Embed Size (px)
Citation preview
Low Back Pain in Athletes: Flexion or Extension?
Terri L. Szajnuk, MPT River v&eY Rehabilitation, Pittsburgh John Norwig, MEd, ATC, Column Editor
$2
-.J i he human spine is the foun- dation from which all movement occurs. Although low back pain does not typically command cen- ter stage for athletic injuries, the literature suggests that some 55% of all athletes will sustain at least one spinal injury during their sports career. The sports with the highest incidence of spinal injuries (Malone, 1989, Sports Injury Man- agement: Back Injuries and Rehab ilitation, Williams & Wilkins), in order from highest to lowest, are the following:
gymnastics football racquet sports wrestling equestrian events rugby weightlifting
Although most low back pain experienced by athletes will be self-limiting and will not require medical intervention, some spinal injuries will inhibit participation from the sporting event and re- quire aggressive rehabilitation.
The first step in treating the athlete with low back pain should be that of determining an accurate diagnosis through evaluation and assessment. The types of spinal injuries typically incurred by ath- letes may include the following:
connective/contractile tissue injuries (sprains, strains) spinal fractures spinal stenosis facet syndrome sacroiliac involvement intervertebral disc disorders spondylolysis spohdylolisthesis contusions
These various diagnoses tend to present themselves with fairly predictable symptoms. Based on the etiology of the symptoms, most ath- letes will describe a preference for either flexion or extension postures. This positional preference has been referred to in the literature as a "flexion/extension bias" (Biondi, 1991, Functional Stabilization Train- ing Northeast Seminars).
For example, athletes who report sleeping prone or supine with the legs extended would be describing a preference for extension. These same athletes are likely to prefer standing/ walking activ- ities, and kneel- ing/quadruped posi t ions ,be- cause in such
positions there is an extension mo- ment to the spine. On the other hand, athletes with a flexion pref- erence tend to sleep in the fetal position or supine with the knees flexed. These athletes tolerate half-kneeling well and tend to stand leaning onto a support or with a foot propped up.
Anatomically speaking, a flexion/extension bias describes the athlete's open-packed position of the spine. This is the position in which the spine undergoes the least amount of compressive forces and stresses and thus is the position of most comfort. This is also the position of maximum stability and efficiency of spinal movement.
Each low back injury will tend to place the athlete into one of these biases, based on the nature of the pathology. For example, spondylolisthesis, facet syndrome,
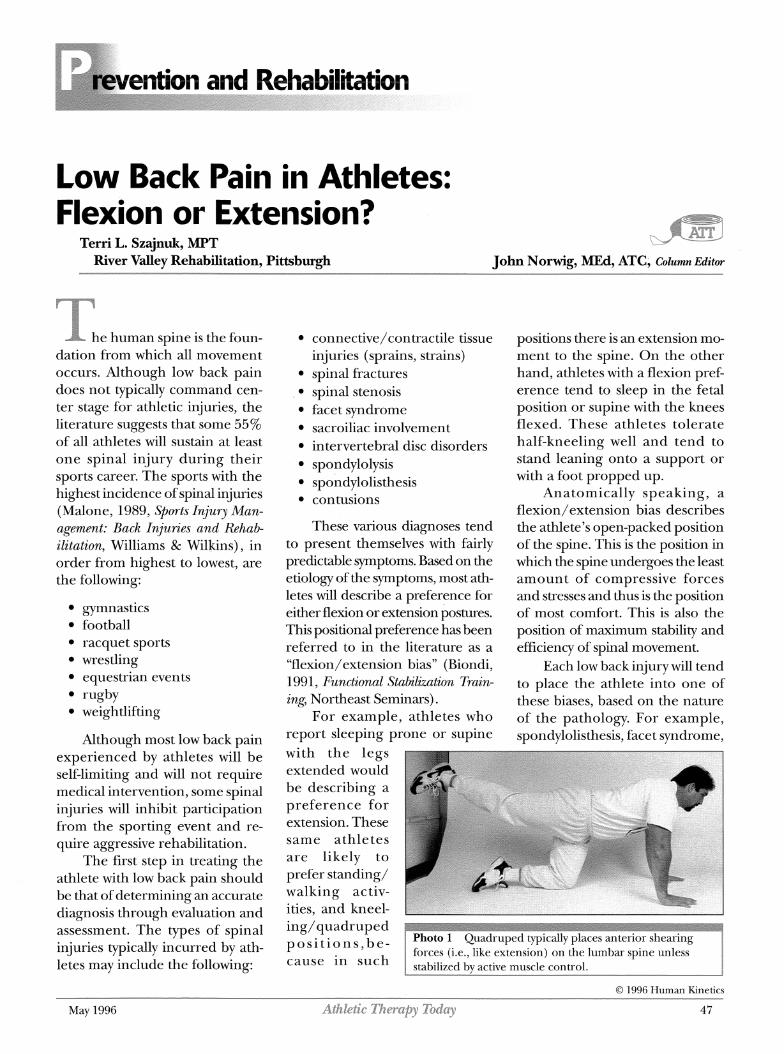
Photo 1 Quadruped typically places anterior shearing
O 1996 Human Kinetics
May 1996 AthbEic 17twapy Today 47

and spinal stenosis will typically present as a flexion bias. On the other hand, intervertebral disc disorders will tend to present as an extension bias. After determining whether the athlete is following a flexion or extension bias, you should develop the rehabilitation program accordingly.
Based on the principles cited above, here are some ideas for treatment:
1. During the acute phase of injury, to ensure comfort, position the athlete passively into the bias preference for modality treat- ments and exercise.
2. Focus strengthening activities on the muscle groups that control mobility and stability of the lum- bar spine. The lumbar spine is controlled by 11 major muscle groups: psoas, quadratus lum- borum, interspinales/intertrans- versarii, multifidus, erector spinae, rectus abdominis, transverse ab- dominis, external/internal ob- liques, rotatores, and latissimus dorsi. When functioning normally,
~-~-.--~hese-mu~1es~~act1sy"ergistically t~---- control spinal activity during ath- letic activities to prevent injury.
3. Resume functional activities to prepare for return to sport.
Have the athlete focus on con- trolling spinal position, in the preferred bias posture, while performing the activity in slow and controlled movement pat- terns. Progress to moving at higher speeds, allow- ing the spine to move in and out of the preferred
bias as long as this does not in- crease the symptoms.
This exercise principle is the focus of the "functional stabiliza- tion" exercise program for low back pain. Because of the versa- tility of this unique program, it is often useful and very effective for treating athletes with low back pain. The program centers around basic principles of neutral spinal position and functional range of motion, taking into con- sideration such factors as the flexion/extension bias.
In short, most low back pa- thologies tend to present them- selves as a preference for either a flexion or extension posture, one that allows maximal relaxation and minimal stress to the involved tissues. When evaluating and treating athletes with low back pain, maximize the rehabilitation potential by incorporating their flexion/extension bias into the treatment program
Terri L. Szajnuk, a 1989 graduate of the Phila- -de4phiaGbllegeof Phanmq&Scknm;is- the senior staff therapist in Occupational Health at St. Margaret Memorial Hospital, Pittsburgh. She has presented over 200 edu- cation programs on low back care, including functional stabilization training programs.
7;he first comprehensive review of i n j ~ y data
in 24 sports 1
Dennis J. Caine, PhD, Caroline G. Caine, PhD,
Koenraad J. Lindner, PhD, Editors
1996 Cloth 472 pp BCAI0466 ISBN 0-87322-466-3
$59.00 ($88.50 Canadian)
For each of 24 activities, this book details injury incidence, injury characteristics, injury severity, and injury risk factors. Each sport-specific chapter also provides suggestions for injury prevention and proposes directions for future research. A one-of-a-kind reference for physical therapists, athletic trainers, and sports physicians.
I r Prices subject to change 11 Place your credit card order today!
(vrsn, AMEX, MC) TOLL FREE: U.S. (800) 747-4457
Canada (800) 465-7301 OR: U.S. (217) 351-5076 Canada (51 9) 944-7774
FAX: U.S. (217) 351-1549 Canada (51 9) 944-7614
Athletic 17Leralby Today
-.g$ HumanXhetics-- TheInfonnatronLeadertnPhyszcalAct~mty http d www humanlunet~cs corn
1219
May 1996
--*- ' - ..





























