangladesh Journal of Hepatology may devote its endeavor to make critical analysis about the effectivity these drugs, especially the content and
quality of generic drugs for HCV infection in a scientifically-amicable manner. This will boost the medical service delivery system of Bangladesh in the context of management of HCV and these approaches may reflect the future activities of ASLDB and its journal to move forward with other such medications.
Editors with leadership capabilities, an editorial board of multidisciplinary specialties and an innovative vision of the ASLDB would make it possible to place Bangladesh Liver Journal to its proper position in the field of medical journal.

Bangladesh Journal of Hepatology
Vol. 3 No. 1 07
Original Articles
Abstract
Causes of jaundice in clinical practice: An observation at Brahmanbaria
Forhad Hossain Mohammad Shahed1, Mamun Al Mahtab2, Mohammad Fakhrul Islam Khaled1, Mohammad Abul Fayaz1, Ashiqur Rahman Khan1
1250 Bedded District Sadar Hospital, Brahminbaria, Bangladesh 2Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
Corresponding authorDr. Forhad Hossain Mohammad Shahed
Senior Consultant (Medicine)250 Bedded District Sadar Hospital, Brahminbaria, Bangladesh. Email: <[email protected]>
Background: Jaundice remains the commonest mode of presentation of liver disease. Identification of the cause at first medical contact is the basis of starting treatment. There is scarcity of study elaborating the common causes of jaundice in Bangladeshi people. We evaluated 100 patients presenting with jaundice at Brahmanbaria, a district of Bangladesh to know aetiologies.
Methods: We performed this observational study on Patients attending with the complaint of jaundice to the private chamber of the only hepatologist at this district from January 2015 to September 2015. Data from 100 patients were collected and analyzed to know cause of jaundice and its relation with age & sex of these patients.
Results: Mean±SD of age of the patients was 28.24±21.57, 57.6% were male. In 73% cases the cause was infectious, with hepatitis B virus (HBV) 44%, hepatitis C virus (HCV) 30%, hepatitis A virus (HAV) 30%, hepatitis E virus (HEV) 26%. Mean±SD of age was 19.7±2.7 in infectious group. Alcoholic liver disease was in 5% cases. Obstruction with gall stone was in 5% cases, Carcinoma of gall bladder (CaGB) in 5%, cholangiocarcinoma in 3%, Carcinoma liver in 1.6% and Carcinoma pancreas in 11.8% cases. Among the CaGB & cholangiocarcinoma patients 16% had gall stone. Mean±SD of age in malignant patients was 62.52±4.9 with 75% female.
Conclusion: We observed that viral hepatitis was common in younger age and malignancy in older age. Most of the study subjects were male whereas malignancy was more common in female. HAV infection was more in pediatric age. Majority of hepatits were HBV related. Among the patients with CaGB & cholangiocarcinoma 16% had gall stone.
Background:
Bangladesh is a densely populated country. Liver disease is the third leading cause of death in tertiary level hospital of this country [1]. Jaundice remains the commonest mode of presentation. Identification of the cause at first medical contact is the basis of starting treatment. There is scarcity of study elaborating the common causes of jaundice in Bangladeshi people. In this study we evaluated 100 patients at Brahmanbaria, a district of Bangladesh to know aetiologies.
Methods:
Patients attending to the private chamber of the only
hepatologist at Brahmanbaria district from January to September 2015 with the complaint of jaundice were enrolled in this study. All patients were investigated to know the cause and status of liver. Viral markers were tested by ELISA, Sonographic evaluation was done by ultrasonography machine. Demographic profiles and the laboratory data were recorded in pre-formed data sheet. Data were analyzed to detect the relative frequencies of causes of jaundice and there relation with age and sex. Analysis was done by MS Excel software.

08
Bangladesh Journal of Hepatology
Vol. 3 No. 1
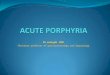
Fig. 1: Age distribution of patients
Table I: Causes of jaundice in different age group.
Results:
Patients presented with the complaint of jaundice were screened and total 100 patients were taken for
analysis. Mean±SD of age of the patients was 28.24±21.57, 57.6% were male. 80 % patients are in 0-45 year age group.
In 76% cases causes were infectious, with HBV 44%, HCV 30%, HAV 30%, HEV 26%. Mean±SD of age was 19.7±2.7 in infectious group. Alcoholic liver disease was in 6% cases. Obstruction with gall stone was in 5% cases, CaGB in 5%, cholangiocarcinoma in 3%, Ca liver in 1.6% and Ca pancreas in 11.8% cases. Among the CaGB & cholangiocarcinoma patients 16% had gall stone. 80% of the patients were in 0-45 years age group, of whom 90% were suffering from infectious
hepatitis. Rest 20% patients age was >45 of whom 75% were suffering from malignancy. HAV infection was the dominant cause at 0—15 years age group, HBV was common at age group 16-30 years and HEV was the second common cause at this age group. All the cases of >60years had malignancy involving hepatobilliary system. Mean±SD of age in malignant patients was 62.52±4.9 with 75% female. Sex distribution of patients is shown in the table II.
27
34
19
119
0
5
10
15
20
25
30
35
40
0--15 16--30 31--45 46--60 >60
% of Patients
% of Patients
Age of patient
Frequencies of different causes of jaundice and their relation with age and sex are shown in table I.
Age group (Years)
No. of patient N=100
HBV (%)
HAV (%)
HCV (%)
HEV (%)
Gall stone (%)
Alcoholic Liver disease (%)
Ca GB (%)
Ca pancreas (%)
HB MA with H/O Gall stone (%)
0—15 27 4 20 3 16—30 34 18 14 2 31—45 19 9 4 2 4 2 46—60 11 2 2 3 2 2 2 >60 9 5 4 5

Bangladesh Journal of Hepatology
Vol. 3 No. 1 09
Table II: Sex distribution of patients.
Discussion:
In this study, it was observed that age of most of the patients presenting with jaundice was less than 45years. Majority of the patients at this age were male. Hepatotrophic viral infections were the most common causes in patients below 45 years age (91%). But less common in patients with >45 years age (5%). HAV infection was the dominant cause at 0—15 years age group, HBV was common at age group 16-30 years and HEV was the second common cause at this age group. This is consistent with reports at home and abroad that patients with viral hepatitis are more common in young adults [2,3] but malignancy in adults. [4,5] Female sex was dominant in patients age >45years. All patients of ages > 60 were female and all were suffering from malignancy.
Conclusion:
We performed this study in a private chamber of a hepatologist at Brahmanbaria district to find the causes of jaundice in clinical practice. It was found that hepatitis was the dominant cause at younger age ad malignancy in elderly. HAV infection was most common cause for childhood jaundice and others were HEV, HBV & HCV. This finding may help the clinician for diagnosis of cause of jaundice in out-patient service. Further large scale study in different part of Bangladesh is needed to
Age group No. of patient N=100
Sex Male Female
P value
0—15 27 16 11 0.03 6—30 34 25 09 0.001 31—45 19 13 13 1.3 46—60 11 5 06 0.9 >60 9 0 09 0.001
find the prevalence of different causes of jaundice in this country.
Reference:
1. Abedin MF, Hoque MM, Islam ASMSM, Chowdhury MFI, Das DC, Begum SA, Mamun AA, Mahtab MA, Rahman S, Saha AK. Chronic liver disease is one of the leading causes of death in Bangladesh, experience by death audit from a tertiary hospital. Euroasian J hepato-Gastroenterology, 2014; 4(1):17-20
2. Jianhua Liu, Yanshan Cai, Jian Chen, et al. Analysis of Viral Hepatitis B prevalence in the natural population of Guang-zhou City, China Vaccines and Immunization, 2010,(05):438.
3. Bane A. Viral hepatitis: epidemiology, treatment, prevention. Ethiop Med J, 2008, 46(2):193.
4. Jizhou Wu, Guojian Li, Wuqing Cheng, et al. Epidemiological studies liver cancer high point in Guangxi. Internal Medicain. 2009,(05):678.
5. Qua CS, Goh KL. Liver cirrhosis in Malaysia-peculiar epide-miology in a multiracial Asian country. LID - 10.1111/j.1440-1746.2011.06732.x [doi]. J Gastroenterol Hepatol, 2011.

10
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Prevalence of Hepatitis B and Hepatitis C in Rural Population of Bangladesh
Mohammad Izazul Hoque1, Mohammad Belalul Islam2, Mostafa Kamal Azad3
1Department of Hepatology, Comilla Medical College, Comilla, Bangladesh, 2Department of Medicine, Comilla Medical College, Comilla, Bangladesh, 3Department of Radiology, Comilla Medical College, Comilla, Bangladesh,
Corresponding authorDr. Mohammad Izazul Hoque
Associate Professor and HeadDepartment of Hepatology, Comilla Medical College, Comilla, Bangladesh. E-mail: <[email protected]>
Background: Prevalence of hepatitis B and hepatitis C in Bangladesh is not well documented. Several small studies from different parts show that Bangladesh is an intermediate prevalent area and very low hepatitis C prevalence.
Methods: This cross-sectional study was carried out in two villages of Comilla district of Bangladesh. Serum samples were collected from both adult males and females and tested for HBsAg for hepatitis B and anti-HCV antibody for hepatitis C by ELISA. Prevalence rates were determined and correlated with different demographic and risk factors involved in the spread of these viruses.
Result: 505 subjects were included in this study among which 160 males (31.7%) and 345 females (68.3%) with the mean age of 42.2 ± 15.04 years. HBsAg was positive in 8 person (1.6 %), Highest prevalence of HBV was among young adults and middle-aged individuals with a male predominance. Anti HCV was positive in 2 person (0.4%). Previous history of jaundice, blood transfusion, dental procedure and intravenous drug use were the main risk factors for acquiring the hepatitis B and C viruses.
Conclusion: Prevalence of HBV was 1.6% and indicates an area of low endemicity for hepatitis B virus infection. Prevalence of HCV was 0.4% and indicates very low endemicity for hepatitis C virus infection in rural community of Bangladesh.
Abstract
Introduction:
Hepatitis B virus (HBV) continues to be a global public health problem. 350-400 million people worldwide are chronic HBV surface antigen (HBsAg) carriers. Carriers of HBV are at increased risk of developing cirrhosis, hepatic decompensation and hepatocellular carcinoma (HCC)1. Although most carriers will not develop hepatic complications from chronic hepatitis B, 15% to 40% will develop serious sequelae during their lifetime1. HBV related end stage liver disease or HCC are responsible for over 0. 5-1 million deaths per year and currently represent 5-10% of cases of liver transplantation2.
One third of world population have serological evidence of present or fast HBV infection. The global prevalence
of HBsAg varies greatly and countries can be defined as having a high, intermediate and low prevalence of HBV infection based on a prevalence of HBsAg carriers of ≥ 8%, 2-7% & <2% respectively3. High prevalence areas are Sub Saharan Africa and part of Asia-Pacific and Low prevalence areas are North America and Europe. Prevalence of hepatitis B among general population of Bangladesh not known. Different studies shows diverse result. One study4 among 1018 general population shows the prevalence of 5.5%, 1.54% health care workers were HBsAg positive in another study.5
The hepatitis C virus (HCV) is a major public health problem and a leading cause of chronic liver disease. The global prevalence of chronic hepatitis C is estimated to average 3% (ranging from 0.1%-5%in

Bangladesh Journal of Hepatology
Vol. 3 No. 1 11
Table I: Socio-demographic features of study population (n=505)
different countries)6 and the highest number of infection reported in Egypt7. In western countries HCV accounts for 20% cases of acute hepatitis, 70% cases of chronic hepatitis, 40% cases of end stage cirrhosis, 60% cases of hepatocellular carcinoma and 30% of liver transplant6.
The incidence of new symptomatic infections has been estimated to be 1-3 cases 100,000 persons annually. The actual incidence of new infections is obviously much higher as the majority cases are asymptomatic6. Intravenous drug use remains the main mode of transmission. Other modes of transmission are transfusion of blood and blood products, health care related procedure, occupational exposure, sexual transmission and vertical transmission.
Hepatitis C virus is a parenterally transmitted virus that may pose an occupational hazard to the health care workers. Epidemiological evidence suggests that health care workers are at an increased risk of Hepatitis C virus infection8, and episodes of hepatitis C virus infection after needle stick incidents9 and transmissionlh of the virus in hospitals in developed countries have also been reported10. There are very few studies from Bangladesh regarding the prevalence of HCV infection in the high risk group of health care staff working in hospitals.
This study was designed to determine the seroprevalence of HBV and HCV infection among the rural population of Bangladesh.
Methodology:
This cross-sectional study was performed in two
villages of Comilla, Bangladesh during a 12-month period in randomly selected sample of adult general population. All inhabitants older than 18 years were invited to participate. Those who agreed to take part in this study, made an appointment with the study team for history and laboratory testing. Informed written consent was taken from all the participants. Serum samples were collected from both adult males and females and tested for HBsAg for hepatitis B and anti-HCV antibody for hepatitis C by ELISA. Prevalence rates were determined and correlated with different demographic and risk factors involved in the spread of these viruses.
Statistical analyses was performed using the SPSS software, version 16.0. The prevalence of Hepatitis B and Hepatitis C was calculated as a proportion of positive HBsAg and anti HCV subjects to included subjects. The results were expressed as mean ± SD and proportions as appropriate.
Results:
505 subjects were included in this study among which were 160 males (31.7%) and 345 females (68.3%) with the mean age of 42.2 ± 15.04 years. The demographic and socioeconomic status of the participants is summarized in Table I. Most of the participants (52.5%) were categorized as mid income while 239 (47.5%) patients where categorized as low income. 34% subjects were illiterate.
Variable N % Age (in years)
• 18 – 40 • 41 – 60 • > 60 • Mean ± SD
256 195 54 42.21 ± 15.04
50.7 38.6 10.7
Gender • Male • Female
160 345
31.7 68.3

12
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Table II: Prevalence of Hepatitis B (HBsAg) (N=505)
Table III: Demographic characteristics of the HBsAg positive study population (n=8)
Table IV: Risk of exposure to HBV in the HBsAg-positive study population
Variable N % Occupation
• Farmer • House wife • Service • Day labourer • Business• Stay abroad • Student • Others
14 320 66 33 30 4 23 15
2.8 63.4 13.1 6.5 5.9 0.8 4.6 3.0
Socioeconomic condition • Low • Middle
239 264
47.5 52.5
Education • Illiterate • Primary • Secondary • Higher secondary • Graduation
171 168 100 31 33
34.0 33.4 19.9 6.2 6.6
HBsAg was positive in 8 person(1.6%), mostly in the 18-40 age group with male predominance(75%).
Previous jaundice, blood transfusion, dental procedure and intravenous drug use were the main risk factors for acquiring the HBV infection.
Test Posi t ive, n(%) Negative HBsAg 8(1.6%) 497(98.4%)
Characteris t ics N % Age distr ibut ion 18 – 40
41 – 60 >60
5 2 1
62.5 25 12.5
Sex dist r ibut ion Male Female
6 2
75 25
Socio -economic condit ion
Lower class Middle class Upper class
5 3 0
62.5 37.5 0
Risk factors N (%) H/O jaundice 3 37.5 Blood transfusion 1 12.5 Denta l procedure 1 12.5 Surgery 0 0 I/V drug abuse 1 12.5 Famil y H/O HBsAg posi t i ve 1 12.5

Bangladesh Journal of Hepatology
Vol. 3 No. 1 13
Table V: Prevalence of Hepatitis C (Anti HCV)
Test Positive, n (%) Negative n (%)
Anti -HCV 2(o.4%) 503 (99.4%)
Discussion:
HBsAg was positive in 8 persons (1.6%). This is lower than one study4 among 1018 general population which shows the prevalence of 5.5%, but nearly same as in another study where 1.54% health care workers were HBsAg positive5. In our study population the highest prevalence of HBV was among young adults and middle-aged individuals with a male predominance.
HBV prevalence in our healthy adult population appears to be on the decline. A study in 1984 reported HBV prevalence in healthy Bangladeshi adults to be 7.2%.11 A similar figure, i.e. 7.5%, was revealed by another study carried out among healthy adult job seekers in 1996.12 The figure has dropped to 1.6%, as revealed by the present study. Several factors may have played a role, including introduction of HBV vaccination in the Expanded Programme of Immunization schedule and equally importantly, public awareness, media-physician partnership, health and family screening, mandatory screening of blood and blood products before donation, after which vaccination of negative individuals against HBV has become a popular exercise.
In a healthy adult Indian population, the prevalence of HBV varies between 2% and 8%, being higher in South than in North and West India.13 The HBV carrier pool in India is estimated at approximately 40 million. From Pakistan, a study reveals HBV prevalence in healthy adults to be 10%.14 In Nepal, this prevalence varies between 0.9% and 1.6%, being higher in Kathmandu valley than in rural Nepal. Sri Lanka has a reported 1% prevalence of HBV in the healthy adult population15. This study result is similar to prevalence of HBV in Nepal and Srilonka
HBV poses a huge burden on the health of Bangladeshis, being the leading cause of all forms of chronic liver diseases (CLD). HBV is responsible for 76.3% of cases of chronic hepatitis16 and 61.15% of cases of cirrhosis.17 Things have changed very little over the years, as a Bangladeshi study in 1994 found HBV to be responsible for 40.5% of cases of CLD in the country.18 In India >60% of cases of CLD is due to
HBV.19,20 The same applies to Pakistan, where HBV is responsible for 60% of cases of CLD.21 In Nepal, 60% of cases of chronic hepatitis and 40% of cases of cirrhosis of the liver are due to HBV.22,23
Anti HCV were positive in 2 person (0.4%). pointing to a low prevalence of the virus in our study population. This is lower than one study in general population of Bangladesh where 0.88% were positive for anti-HCV24 and was similar to another study where 0.5% subjects were positive for anti-HCV25. Both of them were young male with history of intravenous drug abuse. We found none to be co-infected with HBV and HCV.
Conclusion:
Prevalence of HBV was 1.6% and indicates an area of low endemicity for hepatitis B virus infection. Previous jaundice, blood transfusion, dental procedure and intravenous drug use were the main risk factors for acquiring the HBV infection. Prevalence of HCV was 0.4% and indicates very low endemicity of hepatitis C virus infection in rural community of Bangladesh. Multicenter study with large group of people is recommended to get the real picture of prevalence of HBV and HCV infection in Bangladesh.
References:
1. McMahon B J. The natural history of chronic Hepatitis B virus infection. Semin Liver Dis 2004;24: 17-21
2. Ganem D, Prince AM. Hepatitis B virus infection – natural history and clinical consequences. N Eng J Med 2004; 350: 1118-1129
3. Lok ASF, McMahon B J. AASLD PRACTICE GUIDELINES Chronic hepatitis B: Update 2009. Hepatology 2009; 50(3):1
4. Mahtab MA,Rahman S,Karim MF, Khan M. Epidemiology of hepatitis b virus in Bangladeshi general population.Hepatobiliary pancreat dis int 2008;7(6):595-600
5. Latif MA,Hoque MI,Islam FMM. Seroprevalence HBV infection among health care workers- study in

14
Bangladesh Journal of Hepatology
Vol. 3 No. 1
a tertiary care hospital of Bangladesh. Journal of comilla medical college teachers association 2011;13(2):12-14
6. Akbar SMF, Hossain M, Hossain MF, Sarker S, Hossain SAS, Tanimoto K, Masumoto T, Michitaka K, Horiike, Onji M. Seroepidemiology of hepatitis viruses of chronic liver diseases in Bangladesh: high prevalence of HCV among blood donors and healthy persons. Hepatol Research 1997; 7: 113-120.
7. Khan M, Yano M, Hashizume K, Yousuf M, Tanaka E, Matsumoto A, et al. Comparison of seroepidemiology of hepatitis C in blood donors between Bangladesh and Japan. Gastroenterol Jpn 1993; 28(5): 28-31.
8. Zaman M. Khan M, Alam K, Williums I. Primary hepaioocellular carcinoma and viral hepatitis B and C infection in Bangladeshi subjects. J Trop Med Hyg 1995; 98: 64-68.
9. Khan M, Ahmed N, Rabtuan S, Zaki KMJ, Matin MA. Interferon therapy in chronic viral hepatitis in Bangladesh: A preliminary report. Int Hepatol Common 1995; 3 (suppl): 104.
10. Yen T, Keffe EB, Ahmed A. The epidemiology of hepatitis C virus infection. J Clin Gastroenterol 2003; 36: 47-53.
11. Islam MN, Islam KMN, Islam N. Hepatitis B virus infection in Dhaka, Bangladesh. Bangladesh Med Res Council Bull 1984;X:1-6.
12. Khan M, Ahmad N. Seroepidemiology of HBV and HCV in Bangladesh. Int Hepatol Comm 1996;5:27-29.
13. Tandon BN, Gandhi BM, Joshi YK. Etiological spectrum of viral hepatitis and prevalence of markers of hepatitis A and B virus infection in north India. Bull World Health Organ 1984;62:67-73.
14. Malik IA, Legters LJ, Luqman M, Ahmed A, Qamar MA, Akhtar KA, et al. The serological markers of hepatitis A and B in healthy population in northern Pakistan. J Pak Med Assoc 1988;38:69-72.
15. Shrestha SM. Seroepidemiology of Hepatitis B in Nepal. J Com dis 1990;22:27-32.
16. Mahtab MA, Rahman S, Khan M, Kamal M, Karim MF, Ahmed F, et al. Aetiology of chronic hepatitis: Experience from a tertiary centre in Bangladesh. Indian JGastroenterol 2007;26(supple 2):142.
17. Afroz S, Mahtab MA, Rahman S, Khan M. Hepatitis B virus is the leading cause of cirrhosis of liver in Bangladesh. Hepatol Int 2007;1:120.
18. Khan M, Kiyosawa K, Yano M. HCV seroprevalence in liver disease in Bangladesh. IXth Biennial Scientific Meeting, Asian Pacific Association for the Study of the Liver, Kuala Lumpur 1994 (Abstract);128.
19. Sarin SK, Chari S, Sundaram KR, Ahuja RK, Anand BS, Broor SL. Young v adult cirrhotics: a prospective, comparative analysis of the clinical profile, natural course and survival. Gut 1988;29:101-107.
20. Acharya SK, Panda SK, Duphare H, Dasarathy S, Ramesh R, Jameel S, et al. Chronic hepatitis in a large Indian hospital. Natl Med J India 1993;6:202-206.
21. Zuberi SJ. Seroepidemiology of HBV/HCV in Pakistan. Int Hepatol Comm 1996;5:19-26.
22. Shrestha SM, Tsuda F, Okamoto H, Tokita H, Horikita M, Tanaka T, et al. Hepatitis B virus subtypes and hepatitis C virus genotypes in patients with chronic liver disease in Nepal. Hepatology 1994;19:805-809.
23. Shreatha SM. Incidence of HBsAg carrier rate in pregnant women in Kathmandu. J Inst Med 1987;71-76.
24. Mahtab MA, Rahman S, Karim F, Foster G, Solaiman S. Epidemiology of Hepatitis C virus in Bangladeshi General Population. BSMMU J 2009; 2(1):14-17.
25. Khan M, Mustafa MG, Ahmad N et al.Indian J Gastroenterol 2010(January –February);29(1):44-45

Bangladesh Journal of Hepatology
Vol. 3 No. 1 15
Socio-demographic profile of non alcoholic fatty liver disease of 100 patients attended SBMCH Barisal
Golam Mashud1, Jamsed Alom2, Swapon Kumar Sarkar3, Anwar Hossain4, Amolendu Bhattacharia1, Al Mamun Hossain1
1Department of Hepatology, Sher-E-Bangla Medical College, Barisal, Bangladesh 2Department of Hepatology, Shaheed Suhrawardi Medical College, Dhaka, Bangladesh, 3Department of Gastroenterology, Sher-E-Bangla Medical College,
Barisal, Bangladesh, 4Department of Medicine, Sher-E-Bangla Medical College, Barisal, Bangladesh
Corresponding authorDr. Golam MashudAssociate Professor
Department of Hepatology, Sher-E-Bangla Medical College, Barisal, Bangladesh. E-mail: <[email protected]>
Background: Non-alcoholic fatty liver disease (NAFLD) is an important cause of liver disease burden across the world. By definition, although the histopathologic features of NAFLD are identical to that of alcoholic liver disease, its diagnosis requires absence of significant alcohol use and absence of other causes of chronic liver disease. NAFLD is a metabolic disorder originally assumed to be largely confined to residents of affluent, industrialized Western countries4; however, obesity and insulin resistance, the common substrates of NAFLD, are not restricted to the west, as witnessed by their increasingly universal distribution.
Methods: It is a prospective study conducted in Sher e-Bangla Medical College hospital Barishal during the time of 2013 to2015. Sonographically proved fatty liver disease patient were admitted into hospital or attended out patient department.
Results: Majority of population belonged to >40 years in both groups. The mean age was found 38.86±10. (67.0%). Male female ratio was 0.49:1.
Conclusion: In the next few years NFLD may be the principle cause of death due to liver disease and possibility the principal cause of liver transplant we suggest oto expand the number of prospective cohort study in general population44 years with a range from 18 to 70 years. Male was found 33(33.0%). Female was found 67.
Abstract
Background:
Non-alcoholic fatty liver disease (NAFLD) is an important cause of liver disease burden across the world. By definition, although the histopathologic features of NAFLD are identical to that of alcoholic liver disease, its diagnosis requires absence of significant alcohol use and absence of other causes of chronic liver disease. Non-alcoholic fatty liver disease (NAFLD) is one of the causes of fatty liver, occurring when fat is deposited (steatosis) in the liver due to causes other than excessive alcohol use. NAFLD is the most common liver disorder in developed countries.[1][2] A recent study using the National Health and Nutrition Examination Survey (NHANES) found a 30% prevalence of NAFLD in
the United States between 2011 and 2012.[3] Most people with NAFLD have few or no symptoms. Patients may complain of fatigue, malaise, and dull right-upper-quadrant abdominal discomfort. Mild jaundice may be noticed although this is rare. More commonly NAFLD is diagnosed following abnormal liver function tests during routine blood tests. By definition, alcohol consumption of over 20 g/day (about 25 ml/day of net ethanol) excludes the condition.[4]NAFLD is associated with insulin resistance and metabolic syndrome (obesity, combined hyperlipidemia, diabetes mellitus (type II), and high blood pressure).[4][6] NAFLD is a metabolic disorder originally assumed to be largely confined to residents of affluent, industrialized Western

16
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Table I: Socio-demographic variable of the study population (n=100).
countries4; however, obesity and insulin resistance, the common substrates of NAFLD, are not restricted to the west, as witnessed by their increasingly universal distribution5. In particular, there has been an upsurge in obesity-related metabolic syndrome in the Asia-Pacific region, so that in countries such as China, Japan, Korea and probably India, rates of NAFLD are between 12% and 24% of the general population7. There are critical differences with respect to the extent of adiposity between Eastern and Western populations8. In light of these differences, we provide an Asia-Pacific regional perspective of risk factors and settings for NAFLD.Most people with NAFLD have few or no symptoms. Patients may complain of fatigue, malaise, and dull right-upper-quadrant abdominal discomfort. Mild jaundice may be noticed although this is rare. More commonly NAFLD is diagnosed following abnormal liver function tests during routine blood tests. By definition, alcohol consumption of over 20 g/day (about 25 ml/day of net ethanol) excludes the condition.[4]NAFLD is associated with insulin resistance and metabolic syndrome (obesity, combined hyperlipidemia, diabetes mellitus (type II), and high blood pressure).[4][6]
Methods:
It is a prospective study conducted in Sher e-Bangla Medical College hospital Barishal during the time of 2013 to 2015. Sonographically proved fatty liver disease patient were admitted into hospital or attended out patient department. Properhistory was taken and examined thoroughly. Particulars of the patients and information regarding ace, sex occupation, food habit. physical and labrotory findings were documented in a previously formed Case record form and data were analysed statistically.
Results:
A total number of 100 patients who came to the SBMCH,Barisal during the period of July 2013 to Decembar 2013, were enrolled in this study. Of them 100 patients with fatty liver diagnosed on the basis of USG were considering as NAFLD group. The present study findings were discussed and compared with previously published relevant studies.
Socio -demographicNAFLD (n=100)
Age (in years) n %
≤25 12 12.0 26-30 13 13.0 31-35 14 14.0 36-40 20 20.0 >40 41 41.0
Mean±SD 38.86 ±10.44 Range (min -max) (18 -70)
Sex Male 33 33.0 Female 67 67.0
Occupation House wife 49 49.0 Service 33 33.0 Day laborer 8 8.0 Businessman 5 5.0 Others 5 5.0
Socio -economic status Lower* 30 30.0 Middle** 65 65.0 Upper*** 05 5.0

Bangladesh Journal of Hepatology
Vol. 3 No. 1 17
Table II: Distribution of the study population according waist circumference, BMI and Blood pressure (n=100).
* Taka <5000 per month; ** Take 5000-60,000 per month; *** Taka >60,000 per month (Ref. State of children of the world 2007, UNICEF)27
The above table shows population were included in this study were divided into five groups according to age. Majority of population belonged to >40 years in both groups. The mean age was found 38.86±10.44 years with a range from 18 to 70 years.
Male was found 33(33.0%). Female was found
67(67.0%). Male female ratio was 0.49:1. Muslim population was found in 85 (85.0%). Hindu population was found 15(15.0%). Majority population i.e. 49(49.0%) were housewives, followed by 33(33.0%) service holder. Population came from urban area were more frequent in both groups 96% and 55% respectively. Majority population came from middle class socio-economic status 65%.
The above table shows regarding the waist circumference, the mean waist circumference was found in 87.84±9.74 cm.
Regarding the BMI, the mean BMI was found 26.9±2.9 kg/m2. Maximum 58(58.0%) population were obese (BMI >25) and 10(10.0%) population were normal weight (BMI <23) and 32(32.0%) population were
overweight (BMI 23-25). The mean systolic BP was found 133.94±9.74 mmHg. The mean diastolic BP was found 83.45±5.76 mmHg.
Discussion:
Although early studies emphasized that NAFLD was more common in women,10] recent studies have shown
Variables NAFLD (n=100)
Waist circumference (cm) n % Normal 33 33.0 ≥90 (men) ≥80 (women) (abdominal obesity) 67 67.0
Mean±SD 87.84 ±9.74
Range (min -max) (34 -112)
BMI (kg/m 2)
<23 (normal) 10 10.0
23-25 (over weight) 32 32.0
>25 (Obesity) 58 58.0 Mean±SD 26.9 ±2.9
Range (min -max) (20.0 -32.8)
Systolic BP (mmHg) ≥130 mmHg 60 60.0
≥140 mmHg 20 20.0
Mean±SD 133.94 ±9.74 Range (min -max) (110 -150)
Diastolic BP (mmHg)
≥85 mmHg 60 60.0
≥90 mmHg 20 20.0 Mean±SD 83.45 ±5.76

18
Bangladesh Journal of Hepatology
Vol. 3 No. 1
that NAFLD has a more even distribution between men and women, or may even be more prevalent among men. NAFLD can be found in all age groups; however the prevalence appears to increase with age. A study conducted in 1977 using liver biopsy found that the prevalence of fatty liver in the general population was 1% in people below 20 years, 18% between 20 and 40 years, and 39% among 60 and older.11] Several subsequent studies using different methods to define NAFLD have shown similar findings. In a population-based study in the United States, Browning et al found that individuals with MRS defined-NAFLD were slightly older (46 versus 45 years old, p = 0.003) than those with normal HT.1`2, Browning et al found that African Americans have significantly less HT (median 3.2%) and hepatic steatosis (24%) than non-Hispanic whites (HT median 3.6% and hepatic steatosis 33%) or Hispanics (HT median 4.6% and hepatic steatosis 45%) even after adjusting for obesity and diabetes.[12] In another study, Caldwell et al observed that, although there was overrepresentation of African Americans among patients seen with major risk factors for NAFLD and other liver diseases, a disproportionately small fraction of patients with NAFLD were African Americans.13 Worldwide, obesity remains the most important and well-described risk factor for NAFLD (Fig. [1]). The results of several cross-sectional studies and case-control studies have shown that people with NAFLD have higher waist circumference (WC) or BMI than those without NAFLD, and have reported significant associations between abdominal obesity (OR = 1.10-1.13; 95% CI, 1.02-1.22 per 1-cm increase in WC) and NAFLD14 In the Dionysos study, NAFLD was present in 94%, 67%, and 24.5% of the obese, overweight, and normal weight populations, respectively.15 Several studies have reported that patients with obstructive sleep apnea (OSA) have a higher prevalence of NAFLD. Epidemiologic studies showing familial aggregation of NAFLD and insulin resistance further support a genetic basis for NAFLD.16]-17 Additionally, studies have found interethnic variations in the prevalence of NAFLD and NAFLD-related "cryptogenic" cirrhosis, suggesting that susceptibility to NAFLD has a genetic component.[18 The results of epidemiologic studies have been inconsistent and it has been difficult to distinguish the effect of different components of diet per se. Although some
studies have highlighted the positive association between carbohydrate intake and NAFLD occurrence and severity, others have underlined the effect of different types of fat. Until relatively recently, NAFLD was considered a benign condition. However, an increasing number of studies has demonstrated that NAFLD can lead to long-term complications such as cryptogenic cirrhosis and hepatocellular carcinoma, as well as increased liver-related mortality. Additionally, several studies conducted over the last decade have indicated that NAFLD is, by itself and concurrent with other liver disease, a risk factor for diabetes and cardiovascular disease.
Conclusion:
In NASH, steatosis is accompanied by intralobular inflammation and hepatocyte injury, usually in the form of ballooning. Ongoing hepatic damage in NASH can lead to fibrosis and cirrhosis in some cases [6]. However, which conditions drive the progress of NAFLD towards NASH is not yet fully understood. As liver biopsy is mandatory for diagnosis of NASH, larger epidemiologic studies are challenging;owing to increased prevalence and incidence of obesity and diabetes, in the next few years NFLD MAY PRESENT THE principle cause of death due to liver disease and possibility the principal cause of liver transplant we suggest oto expand the number of prospective cohort study in general population even they are more expensive and difficulty to handle.
Refererences:
1. Shaker, Mina, et al. "Liver transplantation for nonalcoholic fatty liver disease: New challenges and new opportunities." World journal of gastroenterology: WJG 20.18 (2014): 5320.
2. Rinella ME (June 2015). "Nonalcoholic fatty liver disease: a systematic review". JAMA (Systematic review) 313 (22): 2263–73. doi:10.1001/jama.2015.5370. PMID 26057287.3. Ruhl, C. E., and J. E. Everhart. "Fatty liver indices in the multiethnic United States National Health and Nutrition Examination Survey." Alimentary pharmacology & therapeutics 41.1 (2015): 65-76.
4. Angulo, P, 2002, ‘Non-alcoholic fatty liver disease’, N Engl J Med, vol. 346, pp.1221-1331.

Bangladesh Journal of Hepatology
Vol. 3 No. 1 19
5. Williams, R 2006, ‘Global challenges in liver disease’, Hepatology, vol.44, pp.521–526.
6. cardiovascular disease: a meta-analysis’, Am. J. Med, vol.119, pp.81216.Galassi, A, Reynolds, K, He, J 2006, ‘Metabolic syndrome and risk of –19.
7. Wu, YF 2006, ‘Overweight and obesity in China. The once lean giant has a weight problem that is increasing rapidly’, BMJ, vol.19, pp.362–3.
8 Adams LA, Angulo P (2006). "Treatment of non‐alcoholic fatty lidisease".PosMed J 82 (967): 315–22. doi:10.1136/pgmj.2005.042200. PMC 2563793. PMID 16679470.
9. Clark JM, Diehl AM (2003). "Nonalcoholic fatty liver disease: an underrecognized cause of cryptogenic cirrhosis". JAMA 289 (22): 3000–4. doi:10.1001/jama.289.22.3000. PMID 12799409
10 .Sheth SG, Gordon FD, Chopra S. Nonalcoholic steatohepatitis. Ann Intern Med 1997;126(2):137–145
11. Hilden M, Christoffersen P, Juhl E, Dalgaard JB. Liver histology in a ''normal'' population: examinations of 503 consecutive fatal traffic casualties. Scand J Gastroenterol 1977;12(5):593–597
12. Browning JD, Szczepaniak LS,Dobbins R, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology 2004;40(6):1387–1395
13 .Caldwell SH, Harris DM, Patrie JT, Hespenheide EE. Is NASH underdiagnosed among African Americans? Am J Gastroenterol 2002;97(6):1496–1500.
14 .Bellentani S, Bedogni G, Miglioli L, Tiribelli C. The epidemiology of fatty liver. Eur J Gastroenterol Hepatol 2004;16(11):1087–1093.
15. Browning JD, Kumar KS, Saboorian MH, Thiele DL. Ethnic differences in the prevalence of cryptogenic cirrhosis. Am J Gastroenterol 2004;99(2):292–298.
16. Toshimitsu K, Matsuura B, Ohkubo I, et al. Dietary habits and nutrient intake in non-alcoholic steatohepatitis. Nutrition 2007;23(1):46–52.
17. Hui JM, Kench JG, Chitturi S, et al. Long-term outcomes of cirrhosis in nonalcoholic steatohepatitis compared with hepatitis C. Hepatology 2003;38(2):420–427.

20
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Background: Endoscopy is a nonsurgical procedure used to examine a patient’s gastrointestinal tract. Fiber optic endoscopy is a highly efficient diagnostic tool, which is now being increasingly used in the diagnosis of GI diseases. This study has been carried out to demonstrate indications for and common findings of endoscopy in adults aging 15 years and above.
Methods: We retrospectively reviewed the medical records for endoscopy indication and result of adults who had endoscopy between June 2014 and May 2005.
Results: We analyzed 1283 adult aged 15 years or above who were referred for upper gastrointestinal endoscopy. There were 731 male and 552 female cases. Highest numbers of participants were in the age group of 25-34 (24.6%). The main indications comprised dyspepsia (49.66%), epigastric pain (29.63%), abdominal pain (7.025), hematemesis (6.12%), recurrent vomiting (3.67%), abdominal distension (2.26%) and others (1.64%). Endoscopic diagnoses included duodenal ulcer (9.6%), gastric ulcer (4.9%), Oesophagealvarices (6.8%), gastritis (5.6%), gastropathy (3.2%), Ca- stomach (2.7%),ca-oesophagus (1.3%), oesophagitis (1.5%), duodenitis (0.7%), pyloric stenosis (0.7%) and others (1.8%).
Conclusion: Upper gastrointestinal endoscopy is a diagnostic procedure in adults, which is increasingly used in government medical college hospitals to explore the upper GI pathologies i.e.- duodenal ulcer, gastric ulcer, ca- stomach and oesophagus, gastritis, gastropathy and oesophagealvarices.
Abstract
Upper gastrointestinal endoscopic findings in adults at Comilla Medical College & Hospital, Bangladesh
Mohammad Forhad Abedin1, Mohammad Asaduzzaman Lashkar2, Mohammad Shah Jamal3, Mohammad Belalul Islam1, Mohammad Izazul Haque4, Mohammad Abdur Rob Sarkar3
1Department of Medicine, Comilla Medical College Hospital, Comilla, Bangladesh, 2Department of Cardiology, Comilla Medical College Hospital, Comilla, Bangladesh, 3Department of Gastroenterology, Comilla Medical College Hospital, Comilla, Bangladesh, 4Department of Hepatology, Comilla Medical College Hospital, Comilla, Bangladesh
Corresponding authorDr. Mohammad Forhad Abedin
Resident Physician (Medicine)Comilla Medical College Hospital, Comilla, Bangladesh, Email: [email protected]
Introduction:
Upper gastrointestinal diseases are leading causes of morbidity and mortality1, 2. Upper gastrointestinal endoscopy (UGIE) has become a corner stone in the diagnosis and treatment of many of gastrointestinal disorders3. The directvisualization of the entire oesophagus,stomach and duodenum with the facility toobtain material for analysis and to performvarious therapeutic measures, make endoscopy superior to other diagnosticprocedures4, 5.
Comilla medical college is the only government medical college in Comilla district. This study was done in the
Departments of Gastroenterology and Hepatology, Comilla Medical College Hospital from June 2014 to May 2015.
Objectives:
The objectives of the study were to determine the demographic characteristics of adult who had upper GI endoscopy from June 2014 to May 2015 at Comilla medical college & hospital as well as determine the indications for upper GI endoscopy in the adults and determine the prevalence of upper GI lesions in the adults.

Bangladesh Journal of Hepatology
Vol. 3 No. 1 21
Table I: Age range and sex distribution
Table II: Indications for endoscopy
Methods and procedures:
Medical records of patients who underwent upper GI endoscopy in Comilla medical college hospital from June 2014 to May 2015 were retrospectively reviewed. Routine diagnostic and therapeutic endoscopies are carried out six days in a week in the Hospital. Approximately 1000 patients undergo upper GI endoscopyper year. Gastrointestinal endoscopy at the hospital is under the department of gastroenterology, and is performed by Gastroenterologist and hepatologist with training and experience in endoscopy. Under topical lidocaine, a Pentax FG-29W fiberoptic Upper GI scope is passed through the mouth of a patient in left lateral position through the upperoesophageal sphincter into the oesophagus stomach and duodenum (upper gut). Cases which were
fifteen years old and above are included in the study. Cases with unclear medical records orthose with missing values were excluded. The following data was collected from the patient: Age, Sex, Residences, Indication for the upper GI Endoscopy, Duration of Symptoms, and Endoscopy findings. Data collected was then analyzed using SPSS Version 17, result presented in tables and Charts.
Results:
A total of 1283 patients underwent upper GI endoscopy during the period (June 2014 to May 201) were included in the study. Among the patient 56.9% were male & 43.1% were female. Highest number of the patients (24.6%) underwent endoscopy at the age range between 25 to 34 years.
Age range
Sex Total
Male Female
No Percent (%) No Percent (%) No Percent (%) 15-24 85 6.6 66 5.1 151 11.8 25-34 177 13.8 139 10.8 316 24.6 35-44 122 9.4 121 9.4 243 18.8
45-54 127 9.9 89 6.9 216 16.8 55-64 116 9.0 93 7.3 209 16.3 65-74 73 5.7 28 2.2 101 7.9 75-84 27 2.1 13 1.0 40 3.1 85-94 2 0.2 2 0.2 4 0.3
95-104 2 0.2 1 0.1 3 0.2 Total 731 56.9 552 43.1 1283 100.0
The three commonest indications for upper GI endoscopy in adults were dyspepsia (49.66%), epigastric pain (29.63%), and abdominal pain
(7.02%).Miscellaneous causes included haematemesis (6.12%), vomiting (3.67%), and abdominal distension (2.26%).
Indication No of case Percent (%)Dyspepsia 637 49.66
Epigastric pain 380 29.63
Abdominal pain 90 7.02
Haematemesis 79 6.12
Vomiting 47 3.67
Abdominal distension 29 2.26
Others 21 1.64

22
Bangladesh Journal of Hepatology
Vol. 3 No. 1
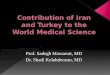
Figure 1: Percentage of endoscopic findings
Table III: Prevalence of endoscopic findings by age range
Approximately 61.2% of the upper GI endoscopy done in adults was negative. Of the 38.8% positive endoscopies, duodenal ulcer were the most common 9.6%, followed by gastritis (5.6%) and gastric ulcer
(4.9%), Oesophageal varices were 6.8%.Among two malignancies Ca-stomach(2.7%) was more prevalent than Ca-oesophagus (1.3%).
Duodenal ulcers (26.83%) were more prevalent at the age range 55 to 64 years, whereas gastric ulcers were more prevalent relatively earlier age at 45 to 54 years. Highest prevalence of Ca-stomach (31.43%) &
Ca-oesophagus (47.06%) were occurred at the age 55 to 64 years. More Oesophageal varices (26.44%) were seen at the age 45 to 55 years.
All the endoscopic positive findings are more in male than female except gastritis which is more in female than male.
Endoscopic finding Highest prevalence Age range
No Percentage (%)Normal 221 28.15 25-34 Pyloric stenosis 3 33.33 65-74 Duodenitis 4 44.44 25-34 Duodenal ulcer 33 26.83 55-64 Gastric ulcer 17 26.98 45-54 Ca - stomach 11 31.43 55-64 Ca - oesophagus 8 47.06 55-64 Gastropathy 15 36.59 25-34 Gastritis 15 20.83 25-34 Oesophagealvarices 23 26.44 45-55 Oesophagitis 6 31.58 55-64 Others 6 25.0 45-54

Bangladesh Journal of Hepatology
Vol. 3 No. 1 23
Figure 3: Prevalence of the findings according to sex
Discussion:
Gastrointestinal diseases affect adults worldwide and in patients with digestive complaints, endoscopy is the gold standard and often the primary exploration5. Comilla medical college is the only government facility centre in Comilla district where endoscopic procedure can be done; beside these some private hospital also have the facility for endoscopic procedure.
In this study, there were more males 56.9% than females 43.1%; similar to findings in majority of other countries, probably because Upper GI tract diseases are more prevalent in males6, 7, 8, 9, 10. A study conducted at Multan by Muhammad Innayatullah et al.11 shows more of male preponderance (50.6 % Males Vs. 49.4 % Females). In the study conducted at Peshawar12 had an almost equal number of males and females, however Nkrumah et al in Saudi Arabia and Khurram et al in Pakistan13, 14 noticed more females as compared to males in their studies, probably more females are being referred in the centers for endoscopy.
The age pattern is closely similar to those of other studies with very few presenting before the age of 20years, peaking in the 25 to 54 years, probably because Upper GI tract diseases are prevalent in the older population age group7, 9, 15.
We noticed dyspepsia in (49.66%), being commonest indication for Upper GI Endoscopy in our study. This is similar to Malu et al (78.1 %) in their study at Zaria and
so did Danbauchi et al, Aduful et al, Nkrumah et al, Khurram in Pakistan, Onyekwere et al in Lagos and Cooper in USA8,17,16. A study from India18 reported dyspepsia in 59%of patients undergoing OGD.
In our study normal Endoscopy was reported in 61.2% (n=785), more common in males 51% (n=400) as compared to females 49% (n=385), which is not consistent with the result of study by Khalid Mahmud et al12, showing more female preponderance (31.2% females vs. 28.6% males). Rate of negative Endoscopy (61.2%) in our study was higher as compared to reported rates in the study of Muhammad et al from Multan11 and was higher as compared to negative Endoscopy 30%12, as reported by Khalid Muhammad12. This observation was also reportedby Shahetal19. Strict selection criteria required to reduce this rate will result in missing significant pathology in large number of patients.
The overall frequency of duodenal ulcer in the studied population was 9.6% as compared to gastric ulcer which was 4.9% in our study, is concordance with the published by Khalid Muhammad et al12in which overall frequency of duodenal ulcer with that of gastric ulcer was 8.1% versus 3.7%.
Gastric carcinoma was reported in 2.7 %(n=35) similar to percentage of gastric carcinoma reported by Emmanuel jeje et al and esophageal carcinoma in 1.3% (n=17), which is less as compared to Emmanuel jeje et al which is 1.7%. Our findings were significantly

24
Bangladesh Journal of Hepatology
Vol. 3 No. 1
high as compared to the percentage (1.17%) as reported by Khalid Muhammad12 and Muhammad Inayatullah et al11.
Conclusion:
Endoscopy is a very important investigative modality to identify the specific pathology in patients of Dyspepsia, Gastritis, Oesophagitis, Duodenitis, Duodenal ulcer, Gastric ulcer, Gastric carcinomas and esophageal malignancies were as the commonest endoscopic diagnostic findings. Strict selection criteria required to reduce this rate will result in missing significant pathology in large number of patients.
References:
1. Spiller R. ABC of the upper gastrointestinaltract (Clinical Review). Anorexia, nausea,vomiting and pain. BMJ 2001; 323: 1354-1357.
2. Kolk H. Evaluation of symptom presentationin dyspeptic patients referred for uppergastrointestinal endoscopy in Estonia. CroatMed J 2004; 45(5): 592-8.
3. Editorial. Endoscopy in general practice. BMJ1995; 310: 816-817.
4. Axon ATR, Bell GD, Jones RH, et al.Guidelines on appropriate gastrointestinal endoscopy. BMJ 1995; 310: 853-856.
5. Agbakwuru EA, Fatusi AO, Ndububa DA, etal. Pattern and validity of clinical diagnosis ofupper gastrointestinal diseases in south-west
Nigeria. Afr Health Sci 2006; 6(2): 98-103.
6. Olokoba AB, Bojuwoye BJ. Indications for oesophagogastroduodenoscopy in Ilorin, Nigeria--a 30 month review. Nigerian Journal of clinical Practice. 2010; 13(3): 260-3.
7. Agbakwuru EA, Fatusi AO, Ndububa DA et al. Pattern and validity of clinical diagnosis of upper gastrointestinal diseases in south-west Nigeria. Afr Health Sci. 2006; 6(2): 98-103.
8. Malu AO, Wali SS, Kazmi R, Macauley D, Fakunle YM.Upper gastrointestinal endoscopy in Zaria, northern Nigeria.West African Journal of Medicine. 1990; 9(4): 279-84.
9. Danbauchi SS, Keshinro IB, Abdu-Gusau K. Fifteen years of upper gastrointestinal endoscopy in Zaria (1978 - 1993). African journal of medicine and medical sciences. 1999; 28(1-2): 87-90.
10. Aduful H, Naaeder S, Darko R, Baako B, Clegg-Lamptey J, Nkrumah K, et al. Upper gastrointestinal endoscopy at the korlebu teaching hospital, accra, ghana. Ghana Med J. 2007; 41(1): 12-6.
11. Muhammad Inayatullah, Zahra Nazish Muhammad Saleem Akhtar, Abdul Hameed Anjum, Altaf Baqir Naqvi. Dyspepsia and Upper Gastrointestinal Endoscopy Professional Med J Mar 2008;15(1);143-147
12. Khalid Mahmood, Mohammad IlyasSaeedi, Riaz Mohammad, Zia ud Din upper gastrointestinal endoscopic findings in patients with dyspepsia jpmi 2006 vol.20 no:70-73
13. Nkrumah KN. Endoscopic evaluation of upper abdominal symptoms in adult patients, Saudi Aramco-Ai Hasa Health Center, Saudi Arabia.West African Journal of Medicine. 2002; 21(1): 1-4.
14. Khurram M, Khaar HT, Hasan Z, Umar M, Javed S, Asghar T, et al. A 12 years audit of upper gastrointestinal endoscopic procedures.Journal of the College of Physicians and Surgeons--Pakistan: JCPSP. 2003; 13(6): 321-4
15. Onyekwere CA, Hameed H, Anomneze EE, Chibututu C. Upper gastrointestinal endoscopy findings in Nigerians: a review of 170 cases in Lagos. The Nigerian Postgraduate Medical Journal. 2008; 15(2): 126-9.
16. Emmanuel Jeje Thomas Olajide, Bashir Akande Upper Gastrointestinal Endoscopy - Our Findings, Our Experience in Lagoon Hospital, Lagos, Nigeria Macedonian Journal of Medical Sciences. 2013 June 1; 6(2):168-173
17. Cooper GS. Indications and contraindications for upper gastrointestinal endoscopy.Gastrointestinal Endoscopy Clinics of North America. 1994; 4(3): 439-54.
18. Katelaris OH, Tippet GH, Norbu P, Lowe DG, Br e n n a n R, F a t h i n g MJ Dyspepsia, Helicobacter pylori and peptic ulcer in a randomly selected population in India. Gut 1992; 33: 1462-6.
19. Shah NH, Shah MS, Khan I, Hameed K An audit of diagnostic upper GI endoscopic and comparison of booked vesus open access cases JCPSP 1999;9(4);174

Bangladesh Journal of Hepatology
Vol. 3 No. 1 25
Hepatic hydrothorax: Challenge for Hepatologist
Syed Abul Foez1, Mohammad Abdur Rahim2, Sheikh Mohammad Noor-E-Alam3, Mohammad Ashraful Alam4, AKM Shoab1, Swapan Kumar Singha1, Joy Vargese5, Chandan Kumar5, Mamun-Al-Mahtab6, Salimur Rahman6, Ziaur
Rahman Chowdhury7
1Department of Medicine, 250 Beded Hospital, Moulvibazar, Bangladesh, 2MATS, Noakhali, Bangladesh, 3Department of Hepatology, Shaheed Suhrawardhy Medical College Hospital, Dhaka, Bangladesh, 4Department of Hepatology, Cox’s Bazar Medical College, Cox's Bazar, Bangladesh, 5Institute of Liver Diseases & Transplantation,
Global Health City, Chennai, India, 6Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh, 7Department of Paediatrics, 250 Beded Hospital, Moulvibazar, Bangladesh.
Corresponding authorDr. Syed Abul Foez
Resident Physician (Medicine)250 Beded Hospital, Moulvibazar, Bangladesh. E-mail: <[email protected]>
Introduction:
Hepatic hydrothorax may be defined as a pleural effusion associated with portal hypertension without any cardiac, pulmonary and pleural disease. This “porous diaphragmatic syndrome” is not a common complication of end-stage liver disease (ESLD) [1]. There is no large randomized-controlled trial establishing the best treatment options and other management strategies [2]. HH thus represents a formidable entity in the management of end-stage liver disease [3]. This clinical review focuses on the recent developments in the pathogenesis as well as the management strategies.
Incidence:
Occur in 4–6% of patients with cirrhosis in studies that used chest x-ray to diagnose pleural effusion [4]. However, in a series of 862 cirrhotic patients from China that used ultrasonography to detect pleural effusion, the incidence was found to be 15% [5-8]. Right-sided in majority (65–87 %), is left-sided in 13–17 %, and could be bilateral in 3 % of cases [9].
Pathophysiology:
Not fully elucidated so far. More than one mechanism may coexist [2].
Most of the studies suggested that transfer of peritoneal fluid into the pleural space via diaphragmatic defects is the predominant mechanism. Others are- azygous vein hypertension, passage of fluid from peritoneal to the pleural space via transdiaphragamtic lymphatics, lymphatic leakage from the thoracic duct, hypoalbuminemia resulting in decreased colloid osmotic pressure also play role [10].
Recently, these diaphragmatic defects associated with the development of hydrothorax have been classified into four morphologic types [11]:
Type 1: No obvious defect
Type 2: Blebs lying in the diaphragm
Type 3: Fenestrations in the diaphragm
Type 4: Multiple gaps in the diaphragm
Discontinuties or gaps in the collagen bundles that make up the tendinous portion of the diaphragm.
Review Articles
AbstractHepatic hydrothorax is an example of porous diaphragmatic syndrome which results from portal hypertension in patient with end stage liver disease. Commonly seen in conjunction with ascites, but isolated hydrothorax may also occur. Liver transplantation is the ultimate treatment of choice. Other management options may serve as a bridge to transplantation.

26
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Ascites raises the intra-abdominal pressure and tends to stretch the diaphragm; thereby, creating or enlarging these microscopic defects 12]. Herniation of peritoneum through these gaps in the pleural cavity leads to the formation of pleuro-peritoneal blebs (typically < 1 cm). Due to increasing intra-abdominal pressure these blebs tend to rupture.
The negative intrapleural pressure facilitates the one-way transfer of fluid [13]. Blebs tend to occur more commonly in the right hemidiaphragm which may be related to embryonic development; the left hemidiaphragm is more muscular, thicker and relatively resistant to blebs formation.
The negative intrathoracic pressure coupled with the increased intra abdominal pressure in the background of diaphragmatic thinning due to chronic malnutrition further form a gradient favoring cephalad transfer of fluid across these defects, possibly with a valvular mechanism [1]
Clinical features:
HH should be suspected in a patient of established cirrhosis and portal hypertension, presenting with pleural effusion [1]. Clinical features depends on volume of the pleural fluid, the rapidity of accumulation of fluid and the presence of associated cardiopulmonary disease. Patients may be asymptomatic or may present with dyspnea, cough, or hypoxemia with or without ascites. Rarely acute tension hydrothorax leading to respiratory failure due to sudden rupture of a large pleuroperitoneal bleb [14, 15].
Diagnosis:
A diagnostic thoracentesis and chest radiograph should be performed in all patients with suspected HH [18]. In a cohort of cirrhosis patients 70% of pleural effusions were due to uncomplicated HH, 15% were due to infected HH, and 15% were due to causes other than liver disease [4]. In another study 80% of right-sided pleural effusions were found to be uncomplicated HH, while only 35% of left-sided pleural effusions were uncomplicated HH [19].
Pleural fluid analysis should include total and differential cell count, Gram stain and culture, serum and fluid protein, albumin, LDH, ADA and bilirubin [12]. Other tests depending on the appropriate clinical circumstances include triglyceride, pleural pH, PCR for
mycobacterium, amylase, and cytology to exclude chylothorax, empyema, tuberculosis, pancreatitis, and malignancy respectively. Characteristics of pleural fluid in an uncomplicated HH are [20, 21]:
• Cell count < 500 cells/mm3
• Polymorphonuclear count < 250 cells/mm3
• Total protein < 2.5 g/dl
• Serum to pleural fluid albumin gradient (SPAG) >1.1 g/dl
• Pleural fluid to serum total protein ratio <0.5
• Pleural fluid LDH/serum LDH < 0.6
• Pleural fluid/serum bilirubin < 0.6
• Glucose level similar to that of serum
• Pleural fluid amylase concentration < serum amylase concentration
• pH >7.4
CT scan of the chest will exclude mediastinal, pulmonary or pleural lesions or malignancies. Echocardiography and BNP should also be performed to evaluate cardiac function in proper clinical setting [1]. Demonstration of a peritoneal-pleural communication by scintigraphy, contrast-enhanced ultrasonography, MRI, or thoracoscopy is not necessary in clinical practice unless surgical repair is being contemplated [16, 17].
SBEM/ SBPL:
Spontaneous bacterial empyema (SBEM) may be defined as bacterial colonization of a pre-existing sterile hydrothorax without any concomitant pneumonia [22].The term SBEM itself is an oxymoron, implying that there is actually no pus or abscess in the pleural space. Spontaneous bacterial pleuritus (SBPL) is a more appropriate term. SBPL develops in 10%-16% of cirrhosis patients with HH. It must be considered in any patient with HH who develops fever, pleuritic pain, encephalopathy or unexplained deterioration in renal function [3]. Dignostic criteria of SBPL [22]:
• PMN >250 cells/mm3 and positive pleural fluid culture OR
• PMN >500 cells/mm3 and negative pleural fluid culture AND
• Absence of pneumonia or contiguous infection on chest imaging

Bangladesh Journal of Hepatology
Vol. 3 No. 1 27
Pathogenesis remains speculative. Direct bacterial spread from the peritoneal cavity or transient bacteremia infecting the pleural space may be the mechanism [23]. However, nearly 40% of episodes were not associated with SBP. Escherichia coli, Streptococcus species, Enterococcus, and Klebsiella species are the usual pathogens [25]. Risk factors includes low pleural fluid C3, low serum albumin, low pleural fluid total protein (<1.5 g/dL), high Child-Pugh score/MELD and SBP [24].
Third-generation cephalosporins are the drug of choice (IV cefotaxime 2gm Q8h for 7-10 days). Carbapenems should be the treatment of choice in high-risk patients with nosocomial episodes, diabetes and patients treated with cephalosporin within the previous 3 months [26]. Albumin therapy: 1.5 g/kg on day 1 and 1.0 g/kg on day 3 may improve outcome. Lifelong antibacterial prophylaxis is recommended. Selective intestinal decontamination with norfloxacine appears to be effective. Chest tube placement is contraindicated except in case of frank pus or pH < 7.1 plus pleural fluid glucose < 40 mg/dl. An episode of SBPL warrants evaluation for LT [1]. Mortality associated with an episode of SBPL is 20%
Management:
Immediate goal: relief of symptoms and prevention of pulmonary complications and infections [3]
Cardinal aspect: prompt evaluation for liver transplantation [27]
There are three aspects of management:
• Pharmacologic/Medical
• Radiological intervention
• Surgical approach
Medical management:
• Aim: to induce and maintain a net negative sodium balance
• Restrict dietary sodium: upto 2,000 mg/day (88 mEq/day) [28]
• Diuretics: typically furosemide 40 mg/day and spironolactone 100 mg/day to produce a renal excretion of sodium of at least 120mEq/day [28]. The doses may be increased simultaneously in a stepwise
fashion: spironolactone up to 400 mg/day and furosemide up to 160 mg/day every 3–5 days [1].
• Other investigational agents: terlipressin, octreotide and midodrine. But there is not enough evidence to recommend routine use
Refractory hydrothorax:
Persistent hydrothorax despite fluid and sodium restriction and use of maximal tolerable doses of diuretics. It is found in approximately 25% of cases [24]. Treatment options are [29]:
• Repeated thoracentesis ± Paracentesis
• Transjigular intrahepatic portosystemic shunt (TIPS)
• Indwelling pleural catheter (IPC)
• Pleurodesis ± Contineous positive airway pressure (CPAP)
• Surgical repair of diaphragmatic by video assisted thoracoscopic surgery (VATS)/ medical thoracoscopy (MT) ± Pleurodesis
• Liver transplantation (LT)
Thoracentesis ± Paracentesis:
Therapeutic thoracocentesis is a simple, effective, safe and well-tolerated procedure for immediate relief of symptoms. Paracentesis should be attempted prior to thoracentesis to prevent the rapid accumulation of fluid in the pleural space after thoracentesis. There is no consensus for the maximal volume of pleural fluid to be drained in a single thoracentesis. It has been postulated that ≥ 2L of fluid should be removed so as to minimize the risk of hypotension or re-expansion of pulmonary edema [30]. It is not advocated as a maintenance therapy in patients requiring more frequent thoracentesis (>1in every 2 weeks) [7]. Chest tube insertions should be avoided at all costs [31].
TIPS:
Should be considered as a bridge to transplant and only in carefully selected group such as age < 65 years, bilirubin < 3 mg/dL, absence of encephalopathy, CTP B and MELD<17 [32-34]. 40–50% reduction of the initial HVPG should provide the optimal outcome of resolution of hydrothorax avoiding significant hepatic encephalopathy [35].

28
Bangladesh Journal of Hepatology
Vol. 3 No. 1
IPC (Pigtail):
Indwelling pleural catheter (IPC) is emerging as a feasible alternative in patients with frequent therapeutic thoracentesis, TIPS is contraindicated and awaiting for liver transplantation [36]. Small bore pigtail is safe, less invasive, well tolerated and little chance of complications.
Pleurodosis ± CPAP:
Because of moderate degree of complications (fever, chest pain, empyema, incomplete re-expansion, pneumonia, wound infection) pleurodosis typically reserved for patients in whom no other options exist [38]. CPAP appears effective in keeping the pleural cavity dry after chemical pleurodesis [40]. CPAP will reverse the peritoneal-pleural pressure gradient and thus prevent the shift of fluid form the peritoneal to the pleural space [37].
VATS/MT:
VATS considered a palliative alternative in patients requiring frequent thoracentesis [39]. It is also done as an alternative to TIPS and used as a bridge to liver transplantation. Medical thoracoscopy (MT) is a minimally invasive that may be used in complicated hepatic hydrothorax (thorasic empyema) [41]. Administration of sclerosing agents for pleurodosis or repair of diaphragmatic defects are reported by these procedure [42-44].
Liver transplantation:
It is the best definitive treatment. Indicated in refractory hydrothorax, MELD >15 and after an episode of SBPL [18]. Presence of preoperative hepatic hydrothorax does not have a significant negative influence on postoperative survival [45]. But uncontrollable hydrothorax is independent risk factors for the postoperative prognosis [46].
Prognosis:
Survival is limited. In one study median survival was found 9.1 months [47]. But it is favorably affected by liver transplantation.
Summary:
Hepatic hydrothorax is an infrequent but an important complication of portal hypertension. Diagnosis involves a high index of suspicion in a cirrhotic patient who presents with pleural effusion. Management is
challenging and frequently associated with poor outcomes. Liver transplantation remains the definitive treatment of choice. Recurrent thoracocentesis, TIPS, IPC, pleurodesis and VATS/MT advocated as a bridge to transplantation.
References:
1. Krok KL, Cardenas A. Hepatic hydrothorax. Semin Respir Crit Care Med. 2012;33(1):3–10.
2. Roussos A, Philippou N, Mantzaris GJ, et al. Hepatic hydrothorax: pathophysiology diagnosis and management. J Gastroenterol Hepatol. 2007;22(9):1388–93.
3. Cardenas A, Kelleher T, Chopra S. Review article: hepatic hydrothorax. Aliment Pharmacol Ther. 2004;20(3):271–9.
4. Chen TA, Lo GH, Lai KH. Risk factors for spontaneous bacterial empyema in cirrhotic patients with hydrothorax. J Chin Med Assoc. 2003;66(10):579–86.
5. Ladero JM. Recurring hepatic hydrothorax: a difficult therapeutic challenge. Rev Esp Enferm Dig. 2001;93(9):561–5.
6. Gur C, Ilan Y, Shibolet O. Hepatic hydrothorax—pathophysiology, diagnosis and treatment—review of the literature. Liver Int. 2004;24(4):281–4.
7. Garcia N Jr, Mihas AA. Hepatic hydrothorax: pathophysiology, diagnosis, and management. J Clin Gastroenterol. 2004;38(1):52–8.
8. Alagiakrishnan K, Patel PJ. Left-sided hepatic hydrothorax with ascites. Int J Clin Pract. 1999;53(3):225–6.
9. Gurung P, Goldblatt M, Huggins JT, et al. Pleural fluid analysis and radiographic, sonographic, and echocardiographic characteristics of hepatic hydrothorax. Chest. 2011;140(2):448–53.
10. Zenda T, Miyamoto S, Murata S, et al. Detection of diaphragmatic defect as the cause of severe hepatic hydrothorax with magnetic resonance imaging. Am J Gastroenterol. 1998;93(11):2288–9.
11. Huang PM, Chang YL, Yang CY, et al. The morphology of diaphragmatic defects in hepatic hydrothorax: thoracoscopic finding. J Thorac

Bangladesh Journal of Hepatology
Vol. 3 No. 1 29
Cardiovasc Surg. 2005;130(1):141–5.
12. Lazaridis KN, Frank JW, Krowka MJ, et al. Hepatic hydrothorax: pathogenesis, diagnosis, and management. Am J Med. 1999;107(3):262–7.
13. Strauss RM, Boyer TD. Hepatic hydrothorax. Semin Liver Dis.1997;17(3):227–32.
14. Kaplan LM, Epstein SK, Schwartz SL, et al. Clinical, echocardiographic, and hemodynamic evidence of cardiac tamponade caused by large pleural effusions. Am J Respir Crit Care Med.1995;151(3 Pt 1):904–8.
15. Castellote J, Gornals J, Lopez C, et al. Acute tension hydrothorax: a life-threatening complication of cirrhosis. J Clin Gastroenterol. 2002;34(5):588–9.
16. Foschi FG, Piscaglia F, Pompili M, et al. Real-time contrastenhanced ultrasound—a new simple tool for detection of peritoneal-pleural communications in hepatic hydrothorax. Ultraschall Med. 2008;29(5):538–42.
17. Nakamura A, Kojima Y, Ohmi H, et al. Peritoneal–pleural communications in hepatic hydrothorax demonstrated by thoracoscopy. Chest. 1996;109(2):579–81.
18. Alonso JC. Pleural effusion in liver disease. Semin Respir Crit Care Med. 2010;31(6):698–705.
19. Castellote J, Xiol X, Cortes-Beut R, et al. Complications of thoracentesis in cirrhotic patients with pleural effusion. Rev Esp Enferm Dig. 2001;93(9):566–75.
20. Xiol X, Castellote J, Cortes-Beut R, et al. Usefulness and complications of thoracentesis in cirrhotic patients. Am J Med. 2001;111(1):67–9.
21. Light RW. Diagnostic principles in pleural disease. Eur Respir J. 1997;10(2):476–81.
22. Xiol X, Castellote J, Baliellas C, et al. Spontaneous bacterial empyema in cirrhotic patients: analysis of eleven cases. Hepatology. 1990;11(3):365–70.
23. AbbaAA, LaajamMA, Zargar SA. Spontaneous neutrocytic hepatic hydrothorax without ascites. Respir Med. 1996;90(10):631–4.
24. Sese E, Xiol X, Castellote J, et al. Low complement levels and opsonic activity in hepatic hydrothorax: its relationship with spontaneous bacterial empyema. J Clin Gastroenterol. 2003;36(1):75–7.
25. Chen CH, Shih CM, Chou JW, et al. Outcome predictors of cirrhotic patients with spontaneous bacterial empyema. Liver Int. 2011;31(3):417–24.
26. Tu CY, Chen CH. Spontaneous bacterial empyema. Curr Opin Pulm Med. 2012;18(4):355–8.
27. Gines P, Cardenas A, Arroyo V, et al. Management of cirrhosis and ascites. N Engl J Med. 2004;350(16):1646–54.
28. Runyon BA. Management of adult patients with ascites due to cirrhosis: an update. Hepatology. 2009;49(6):2087–107.
29. Kiafar C, Gilani N. Hepatic hydrothorax: current concepts of pathophysiology and treatment options. Ann Hepatol. 2008; 7(4):313–20.
30. Sherman SC. Reexpansion pulmonary edema: a case report and review of the current literature. J Emerg Med. 2003;24(1):23–7.
31. Orman ES, Lok AS. Outcomes of patients with chest tube insertion for hepatic hydrothorax. Hepatol Int. 2009;3(4):582–6.
32. Spencer EB, Cohen DT, Darcy MD. Safety and efficacy of transjugular intrahepatic portosystemic shunt creation for the treatment of hepatic hydrothorax. J Vasc Interv Radiol. 2002;13(4): 385–90.
33. Salerno F, Merli M, Cazzaniga M, et al. MELD score is better than Child–Pugh score in predicting 3-month survival of patients undergoing transjugular intrahepatic portosystemic shunt. J Hepatol. 2002;36(4):494–500.
34. Wilputte JY, Goffette P, Zech F, et al. The outcome after transjugular intrahepatic portosystemic shunt (TIPS) for hepatic hydrothorax is closely related to liver dysfunction: a long-term study in 28 patients. Acta Gastroenterol Belg. 2007;70(1):6–10.
35.Dhanasekaran R, West JK, Gonzales PC, et al. Transjugular intrahepatic portosystemic shunt for symptomatic refractory hepatic hydrothorax in patients with cirrhosis. Am J Gastroenterol. 2010;105(3):635–41.
36. Milanez de Campos JR, Filho LO, de Campos Werebe E, et al. Thoracoscopy and talc poudrage in the management of hepatic hydrothorax. Chest. 2000;118(1):13–7.

30
Bangladesh Journal of Hepatology
Vol. 3 No. 1
37. Takayama T, Kurokawa Y, Kaiwa Y, et al. A new technique of thoracoscopic pleurodesis for refractory hepatic hydrothorax. Surg Endosc. 2004;18(1):140–3.
38. Ferrante D, Arguedas MR, Cerfolio RJ, et al. Video-assisted thoracoscopic surgery with talc pleurodesis in the management of symptomatic hepatic hydrothorax. Am J Gastroenterol. 2002; 97(12):3172–5.
39. Northup PG, Harmon RC, Pruett TL, et al. Mechanical pleurodesis aided by peritoneal drainage: procedure for hepatic hydrothorax. Ann Thorac Surg. 2009;87(1):245–50.
40. Drouhin F, Fischer D, Law Koune JD, et al. Treatment of hydrothorax in liver cirrhosis with chemical pleurodesis associated with continuous positive airway pressure ventilation. Preliminary results. Gastroenterol Clin Biol. 1991;15(3):271–2.
41. Lee WJ, Kim HJ, Park JH, et al. Chemical pleurodesis for the management of refractory hepatic hydrothorax in patients with decompensated liver cirrhosis. Korean J Hepatol. 2011;17(4): 292–8.
42. Medford AR, Bennett JA, Free CM, et al. Current status of medical pleuroscopy. Clin Chest Med. 2010;31(1):165–72.
43. Shaw P, Agarwal R. Pleurodesis for malignant pleural effusions. Cochrane Database Syst Rev. 2004;1:CD002916.
44. Lin DJ, Zhang M, Gao GX, et al. Thoracoscopy for diagnosis and management of refractory hepatic hydrothorax. Chin Med J (Engl). 2006;119(5):430–4.
45. Serste T, Moreno C, Francoz C, et al. The impact of preoperative hepatic hydrothorax on the outcome of adult liver transplantation. Eur J Gastroenterol Hepatol. 2010;22(2):207–12.
46. Xiol X, Tremosa G, Castellote J, et al. Liver transplantation in patients with hepatic hydrothorax. Transpl Int. 2005;18(6):672–5.
47. Porcel JM1, Mas E, Reñé JM, Bielsa S. Hepatic hydrothorax: report of a series of 77 patients. Med Clin (Barc). 2013;141(11):484-6

Bangladesh Journal of Hepatology
Vol. 3 No. 1 31
Current strategies in the management of hepatocellular carcinoma
Premashish Kar, Department of Gastroenterology & Hepatology, Max Superspeciality Hospital, New Delhi, India
Corresponding authorDr. Premashis Kar
Retd Director and Professor of MedicineMaulana Azad Medical College, Dipu Bharali
E-mail: <[email protected]>
Introduction:
Hepatocellular carcinoma (HCC) is considered to be the 5th commonest cancer and also considered an important cause of death all over the world, more so in Asia and Africa (1). The regions with hepatitis B and C virus infection are considered to be endemic areas and are considered to be more prone to HCC where in those areas HCC is extremely common (2). India belongs to an endemic zone for hepatitis B virus infection but the representative data on epidemiology of HCC in India is very scanty. The cancer registries in India are mostly urban (3). Etiology:
The Comprehensive analyzed data for HCC occurrence in India has not been established yet. HCC occurs in the age range of 40- 55 years and above 60 years in India (3, 4). Eighty per cent of all HCCs occurring in India occur with cirrhosis of liver in the background and 60% of all these cases are hepatitis B positive carriers (5, 6). The estimated number of cases as well as mo1iality per year in India is approximately close to 22,000 has been suggested (3). 45 million people who are suffering from chronic Hepatitis B virus (HBV) infection and approximately 15 million people who are afflicted with chronic Hepatitis C virus (HCV) infection in India (7). HBV and HCV infection is considered an important etiologic factor in HCC. Positive association between HCC and consumption of alcohol where alcohol contribute as a cofactor for hepatotoxins and hepatitis viruses (7). Aflatoxin contamination in the diets, Hepatitis B virus infection and liver cirrhosis in Andhra Pradesh, India and direct chronic exposure to aflatoxins was shown to cause liver cirrhosis. Cirrhosis of liver of any cause lead to develop about 70%-90% of HCC. Aflatoxin interacts synergistically with Hepatitis B virus
(HBV)/Hepatitis C virus (HCV) infection which increases the risk of HCC. HBV infection, HBV infection with Aflatoxin exposure, viral infection and alcohol consumption leading to overt cirrhosis of the liver, alcohol consumption leading to cirrhosis of the liver with viral infection are the predominant risk factor for the development of HCC. HCV and alcohol are also associated with HCC in India. Indians develop diabetes at younger age, Asians have strong genetic susceptibility for type II diabetes. Diabetes mellitus is identified as a risk factor for HCC. Prevention of viral infection by universal vaccination against hepatitis virus, HCC surveillance program, preventing alcoholic liver diseases, fungal contamination of grains and ground crops to prevent basically Aflatoxin exposure are important measures to prevent liver diseases and HCC among those at risk. In India, 70% to 80% of all HCCs are related to the hepatitis B virus (HBV), approximately 15% are related to hepatitis C virus (HCV), and 5% to both HBV and HCV (3). Alcohol alone accounts for approximately 8% of all HCCs. In about 10%, no direct etiology is seen. Iron overload and Aflatoxin may have a role to play in some geographical areas in India (3, 6). The prevalence of hepatitis Bin India varies between 0.2 to 1.6 per 100,000; 2.77 for males and 1.38 for females. This relative low prevalence is due to an under-reporting of the disease, thus India erroneously falls in the low incidence zone (3, 8). The under-reporting of HCC is possibly due to non-surveillance of chronic hepatitis B patients and carriers, and cirrhotic patients (3, 8). This also attributes to majority of cases being diagnosed at a late stage of the disease. The majority of patients with a viral etiology have a silent course, picked up by foeto-matemal transfusion.
Brief Review

32
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Clinical features:
The mean age of presentation of HCC was found in higher age groups peaking around 45 to 55 years (5, 9). Hepatitis B positive patients in the age group below 14 years were described to be present of HCC occurrence (10). The duration of symptoms of HCC was usually detected from five months to almost a year of occurrence. 90% of patients were symptomatic at diagnosis and 15% of these patients were diagnosed after one year of symptoms. The clinical presentations commonly seen are anorexia, fever (11). Worldwide distribution of HCC is predominated by males compared to females in the ratio of 5:1 (6). 10% to 15% cases are found to have liver cirrhosis found during diagnosis. Out of 70% of the total patient population was with liver cirrhosis in which 60% were found to be developed to HCC. 50% cases were found to be presence of hepatic decompensation while 5% of patients presenting with encephalopathy. Hematemesis and melena occur in 25% (6, 10, 12) of patients.
Weakness, anorexia, abdominal pain, weight loss, ascites with jaundice, fever and gastrointestinal bleeding are common symptoms. Patients present commonly with hepatomegaly, pallor, edema, and clubbing (in about 20%). Massive hepatomegaly is seen in about 50% of patients. The enlarged liver is usually firm to hard. Approximately 15% of patients do not have an enlarged liver. About 60% of patients present with ascites while worsening of ascites occurs in about 20%. Sometimes fever, leukocytosis and recurrent hypoglycemia occur as a paraneoplastic syndrome (13, 14).
Management
Treatment management of HCC patients was different for different conditions depend on to various factors such as patient factors, socioeconomic factors, etiological and the disease status. All modern facilities required for the treatment and management of HCC patients should be demanded basically in rural areas while in tertiary hospitals of urban areas those facilities are available, but in rural areas such facilities are scanty. Resection and hepatic transplants are available for surgical therapy and only applicable in early stage of HCC disease in a few centers. Therapy occurs possibly in less than 1 in 10,000 patients and liver transplants were done in five to six cases in India. The deterrent
factors are cost, availability and patients' ability to withstand (6). Radio frequency ablation (RFA) is available in very few centers while RFA may have similar results as hepatic resection in properly selected cases (6, 14). Use of trans-arterial chemoembolization (TACE) or RFA is available in some centers, but these are extremely small in number. No organized data is available. Counseling and discussion of HCC with experts might encourage in awareness of the HCC disease management and treatment in certain early cases (4, 6).
There is no established standard chemotherapy for HCC for advanced HCC although sporadic use of doxorubicin, interferon and thalidomide is available but not organized systematically and practically. There are options of targeted therapy for HCC. The drug commonly used is Sorafenib and the benefit of this drug seems to be around four months more than the Best Supportive Care (15). All patients are usually offered Best Supportive Care, which includes management of ascites, nutritional manipulation, treatment of co-morbidities and prevention of deterioration of hepatic functions which includes the anti-virals for hepatitis B and hepatitis C. Prevention of hepatitis B and hepatitis C, which are predominant causes of HCC, is the primary prevention for HCC. Pegylated interferon alfa and the anti-viral drug ribavirin based on the type of HCV genotype is followed for management of hepatitis C. Most often single drug pegylated interferon is used and viral control is seen in 80%. For hepatitis B lamivudine is usually used as a single drug. 65% per cent of the patients have control of hepatitis B proliferation (14, 16). Neonatal vaccination of HBV has decreased not only the prevalence of HBV carriers (17) but also the incidence of HBV related HCC. Increasing awareness of blood bone infection control can also bring down the incidence of hepatitis B and hepatitis C. Therapeutic use of interferon and antiviral in chronic infections of hepatitis can bring down the incidence of viral hepatitis induced HCC (18, 19).
Summary
Prognosis, diagnosis, treatment and management of HCC in India is very critical and challenging. Since routine tests for screening of HCC are not followed to perform in developing countries such as India therefore the advanced HCCs are common at diagnosis. It is

Bangladesh Journal of Hepatology
Vol. 3 No. 1 33
imperative to develop effective and affordable therapy and treatment strategies for such advanced disease. There is no systemic chemotherapy other than application of drug Sorafenib which has shown survival benefit. Multimodality approach is the need of the hour and has shown much better survival benefit, in single modality, in developed countries. Researchers need to unravel the underlying hepato-carcinogenesis and key molecular targets for development of more effective chemotherapy agents to improve survival in advanced HCC. Vaccination against hepatitis B and antivirals for hepatitis B and hepatitis C in chronic state, screening program as well awareness program for early diagnosis of HCC are the challenging tasks in the field of hepatology science for developing countries.
References:
1. S Ashtari, Md A Pourhoseingholi, A Sharifian, and Md R Zali; Hepatocellular carcinoma in Asia: Prevention strategy and planning; World J Hepatol. 2015 Jun 28; 7(12): 1708-1717
2. H B El-Serag; Epidemiology of Viral Hepatitis and Hepatocellular Carcinoma; Gastroenterology. 2012 May; 142(6): 1264-1273.el.
3. Durga R, Muralikrishna P. Viral markers in hepatocellular carcmoma. Indian J Gastroenterol1994;13:A57.
4. Indian Association for Study of the Liver (INASL). Hepatitis B in India: Therapeutic options and prevention strategies - Consensus statements. Indian J Gastroenterol 2000;19:54-74.
5. Melbye M, Skinh0j P, Nielsen NH, et al. Virus-associated cancers in Greenland: frequent hepatitis B virus infection but low primary hepatocellular carcinoma incidence. J Natl Cancer Inst 1984;73:1267-72.
6. Kumar R, Saraswat MK, Sharma BC, et al. Characteristics of hepatocellular carcinoma in India: a retrospective analysis of 191 cases. QJM 2008;101:479-85.
7. KarP; Risk Factors for Hepatocellular Carcinoma in India; J CLIN EXP HEPATOL 20I4;4:S34- S42.
8. Parkin DM. The global health burden of infection-associated cancers in the year 2002. Int J Cancer 2006;118:3030-44.
9. Javid G, Khan BA, Shah A, et al. Hepatocellular carcinoma mimicking liver abscess. Indian Pediatr 1998;35:1126-9.
10. Singh SV, Goyal SK, Chowdhury BL. Primary carcinoma of liver in Udaipur. J Assoc Physicians India 1971;19:693-5.
11. Saini N, Bhagat A, Sharma S, et al. Evaluation of clinical and biochemical parameters in hepatocellular carcinoma: experience from an Indian center. Clin Chim Acta 2006;371:183-6.
12. Agarwal AK, Manvi KN, Mehta JM, et al. Clinical diagnosis of hepatoma. J Assoc Physicians India 1966;14:465-8.
13. Bruix J, Sherman M, Llovet JM, et al. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol2001;35:421-30.
14. Sarin SK, Thakur V, Guptan RC, et al. Profile of hep:;tocellular carcinoma in India: an insight into the possible etiologic associations. J Gastroenterol Hepatol2001;16:666-73.
15. G.S.Bhattacharyya, K.G. Babu, H. Malhotra, A. A. Ranade, S. Murshed, D. Datta; Hepatocellular carcinoma in India; Chin Clin Onco/2013;2(4):41.
16. Kumar A, Sreenivas DV, Nagarjuna YR. Hepatocellular carcinoma. The Indian scenario. Indian J Gastroenterol1995;14:A95.
17. Chadha MS, Arankalle VA. Ten-year serological follow up of hepatitis B vaccme recipients. Indian J Gastroenterol 2000;19:168-71.
18. Chang MH, You SL, Chen CJ, et al. Decreased incidence of hepatocellular carcinoma in hepatitis B vaccinees: a 20-year follow-up study. J Natl Cancer Inst 2009;101:1348-55.
19. Morgan RL, Baack B, Smith BD, et al. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med 2013;158:329-37.

34
Bangladesh Journal of Hepatology
Vol. 3 No. 1
A case of occult hepatitis B virus infection and hepatocellular carcinoma from Bangladesh
Ponkaj Kumar Naha1, Mamun-Al-Mahtab1, Sarkar Mohammad Shahadat Hossain1, Rokshana Begum1, Abul Hayet Manik1, Debraj Malakar1, Partho Pratic Roy1, Ayub Al Mamun1, Salimur Rahman1
1Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
Corresponding authorDr. Mamun Al Mahtab
Associate ProfessorDepartment of Hepatology, Bangabandhu Sheikh Mujib Medical university, Dhaka, Bangladesh.
E-mail: <[email protected]>
Introduction:
HBV infection remain a major public health problem worldwide with more than 350 million people chronically infected and about 600000 related death annually. HBV infection has five different clinical categories; asymptomatic, acute, chronic, fulminant, OBI. OBI is characterized by the presence of HBV viral genome in the patients liver, but no virus surface Ag (HBsAg) detected in serum by commonly used immunoassays. HCC may develop in HBsAg negative patient accounted for 15.9% of all liver cancer patients. A study in Bangladesh found that HBV DNA was detected in several group of patients where HBsAg was negative.
Case report:
Thirty six years aged Mr. Abdur Rahim, a garments product manager, normotensive, nondiabetic, smoker, nonalcoholic, presented with upper abdominal pain associated with anorexia and weight loss. He also had abdominal swelling for 1 month, but no history of
altered consciousness, oliguria, haematemesis and melaena, altered bowel habit, any nodular swelling of body, fever, cough, breathlessness during his illness. He had past H/O jaundice 15 years back. On examination, patient was non icteric, abdominal exam revealed tender hepatomegaly and ascites. Investigation report revealed normal LFT, but enlarged coarse liver with mild ascites on USG. The triphasic CT scan of HBS showed characteristic feature of HCC and AFP >200000 ng/ml. Regarding viral marker only Anti HBc(T) is positive, other viral markers are negative. Ascitic fluid study showed high SAAG with low protein. Above all evidences were suggestive of HCC on the back ground of cirrhosis of liver.
Discussion:
The Hepatitis B virus is an enveloped and double strand relaxed circular DNA virus that belong to the family Hepadna viridae. HBsAg is formed through several pathways in the life cycle of HBV and the virus cccDNA(Covalently close circular DNA) is used as template. HBsAg level in serum are associated with the
Abstract
Hepatitis B virus (HBV) is the major causative agent of chronic hepatitis, hepatic decompensation, liver cirrhosis and hepatocellular carcinoma (HCC). HBV related serum markers are widely used in clinical diagnosis and prognosis of HBV infection. Serum HBsAg is regarded as the sole marker for HBV infection. But negative result for serum HBsAg test do not always represent a clearance or inactivating status of HBV infection, rather HCC can still develop in the absence of detectable HbsAg in serum. The situation is called occult HBV infection (OBI). Here we reported a case of 36 years old patient attended Hepatology OPD, BSMMU with abdominal pain for 3 month. After evaluation he was diagnosed as a case of HCC due to OBI based on high AFP (>20000ng/ml), suggestive triphasic CT scan of HBS and positive anti HBc(T), detectable HBV-DNA but negative HBsAg in serum.
Case Reports

Bangladesh Journal of Hepatology
Vol. 3 No. 1 35
level of active cccDNA. 1HBV viruses in HBsAg negative patients usually have higher genetic diversity and higher mutation frequency than HBsAg positive patients. Many type of mutation are only found in HBsAg negative patients, but not in HBsAg positive patients. So HBsAg specific antibody cannot recognize and bind to the surface antigen. The wide application of HBV vaccination and to antiviral treatment increase the chance of viral mutation.2 3 The reason of negative HBsAg in serum may be for low specificity and sensitivity of the reagents for detecting HBsAg, co-infection with HCV and HIV, disruption of HBV gene during integration into the chromosomal DNA in host hepatocyte, deamination and methylation of HBV genome.4 5 6 HBV DNA can present in the hepatocytes either by integration into host cell genome remaining a free epsomes. The integration itself could trigger carcinogenesis by activating other genes.7 8 9 The occult virus infection may be mild but continuous necroinflamation in the liver could provoke repeated cycles of apoptosis, necrosis and complementary regeneration. All these reaction in liver contribution to the progression toward cirrhosis and HCC.7
Conclusion:
OBI is attributing to the long lasting presence of HBV cccDNA in the hepatocyte. So there is risk of cancer development in OBI patients .There is a pressing demand for accurate diagnosis of OBI for effectively prevent the development of HCC.
References:
1. Werie-Lapostolle B, Bowden S, Lacornini, Wursthorn K, Petersen J, Lau G, Trep C, Mercellin P, Goodman Z, Delaney WET, Xiong S, Brosgart CL, Chen SS, Gibbs CS, Zoulim F. Persistence of cccDNA during the natural history of chronic hepatitis B and decline during adefovir dipivoxil therapy. Gastroenterology 126(7): 1750-1758, 2004.
2. Lee KM, Kim YS, Ko YY, Yoo BM, Lee KJ, Kim JH, Hahm KB, Cho SW. Emergence of vaccine – induced escape mutant of hepatitis B virus with multiple surface gene mutation in a Korean child. J Korean Med Sci. 16(3):359-362, 2001.
3. Louisirirotchanakul S, Kanoksinsombat C, Theambooniert A, Puthavatana P, Wasi C, Poovorawan Y. Mutation of the “a” determinant of HBsAg with discordant HBsAg diagnostic kits.Viral Immuunol 17(3):440-444, 2004.
4. Chen CY, Wu JR, Wang SY. [Occult hepatitis B virus infection] Zhonnghua Gan Zang Bing Za Zhi 13(11): 873-875, 2005.
5. Huang FY, Wong DK, Seto WK, Zhang AY, Lee CK, Lin CK, Fung J, Lai CL, Yuen MF. Sequence variations of full-length hepatitis B virus genomes in Chinese patients with HBsAg-nagative hepatitis B infection. Pios One 9(6):e99028, 2014.
6. Raimondo A, Pollicino T, Romano L, Zanetti AR. A 2010 update on occult hepatitis B infection. Pathol Biol 58(4):254-257.2010.
7. Elmore LW, Hancock AR, Chang SF, Wang XW, Chang S, Collahan CP, Geller DA, Will H, Harris CC. Hepatitis B virus X protein and p53 tumour suppressor interaction in the modulation of apoptosis. Proc Nati Acad Sci U S A 94(26): 14707-14712, 1997.
8. Mahmoud OA, Ghazal AA, Metwally Del S, Elnor AM,Yousif GE. Detetion of occult hepatitis B virus infection among blood in Sudan. J Egypt Public Health Assoc 88(1), 2013.
9. Ohba K,Kubo S, Tamori A, Hirohashi K, Tanaka H, Shuto T, Nishiguchi S, Kinoshita H. previous or occult hepatitis B virus infection in hepatitis B surface antigen-negative and anti hepatitis C negative patients with hepatocellular carcinoma. Surg Today 34(10):842-848, 2004.

36
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Association of portal vein tumor thrombus in hepatitis B related hepatocellular carcinoma
Abu Saleh Mohammad Sadequl Islam1, Mamun Al Mahtab2, Ayub Al Mamun2, Sheikh Mohammad Fazle Akbar3, Mohammad Kamal Hossain1, Zia Hayder Bosunia4, Salimur Rahman2
1Department of Medicine, SZR Medical College Hospital, Bogra, Bangladesh. 2Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. 3Department of Medical Sciences, Toshiba
General Hospital, Tokyo, Japan, 4Department of Hepatology, Rangpur Medical College Hospital, Rangpur, Bangladesh.
Abstracts of LIVERCON 2016
Background:
The highest incidence of Hepatocellular carcinoma (HCC) is in Asia, accounting for about 76% of all cases worldwide. In South East Asia, hepatitis B is the most common underlying cause.HCC is the sixth most common type of cancer and the third highest cause of cancerrelated mortality worldwide. HCC exhibits intense neoangiogenic activity during its progression. In the early stages the tumor is not highly vascularized and its blood supply comes from the portal vein. However, as the tumor grows the blood supply becomes progressively arterialized.11% to 42% of patients with HCChave to invasion the portal venous system, which results in portal vein tumor thrombus (PVTT). To find out the relationship ofportal vein tumor thrombus (PVTT) with the hepatitis B-related hepatocellular carcinoma.
Methods:
This observational study was carried out in the Department of Hepatology, BSMMU from January 2012 to December 2013. The study was approved by the Ethical Institutional Review Board (IRB) of BSMMU, Dhaka. The diagnosis of HCC was confirmed by pathological examination or AFP elevation (400ng/ml) combined imaging (CT/MRI) and diagnosis of PVTT was made by non-enhanced and contrast-enhanced (10
mm slice thickness) multi-detector CT (MDCT). All CT images were evaluated by 2 trained radiologists by consensus after exclusion of hepatitis C virus infection (Anti HCV+ve) and significant alcohol intake (>20 gm. /day). All patients were HBsAg positive done by ELISA test.
Results:
A total 44 patients were included in this study. Among them, 91% were male (n=40) and 09 % were female (n=4).The mean age was 48.2 (±12.9) years with range from 23 to 80. Maximum (50%) patient’s ages were belonged to 35-54 years. Urban was found 23 (52.3%). Cirrhosis was 79.5% (n=35) and no cirrhosis was found 20.5% (n=9).PVTT was found 40.9% (n=18)and no PVTT was found 59.1% (n=26). Among cirrhosis and non-cirrhosis group, PVTT was 83% (n=15) and 17% (n=03) respectively.BCLC (Barcelona Cancer of the Liver Clinic) staging showed 100% (n=18) of patients were advanced and terminal stage (Stage C & D).Conclusions:Median survival time of patients with PV invasion was 2.7 to 4 months if left untreated, whereas the median survival time of patients without PV invasion was 24.4 months if left untreated. Detection of PVTT inHCC leads to extremely poor prognosis.

Bangladesh Journal of Hepatology
Vol. 3 No. 1 37
Metabolic syndrome is a good predictor for diagnosing non-alcoholic steatohepatitis.
Sheikh Mohammad Noor-E-Alam1, Ahmed Lutful Moben2, Zia Hayder Basunia3, Amalendu Bhattacharyya4, Abdur Rahim5, Syed Abul Foez6, Mohammad Shahed Ashraf1, Faiz Ahmad Khandoker1, Md. Jahangir Alam Sarker1, Abu Saleh Mohammad Sadequl Islam7, Mohammad Forhad Abedin8, Utpal Das Gupta9, Mohammad Jahangir Kabir2,
Mamun-Al-Mahtab10, Salimur Rahman10
1Department of Hepatology, Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh, 2Kurmitola General Hospital, Dhaka, Bangladesh, 3Rangpur Medical College, Rangpur, Bangladesh, 4Shere-E-Bangla Medical College Hospital, Barisal, Bangladesh, 5MATS, Noakhali, Bangladesh, 6250 Bed Hospital, Moulvibazar, Bangladesh
7SZR Medical College Hospital, Bogra, Bangladesh, 8Comilla Medical College Hospital, Comilla, Bangladesh, 9Ali Hospital, Dhaka, Bangladesh, 10Department of Hepatology, Bangabandhu Sheikh Mujib Medical University,
Shahbag, Dhaka, Bangladesh
Background:
Nonalcoholic fatty liver disease (NAFLD) is a metabolic liver disease that has become a worldwide public health concern. The conditions ranging from simple steatosis to nonalcoholic steatohepatitis (NASH), fibrosis, cirrhosis and end stage liver disease. To evaluate metabolic syndrome for diagnosing non-alcoholic steatohepatitis.
Methods:
An observational, cross sectional study was carried out in the Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. Patients of Metabolic syndrome having NAFLD on ultrasonography attending at outpatient and inpatient Departments of Hepatology were selected as cases. 43
patients underwent liver biopsy and NAFLD activity score (NAS) was assessed.
Results:
Metabolic syndrome was present in 79% of study population according to International Diabetes Federation 2006 criteria for South Asians and 55.9% metabolic syndrome patients presented with NASH. 95% NASH patients presented with metabolic syndrome. In this study presence of metabolic syndrome significantly correlated (p=0.01, chi-square test) NASH from non-NASH fatty liver.
Conclusion:
Metabolic syndrome can significantly predict NASH from non-NASH Fatty Liver.

38
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Upper gastrointestinal endoscopic findings in adults at Comilla Medical College & Hospital, Bangladesh
Mohammad Forhad Abedin1, Mohammad Asaduzzaman Lashkar2, Mohammad Shah Jamal3, Mohammad Belalul Islam1, Mohammad Izazul Haque4, Mohammad Abdur Rob Sarkar3
1Department of Medicine, Comilla Medical College Hospital, Comilla, Bangladesh, 2Department of Cardiology, Comilla Medical College Hospital, Comilla, Bangladesh, 3Department of Gastroenterology, Comilla Medical College Hospital, Comilla, Bangladesh, 4Department of Hepatology, Comilla Medical College Hospital, Comilla, Bangladesh
Background:
Endoscopy is a nonsurgical procedure used to examine a patient’s gastrointestinal tract. Fiber optic endoscopy is a highly efficient diagnostic tool, which is now being increasingly used in the diagnosis of GI diseases. This study has been carried out to demonstrate indications for and common findings of endoscopy in adults aging 15 years and above.
Methods:
We retrospectively reviewed the medical records for endoscopy indication and result of adults who had endoscopy between June 2014 and May 2005.
Results:
We analyzed 1283 adult aged 15 years or above who were referred for upper gastrointestinal endoscopy. There were 731 male and 552 female cases. Highest numbers of participants were in the age group of 25-34
(24.6%). The main indications comprised dyspepsia (49.66%), epigastric pain (29.63%), abdominal pain (7.025), hematemesis (6.12%), recurrent vomiting (3.67%), abdominal distension (2.26%) and others (1.64%). Endoscopic diagnoses included duodenal ulcer (9.6%), gastric ulcer (4.9%), Oesophagealvarices (6.8%), gastritis (5.6%),gastropathy (3.2%), Ca- stomach (2.7%),ca-oesophagus (1.3%), oesophagitis (1.5%), duodenitis (0.7%), pyloric stenosis (0.7%) and others (1.8%).
Conclusion:
Upper gastrointestinal endoscopy is a diagnostic procedure in adults, which is increasingly used in government medical college hospitals to explore the upper GI pathologies i.e.- duodenal ulcer, gastric ulcer, ca- stomach and oesophagus, gastritis, gastropathy and oesophagealvarices.

Bangladesh Journal of Hepatology
Vol. 3 No. 1 39
Causes of jaundice in clinical practice: An observation at Brahmanbaria
Forhad Hossain Mohammad Shahed1, Mamun Al Mahtab2, Mohammad Fakhrul Islam Khaled1, Mohammad Abul Fayaz1, Ashiqur Rahman Khan1
1250 Bedded District Sadar Hospital, Brahminbaria, Bangladesh 2Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
Background:
Jaundice remains the commonest mode of presentation of liver disease. Identification of the cause at first medical contact is the basis of starting treatment. There is scarcity of study elaborating the common causes of jaundice in Bangladeshi people. We evaluated 100 patients presenting with jaundice at Brahmanbaria, a district of Bangladesh to know aetiologies.
Method:
We performed this observational study on Patients attending with the complaint of jaundice to the private chamber of the only hepatologist at this district from January 2015 to September 2015. Data from 100 patients were collected and analyzed to know cause of jaundice and its relation with age & sex of these patients.
Result:
Mean±SD of age of the patients was 28.24±21.57, 57.6% were male. In 73% cases the cause was
infectious, with Hepatitis B Virus (HBV) 44%, Hepatitis C Virus (HCV) 30%, Hepatitis A Virus (HAV) 30%, Hepatitis E Virus (HEV) 26%. Mean±SD of age was 19.7±2.7 in infectious group. Alcoholic liver disease was in 5% cases. Obstruction with gall stone was in 5% cases, Carcinoma of gall bladder (CaGB) in 5%, cholangiocarcinoma in 3%, Carcinoma liver in 1.6% and Carcinoma pancreas in 11.8% cases. Among the CaGB & cholangiocarcinoma patients 16% had gall stone. Mean±SD of age in malignant patients was 62.52±4.9 with 75% female.
Conclusion:
We observed that viral hepatitis was common in younger age and malignancy in older age. Most of the study subjects were male whereas malignancy was more common in female. HAV infection was more in pediatric age. Majority of hepatits were HBV related. Among the patients with CaGB & cholangiocarcinoma 16% had gall stone.

40
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Non favorable genotype is predominant at IL28B rs12979860 polymorphism in hepatitis B related hepatocellular carcinoma
Abu Saleh Mohammad Sadequl Islam1, Mamun Al Mahtab2, Ayub Al Mamun2, Sheikh Mohammad Fazle Akbar3, Mohammad Eunus Ali4, Zia Hayder Bosunia5, Salimur Rahman2
1Department of Medicine, SZR Medical College Hospital, Bogra, Bangladesh, 2Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh, 3Department of Medical Sciences, Toshiba
General Hospital, Tokyo, Japan, 4Department of Microbiology & Immunology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh, 5Department of Hepatology, Rangpur Medical College, Rangpur, Bangladesh.
Background:
The highest incidence of HCC is in Asia, accounting for about 76% of all cases worldwide. In South East Asia, hepatitis B is the most common underlying cause. Although numerous associations between environmental factors (e.g. cigarette smoking, heavy alcohol drinking, male gender, older age), viral factors (e.g. viral load, active replication, genotype, core promoter mutations) and the development of HCC in chronic HBV infection have been identified, a clear understanding of the role of host genetics remains illusive. Bangladesh is a densely populated country with about 160 million populations, where HBsAg positivity in the healthy population is 5.4%. To evaluate the role of host IL28B (interleukin 28B; interferon lambda 3) single nucleotide polymorphism (SNP) in predicting hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC) susceptibility.
Methods:
Single SNP in the IL28B gene (rs12979860C/T) were examined in 116 subjects (including 44 HBV-related HCC patients, 42 non-HCC patients with chronic hepatitis B and 30 healthy controls). The study was
done at the Department of Hepatology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka from January 2012 to December 2013.The polymorphism of IL28B rs12979860 was analyzed by a genotyping technique, based on polymerase chain reaction (PCR) followed by restriction enzyme analysis at the Department of Microbiology & Immunology, BSMMU.
Results:
The frequency of CC homozygosity was 70% in healthy controls and 45.5% in HCC, the difference being statistically significant (χ2=4.35, P=0.03). Statistically significant difference was also seen between non-HCC patients with chronic hepatitis B (CHB) (69%) and HCC (45.5%) (χ2=4.35, P=0.03). However, this significant finding was not seen between non-HCC patients with chronic hepatitis B (CHB) and healthy controls. Carriers of the minor T allele in rs12979860 had a higher risk of HCC compared with non-carriers (χ2=4.78, P=0.02). Conclusions: Our results suggest that, T allele and non-CC genotypes have strong predictive effect of developing HCC and IL28Brs 12979860 C/T polymorphism might influence susceptibility to HCC.

Bangladesh Journal of Hepatology
Vol. 3 No. 1 41
Professor Baruch Samuel BlumbergBaruch Samuel "Barry" Blumberg (July 28, 1925 – April 5, 2011), was an American doctor and co-recipient of the 1976 Nobel Prize in Physiology or Medicine (with Daniel Carleton Gajdusek), and the President of the American Philosophical Society from 2005 until his death.
Blumberg received the Nobel Prize for "discoveries concerning new mechanisms for the origin and dissemination of infectious diseases." Blumberg identified the Hepatitis B virus, and later developed its diagnostic test and vaccine.
Early life and education
Blumberg was born in Brooklyn, New York. He first attended the Orthodox Yeshivah of Flatbush for elementary school, where he learned to read and write in Hebrew and to study the Bible and Jewish texts in their original language. (That school also had among its students a contemporary of Blumberg, Eric Kandel, who is another recipient of the Nobel Prize in medicine.)
Blumberg then attended Far Rockaway High School in the early 1940s, a school that also produced fellow laureates Burton Richter and Richard Feynman. Blumberg served as a U.S. Navy deck officer during World War II. He then attended Union College in Schenectady, New York and graduated from there with honors in 1946.
Originally entering the graduate program in mathematics at Columbia University, Blumberg switched to medicine and enrolled at Columbia's College of Physicians and Surgeons, from which he received his M.D. in 1951. He remained at Columbia Presbyterian Medical Center for the next four years, first as an intern and then as a resident. He then began graduate work in biochemistry at Balliol College, Oxford and earned his Ph.D there in 1957.
Scientific career
1999 press conference at which Blumberg was introduced as the first director of the NASA Astrobiology Institute
Throughout the 1950s, Blumberg traveled the world taking human blood samples and studying the inherited variations in human beings, focussing on why some people contracted diseases in similar environments that others did not. In 1964, while studying yellow jaundice, he discovered a surface antigen for hepatitis B in the blood of an Australian aborigine. Blumberg and his team were able to develop a screening test for the virus
Life Sketch of Professor Baruch Samuel Blumberg

42
Bangladesh Journal of Hepatology
Vol. 3 No. 1
to prevent its spread in blood donations and developed a vaccine. Blumberg later freely distributed his vaccine patent in order to promote its fielding by drug companies. Deployment of the vaccine reduced the infection rate of hepatitis B in children in China from 15% to 1% in 10 years.
Blumberg became a member of the Fox Chase Cancer Center in Philadelphia in 1964, and held the rank of University Professor of Medicine and Anthropology at the University of Pennsylvania starting in 1977. Concurrently, he was Master of Balliol College from 1989 to 1994. He was elected a Fellow of the American Academy of Arts and Sciences in 1994. From 1999 to 2002, he was also director of the NASA Astrobiology Institute at the Ames Research Center in Moffett Field, California.
In November 2004, Blumberg was named Chairman of the Scientific Advisory Board of United Therapeutics Corporation, a position he held until his death. As Chairman he convened three Conferences on Nanomedical and Telemedical Technology, as well as guiding the biotechnology company into the development of a broad-spectrum anti-viral medicine.
Beginning in 2005, Blumberg also served as the President of the American Philosophical Society. He had been first elected to membership in the society in 1986.
In October of 2010 Blumberg participated in the USA Science and Engineering Festival's Lunch with a Laureate program whereby middle and high school students of the Greater Washington D.C., Northern Virginia and Maryland area get to engage in an informal conversation with a Nobel Prize winning scientist over a brown bag lunch. Blumberg came to General George A.
McCall Elementary on Sept. 29, 2010 as part of the program.
In an interview with the New York Times in 2002 he stated that "[Saving lives] is what drew me to medicine. There is, in Jewish thought, this idea that if you save a single life, you save the whole world".
In discussing the factors that influenced his life, Blumberg always gave credit to the mental discipline of the Jewish Talmud, and as often as possible he attended weekly Talmud discussion classes until his death.
Death
Blumberg died on April 5, 2011, shortly after giving the keynote speech at the International Lunar Research Park Exploratory Workshop held at NASA Ames Research Center. At the time of his death Blumberg was a Distinguished Scientist at the NASA Lunar Science Institute, located at the NASA Ames Research Center in Moffett Field, California.
Jonathan Chernoff, the scientific director at the Fox Chase Cancer Center where Blumberg spent most of his working life said, "I think it’s fair to say that Barry prevented more cancer deaths than any person who’s ever lived." In reference to Blumberg's discovery of the Hepatitis B vaccine, former NASA administrator Daniel Goldin said, "Our planet is an improved place as a result of Barry's few short days in residence."
His funeral was held on April 10, 2011 at Society Hill Synagogue, where he was a long time member. The eulogy was delivered by his son-in-law Mark Thompson, the Director-General of the BBC.

Bangladesh Journal of Hepatology
Vol. 3 No. 1 43
Email from Professor Baruch Samuel Blumberg
Email received from Professor Baruch Blumberg endorsing “Blumberg Oration” introduced by Association for the Study of the Liver, Dhaka, Bangladesh
Delivered-To: [email protected]: RE: Blumberg Lecture in Dhaka on World Hepatitis day 2010.Date: Mon, 17 May 2010 00:32:29 -0400From: "Blumberg, Baruch" <[email protected]>
ToDr. Mamun-Al-MahtabSecretary GeneralAssociation for the Study of the Liver, Dhaka, Bangladesh
Dear Dr. Mamun-Al-Mahtab,
I am very pleased to know that the first Blumberg Lecture will be presented on World Hepatitis Day 2010 in Dhaka It is a great honor to have been selected by the Association for the Study of the Liver, Dhaka, Bangladesh and the Viral Hepatitis Foundation Bangladesh to have this important event include my name.
The research that resulted in the discovery of the hepatitis B virus and the invention of the vaccine conducted by my colleagues and me at the Fox Chase Cancer Center in Philadelphia. USA, started as an exercise in basic clinical research. We did not set out with the goal of finding HBV but rather to understand the nature of human protein genetic and environmental variation and how it relates to susceptibility to disease. However, we had the conviction, the faith, that we would in time find means to prevent and treat disease. When we recognized that we had discovered an important pathogenic virus, methods of detection, and a vaccine, we dedicated ourselves to these applications. Basic science is an effective means to discover new natural phenomenon and new medical applications.
HBV is prevalent world wide and the field work that was essential to the research was conducted in Asia, Africa, Europe, the Islands of the Pacific, the sub-Arctic as well as North and South America. In all of these places we had excellent cooperation with our international colleagues; the success of the project was dependent on them. Following our initial publications, scientists and physicians in many parts of the world greatly extended the understanding of the virus and the applications of research. It is gratifying that the results of all this research have benefited people worldwide. Disease does not know boundaries and cooperation between many nations has been effective in achieving widespread relief from sickness and death. World Hepatitis Day will greatly extend the benefits to those not yet included in effective programs, improve projects already in place, and increase knowledge about HBV and other infectious agents.
Congratulations to your organization in achieving this national and international campaign to help control HBV infection worldwide.
Sincerely yours,Baruch Blumberg

44
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Brief Introduction of Dr. Nagaraja Rao Padaki: Blumberg Orator 2016
Dr. Nagaraja Rao PadakiDr. Nagaraja Rao Padaki was best outgoing student of Kurnool Medical College. He was recipient of merit certificates and gold medals during undergraduate career. He was Sri Venkateswara University first in the final M.B.B.S. Dr.P.N.Rao is an alumnus (M.D and D.M.) of prestigious postgraduate medical institution in our country, the Post Graduate Institute of Medical Education and Research (PGI), Chandigarh. He served as Assistant Professor in Gastroenterology at Osmania Mediacl College, Hospital before becoming Professor of Gastroenterology at Nizams Institute of Medical sciences (NIMS) Hyderabad. Subsequently he was chief of Gastroenterology at Medwin Hospitals & Mediciti Hospitals, Hyderabad. He was Chief Gastroenterologist
at CARE hospitals Hyderabad with before taking up the current position of Chief of Hepatology and Nutrition at Asian Institute of Gastroenterology. He served as Governing Council Member for Indian Society of Gastroenterology, Indian Association for Study of Liver Diseases and Editorial Board Member for Indian Journal of Gastroenterology in the past. He is a visiting faculty at National Institute of Nutrition, Hyderabad. He is one of the founding members of Coalition for Eradication of Viral Hepatitis in Asia Pacific (CEVHAP) an NGO with members from all over the globe.
He is currently the founder and Honorary Secretary of Indian National Association for Study of the Liver (INASL) Andhra Pradesh chapter.
He has contributed chapters in API textbook, INASL monograms and original articles in basic research of HBV,HCV and NAFLD in peer reviewed journals
His fields of interest in Hepatology include non alcoholic fatty liver disease, alcoholic liver disease, hepatic hemodynamic studies, drug induced liver injury and nutrition.

Bangladesh Journal of Hepatology
Vol. 3 No. 1 45
Blumberg Orator, 2010Professor Mahmud HasanFormer Vice Chancellor, Bangabandhu Sheikh Mujib Medical University
President, Bangladesh Medical Association
President, Bangladesh College of Physicians & Surgeons
Chairman, Bangladesh Medical Research Council
President, Bangladesh Gastroenterology Society
Topic: Management of Hepatitis B: An Update
Blumberg Orator, 2011Professor Salimur RahmanProfessor of Hepatology, Bangabandhu Sheikh Mujib Medical University
Executive Council Member, Asia Pacific Association for the Study of the Liver
President, Association for the Study of the Liver, Dhaka, Bangladesh
Chairman, Viral Hepatitis Foundation Bangladesh
Senior Vice President, Association of Physicians of Bangladesh
Editor in Chief, Euroasian Journal of Hepato-Gastroenterology
Topic: Hepatitis B: from Blumberg to Bangladesh
Blumberg Orator, 2012Professor George K. K. LauClinical Trial Center
LKS Faculty of Medicine, The University of Hong Kong
Humanity and Health GI and Liver Clinic, Hong Kong, SAR
Topic: Hepatitis B research in Asia-Pacific region-past 5 decades and future
List of Blumberg Orators

46
Bangladesh Journal of Hepatology
Vol. 3 No. 1
Blumberg Orator, 2013Professor Subrata K. Acharya Head, Department of Gastroenterology
All India Institute of Medical Sciences (AIIMS)
New Delhi, India
Topic: Ammonia in acute liver failure: It’s role in pathogenesis, prognosis and implication in medical therapy
Blumberg Orator, 2015Dr. Pietro LamperticoAssistant Professor
Gastroenterology and Hepatology Division
University of Milan, Italy
Topic: HBV-An overview

Bangladesh Journal of Hepatology
Vol. 3 No. 1 47
Guideline for Authors
Submission of Papers
Manuscripts for Bangladesh Journal of Hepatology are to be submitted by e-mail. This is the preferred method of submission and facilitates early processing of manuscripts. In exceptional cases where there is no email access, authors may submit one original copy of the manuscript with a soft copy on disk.
Authors may submit, their manuscripts on Hepato-Pancreato-Biliary diseases with their names and full contact details, including e-mail address.
It is the author’s responsibility to ensure that papers are written in clear and comprehensible English. Authors whose native language is not English are strongly advised to have their manuscripts checked by an English speaking colleagues prior to submission.
Submission of a paper implies that it has not been published previously (except in the form of an abstract or as part of a published lecture or academic thesis), that it is not under consideration for publication elsewhere, that it’s publication is approved by all authors and that, if accepted, it will not be published elsewhere in the same form, in English or in any other language, without the written consent of the Publisher.
Types of ContributionsOriginal research paper, review article, case report, rapid communication, short communication, letter to Editor and book review.
1. Research paper: Original full length research papers not exceeding 8,500 words (including allowance for no more than 6 tables and illustrations).
2. Review article: - With focus on literature published over the previous fi ve years and not exceeding 12,000 words (including allowance for no more than 6 tables and illustrations).
3. Case report: Interesting case reports of Hepato-Pancreato-Biliary diseases.
4. Rapid communication: Original research papers reporting signifi cant scientifi c results or findings with signifi cant implications.
5. Short communication: Short communications of upto 3500 words, describing works that may be of a preliminary nature, but which merits immediate publication.
6. Letter to the Editor: Letters will be considered for publication from time to time.
7. Book review: Review of books on Hepato-Pancreato-Biliary diseases will be published.
Manuscript PreparationGeneral: Manuscripts must be type-written, double-spaced with wide margins on one side of white paper. Each page must be numbered. Font size of 12 point is required. The corresponding author should be identifi ed including fax number and email address. Institutional affi liation must be given for all co-authors. The Editors reserve the right to adjust style to certain standards of uniformity. Authors should retain a copy of their manuscript since we cannot accept responsibility for damage or loss of papers. Original manuscripts will be discarded one month after publication.
Abstracts: Each paper should be provided with an abstract of 100-150 words.
Keywords: 3-5 words characteristic of the manuscript.
Text: Please follow this order when typing manuscripts: title, authors, affi liations, abstract, keywords, main text, acknowledgements, appendix, references, fi gures and then tables. Please do not import fi gures or tables into your text. The corresponding author should be identifi ed with an asterisk and footnote. The title of the paper should unambiguously refl ect its contents. A suggestion for an abbreviated running title should be given.
Units: The SI system should be used for all scientific and laboratory data; if in certain instances, it is necessary to quote other units, these should be added in parentheses. Temperatures should be given in degrees Celsius.
Symbols: Abbreviations for units should follow the suggestions of the British Standards publication (BS

48
Bangladesh Journal of Hepatology
Vol. 3 No. 1
1991). The full stop should not be included in abbreviations, e.g. ppm (not p.p.m.), % and / should be used in preference to ‘per cent’ and ‘per’. Where abbreviations are likely to cause ambiguity or may not be readily understood by an international readership, units should be put in full.
Current recognized chemical nomenclature should be used, although commonly accepted trivial names may be used where there is no risk of ambiguity. The use of proprietary names should be avoided. Papers essentially of an advertising nature will not be accepted.
References: All publications cited in the text should be presented in a list of references following the text of the manuscript. No more than 50 references should be cited in the manuscript. In the text please refer to the
number cited. The list of references should be arranged according to the citation by author’s names and should be as full as possible, listing all authors, the full title of articles and journals, publisher and year.
References should be given in the following form:
Mahtab MA, Kumar S, S Rahman, Aggarwal R. Genotypes of hepatitis B virus: fi rst report of coinfection between genotypes C and D from the Indian sub-continent. Arab J Gastroenterol 2006; 7(3): 35-37.
Mahtab MA, Kumar S, Rahman S, Khan M, Aggarwal R. Genotypes of hepatitis B virus in Bangladeshi population. Proceedings of the 16th Conference of the Asian Pacifi c Association for the Study of the Liver, Manila, Philippines, 2006; 45-48.
Correspondence to Bangladesh Journal of Hepatology:
Dr. Mamun-Al-MahtabAssociate Professor of HeptologyBangabandhu Sheikh Mujib Medical UniversitySecretary General, Association for the Study of the Liver, Dhaka, Bangladesh
Address:Room # 506 (4th fl oor), Bangabandhu Sheikh Mujib Medical University, Kazi Nazrul Islam Avenue, Shahbag,Dhaka-1000, Bangladesh. Tel. +880-2-8621142, Email: [email protected], [email protected]

• LabAid Pharma
• Incepta Pharmaceuticals Ltd
• Square Pharmaceuticals Ltd.
• Healthcare Pharmaceuticals
• Opsonin Pharma Limited
• Aristopharma Ltd
• Beacon Pharmaceuticals Ltd.
• Beximco Pharma
• Julphar Bangladesh
• General Pharmaceuticals Ltd.
• Eskayef Bangladesh Limited
• ACI Pharmaceuticals
• Renata Limited
• Drug International Limited
• The ACME Laboratories Ltd.
• Sun Pharmaceutical Bangladesh Ltd
• M/s Swadesh
• Mundipharma (Bangladesh) Pvt. Ltd
• Ziska Pharmaceuticals Ltd
• Popular Pharmaceuticals Ltd
• NIPRO JMI Pharma Ltd
• Welhealth Pvt. Limited
List of Sponsors

Association for the Study of Liver Diseases Bangladesh(National Association of Hepatologists of Bangladesh)
ASSOCIATION FOR THESTUDY OF LIVER
DISEASESBANGLADESH