Embed Size (px)
Citation preview
Journal of Surgical Oncology 2006;94:248–251
Autologous Diaphragm Reconstruction With thePedicled Latissimus Dorsi Flap
M.O. MCCONKEY, BSc,1 C.L.F. TEMPLE, MD, FRCSC,2* S. MCFADDEN, MD, FRCSC,3 AND W.J. TEMPLE, MD, FACS, FRCSC31School of Medicine, University of British Columbia, Vancouver, British Columbia, Canada
2Division of Plastic Surgery, University of Western Ontario, London, Ontario, Canada3Division of Surgical Oncology, University of Calgary, Calgary, Alberta, Canada
The latissimus dorsi (LD) muscle has been previously described to repairdiaphragmatic defects, but as a ‘‘reverse’’ flap, relying on secondary blood supplyfrom the perforating lumbar vessels rather than primary inflow from the dominantthoracodorsal artery. We report resection of a retroperitoneal synovial sarcoma, withreconstruction of the hemidiaphragm using the LD rotated on its primaryneurovascular bundle. By using the dominant pedicle, the vascularity of the flap isimproved, minimizing the chance of flap tip loss. Maintaining an intact nerve supplyprevents atrophy. As the distal origin of the LD is broad and flat, it is ideally suited fordiaphragm repair. A latissimus-sparing thoracotomy incision is required to enable thismethod of diaphragm reconstruction.J. Surg. Oncol. 2006;94:248–251. � 2006 Wiley-Liss, Inc.
KEY WORDS: latissimus dorsi; diaphragm; reconstructive surgery; flap
INTRODUCTION
A large defect in the diaphragm is a difficult surgicalchallenge. The etiology of these defects are mostcommonly congenital, traumatic or the result of tumorresection. Reconstructive options are limited as potentialflaps may be compromised by prior surgery, radiation,trauma, or tumor invasion. To date, repair of diaphragmdefects not amenable to primary closure has beenaccomplished with either synthetic patches or a varietyof vascularized flaps.
Synthetic patches are frequently used in the repair ofcongenital diaphragmatic hernias [1,2] in neonates toosick to undergo extensive flap dissection. Althoughalloplastic materials avoid donor site morbidity, syntheticpatches cannot expand as the child grows, necessitatingreplacement with a larger patch or a flap in the future [3].Using patches in adults carries a risk of failure in thesetting of infection or radiation.
A variety of muscle flaps are available to closediaphragmatic defects. Abdominal wall flaps have beenused, including the rectus abdominis myocutaneous flap[4], the transversus abdominis/internal oblique muscleflap [5] and the external oblique muscle flap [6]. Chestwall flaps including the ‘reverse’ latissimus dorsi (LD)flaps [7–11] and the combination LD/serratus anteriorflaps [12] have been applied, as have omental flaps [13].
The LD flap is a work-horse flap as a pedicled or freeflap to cover large regional or distant defects, respec-tively. Transferred free, the LD is used for large complexdefects essentially anywhere on the body that suitablerecipient vessels can be found. On its subscapular axis,the LD muscle has a broad, large, flat muscle belly withan arc of rotation that reaches from the ear to the elbowand from the sternum to the spine. This case report alsoshows the ability for the LD to reach intraabdominally tothe contralateral diaphragmatic crus.
CASE REPORT
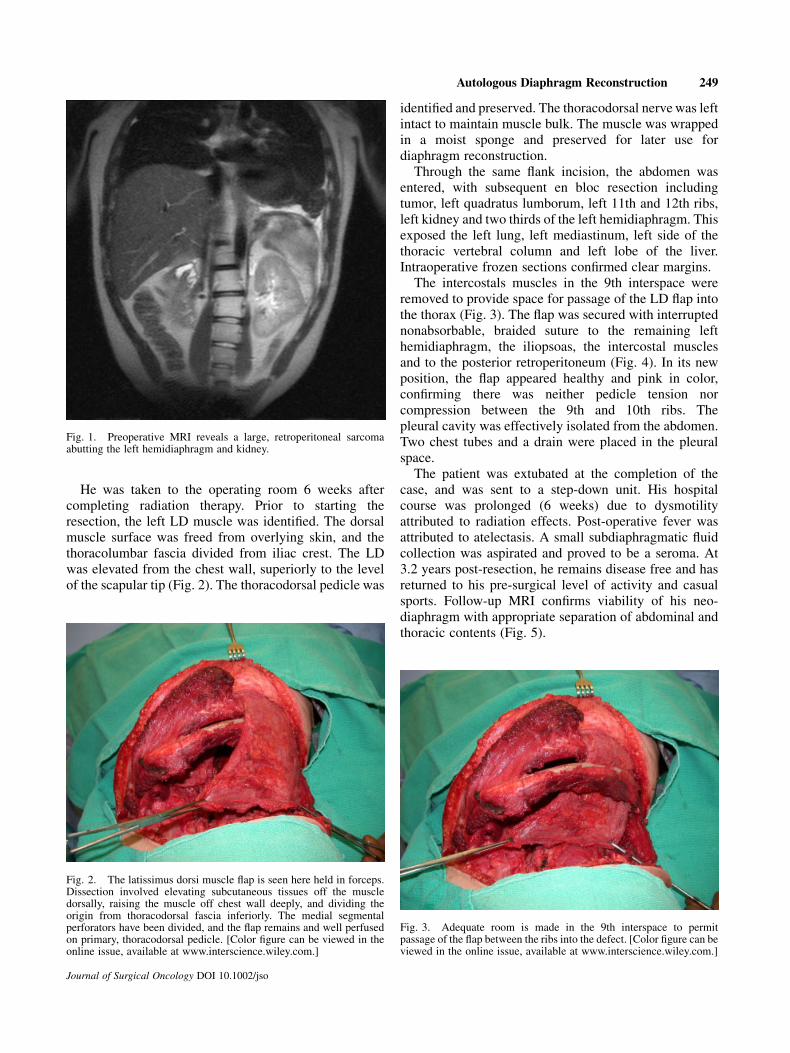
An 18-year-old male with a biopsy-proven grade threesynovial sarcoma of the left retroperitoneum (Fig. 1) wasplanned for multimodality therapy, including neoadju-vant radiotherapy (50 Gy in 25 fractions) followed byresection and reconstruction. To diminish bowel toxicityduring radiotherapy, a tissue expander was inserted atlaparotomy to displace the bowel from the radiation field.Two weeks after laparotomy, radiotherapy commenced.
*Correspondence to: Dr. C.L.F. Temple, Assistant Professor, Hand andUpper Limb Clinic, Division of Plastic Surgery, University of WesternOntario, Ont., Canada. Fax: 519-646-6049. E-mail: [email protected]
Received 15 September 2004; Accepted 27 July 2005
DOI 10.1002/jso.20317
Published online in Wiley InterScience (www.interscience.wiley.com).
� 2006 Wiley-Liss, Inc.
He was taken to the operating room 6 weeks aftercompleting radiation therapy. Prior to starting theresection, the left LD muscle was identified. The dorsalmuscle surface was freed from overlying skin, and thethoracolumbar fascia divided from iliac crest. The LDwas elevated from the chest wall, superiorly to the levelof the scapular tip (Fig. 2). The thoracodorsal pedicle was
identified and preserved. The thoracodorsal nerve was leftintact to maintain muscle bulk. The muscle was wrappedin a moist sponge and preserved for later use fordiaphragm reconstruction.
Through the same flank incision, the abdomen wasentered, with subsequent en bloc resection includingtumor, left quadratus lumborum, left 11th and 12th ribs,left kidney and two thirds of the left hemidiaphragm. Thisexposed the left lung, left mediastinum, left side of thethoracic vertebral column and left lobe of the liver.Intraoperative frozen sections confirmed clear margins.
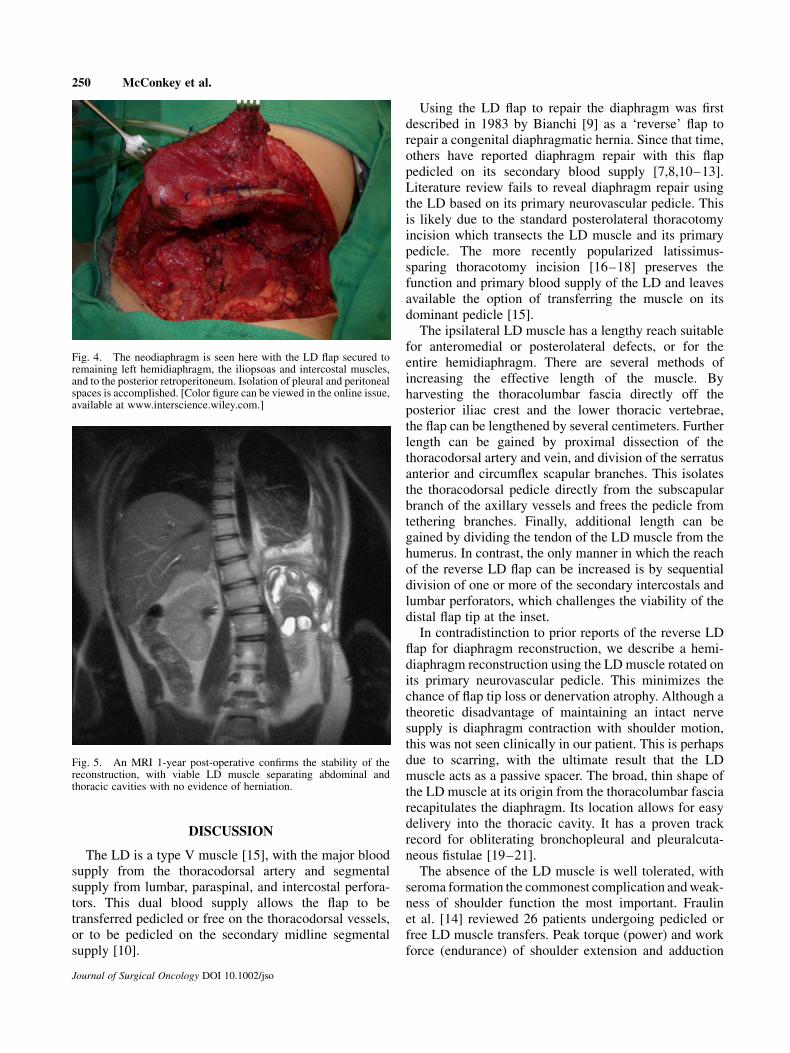
The intercostals muscles in the 9th interspace wereremoved to provide space for passage of the LD flap intothe thorax (Fig. 3). The flap was secured with interruptednonabsorbable, braided suture to the remaining lefthemidiaphragm, the iliopsoas, the intercostal musclesand to the posterior retroperitoneum (Fig. 4). In its newposition, the flap appeared healthy and pink in color,confirming there was neither pedicle tension norcompression between the 9th and 10th ribs. Thepleural cavity was effectively isolated from the abdomen.Two chest tubes and a drain were placed in the pleuralspace.
The patient was extubated at the completion of thecase, and was sent to a step-down unit. His hospitalcourse was prolonged (6 weeks) due to dysmotilityattributed to radiation effects. Post-operative fever wasattributed to atelectasis. A small subdiaphragmatic fluidcollection was aspirated and proved to be a seroma. At3.2 years post-resection, he remains disease free and hasreturned to his pre-surgical level of activity and casualsports. Follow-up MRI confirms viability of his neo-diaphragm with appropriate separation of abdominal andthoracic contents (Fig. 5).
Journal of Surgical Oncology DOI 10.1002/jso
Fig. 1. Preoperative MRI reveals a large, retroperitoneal sarcomaabutting the left hemidiaphragm and kidney.
Fig. 2. The latissimus dorsi muscle flap is seen here held in forceps.Dissection involved elevating subcutaneous tissues off the muscledorsally, raising the muscle off chest wall deeply, and dividing theorigin from thoracodorsal fascia inferiorly. The medial segmentalperforators have been divided, and the flap remains and well perfusedon primary, thoracodorsal pedicle. [Color figure can be viewed in theonline issue, available at www.interscience.wiley.com.]
Fig. 3. Adequate room is made in the 9th interspace to permitpassage of the flap between the ribs into the defect. [Color figure can beviewed in the online issue, available at www.interscience.wiley.com.]
Autologous Diaphragm Reconstruction 249
DISCUSSION
The LD is a type V muscle [15], with the major bloodsupply from the thoracodorsal artery and segmentalsupply from lumbar, paraspinal, and intercostal perfora-tors. This dual blood supply allows the flap to betransferred pedicled or free on the thoracodorsal vessels,or to be pedicled on the secondary midline segmentalsupply [10].
Using the LD flap to repair the diaphragm was firstdescribed in 1983 by Bianchi [9] as a ‘reverse’ flap torepair a congenital diaphragmatic hernia. Since that time,others have reported diaphragm repair with this flappedicled on its secondary blood supply [7,8,10–13].Literature review fails to reveal diaphragm repair usingthe LD based on its primary neurovascular pedicle. Thisis likely due to the standard posterolateral thoracotomyincision which transects the LD muscle and its primarypedicle. The more recently popularized latissimus-sparing thoracotomy incision [16–18] preserves thefunction and primary blood supply of the LD and leavesavailable the option of transferring the muscle on itsdominant pedicle [15].
The ipsilateral LD muscle has a lengthy reach suitablefor anteromedial or posterolateral defects, or for theentire hemidiaphragm. There are several methods ofincreasing the effective length of the muscle. Byharvesting the thoracolumbar fascia directly off theposterior iliac crest and the lower thoracic vertebrae,the flap can be lengthened by several centimeters. Furtherlength can be gained by proximal dissection of thethoracodorsal artery and vein, and division of the serratusanterior and circumflex scapular branches. This isolatesthe thoracodorsal pedicle directly from the subscapularbranch of the axillary vessels and frees the pedicle fromtethering branches. Finally, additional length can begained by dividing the tendon of the LD muscle from thehumerus. In contrast, the only manner in which the reachof the reverse LD flap can be increased is by sequentialdivision of one or more of the secondary intercostals andlumbar perforators, which challenges the viability of thedistal flap tip at the inset.
In contradistinction to prior reports of the reverse LDflap for diaphragm reconstruction, we describe a hemi-diaphragm reconstruction using the LD muscle rotated onits primary neurovascular pedicle. This minimizes thechance of flap tip loss or denervation atrophy. Although atheoretic disadvantage of maintaining an intact nervesupply is diaphragm contraction with shoulder motion,this was not seen clinically in our patient. This is perhapsdue to scarring, with the ultimate result that the LDmuscle acts as a passive spacer. The broad, thin shape ofthe LD muscle at its origin from the thoracolumbar fasciarecapitulates the diaphragm. Its location allows for easydelivery into the thoracic cavity. It has a proven trackrecord for obliterating bronchopleural and pleuralcuta-neous fistulae [19–21].
The absence of the LD muscle is well tolerated, withseroma formation the commonest complication and weak-ness of shoulder function the most important. Fraulinet al. [14] reviewed 26 patients undergoing pedicled orfree LD muscle transfers. Peak torque (power) and workforce (endurance) of shoulder extension and adduction
Journal of Surgical Oncology DOI 10.1002/jso
Fig. 5. An MRI 1-year post-operative confirms the stability of thereconstruction, with viable LD muscle separating abdominal andthoracic cavities with no evidence of herniation.
Fig. 4. The neodiaphragm is seen here with the LD flap secured toremaining left hemidiaphragm, the iliopsoas and intercostal muscles,and to the posterior retroperitoneum. Isolation of pleural and peritonealspaces is accomplished. [Color figure can be viewed in the online issue,available at www.interscience.wiley.com.]
250 McConkey et al.

declined significantly postoperatively. Despite measur-able shoulder weakness after LD harvest, subjectivemorbidity in terms of impairment of activities of dailyliving was minimal [22].
CONCLUSION
The LD flap, perfused on its primary pedicle, is anideal autologous tissue option for hemidiaphragmreconstruction. Its use in this case facilitated successfulseparation of the pleural and peritoneal spaces, andpromoted primary healing in an unfavorable, previouslyradiated bed. Its use requires foresight in incision-planning to avoid transection of the LD and itsneurovascular supply. Options for preservation of theLD include muscle-sparing thoracotomy, or in this case,elevation of the flap prior to embarking on a radicalretroperitoneal/diaphragmatic resection.
REFERENCES
1. Clark RH, Hardin WD, Jr., Hirschl RB, et al.: Current surgicalmanagement of congenital diaphragmatic hernia: A report fromthe Congenital Diaphragmatic Hernia Study Group. J Pediatr Surg1998;33:1004–1009.
2. Lacey SR, Goldthorn JF, Kosloske AM: Repair of agenesis ofhemidiaphragm by prosthetic material. Surg Gynecol Obstet1983;156:310–312.
3. Lee SL, Poulos ND, Greenholz SK: Staged reconstruction of largecongenital diaphragmatic defects with synthetic patch followed byreverse latissimus dorsi muscle. J Pediatr Surg 2002;37:367–370.
4. Hallock GG, Lutz DA: Turnover TRAM flap as a diaphragmaticpatch. Ann Plast Surg 2004;52:93–96.
5. Simpson JS, Gossage JD: Use of abdominal wall muscle flap inrepair of large congenital diaphragmatic hernia. J Pediatr Surg1971;6:42–44.
6. Shimamura Y, Gunven P, Ishii M, et al.: Repair of the diaphragmwith an external oblique muscle flap. Surg Gynecol Obstetr1989;169:159–160.
7. Bedini AV, Andreani SM, Muscolino G: Latissimus dorsi reverseflap to substitute the diaphragm after extrapleural pneumonect-omy. Ann Thorac Surg 2000;69:986–988.
8. Bedini AV, Valente M, Andreani S, et al.: Reverse flap of distallatissimus dorsi for diaphragm reconstruction in the adult:Specification of the technical procedure and report on six cases.J Thorac Cardiovasc Surg 1997;114:846–848.
9. Bianchi A, Doig CM, Cohen SJ: The reverse latissimus dorsi flapfor congenital diaphragmatic hernia repair. J Pediatr Surg 1983;18:560–563.
10. Bostwick J, Scheflan M, Nahai F, et al.: The ‘reverse’ latissimusdorsi muscle and musculocutaneous flaps: Anatomical andclinical considerations. Plast Reconstr Surg 1980;65:395–399.
11. Wallace CA, Roden JS: Reverse, innervated latissimus dorsi flapreconstruction of congenital diaphragmatic absence. PlastReconstr Surg 1995;96:761–769.
12. Samarakkody U, Klaassen M, Nye B: Reconstruction ofcongenital agenesis of hemidiaphragm by combined reverselatissimus dorsi and serratus anterior muscle flaps. J Pediatr Surg2001;36:1637–1640.
13. Edington HD, Evans S, Sindelar WF: Reconstruction of afunctional hemidiaphragm with use of omentum and latissimusdorsi flaps. Surgery 1989;105:442–445.
14. Fraulin FO, Louie G, Zorrilla L, et al.: Functional evaluation ofshoulder function following latissimus dorsi muscle transfer. AnnPlast Surg 1995;35:349–355.
15. Mathes SJ, Nahai F: Classification of the vascular anatomy ofmuscles: Experimental and clinical correlation. Plast ReconstrSurg 1981;67:177–187.
16. Akcali Y, Demir H, Tezcan B: The effect of standard poster-olateral versus muscle-sparing thoracotomy on multiple para-meters. Ann Thorac Surg 2003;76:1050–1054.
17. Karwande SV, Pruitt JC: A muscle-saving posterolateral thor-acotomy incision. Chest 1989;96:1426–1427.
18. Pearson FG, Deslauriers J, Ginsberg RJ, et al.: Thoracic Surgery.New York: Churchill Livingstone; 1995.
19. Hanaoka T, Nakajima Y, Shiraishi Y, et al.: Transposition ofmodified latissimus dorsi musculocutaneous flap in the treatmentof persistent bronchopleural fistula after posterolateral incision.Jpn J Thorac Cardiovasc Surg 2004;52:84–87.
20. Meyer AJ, Krueger T, Lepori D, et al.: Closure of largerintrathoracic airway defects using intrathoracic muscle flaps. Annof Thorac Surg 2004;77:397–404.
21. Molnar JA, Remington DG: Management of postpneumonectomybronchopleural-cutaneous fistula with a single free flap. Ann PlastSurg 2002;48:88–91.
22. Salmi A, Tuominen R, Tukiainen E, et al.: Morbidity of donor andrecipient sites after free flap surgery. A prospective study. Scand JPlast Reconstr Surg Hand Surg 1995;29:337–341.
Journal of Surgical Oncology DOI 10.1002/jso
Autologous Diaphragm Reconstruction 251