Embed Size (px)
Citation preview

Kidney Care Partners • 601 13th St NW, 11th Floor • Washington, DC • 20005 • Tel: 202.534.1773
August12,2020TheHonorableSeemaVermaAdministratorCentersforMedicare&MedicaidServices7500SecurityBoulevardBaltimore,MD21244Re:CMS–1732–P:“End-StageRenalDiseaseProspectivePaymentSystem,PaymentforRenalDialysisServicesFurnishedtoIndividualswithAcuteKidneyInjury,andEnd-StageRenalDiseaseQualityIncentiveProgram”DearAdministratorVerma: KidneyCarePartners(KCP)appreciatestheopportunitytoprovidecommentsonthe“End-StageRenalDiseaseProspectivePaymentSystem,PaymentforRenalDialysisServicesFurnishedtoIndividualswithAcuteKidneyInjury,andEnd-StageRenalDiseaseQualityIncentiveProgram”(ProposedRule).ThisletteroutlinesoursupportfortheproposalsrelatedtotheEnd-StageRenalDisease(ESRD)QualityIncentiveProgram(QIP)andhighlightsconcernsaboutthevalidityandreliabilityofsomeofthemeasures,aswellasstructuralproblems,includingtheimpactofthepandemicontheQIP.Ourcommentsontheprospectivepaymentsystemwillbesharedinaseparateletter. KCPisanallianceofmorethan30membersofthekidneycarecommunity,includingpatientadvocates,healthcareprofessionals,providers,andmanufacturersorganizedtoadvancepoliciesthatsupporttheprovisionofhigh-qualitycareforindividualswithchronickidneydisease(CKD),includingthoselivingwithEnd-StageRenalDisease(ESRD). Asdescribedinmoredetailbelow,KCPstronglysupportsthefourproposalsCMSoutlinesintheProposedRulefortheESRDQIP:
• UpdatingthespecificationsusedtocalculatetheUltrafiltrationRateandMedicationReconciliationmeasures;
• ReducingthenumberofrecordsfacilitiesselectedfortheNationalHealthSafetyNetwork(NHSN)validationarerequiredtosubmit;
• ClarifyingthetimelineforfacilitiestomakechangestotheirNHSN
BloodstreamInfection(BSI)clinicalmeasureandNHSNDialysisEventreportingmeasures;and

TheHonorableSeemaVermaAugust12,2020Page2of39
• EstablishingtheperformancestandardsandpaymentreductionsthatwouldapplyforPY2023.
Inaddition,KCPispleasedthatCMShasaffirmedits“plantore-evaluateour
reportingmeasuresforopportunitiestomorecloselyalignthemwithNQFmeasurespecifications.”1Inlightofthiseffort,KCPalsoofferssuggestionswithregardtospecificmeasuresthatwouldallowtheAgencytomeetthisgoal.WealsoencourageCMStoevaluatetheexistingQIPmeasuresconsistentwiththefollowingprinciplesandincludethosemodificationsinthefinalrulethisyear.Aswenotedinour2019commentletterontheESRDQIP,weaskthatCMS:
• UsevalidandreliablemeasuresasestablishedthroughNQFendorsement;• Adoptendorsedmeasureswhentheyareavailableovermeasuresthathavenot
beenendorsed;• NotuseorremovemeasuresthatNQFhasrejectedaspartofitsendorsement
processfromtheESRDQIPorthathavebeenassignedtoreservestatus;• AvoidmodifyingNQF-endorsedmeasureswhenadoptingthemfortheESRD
QIP;• SeekNQFendorsementfornewmeasurespriortoadoptingthemintheESRD
QIPoratleastusethemonlyasreportingmeasureswhileseekingNQF-endorsement;
• Honoritscommitmenttouseratemeasuresinfavorofratiomeasures;• Continuetoworkwithstakeholdersinatransparentprocesstoidentifyand
addressthepotentialcausesthatcouldleadtothepenaltiesincreasingwhenactualperformancehasimproved;
• WorkwiththecommunityandNQFtodevelopabetterapproachtothesmallnumbersproblem;and
• AligntheESRDQIPandESRDDFC/FiveStar.
Inadditiontothecommentsonthespecificmeasures,KCPprovidessuggestionstoaddressthedifferentialhandlingofMedicareAdvantagepatientsinseveralmeasuresintheESRDQIPandhowtoaddressthepandemicinamannerthatensurestheintegrityoftheESRDQIPlong-term.
WecontinuetosupportthetwovascularaccessmeasuresintheESRDQIP.Wealso
supportthedecisionnottoaddanynewmeasurestotheESRDQIPatthistime.Therearenow14ESRDQIPmeasures(notcountingthepooledmeasurefordialysisadequacy),whichdilutestheimpactofanyoneofthesemeasures.Asnotedbelow,weproposereducingthecurrentmeasuresetbyremovingsomeofthemeasures.WelookforwardtoworkingwithCMStomakesurethatthereisaparsimonioussetofmeasuresreflectingthe
1CMS,“MedicareProgram;End-StageRenalDiseaseProspectivePaymentSystem,PaymentforRenalDialysisServicesFurnishedtoIndividualsWithAcuteKidneyInjury,andEnd-StageRenalDiseaseQualityIncentiveProgram”85Fed.Reg.42132(July13,2020).

TheHonorableSeemaVermaAugust12,2020Page3of39
mostcriticaloutcomesforpatientsandaccuratelyreflectingthecareactuallyprovidedbythefacilities.
I. TheuseofvalidandreliablemeasuresthatalignwithNQF-endorsedmeasures
MeasuresusedintheESRDQIPshouldbeendorsedbyNQFtobeconsistentwith
thestatutorymandate,unlessasthestatutenotes,thereisnoendorsedmeasureinaspecificdomain.Section1890oftheSocialSecurityAct(SSA)requiresCMStocontractwithaconsensus-basedentityfordevelopingmeasuresusedinVBPs.Thesecondstatutorydutylistedfortheconsensus-basedentity,whichiscurrentlyNQF,istoendorsemeasuresforCMS’use.WhentheCongressestablishedtheESRDPPS,itwasevenmorespecificinitsmandatetouseNQFendorsedmeasures.TheStatuterequiresthat“anymeasurespecifiedbytheSecretaryundersubparagraph(A)(iv)musthavebeenendorsedbytheentitywithacontractundersection1890(a).”2Thus,KCPispleasedthatthepreamblestatesthatCMSplanstomorecloselyaligntheQIPmeasureswiththeNQFmeasurespecifications.KCPrecommendsthattoachievethisgoalnotonlyforreportingmeasures,butalsoclinicalmeasures,CMStakethefollowingstepsoutlinedbelow.KCPalsostronglyopposesuseofmeasuresintheQIPthatNQFhasrejectedthroughtheendorsementevaluationprocess.Simplyput,CMSshouldusevalidandreliablemeasuresasestablishedthroughNQFendorsement.
A. KCPsupportsaligningtheQIPUltrafiltrationandMedicationReconciliationDenominatorswiththeNQF-EndorsedSpecifications:CMSshouldavoidmodifyingNQF-endorsedmeasureswhenadoptingthemfortheESRDQIP.
KCPispleasedthatCMShasproposedtoupdatethespecificationsusedforthe
UltrafiltrationRate(UFR;NQF2701)reportingmeasurebystatingthatitwillusethepatient-monthsconstructionthatcomportswiththeNQF-endorsedmeasure.WealsoappreciatetheclarificationthatthisreportingmeasureisbasedontheoneforwhichtheKidneyCareQualityAlliance(KCQA)isthesteward.Similarly,wearepleasedthatthepreamblealsoreaffirmsthatitwillnolongerusethe“facility-months”constructionfortheMedicationReconciliation(NQF2988).Usingthea“patient-months”denominatorconstructionalignsbothofthesemeasureswiththespecificationssubmittedbythemeasuredeveloperandsteward(theKCQA),whichwereendorsedbyNQF.KCPappreciatesandconcurswiththechangetothe“patient-months”constructionforbothmeasures.
2SSA§1881(h)(2)(B)(emphasisadded).

TheHonorableSeemaVermaAugust12,2020Page4of39
B. KCPsupportstheefforttoreducetheburdenscreatedbytheNHSNvalidationstudy;KCPalsoreiteratesconcernsthattheNHSNBloodstreamInfectionmeasureisnotvalidandneedstobemodifiedtoprovideaccurateinformationtopatientsandactionableinformationtofacilities.
CMSproposestoreducethesubmissionrequirementforfacilitiesselectedto
participateintheNHSNvalidationstudyfrom40to20patientrecordsfromanytwoquartersduringtheapplicablecalendaryear.KCPconcurswiththisreductionandappreciatesthisrevision,whichwillreducefacilityburden.WealsosupporttheclarificationforboththeNHSNDialysisEventandtheNHSNBloodstreamInfectionmeasuresthat“anychangesthatafacilitymakestoitsdataaftertheESRDQIPdeadlinethatappliestothosedatawillnotbeincludedinthequarterlypermanentdatafilethattheCDCgeneratesforpurposesofcreatingtheannualCMSESRDQIPFinalComplianceFile.”3
WhileKCPcontinuestosupporttheNHSNDialysisEventmeasureasareporting
measure,weencourageCMStosubmitthismeasureforNQFreview,consistentwiththestatutorylanguageindicatingthatCMSshouldusemeasuresendorsedbythebodyselectedtoreviewthem,whichinthiscaseistheNQF.Therefore,wealsoaskthatCMSsubmitthemeasuretoNQFforreviewinthenextcycle.Wereiterateourrecommendationthattherecentadditionofasetofsubjectivefactors(e.g.,redness,swelling)tothemeasurebeeliminatedbecausethesefactorsdonotsupportthepurposeofthemeasure.
Consistentwithourpreviousrecommendations,KCPasksCMStoeliminatethe
NHSNBloodStreamInfection(BSI)measurewhileitdetermineshowtorevisethespecificationssothatthevalidityproblemswiththemeasurecanberesolvedandtheNQFhastheopportunitytoreviewthemeasure.CMShasnotidentifieddataindicatingthattheproblemthatasmanyas60-80percentofdialysiseventsmaybeunder-reportedwiththeNHSNBSImeasurehasbeenresolved.Themeasuredoesnotmeetthecriterionofvalidityforendorsement.Thus,patientswhorelyupontheinformationgeneratedbythismeasureare,inmanyinstances,relyingoninaccuratedatathatsuggestthataparticularfacilityhasalownumberofbloodstreaminfectionswhen,infact,thefacilityhasahighernumber.Theimportanceofunderstandinghowafacilitymanagesbloodstreaminfectionsiscriticalforpatientdecision-making.Ameasurethatfailstoaccuratelyrepresentthefacility’sperformancedeprivespatientsoftheirabilitytomakeinformedhealthcaredecisions.Italsounfairlypenalizesfacilitiesthatdiligentlypursueandreportthehospitalinfectiondatanecessaryforafullpictureofinfectionrates.
Thus,wereiterateourrequestthatCMSremovetheNHSNBSIclinicalmeasure
immediatelyandusetheDialysisEventReportingMeasurealone.KCPstronglysupports
3Id.

TheHonorableSeemaVermaAugust12,2020Page5of39
transparencyandeffortstoreducebloodstreaminfections.Therefore,weaskCMStoworkwiththecommunitytoidentifyspecificmodificationstotheNHSNBSImeasuretoaddressthevalidityconcernsandsubmitthatrevisedmeasuretotheNQFforreview.
C. KCPcontinuestosupporttheconversionoftheStandardizedTransfusionRatio(STrR)measurestoareportingmeasure,becauseofconcernsaboutvalidityarisingfromtheshifttoICD-10coding,buturgesCMStoreplaceitwithamoreappropriateanemiamanagementmeasureandseekendorsementofthenewmeasure.
KCPcontinuestosupportthestatutoryrequirementthatCMSadoptendorsed
measureswhentheyareavailable,butrecognizesthattheremaybetimeswhenchangingcircumstancesresultinanendorsedmeasurenolongerbeingappropriate.Aswenotedduringlastyear’srulemaking,wesupportCMSaddressingtheseproblemsastheyarise.
Forexample,KCPcontinuestosupportthedecisionCMSmadetoconvertthe
StandardizedTransfusionRatio(STrR/NQF2979)toareportingmeasure.BecauseitbecameclearaftertheICD-9toICD-10transitionthatthecodesusedintheSTrRmeasurewerenotaccuratelycapturingbloodtransfusionstoensurevalidityofthemeasure,CMSconvertedthemeasuretoareportingmetricintheCY2019FinalRuletoallowforanexaminationoftheproblem.Goingforward,however,KCPrecommendsshiftingawayfromtheSTrRmeasureandadoptingameasurethatmoredirectlyreflectspatientqualityofcare,ismoreclearlyactionable,andreducesburden.WeagainrecommendthatCMSreplacetheSTrRwithalowhemoglobin(Hgb)measure(e.g.,aHgb<10g/dL).
Whileitwillbenecessarytodevelopupdatedspecifications,exclusions,testing,and
businessrules,KCPwouldwelcometheopportunitytoworkwithCMSonsuchameasure;wenotethatCMSdevelopedasimilarmeasureseveralyearsagothatwouldbeanappropriatestartingpoint.WeareawaresuchameasurewasnotendorsedbyNQF,butbelieveNQF’supdatedevidencealgorithmprovidesapathforitsconsiderationanew.AlowHgbmeasurewouldreduceburden,becauseanytransfusionmeasurerequiresdialysisfacilitiestochasepaperworkcreatedbyotherproviders.ItalsoisabettermeasurethantheSTrRbecausefacilitiesandphysicianshaveaccesstopatientHgbdatainthefacility,whereastheydonothaveaccesstotransfusiondata.Moreover,itisactionablebyphysiciansandwillhaveadirectapositiveimpactonanissueofcriticalimporttopatients.Additionally,aswenoteinthefollowingsection,KCPhassignificantconcernsaboutthereliabilityoftheSTrR.
TheHonorableSeemaVermaAugust12,2020Page6of39
D. WhenNQFhasrejectedameasureormovedameasuretoreservestatus,CMSshouldnotincludeitintheQIPtobeconsistentwiththestatute;thus,KCPasksCMStoremovethePrevalentPatientsWaitlistedmeasureandretiretheHypercalcemiameasurefromtheQIPandreplacetheDialysisAdequacyComprehensiveMeasurewiththeindividualKt/VmeasuresthatNQFhasendorsed.
KCPstronglysupportsthePresident’sinitiativetoincreasethenumberofsuccessful
kidneytransplants.Toachievethegoal,itisimportantthatpatientsareempoweredbyhavingaccurateinformationtoassesswhethertheirprovidersaredoingwhattheycanandshouldbetohelpthemqualifyforatransplant.HavingavalidandreliablemeasureintheESRDQIPthatsupportstransplantsisaworthygoal.
Unfortunately,thePercentageofPrevalentPatientsWaitlisted(PPPW)measure
hasbeendeterminedtolackvaliditybytheNQF.Thus,itshouldnotbeincludedintheQIP,becauseitwillmisleadpatients.WhileCMShasflexibilitytoadoptameasurewhenNQFhasnotendorsedameasureinaparticulardomain,itisacontortedreadingtosuggestthatthisflexibilitymeanstheAgencycanorshoulduseameasurethathasfailedtomeetthescientific,consensus-basedendorsementcriteria.
Ratherthancontinuewiththismeasure,weencourageCMStoworkwithKCPand
othersinthecommunitytoaddresstheproblemsunderlyingthismeasuresothatthereisavalidandreliablemeasurethatwillprovideaccurateinformationrelatedtotransplantationandempowerpatientsintheirdecision-making.
Similarly,theNQFhasconcludedafterextensivereviewthatthe(Kt/V)Dialysis
AdequacyComprehensiveMeasuredoesnotmeettheendorsementcriteria,becauseitfailedonmeasuringaperformancegap,whichisathresholdrequirementforfurtherdiscussiononfactorssuchasvalidityandreliability.KCPisalsoconcernedthatapooledmeasurefailstoprovidethetransparencynecessarytopromotepatientdecision-makingwhenitcomestohomedialysis.ByreportingallKt/Vscores,ithidesfromviewhoweachfacilityperformswhenitcomestoprovidinghomedialysis.GiventheAdministration’semphasisonhomedialysis,weurgeCMStoremovetheDialysisAdequacyComprehensiveMeasurefromtheQIPandreplaceitwiththefollowingmeasuresthathavemeettheendorsementcriteria:
• NQF#0249DeliveredDoseofHDAboveMinimum;• NQF#0318DeliveredDoseofPDAboveMinimum;• NQF#1423MinimumspKt/VforPediatricHDPatients• NQF#2704,MinimumDeliveredPDDose;• NQF#2706,PediatricPDAdequacy—AchievementofTargetKt/V
Thisstepwouldalignwiththestatutorymandateandprovidepatientswiththeabilitytounderstandeachfacility’sactualperformanceonthedifferentdialysismodalities.

TheHonorableSeemaVermaAugust12,2020Page7of39
KCPalsorecommendsthatCMSworkwithKCPtore-specifyandtestnewindividualPDmeasuressothatfacilitiesthatprovidehomedialysisarenotdisadvantagedbecauseofthedifferencesinthefrequencyoftestinghomedialysispatients.
Finally,CMSshouldretiretheHypercalcemiaMeasurefromuseintheESRDQIP,
becauseitisbasedonNQF#1454,whichtheNQFhasplacedinreservestatusbecauseithas“topped-out”(i.e.,thereislittleroomforadditionalimprovementinthisclinicalarea)andprovidesnosignificantbenefitforpatients.Therefore,CMSshouldretirethemeasure.
Inaddition,KCPreiteratesthatitwouldbeappropriate,forpurposesofhavinga
bonemineralmetabolismmeasure,tousetheNQFserumphosphorusmeasureasareportingmeasureintheQIP.Eventhoughthemeasureisinreservestatus,physiciansrelyupontheserumphosphorusmeasuretomakeclinicaldecisions.Whileworkstillneedstobedonetoidentifytheoptimalphosphorustarget,howtoaddressthetargetforcertainsubpopulations,andwhenphosphorusshouldbeassessed,areportingmeasureemphasizestheneedtomonitorphosphoruslevelswhileallowingtimetoaddresstheseunresolvedissues.
E. KCPencouragesCMStoaddressthereliabilityproblemswiththe
standardizedratiomeasuresandtouserisk-standardizedratemeasuresinstead.
KCPmembersbelievethathospitalizationandreadmissionratesareessential
metricsthatshouldbethecoreofanyvalue-basedpurchasingprogram.However,forsuchmetricstobeeffectivetheymustbereliable–meaningaccurateandreplicableinhowtheymeasurefacilityperformance–andtransparent.Unfortunately,theStandardizedHospitalizationRatio,(SHR/NQF1463)andStandardizedReadmissionRatio(SRR/NQF2496)measures,aswellastheSTrR,donotmeettheserequirements,asCMS’sowndatademonstrate.
CMS’decisiontoprovideonlyaveragereliabilitystatisticsacrossallfacilitysizeslackstransparency.Toimprove,afacilityshouldbeabletoassessthedegreetowhichitsownSHRorSRRscoresrepresentnoiseoractualqualityresults.WhilereliabilitydatastratifiedbysizemaynolongerberequiredbyNQFforendorsement,itiscriticaldataforfacilitiestounderstandtheirperformanceandimproveuponit.KCPstronglyrecommendsthatCMSprovidethesedatainitsNQFsubmissionsormakethempubliclyavailableelsewhere.
InthemostrecentiterationoftheSRR,currentlyunderreviewatNQF,theoverallIURwas0.35—adramaticdeclinefromthe2009NQFsubmissionvalueof0.55.Statistical
TheHonorableSeemaVermaAugust12,2020Page8of39
literaturetraditionallyinterpretsareliabilitystatistic<0.5as“unacceptable”.4Ameasurewherein65percentofafacility’sscoreisduetorandomnoiseandnotaqualitysignalisinappropriateforuseintheQIP.Moreover,theSRR’sreliabilityof0.35istheaverageacrossallfacilities.Thereliabilityforsmallerfacilitieswillbesignificantlyless,asacknowledgedbyCMS’contractdeveloper.
Likewise,theoverallIURfortheone-yearSHRwas0.53-0.59for2015-2018;a“poor”reliabilitystatisticthatalsorepresentsadeclinefromthe2010-2013IURs(0.7).BasedoncurrentCMSdata,41-47percentofafacility’sSHRscoreisduetorandomnoise,andsmallerfacilitiesagainwillhaveasignificantlygreatercontributionofnoisetotheirscore.
Again,KCPalsonotesthatCMSnowdeclinestoprovidetestingdatastratifiedby
facilitysizeforanymeasuresitsubmitstoNQFbecauseitis“notrequired”byNQF.AsthemostrecentCMSreliabilitydatastratifiedbysizereveal,theIURforsmallfacilities(definedbyCMSatthetimeas<50fortheSHRand<70fortheSRR)forbothmeasureswas0.46in2009(SRR)and2013(SHR)—i.e.,forapproximatelyonethirdofallfacilities(thosemeetingCMS’owndefinitionof“small”),54percentofthescoretheyreceivedontheSRRandSHRcouldbeattributedtorandomnoiseandnotsignal.
AnyscoreassignedtoafacilityfortheSRRhasnoqualitymeaningbasedonCMS
testingresults,andtheSRRshouldberemovedfromtheQIP.TheSHRshouldbedeployedonlyforlargefacilities,asdefinedbyCMS’historicalstratificationresultsinitssubmissionstoNQF.Finally,althoughtheclinicalversionoftheSTrRisnotyetproposed,KCPfeelsitisimportantalsotoemphasizeitspoorreliability,especiallyforsmallfacilities.Inthemostrecentiterationofthemeasure,theoverallIURfortheone-yearSTrRwas0.63-0.68acrosstheyears2014-2017.Datafrom2011-2014,forwhichtherewasasimilaroverallIUR,revealedvaluesaslowas0.30forsmallfacilities—thatis,forapproximatelyonethirdoffacilities,70%ofthescoretheyreceivedontheSTrRcouldbeattributabletorandomnoiseandnotsignal.Whilenewdetailswerenotprovided,CMS’contractmeasuredeveloperacknowledgedthattheSTrRwaslessreliableinsmallerfacilitiesforthe2014-2017dataperiod.
Lastly,althoughnotmentionedperseintheProposedRule,wenotethatCMSnowreliesonanovel,additionalmetricofreliability,referredtoastheprofile-IUR(PIUR).5PerCMS,“ThePIURindicatesthepresenceofoutliersorheaviertailsamongtheproviders,whichisnotcapturedintheIURitself....[When]thereareoutlierproviders,evenmeasureswithalowIURcanhavearelativelyhighPIURandcanbeveryusefulfor
4AdamsJL.TheReliabilityofProviderProfiling:ATutorial.SantaMonica,CA:RANDCorporation.TR-653-NCQA,2009.5HeK,DahlerusC,XiaL,LiY,KalbfleischJD.Theprofileinter-unitreliability.Biometrics.2019Oct23.doi:10.1111/biom.13167.[Epubaheadofprint].

TheHonorableSeemaVermaAugust12,2020Page9of39
identifyingextremeproviders.”6ThePIURwas0.61fortheSRRand0.75-0.85fortheSHR,whichCMSinterpretsasdemonstratingthemeasuresare“effectiveatdetectingoutlierfacilitiesandstatisticallymeaningfuldifferencesinperformancescoresacrossdialysisfacilities.”7KCPstronglyconcurswiththeNQF’sScientificMethodsPanel(SMP)conclusionthatthePIURisnotanappropriatemeasureofreliabilityforanyQIPmeasure.QIPmeasuresareusedtodistinguishperformancealongacontinuum,inparticularamongprovidersfallinginthemiddleofthecurve,todeterminepenalties;theabilitytoreliablydistinguishoutliersforimplementationofthesemeasuresisnotthepoint.TheIURisandremainstheappropriatemeasureofreliabilityformeasuresproposedfortheQIP.
F. ModifyingICH-CAHPSmeasuretoaddressvalidityproblemsand
makeitmeaningfultopatientsandproviders.
KCPcontinuestosupportpatientsatisfactionmeasures,suchastheICH-CAHPSmeasure.However,thelowresponseratesthreatenthevalidityofICH-CAHPSasanaccountabilitymeasure.Inaddition,thecurrentmeasuredoesnotallowforfeedbackfromhomedialysispatients.WeappreciatetheTechnicalExpertPanelthatCMSconvenedearlierthisyearandsupporttheclosereviewofthemeasure.However,therearesomeimmediatemodificationsCMScouldadoptthatwouldreducetheburdenonpatientsaskedtorespondandaddresssomeoftheresponserateproblems.Specifically,CMScould:
• AdministerICH-CAHPStopatientsonceayear(nottwice)toreduceburdenon
patients;and
• Askindividualpatientstocompleteonlyoneofthethreeindependentlyvalidatedsectionsonthesurvey;thus,whilefacilitiesaresubjecttotheentiresurveyinstrument,noonepatientwillbeaskedtocompletethemorethan60questionsinasingleresponse.
Inaddition,wereiterateouroutstandingrequestthatthesurveyberevisedto
includehomedialysispatientsandthatCMSobtainNQFendorsementofthenewmeasure,whichMedPACandothersinthecommunityalsohaveconsistentlyrequested.ItisalsoimportantthatCMSallowfacilitiesandpatientstousetheICH-CAHPSsurveyresultstoimprovecare.
II. DifferentialHandlingofMedicareAdvantagePatientsinQIPmeasures
threatensthevalidityofseveralQIPmeasures.
TheincreasingnumbersofMApatientsintheESRDprogram—andtheunavailabilityofoutpatientclaimsdataforthesepatients—threatenthevalidityofseveral
6KalbfleischJD,HeK,XiaL,LiY.Doestheinter-unitreliability(IUR)measurereliability?HealthServicesandOutcomesResearchMethodology.2018;18(3):215-225.Doi:10.1007/s10742-018-0185-4.
7Citation:SHRmeasuressubmissionmaterialstoNQF.

TheHonorableSeemaVermaAugust12,2020Page10of39
QIPmeasures.DataprovidedbyCMSindicatethatattheendof2017,27percentofdialysispatientshadMAcoverage(presumablyhighernow),andthisvariedwidelyacrossstates—fromabout2percentinWyomingto34percentinRhodeIsland,andmorethan44percentinPuertoRico.SuchgeographicvariationcompromisesthevalidityofthemeasuresifMApatientsarenotaccuratelyaccountedforintheQIPmetrics.Specifically,withoutchangestothecurrentspecifications,theevolvingpatientmixwillintroducesignificantbiasintomeasurecalculationsthatcouldaffectresultsforfacilitieswitheitherveryloworhighMApatientpopulations.Recognizingthis,KCPconcurswiththeneedtochangespecificationsforseveralCMSmeasurestoaccommodatetheincreaseinMApatientsandtoavoiddisparitiesinperformanceduetogeography.KCPstronglybelieves,however,thatgreatertransparencyisrequiredbyCMSasitupdatestherelevantmeasures.
WhiletheapproachtohandlingMApatientsvariesconsiderablyacrossCMS’metrics(Table1,AttachmentB),KCPrecognizesthedifficultyCMSfacesinaddressingthisissueacrossmeasuresofvaryingconstructionandnotesthereappearstobealogicalrationaleformostofthedecisionsmadebecauseofthepropertiesandintendedpurposeofeachmeasure.Nevertheless,KCPstronglyrecommendsthatCMSperformasensitivityanalysisofperformancewithandwithoutMApatientsforeachoftheapplicableQIPmeasuresandmaketheresultspubliclyavailable.SuchdatawillprovideanopportunityforKCPandotherstoofferpotential,evidence-basedmitigationstrategies(e.g.,amodelthataccountsforbothpopulations,useofriskcoefficientsasnecessary).
WealsoaskCMStoperformandprovideananalysisofriskmodelfitunderthepreviousapproachandthenewin-patient-claims-onlyapproach;currentlyweareunabletoassesswhethermodelfitimprovedorworsenedwiththisapproach.KCPisparticularlyconcernedthatlimitingcomorbiditydatatoinpatientclaimsmightskewthemodelstowardsasickerpopulation,andthatsuchaskewmightreflectunfavorablyonfacilitiesthatsuccessfullykeephospitalizationrateslow.Thatis,becausecomorbidityadjustorsdevelopedexclusivelyfromhospitalizationdatawillnecessarilyunderestimatethecomorbidityprofileofpatientsinfacilitieswithlowhospitalizationrates,the“expected”hospitalizationormortalityratescalculatedforsuchfacilitieswillbeerroneouslylow,andthefacilities’scoreswillbeerroneouslyhigh.OnlywithtransparencyinthesematterscanthecommunityassesstheimpactMApatientmixhasontheQIPmeasures.
Finally,KCPnotesthattheSHRandSFR(andStandardizedMortalityRatio(SMR),whichisnotpartoftheQIP)obtainpast-yearcomorbiditydatafrommultiplePartAsources(inpatient,SNFs,homehealth,hospice).Conversely,thepast-yearcomorbiditysourcefortheSRRislimitedtoinpatientclaims.WeaskthatCMSincorporatedatafromthemultiplePartAsourcesusedintheSMR,SHR,andSFRmodels—inpatient,aswellasSNF,homehealth,andhospicedata—tomaketheSRRadjustmentpotentiallymorerobust.Asamatterofmeasureconstruction,italsoisalogicalharmonizationissue.WerecommendCMSperformthisanalysisandmakeitpubliclyavailableorreleaseexistingdataandjustifythecurrentapproach.

TheHonorableSeemaVermaAugust12,2020Page11of39
III. KCPasksCMStoaddresstheimpactofCOVID-19measureperformance.
TheCOVID-19pandemichaspresentedunprecedentedchallengestopatientswithESRDandthedialysiscommunityandhassignificantlyaffectedpatientcare—andhasthepotentialtoimpacttheQIP.ThepandemicwillimpactperformancebeyondtheobviousoutcomemeasuressuchastheSHRandSRRinareaswithaheavyCOVIDburden,butalso“upstream”processandintermediate-outcomemetrics,eveninrelativelyunaffectedlocales.Forinstance,toavoidorminimizepotentialexposuretothevirus,patientsandprovidershavepostponedelectivefistulaplacementanddelayedroutinelabdraws,andadequacytargetshavenotbeenmetinsomecasesasanxietysometimesmeansanearlyendtoadialysissession.
A. KCPasksCMStoextendthenationwideExtraordinary
CircumstancesExceptionfortheESRDQIPthroughtheendofthepublichealthemergency,plusashortgraceperiod.
KCPappreciatesCMS’proactivegrantingofauniversalExtraordinaryCircumstance
Exception(ECE)fortheESRDQIPinresponsetoCOVID-19.WelikewisethankCMSforallowingfacilitiestheflexibilitytooptoutoftheECE,attheirdiscretion.Wenote,however,thattherecentlywitnessedprogressiveandunpredictableregionalspreadofthevirusnowrendersthecurrentJune20deadlineforthisdecisionobsolete.PreviouslyunaffectedfacilitiesthatchosetooptoutoftheECEpriortoJune20maynowbeinthecenterofanew“hotspot”,nolongerabletomeettherequireddatasubmissionthatpreviouslyseemedfeasible.KCPthusrequeststhatCMSrevisittheJune20deadline,allowingfacilitiesthatpreviouslyoptedoutoftheECEtonowopt-in,withoutpenalty.
WebelievethatCMShastheauthoritytoextendtheflexibilityprovidedinthe
universalECE.CMScreatedtheECEpolicythroughregulation.42C.F.R.§413.178(d)(3)indicatesthatthetimeframeforanECEmaybe“foroneormorecalendardays,whentherearecertainextraordinarycircumstancesbeyondthecontrolofthefacility.”Theregulationsalsoindicatedthat“CMSmaygrantexceptionstofacilitieswithoutarequestifitdeterminesthatoneormoreofthefollowinghasoccurred:(i)Anextraordinarycircumstanceaffectsanentireregionorlocale.”8Thereisnoothertimerestriction.
ThestatutegoverningtheESRDQIPdoesnotprohibitCMSfromextending
exceptionstothereportingrequirements.WhilethestatuterequiresCMStoreducepaymentstoadialysisfacilitythatdoesnotmeetorexceedthetotalperformancescorewithrespecttotheperformancestandards,thisrequirementissubjecttothediscretionoftheSecretaryasevidencedbytheclausetowhichtherequirementissubject“as
842C.F.R.§413.178(d)(6).

TheHonorableSeemaVermaAugust12,2020Page12of39
determinedappropriatebytheSecretary.”9ThisphrasegivestheSecretarytheauthoritytoestablishtheECE.
Inaddition,CMSindicatedthestatuteclearlyauthorizestheECEthroughthe
discretiontheSecretaryisprovidedtodevelopthemethodologyforsettingthetotalperformancescore.Thereisnotimelimitationonthisauthorityeither.
Section1881(h)(3)(A)(i)oftheActstates,“[T]heSecretaryshalldevelopamethodologyforassessingthetotalperformanceofeachproviderofservicesandrenaldialysisfacilitybasedonperformancestandardswithrespecttothemeasuresselectedunderparagraph(2)foraperformanceperiodestablishedunderparagraph(4)(D).”Giventhepossibilitythatfacilitiescouldbeunfairlypenalizedforcircumstancesthatarebeyondtheircontrol,webelievethebestwaytoimplementanextraordinarycircumstancesexceptionisundertheauthorityofthissection.Wethereforeproposedtointerpretsection1881(h)(3)(A)(i)oftheActtoenableustoconfigurethemethodologyforassessingfacilities’totalperformancesuchthatwewillnotrequireafacilitytosubmit,norpenalizeafacilityforfailingtosubmit,dataonanyESRDQIPqualitymeasuredatafromanymonthinwhichafacilityisgrantedanextraordinarycircumstancesexception.10
ThisauthorityandtherationaleoutlinedwhenCMSfinalizedtheECEpolicy
forCY2015supportsextendingtheECEperiodduringthepublichealthemergency,andweencourageCMStodosoimmediately.WealsoencourageCMStoalsoconsiderextendingtheECEforagraceperiodbeyondoncethepublichealthemergencyhasended(e.g.,30-60days)toprovidetimeforproviderstorampbackup,becauseareas/stateswillbehitunevenly.
B. KCPasksCMStoworkwiththeKCPtoaddresschallengesthe
pandemichascreatedfortheESRDQIP.
AsCMShasrecognizedthroughthenationwideECE,thepandemicisanextraordinarycircumstanceoverwhichwehavenocontrol.Ithasbeendevastatingtoprovidersandpatientsalike.TheimpactoftheoutbreaksintheUnitedStateshasrequiredanunprecedentedresponseandchangesinpracticepatternsthatwillremainwithusthroughoutthedurationofthepublichealthemergencyand,perhaps,evenlonger.
Wenotethat,inadditiontotheshort-termimpactonpatientcareand
outcomes,theCOVID-19pandemicwillhaveeffectsontheQIPforseveralyearsafterthepandemicends.ThisisbecausetheQIPreliesonbenchmarkssetthrough
942U.S.C.§1395rr(h)(1).10CMS,“End-StageRenalDiseaseProspectivePaymentSystem,QualityIncentiveProgram,andDurableMedicalEquipment,Prosthetics,Orthotics,andSupplies”DisplayCopy240(November2014).

TheHonorableSeemaVermaAugust12,2020Page13of39
previousyears’performance.TotheextentthatdialysisperformanceandmeasurereportingisanomalousduetoCOVID-19,thoseanomalieswillaffectthebenchmarksinsubsequentyears.
KCPaskedDiscernHealthtohelpusunderstandthepotentialimpactofthe
disruptionscreatedbythepandemicandhowthosedisruptionscouldimpacttheaccuracyandreliabilityoftheESRDQIP.DiscernmodeledthreedistinctscenariostoevaluatetheimpactoftheECEonQIPperformance.ItusedtheCY2019QIPperformancedatatomodeleachofthefollowingscenarios.
• Scenario1–BaselineScenario–Thebaselinescenariorepresentsa“normal”QIP
year,assumingnoECEandnoimpactfromCOVID.
• Scenario2–CurrentECEMaintained–ThisscenarioassumesthatthetermsoftheECEexpiringinJunearenotamended.Accordingly,weareassumingsmallermeasuredenominatorsasaresultoftheECE,andpoorerperformancefromJuly2020throughDecember2020.Wealsonotethatsmallerdenominatorsresultinlessreliabilityofthemeasurescores,butsincewecannotestimatetheimpactofpoorreliabilityonthedistribution,themodeldoesnotaccountforthissecond-ordereffect.
• Scenario3–ECEExtended3Months–ThisscenarioassumesthattheECEis
extendedanotherthreemonthsformeasuresreportedthroughCROWNWeborClaims.
Thecomponentsofthemodelwere:
• Measurethresholdeligibility–EachmeasureincludedinQIPhasarequired
denominatortoevaluateafacility.Forexample,theStandardizedHospitalizationRatio(SHR)measureisnotreportediftherearefewerthan5patientyearsatrisk.AnaturalconsequenceoftheECEisareductioninthedenominator,whichwillpushmorefacilitiesbelowthatthreshold.
• Impairedperformance–TheECEwasinitiallyissuedthroughtheendofJune.Ifthe
ECEislefttoexpireinJune(Scenario2)orisonlyextendedanother3months(Scenario3),CY2020willincludedatacollectedduringtheCOVID-19Pandemic.Evenatlowlevelsofcommunityprevalence,thepandemicwilllikelyaffectmeasureperformance.Thisinteractionisdynamicandisitsdirectionandmagnitudearenotknown.Forexample,thepandemichasbeenshowntodiscouragecareseekingbehavior,whichmayreducehospitalizationsmeasuredbytheStandardizedHospitalizationRatio(SHR)11.Ontheotherhand,somedataillustratetherelatively
11https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0193

TheHonorableSeemaVermaAugust12,2020Page14of39
highrateofhospitalizationforthosewithESRD12.Accordingly,aspecificimpactonperformanceisnotmodeled,butpotentialimplicationsofthisvariabilityareoutlinedasappropriate.
Inaddition,DiscernconsideredhowtheECEwouldaffecttheQIPduringthree
calendaryears,asoutlinedbelow:• PY2022/CY2020–FacilitieswithlowvolumeinCY2020asaresultofECEwill
beineligibleforperformancescores.
• PY2023/CY2021–FacilitieswithlowvolumeinCT2020asaresultofECEwillbeineligibleforimprovementscores.
• PY2024/CY2022–TheECEwillaffectthenationalperformancestandardused
tocalculatetheAchievementScore.
ResultsforPY2022/CY2020MeasureEligibility:DiscernestimatedthedenominatorsforeightmeasuresbasedonCY2018ESRDperformanceQIPdataandtheCOVID-19ECEFAQ.TheseeightmeasureswereselectedbasedonavailabilityofdataanddenominatorsintheCY2018QIPdataset.Below,thenumberoffacilitieseligibleforeachmeasure(Facilities),andthepercentofallfacilities(%Ttl)theyrepresentareshown:
Figure3.ESRDFacilitiesEligibleforEachMeasure
Scenario1 Scenario2 Scenario3
Facilities %Ttl Facilities %Ttl Facilities %TtlLongTermCatheter 6,475 87% 5,673 76% 3,598 48%SFR 6,442 87% 5,579 75% 3,341 45%Kt/V 7,055 95% 6,620 89% 5,403 73%Hypercalcemia 6,981 94% 6,582 89% 5,389 73%ICHCAHPSMeasures 2,957 40% 566 8% 566 8%SRR 6,859 92% 6,572 89% 6,030 81%STrR 6,292 85% 5,694 77% 4,431 60%SHR 6,895 93% 6,734 91% 6,403 86%
Fromthistable,6,895facilitieshavesufficientvolumetobeeligiblefortheSHRinScenario1;6,734inScenario2;and6,403inScenario3.Fromthisanalysis,SRRandSHRmeasuresretainfairlyhighcoverage;Kt/V,Hypercalcemia,STrR,LongTermCatheter,andSFRhavemodestcoverage;andtheICHCAHPSmeasurehaspoorcoverage.
12https://www.cms.gov/blog/medicare-covid-19-data-release-blog
TheHonorableSeemaVermaAugust12,2020Page15of39
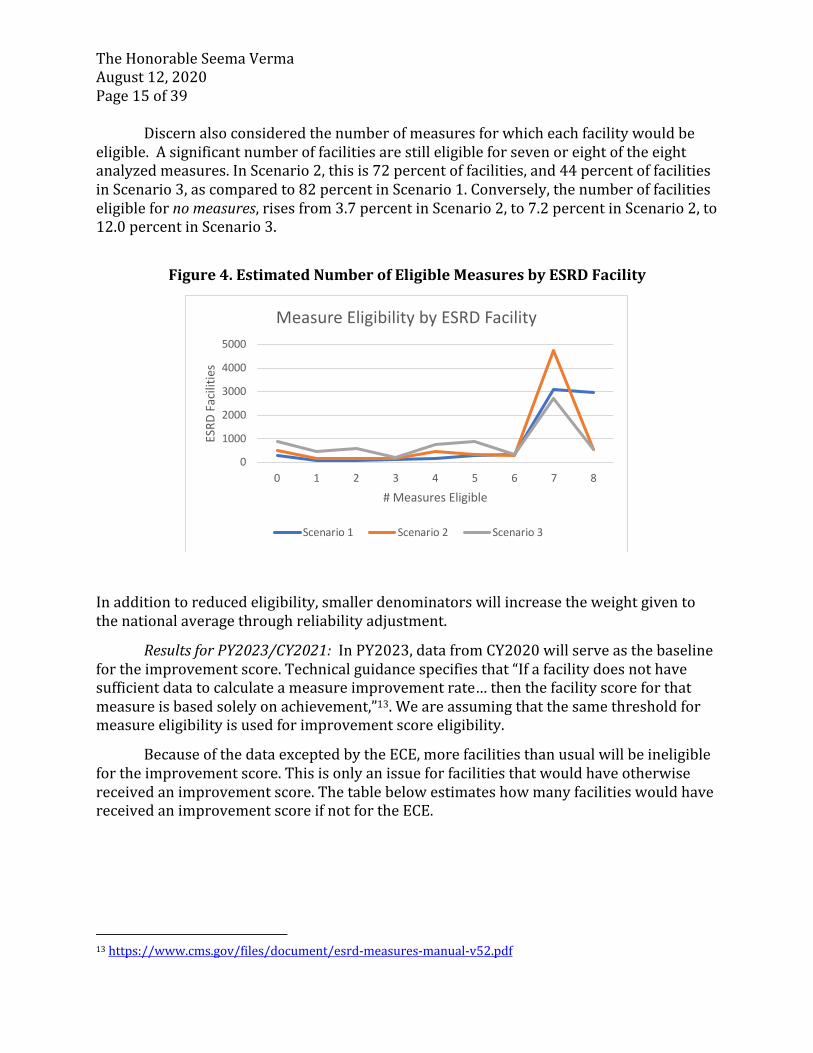
Discernalsoconsideredthenumberofmeasuresforwhicheachfacilitywouldbeeligible.Asignificantnumberoffacilitiesarestilleligibleforsevenoreightoftheeightanalyzedmeasures.InScenario2,thisis72percentoffacilities,and44percentoffacilitiesinScenario3,ascomparedto82percentinScenario1.Conversely,thenumberoffacilitieseligiblefornomeasures,risesfrom3.7percentinScenario2,to7.2percentinScenario2,to12.0percentinScenario3.
Figure4.EstimatedNumberofEligibleMeasuresbyESRDFacility
Inadditiontoreducedeligibility,smallerdenominatorswillincreasetheweightgiventothenationalaveragethroughreliabilityadjustment.
ResultsforPY2023/CY2021:InPY2023,datafromCY2020willserveasthebaselinefortheimprovementscore.Technicalguidancespecifiesthat“Ifafacilitydoesnothavesufficientdatatocalculateameasureimprovementrate…thenthefacilityscoreforthatmeasureisbasedsolelyonachievement,”13.Weareassumingthatthesamethresholdformeasureeligibilityisusedforimprovementscoreeligibility.
BecauseofthedataexceptedbytheECE,morefacilitiesthanusualwillbeineligiblefortheimprovementscore.Thisisonlyanissueforfacilitiesthatwouldhaveotherwisereceivedanimprovementscore.ThetablebelowestimateshowmanyfacilitieswouldhavereceivedanimprovementscoreifnotfortheECE.
13https://www.cms.gov/files/document/esrd-measures-manual-v52.pdf
0
1000
2000
3000
4000
5000
0 1 2 3 4 5 6 7 8
ESRD
Fac
ilitie
s
# Measures Eligible
Measure Eligibility by ESRD Facility
Scenario 1 Scenario 2 Scenario 3

TheHonorableSeemaVermaAugust12,2020Page16of39
Figure5.NumberofESRDFacilitiesReceivingLowerScoreDuetoIneligibilityfor
ImprovementScoreScenario2
Scenario3
VATCatheterMeasure 78 199VATFistulaMeasure 73 170Kt/VComprehensiveMeasure 93 191HypercalcemiaMeasure 50 155ICHCAHPSNephCommandCaringMeasure 98 98ICHCAHPSQualityofDialysisCareandOpsMeasure
71 71
ICHCAHPSProvidingInfotoPatientsMeasure 88 88ICHCAHPSOverallRatingofNephMeasure 133 133ICHCAHPSOverallRatingofDialysisStaffMeasure
108 108
ICHCAHPSOverallRatingofDialysisFacilityMeasure
86 86
SRRMeasure 20 51STrRMeasure 58 206SHRMeasure 20 64
Forexample,underScenario3,199facilitieswillbeineligibleforanimprovementscoreontheVATCatheterMeasureinPY2023,andwillreceivealowerscoreundertheAchievementScore.
ResultsforPY2024/CY2022:InPY2024/CY2022,datafromCY2020willserveasthenationalperformancestandardusedtocalculatetheAchievementScore.Giventhatthesetargetsaresetnationally,evenwithapartialyearofresults,smallnumberproblemsareunlikelyformostmeasures.However,iftheECEcontinuesthroughtheendof2020,theICHCAHPSmeasureswillhavenodatafor2020.
WhilethedirectionandmagnitudeofCOVID-19’sinfluenceonmeasureperformanceisnotknown,theimpactonthePY2024nationalperformancestandardwouldcounterbalancetheeffectonthePY2022performancescore.Forexample,ifCOVID-19isanetharmtofacilityperformance,morefacilitieswouldreceivepenaltiesinPY2022,buttheAchievementtargetswouldbelowerinPY2024.Whiletheseimpactscounterbalanceeachother,theirneteffectisunclear.
AstheDiscerndatashow,thereareseveralshort-andlong-termexpectedresultsoftheECEontheQIPandareasofuncertainty.GiventhesignificantfinancialeffectoftheQIPanduncertaintyaroundCOVID-19’seffectontheQIP,weaskthatCMS:

TheHonorableSeemaVermaAugust12,2020Page17of39
• Performanevidence-basedimpactassessmenttodeterminethelong-termeffectofCOVID-19onmeasuresusedforQIP.Long-termconsequencesofCOVID-19arestillbeingunderstoodbythescientificcommunity,andpreliminaryresearchsuggestseffectsonmultiplebodysystems.14OtherevidencesuggeststhatCOVID-19leadstokidneydamage,with15percentofthosehospitalizedrequiringdialysisafterdischarge.TheAmericathatemergesfromthePHEwillbedifferentfromtheonethatentersit.
• BaseImprovementandAchievementbenchmarksuponthelastfullyearofpre-COVID-19performance,CY2019.Basedupontheimpactassessment,modificationofthesescalendaryearbenchmarksmaybeneeded.
COVID-19presentsauniquechallengeforwhichthereislittleprecedent,andtherearelikelynosimplesolutions(especiallywhenwedonotyetknowthefullimpact).WebelievetheserecommendationswillstabilizetheQIPintothefuture,andpromotequalityoutcomes.
IV. KCPsupportsmaintainingthestructuralaspectsoftheESRDQIP
forPY2024,butencouragesCMStoconsiderchangesthatwillmakepaymentreductionsundertheprogrammorepredictable.
Aswehaveindicatedinpreviouscommentletters,weappreciatethatCMS
recognizestheimportanceofmaintainingthestructuralaspectsoftheESRDQIPyear-to-yearthatallowformulti-yearcomparisonsofproviders.Thisconsistencyisappropriateandhelpful.Thus,KCPtheproposalsforPY2024thatmaintaintheperformanceperiod,performancestandards,andscoringaspectsoftheprogram.WecontinuetourgeCMStoweightcertainmeasures,suchasthereductionincathetermeasure,moreheavilythanothers.
A. Addressingunintendedpaymentreductions.
Wealsoreiterateourconcernsthatinpastrulemakingsthepaymentreductionscale
hasresultedinasubstantialincreaseinthenumberoffacilitiesbeingpenalizedundertheESRDQIP,eventhoughtheactualperformanceofthefacilitieswasimproving.WealsoreiterateourconcernsthatinpastrulemakingsthepaymentreductionscalehasresultedinunpredictablepercentagesoffacilitiesbeingpenalizedundertheESRDQIP,eventhoughtheactualperformanceofthefacilitieswasimproving.
14https://www.advisory.com/daily-briefing/2020/06/02/covid-health-effects
TheHonorableSeemaVermaAugust12,2020Page18of39
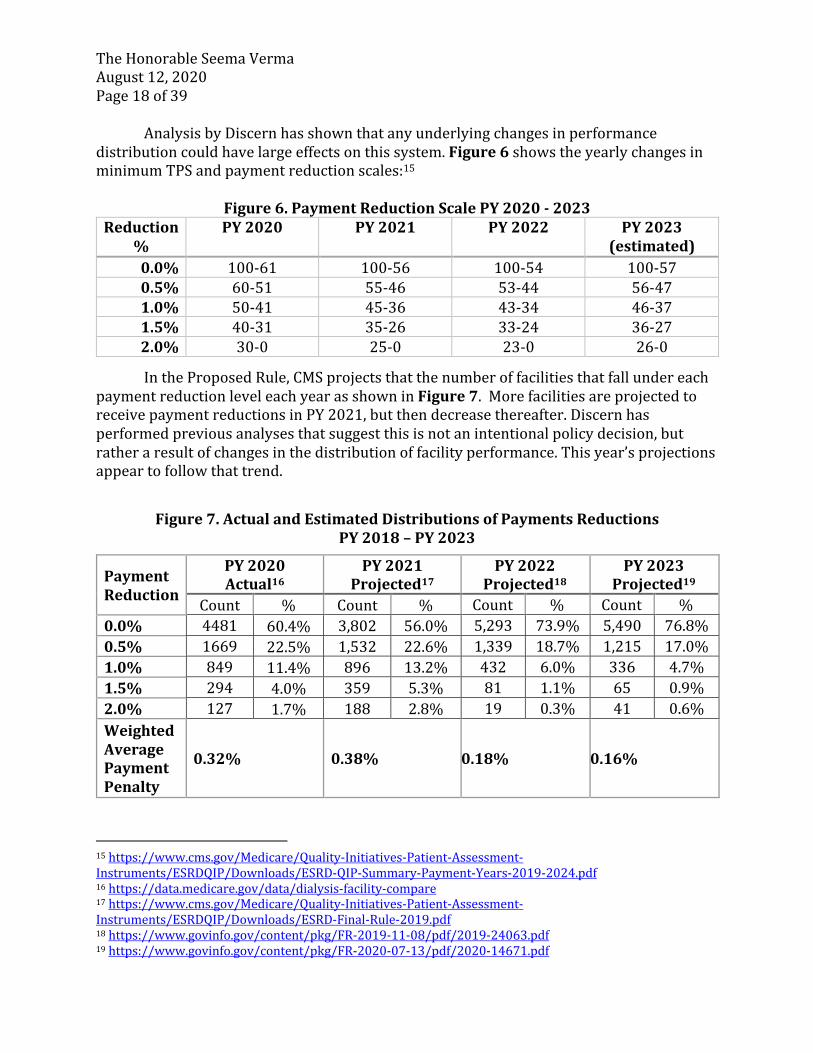
AnalysisbyDiscernhasshownthatanyunderlyingchangesinperformancedistributioncouldhavelargeeffectsonthissystem.Figure6showstheyearlychangesinminimumTPSandpaymentreductionscales:15
Figure6.PaymentReductionScalePY2020-2023
Reduction%
PY2020 PY2021 PY2022 PY2023(estimated)
0.0% 100-61 100-56 100-54 100-570.5% 60-51 55-46 53-44 56-471.0% 50-41 45-36 43-34 46-371.5% 40-31 35-26 33-24 36-272.0% 30-0 25-0 23-0 26-0
IntheProposedRule,CMSprojectsthatthenumberoffacilitiesthatfallundereachpaymentreductionleveleachyearasshowninFigure7.MorefacilitiesareprojectedtoreceivepaymentreductionsinPY2021,butthendecreasethereafter.Discernhasperformedpreviousanalysesthatsuggestthisisnotanintentionalpolicydecision,butratheraresultofchangesinthedistributionoffacilityperformance.Thisyear’sprojectionsappeartofollowthattrend.
Figure7.ActualandEstimatedDistributionsofPaymentsReductions
PY2018–PY2023
15https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/ESRDQIP/Downloads/ESRD-QIP-Summary-Payment-Years-2019-2024.pdf16https://data.medicare.gov/data/dialysis-facility-compare17https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/ESRDQIP/Downloads/ESRD-Final-Rule-2019.pdf18https://www.govinfo.gov/content/pkg/FR-2019-11-08/pdf/2019-24063.pdf19https://www.govinfo.gov/content/pkg/FR-2020-07-13/pdf/2020-14671.pdf
PaymentReduction
PY2020Actual16
PY2021Projected17
PY2022Projected18
PY2023Projected19
Count % Count % Count % Count %0.0% 4481 60.4% 3,802 56.0% 5,293 73.9% 5,490 76.8%0.5% 1669 22.5% 1,532 22.6% 1,339 18.7% 1,215 17.0%1.0% 849 11.4% 896 13.2% 432 6.0% 336 4.7%1.5% 294 4.0% 359 5.3% 81 1.1% 65 0.9%2.0% 127 1.7% 188 2.8% 19 0.3% 41 0.6%WeightedAveragePaymentPenalty
0.32% 0.38% 0.18% 0.16%

TheHonorableSeemaVermaAugust12,2020Page19of39
Giventhatpaymentreductionsshiftbasedonunderlyingprogramperformancetrends,KCPhaspreviouslyurgedCMStoconsidersettingpaymentpenaltiesatspecificdistributionpoints.ThiswouldcreateamorepredictablemodelforfacilitiesandCMS,whilestillincentivizingfacilitiestomaximizetheirQIPperformance.
KCPcontinuestobelievethatqualityisnotrelativeandthatanyprogramthat
requirespublicreportingandpenalizesprovidersshouldreflecttheactualqualityofcarebeingprovided.Tothatend,KCPreiteratesthatwewouldprefertheTotalPerformanceScore(TPS)cutpointsandthebenchmarksandthresholdsforattainmentandimprovementtobebasedobjectivegoals.WeremainconcernedthatsettingafixednumberoffacilitiesinanyofthefiveTPScategoriesdistortsqualityandeliminatestransparency.Itresultsinapre-determinednumberoffacilitiesbeinglabeledasprovidingpoorquality,wheninrealitytheremayactuallyagreaterorlessernumberoffacilitiesthatshouldfallintothelowestquintilebasedontheiractualperformance.Ifthisapproachweretaken,theresultsprojectedbyearlierrulemakingsshouldnothaveoccurred.WewouldliketomeetwithCMStodiscussspecificproposalsforresolvingthisproblem.
B. KCPcontinuestoencourageCMStoworkwiththecommunityand
NQFtodevelopabetterapproachtothesmallnumbersproblem.
AnotherissuethatweaskCMStoaddressrelatestothesmallnumberproblem.Thedecisiontoincludefacilitieswith11ormorecasesasthebasisformeasureapplicabilityinsteadofthemorewidelyaccepted25ormorecasesthatcommercialinsurersandotherprivatequalityprogramstypicallyapplyunderminesthestatisticalreliabilityofthemeasureresults.WeappreciatetheworkCMShasdoneonthesmallfacilityadjuster,butasDiscernHealthanalyseshaverepeatedlyshown(whichwehaveprovidedinseveralofthepreviousKCPcommentletters),thecurrentpolicyunfortunatelydoesnoteliminatetherandomresultsassociatedwithsmallnumbers.WeencourageCMStoreviewtheworkthattheNQFhascompletedinrelationtoruralareasthatidentifieswaystodevelopedmeasuresthatcanbeusedwithoutsmallnumbersnegativelyimpactingtheoutcomesreported,aswell.20
V. AlignmentofESRDQualityPrograms
Asafinalissue,KCPwouldliketoreiterateourcommitmenttoworkwithCMStoeliminatetheinconsistenciesandconflictsthathavearisenamongthevariousMedicareESRDqualityprograms.Inpreviouscommentletters,KCPhassuggestedawaytoaligntheprograms,bothintermsofmeasuresandstructuralscoringissues.WeaskagainthatCMSreviewtheserecommendationsandworkwithKCPtostrengthenbothprogramstoDialysisFacilityCompare(DFC)andtheQIPtoachievetheindependentgoalsCMShasidentifiedforeachandthatwouldpreservetheCongressionalintentfortheESRDQIP.
20Id.at6.

TheHonorableSeemaVermaAugust12,2020Page20of39
Figure8belowoutlinesthesuggestionsofthemembersofKCPforfocusingDFConmeaningfulmeasuresthatarenotusedintheESRDQIPandprovidingpatientswiththedataabouteachmeasureonitswebsiteinawaythatallowspatientstoprioritizethemeasureresultstheywanttosee.TheESRDQIPwouldbeasmallersetofmeaningfulmeasuresthatensurethateachmeasurehassubstantialweighttoavoidanyonemeasurebeingdilutedbytheothers.BecausetheCongressmandatedthattheQIPbeapublicreportingprogram,wesuggestedthatCMSshiftthestarratingstotheQIPTPSscores.Figure8:KCPRecommendationsforDistributingMeasuresAcrosstheQIPandDFCESRDQIPMeasures ESRDDFCMeasures
Standardizedhospitalizationratemeasure(currentratiomeasuremodifiedtoatruerisk-standardizedrate)
KCQAUFRMeasure
Standardizedreadmissionsratemeasure(currentratiomeasuremodifiedtoatruerisk-standardizedrate)
KCQAMedicationReconciliation(MedRec)Measure
Catheter>90DaysClinicalMeasure NHSNHealthcarePersonnelInfluenzaVaccinationReportingMeasure
Bloodstreaminfectionmeasure(notthecurrentmeasures,butonethatisvalidandreliableandmeetsotherNQFcriteria)
Kt/VDialysisAdequacyComprehensiveClinicalMeasure(modifiedtoreturntoindividualdialysisadequacymeasures)
PatientExperienceofCare:In-CenterHemodialysisConsumerAssessmentofHealthcareProvidersandSystems(ICHCAHPS)SurveyClinicalMeasure(modifiedperhistoricrecommendations)
Fistulameasures(CurrentAVmeasure;futurestandardizedfistularate)
Hgb<10g/dL ClinicalDepressionScreeningandFollow-UpReportingMeasure
Serumphosphorous StandardizedMortalityRatemeasure(currentratiomeasuremodifiedtoatruerisk-standardizedrate)
Transplantreferralmeasure,includingassistancewithfirstvisit
PatientReportedOutcomeMeasure(whendevelopedandendorsed)
WealsowouldaskthateachofthesemeasuresberefinedbasedonKCPrecommendationsforthespecificmeasures.WehavealsosuggestedthatCMScouldalignthetwoprogramsbyensuringthattheDFCandQIPmeasureshavethesamespecificationsandthesamescoringmechanism.
WeencourageCMStocarefullyreviewtheseproposalsandwouldwelcomethe
opportunitytoidentifywaysofbetteraligningtheESRDQIPandDFCsothatpatientscould

TheHonorableSeemaVermaAugust12,2020Page21of39
usebothprogramsfordecision-making,buteachonewouldbesupportiveoftheotherratherthanconflictingastheyaretoday.
V. ConclusionKCPappreciatestheopportunitytoprovidecommentsontheProposedRule.Kathy
Lester,ourcounselinWashington,willbeintouchtoscheduleameeting.However,pleasefeelfreetocontactheratanytimeifyouhavequestionsaboutourcommentsorwouldliketodiscussanyoftheminfurtherdetails.Shecanbereachedatklester@lesterhealthlaw.comor202-534-1773.Thankyouagainforconsideringourrecommendations.
Sincerely,
JohnButler
Chairman

TheHonorableSeemaVermaAugust12,2020Page22of39
AppendixA:KCPMembers
AkebiaTherapeuticsAmericanKidneyFund
AmericanNephrologyNurses’AssociationAmericanRenalAssociates,Inc.
AmericanSocietyofPediatricNephrologyAmgenArdelyx
AmericanSocietyofNephrologyAstraZeneca
AtlanticDialysisBaxterBBraun
CaraTherapeuticsCentersforDialysisCare
DaVitaDialyzeDirect
DialysisPatientCitizensFreseniusMedicalCareNorthAmerica
FreseniusMedicalCareRenalTherapiesGroupGreenfieldHealthSystems
KidneyCareCouncilNephrologyNursingCertificationCommissionNationalRenalAdministratorsAssociation
RenalPhysiciansAssociationRenalSupportNetworkRockwellMedicalRogosinInstituteSatelliteHealthcareU.S.RenalCare
VertexViforPharma

AppendixB:Table1:KCPMeasureSummaryandRecommendationsAnalysis
NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
1 0258 In-CenterHemodialysisConsumerAssessmentofHealthcareProvidersandSystems(ICHCAHPS)SurveyAdministration(clinicalmeasure):Measureassessespatients’self-reportedexperienceofcarethroughpercentageofpatientresponsestomultipletestingtools.
MeasureValidityCMS’owndatashowthattheICH-CAHPSresponserateislowandcontinuestodrop,andthattheincreasinglylowerresponseratesthreatenthevalidityofICH-CAHPSasanaccountabilitymeasure.ThePatient-ReportedOutcomesTEPsuggestedthatthelowresponserateisduetopatientfatigue;themannerinwhichthemeasureisfieldedexhaustspatientsanddiscouragesthemfromcompletingthesurvey.Understandingthepatient’sperspectiveandincorporatingitintohealthcaredecision-makingiscritical.
Recommendation:KCPsuggestmaintainingthemeasureasareportingmeasureuntiltheresponserateisimproved.Inpreviousletters,KCPhasofferedsuggestionsastohowtoaddresstheproblemoffatiguebydividingthesurveyintothethreevalidatedsectionandfieldingeachone.Then,whileafacilityissurveyedonthecompletetool,anyonepatienthastocompleteonlyathirdofthequestions.HomeDialysisPatientsDespiterequestsfromMedPACandothersinthecommunity,thesurveydoesnotincludehomedialysispatients.GiventheAdministration’sstrongdesiretoincentivizehomedialysis,havinganin-centeronlytoolseemstocontradictthatposition.
Recommendation:Thesurveyshouldberevisedtoincludehomedialysispatients;NQFendorsementofthenewmeasureshouldbesought.HomelessPatientsThesurveydoesnotexcludethehomeless.Becausefacilitiesarenotallowedtoprovidethesurveydirectlytopatients,distributiontohomelesspatientsisnotpossible.
Recommendation:CMSshouldexcludethehomelesstowhomthesurveycannotbedistributedgiventhatfacilitiesarenotallowedtoprovideitdirectlytopatients.BurdenReductionTwiceyearlyfieldingofthesurveyimposessubstantialadministrativeburdenonfacilitiesandcontributestopatient“survey-fatigue.”
Recommendation:CMSshouldfieldthesurveyonceayearandnottwicetoreduceburdenonfacilitiesandpatients.PatientEmpowermentFacilitiesdonotseeandsocannotusesurveyresultstoimprovecare.Thefactthatfacilitiesneverseethesurveyresultsandcannotcommunicatewithpatientsabouttheresultsleavespatientsfeelingunheard.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
Recommendation:CMSshouldallowfacilitiestoseetheresultsofthesurveyssotheycanrespondtothespecificpatientconcerns.PatientmembersoftheTEPshaverecommendedthisstep.KCPhasconsistentlyrecommendedextendingthesurveytoincludequestionsrelatedtohomedialysispatients.GiventheAdministration’sAdvancingKidneyCareInitiative,CMSshouldprioritizeaddingthesequestionstothesurveyandseekingNQFendorsementofthenewmeasure.
2 2496 StandardizedReadmissionRatio(SRR)(clinicalmeasure):Ratioofthenumberofobservedunplanned30-dayhospitalreadmissionstothenumberofexpectedunplanned30-dayreadmissions.
OverallReliabilityCMSdatahaveshowntheSRRisnotreliable.InthemostrecentiterationofthemeasurecurrentlyunderreviewatNQF,theoverallIURwas0.35.Statisticalliteraturetraditionallyinterpretsareliabilitystatisticof0.5-0.6as“unacceptable”.21
Recommendation:WeagainrecommendCMSimplementthemeasureand/oradjustmenttoyieldareliabilitystatistic>=0.70,consistentwithhowNQFbasesitsevaluationofmeasuresandmoregenerousthantheliterature.22Thisand/oranupdatetotheSFArangesisnecessarytopreventsmallfacilitiesfromhavingscoreshighlysubjecttorandomvariability.ReliabilityNotStratifiedbyFacilitySizeTestingdatastratifiedbyfacilitysizewerenotprovidedforthemeasureiterationcurrentlyunderreviewbyNQFbecauseit“isnotrequired.”CMSdatafrom2009revealedanIURof0.46forsmallfacilities—i.e.,forapproximatelyone-thirdofallfacilities,54percentofthescoretheyreceiveonthe2009SRRcouldbeattributabletorandomnoiseandnotsignal.
Recommendation:KCPbelievespenalizingfacilitiesforperformanceduetorandomchanceisnotappropriateandthatitisimperativethatCMSprovidethemostrecentreliabilityresultsstratifiedbyfacilitysize.Absentthatinformation,wesubmitthatthedemonstrablyunreliableSRR,ascurrentlyspecified,isparticularlyunreliableandunsuitableforuseinsmallfacilities.KCPmaintainsthatuntilitisreliableforallfacilities,theSRRshouldnotbeusedintheESRDQIP.PIURisNotanAppropriateMeasureofReliabilityCMS/UM-KECCcraftedanadditionalmetricofreliabilitytermedtheprofile-IUR(PIUR)23to“indicatethepresenceofoutliersorheaviertailsamongtheproviders,whichisnotcapturedintheIURitself....[When]thereareoutlierproviders,evenmeasureswithalowIURcanhavearelativelyhighPIURandcan
21AdamsJL.TheReliabilityofProviderProfiling:ATutorial.SantaMonica,California:RANDCorporation.TR-653-NCQA,2009.22Kline,P.(2000).Thehandbookofpsychologicaltesting(2nded.).London:Routledge,p.13;DeVellis,RF.(2012).Scaledevelopment:Theoryandapplications.LosAngeles:Sage.pp.109–110;Adams,JL.(2009).Thereliabilityofproviderprofiling.RANDHealth.
23HeK,DahlerusC,XiaL,LiY,KalbfleischJD.Theprofileinter-unitreliability.Biometrics.2019Oct23.doi:10.1111/biom.13167.[Epubaheadofprint.]

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
beveryusefulforidentifyingextremeproviders.”24ThePIURfortheSRRwasPIURis0.61,whichCMSinterpretsasdemonstratingthat“theSRRiseffectiveatdetectingoutlierfacilitiesandstatisticallymeaningfuldifferencesinperformancescoresacrossdialysisfacilities.”25Initsreviewofthismeasure,however,NQF’sScientificMethodsPanel(SMP),noneofwhomwerefamiliarwiththePIUR,disagreedthatitisanappropriatemeasureofreliabilityforanyQIPmeasure,whichareusedtodistinguishperformancebetweenprovidersfallinginthemiddleofthecurvetodeterminepenalties.TheSMPconcludedthattheIURisandremainstheappropriatemeasureofreliabilityforthispurpose.
Recommendation:KCPstronglyconcurswiththeNQF’sScientificMethodsPanel(SMP)conclusionthatthePIURisnotanappropriatemeasureofreliabilityforanyQIPmeasure.QIPmeasuresareusedtodistinguishperformancealongacontinuum,inparticularamongprovidersfallinginthemiddleofthecurvetodeterminepenalties;theabilitytoreliablydistinguishoutliersforimplementationofthesemeasuresisnotthepoint.TheIURisandremainstheappropriatemeasureofreliabilityformeasuresproposedfortheQIP.DoublePenaltiesThereisunnecessaryoverlapwiththeSRRandtheStandardizedHospitalizationRatiomeasure(SHR,NQF1463),whichresultsinafacilitybeingtwicepenalizedforareadmissionoccurringwithin30daysoftheindexdischarge.InresponsetostakeholdersexpressingthisconcernduringNQF’scurrentreviewofthemostrecentiterationofthemeasures,CMSacknowledgedthatthesamehospitalizationeventmayindeedbecountedtwice,butbelieves“thisisappropriatebecauseitplacesadditionalemphasisontheimportanceofavoidinghospitalizationsandre-hospitalizationfordialysispatients...[andcan]helpreducethismajorcostdriver.”Recommendation:WhileKCPagreesreductionofhospitalizationsandreadmissionsisparamount,wedonotbelieveinflictingspeciouspenaltiesondialysisfacilitiesisanappropriateorethicalsolutionandmayultimatelylimitaccesstocare.Toavoidthis“doublepenalty”,weagainaskthatCMSincludeanexclusionintheSHRforhospitalizationsthatoccurwithin29daysoftheindexdischarge.IncorporatingthisexclusionwillavoidreadmissionsbeingcapturedasahospitalizationbytheSHR,butitwillbecapturedasareadmissionbytheSRR.Thischangepreventsafacilityfrombeingpenalizedtwiceforeachsuchreadmission.Ratesvs.Ratios
24KalbfleischJD,HeK,XiaL,LiY.Doestheinter-unitreliability(IUR)measurereliability?HealthServicesandOutcomesResearchMethodology.2018;18(3):215-225.Doi:10.1007/s10742-018-0185-4.
25Citation:SHRmeasuressubmissionmaterialstoNQF.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
TheQIPshoulduseatruerisk-standardizedratemeasure;theratiomeasurehasrelativelywideconfidenceintervalsthatcanleadtofacilitiesbeingmisclassifiedandtheiractualperformancenotbeingreported.Aratiothatisthenmultipliedbyanationalmedianisnotatruerisk-standardizedrate.
Recommendations:CMScouldusetheunderlyingreadmissionrateandappropriatelyriskadjustitusingrace/ethnicity(asisdonewiththestandardizedmortalityratio).ItshouldalsobuildoffofitscontractedworkwithNQFanddevelopsocio-demographicadjusters,consistentwithKCP’s2018commentletterrecommendations.WhileCMSsubmitsthenewmeasuretotheNQFforendorsement,itcouldusethisimprovedreadmissionsratemeasureintheQIP.
CMShasacknowledgedinpreviousrulemakingthatratemeasuresaremoretransparentandeasierforpatientsandcaregiverstounderstand.CMSshouldactquicklytoestablishameaningfulreadmissionsmeasurefortheQIP.SDSFactorsCMScouldusetheunderlyingreadmissionrateandappropriatelyriskadjustitusingrace/ethnicity(asisdonewiththeSMR).ItshouldalsobuildoffofitscontractedworkwithNQFanddevelopsocio-demographicadjusters,consistentwithKCP’s2018commentletterrecommendations.WhileCMSsubmitsthenewmeasuretotheNQFforendorsement,itcouldusethisimprovedtransfusionratemeasureasareportingmeasureintheQIP.
Recommendation:CMSshouldappropriatelyadjusttheunderlyingtransfusionrateusingrace/ethnicity.BurdenReductionIncorporationofameasurewithscoresknowntobehighlysubjecttorandomvariabilityanddoublepenalizesprovidersimposesanunnecessaryburdenonfacilities,aswellaspatientswhoareinterestedinunderstandingtheactualperformanceoffacilitiesandcannot.
Recommendation:Asabove,KCPbelievesensuringthatperformancemeasuresaddressingthiscriticalclinicaltopicarefairandreliableisvitalandnecessarytoreducefacilityandpatientburdenandconfusion.PatientEmpowermentReadmissionsisanimportantfactorinmakinghealthcaredecisionsforpatients.
Recommendation:Asabove,KCPbelievesensuringthatperformancemeasuresaddressingthiscriticalclinicaltopicarereliableandavalidrepresentationofperformanceforallfacilitiesisvitalandnecessarytoinformpatientsinmakingtheseweightydecisions.
3 BasedonNQF2979
StandardizedTransfusionRatio(STrR)(areportingmeasure):Dialysisfacility
MeasureValidity

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
reportingofdataonMedicareclaimsandinCROWNWebthatareusedtodeterminethenumberofeligiblepatientyearsatriskforcalculatingtheriskadjustedfacilityleveltransfusionratio(STrR)foradultMedicaredialysispatients.
TheSTrRmeasurelacksvalidity;KCPispleasedthatCMShasacknowledgedthisconcernandsupportsitsdecisiontochangethemeasuretoareportingmetricwhilereviewingtheproblem.
InsufficientReliabilityforSmallFacilitiesTheSTrRclinicalmeasurehasnotbeendemonstratedreliableforsmallfacilities.Inthemostrecentiterationofthemeasure,currentlyunderreviewatNQF,theoverallIURfortheone-yearSTrRwas0.63-0.68acrosstheyears2014-2017.CMSdidnotprovidetestingdatastratifiedbyfacilitysizetoNQFbecauseit“isnotrequired”.Yetdatafrom2011-2014forwhichtherewasasimilaroverallIURrevealedvaluesaslowas0.30forsmallfacilities—thatis,forapproximatelyonethirdoffacilities,70percentofthescoretheyreceivedontheSTrRcouldbeattributabletorandomnoiseandnotsignal.Absentthisinformationforthenewclinicalmeasureiteration(currentlyunderreviewatNQF),wesubmitthattheSTrRclinicalmeasureremainsunreliableandunsuitableforuseinsmallfacilities,andthatuntilitisreliableforallfacilitiesthemeasureshouldnotbeusedintheESRDQIP.
Recommendation:KCPdoesnotbelievethatpenalizingfacilitiesforperformanceduetorandomchanceisappropriateandthatitisimperativethatCMSprovidethemostrecentreliabilityresultsstratifiedbyfacilitysize.WeagainrecommendthatCMSimplementthemeasureand/oradjustmenttoyieldareliableresult(reliabilitystatistic>=0.70),whichisconsistentwithhowtheNQFbasesitsevaluationofmeasuresandmoregenerousthantheliterature.26Thisstepisnecessarytopreventsmallfacilitiesfromhavingscoresthatarehighlysubjecttorandomvariabilityand/ortoupdatetheSFAranges.Untilitisreliableforallfacilities,theclinicalmeasureshouldnotbeusedintheESRDQIP.
TheSTrRisNotanAppropriateMeasureofAnemiaManagementGiventhatphysiciansandhospitals,notdialysisfacilities,controlwhetherornotapatientreceivesatransfusion,KCPagainrecommendsshiftingawayfromtheSTrRtoassessanemiamanagementtoamoreappropriatemeasurethatmoredirectlyreflectspatientqualityofcare,ismoreclearlyactionable,andreducesburden.TheSTrRshouldbereplacedwithlowhemoglobin(Hgb)measure(e.g.,aHgb<10g/dL).Whileitwillbenecessarytodevelopupdatedspecifications,exclusions,testing,andbusinessrules,KCPwouldwelcometheopportunitytoworkwithCMSonsuchameasure;wenotethatCMSdevelopedasimilarmeasureseveralyearsagothatwouldbeanappropriatestartingpoint.AlowHgbmeasurewouldreduceburden,becauseanytransfusionmeasurerequiresdialysisfacilitiestochasepaperworkcreatedbyotherproviders.ItalsoisabettermeasurethantheSTrRbecausefacilitiesandphysicianshaveaccesstopatienthemoglobindatainthefacility,whereastheydonothaveaccesstoSTrRdata.Moreover,itisactionablebyphysiciansandwillhaveadirectapositiveimpactonanissueofcriticalimporttopatients.
26Kline,P.(2000).Thehandbookofpsychologicaltesting(2nded.).London:Routledge,p.13;DeVellis,RF.(2012).Scaledevelopment:Theoryandapplications.LosAngeles:Sage.pp.109–110;Adams,JL.(2009).Thereliabilityofproviderprofiling.RANDHealth.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
Recommendation:KCPagainurgesCMStoadoptamoreappropriateanemiamanagementmeasure,suchastheHgb<10g/dL.WeareawarethatsuchameasureisnotcurrentlyendorsedbyNQF,butbelieveNQF’supdatedevidencealgorithmwouldprovideapathforitsconsiderationanew,andthattheHgb<10measure,stewardedbyCMS,representsaframeworktowhichupdatedspecifications,exclusions,andbusinessrulescouldbeapplied.KCPvolunteerstoworkwithCMStodevelopsuchameasure.Onceanappropriatemeasureisdeveloped,KCPasksthatCMSsubmitittoNQFforendorsement.Ratesvs.RatiosTheQIPshouldusetruerisk-standardizedratemeasures,becauseratiomeasureshaverelativelywideconfidenceintervalsthatcanleadtofacilitiesbeingmisclassifiedandtheiractualperformancenotbeingreported.Aratiothatisthenmultipliedbyanationalmedianisnotatruerisk-standardizedrate.
Recommendation:TheQIPshouldusetruerisk-standardizedratemeasures.SDSFactorsCMScouldusetheunderlyingtransfusionrateandappropriatelyriskadjustitusingrace/ethnicity(asisdonewiththeSMR).ItshouldalsobuildoffofitscontractedworkwithNQFanddevelopsocio-demographicadjusters,consistentwithKCP’s2018commentletterrecommendations.WhileCMSsubmitsthenewmeasuretotheNQFforendorsement,itcouldusethisimprovedtransfusionratemeasureasareportingmeasureintheQIP.
Recommendation:CMSshouldappropriatelyadjusttheunderlyingtransfusionrateusingrace/ethnicity.BurdenReductionShiftingtoamoreappropriateanemiamanagementmeasurefordialysisfacilitieswouldreduceburden,becauseanytransfusionmeasure(includingaratemeasure)requiresdialysisfacilitiestochasepaperworkcreatedbyotherproviderswhoalsoexperiencetheburdenonhavingtoprovidethedata/documentationofprovidingthetransfusion.
Recommendation:Asabove,KCPagainurgesCMStoadoptamoreappropriateanemiamanagementmeasure,suchastheHgb<10g/dL,tominimizefacilityburden.PatientEmpowermentAnemiamanagementisanimportantfactorinmakinghealthcaredecisionsfordialysispatients.Transfusionsalsoplacepatientsatriskofbecomingineligiblefortransplant.CMShasacknowledgedinpreviousrulemakingthatratemeasuresaremoretransparentandeasierforpatientsandcaregiverstounderstand.CMSshouldactquicklytoestablishameaningfultransfusionratemeasurefortheQIP.
Recommendation:TheQIPshouldusetruerisk-standardizedratemeasurestomakethemetricsmoremeaningfultopatients.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
4 NQFendorsed
differentmeasureandhasrejectedthepooledmeasure
(Kt/V)DialysisAdequacyComprehensive(clinicalmeasure):AmeasureofdialysisadequacywhereKisdialyzerclearance,itisdialysistime,andVistotalbodywatervolume.Percentageofallpatientmonthsforpatientswhosedelivereddoseofdialysis(eitherhemodialysisorperitonealdialysis)metthespecifiedthresholdduringthereportingperiod.
LackofNQFEndorsementCMSshouldremovemeasuresthatNQFhasrejectedaspartofitsendorsementprocess.AlthoughNQFhadendorsedadistinctcompositedialysisadequacymeasure,theNQFRenalStandingCommitteehassincereviewedthe(Kt/V)DialysisAdequacyComprehensivemeasureandrecommendedagainstendorsement.
Recommendation:CMSshouldadoptendorsedmeasureswhentheyareavailableovermeasuresthathavenotbeenendorsed.NQFhasendorsedothermeasuresinthedomainofdialysisadequacy:NQF#0249DeliveredDoseofHDAboveMinimum;NQF#0318DeliveredDoseofPDAboveMinimum;NQF#1423MinimumspKt/VforPediatricHDPatients;NQF#2704,MinimumDeliveredPDDose;NQF#2706,PediatricPDAdequacy—AchievementofTargetKt/V.PooledMeasureUsingapooledmeasureapproachresultsinallpatientsfromthefourdialysispopulations(adultandpediatric/peritonealandhemodialysis)tobepooledintoasingledenominatorandinscoresbeingcalculatedaswouldbedoneforasinglemeasure.Thisapproacheliminatestheabilitytodetermineperformanceonanyspecificpatientpopulationordialysismodality.
Thepooledmeasurealsodisincentivizeshomedialysis.Homefacilitieswillhaveloweradequacyscoresunderthepooledmeasure,whichwillmakethemmorelikelytobepenalized.
Recommendation:Topromotetransparencyindialysisperformanceandtheadoptionofhomedialysisbypatientsintheirfacilities,KCPsuggestsusingthedistinctadultHDandPDadequacyadultandpediatricmeasuresendorsedbytheNQF.KCPvolunteerstoworkwithCMStoaddressthesmallnumbersproblemforpediatricfacilitiesandsuggestsbuildingonthelessonslearnedfromtheNQF’sruralhealthprojectinwhichsmallnumberswereaddressedthroughothermeansthanpoolingmeasures.BurdenReductionTheconfusioncreatedbypoolingtheadequacymeasurescreatesanunnecessaryburdenonfacilities,aswellasonpatientswhoareinterestedinunderstandingtheactualperformanceoffacilitiesandcannot.
Recommendation:Toreducebothfacilityandpatientburden,KCPagainurgesCMStoreplacethepooledKt/VComprehensiveMeasurewiththeindividualNQF-endorsedadequacymeasures,asabove.PatientEmpowermentTomakeinformeddecisionsaboutmodalitychoice,patientsneedtounderstandafacility’sactualperformanceonthedifferentmodalitytypes.Thepooledmeasurehidesthisinformationfrompatients.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
Recommendation:Tofacilitatetheconveyanceofactionable,meaningfulinformationtopatients,KCPagainurgesCMStoreplacethepooledKt/VComprehensiveMeasurewiththeindividualNQF-endorsedadequacymeasures,asabove.
5 2977 HemodialysisVascularAccess:StandardizedFistulaRate(clinicalmeasure):MeasurestheuseofanAVfistulaasthesolemeansofvascularaccessasofthelasthemodialysistreatmentsessionofthemonth.
Ratesvs.RatiosTheQIPshouldusetruerisk-standardizedratesbecausetheratiomeasureshaverelativelywideconfidenceintervalsthatcanleadtofacilitiesbeingmisclassifiedandtheiractualperformancenotbeingreported.Aratiothatisthenmultipliedbyanationalmedianisnotatruerisk-standardizedrate.
Recommendation:CMScouldusetheunderlyingfistularatemeasure.WhileCMSsubmitsthenewmeasuretotheNQFforendorsement,itcouldusethecurrentmeasureintheQIP.
InsuranceStatusKCPnotesCMSmaywishtoworkwiththecommunitytodetermineifinsurancestatuspriortoreceivingdialysisshouldbeariskadjusterforthismeasure.
Recommendation:CMSshouldconsiderworkingwiththecommunitytodetermineifinsurancestatuspriortoreceivingdialysisshouldbeariskadjusterforthismeasure.PatientEmpowermentVascularaccessmaybethemostimportantmeasureforpatientsmakingdecisionsaboutdialysisfacilitiesintheESRDQIP,withcatheterreductionbeingthemostimportantofthetwoaccessmeasures.CMShasacknowledgedinpreviousrulemakingthatratemeasuresaremoretransparentandeasierforpatientsandcaregiverstounderstand.CMSshouldactquicklytomakethisaratemeasure.
Recommendation:TheQIPshouldusetruerisk-standardizedratemeasurestomakethemetricsmoremeaningfultopatients.BurdenReductionTheconfusionaroundtheratiomeasureandmisclassificationoffacilitiescreateanunnecessaryburdenonfacilities,aswellaspatientswhoareinterestedinunderstandingtheactualperformanceoffacilitiesandcannot.
Recommendation:TheQIPshouldusetruerisk-standardizedratemeasurestoreducefacilityandpatientburdenandconfusion.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
6 2978 HemodialysisVascularAccess:Long-TermCatheterRate(clinicalmeasure):Measurestheuseofacathetercontinuouslyfor3monthsorlongerasofthelasthemodialysistreatmentsessionofthemonth.
InsuranceStatusGenerally,KCPsupportsthismeasure,butnotesCMSmaywishtoworkwiththecommunitytodetermineifinsurancestatuspriortoreceivingdialysisshouldbeariskadjusterforthismeasure.
Recommendation:CMSshouldconsiderworkingwiththecommunitytodetermineifinsurancestatuspriortoreceivingdialysisshouldbeariskadjusterforthismeasure.
PatientEmpowermentVascularaccessmaybethemostimportantmeasureforpatientsmakingdecisionsaboutdialysisfacilitiesintheESRDQIP,withcatheterreductionbeingthemostimportantofthetwoaccessmeasures.
7 Basedon1454,(NQFreservestatus);theMeasureApplicationsPartnership(MAP)didnotsupportthemeasureinits2016report
Hypercalcemia(clinicalmeasure):Proportionofpatient-monthswith3-monthrollingaverageoftotaluncorrectedserumorplasmacalciumgreaterthan10.2mg/dL.
TheMeasureis“ToppedOut”Themeasureisnotusedtomakeclinicaldecisionsandistoppedout.
Recommendation:CMSshouldretirethemeasure.BurdenReductionReportingameasurethathasprovidesneitherclinicalvaluenordifferentiatesamongfacilitiesimposesaburdenwithoutprovidingbenefit.
Recommendation:CMSshouldretiretheHypercalcemiameasure.PatientEmpowermentGiventhetopped-outnatureofthismeasure,thereisnosignificantbenefitforpatients.
Recommendation:CMSshouldretiretheHypercalcemiameasure.
8 1463 StandardizedHospitalizationRatio(SHR)(clinicalmeasure):Risk-adjustedSHRofthenumberofobservedhospitalizationstothenumberofexpectedhospitalizations.
OverallReliabilityCMSdatahaveshownthattheSHRmeasureisnotreliable.InthemostrecentiterationofthemeasurecurrentlyunderreviewatNQF,theoverallIURfortheone-yearSHRwas0.53-0.59for2015-2018.Wenotethatthisvaluerepresentsadeclinefromthe2010-2013IURs(0.7),andthatstatisticalliteraturetraditionallyinterpretsareliabilitystatisticof0.50-0.60as“poor”.27
Recommendation:WeagainrecommendedthatCMSimplementthemeasureand/oradjustmenttoyieldareliableresult(reliabilitystatistic>=0.70),whichisconsistentwithhowtheNQFbasesitsevaluationof
27AdamsJL.TheReliabilityofProviderProfiling:ATutorial.SantaMonica,California:RANDCorporation.TR-653-NCQA,2009.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
measuresandmoregenerousthantheliterature.28Thisstepisnecessarytopreventsmallfacilitiesfromhavingscoresthatarehighlysubjecttorandomvariabilityand/ortoupdatetheSFAranges.
ReliabilityNotStratifiedbyFacilitySizeWhiletestingdatastratifiedbyfacilitysizewerenotprovidedforthemeasureiterationcurrentlyunderreviewbyNQFbecauseit“isnotrequired”,2010-2013datarevealedanIURaslowas0.46forsmallfacilities—thatis,forapproximatelyone-thirdoffacilities,54percentofthescoretheyreceivedontheSHRcouldbeattributabletorandomnoiseandnotsignal.Webelieveit'sdisingenuous,atbest,nottoprovidereliabilitybasedonfacilitysizemerelybecauseNQF"doesnotrequire"it.
Recommendation:KCPbelievespenalizingfacilitiesforperformanceduetorandomchanceisnotappropriateandthatitisimperativethatCMSprovidethemostrecentreliabilityresultsstratifiedbyfacilitysize.Absentthatinformation,wesubmitthatthedemonstrablyunreliableSHR,ascurrentlyspecified,isparticularlyunreliableandunsuitableforuseinsmallfacilities.Untilitisreliableforallfacilities,themeasureshouldnotbeusedintheESRDQIP.PIURisNotanAppropriateMeasureofReliabilityToassessmoredirectlythevalueofSHRinidentifyingfacilitieswithextremeoutcomes,CMSandUM-KECCcraftedanadditionalmetricofreliabilitytermedtheprofile-IUR(PIUR).29PerCMS,“ThePIURindicatesthepresenceofoutliersorheaviertailsamongtheproviders,whichisnotcapturedintheIURitself....[When]thereareoutlierproviders,evenmeasureswithalowIURcanhavearelativelyhighPIURandcanbeveryusefulforidentifyingextremeproviders.”30ThePIURfortheSHRwasPIURis0.75-0.85for2015-2018,whichCMSinterpretsasdemonstratingthat“theSHRiseffectiveatdetectingoutlierfacilitiesandstatisticallymeaningfuldifferencesinperformancescoresacrossdialysisfacilities.”31Wenotethatinitsreviewofthismeasure,however,NQF’sScientificMethodsPanel(SMP),noneofwhomwerefamiliarwiththePIUR,disagreedthatitisanappropriatemeasureofreliabilityforanyQIPmeasure,whichareusedtodistinguishperformancebetweenprovidersfallinginthemiddleofthecurvetodeterminepenalties.TheSMPconcludedthattheIURisandremainstheappropriatemeasureofreliabilityforthispurpose.
Recommendation:KCPstronglyconcurswiththeNQF’sScientificMethodsPanel(SMP)conclusionthatthePIURisnotanappropriatemeasureofreliabilityforanyQIPmeasure.QIPmeasuresareusedtodistinguish
28Kline,P.(2000).Thehandbookofpsychologicaltesting(2nded.).London:Routledge,p.13;DeVellis,RF.(2012).Scaledevelopment:Theoryandapplications.LosAngeles:Sage.pp.109–110;Adams,JL.(2009).Thereliabilityofproviderprofiling.RANDHealth.
29HeK,DahlerusC,XiaL,LiY,KalbfleischJD.Theprofileinter-unitreliability.Biometrics.2019Oct23.doi:10.1111/biom.13167.[Epubaheadofprint]30KalbfleischJD,HeK,XiaL,LiY.Doestheinter-unitreliability(IUR)measurereliability?HealthServicesandOutcomesResearchMethodology.2018;18(3):215-225.Doi:10.1007/s10742-018-0185-4.
31Citation:SHRmeasuressubmissionmaterialstoNQF.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
performancealongacontinuum,inparticularamongprovidersfallinginthemiddleofthecurvetodeterminepenalties;theabilitytoreliablydistinguishoutliersforimplementationofthesemeasuresisnotthepoint.TheIURisandremainstheappropriatemeasureofreliabilityformeasuresproposedfortheQIP.Ratesvs.RatiosTheQIPshouldusetruerisk-standardizedratesbecausetheratiomeasureshaverelativelywideconfidenceintervalsthatcanleadtofacilitiesbeingmisclassifiedandtheiractualperformancenotbeingreported.Aratiothatisthenmultipliedbyanationalmedianisnotatruerisk-standardizedrate.
Recommendation:TheQIPshouldusetruerisk-standardizedratemeasures.SDSFactorsCMScouldusetheunderlyinghospitalizationrateandappropriatelyriskadjustitusingrace/ethnicity(asisdonewiththeSMR).ItshouldalsobuildoffofitscontractedworkwithNQFanddevelopsocio-demographicadjusters,consistentwithKCP’s2018commentletterrecommendations.WhileCMSsubmitsthenewmeasuretotheNQFforendorsement,itcouldusethisimprovedhospitalizationratemeasureintheQIP.
Recommendation:CMSshouldappropriatelyadjusttheunderlyinghospitalizationrateusingrace/ethnicity.BurdenReductionTheconfusionaroundtheratiomeasureandmisclassificationoffacilitiescreateanunnecessaryburdenonfacilities,aswellaspatientswhoareinterestedinunderstandingtheactualperformanceoffacilitiesandcannot.
Recommendation:TheQIPshouldusetruerisk-standardizedratemeasurestoreducefacilityandpatientburdenandconfusion.PatientEmpowermentHospitalizationratesarecriticalindicatorsofqualityperformanceforbothpatientsandproviders.ThelackofreliabilityfortheSHRmeansthatthemeasureisnotaccuratelyreflectingtheperformanceofsmallfacilitiesandprovidesinaccurateinformationuponwhichpatientsarethenaskedtomakehealthcaredecisions.Recommendation:TheQIPshouldusetruerisk-standardizedratemeasurestomakethemetricsmoremeaningfultopatients.
9 BasedonNQF#0418
ClinicalDepressionScreeningandFollow-Up(reportingmeasure):FacilityreportsinCROWNWeboneofsixconditionsforeach
CMSShouldImplementMeasuresasEndorsedbyNQFCMShaschangedthespecificationsmakingthemeasuredifferentthantheonethatNQFendorsed.ThesechangesmeanthattheQIPmeasurehasnotbeenreviewedorendorsedbyNQF.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
qualifyingpatienttreatedduringperformanceperiod.
Recommendation:IfitweretoremainintheQIP,KCPcontinuesrecommendingthatCMSuseitasareportingmeasurebutencouragesCMStoworkwiththekidneycarecommunitytoestablishastandardizedESRD-specifictool.BurdenReductionWhenCMSchangesthespecificationsofanNQF-endorsedmeasure,itcreatesaburdenonfacilitiesbecausetheyarereportingameasurethatmayormaynotmeetmeasuredevelopmentcriteria,andifitdoesnot,reportingtheinformationdoesnotprovideanyvalue.Patientsareburdenedbyhavingtofigureoutontheirownwhetherornotthemeasureisaccuratelyreportingonafacility’sperformance.
Recommendation:Toreducebothfacilityandpatientburden,KCPagainurgesCMStoimplementonlyNQF-endorsedmeasurespecificationsintheQIP.PatientEmpowerment:ClinicalDepressionisanimportantcomponentinmanagingpatientslivingwithkidneyfailure.However,thismeasureisbettersuitedfortheDialysisFacilityCompareprogramsothatafacility’sperformanceonthemeasureisnotdilutedbyothermeasures,makingitdifficultforpatientstouseittomakedecisions.CMShasindicatedthatthepurposeofDFCisspecifictothistask.
Recommendation:Tofacilitatepatientusability,theClinicalDepressionScreeningandFollow-UpmeasureshouldbelimitedtouseintheDialysisFacilityCompareprogram.
10
BasedonNQF2701:AvoidanceofUtilizationofHighUltrafiltrationRate(>13ml/kg/hour)
UltrafiltrationRate(reportingmeasure):Numberofmonthsforwhichafacilityreportselementsrequiredforultrafiltrationratesforeachqualifyingpatient.
Patient-MonthsConstructionKCPappreciatesthatCMSnowconcurswithourlongstandingpositionthattheNQF-endorsedUFRmeasurespecificationsshouldbeusedandhasrevisedthespecificationstothepatient-monthsconstruction.Aswehavepreviouslynoted,KCPstronglyobjectedtothechangeto“facility-months”;thepatient-monthsmeasureconstructionwascarefullyanddeliberatelyselectedbyKCQAwhendevelopingthemeasuresothatpatientsreceivingcareatagivenfacilityforfewerthan12monthswouldstillbecapturedandcountedinmeasurecalculationsandwouldcontributetothefacilityscoreinaccordancewiththenumberofmonthstheyreceivedcarethere.Thisspecific—andintended—constructionwassupportedbytheNQFRenalStandingCommitteewhenitendorsedthemeasurein2017.Thecalculationusingthepatient-monthsconstructionnowcomportswiththeNQF-endorsedmeasureandshouldbeused.
BasedonNQF2701KCPalsoappreciatesCMS’explicitnotationinthisProposedRulethattheUFRReportingMeasureisbasedontheKidneyCareQualityAlliance’sNQF-endorsedAvoidanceofUtilizationofHighUFR,NQF#2701.PatientEmpowerment

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
KCPcontinuestobelievethatfluidmanagementisanimportantqualityarea,whichiswhyitfundedtheKidneyCareQualityAlliance(KCQA)toundertakesuchmeasuredevelopment.KCPmembersidentifiedaddressingfluidmanagementasthehighestpriorityinKCP’sStrategicBlueprintforKidneyCareQuality.
11
BasedonNQF1460
NHSNBloodstreamInfection(BSI)inHemodialysisPatients(clinicalmeasure):TheStandardizedInfectionRatio(SIR)ofBSIswillbecalculatedamongpatientsreceivinghemodialysisatoutpatienthemodialysiscenters.
NHSNValidationStudyKCPappreciatesCMS’proposaltoreducethesubmissionrequirementforfacilitiesselectedtoparticipateintheNHSNvalidationstudyfrom40to20patientrecordsfromanytwoquartersduringtheyearfortheapplicablecalendaryear.Weconcurthatthisrevisedapproachwillreducefacilityburdenwhilemaintaininganadequatesamplesizeforthemeasurevalidationanalysis.
TheMeasureisNotReliableorValidThemeasureisnotmeetingtherigorouscriteriaofreliabilityandvalidity;asaresult,themeasureisnotreportingaccuratedatatopatientsorproviders.ResearchconductedbytheCDC(themeasure’sdeveloper)andothers,includingCMS,showthatthemeasureisnotvalidorreliable.CMSdatashowsthatasmanyas60-80percentofdialysiseventsmaybeunder-reportedwiththeNHSNBSImeasure.32Inafollow-upTEP,CMSandotherHHSagencyofficialsindicatedthatthepercentagewasslightlylower,butTEPmembersraisedconcernsthatthepercentageremainsunacceptablyhigh.Inlightofthesedata,itisclearthatthemeasuredoesnotmeetthecriterionofvalidityforendorsement.Thismeansthatthemeasureinmanyinstancesmayincorrectlyreportthatafacilityhasalownumberofbloodstreaminfectionswhen,infact,thefacilityhasahighernumber.Giventheunderstandableimportancethatpatientsplaceonafacility’sabilitytomanagebloodstreaminfections,ameasurethatfailstoaccuratelyrepresentthefacility’sperformancedeprivespatientsoftheirabilitytomakeinformedhealthcaredecisions.Italsounfairlypenalizesfacilitiesthatdiligentlypursueandreportthehospitalinfectiondatanecessaryforafullpictureofinfectionrates.
Recommendation:Intheshort-term,removingtheclinicalmeasureandusingtheDialysisEventReportingMeasurealonewouldletpatientsknowwhetherafacilityisreportingsuchinfectionswhileallowingCMSandthecommunitytofixtheproblems.Inpreviouscomments,KCPhassuggestedthatCMSconverttheNHSNBSImeasuretoareportingmeasurewhileitconvenesaTEPtoidentifytheproblemwiththemeasureandproposesolutions.Onceanewmeasureisspecified,CMSshouldsubmitittoNQFforendorsementbeforeadoptingitasaclinicalmeasurefortheESRDQIP.CMSShouldImplementMeasuresasEndorsedbyNQFCMSshouldavoidmodifyingNQF-endorsedmeasureswhenadoptingthemfortheESRDQIP;theNHSNBloodstreamInfection(BSI)inHemodialysisPatientsisnotedtobe“basedon”NQF1460butdoesnotfullycomportwiththeendorsedspecifications.
322018ProposedRuleDisplayCopy90.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
Recommendation:Asdescribedabove,CMSshouldeliminatetheNHSNBSImeasureandrelyupontheNHSNdialysiseventreportingmeasurewhileCMSconvenesaTEPtoidentifytheproblemswiththeBSImeasure.Onceithasrevisedthemeasure,CMSshouldsubmittherevisedmeasure[toNQF],whichwouldmeetthevalidityrequirementsofendorsements,totheNQF.
BurdenReductionResearchsuggeststhattheunderreportingidentifiedwiththismeasuremaybeduetothefactthathospitals,notdialysisfacilities,havetherequisitedata.Itisaburdenonhospitalstoprovidethedatatofacilitiesandonfacilitiestochasehospitalsforthedata.Addressingthisproblemthroughavalidmeasurewouldreduceunnecessaryburdenonthehospitalsandfacilities.
Recommendation:Tominimizefacilityburdens,KCPagainurgesCMStoeliminatetheNHSNBSImeasureandrelyupontheNHSNdialysiseventreportingmeasurewhileCMSexploresandidentifiestheproblemswiththeBSImeasure.PatientEmpowermentThismeasuretopicareaiscriticallyimportanttopatients.AmeasurethatincorrectlyreportsafacilityashavingalownumberofBSIwheninfactitdoesnotdistortsthecarebeingprovidedandmisleadspatientsinawaythatdisruptstheirabilitytomakeaninformedhealthcaredecision.
Recommendation:KCPagainurgesCMStoeliminatetheNHSNBSImeasureandrelyupontheNHSNdialysiseventreportingmeasurewhileCMSexploresandidentifiestheproblemswiththeBSImeasure.
12
NeversubmittedforNQFendorsement
NHSNDialysisEvent(reportingmeasure):NumberofmonthsforwhichfacilityreportsNHSNDialysisEventdatatoCDC.
CMSHasNotSubmittedthisMeasuretoNQFforEndorsementThisisinconsistentwiththeintentoftheCongressforCMStouseNQFendorsedmeasuresintheQIP(seeSSA§1881(h)(2)(B)).Withouttherigorofendorsement,thereliabilityandvalidityofthemeasureremainuncertainandthespecificationhavebeenallowedtomorphsothattherearenowseveralsubjectivelyinterpretedsignsofinfection(e.g.,swelling,redness)included.
Recommendation:CMSshouldremovethesubjectivefactorsandseekNQFendorsementofthemeasure.BurdenReductionTheexpansionofthereportingprotocoltobehighlysubjectiveisextremelyburdensomeanddoesnotcontributetothemeasure’sunderlyingpremise—toidentifyBSIsverifiedbypositivebloodcultures.Eliminatingthesubjectivefactorswouldhelpreducetheburdenofthismeasure.
Recommendation:CMSshouldremovethesubjectivefactorsspecifiedinthemeasure.PatientEmpowerment
NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
ItisimportanttopatientsandKCPthatfacilitiesareappropriatelymonitoringBSI.However,theinformationreportedshouldbeobjectiveandservethepurposeofidentifyingpatientsatriskforBSIsotheycanreceiveappropriatetreatment.Thesubjectivefactorsaddedtothemeasurespecificationslastyeardonotachievethisgoal.
Recommendation:CMSshouldremovethesubjectivefactorsspecifiedinthemeasure.
13
RejectedbyNQF
PercentageofPrevalentPatientsWaitlisted(PPPW)(clinicalmeasure):Percentageofpatientsateachdialysisfacilitywhowereonthekidneyorkidney-pancreastransplantwaitlistaveragedacrosspatientsprevalentonthelastdayofeachmonthduringtheperformanceperiod.
CMSShouldRemoveMeasuresNQFhasRejectedfromtheQIPNQFhasrejectedthePPPWmeasureaslackingvalidity.
Recommendation:CMSshouldremovethePPPWfromtheQIP.KCPstandsreadytodevelopanappropriatetransplant-relatedmeasurewithCMSandothersinthekidneycarecommunitythatmeetstheendorsementcriteriaofNQFandtheintentoftheCongress.KCPDoesNotSupportAttributiontoDialysisFacilitiesofSuccessful/UnsuccessfulWaitlistingKCPbelievesthatwhileareferraltoatransplantcenter,initiationofthewaitlistevaluationprocess,orcompletionofthewaitlistevaluationprocessmaybeappropriatefacility-levelmeasuresthatcouldbeusedinESRDqualityprograms,thePPPWisnot.Waitlistingperseisadecisionmadebythetransplantcenterandisbeyondadialysisfacility’slocusofcontrol.Inreviewingthesemeasures,weofferthefollowingcomments.
Recommendation:CMSshouldremovethePPPWfromtheQIP.KCPstandsreadytodevelopanappropriatetransplant-relatedmeasurewithCMSandothersinthekidneycarecommunitythatmeetstheendorsementcriteriaofNQFandtheintentoftheCongress.
StratificationofReliabilityResultsbyFacilitySizeCMShasprovidednostratificationofreliabilityscoresbyfacilitysizeforeithermeasure;wearethusunabletodiscernhowwidelyreliabilityvariesacrossthespectrumoffacilitysizes.WeareconcernedthatthereliabilityforsmallfacilitiesmightbesubstantiallylowerthantheoverallIURs,ashasbeenthecase,forinstance,withotherCMSstandardizedratiomeasures.
Recommendation:KCPbelievesitisincumbentonCMStodemonstratereliabilityforallfacilitiesbyprovidingdatabyfacilitysize.BurdenReductionCollectingandsubmittingdataonthePPPWmeasurewhenitdoesnotprovideanaccurateviewofdialysisfacilityqualityisaburdenwithoutbenefit.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
Recommendation:CMSshouldremovethePPPWfromtheQIP.KCPstandsreadytodevelopanappropriatetransplant-relatedmeasurewithCMSandothersinthekidneycarecommunitythatmeetstheendorsementcriteriaofNQFandtheintentoftheCongress.PatientEmpowermentMakingsurethatfacilitiesaredoingeverythingwithintheirscopetopromotetransplants(e.g.,educatingpatientsabouttransplantoptions,protectingpatientsfrominfection,referringpatientstotransplantcenters,etc.)isimportanttopatients,thecommunity,andtheAdministration.However,usingameasurethatisnotaccuratelyreportingonfacilityactionmisleadspatientsandforcesthemtomakehealthcaredecisionsbasedonfalsedata.
Recommendation:CMSshouldremovethePPPWfromtheQIP.KCPstandsreadytodevelopanappropriatetransplant-relatedmeasurewithCMSandothersinthekidneycarecommunitythatmeetstheendorsementcriteriaofNQFandtheintentoftheCongress.
14
BasedonNQF2988
MedicationReconciliationforPatientsReceivingCareatDialysisFacilities(MedRec)(reportingmeasure):Percentageofpatient-monthsforwhichmedicationreconciliationwasperformanceanddocumentedbyaneligibleprofessional.
Patient-MonthsConstructionKCPappreciatesthatCMSnowconcurswithourlongstandingpositionthattheNQF-endorsedMedicationReconciliationmeasurespecificationsshouldbeusedandhasrevertedtothepatient-monthsconstruction.Aswehavepreviouslynoted,KCPstronglyobjectedtothechangeto“facility-months”;themeasurewasdeliberatelyconstructedandendorsedusingpatient-monthstoaddressthefactthatpatientsmaycontributevaryingamountsoftimetotheannualdenominatorpopulation.Thecalculationusingthepatient-monthsconstructionnowcomportswiththeNQF-endorsedmeasureandshouldbeused.DiscrepanciesBetweenthePublishedandtheEndorsedSpecificationsRemainCMShaschangedthespecificationsfromthosethatNQFendorsed.Specifically,theQIPrevisionsdeletespecificitemsthatmustbeaddressedinthemedicationreconciliation(e.g.,medicationname,dosage,etc.).ThesechangesmeanthatNQFhasnotreviewedorendorsedthenewmeasure.Recommendation:KCPsupportsusingtheMedicationReconciliationmeasureintheQIPandasksthatCMSusesthespecificationsasendorsedbytheNQF.BurdenReductionWhenCMSchangesthespecificationofanNQF-endorsedmeasure,itcreatesaburdenonfacilitiesbecausetheyarereportingameasurethatmayormaynotmeetmeasuredevelopmentcriteriaand,ifitdoesnot,reportinginformationthathasquestionablevalue.Patientsareburdenedbyhavingtofigureoutontheirownwhetherornotthemeasureisaccuratelyreportingafacility’sperformance.
Recommendation:KCPsupportsusingtheMedicationReconciliationmeasureintheQIPandasksthatCMSusesthespecificationsasendorsedbytheNQF.

NQFNUMBER
MEASURETITLE/DESCRIPTION
KCPCONCERNSANDRECOMMENDATION
PatientEmpowermentTEPshaveconsistentlyendorsedtheadoptionofamedicationreconciliationmeasure.TobeconsistentwithCMS’ownprinciplesandthoseofexpertslikeNQF,themeasureusedshouldbereliableandvalidsothatpatientscanusetheinformationtomakeinformeddecisions.Changingthespecificationscallsthenew,revisedmeasure’svalidityandreliabilityintoquestion.
Recommendation:KCPsupportsusingtheMedicationReconciliationmeasureintheQIPandasksthatCMSusesthespecificationsasendorsedbytheNQF.





























