-
7/27/2019 Avaliacao TC Acetabulo
1/7
ORIGINAL ARTICLE
Evaluation of Computed Tomography forDetermining the Diagnosis
of Acetabular Fractures
Robert V. OToole, MD, Garrick Cox, MD, K. Shanmuganathan, MD,
Renan C. Castillo, MS,
Clifford H. Turen, MD, Marcus F. Sciadini, MD, and Jason W.
Nascone, MD
Objective: We assessed whether, in contrast to reports in
theliterature, computed tomographic (CT) scans improve the ability
to
classify acetabular fractures in comparison with plain
radiographs.
Design: Prospective.
Setting: Level I trauma center.
Patients: Seventy-five patients with 75 acetabular fractures
treatedbetween June 2005 and May 2006.
Intervention: Four different image sets for each patient
wereevaluated: image set A, Judet view plain radiographs plus axial
view
CT scans; image set B, Judet view plain radiographs alone; image
set
C, three-dimensional CT reconstructions; and image set D,
CT-
simulated anteroposterior and Judet views of the pelvis. The
300
image sets were viewed in random order by four orthopaedic
trauma
fellowship-trained surgeons who independently recorded a
diagnosis.
A gold standard diagnosis was determined by group consensus.
Main Outcome Measurements: Agreement among four imagingmethods
was evaluated by using kappa statistics for multiple raters
and nominal data.
Results: Comparing the gold standard diagnosis with the four
imagesets, Judet view plain radiographs had a worse kappa value
than
CT scans (P, 0.05). The adjusted kappa values for all three
image
sets that included CT scans averaged greater than 0.62,
showing
substantial agreement, whereas the image set with plain
radiographs
alone (image set B) had a lower kappa value of only 0.48 (P,
0.05).
Conclusions: In contrast to previous reports in the literature,
theaccuracy of plain radiographs alone was less than the accuracy
of CT
scans in terms of diagnosis. The interobserver reliability was
also
worse for plain radiographs alone.
Key Words: acetabular fractures, computed tomography, plain
radiographs, diagnosis, three dimensional reconstructions,
simulated
Judet views
(J Orthop Trauma 2010;24:284290)
INTRODUCTIONAdequate radiographic assessment is essential for
the
diagnosis and treatment of acetabular fractures. Three
plainradiographic views traditionally have been used to define
thefracture pattern: anteroposterior view, obturatoroblique
Judetview, and iliacoblique Judet view of the pelvis.13
Oncecomputed tomography came into common use, axial viewcomputed
tomographic (CT) scans were added to the Judetviews for
preoperative evaluation.4
Preoperative radiographic evaluation with the Letourneland Judet
classification system typically is used to classifyacetabular
fractures18 and to plan for operative approaches.The Letournel and
Judet system includes 10 fracture types that
are divided into five elementary fracture patterns and
fiveassociated fracture patterns.3 One previous study analyzed
theinterobserver reliability of the Letournel and Judet
fractureclassification system and found substantial
interobserverand intraobserver agreement with kappa values on the
orderof 0.7.5
Recent advances in CT include the capability to
producethree-dimensional CT reconstructions and simulated
ante-roposterior and Judet view radiographs derived from
CTscans.912 Despite the emerging use of the new three-dimensional
CT imaging modalities to help classify and planfor treatment of
acetabular fractures, the influence of theimaging modalities on
diagnosis has not yet been wellcharacterized. The few studies
examining the issue have
questioned the usefulness of CT scans for evaluatingacetabular
fractures.5,13 Our hypothesis was that the use ofCT scans improves
accuracy in classifying acetabular fracturesin comparison with
plain radiographs alone.
PATIENTS AND METHODS
Inclusion CriteriaAfter obtaining Institutional Review Board
approval, we
retrospectively reviewed a database that had been prospec-tively
collected and designed for this study. Between June
Accepted for publication October 28, 2009.From the R Adams
Cowley Shock Trauma Center, Department of Orthopaedics,
University of Maryland School of Medicine, Baltimore, MD.The
authors report no financial disclosures related to the content of
this
manuscript.Reprints: Robert V. OToole, MD, 22 S. Greene Street,
T3R62, R Adams
Cowley Shock Trauma Center, Department of Orthopaedics,
University ofMaryland School of Medicine, Baltimore, MD 21201
(e-mail: [email protected]).
Copyright 2010 by Lippincott Williams & Wilkins
284 | www.jorthotrauma.com J Orthop Trauma Volume 24, Number 5,
May 2010
-
7/27/2019 Avaliacao TC Acetabulo
2/7
2005 and May 2006, 178 consecutive patients presented at
ourLevel I trauma center with acetabular fractures. Patients
wereexcluded from the study for the following reasons: if any of
thetypes of images we were studying were not available forviewing;
if the imaging studies had not been completed; andif any
identifiable markers such as associated fractures or
hardware from previous treatment were seen on the images.Most of
the exclusions were because three-dimensional CTreconstructions
were not available for analysis. However, no
patient was excluded because of poor image quality becausewe
wanted to study the imaging modalities as they were usedin clinical
practice as opposed to including only idealimages that might be
very difficult to routinely obtain. Afterexclusions, the study
group included 75 patients with 75fractures.
Image SetsFour different image sets were evaluated for each
patient: image set A, Judet view plain radiographs plus
axial
view CT scans; image set B, Judet view plain radiographsalone;
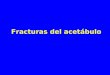
image set C, three-dimensional CT reconstructions(Fig. 1); and
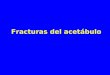
image set D, CT-simulated anteroposterior andJudet views of the
pelvis (Fig. 2). This created 300 total imagesets for viewing. The
300 individual image sets were eachassigned a random number using a
computerized randomnumber generator (Microsoft Office Excel 2003
Version 11.8;Microsoft Corporation, Redmond, WA) and had all
patientidentifiers removed. The image sets were then
randomlyarranged by sorting the random numbers into
ascendingnumerical order for viewing. The CT scans were obtained
byusing a Phillips Vitrea 2.0 CT scanner (Andover, MA) with3-mm
thick soft copy section thickness. The scanning protocolwas use of
a 16-section multidetector CT scanner (Brilliance
16 Power CT scanner; Philips Medical Systems, Cleveland,OH) with
a detector width of 0.75 mm, pitch of 0.938, androtation time of
0.5 seconds.
The three-dimensional CT reconstructions and CT-simulated
anteroposterior and Judet views of the pelvis werecreated by
radiologists who used a standardized computerworkstation and
software (TeraRecon, San Mateo, CA). Thereconstructions (image set
C) and simulated views (image setD) allowed for multiple viewing
directions as controlled by theviewer, as is typical clinically. To
obtain the three-dimensionalimages, 2 3 2 mm thick images were
used. All images wereviewed with a General Electric Picture
Archiving and Com-munication System (General Electric Corporation,
Waukesha,WI) on an Agfa-Gevaert computerized workstation (Agfa-
Gevaert Group, Mortsel, Belgium).
Image EvaluationEach image set was evaluated in random order
(as
described previously) by four trauma
fellowship-trainedorthopaedic surgeons who routinely treat
acetabular fracturesin separate sessions. The diagnosis was
recorded by eachsurgeon as either no fracture evident or as one of
the 10types of acetabular fractures of the Letournel and
Judetclassification system3: anterior wall, anterior column,
posteriorwall, posterior column, transverse, T-type, anterior
column or
wall with posterior hemitransverse, both-column, posteriorcolumn
and posterior wall, or transverse and posterior wall.
Five weeks after all images had been reviewed by allsurgeons,
the gold standard diagnosis was determined by allfour surgeons
through a group consensus meeting. For thegold standard diagnosis,
all 75 fractures were evaluated withall four imaging methods
available; the viewers were still
FIGURE 1. Three-dimensional computed tomography recon-structions
of an acetabular fracture. Two views are shown
(AB). The contralateral hemipelvis and femoral head havebeen
removed for better visualization. The images can berotated 360 in
both the vertical and horizontal planes.
q 2010 Lippincott Williams & Wilkins www.jorthotrauma.com |
285
J Orthop Trauma Volume 24, Number 5, May 2010 Determining the
Diagnosis of Acetabular Fractures
-
7/27/2019 Avaliacao TC Acetabulo
3/7
blinded to the patient identifiers and to the diagnoses made
bythe individual surgeons. For any diagnosis with disagreementafter
discussion, a vote was taken to determine the goldstandard
diagnosis. Disagreement existed regarding only twoof the 75
fractures.
AnalysisWe first compared the four imaging methods regarding
ability to agree with the gold standard diagnosis.
Consideringthat the frequencies of the 10 types of acetabular
fractures arenot equal in clinical practice nor were they in our
data set, theanalysis had to be weighted so that common fracture
patternsdid not falsely elevate the level of agreement. Agreement
wasassessed with the use of kappa statistics for multiple raters
andnominal data.
We next compared the four imaging methods regardingability to
consistently predict the diagnosis among surgeons.Again, agreement
was assessed with the use of kappa statisticsfor multiple raters
and nominal data. Additionally, a sensitivityanalysis was conducted
to ascertain that no single rater was
driving the results of the study. Repetition of the analyses
afterexclusion of a single rater did not substantially change
theoverall study conclusions.
Based on clinical experience of what fracture diagnosesare often
debated by residents, fellows, and attendings, wehypothesized that
three of the fracture types would be par-ticularly likely to cause
disagreement: associated both-column,T-type, and anterior column or
wall with posterior hemitrans-verse. Therefore, we repeated these
analyses after compressingthe 10 fracture types down to eight. That
is, we considered thethree aforementioned fracture types as
identical for purposesof this subanalysis to learn whether removing
disagreementregarding the three fracture types would change our
results.
Statistical AnalysisAgreement between the imaging methods and
the gold
standard diagnosis was evaluated with the use of kappastatistics
for multiple raters and nominal data. The kappavalues were
interpreted by using the method described byLandis and Koch.14 The
guidelines propose that kappa valuesof 0 to 0.20 indicate poor
agreement, 0.21 to 0.40 fairagreement, 0.41 to 0.60 moderate
agreement, 0.61 to 0.80substantial agreement, and greater than 0.80
almost
perfect agreement. Ninety-five percent confidence intervalswere
generated by using bootstrap techniques in a commer-cially
available statistical package (STATA; SAS Institute,Inc., Cary, NC)
yielding comparable results.
RESULTSFor each of the imaging methods (image sets A, B, C,
and D), we assessed agreement with the gold standarddiagnosis.
Statistically significant variation in agreement withthe gold
standard was shown based on imaging method (P,0.01, analysis of
variance). Image set B (Judet view plainradiographs alone)
performed more poorly than did the otherthree image sets (P, 0.05,
Duncans multiple range test) withonly a 52% rate of agreement with
the gold standard diagnosis(Table 1).
FIGURE 2. Simulated anteroposterior (A) and Judet views
(BC)created from computed tomography (CT) scans of an
acetabularfracture. The images simulate radiographs but are based
on CTdata. The images can be rotated 360 about vertical
andhorizontal axes. The images are not affected by body
habitus,bowel gas, or the presence of contrast agent in the
bladder. Thisis the same patient whose images are shown in Figure
3.
286 | www.jorthotrauma.com q 2010 Lippincott Williams &
Wilkins
OToole et al J Orthop Trauma Volume 24, Number 5, May 2010
-
7/27/2019 Avaliacao TC Acetabulo
4/7
The results reported in the previous paragraph are
notsatisfactory because they do not adjust for chance
agreement.That is, raters are likely to agree regarding certain
diagnoses(such as posterior wall fractures) that are highly
prevalent,even if all the raters do is guess posterior wall for all
the
fractures. As discussed, we then adjusted for this effect
andcalculated kappa values, which account for the fact that
agree-ment exists between raters based on chance alone (Table
2).
When we used the more methodologically rigoroustechnique, image
set B (Judet view plain radiographs alone)was again shown to be
statistically significantly less accuratethan image sets A, C, and
D (P, 0.05, analysis of variance,Duncans multiple range test) in
terms of agreeing with thegold standard diagnosis. The image sets
that included CT data(image sets A, C, and D) all had kappa values
that indicatedsubstantial agreement, whereas the image set that
included
plain radiographs alone (image set B) was rated as
havingmoderate agreement.
We next analyzed the number of times the raters agreed
on a diagnosis (interobserver reliability) for each of the
fourimaging methods to determine which produced the mostconsistent
results (Table 3). Image set B (plain radiographsalone) was
statistically significantly less consistent than theimage sets that
included CT data (image sets A, C, and D)(P, 0.05, analysis of
variance, Duncans multiple range test).
We repeated these analyses after compressing the classi-fication
system down to only eight fracture types by consider-ing three of
the fracture types to be the same (associated
both-column, anterior column or wall with posterior
hemi-transverse, and T-type), as discussed previously. Doing
soremoved any differences from the data on these three
fracturetypes that we thought might cause particularly high levels
of
disagreement; however, the reanalysis yielded results similarto
those of the initial analysis that analyzed all 10 fracturetypes
(data not shown). We then analyzed the data by fracturetype (Table
4); however, the large number of fracture types
presents too small a sample size for statistical analysis
regardingthis issue.
DISCUSSIONThe current standard radiographic assessment of
a patient with an acetabular injury begins with three viewsof
the pelvis: anteroposterior, obturatoroblique, and iliacoblique.47
With the addition of newer types of images suchas axial view CT
scans11,12,1520 and three-dimensionalCT reconstructions,911 it was
thought that not only wouldsurgeons be able to better identify
marginal impaction or loose
bodies within the acetabulum but the diagnostic accuracy ofthe
acetabular fracture patterns might improve.5,13
Little previous work has investigated the influence ofimaging
techniques on the diagnosis of acetabular fractures.One study
showed that reliability in classifying acetabularfractures by using
the anteroposterior view pelvic radiographalone was not improved
with additional oblique (Judet)views21; however, the study
participants were junior residentsand community orthopaedic
surgeons who presumably did nottreat acetabular fractures, so the
applicability of that study foracetabular surgeons is unclear. A
study of orthopaedic traumasurgeons of various experience failed to
show an advantageof axial view CT scans in improving the
reliability of theclassification system.5 That study did not
analyze three-dimensional CT-based data and used the surgeons
opinionfrom the operating room as a gold standard.
Two previous studies have investigated the role of
three-dimensional CT scans in the classification of
acetabularfractures.13,22 In a smaller study of 20 fractures, only
one of the
five participants was an orthopaedic trauma surgeon and thekappa
values were low (kappa = 0.24), representing only fairagreement
when using either plain radiographs or three-dimensional CT
scans.13 The kappa values were much lowerthan those previously
reported in the literature5 and muchlower than those in our study
in which all the participants wereorthopaedic trauma surgeons. A
second larger study of 101fractures evaluated two radiologists
diagnoses and foundresults similar to those of our study with
interobserveragreement rated as substantial (kappa = 0.70) with
multi-detector CT using three-dimensional reconstructions but
onlymoderate (kappa = 0.42) with Judet films alone.22 When
TABLE 1. Number of Raters Agreeing With Gold StandardDiagnosis
by Imaging Method
Imaging Method
A B C D
4 of 4 30 19 35 33
3 of 4 17 13 10 122 of 4 17 16 10 13
1 of 4 7 9 6 9
0 of 4 4 18 14 8
Percentage agreement 71% 52%* 65% 68%
*Lower agreement with gold standard, P, 0.05.
TABLE 2. Chance-Adjusted Agreement With GoldStandard
Diagnosis*
Imaging Method
A B C D
Kappa 0.647 0.480 0.620 0.642
95% confidenceinterval
0.6130.688 0.4370.546 0.5790.656 0.6070.709
*Kappa statistics with 95% confidence intervals.Significant
difference at the P, 0.05 level.
TABLE 3. Chance-Adjusted Agreement on Diagnosis AmongImaging
Methods*
Imaging Method
A B C D
Kappa 0.560 0.512 0.640 0.659
95% confidenceinterval
0.5190.630 0.4280.581 0.5840.689 0.6170.717
*Kappa statistics with 95% confidence intervals.P, 0.05.
q 2010 Lippincott Williams & Wilkins www.jorthotrauma.com |
287
J Orthop Trauma Volume 24, Number 5, May 2010 Determining the
Diagnosis of Acetabular Fractures
-
7/27/2019 Avaliacao TC Acetabulo
5/7
comparing the diagnoses made during the study with the
diagnoses from the operative reports, agreement was higherwhen
based on CT scans than when based on radiographs,although the
difference was statistically significant for onlyone of the
radiologists (P = 0.01 and 0.06). The applicabilityof the
conclusions presented in these studies to diagnosesmade by surgeons
who regularly treat acetabular fractures isunknown.
With our study, we retested the hypothesis that CT scansin
comparison with plain radiographs alone will improveaccuracy in
classifying different acetabular fracture patterns.In contrast to
findings previously presented in the literature,5,13
we found that the diagnostic accuracy of plain radiographsalone
was worse than that of CT scans, questioning theusefulness of plain
radiographs for diagnosis of fracture
pattern. Comparing the gold standard diagnosis with the
fourimaging sets, Judet view plain radiographs had a lower
percentage of agreement (52% versus 71%, 65%, and 68%;P, 0.05,
analysis of variance, Duncans multiple range test)and a worse kappa
value than did the CT scans (P, 0.05,analysis of variance, Duncans
multiple range test) (Tables 1and 2). The kappa values for all
three imaging methods thatincluded CT scans showed substantial
agreement, whereas thekappa values for the plain radiographs alone
showed only fairagreement.
Several possible explanations exist to explain why ourfindings
differ from those of previous work. In clinical
practice, poor-quality radiographs are somewhat common,
often because of body habitus, inadequate patient
rotation,improper x-ray penetration, bowel gas, or contrast agent
in thebladder (Fig. 3). We did not exclude any patients from
ourstudy because of poor film quality; the included films werethose
the surgeon actually used for management of the case.In that
manner, we hoped to realistically characterize theinfluence of the
imaging studies on surgeons diagnosis. It isunclear whether
previous studies included only patientswith adequate plain films,
so it is possible that a selection
bias was introduced in the study population of those
otherstudies as a result of excluding patients with lower
qualityradiographs.
Another possible explanation for the difference between
our findings and the findings of previous reports in
theliterature is the detail of the CT reconstructions.
Modernsoftware has improved such that recreated images have
betterresolution and more options are available for viewing the
data.For example, the three-dimensional and simulated views can
be rotated 360 in any direction. Also, the femoral head can
besubtracted out of the acetabulum, providing the surgeon withan
inside view of the pelvis unlike that of any plain radiograph.
Other possibilities include differences in the details ofour
methodology. We used a statistical methodology thatcorrected for
chance agreement and unequal fracture patternfrequencies, unlike
previous studies. We used a consensusgold standard based on
radiographs because we were notconvinced that the operative
surgeons opinion of the fracturemorphology should be the gold
standard, particularly forfractures with which the approach would
not allow access tofracture lines on the opposite column.
Our present study followed patients in a consecutivefashion,
recreating clinical practice. This approach caused thenumber of
certain types of acetabular fracture patterns to beseen more
frequently, such as posterior wall and transverse
posterior wall types (Table 4). Furthermore, a selection
biasmight have been introduced toward the radiologists obtainingand
saving three-dimensional reconstructions of more in-teresting
fracture patterns, because we had to exclude any
patient who did not have three-dimensional
reconstructionsavailable for analysis, thus biasing the data set
away from
simple fractures and toward fractures that are more prone
todisagreement regarding classification. However, we attemptedto
account for these factors by adjusting for chance agreementamong
imaging methods regarding diagnosis with ourstatistical
methods.
Strengths of our study include the randomized, blindedfashion in
which four independent trauma fellowship-trainedsurgeons rated each
image set for a diagnosis. We looked ata relatively large
consecutive series of patients and includedJudet view plain
radiographs without regard for image quality,axial view CT scans,
three-dimensional CT reconstructions,and CT-simulated
anteroposterior and Judet views to best
TABLE 4. Accuracy in Diagnosis as a Function of Fracture
Type
Fracture Type(by gold standard)
No. of
Fractures(Total = 75)
Percent
AgreementCT + Judet (A)
Percent Agreement
Actual JudetAlone (B)
Percent
Three-DimensionalCT (C)
Percent AgreementSimulated Judet (D)
Percent Average
Across All FourImaging Modalities
Anterior wall 0
Anterior column 5 75 45 75 65 65
Posterior wall 20 89 79 85 95 87
Posterior column 2 63 63 50 63 60
Transverse 4 81 75 100 81 84
T-type 3 33 0 17 58 27
Anterior column or wall withposterior hemi-transverse
7 43 14 29 39 31
Both-column 11 86 89 95 89 90
Posterior column and posterior wall 4 63 50 75 75 66
Transverse and posterior wall 19 68 36 46 47 49
CT, computed tomography; , not applicable.
288 | www.jorthotrauma.com q 2010 Lippincott Williams &
Wilkins
OToole et al J Orthop Trauma Volume 24, Number 5, May 2010
-
7/27/2019 Avaliacao TC Acetabulo
6/7
mimic images currently available to acetabular surgeons. Wethink
our statistical methods adequately accounted for chance
agreement and variation in the observed frequency of
fracturepatterns.Another component of evaluating imaging modalities
is
the cost. The professional fee plus the hospital charges for
eachof the image sets at our hospital in 2009 are as follows:
imageset A, $262; image set B, $687; and image sets C and D,
$405.Many institutions obtain A, B, C, and D, which would
cost$1354. These cost values represent only one hospitals
feeschedule, and further work is required to conduct
cost:benefitanalysis of these imaging modalities.
The results of this study suggest future directions forresearch
and clinical practice. With improving CT software
and different imaging modality techniques, the
preoperativeradiographic workup for patients with acetabular
fracturesmight ultimately change. Perhaps after identifying
anacetabular fracture on a routine anteroposterior view radio-graph
of the pelvis, the only other imaging modality requiredis CT. We
have begun to study this protocol at our center.
It has been our experience that it often is not practicalor even
possible to obtain additional radiographs of patientswhose images
are of poor quality, because the patients might
be hemodynamically unstable or have associated injuries suchas
unstable spinal trauma. Furthermore, obtaining Judet
viewradiographs of awake patients typically is painful for the
patients. Reshooting additional radiographs in pursuit of
theperfect Judet view radiograph subjects patients to
additional
pain, radiation, increased costs, and preoperative
evaluationtime. CT scans can eliminate all the confounding factors
andrecreate a similar image virtually every time. One
theoreticaladvantage of actual Judet films is that after rotating
the patient45 onto a foam block to elevate one hip to obtain
theradiographs, gravity provides stress to the hip that might
reveal
subluxation that might not be evident while the patient
issupine; however, this phenomenon is unlikely to affect
thediagnosis of fracture type and so will require further
inves-tigative research.
The CT data obtained during the initial CT scanningcan be used
to construct traditional axial view images, three-dimensional
reconstructions, and simulated Judet views. Thesimulated Judet
views have an appearance similar to that ofa standard radiograph
without the imperfections that a plainradiograph might have and can
be used in the operating roomor clinic (Fig. 2). The views can be
digitally rotated at thesurgeons discretion, recreating the perfect
Judet view. Also,the femoral head can be digitally subtracted from
three-dimensional views, creating an internal acetabular view that
no
plain radiograph has been able to show (Fig. 1).It is important
to note that our study investigated only
the usefulness of these imaging modalities in making
thediagnosis. Imaging is used to obtain other information such
asthe presence of joint impaction, intra-articular fragments,
andthe degree of fracture comminution, and to decide on
thetreatment and surgical approach, if surgery is indicated.
Ourstudy did not assess any of these additional issues.
Furtherresearch is required to investigate whether
three-dimensionalreconstructions and CT-simulated views are
reliable andclinically efficacious and whether they potentially
limitradiation exposure, cost, and pain for patients who
sustainacetabular fractures.
ACKNOWLEDGMENTSWe acknowledge the important assistance of
Mary
Zadnik Newell, OTR/L, Med, and Senior Editor and Writer,Dori
Kelly, MA, Department of Orthopaedics, University ofMaryland School
of Medicine.
REFERENCES1. Letournel E. Fractures of the acetabulum: a study
of a series of 75 cases [in
French]. J Chir (Paris). 1961;82:4787.2. Judet R, Judet J,
Letournel E. Fractures of the acetabulum: classification
and surgical approaches for open reduction: preliminary report.
J BoneJoint Surg Am. 1964;46:16151646.
FIGURE 3. Example of poor-quality obturatoroblique Judetview (A)
and poor-quality iliac-oblique Judet view (B) plainradiographs
obtained before operative treatment of anacetabular fracture. Image
quality was limited by the patientsbody habitus and bowel gas. This
is the same patient whoseimages are shown in Figure 2.
q 2010 Lippincott Williams & Wilkins www.jorthotrauma.com |
289
J Orthop Trauma Volume 24, Number 5, May 2010 Determining the
Diagnosis of Acetabular Fractures
-
7/27/2019 Avaliacao TC Acetabulo
7/7
3. Letournel E. Acetabulum fractures: classification and
management. ClinOrthop Relat Res. 1980;151:81106.
4. Letournel E, Judet R. Fractures of the Acetabulum, 2nd ed.
New York:Springer; 1993.
5. Beaule PE, Dorey FJ, Matta JM. Letournel classification for
acetabularfractures: assessment of interobserver and intraobserver
reliability. J Bone
Joint Surg Am. 2003;85:1704 1709.6. Tornetta P III. Displaced
acetabular fractures: indications for operative
and nonoperative management. J Am Acad Orthop Surg.
2001;9:1828.7. Mack LA, Harley JD, Winquist RA. CTof acetabular
fractures: analysis of
fracture patterns. AJR Am J Roentgenol. 1982;138:407412.8. Mayo
KA. Open reduction and internal fixation of fractures of the
acetabulum: results in 163 fractures. Clin Orthop Relat Res.
1994;305:3137.9. Billet FP, Schmitt WG, Gay B. Computed tomography
in traumatology
with special regard to the advances of three-dimensional. Arch
OrthopTrauma Surg. 1992;111:131137.
10. Burk DL Jr, Mears DC, Kennedy WH. Three-dimensional
computedtomography of acetabular fractures. Radiology.
1985;155:183186.
11. Gautsch TL, Johnson EE, Seeger LL. True three
dimensionalstereographic display of 3D reconstructed CT scans of
the pelvis andacetabulum. Clin Orthop Relat Res.
1994;305:138151.
12. Harley JD, Mack LA, Winquist RA. CT of acetabular fractures:
compari-son with conventional radiology.AJR Am J Roentgenol.
1982;138:413417.
13. Visutipol B, Chobtangsin P, Ketmalasiri B, et al. Evaluation
of Letournel
and Judet classification of acetabular fracture with plain
radiographs and
three-dimensional computerized tomographic scan. J Orthop Surg
(HongKong). 2000;8:3337.
14. Landis JR, Koch CG. The measurement of observer agreement
forcategorical data. Biometrics. 1977;33:159174.
15. Hayes CW, Balkissoon AR. Current concepts in the imaging of
the pelvisand hip. Orthop Clin North Am. 1997;28:617642.
16. Rafii M, Firooznia H, Golimbu C, et al. The impact of CT in
the clinicalmanagement of pelvic and acetabular fractures. Clin
Orthop Relat Res.1983;178:228235.
17. Brandser E, Marsh JL. Acetabular fractures: easier
classification witha systematic approach. AJR Am J Roentgenol.
1998;171:12171228.
18. Hunter JC, Brandser EA, Tran KA. Pelvic and acetabular
trauma. RadiolClin North Am. 1997;35:559590.
19. Martin JS, Marsh JL. Current classification of fractures:
rational andutility. Radiol Clin North Am. 1997;35:491506.
20. Resnik CS, Stackhouse DJ, Shanmuganathan K, et al. Diagnosis
of pelvicfractures in patients with acute pelvic trauma: efficacy
of plainradiographs. AJR Am J Roentgenol. 1992;158:109112.
21. Petrisor BA, Bhandari M, Orr RD, et al. Improving
reliability in theclassification of fractures of the acetabulum.
Arch Orthop Trauma Surg.2003;123:228233.
22. Ohashi K, El-Khoury GY, Abu-Zahra KW, et al.
Interobserveragreement for Letournel acetabular fracture with
multidetector CT:are standard Judet radiographs necessary?
Radiology. 2006;241:
386391.
290 | www.jorthotrauma.com q 2010 Lippincott Williams &
Wilkins
OToole et al J Orthop Trauma Volume 24, Number 5, May 2010