Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
Magnetic Resonance Imaging 29 (2011) 391–400
Automated vessel segmentation using cross-correlation and pooledcovariance matrix analysis☆
Jiang Dua,⁎, Afshin Karimia, Yijing Wub, Frank R. Korosecb,Thomas M. Gristb, Charles A. Mistrettab
aDepartment of Radiology, University of California, San Diego, San Diego, CA 92103-8226, USAbDepartment of Medical Physics and Radiology, University of Wisconsin, Madison, WI 53792, USA
Received 19 December 2009; revised 17 March 2010; accepted 3 September 2010
Abstract
Time-resolved contrast-enhanced magnetic resonance angiography (CE-MRA) provides contrast dynamics in the vasculature and allowsvessel segmentation based on temporal correlation analysis. Here we present an automated vessel segmentation algorithm includingautomated generation of regions of interest (ROIs), cross-correlation and pooled sample covariance matrix analysis. The dynamic images aredivided into multiple equal-sized regions. In each region, ROIs for artery, vein and background are generated using an iterative thresholdingalgorithm based on the contrast arrival time map and contrast enhancement map. Region-specific multi-feature cross-correlation analysis andpooled covariance matrix analysis are performed to calculate the Mahalanobis distances (MDs), which are used to automatically separatearteries from veins. This segmentation algorithm is applied to a dual-phase dynamic imaging acquisition scheme where low-resolution time-resolved images are acquired during the dynamic phase followed by high-frequency data acquisition at the steady-state phase. The segmentedlow-resolution arterial and venous images are then combined with the high-frequency data in k-space and inverse Fourier transformed to formthe final segmented arterial and venous images. Results from volunteer and patient studies demonstrate the advantages of this automatedvessel segmentation and dual phase data acquisition technique.© 2011 Elsevier Inc. All rights reserved.
Keywords: Contrast-enhanced MR angiography; Time-resolved; Matched filtering; Cross correlation; Pooled covariance matrix analysis; Vessel segmentation
1. Introduction
Conventional contrast-enhanced magnetic resonanceangiography (CE-MRA) produces a single image volumeproperly timed to capture the first pass of a contrast agent formaximal arterial enhancement [1]. Retrograde flow, delayedor asymmetric filling of contrast agent, or cases with fastarterial-venous transit of the agent may result as anadaptation to vessel occlusive disease or produce suboptimalarterial angiography with significant venous contamination[1–4]. Time-resolved acquisitions can resolve these diffi-culties by acquiring a series of three-dimensional (3D)images to capture the detail of the contrast dynamics of thevasculature system [2–8], but at the cost of reduced spatial
☆ The contract grant sponsor is the American Heart Association andGE Healthcare.
⁎ Corresponding author. Tel.: +1 619 471 0519; fax: +1 619 471 0503E-mail address: [email protected] (J. Du).
0730-725X/$ – see front matter © 2011 Elsevier Inc. All rights reserved.doi:10.1016/j.mri.2010.09.003
.
resolution and signal-to-noise ratio (SNR) [9]. It is ofsignificant interest to generate dynamic images together witharterial and venous images with high spatial resolution, highSNR and contrast-to-noise ratio (CNR) in a single scan.
Time-resolved CE-MRA provides contrast dynamics inthe vasculature. This temporal information can be used toseparate arteries from veins using a variety of algorithmssuch as correlation analysis [10], matched filtering [11–13],eigenimage filtering [14], feature space analysis [15] orMahalanobis distance (MD) analysis [16–18]. The ability toseparate arteries from veins allows extended acquisition atthe steady state as well as matched filtering of the whole datato improve both spatial resolution and SNR withoutsignificant CNR reduction [17,18]. Segmented arterialimages with high SNR and CNR have been demonstratedby several groups [10–18]. However, most of the segmen-tation algorithms require operator intervention such asthresholding [19]. Improper thresholding may significantlyreduce the image quality. Furthermore, the contrast

392 J. Du et al. / Magnetic Resonance Imaging 29 (2011) 391–400
dynamics pattern may vary significantly within a largeimaging field of view (FOV) due to delayed filling,asymmetric filling or slow blood flow in the tortuous vessels[1–8]. Correlation with single arterial and/or venousreference curves may result in misclassification. A singleglobal thresholding of the correlation coefficients or MDmay not work well. Fully automated segmentation withconsideration of the contrast variation within the imagingFOV is highly desirable to reduce the labor cost and improvethe robustness of the segmentation technique.
In this article, we present a fully automated region-specific segmentation algorithm for effective separation ofarteries from veins based on cross-correlation and pooledcovariance matrix analysis. This segmentation algorithm isapplied to a dual phase dynamic imaging acquisition schemewhere low-resolution time-resolved images are acquiredduring the dynamic phase followed by high-frequency dataacquisition at the steady-state phase. Matched filtering of thetime-resolved data and steady state is used to improve SNR.The 3D dynamic images are divided into multiplesubregions to account for the variation of contrast arrivaltimes. Arteries, veins and background are separated usingregion-specific cross-correlation and pooled covariance
Fig. 1. Flow chart for region-s
matrix analysis. The segmented low-resolution arterial andvenous images are then combined with the high-frequencydata in k-space and inverse Fourier transformed to form thefinal segmented arterial and venous images. Results fromvolunteer and patient studies demonstrate the advantages ofthis automated vessel segmentation and dual phase dataacquisition technique.
1.1. Theory
The fully automated vessel segmentation algorithmincludes the following five steps: (1) automated region-specific regions of interest (ROIs) generation; (2) region-specific matched filtering; (3) region-specific cross-correla-tion analysis; (4) region-specific pooled covariance matrixanalysis; (5) formation of the composite images. Details ofeach step are given in the following sections.
1.2. Automated region-specific ROI generation
ROIs and reference curves for artery, vein and back-ground are needed for matched filtering and subsequentcross-correlation and pooled covariance matrix analysis [16].Fig. 1 shows the flow chart for this algorithm. First, the 3D
pecific ROI generation.

393J. Du et al. / Magnetic Resonance Imaging 29 (2011) 391–400
dynamic images are divided into multiple subregions (suchas 16 equal-sized subregions: eight on the left half andeight on the right half of the imaging FOV). In eachregion, contrast arrival time (time to reach 75% of the peaksignal) map and contrast enhancement (peak signal minuspre-contrast signal) map are generated as shown in Fig. 2Aand B. The region-specific contrast arrival time histogramsare generated for voxels surviving an iteratively reducedcontrast enhancement thresholding. Initially, the contrastarrival time histogram shows only one peak with maximalcontrast enhancement. The iteration stops when two ormore peaks appear in the contrast arrival time histograms.The first peak corresponds to the contrast arrival time forartery. The second peak corresponds to the contrast arrivaltime for vein or enhancing background tissue. Finally,voxels are ordered in terms of contrast enhancement andthe arterial ROIs are generated by choosing voxels witharterial contrast arrival time and highest contrast enhance-ment. The venous ROIs are generated by choosing voxelswith venous contrast arrival time and highest contrastenhancement. The background ROIs are generated forvoxels with lowest CE. A relatively large size of voxels(NREF=500) is chosen to increase the statistical informationin the ROIs [16–18]. Fig. 2C shows automatically generatedROIs with eight subregions (for simplicity) for artery(brighter in signal intensity) and vein (darker in signalintensity), respectively. In regions without venous signals,the enhancing background tissues are treated as the venousfeature. The value of the reference curve, SREF
j (ti) for regionj at time ti is calculated as the mean ROI signal for that timeframe. Here REF can be artery, vein or background.
1.3. Region-specific matched filtering
Matched filtering provides optimal SNR in an arterial/venous image by weighting each time frame data depending
Fig. 2. Contrast enhancement map (A), contrast arrival time map (B) and the auto
on the signal intensity within the artery/vein of eachsubregion [11–13]. The signal curve is measured from thereconstructed time series of images using the automaticallygenerated ROIs in the artery and vein, respectively. Thearterial reference curve for region j is defined as SA
j (ti) forthe ith time frame. The venous reference curve for region j isdefined as SV
j (ti) for the ith time frame. A white noise powerspectrum is considered for all the images, where the noisepower (denoted as σ) is uniform over all the spatialfrequencies, although MRI magnitude images are typicallymodeled by a Rician distribution [20]. To form a matchedfiltered arterial/venous image, the weighting coefficientdefined as WA
j (ti) or WVj (ti) for region j and time frame i
is just the arterial or venous reference signal level:
W jA tið Þ = S j
A tið Þ ð1Þ
W jV tið Þ = S j
V tið Þ ð2ÞThe corresponding matched filtered arterial/venous
image signal and noise for voxel k at region j can becalculated as follows:
S jk MFAð Þ =
Xi
W jA tið ÞS j
k tið Þ =Xi
S jA tið ÞS j
k tið Þ ð3Þ
S jk MFVð Þ =
Xi
W jV tið ÞS j
k tið Þ =Xi
S jV tið ÞS j
k tið Þ ð4Þ
r jk MFAð Þ2 =
Xi
W jA tið Þ2r tið Þ2 ð5Þ
r jk MFVð Þ2 =
Xi
W jV tið Þ2r tið Þ2 ð6Þ
To evaluate this SNR gain quantitatively, we performed asimulation as shown in Fig. 3. A small square object with
matically generated region-specific (eight regions for this case) ROIs (C).

Fig. 3. A typical contrast time course used for simulation (A), the peak frame with white noise added (B) and the corresponding matched filtered image (C). SNRis increased by 2.3 times after matched filtering relative to the peak frame.
394 J. Du et al. / Magnetic Resonance Imaging 29 (2011) 391–400
typical temporal curve as shown in Fig. 3A was added withwhite noise. The peak image has a relative SNR of 1, whichis increased to 2.3 after the matched filtering.
1.4. Region-specific cross-correlation analysis
Temporal correlation analysis is applied to the time-resolved 3D data sets. The time series of images areinspected and the automatically generated region-specificROIs are used to define arterial, venous and backgroundreference curves for the cross-correlation analysis. The timecourse for each voxel from region j is compared to theregion-specific arterial reference curve SA
j (ti), venousreference curve SA
j (ti) and background reference curve SBj
(ti) using temporal cross correlation. The cross-correlationcoefficient (CC) of the time course of voxel k from regionj, Sk
j (ti), with the arterial, venous or background referencetime course, SREF
j (ti) from the same region, is calculatedas follows:
CC jk;REFðS j
k ;SjREFÞ =
Pi
S jREFðtiÞ − S j
REF
� �� SjkðtiÞ − S j
k
� �ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiPi
S jREFðtiÞ−S j
REF
� �2r
�ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiPi
S jk ðtiÞ−S j
k
� �2r
ð7Þ
where S jREF and S j
k are the time-averaged values of thereference ROI and the voxel from region j, respectively.
1.5. Region-specific pooled covariance matrix analysis
Voxel k from region j is considered to be located in a3D feature space having arterial (CCkA
j (Skj, SA
j )), venous(CCkV
j (Skj, SV
j )) and background (CCkBj (Sk
j, SBj ))
correlation coefficients as axes. In the 3D feature spacethe voxels included in the region-specific ROIs definearterial, venous and background peaks, respectively. Thecross-correlation coefficients of the NREF voxels in each ofthe three reference ROIs determine a 3×1 matrix. Thevector for the kth voxel from region j is given by
CC jk = CC j
k;A S jA; S
jk
� �; CC j
k;V S jV; S
jk
� �; CC j
k;B S jB; S
jk
� �� �.
The mean vector for each reference ROI from region j,
m j , is given by:
m j =1
Nref
XNref
l =1
CC jl ð8Þ
The 3×3 variance matrix, Ω j, for region j is given by:
X j =1
NREF − 1
XNREF
l =1
CC jl − m j
� �CC j
l −m j
� �T
ð9Þ
Pooled sample covariance matrix is the normalization ofmultiple-feature covariance matrix. In the case of threefeatures— artery (covariance matrixΩA
j , ROI size NAj ), vein
(covariance matrix ΩVj , ROI size NV
j ) and background(covariance matrix ΩB
j , ROI size NBj ) — the pooled sample
covariance matrix Ω j (P) can be calculated as follows:
X j Pð Þ =X3i=1
Nji − 1
� �Ω j
i
=X3i =1
N ji − 1
� � ð10Þ
Automated processing is performed by calculating theMD, which is a statistical distance measurement thataccounts for the widths of the reference cross-correlationcoefficient distributions [16], of each voxel relative to thearterial, venous and background peaks. The pooled MD of avoxel k from region j relative to each feature is estimated as:
MD jk = CC j
k −m j
� �T
X j Pð Þ−1 CC jk − m j
� �ð11Þ
Here MDkJ is a 1×3 matrix providing MD of voxel k
from region j relative to the arterial, venous andbackground features, respectively. In general, the distribu-tion of arterial, venous and background voxels falls off at

395J. Du et al. / Magnetic Resonance Imaging 29 (2011) 391–400
different rates as one moves in different directions from thepeaks in the 3D feature space. Therefore, voxels that areequidistant from a particular peak in the 3D feature spacecan be situated at different MDs from the peak. Voxel kfrom region j is automatically allocated to the group withthe smallest MD.
1.6. Formation of the composite images
In this article, the segmentation algorithm is combinedwith a dual phase dynamic imaging acquisition schemewhere low spatial resolution time-resolved images areacquired during the dynamic phase followed by high spatialfrequency data acquisition at the steady-state phase [4]. Thefully automated region-specific segmentation algorithm isapplied only to the low-resolution dynamic data, with high-frequency data added back in the last step to improve spatialresolution [17]. Fig. 4 shows details of this region-specificdata acquisition and image processing strategy. The dynamicimages are acquired with relatively low spatial resolution sothat high temporal resolution images can be generated withhigh SNR for more robust segmentation. The segmentedarterial and venous images are then Fourier transformed intok-space and combined with the high spatial frequency dataacquired in the steady state. Finally, the composite k-spacedata is inverse Fourier transformed back to the image space
Fig. 4. Flow chart for steps to generate the segmented composite image: the dynamicwhich are used to generate the matched filtered images as well as the subsequent temvenous mask is applied to the low-frequency matched filtered images to produce lwith the high frequency matched filtered images in k-space and Fourier transformedand CNR.
to produce the segmented arterial and venous images withhigh spatial resolution, high SNR and CNR.
2. Materials and methods
Time-resolved 3D acquisitions of the peripheral MRAwere acquired in four volunteers and five patients using apreviously reported PR-HyperTRICKS pulse sequence [4],where undersampled PR acquisition is used in the kx–kyplane while Cartesian-encoded variable k-space sampling isperformed in the kz direction. The whole k-space is dividedinto four regions — A, B, C and D — along the through-plane direction. A, B and C regions were acquired during thedynamic phase, while the D region was acquired during thesteady-state phase. Details of the PR-HyperTRICKS acqui-sition were described in previous works [4]. Images werereconstructed on a standalone workstation (Impact 10000,Silicon Graphics, Mountain View, CA, USA) with softwarethat was developed in our laboratory.
The acquisition parameters for the volunteer/patientexams were as follows: FOV=44 cm, readout matrix=512,acquired slices=72, slice thickness=1.0 mm, TR/TE/flipangle=7.4 ms/2.6 ms/30°. The total acquisition time was 3min 58 s during which 24 time frames were acquired, withthe first 82 s for mask data acquisition and the last 58 s for the
images were first subjected to automatic generation of region-specific ROIsporal cross-correlation and pooled covariance matrix analysis; then, arterialow-resolution segmented matched filtered image, which are then combinedback to generate the final segmented arterial/venous images with high SNR
,/

Fig. 6. Segmentation of human thigh: matched filtering of low-resolutionsegmented matched filtered image with high spatial frequency data combinepeak arterial frame to 41/33 for the final segmented arterial image.
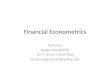
Fig. 5. Two-dimensional cross-correlation coefficient map in the arterial–venous feature space. The arterial ROIs (long arrow) and venous ROIs (shorarrow) have high cross-correlation coefficients.
396 J. Du et al. / Magnetic Resonance Imaging 29 (2011) 391–400
t
D region data acquisition. A total of 10 ml gadolinium-basedcontrast agent injection was administered through anintravenous catheter. All the volunteer and patient examswere performed on a standard 1.5-T MR scanner (Signa,GEMS, Waukesha, WI, USA) with a multi-channelquadrature/phased array peripheral vascular coil (MedicalAdvances, Milwaukee, WI, USA). The sum-of-squaresalgorithm was used to combine images from each channel.Written informed consent in accordance with regulations setforth by the institutional review board was obtained beforeimaging procedures.
dynamid (C); a
The dynamic images were processed using the fullyautomated segmentation algorithm discussed above. SNRand CNR were measured to quantitatively evaluate theefficiency of the segmentation technique. SNR was calcu-lated by dividing the mean signal intensity in an ROI drawnon a single slice in an arterial vessel by the standard deviationof the background signal [21]. CNR was calculated bydividing the mean difference signal intensity in an ROIdrawn on a single slice in an arterial vessel and vein/background by the standard deviation of the background.
3. Results
Fig. 5 shows a typical 2D map of the cross-correlationcoefficients from a typical slice relative to the arterial andvenous reference curves. The arterial ROIs are highlycorrelated with the arterial reference curve, while the venousROIs are highly correlated with the venous reference curve.Meanwhile, the arterial and venous ROIs are significantlycross correlated with correlation coefficients of more than0.5. For arterial ROIs, there is a small variation in correlationto the arterial reference curve but a big variation incorrelation to the venous reference curve. The same trendexists for the venous ROIs. This multidimensional distribu-tion is converted to a 1D MD distribution relative to eachfeature for better separation of arteries and veins as will bediscussed in the following section.
Fig. 6 shows an example of the multistep processingalgorithm. The low-resolution matched filtered image (Fig.6A) with a high SNR of 58 was subject to segmentation toproduce a low-resolution arterial image (Fig. 6B) with a highSNR of 50. The matched filtered image has a relatively lowCNR of 6.8 between artery and vein, which is increased to 41for the segmented matched filtered image. The segmentedarterial image was then combined with the high-frequency
c images (A); vein and background suppressed matched filtered image (B)nd peak arterial time frame (D). SNR/CNR are increased from 25/22 for the
;

397J. Du et al. / Magnetic Resonance Imaging 29 (2011) 391–400
data to generate the final segmented arterial image (Fig. 6C)with a high SNR of 41, which is 64% higher than that of thepeak arterial time frame (Fig. 6D) with an SNR of 25. Thevenous and background edge contamination is minimal inthe final segmented arterial images, which has a high CNR of33 between artery and vein, significantly higher than that of22 for the peak arterial frame.
Fig. 7A–D shows selected time frames of the lowerextremity of a healthy volunteer. The high temporalresolution of 4.2 s per frame provides excellent depictionof the contrast enhancement pattern in the tibia arteries. Thepopliteal–tibial artery was enhanced significantly earlierthan the plantar arch. Region-specific matched filteringprovides optimal SNR for all the arterial vasculature in thewhole FOV, as shown in Fig. 7E. If the whole FOV approach
Fig. 7. Selected dynamic images (every third frame) of the distal extremity of a vimage with the whole FOV approach (F), segmented image with the region-specifibetween artery and vein is increased from 3.6 for the matched filtered image to 54
was used, the distal arteries would be missed due tomisclassification of the arteries with contrast enhancementpattern quite different from the popliteal–tibial artery asshown in Fig. 7F. The region-specific segmentationalgorithm results in excellent separation of artery from veinand background, providing high-quality angiogram andvenogram as shown in Fig. 7G and H. The CNR betweenartery and vein is increased from 3.6 for the matched filteredimage to 54 for the segmented angiogram. The segmentedvenogram has a high CNR of 46 between vein and artery,providing excellent depiction of the venous vessels.
Fig. 8 shows a patient study of the distal extremity. Thematched filtered image (Fig. 8A) has a high SNR of 64 butvery poor CNR of 1.8 between the arteries and veins. Theautomated region-specific segmentation algorithm signifi-
olunteer (A–D), coronal MIP of the matched filtered image (E), segmentedc ROI approach (G) and the corresponding segmented venogram (H). CNRfor the segmented angiogram and 46 for the segmented venogram.

Fig. 8. MIP of the matched filtered image (A), the segmented arterial image (B) and venous image (C). CNR between artery and vein is increased from 1.8 for thematched filtered image to 24 for the segmented angiogram and 29 for the segmented venogram.
398 J. Du et al. / Magnetic Resonance Imaging 29 (2011) 391–400
cantly suppressed all the venous signals, providing a highCNR of 24 for the arterial image across all the FOV as shownin Fig. 8B. Meanwhile, high-quality venogram was alsogenerated with significant arterial suppression as shown inFig. 8C. The measured CNR between vein and artery is 29.
Fig. 9 shows another patient study of the distal extremity.The matched filtered images in the coronal and sagittalreprojections show high-resolution SNR but with significantvenous overlay. The region-specific automated segmentationalgorithm effectively suppressed all the venous signals,providing high-contrast arterial images in both the coronaland sagittal 3D maximal intensity projection (MIP). Themeasured CNR between artery and vein increased from 1.3for the matched filtered image to 16 for the segmentedarterial image.
High-quality arteriograms and venograms have beengenerated for all four volunteers and five patients. An SNRgain up to 32–68% and a CNR gain up to 26–51% relative tothe peak arterial frame are observed depending on where theROI is placed.
4. Discussion
The region-specific image processing has been widelyused in medical imaging [22–27]. Local details may be moreimportant than global contrast in diagnostic medical images.Adaptive histogram equalization and adaptive contrastenhancement are both well-known local enhancementmethods [22,23]. For example, Chang et al. [23] investigatedimage contrast enhancement based on a histogram transfor-mation of local standard deviation and reported significantedge enhancement with little noise overenhancement. Liuand Shaw [24] investigated regional improvement of SNRand CNR in dual-screen computed radiography chestimaging, where 12 ROIs were manually selected for
respective processing. The spatial variation of optimalweighting factors was investigated for four differentcombinations of standard resolution and high-resolutionscreens, and used to form the final composite image. AnSNR gain up to 19.1–45.7% and a CNR gain up to 29.2–43.9% were observed depending on the ROI and screencombination used [24].
However, most of the region-specific imaging processingalgorithms have focused on a single image rather than ondynamic image series. The time-resolved CE-MRA imageseries provide a wealth of information and can be employedto generate arterial and venous images with significantlyimproved spatial resolution and SNR. In this article, a fullyautomated segmentation algorithm for the generation ofperipheral MR arteriograms and venograms from time-resolved 3D CE-MRA was presented. This algorithmincluded automatic generation of region-specific ROIs,multifeature cross-correlation analysis and pooled covari-ance matrix analysis. The segmented match-filtered lowspatial frequency data was then combined with high spatialfrequency data in k-space and Fourier transformed to formthe final composite image with high resolution, high SNRand CNR with minimal venous and background edgecontamination. The preliminary results shown in Figs. 6 to9 demonstrate the robustness of the technique.
The multifeature correlation algorithm compares theshape of the arterial, venous and background signal–timecurves with the local signal curves, respectively. When thearrival of the contrast agent bolus in an arterial vesselsegment is delayed by a pathological process, or due to slowblood flow in a large imaging FOV such as the case shown inFig. 7A–D, its signal time course is shifted in time. This mayproduce a higher correlation coefficient for the arterialvoxels located in the distal of the imaging FOV with thevenous rather than with the arterial reference curve, resultingin misclassification [10]. The region-specific algorithm

Fig. 9. Coronal and sagittal MIP of the matched filtered images (A and B) aswell as the corresponding segmented images (C and D). The measured CNRbetween artery and vein increased from 1.3 for the matched filtered image to16 for the segmented arterial image.
399J. Du et al. / Magnetic Resonance Imaging 29 (2011) 391–400
resolves this uncertainty by dividing the whole imaging FOVinto multiple subregions. Within each subregion, automat-ically generated reference curves for the artery, vein andbackground features are used for cross-correlation andsubsequent pooled covariant matrix analysis. The robustnessof this technique has been demonstrated through Fig. 7G,where 16 subregions were used to address the significantcontrast variation across the whole FOV shown in Fig. 7A–D. In contrast, a global ROI for each feature results inmisclassification of arteries in the distal extremities as shownin Fig. 7F where only arterial edge information was shownfor the lower half of the imaging FOV.
The cross-correlation coefficients themselves can be usedto represent arterial and venous images, with limited
dynamic range especially for edge voxels with coefficientsbetween the arterial and venous reference curves [10].Transformation of the 2D arterial–venous feature space into1D MD has been proposed for better arterial–venousseparation [16–18]. However, global thresholding or Fermiweighting filter is needed to manually separate arteries fromveins [17,18]. The introduction of pooled covariance matrixanalysis of three-feature space (artery, vein and background)allows fully automated segmentation based on simplecomparison of the MD distance relative to each feature.The combination of this pooled covariance matrix analysiswith region-specific ROI generation and multifeature cross-correlation analysis improves the robustness of this tech-nique in segmenting arteries and veins in dynamic CE-MRAof the peripheral vasculature, as shown in Figs. 7–9.
In our case, an SNR gain up to 68% and a CNR gain up to51% are observed for the segmented images over the peakarterial frame. This is lower than what the simulation resultsshow. The SNR gains achieved through the automatedsegmentation technique were limited by the fact that onlyhalf of the low spatial frequency data were subject tosegmentation [4]. About half of the high spatial frequencydata were sampled during the steady state and werecombined with the segmented low spatial frequency datato form the composite image. Matched filtering only reducesthe low-frequency noise, with little effect on the high-frequency noise unless repeated high-frequency data wereacquired. Therefore, the SNR gain is much less than what ispredicted in Fig. 3 where all spatial frequencies wererepeatedly acquired so that the whole spectrum of the whitenoise is averaged. It is further complicated by the highlynonlinear operation of the MIP algorithm [28]. Thetheoretical predictions for the SNR improvement ofcorrelation over difference CE-MRA were reported to besignificantly lower than the measured SNR ratios by othergroups [10].
Although the automated region-specific segmentationalgorithm was only tested on the dynamic images acquiredwith the PR-HyperTRICKS sequence, it should work withany advanced techniques with high spatial and temporalresolution. Recently, several new techniques such as HYPR[29,30], VIPR [31], CAPR [32] and TRIPPS [33] have beenproposed for ultrafast imaging. The drawback of thesetechniques is the limited SNR for each dynamic frame. Thedynamic data can be low-pass filtered to generate low-resolution dynamic images which are then subject to theautomated region-specific segmentation algorithm. In thelast step, the segmented low-resolution arterial and venousimages can be combined with the match-filtered high-resolution data in k-space and inverse Fourier transformed toform the final composite arterial and venous images. Thisimage processing algorithm may provide significant SNR/CNR improvement for the final arteriogram and venogram.
One limitation of the technique is that the multiplesubregions were processed respectively, which may leavesome boundary artifacts as shown in Figs. 7 and 9. Another

400 J. Du et al. / Magnetic Resonance Imaging 29 (2011) 391–400
limitation is that the processing time will be increased,especially when more subregions are used. Region-specificsegmentation addresses the contrast dynamics variationacross the imaging FOV. The more subregions are used,the more robust the technique is in case of delayed filling,retrograde filling and other complex flowing pattern.However, the automated ROI generation technique will beless robust when a very small subregion is used or, to theextreme case, part of a single line is used because of the lackof clear separation between artery, vein and background. Therelation between region size and technical robustness needsfurther investigation, especially for clinical cases with verycomplex flow patterns.
5. Conclusions
Fully automated vessel segmentation can be applied totime-resolved CE-MRA to generate 3D angiograms andvenograms with high spatial resolution, high SNR and CNRwith minimal high-frequency venous/arterial and back-ground signal contamination.
References
[1] Prince MR, Grist TM, Debatin JF. 3D Contrast-enhanced MRangiography. New York (NY): Springer; 1998.
[2] Korosec FR, Frayne R, Grist TM, Mistretta CA. Time-resolvedcontrast-enhanced 3D MR angiography. Magn Reson Med 1996;36:345–51.
[3] Hany TF, Carroll TJ, Omary RA, Esparza-Coss E, Korosec FR,Mistretta CA, et al. Contrast-enhanced, single-injection, MRA withautomated table movement compared to multi-injection, time-resolvedCE 3D-MRA of the aorta and run-off vessels — initial results.Radiology 2001;72:221–66.
[4] Du J, Carroll TJ, Wagner HJ, Vigen K, Fain SB, Block WF, et al.Time-resolved, undersampled projection reconstruction imaging forhigh resolution CE-MRA of the distal runoff vessels. Magn ResonMed2002;48:516–22.
[5] Vigen KK, Peters DC, Grist TM, Block WF, Mistretta CA. Under-sampled projection–reconstruction imaging for time-resolved contrast-enhanced imaging. Magn Reson Med 2000;43:170–6.
[6] Grist TM, Korosec FR, Witte S, Waldovitch RC, Dolan RP, BridsonWE, et al. Steady-state and dynamic MR angiography with MS-325:initial experience in humans. Radiology 1998;207:539–44.
[7] Du J, Carroll TJ, Brodsky E, Lu AM, Mistretta CA, Block WF.Contrast enhanced peripheral magnetic resonance angiography usingtime-resolved vastly undersampled isotropic projection reconstruction.J Magn Reson Imaging 2004;20:894–900.
[8] Liu J, Redmond MJ, Brodsky EK, Alexander AL, Lu A, Thornton FJ,et al. Generation and visualization of four-dimensional MR angiog-raphy data using an undersampled 3D projection trajectory. IEEETrans Med Imaging 2006;25:148–57.
[9] Mistretta CA, Grist TM, Korosec FR, Frayne R, Peters DC, MazaheriY, et al. 3D Time-resolved contrast-enhanced MR DSA: advantagesand tradeoffs. Magn Reson Med 1998;40:571–81.
[10] Bock M, Schoenberg SO, Floemer F, Schad LR. Separation of arteriesand veins in 3D angiography using correlation analysis. Magn ResonMed 2000;43:481–7.
[11] Wang Y, Webber DM, Korosec FR, Mistretta CA, Grist TM, Swan JS,et al. Generalized matched filtering for time-resolved MR angiographyof pulsatile flow. Magn Reson Med 1993;30:600–8.
[12] Xue Q, Hu YH, Tompkins WJ. Neural-network-based adaptivematched filtering for QRS detection. IEEE Trans Biomed Eng1992;39:317–29.
[13] Huang Y, Merchant N, Wright GA. Comparison of matched-filteredtwo-dimensional projection and elliptical centric-ordered three-dimen-sional contrast-enhanced magnetic resonance angiography. J MagnReson Imaging 2004;20:435–42.
[14] Kaandorp DW, Kopinga K, Wijn PF. Venous signal suppression in 3Ddynamic Gd-enhanced carotid artery imaging using the eigenimagefilter. Magn Reson Med 1999;42:307–13.
[15] Zadeh HS, Windham JP, Peck DJ, Mikkelsen T. Feature space analysisof MRI. Magn Reson Med 1998;40:443–53.
[16] Afifi AA, Azen SP. Statistical analysis: a computer oriented approach.2nd ed. New York: Academic Press; 1979. p. 366.
[17] Mazaheri Y, Carroll TJ, Du J, Korosec FR, Block WF, Fain SB, et al.Combined time-resolved and high spatial resolution 3DMRA using anextended adaptive acquisition. J Magn Reson Imaging 2002;15:291–301.
[18] Du J, Carroll TJ, Block WF, Fain SB, Korosec FR, Grist TM, et al.SNR improvement for multiinjection time-resolved high-resolutionCE-MRA of the peripheral vasculature. Magn Reson Med 2003;49:909–17.
[19] Sahoo PK, Soltani S, Wong KC, Chen YC. A survey of thresholdingtechniques. Comput Graph Image Process 1988;41:233–60.
[20] Gudbjartsson H, Patz S. The Rician distribution of noisy MRI data.Magn Reson Med 1995;34:910–4.
[21] Kaufman L, Kramer DM, Crooks LE, Ortendahl DA. Measuringsignal-to-noise ratios in MR imaging. Radiology 1989;173:265–7.
[22] Sherrir RH, Johnson GA. Regionally adaptive histogram equalizationof the chest. IEEE Trans Med Imaging 1987;6:1–7.
[23] Chang DC, Wu WR. Image contrast enhancement based on ahistogram transformation of local standard deviation. IEEE TransMed Imaging 1998;17:518–30.
[24] Liu X, Shaw CC. Regional improvement of signal-to-noise andcontrast-to-noise ratios in dual-screen CR chest imaging— a phantomstudy. Med Phys 2001;28:1080–92.
[25] Du YP, Parker DL. Vessel enhancement filtering in three-dimensionalMR angiograms using long-range signal correlation. J Magn ResonImaging 1997;7:447–50.
[26] Du YP, Parker DL, Davis WL. Vessel enhancement filtering in three-dimensional MR angiography. J Magn Reson Imaging 1995;5:353–9.
[27] Saloner D, Hanson WA, Tsuruda JS, van Tyen R, Anderson CM, LeeRE. Application of a connected-voxel algorithm to MR angiographicdata. J Magn Reson Imaging 1991;4:423–30.
[28] Laub GA. Display for MR angiography. Magn Reson Med 1990;14:222–9.
[29] Mistretta CA, Wieben O, Velikina J, Block W, Perry J, Wu Y, et al.Highly constrained backprojection for time-resolved MRI. MagnReson Med 2006;55:30–40.
[30] Huang Y, Wright GA. Time-resolved MR angiography with limitedprojections. Magn Reson Med 2007;58:316–25.
[31] Barger AV, Block WF, Toropov Y, Grist TM, Mistretta CA. Time-resolved contrast-enhanced 3D MR angiography. Magn Reson Med2002;48:297–305.
[32] Haider CR, Hu HH, Campeau NG, Huston J, Riederer SJ. 3D Hightemporal and spatial resolution contrast-enhanced MR angiography ofthe whole brain. Magn Reson Med 2008;60:749–60.
[33] Du J. Contrast-enhanced MR angiography using time resolvedinterleaved projection sampling with three-dimensional Cartesianphase and slice encoding (TRIPPS). Magn Reson Med 2009;61:918–24.