Embed Size (px)
Citation preview
Avoiding errors and risks in Avoiding errors and risks in aseptic workaseptic work
Mark Oldcorne
What errors can occur 1What errors can occur 11990: Johannesburg
◦ Death of 15 babiesContaminated IV feeds
2000: India2000: India ◦ Death of 3 young mothers and 3 newborn
babies Contaminated IV fluids
2001: USA 2001: USA ◦ FDA recall contaminated eye drops◦ containing
Pseudomonas mendocina Klebsiella pneumoniae
What errors can occur 2What errors can occur 22004: South Africa 2004: South Africa
◦ 6 premature babies died◦ Enterobacter cloacae
three containers one infusion set
A pharmacist's dirty hands the main reason2002: Brazil 2002: Brazil
◦ 36 n36 neonatal deaths in Brazil ◦ contaminated intravenous fluids.
Endotoxin contaminated IV medication
What errors can occur 3What errors can occur 3Evans Medical in Speke
(not connected with present trading company)
Tue 6th April 19715% Sterile Dextrose Solution Lot D1192
29th Feb – 2nd Mar 19715 deaths at Devonport Hospital
6th Mar 1972 - Investigation begins
12th Jul 1972 - Clothier Report issued by Department of Health &
Social SecurityReport of the Committee appointed to inquire into the circumstances, including the
production, which led to the use of contaminated infusion fluids in the Devonport section of Plymouth General Hospital. (London: HMSO, 1972)
What errors can occur 4What errors can occur 4
What errors can occur 5What errors can occur 5

What errors can occur 6What errors can occur 6
Error Incident RatesError Incident RatesBateman, R; 2003
◦Pilot n=198,000 items 357 errors reported 0.18% processes containing errors 7 left department; 1 administered
◦UK n=155,000 items 1697 errors reported 1.09% processes containing errors 31 left department; 3 administered
Taxis and Barber; 2003◦13% error rate for ward based preparation
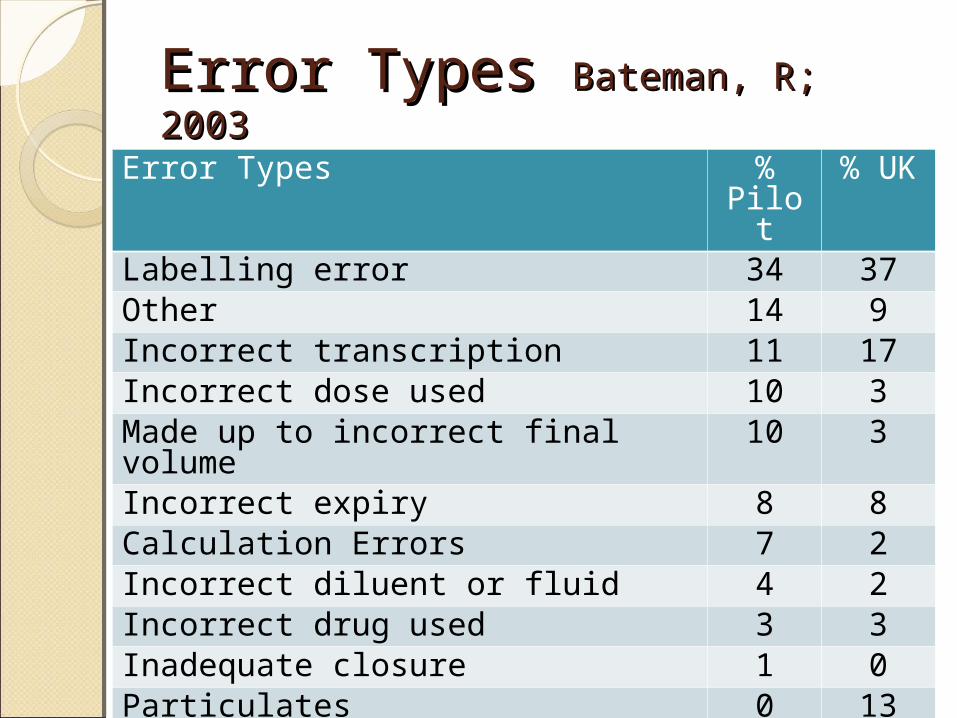
Error Types Error Types Bateman, R; 2003Bateman, R; 2003
Error Types % Pilot
% UK
Labelling error 34 37Other 14 9Incorrect transcription 11 17Incorrect dose used 10 3Made up to incorrect final volume 10 3Incorrect expiry 8 8Calculation Errors 7 2Incorrect diluent or fluid 4 2Incorrect drug used 3 3Inadequate closure 1 0Particulates 0 13Incorrect container 0 3
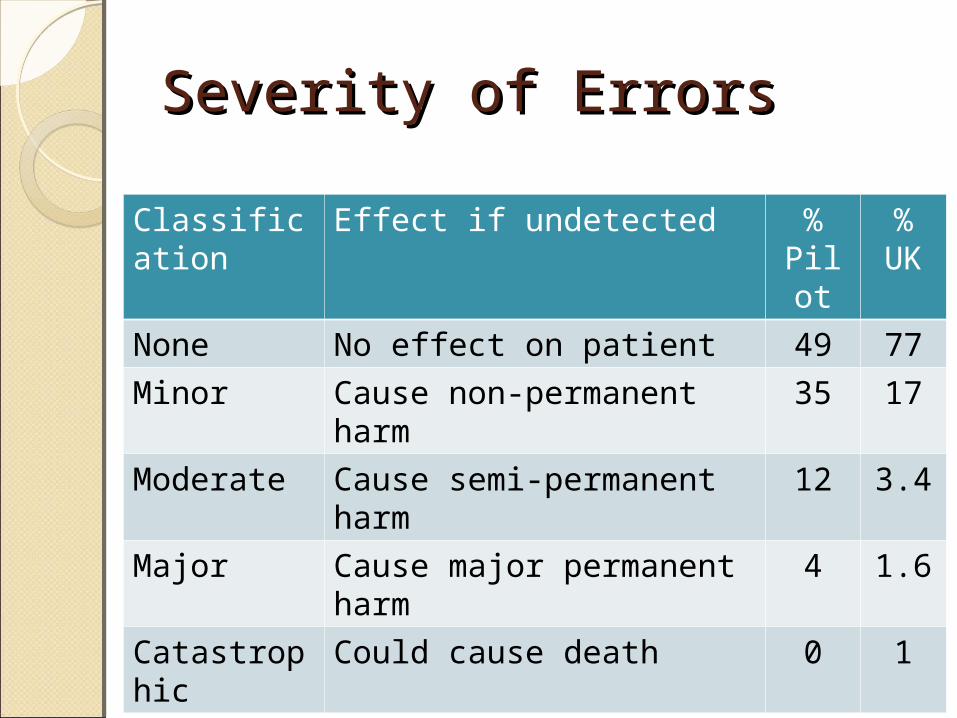
Severity of ErrorsSeverity of Errors
Classification
Effect if undetected % Pilot
% UK
None No effect on patient 49 77
Minor Cause non-permanent harm
35 17
Moderate Cause semi-permanent harm
12 3.4
Major Cause major permanent harm
4 1.6
Catastrophic
Could cause death 0 1
Additional Error TypesAdditional Error TypesAseptic preparation units vs
Traditional Manufacturing Units
Microbiological Contamination operator transfer disinfection environment aseptic processing
Chemical◦right drug ◦correct amounts of drug◦right diluent◦right salt \ hydration states
Factors Contributing to Factors Contributing to errorserrors
Factors Influencing of Factors Influencing of ErrorsErrors Red – Clothier Report 1972!
People◦ poor staff training (or not at all!)◦ staff capability - technical and management◦ inappropriate staffing levels – excessive workloads◦ inappropriately supervised staff ◦ not following procedures◦ individual staff concentration◦ seeing what you want to see
Environment◦ air pressures – record but not acted on◦ poor transfer disinfection◦ cleanliness of work areas\equipment - inadequate
cleaning◦ cleanliness of storage areas – high bioburdens◦ filtration◦ appropriate temperature and humidity
Factors Influencing of Factors Influencing of ErrorsErrors
Records◦ transcription errors◦ actions not completed at time of action ◦ calculation errors◦ incorrect dose & strength◦ incorrect diluent◦ incorrect final volume
Instruments \ Equipment◦ inadequate equipment◦ lack of calibration◦ lack of maintenance activity and logs◦ functioning correctly◦ use for appropriate use◦ validation
Factors Influencing of Factors Influencing of ErrorsErrors
Procedures◦ lack of procedures◦ inadequate procedures (reflect practice –
contemporary) ◦ operators own interpretation of procedures◦ accessible◦ latest version
Ingredients◦ reconciliation checks◦ checks◦ selection errors – incorrect drug / diluent /
containerProduct
◦ inspection and batch review◦ incorrect expiry◦ lack or failure of final product testing
chemical, particulates, microbiology, endotoxins ◦ labelling errors
Sources of ErrorsSources of ErrorsHuman Errors
◦ never deliberate◦ usually careless◦ system shortfalls◦ overwork◦ ignorance
Mechanical Malfunction◦ software malfunction◦ hardware malfunction◦ lack of calibration◦ inappropriate use (e.g. re-use of single use
equipment)
Combinations - Swiss Cheese Scenario
Minimising ErrorsMinimising ErrorsPhil CrosbyZero defects or Right First Time philosophy
◦ emphasis on prevention◦ relies on measurement and data collection -
eliminate errors (and waste)
Zero defect does not mean that people NEVER make mistakes
Rather – they are not assumed or expected to make mistakesAim for perfection and miss it
RATHER THANAim for imperfection and hit it
Minimising ErrorsMinimising Errors“To err is human”
“human error is caused by a lack of attention rather than a lack of
knowledge”
“lack of attention is created when we assume that error is inevitable”
(or perhaps we think that the responsibility lies elsewhere)
It means that accepting a 0.1% or even a 0.001% error rate is just not on, and that
the only level worth striving for is 0%
Minimising RisksMinimising RisksAdoption of GxP systems
Rules and Guidance for Pharmaceutical Manufacturers and Distributors, 2007
Quality Assurance of Aseptic Preparation Services
Is that it? Unlimited ResourcesIntegration with
Risk managementRisk managementICH 9 Quality Risk Management
Principles of Quality Risk Management◦ evaluation of risk to quality – based on
scientific knowledge and ultimately link to patient safety
◦ level of effort, formality and documentation of quality risk management process – commensurate with level of risk
Apply to◦ development, manufacturing, release,
distribution, inspection, review processes◦ starting and final drug products
When◦ lifecycle of product
Risk AssessmentRisk Assessment1. Risk Identification
◦ What might go wrong?2. Risk Analysis
◦ What is the likelihood (probability) it will go wrong?
◦ What are the consequences (severity)?
3. Risk Evaluation◦ Compares identified risk and analysed
risk against given risk criteria◦ Risk score

Risk assessmentRisk assessmentObjective
◦Elimination to reduction to acceptable levels
Outcomes◦Patient safety◦Regulatory compliance◦Financial ◦Reputation

Risk ManagementRisk Management
Minimising ErrorsMinimising ErrorsRetrospectiveRetrospective
Deviation Management \ Change Control
Risk Management Tools
◦CAPA
◦RCA
Compare to Other Reporting Schemes
CAPACAPACorrective and Preventive ActionClosed loop process
1. Corrective Action ◦action taken to rectify the non-
conformance/error
2. Preventive Action◦action taken to avoid repetition of the
same non-conformance. This could involve modification or enforcement of procedures, or implementation of further controls
3. Change Control
RCARCARoot Cause Analysis
Structured and objective method - Asking◦What? How? Why?
Team approach – Facilitator
Analysing Errors - Human Error◦timelines etc.◦nominal group technique, brainstorming, brain-writing, fishbone, 5-whys, barrier analysis
Reporting SystemsReporting Systems
Local Reporting Scheme
◦Hospital or Trust based
National Reporting Schemes
◦Regional
◦National National Reporting and Learning System - NPSA
Pharmaceutical Aseptic Services Group / R.
Bateman
No Blame
Use of Quality IndicatorsUse of Quality Indicators
Trending environmental monitoring data
Deviation\Exception reports
Contamination rates
Trigger Tools
Safer Patient Initiative (SPI)
Minimising ErrorsMinimising ErrorsProspectiveProspective
Minimising errors by prospective
analysis
Process mapping
Risk Management Tools
◦FMEA
◦HACCP
FMEAFMEA Failure Mode Effects Analysis
◦easy to use!!◦evaluation of failure modes and likely
outcomes◦risk reduction◦need in depth understanding of product and
processes methodically breaks analysis of complex processes
into manageable steps
◦Used to prioritize risks monitor effectiveness of risk control activities prioritize validation activities
◦Applied to equipment, facilities, products & processes
HACCPHACCPHazard Analysis and Critical Control Points
◦ Systematic, proactive and preventive tool
◦ Quality, Reliability and Safety aspects◦ 7 steps
1. Conduct hazard analysis and ID preventive measures – each step
2. Determine critical control points3. Establish critical limits4. Establish – system to monitor the CCP5. Establish corrective action when CCP not
controlled6. Establish system to prove HACCP system
working7. Establish record keeping system
Summary Summary Gauge your risks!Gauge your risks!
Prospective
Retrospective
Use Risk Management Tools
Remember they are only tools





























