Embed Size (px)
Citation preview

L E T T E R TO T H E E D I T O R S J Neurol (1995) 242 : 541-546 © Springer-Verlag 1995
N. Yuki M. Yamada T. Yuasa K. Kaneko T. Inuzuka M. Arai S. Sato S. Tsuji S. Takeda K. Kawasaki K. Oyanagi F. Ikuta T. Miyatake
Atypical motor neuron disease with severe ophthalmoloplegia: a report of two cases
Received: 27 September 1994 Received in revised form: 19 December 1994 Accepted: 2 February 1995
Sirs: Komachi et al. [5] recently re- ported a patient with atypical motor neuron disease (MND) who exhib- ited external ophthalmoplegia and frontal dementia. Neuropathological findings of the patient showed cen- tral chromatolysis of the neurons in the oculomotor nucleus and a spongy state in the frontal cortex. The au- thors proposed that the case was a new subtype of MND. We describe the cases of and autopsy findings of two patients who presented with ophthahnoplegia, but did not develop dementia. To clarify the nosological position of our patients, we reviewed the clinical features and the patho- logical findings of sporadic MND cases in which severe external oph- thalmoplegia without dementia was reported.
Patient 1 was a 61-year-old man who experienced easy fatigability and muscular weakness in the proxi- mal upper limbs in May 1984. In July, weakness of the neck and prox- imal lower limbs had developed and he was unable to stand alone. On ad-
mission to our hospital in August, he was alert and showed normal intel- lectual ability. Neurological exami- nation revealed facial muscular weakness, proximal-dominant mus- cle weakness and wasting of the ex- tremities. Fasciculations were pre- sent in the tongue, biceps brachii and quadriceps muscles. Tendon reflexes were diminished in biceps and radi- alis, but present in triceps, knee and ankle. Clonus at knee and ankle was not elicited. Hoffmann and Babinski signs were absent. Vibration sense was impaired in the feet. He showed hypohidrosis and impotence. Crea- tine kinase activity was normal. Serum immunoelectrophoresis de- tected no M-protein. Serum antibody to GM1, GM2, GDla , GDlb , G T l b and G Q l b was negative. Cere- brospinal fluid (CSF) protein content was 215 mg/dl (IgG 23.0 mg/dl) with normal cellularity. No anti- HTLV-I antibody was elicited in the serum or CSF. His brain CT was nor- mal. A motor nerve conduction study showed normal action potentials, normal latencies and decreased con- duction velocities (ulnar nerve, 45.3 m/s; posterior tibial nerve 36.7 m/s). Neither conduction block nor abnor- mal temporal dispersion were seen. Sensory nerve action potentials and conduction velocity in the ulnar nerve were normal. No action poten- tials were elicited in the sural nerve. EMG showed long-duration units, polyphasic units and poor interfer- ence. No high amplitude units were found.
He was prescribed 60 mg pred- nisolone daily because chronic in- f lammatory demyelinating polyneu- ropathy was suggested by the ele- vated CSF protein and the reduced nerve conduction velocities, but this treatment was not effective. Five months after the onset of neurologi- cal symptoms he required constant mechanical ventilation. Hypaesthe- sia, hypalgesia and paraesthesias of glove and stocking distribution de-
veloped. No voluntary muscle con- tractions in the limbs were seen in November. Atrophy of the tongue and facial muscles as well as of the limb muscles was progressive. Urine retention developed in August 1985. Cystometry revealed an atonic blad- der. Right Horner 's syndrome devel- oped in December 1985, but the pupil returned to normal in February 1986. Upward gaze palsy developed in April 1986 (24 months after on- set), then downward and lateral gaze palsy. The oculocephalic reflex was present. Communication was diffi- cult for him even though he did not develop complete external ophthal- moplegia. His light reflexes became sluggish. In September 1986, he showed complete vertical gaze palsy and severe lateral gaze palsy, and the oculocephalic and light reflexes were absent. He had bedsores on his but- tocks. He died of pneumonia in Oc- tober 1986 after a total clinical course of 29 months. There was no positive family history of MND.
The brain weighed 1260 g. There was severe loss of pyramidal neurons in the pre-central gyrus, including Betz's cells. Mild neuronal loss and gliosis were found in the globus pal- lidus and subthalamic nucleus. The cranial nerves and nuclei showed variable degeneration, in particular the ocular nerve nuclei, as did the motor and mesencephalic trigeminal, facial, vestibular, ambiguus, dorsal vagal, solitary and hypoglossal nu- clei. The oculomotor, trochlear and abducens nerves showed moderate to severe degeneration. The substantia nigra and locus ceruleus showed gliosis and moderate loss of neurons. The superior colliculus and periaque- ductal grey matter were moderately degenerated. The brain stem reticular formation was atrophic with exten- sive loss of neurons and gliosis. The gracile and cuneate nuclei and the medial lemniscus were mildly to moderately degenerated. The dentate nucleus showed mild neuronal loss.

542
Table 1 Clinical features seen in sporadic cases of motor neuron disease presenting with severe or complete external ophthalmoplegia (/, not mentioned or not examined, c complete)
Akiyama Hayashi and Kato [2] Mizutani et al. Our cases et al. [1] [8, 9, 13]
Patient 1 Patient 2 Patient 3 Patient 1 Patient 2
Patient 1 Patient 2
Age (years)/sex 43/M 69/M From onset to respirator (months) 17 16 Development of upward gaze palsy (months) 33 40 Severe external ophthalmoplegia + +, c Sensory dysfunction + / Neurogenic bladder + / Bedsores + / CSF protein (mg/dl) / / Slow wave in EEG / + Autopsy + + Total clinical course (years) 5 10
69/M 58/M 38/M 38/M 61/M 73/M 12 8 11 36 5 5 33 12 20 72 24 11 + , C +, C + , C + , C + + , C
/ / + + + + / / + + + + / / + + + + / / 135 / 215 182 / + + + / + + / + + + +
5 / 5 13 2.5 7
The fastigeal nucleus showed almost complete loss of neurons, as did the anterior horn and intermediate zone of the spinal cord. Clarke's nucleus was severely degenerated. The poste- rior horn and intermediolateral nu- cleus were well preserved. Group "X" in the anterior horn at the level of the $2 segment of the spinal cord (Onufrowicz's nucleus) [11] showed mild degeneration. The anterior and lateral funiculi, including the corti- cospinal and spinocerebellar tracts, showed severe degeneration with gliosis and scattering of macro- phages. The posterior funiculus was moderately degenerated with macrophage infiltration. The anterior spinal nerve roots were severely de- generated, and the posterior spinal nerve roots moderately so. Severe neurogenic muscle atrophy was seen in the skeletal muscles. No Bunina or hyalin inclusion bodies were pre- sent in the brain.
Patient 2 was a 73-year-old man who became aware of being easily fatigued and progressive neck weak- ness in June 1985. Two months later, he experienced shortness of breath on exertion and developed difficulty in articulating and swallowing. Gag reflexes were absent. The upper limbs became weak. He was admit- ted to our hospital in October. He had lost 10 kg of weight since the onset of neurological symptoms.
During the neurological examination, he was alert and showed good orien- tation and cooperation. Fascicula- tions were present in the tongue, bi- ceps brachii and quadriceps femoris muscles. Distal dominant muscular atrophy and weakness were noted in the upper limbs. Tendon reflexes were diminished in radialis, but pre- sent in biceps and triceps, and nor- mal in knee and ankle. Hoffmann and Babinski signs were absent. Clonus at knee and ankle was not elicited. Superficial and deep sensa- tions were normal. His creatine ki- nase activities and blood sugar levels were normal. Serum antibody to GM1, GM2, GDla , GDlb , G T l b and G Q l b was negative. The CSF protein concentration was normal. There was no elevation of anti- HTLV-I antibody titres in the serum or CSF. His brain CT was normal. A motor nerve conduction study showed normal action potential am- plitudes, distal latencies and conduc- tion velocities with no evidence of conduction block or abnormal tem- poral dispersion. A sensory nerve conduction study was normal. EMG results suggested the presence of neuropathic changes in the tongue and all the extremities.
Weakness of the extremities and dyspnoea progressively worsened, and he became bedridden and depen- dent on a respirator 5 months after
the onset of neurological symptoms. Hypaesthesia and paraesthesias de- veloped in the left foot in December 1985. The oculocephalic reflex was present, but vertical gaze palsy de- veloped in May 1986 (12 months af- ter onset) and horizontal gaze palsy in December. By March 1987, the deep tendon reflexes and voluntary muscular contractions in the extremi- ties had disappeared. Eye position became fixed in November (30 months after onset), and the oculo- cephalic reflex disappeared in May 1988. He communicated by blinking for the next few months. Bedsores developed on the buttocks.
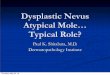
In April 1990, the CSF protein concentration was 182 mg/dl (IgG 28.3 mg/dl) with normal cellularity. Tl-weighted brain MRI showed atro- phy of the brain stem, predominantly of the tegmentum, and dilatation of the ventricular systems (Fig. 1). The frontotemporal lobes showed atro- phy. On T2-weighted images, there were extensive high-intensity areas in the cerebral white matter and the left cerebellar hemisphere. Cystome- try showed evidence of neurogenic bladder. EEG showed 6-7 Hz theta waves, mixed with 2-3 Hz delta waves in the background activity, and the auditory brain stem response had prolonged interpeak latencies from I-I I I . No compound muscle ac- tion potentials were elicited. The la-

543
Fig. 1A-E Tl-weighted MRI of patient 2 (4 years after onset of neurological symp- toms). A-D axial MR1 showing moderate atrophy of the brain stem and the fmn- totemporal lobes. E sagittal MRI shows the same findings
tencies of the somatosensory evoked potentials were prolonged peripher- ally and centrally. Sural nerve biopsy revealed severe nerve fibre loss, pre- dominantly for the large myelinated fibres. Neither inflammatory infil- trates nor onion bulbs were present. Clusters of small myelinated fibres were present.
The patient suffered recurrent episodes of acute pneumonia and uri- nary tract infection. Bedsores devel- oped on the left ankle in September 1991. His body temperature re- mained at 34°C during October. He died of complete atrioventricular block in November 1991. The total duration of this illness was 7 years. His family history was negative for MND.
The brain weighed 1395 g. Sev- eral old infarcts were found in the
cerebral cortex and left cerebellar hemisphere. There was diffuse loss of Purkinje cells, mainly in the supe- rior vennis. Many senile plaques and neurofibrillary tangles were present in the cerebral cortex. There was se- vere loss of Betz's cells in the pre- central gyri bilaterally. Neuronal loss of the frontal cortex was mild (Fig. 2). The globus pallidus and thalamus showed definite degeneration. The oculomotor nerves and nuclei were degenerated (Fig. 3), as were the fa- cial nerves and nuclei and the hypo- glossal nerves and nuclei. The sub- stantia nigra (Fig. 4) and superior colliculus had degenerated. The brain stem tegmentum showed marked at- rophy with degeneration of the retic- ular formation (Fig. 5). The dentate and fastigeal nuclei showed definite degeneration. In the spinal cord, the anterior horn and intermediate zone showed severe degeneration (Fig. 6). Clarke's nucleus, the intermediolat- eral nucleus and Onufrowicz's nu- cleus showed mild degeneration. The pyramidal tracts and anterior portion
of the lateral funiculi showed severe degeneration, as did the anterior spinal nerve. The posterior spinal nerve had mild degeneration. The sural nerve was severely degener- ated. The skeletal muscles showed severe neurogenic atrophy. No Bun- ina or hyalin inclusion bodies were present in the brain.
Because ocular movement is well preserved in patients with arny- otrophic lateral sclerosis (ALS) even in those supported by respirators for many years [3, 7, 10], the severe ex- ternal ophthalmoplegia that devel- oped on our patients is the most striking feature that differs from classic ALS. These patients did not show dementia, which is different from the clinical feature of the pa- tient reported by Komachi et al. [5]. Neither patient had a positive family history of MND. Several reports of sporadic cases of MND in which there was severe or complete exter- nal ophthalmoplegia without demen- tia have been reported (Table 1) [l, 2, 8, 9, 13]. The clinical features in

544
these cases are: (1) older onset (mean 56.1 years, range 38-73); (2) male predominance (males 7, female 1); (3) supranuclear ophthalmoplegia during the early stages of the disease (mean 30.6 months, range 11-72) with subsequent rapid deterioration, then complete fixation of the eye- balls; (4) bedsores, sensory dysfunc- tion and neurogenic bladder, which are not seen in classic ALS [14]; (5) slow wave abnormalities in EEGs and high CSF protein; and (6) severe atrophy of the brain stem tegmentum and frontotemporal lobes as revealed by MRI or CT [4]. These unique findings enable us to distinguish this entity clinically from classic ALS. Although Hayashi and Kato [2] used the term "totally locked-in state" for the complete external ophthalmople- gia seen in these patients, it is inade- quate because patients showed se- vere pathological changes in the reticular formation of the brain stem and abnormal EEG findings. In fact, patient 1 had difficulty communicat-
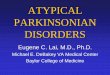
F i g . 3 0 c u l o m o t o r nerve showing moder- ate loss of myelinated fibres with en- doneurial fibrosis. Patient 2. Epoxy-em- bedded section. Toluidine blue and safra- nine stain. B a r = 30 gm
Fig.4 Substantia nigra showing moderate loss of neurons with gliosis. Patient 2. Haematoxylin and eosin stain. B a r =
100 gm
Fig. 2 Cerebral cortex in the superior frontal gyrus showing mild loss of neu- rons. Patient 2. Kliiver-Barrera stain. B a r =
300 btm
ing even though external ophthalmo- plegia was not complete.
Neuropathological studies of our patients revealed widespread degen- erative changes in the central and pe- ripheral nervous system regions: in the upper and lower motor neuron systems, oculomotor nerve nuclei, reticular formation, spinocerebellar tract, somatic sensory nerves, globus pallidus, subthalamic nucleus, den- tate nucleus, substantia nigra, locus ceruleus and Onufrowicz's nucleus. Patients with sporadic MND who have severe or complete external ophthalmoplegia show similar patho- logical changes [1, 2, 8, 9, 13]. In contrast, the patient reported by
Komachi et al. [5], who had ophthal- moplegia and dementia, showed changes in the motor neuron sys- tems, oculomotor nucleus, substantia nigra, red nucleus and frontal cortex. Long-term respiratory support is considered to produce the negative signs of ALS such as severe ophthal- moplegia, bedsores, sensory dysfunc- tion and vesicorectal disturbances, and these patients have been diag- nosed as having ALS [1, 2, 8, 9, 13]. Yoshida et al. [15], however, report- ed autopsy findings of two patients with ALS whose course of illness lasted 10 years. These patients had been placed on ventilators 27 and 32 months after the onset of neurologi-

545
cal symptoms , and both showed nor- mal external ocular movement , nor- mal pe lv ic sphincter function, nor- mal sensory funct ion and no bed- sores during the 10 years. Pa thologi - cal changes were res t r ic ted to the cor t icospina l tract and the upper and lower motor neurons. In contrast , the total c l in ical course in our pat ient 1 was only 2.5 years , and he had wide- spread pa tho log ica l lesions in addi- t ion to those o f the motor neuron systems. Ex tens ive neuro log ica l in- vo lvement , such as that seen in our patient, therefore cannot s imply be the consequence of p ro longed sur- v ival due to vent i la tory assistance.
Pat ients with A L S rare ly have C S F prote in concent ra t ion above 100 mg/dl [ 16]. The marked e levat ion o f C S F prote in in our pat ients suggests under ly ing in f l ammato ry disorders . Ret rovi rus infect ion has been postu- lated as the ae t io logy o f A L S [12]. Kuroda and Sugihara [6] repor ted on an HTLV-I- infec ted pat ient with A L S - l i k e manifes ta t ions . The au- topsy f indings for that pat ient were s imi lar to those of our patients , ex- cept for the th ickness o f the lep- tomeninges and in f l ammatory cell infi l t rat ion. Our pat ients had no anti- HTLV-I an t ibody titres, but the pos- s ibi l i ty o f pers is tent infect ion (such as an unde te rmined retrovirus infec- tion) could not be excluded. We con- c lude that the synd rome d iscussed here (a typica l M N D with ophtha lmo- plegia) should be r ecogn ized as a subtype o f MND.
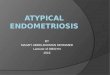
Fig.S Medulla oblongata showing severe atrophy of the reticular formation and pyr- amid. Patient 2. The inferior olivary nu- cleus is preserved. Klaver-Barrera stain, x 5
Fig. 6 Spinal cord (C4) showing severe degeneration and atrophy of the anterior horn and intermediate grey matter. Patient 2. The anterior and lateral funiculi also are severely degenerated. Kltiver-Barrera stain, × 7
References
1. Akiyama K, Tsutsumi Y, Onoda N, Ogawa K, Saito H, Yoshii H, Shino- hara Y (1987) An autopsy case of amyotrophic lateral sclerosis associated with sensory disturbance and eye movement disorder: pathological con- sideration on development of multisys- tern degeneration of the nervous sys- tem in a patient with prolonged sur- vival (in Japanese with English ab- stract). Byori To Rinsho 5 : 921-028
2. Hayashi H, Kato S (1989) Total mani- festations of amyotrophic lateral scle- rosis: ALS in the totally locked-in state. J Neurol Sci 93 : 19-35
3. Hayashi H, Kato S, Kawada A (1991) Amyotrophic lateral sclerosis patients living beyond respiratory failure. J Neurol Sci 105 : 73-78
4.Kato S, Hayashi H, Yagishita A (1993) Involvement of the frontotemporal lobe and limbic system in amyotrophic lat- eral sclerosis as assessed by serial computed tomography and magnetic resonance imaging. J Neurol Sci 116: 52-58
5. Komachi H, Okeda R, Ishii N, Yanagi- sawa K, Yamada M, Miyatake T (1994) Motor neuron disease with de- mentia and ophthalmoplegia: a clinical and pathological study. J Neurol 241 : 592-596
6. Kuroda Y, Sugihara H (1991) Autopsy report of HTLV-I-associated myelopa- thy presenting with ALS-like manifes- tations. J Neurol Sci 106:199-205
7. Marti-Fabregas J, Roig C (1993) Ocu- lomotor abnormalities in motor neuron disease. J Neurol 240:475-478
8. Mizutani T, Aki N, Shiozawa R, Un- akami M, Nozawa T, Yajima K, Tan- abe H, Hara M (1990) Development of ophthalmoplegia in amyotrophic lateral sclerosis during long-term use of respi- rators. J Neurol Sci 99 : 311-319

546
9. Mizutani T, Sakamaki S, Tsuchiya N, Kamei S, Kohzu H, Horiuchi R, Ida M, Shiozawa R, Takasu T (1992) Amy- otrophic lateral sclerosis with ophthal- moplegia and multisystem degeneration in patients on long-term use of respira- tors. Acta Neuropathol 84 : 372-377
10. Okamoto K, Hirai S, Amari M, Iizuka T, Watanabe M, Murakami N, Takatama M (1993) Oculomotor nu- clear pathology in amyotrophic lateral sclerosis. Acta Neuropathol (Berl) 85 : 458--462
11. Onufrowicz B (1900) On the arrange- ment and function of the cell groups of sacral region of the spinal cord in man. Arch Neurol Psychopathol 3 : 387-412
12. Rowland LP (1991) Ten central themes in a decade of ALS Research. Adv Neurol 56 : 3-23
13. Takasu T, Mizutani T, Sakamaki S, Tsuchiya N, Kamei S, Kohzu H (1985) An autopsy case of sporadic amy- otrophic lateral sclerosis with degener- ations of the spinocerebellar tracts and the posterior column (in Japanese with English abstract). Annual Report of the Neurodegenerative Disease Research Committee of Japan, Tokyo, pp 94-100
14. Toyokura A (1979) Negative features in ALS. In: Japanese Medical Research Foundation (ed) Amyotrophic lateral sclerosis. University of Tokyo Press, Tokyo, pp 53-58
15. Yoshida M, Murakami N, Hashizume Y, Itoh E, Takahashi A (1992) A clini- copathological study of two respirator- aided long-survial cases of amy- otrophic lateral sclerosis (in Japanese with English abstract). Clin Neurol (Tokyo) 32 : 259-265
16. Younger DS, Rowland LP, Latov N, Sherman W, Pesce M, Lange DJ, Tro- jaborg W, Miller JR, Loveralse RE, Hays AP, Kim TS (1990) Motor neu- ron disease and amyotrophic lateral sclerosis: relation of high CSF protein content to paraproteinemia and clinical syndromes. Neurology 40 : 595-599
N. Yuki • T. Yuasa • K. Kaneko T. Inuzuka • M. Arai • S. Sato • S. Tsuji T. Miyatake Department of Neurology, Brain Research Institute, Niigata University, Niigata, Japan
M. Yamada • S. Takeda - K. Kawasaki F. Ikuta Department of Pathology, Brain Research Institute, Niigata University, Niigata, Japan
K. Oyanagi Center for Materials of Brain Diseases, Brain Research Institute, Niigata University, Niigata, Japan
N. Yuki (I~) Department of Biochemistry, Tokyo Medical and Dental University, 1-5-45 Yushima, Bunkyo-ku, 113 Tokyo, Japan