Embed Size (px)
Citation preview

1
Aviation Aviation Patient SafetyPatient Safety
andand
Bryce TaylorBryce TaylorHospital Authority ConventionHospital Authority Convention
Hong KongHong KongMay 11, 2010May 11, 2010
We have learned a lot, but We have learned a lot, but we have a long way to go!we have a long way to go!

2
Aviation and Health CareAviation and Health Care
““ …… both involve hours ofboth involve hours ofboredom punctuated byboredom punctuated bymoments of sheer terrormoments of sheer terror””
Dr. David Dr. David GabaGaba, Associate Dean, Associate DeanStanford University School of MedicineStanford University School of Medicine

3
“…“…flying and surgery are rewarding, highlyflying and surgery are rewarding, highlycomplex disciplines very dependent on effectivecomplex disciplines very dependent on effective
communication. They both deal with natural communication. They both deal with natural forces forces ------ weather on one hand and illness weather on one hand and illness
on the other. In both the consequences on the other. In both the consequences of error have the potential to be catastrophicof error have the potential to be catastrophic””
Dr. Richard KarlDr. Richard Karlsurgeon & pilotsurgeon & pilot
4
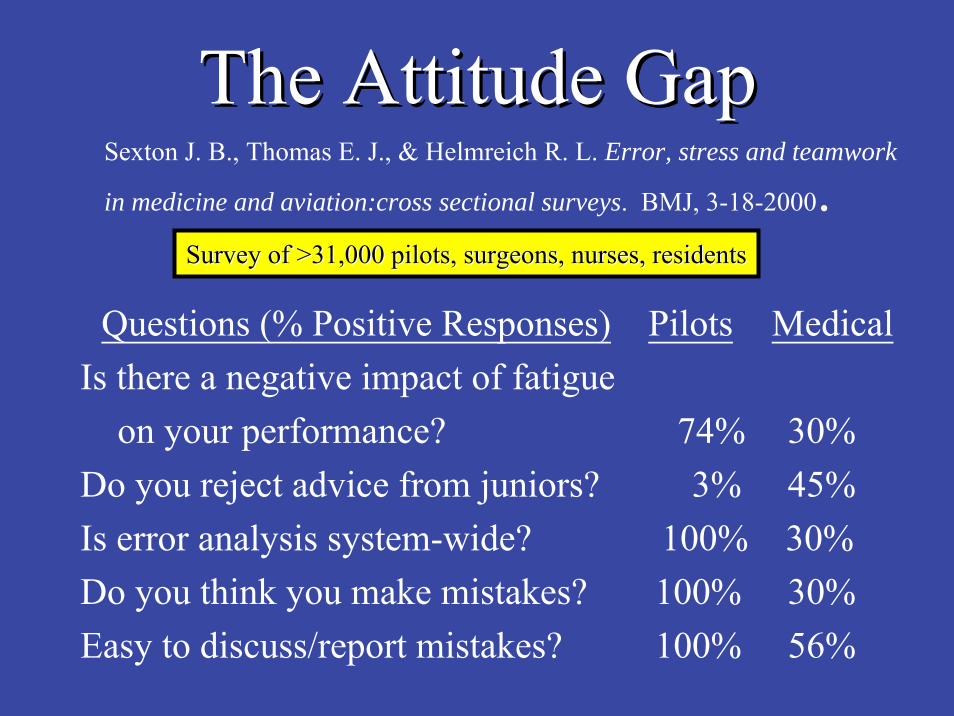
The Attitude GapThe Attitude Gap
Questions (% Positive Responses) Pilots MedicalIs there a negative impact of fatigue
on your performance? 74% 30%Do you reject advice from juniors? 3% 45%Is error analysis system-wide? 100% 30%Do you think you make mistakes? 100% 30%Easy to discuss/report mistakes? 100% 56%
Sexton J. B., Thomas E. J., & Helmreich R. L. Error, stress and teamwork
in medicine and aviation:cross sectional surveys. BMJ, 3-18-2000.Survey of >31,000 pilots, surgeons, nurses, residentsSurvey of >31,000 pilots, surgeons, nurses, residents

5

6Michael PorterMichael Porter

7
health outcomeshealth outcomesdollar expendeddollar expended
Michael E. PorterMichael E. Porter
Increasing safety can be expensive!Increasing safety can be expensive!
Value =Value =

8

9
Medicine learns from other industries!Medicine learns from other industries!
•• EfficiencyEfficiency –– car industry, TOYOTA car industry, TOYOTA LEAN manufacturing (LEAN manufacturing (VSMVSM’’ss, , RIERIE’’ss))
•• SafetySafety –– MOTOROLA 6MOTOROLA 6ΣΣ, AIRLINES, AIRLINES
(Efficiency (Efficiency savessaves money)money)
(safety (safety costscosts money!)money!)

10

11

12
In In game theorygame theory and and economic theoryeconomic theory, , zerozero--sumsum describes a situation in which describes a situation in which
a participant's gain or loss is exactly a participant's gain or loss is exactly balanced by the losses or gains of the balanced by the losses or gains of the
other other participant(sparticipant(s). If the total gains of ). If the total gains of the participants are added up, and the the participants are added up, and the total losses are subtracted, they will total losses are subtracted, they will
sum to zero. sum to zero.
The zeroThe zero--sum competitionsum competition

13
…… results in a positiveresults in a positive--sum competitionsum competitionin which all system participants canin which all system participants canbenefit. When we providers win bybenefit. When we providers win by
providing superior care more efficiently providing superior care more efficiently and safely, patients, employers and and safely, patients, employers and
health plans also win. health plans also win.
The The valuevalue--basedbased competitioncompetition
Michael E. PorterMichael E. Porter

14
ValueValue--basedbased competitioncompetition•• Focus in Focus in valuevalue for patients, not lowering costsfor patients, not lowering costs•• Competition must be based on Competition must be based on resultsresults•• Centre on conditions over Centre on conditions over full cycle of carefull cycle of care•• High quality should be High quality should be less costlyless costly•• Value driven by provider experience and learningValue driven by provider experience and learning•• Competition should be Competition should be regional and nationalregional and national•• Results must be Results must be widely availablewidely available•• InnovationsInnovations increasing value increasing value must be rewardedmust be rewarded
Redefining HealthcareRedefining Healthcare

15
The The ““ClientClient”” AssumptionAssumption
••How was your flight?How was your flight?---- the food, the service, the the food, the service, the courtesy of the airline staffcourtesy of the airline staff

16
The The ““ClientClient”” AssumptionAssumption
••How was your flight?How was your flight?---- the food, the service, the the food, the service, the courtesy of the airline staffcourtesy of the airline staff
••How was your operation?How was your operation?---- the food, the service, thethe food, the service, thecourtesy of the hospital staffcourtesy of the hospital staff

17
The The ““ClientClient”” AssumptionAssumption
••How was your flight?How was your flight?---- the food, the service, the the food, the service, the courtesy of the airline staffcourtesy of the airline staff
••How was your operation?How was your operation?---- the food, the service, thethe food, the service, thecourtesy of the hospital staffcourtesy of the hospital staff
••The food was terrible and coldThe food was terrible and cold
••The hospital staff was uncaringThe hospital staff was uncaring
••My pain was uncontrolledMy pain was uncontrolled
••I developed a wound infectionI developed a wound infection
••II’’m complaining to the CEOm complaining to the CEO
••II’’m thinking of suing!m thinking of suing!

18
Aviation and Patient SafetyAviation and Patient Safety
The airlines embraced safety long agoThe airlines embraced safety long ago……why has medicine been so slow towhy has medicine been so slow toadopt even the simplest measures?adopt even the simplest measures?
The Question:The Question:
Medicine can learn much fromMedicine can learn much fromthe Airlines, but in many aspects,the Airlines, but in many aspects,
we are we are different!different!

19
Aviation and Patient SafetyAviation and Patient Safety
••How are we different?How are we different?
••Where do we go next?Where do we go next?

20
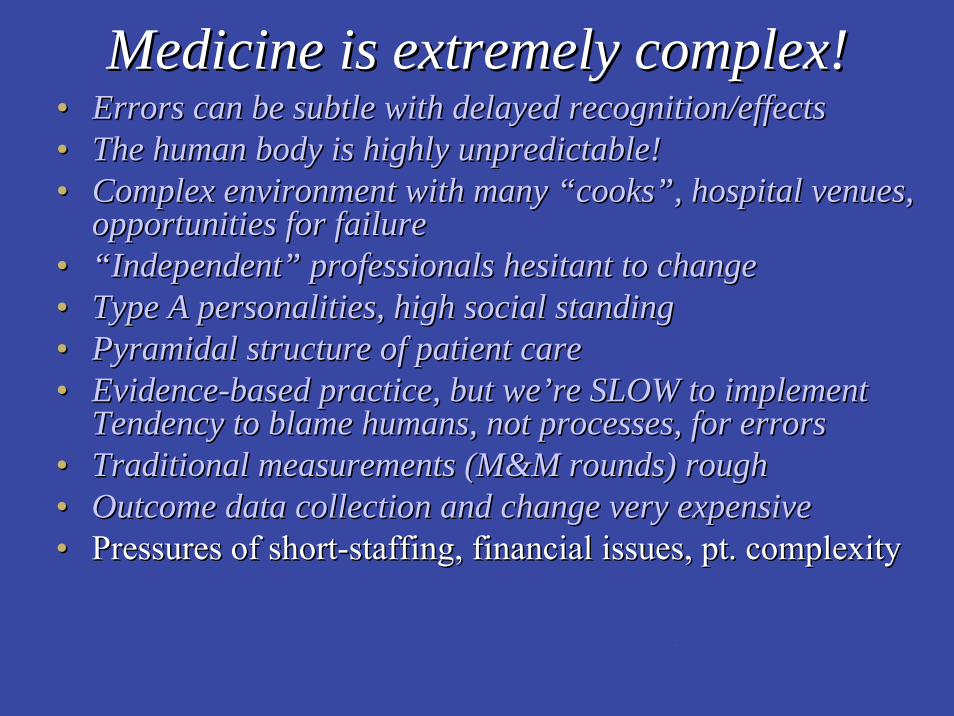
Medicine is extremely complex!Medicine is extremely complex!

21
Medicine is extremely complex!Medicine is extremely complex!•• Errors can be subtle with delayed recognition/effectsErrors can be subtle with delayed recognition/effects•• The human body is highly unpredictable!The human body is highly unpredictable!
(On the other hand, Airline mishaps (On the other hand, Airline mishaps are sudden, with immediate are sudden, with immediate
dramatic effects, often dramatic effects, often with identifiable causes)with identifiable causes)

22

23
Medicine is extremely complex!Medicine is extremely complex!•• Errors can be subtle with delayed recognition/effectsErrors can be subtle with delayed recognition/effects•• The human body is highly unpredictable!The human body is highly unpredictable!•• Complex environment with many Complex environment with many ““cookscooks””, hospital venues, , hospital venues,
opportunities for failureopportunities for failure
The cockpit is moreThe cockpit is morecontrolled and containedcontrolled and contained

24
Medicine is extremely complex!Medicine is extremely complex!•• Errors can be subtle with delayed recognition/effectsErrors can be subtle with delayed recognition/effects•• The human body is highly unpredictable!The human body is highly unpredictable!•• Complex environment with many Complex environment with many ““cookscooks””, hospital venues, , hospital venues,
opportunities for failureopportunities for failure•• ““IndependentIndependent”” professionals hesitant to changeprofessionals hesitant to change•• Type A personalities, high social standingType A personalities, high social standing•• Pyramidal structure of patient carePyramidal structure of patient care
(pilots and staff are (pilots and staff are employeesemployeesand must follow the rules!)and must follow the rules!)

25
The Pyramid The Pyramid ……and..and..The PowerThe Power--DistanceDistanceIndexIndexPilots
SurgeonsAnesthesiologists
E v e r y o n e E l s e

26
The surgeon The surgeon circa 1509circa 1509-- 19991999
““My way or the highwayMy way or the highway””
oror
““My scene or the guillotineMy scene or the guillotine””
27
The PowerThe Power--DistanceDistanceIndexIndex
The pyramid The pyramid ……and..and..

28
Medicine is extremely complex!Medicine is extremely complex!•• Errors can be subtle with delayed recognition/effectsErrors can be subtle with delayed recognition/effects•• The human body is highly unpredictable!The human body is highly unpredictable!•• Complex environment with many Complex environment with many ““cookscooks””, hospital venues, , hospital venues,
opportunities for failureopportunities for failure•• ““IndependentIndependent”” professionals hesitant to changeprofessionals hesitant to change•• Type A personalities, high social standingType A personalities, high social standing•• Pyramidal structure of patient carePyramidal structure of patient care•• EvidenceEvidence--based practice, but webased practice, but we’’re SLOW to implementre SLOW to implement
(The mean time for implementation(The mean time for implementationof new scientifically provenof new scientifically proven
treatments is 17 years!)treatments is 17 years!)-- CLI checklistCLI checklist-- surgical checklistsurgical checklist

29

3030
World View of SSCLWorld View of SSCL

31
Medicine is extremely complex!Medicine is extremely complex!•• Errors can be subtle with delayed recognition/effectsErrors can be subtle with delayed recognition/effects•• The human body is highly unpredictable!The human body is highly unpredictable!•• Complex environment with many Complex environment with many ““cookscooks””, hospital venues, , hospital venues,
opportunities for failureopportunities for failure•• ““IndependentIndependent”” professionals hesitant to changeprofessionals hesitant to change•• Type A personalities, high social standingType A personalities, high social standing•• Pyramidal structure of patient carePyramidal structure of patient care•• EvidenceEvidence--based practice, but webased practice, but we’’re SLOW to implement re SLOW to implement •• Tendency to blame humans, not processes, for errorsTendency to blame humans, not processes, for errors•• Traditional measurements (M&M rounds) roughTraditional measurements (M&M rounds) rough
(Pilots think (Pilots think processprocess first!)first!)

32
Medicine is extremely complex!Medicine is extremely complex!•• Errors can be subtle with delayed recognition/effectsErrors can be subtle with delayed recognition/effects•• The human body is highly unpredictable!The human body is highly unpredictable!•• Complex environment with many Complex environment with many ““cookscooks””, hospital venues, , hospital venues,
opportunities for failureopportunities for failure•• ““IndependentIndependent”” professionals hesitant to changeprofessionals hesitant to change•• Type A personalities, high social standingType A personalities, high social standing•• Pyramidal structure of patient carePyramidal structure of patient care•• EvidenceEvidence--based practice, but webased practice, but we’’re SLOW to implement re SLOW to implement •• Tendency to blame humans, not processes, for errorsTendency to blame humans, not processes, for errors•• Traditional measurements (M&M rounds) roughTraditional measurements (M&M rounds) rough

33
Medicine is extremely complex!Medicine is extremely complex!•• Errors can be subtle with delayed recognition/effectsErrors can be subtle with delayed recognition/effects•• The human body is highly unpredictable!The human body is highly unpredictable!•• Complex environment with many Complex environment with many ““cookscooks””, hospital venues, , hospital venues,
opportunities for failureopportunities for failure•• ““IndependentIndependent”” professionals hesitant to changeprofessionals hesitant to change•• Type A personalities, high social standingType A personalities, high social standing•• Pyramidal structure of patient carePyramidal structure of patient care•• EvidenceEvidence--based practice, but webased practice, but we’’re SLOW to implementre SLOW to implement•• Tendency to blame humans, not processes, for errorsTendency to blame humans, not processes, for errors•• Traditional measurements (M&M rounds) roughTraditional measurements (M&M rounds) rough•• Outcome data collection and change very expensiveOutcome data collection and change very expensive

34
Cost of data collection for TGHCost of data collection for TGHduring WHO checklist study:during WHO checklist study:
-- ~1000 patients followed for~1000 patients followed forACS/NSQIP complicationsACS/NSQIP complications
-- $60,000 CDN$60,000 CDN
35
Medicine is extremely complex!Medicine is extremely complex!•• Errors can be subtle with delayed recognition/effectsErrors can be subtle with delayed recognition/effects•• The human body is highly unpredictable!The human body is highly unpredictable!•• Complex environment with many Complex environment with many ““cookscooks””, hospital venues, , hospital venues,
opportunities for failureopportunities for failure•• ““IndependentIndependent”” professionals hesitant to changeprofessionals hesitant to change•• Type A personalities, high social standingType A personalities, high social standing•• Pyramidal structure of patient carePyramidal structure of patient care•• EvidenceEvidence--based practice, but webased practice, but we’’re SLOW to implement re SLOW to implement
Tendency to blame humans, not processes, for errorsTendency to blame humans, not processes, for errors•• Traditional measurements (M&M rounds) roughTraditional measurements (M&M rounds) rough•• Outcome data collection and change very expensiveOutcome data collection and change very expensive•• Pressures of shortPressures of short--staffing, financial issues, pt. complexitystaffing, financial issues, pt. complexity

36

37
Medicine is extremely complex!Medicine is extremely complex!•• Errors can be subtle with delayed recognition/effectsErrors can be subtle with delayed recognition/effects•• The human body is highly unpredictable!The human body is highly unpredictable!•• Complex environment with many Complex environment with many ““cookscooks””, hospital venues, , hospital venues,
opportunities for failureopportunities for failure•• ““IndependentIndependent”” professionals hesitant to changeprofessionals hesitant to change•• Type A personalities, high social standingType A personalities, high social standing•• Pyramidal structure of patient carePyramidal structure of patient care•• EvidenceEvidence--based practice, but webased practice, but we’’re SLOW to implement re SLOW to implement •• Tendency to blame humans, not processes, for errorsTendency to blame humans, not processes, for errors•• Traditional measurements (M&M rounds) roughTraditional measurements (M&M rounds) rough•• Outcome data collection and change very expensiveOutcome data collection and change very expensive•• Pressures of shortPressures of short--staffing, financial issues, pt. complexitystaffing, financial issues, pt. complexity•• Ongoing assessments of doctor competence crude or 0Ongoing assessments of doctor competence crude or 0•• Poor and local control of regulations for whole industryPoor and local control of regulations for whole industry

38
Maintenance of competenceMaintenance of competence
• MOCOMP in Canada (RCPSC)• CPD (CME) time credits in US and Canada• Recertification in US• SWOT team in Britain in past• Procedure-based assessment in Britain• Physician Achievement Review in Alberta

39

40
The Era of AccountabilityThe Era of Accountability
Are we experiencing“Accountability fatigue”?
“The Hawthorne effectin action”

41

42
Medicine is extremely complex!Medicine is extremely complex!•• Errors can be subtle with delayed recognition/effectsErrors can be subtle with delayed recognition/effects•• The human body is highly unpredictable!The human body is highly unpredictable!•• Complex environment with many Complex environment with many ““cookscooks””, hospital venues, , hospital venues,
opportunities for failureopportunities for failure•• ““IndependentIndependent”” professionals hesitant to changeprofessionals hesitant to change•• Type A personalities, high social standingType A personalities, high social standing•• Pyramidal structure of patient carePyramidal structure of patient care•• EvidenceEvidence--based practice, but webased practice, but we’’re SLOW to implement re SLOW to implement •• Tendency to blame humans, not processes, for errorsTendency to blame humans, not processes, for errors•• Traditional measurements (M&M rounds) roughTraditional measurements (M&M rounds) rough•• Outcome data collection and change very expensiveOutcome data collection and change very expensive•• Pressures of shortPressures of short--staffing, financial issues, pt. complexitystaffing, financial issues, pt. complexity•• Ongoing assessments of doctor competence crude or 0Ongoing assessments of doctor competence crude or 0•• Poor and local control of regulations for whole industryPoor and local control of regulations for whole industry•• Fear of litigation is a strong motivatorFear of litigation is a strong motivator

43
(Pilots aren(Pilots aren’’t worried about this guy!)t worried about this guy!)

44
““The estimate that up to 23,000 people died in 2004 The estimate that up to 23,000 people died in 2004 in Canadian hospitals because of preventable adverse in Canadian hospitals because of preventable adverse events is staggering. Checklists in aviation have beenevents is staggering. Checklists in aviation have been
in use pretty well since the Wright brothers.in use pretty well since the Wright brothers.One wonders whether such checklists would haveOne wonders whether such checklists would have
been introduced much earlier in medicine if surgeons been introduced much earlier in medicine if surgeons shared the fate of their patients, as pilots share shared the fate of their patients, as pilots share
that of their passengers.that of their passengers.””
Adrian Boelen, retired A/C pilot, Dorval, QueAdrian Boelen, retired A/C pilot, Dorval, Que

45
Aviation Aviation Patient SafetyPatient Safety
Where to now?Where to now?
We have learned a lot, but We have learned a lot, but we have a long way to go!we have a long way to go!
andand

46
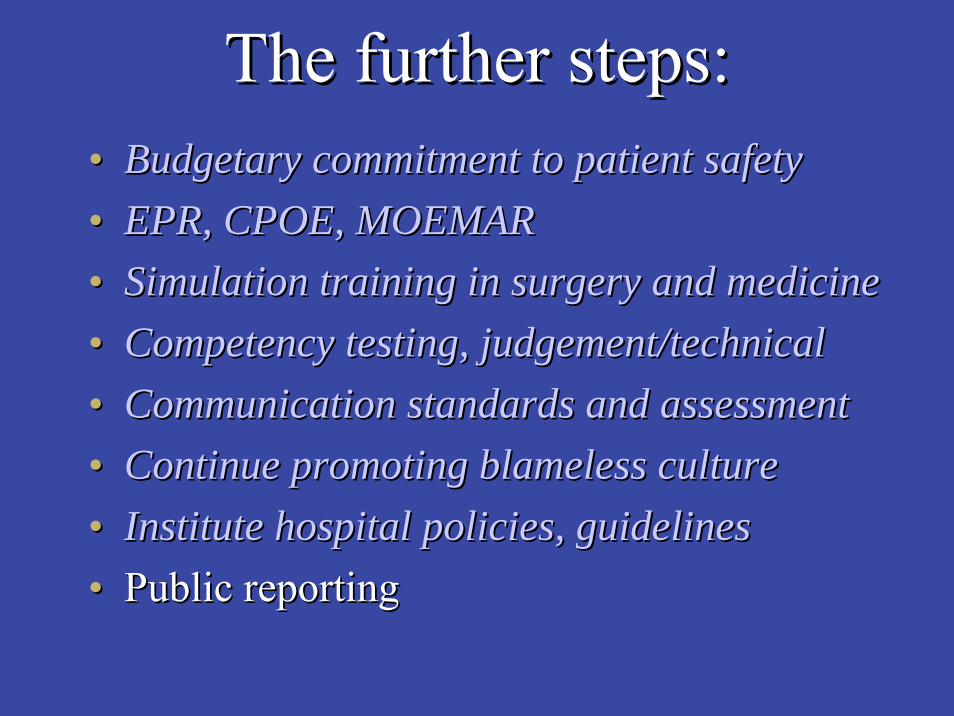
The further steps:The further steps:

47
The further steps:The further steps:•• Budgetary commitment to patient safetyBudgetary commitment to patient safety•• EPR, CPOE, MOEMAREPR, CPOE, MOEMAR
The profile of patient safetyThe profile of patient safetymust be raised in must be raised in everyevery hospitalhospital
and in and in everyevery hospital system!hospital system!

48
Surgical site infectionSurgical site infection
•• 2965 US hospitals, 34133 in2965 US hospitals, 34133 in--pt operationspt operations•• 55% received timely and appropriate antibiotics55% received timely and appropriate antibiotics•• 300,000 of 15M patients/yr develop SSI300,000 of 15M patients/yr develop SSI•• Calculated increased costs of $1.5 BillionCalculated increased costs of $1.5 Billion•• Patient who develops SSI has 2xOMR, 5Patient who develops SSI has 2xOMR, 5--6x 6x
readmission, 2xLOSreadmission, 2xLOS•• Cost for orthopedic, cardiac SSI = $30Cost for orthopedic, cardiac SSI = $30--50K50K
(the surgical infection prevention project)(the surgical infection prevention project)
Bratzler et al, Arch Surg 2005:140;174Bratzler et al, Arch Surg 2005:140;174--8282

49
The further steps:The further steps:•• Budgetary commitment to patient safetyBudgetary commitment to patient safety•• EPR, CPOE, MOEMAREPR, CPOE, MOEMAR•• Simulation training in surgery and medicineSimulation training in surgery and medicine

50

51

52
SimulatorsSimulatorsHigh TechHigh TechVR SimulatorsVR Simulators

53
Virtual Reality SimulatorsVirtual Reality Simulators

54
The further steps:The further steps:•• Budgetary commitment to patient safetyBudgetary commitment to patient safety•• EPR, CPOE, MOEMAREPR, CPOE, MOEMAR•• Simulation training in surgery and medicineSimulation training in surgery and medicine•• Competency testing, judgement/technicalCompetency testing, judgement/technical

55
The further steps:The further steps:•• Budgetary commitment to patient safetyBudgetary commitment to patient safety•• EPR, CPOE, MOEMAREPR, CPOE, MOEMAR•• Simulation training in surgery and medicineSimulation training in surgery and medicine•• Competency testing, judgement/technicalCompetency testing, judgement/technical•• Communication standards and assessmentCommunication standards and assessment
(Patient(Patient--centred care becomescentred care becomesRelationshipRelationship--centred care!)centred care!)

56

57

58
TheThe““Black BoxBlack Box””of Surgeryof Surgery

59
The further steps:The further steps:•• Budgetary commitment to patient safetyBudgetary commitment to patient safety•• EPR, CPOE, MOEMAREPR, CPOE, MOEMAR•• Simulation training in surgery and medicineSimulation training in surgery and medicine•• Competency testing, judgement/technicalCompetency testing, judgement/technical•• Communication standards and assessmentCommunication standards and assessment•• Continue promoting blameless cultureContinue promoting blameless culture
((rewardreward, not punish incident reporting!), not punish incident reporting!)

60
The further steps:The further steps:•• Budgetary commitment to patient safetyBudgetary commitment to patient safety•• EPR, CPOE, MOEMAREPR, CPOE, MOEMAR•• Simulation training in surgery and medicineSimulation training in surgery and medicine•• Competency testing, judgement/technicalCompetency testing, judgement/technical•• Communication standards and assessmentCommunication standards and assessment•• Continue promoting blameless cultureContinue promoting blameless culture•• Institute hospital policies, guidelinesInstitute hospital policies, guidelines
61
The further steps:The further steps:•• Budgetary commitment to patient safetyBudgetary commitment to patient safety•• EPR, CPOE, MOEMAREPR, CPOE, MOEMAR•• Simulation training in surgery and medicineSimulation training in surgery and medicine•• Competency testing, judgement/technicalCompetency testing, judgement/technical•• Communication standards and assessmentCommunication standards and assessment•• Continue promoting blameless cultureContinue promoting blameless culture•• Institute hospital policies, guidelinesInstitute hospital policies, guidelines•• Public reportingPublic reporting
62
Hospital reporting/The FunderHospital reporting/The Funder•• Outcomes Outcomes
-- HSMR, CLI, CDiff, MRSA, VRE, VAPHSMR, CLI, CDiff, MRSA, VRE, VAP-- Falls, pressure ulcers, pt. satisfactionFalls, pressure ulcers, pt. satisfaction-- Wait times for emerg admission, surgeryWait times for emerg admission, surgery
•• EfficiencyEfficiency-- CPWC, SETP indicatorsCPWC, SETP indicators
•• Senior leadersSenior leaders’’ salaries tied to performance!salaries tied to performance!•• US hospitals rewarded for performance (actual P4P!)US hospitals rewarded for performance (actual P4P!)

63
The further steps:The further steps:•• Budgetary commitment to patient safetyBudgetary commitment to patient safety•• EPR, CPOE, MOEMAREPR, CPOE, MOEMAR•• Simulation training in surgery and medicineSimulation training in surgery and medicine•• Competency testing, judgement/technicalCompetency testing, judgement/technical•• Communication standards and assessmentCommunication standards and assessment•• Continue promoting blameless cultureContinue promoting blameless culture•• Institute hospital policies, guidelinesInstitute hospital policies, guidelines•• Public reportingPublic reporting•• Develop Develop internationalinternational standardsstandards

64
The further steps:The further steps:•• Budgetary commitment to patient safetyBudgetary commitment to patient safety•• EPR, CPOE, MOEMAREPR, CPOE, MOEMAR•• Simulation training in surgery and medicineSimulation training in surgery and medicine•• Competency testing, judgement/technicalCompetency testing, judgement/technical•• Communication standards and assessmentCommunication standards and assessment•• Continue promoting blameless cultureContinue promoting blameless culture•• Institute hospital policies, guidelinesInstitute hospital policies, guidelines•• Public reportingPublic reporting•• Develop international standardsDevelop international standards•• Doctors as employees? Doctors as employees? –– pay structurepay structure

65
The further steps:The further steps:•• Budgetary commitment to patient safetyBudgetary commitment to patient safety•• EPR, CPOE, MOEMAREPR, CPOE, MOEMAR•• Simulation training in surgery and medicineSimulation training in surgery and medicine•• Competency testing, judgement/technicalCompetency testing, judgement/technical•• Communication standards and assessmentCommunication standards and assessment•• Continue promoting blameless cultureContinue promoting blameless culture•• Institute hospital policies, guidelinesInstitute hospital policies, guidelines•• Public reportingPublic reporting•• Develop international standardsDevelop international standards•• Doctors as employees? Doctors as employees? –– pay structurepay structure

66
Aviation Aviation Patient SafetyPatient Safety
andand
Bryce TaylorBryce TaylorHospital Authority ConventionHospital Authority Convention
Hong KongHong KongMay 11, 2010May 11, 2010
We have learned a lot, but We have learned a lot, but we have a long way to go!we have a long way to go!





























