Embed Size (px)
Citation preview

Attenuation of the Ventilatory and Heart Rate Responses
to Hypoxia and Hypercapnia with Aging in Normal MenRICHARDS. KRONENBERGand CHAuLEs W. DRAGE
From the Department of Medicine, University of Minnesota Hospitals,Minneapolis, Minnesota 55455
A B S T R A C T The response of ventilation and ofheart rate to hypoxia and hypercapnia was determinedin eight young normal men age 22-30 yr and eight elderlymen age 64-73. The elderly men were selected and care-fully screened to eliminate the possibility of cardiopul-monary disease. All the subjects were born at low alti-tude and had no significant prior exposure to hypoxia.The ventilatory response to hypoxia was measured asthe exponential slope constant, k, of regression lines re-lating the logarithm of incremental ventilation to PAo,during isocapnic progressive hypoxia. The heart rateresponse to hypoxia was measured as the percentagechange in heart rate between PAO2= 100 and PAO2= 40mmHg. The ventilatory response to hypercapnia wasmeasured as the slope of regression lines relating ven-tilation to PACO2 during rebreathing with PAO2> 200mmHg. The heart rate response to hypercapnia wasmeasured as the percentage change in heart rate betweencontrol values at the start of the rebreathing test andPACO2=55 mmHg.
The ventilatory and heart rate responses to both hy-poxia and hypercapnia were significantly decreased inthe elderly men as compared to the young men. Hypoxicventilatory drive was decreased by 51±6% (mean+-SEM; P< 0.001) and hypercapnic drive by 41±7%(P < 0.025). The percentage change in heart rate pro-duced by hypoxia was 34±5% (mean +SEM) in theyoung normals and 12±2% in the old normals (P <0.005). Similar figures for heart rate in response to hy-percapnia were 15±3% and - 1±1% for the young andold normal groups (P < 0.001).
Weconclude that ventilatory and heart rate responsesto hypoxia and hypercapnia diminish with age. Thesealterations in both ventilatory and circulatory controlscould make older individuals more vulnerable to hypoxicdisease states.
This paper was presented in part at the Central Societyfor Clinical Research Meeting, November 1972, Chicago, Ill.
Received for publication 29 September 1972 and in revisedform 3 April 1973.
INTRODUCTION
Within a group of normal subjects, there may be con-siderable variation in the ventilatory response to hy-poxia and hypercapnia (1, 2). The reasons for this vari-ation are unclear, but two important factors that appearto reduce the ventilatory response to hypercapnia andgreatly diminish or abolish the response to hypoxia, areprolonged exposure to hypoxia (3) and athletic physicalconditioning (4). This report will present evidence thata third factor, increasing age, can also attenuate hypoxicand hypercapnic ventilatory drive.
METHODS
Sutbjects. The old normal subjects were selected volun-teers from a larger group of elderly normal men partici-pating in a long term epidemiological study on heart disease(5). In connection with this epidemiological study, theyhave been followed with periodic history questionnaires,physical examinations, chest X rays, electrocardiograms,and the pulmonary function tests listed in Table I. Noneof the old normal subjects had ever smoked cigarettes.Criteria for subject selection were no evidence for heartdisease or cerebrovascular disease and birth at or near sealevel with no previous sojourns at high altitude for over 2mo in any 1 yr. Thus the old normal men in this studyconstitute a select subject group free of significant heart,lung, and vascular disease and with no significant priorexposure to hypoxia.
The young normal control subjects were male collegestudents who had no previous experience with respiratorystudies, who had not spent over 2 mo at high altitude, andwho were not using drugs. Hypoxic ventilatory responsedata on the control subjects has been previously reported(6).
Hypoxic response. A detailed description of the methodused in these studies has been reported elsewhere (6). Thesubject breathed through a respiratory valve (Lloyd) into acircle with a variable C02 absorber bypass rebreathing sys-tem. CO2 was continuously sampled by an infrared C02analyzer (Beckman LB-1; Beckman Instruments, Inc.,Fullerton, Calif.). End-tidal 02 was automatically sampledfrom beyond the expiratory valve using the method describedby Severinghaus and Hamilton (10). Differences betweenalveolar Po2 obtained by this method and arterial Po2 wereless than 4 mmHg when PAo, = 40 mmHg in the young
The Journal of Clinical Investigation Volume 52 August 1973*1812-18191812

normal subjects. Arterial blood samples were not obtainedfrom the old normal men. Various gas mixtures (N2, 02,C02) were added via flow meters to ports in the circuitfor control of desired gas tensions. A suction flow meterpermitted this addition of gases without changing thevolume of the system. Heart rate was recorded from ECGelectrodes applied to the chest. Ventilation was transducedby a potentiometer coupled to a 13.5 1 spirometer (WarrenE. Collins, Inc., Braintree, Mass.) within the circle re-breathing system. All variables were recorded on a poly-graph recorder (Grass Model 7, Grass Instrument Co.,Quincy, Mass., or a Gilson MSP, Gilson Medical Elec-tronics, Inc., Middleton, Wisc.). Alveolar Po2 was held at120 mmHg for 2 min before beginning the hypoxic re-sponse tests in order to determine each subject's restingPAC02. PAo2 was then lowered from 120 to 40 mmHg overa period of 4-5 min. The induction of hypoxia in this studywas somewhat more rapid than that employed by otherinvestigators (11). We have found that there is no differ-ence in results obtained by this method and slower ones (6).Byrne-Quinn, Sodal, and Weil, using the same isocapnicprogressive hypoxia technique but a different method ofdata analysis, also found no difference in results whenlowering PAo, over 5 min as compared with 15 min (12).With practice, the variable CO absorber bypass could beadjusted to hold PAco2 within 1 mmHg of the previouslydetermined resting level. It was occasionally necessary toadd CO2 to the circuit to achieve this degree of PAco2 con-trol. Two isocapnic hypoxic response tests were done ineach subject with an intervening rest period.
Ventilation in the hypoxic response tests was measuredby averaging inspiratory volume over a minimum of fivebreaths at approximately each 10 mmHg fall in PAos. Therelationship of ventilation to Po2 at a constant Pco2 hasbeen described as hyperbolic (11). Previously reportedwork using this technique, however, demonstrated that thelogarithm of incremental ventilation is approximately alinear function of Po, (6). Incremental ventilation is deter-mined by subtracting from all ventilation measurements theirnon-hypoxic component. The figure used to represent thisnon-hypoxic component was 85% of the ventilation at PAo2= 100 mmHg. This constant is based on calculations madeby Severinghaus, Bainton, and Carcelen in high altitudenatives showing that about 15%7o of the resting ventilatorydrive at Po%= 100 mmHg is provided by the peripheralchemoreceptors (13). This figure was confirmed by Wade,Larson, Hickey, Ehrenfeld, and Severinghaus in a study ofpatients with denervated peripheral chemoreceptors (14).Using this method of analysis, the relationship betweenventilation and Po2 at constant Pco2 can be expressed by theequation
;AVI = AVoe(P2/k)
where AVo is the ventilation intercept at Po. = 0 and kis the decrement in Po2 required to increase ventilation bya factor of e(2.718). Thus a small value for k indicatesa large hypoxic ventilatory drive. Constants for the equa-tion were determined by the linear regression of In (Vi- 0.85 Vis) on Poe. At least 12 points were used in eachregression analysis. These data were tested for fit of anexponential distribution with the Komolgorov-Smirnov testfor the distribution of points around a curve (15). Thistest indicated that the actual data points correlated sig-nificantly with the distribution described by the calculatedregression line.
TABLE IResults of Pulmonary Function Testing in the
Old Normal Men
TotalVital lung FEVI.os/
Subject capacity capacity* FEV..os FVC DLcoSB
ml ml ml % ml/minX mmHg-
H. C. 4,549 7,520 3,000 69 24(I 10)t (I 10) (100) (104)
A. N. 4,149 6,786 3,275 75 24(98) (103) (101) (111)
L. C. 3,918 6,334 2,800 75 19(97) (100) (97) (97)
W. K. 3,651 5,831 2,175 68 17(91) (92) (75) (75)
E. M. 3,652 6,123 2,150 71 17(84) (77) (67) (62)
L. M. C. 4,867 7,540 2,825 66 28(114) (113) (92) (135)
J. H. 4,619 7,952 2,750 57 20(111) (121) (93) (97)
W. L. 2,400 4,320 1,950 83 19(65) (73) (74) (97)
Mean 3,976 6,551 2,616 71 21-A--SEM 276 415 165 3 1.4
FEVi.os, forced expiratory volume in 1.0 s; FVC, forced vital capacity;DL.,OSB, single breath carbon monoxide diffusing capacity.* Total lung capacity was calculated from functional residual capacitymeasured by open circuit N2 washout.t Numbers in parenthesis indicate percent of predicted value obtainedfrom references 7-9.
Heart rate in the hypoxic response test was measuredby comparing actual rates and percentage change betweencontrol heart rates at Po2 = 100 mmHg and heart rates atPo2 = 40 mmHg.
CO. response. The ventilatory response to hypercapniawas determined by the rebreathing method described byRead (16). A 6 liter bag in a bottle was arranged so thatthe subject could rebreathe from the main circuit or backin forth into the bag. The rebreathing bag was prefilledwith 5% CO in 02. Each subject rebreathed from thebag for 4 min or until PAco-, = 65 mmHg. Two rebreathingtests were done with an intervening rest period. PAO2 re-mained over 200 mmHg throughout the rebreathing period.
Ventilation in the hypercapnic response test was measuredby averaging inspiratory volume over 30-s intervals afterdiscarding the first 30 s of the test. Thus approximately 14points were obtained for analysis on each subject. The re-lationship relating ventilation to Pco2 is VI = S(PACo2-B)where B is the extrapolated PAco, at Vi = O (intercept onthe abscissa or PACo2 axis) and S is the slope of the CO2response line (liter/min X mmHg-') (17). Constants forthis equation were obtained by the linear regression ofVi on PAcO2-
Analysis of the heart rate response to hypercapnia wasidentical to that done for hypoxia. Percentage change andactual rate differences were calculated between control heartrates immediately after the start of rebreathing and heartrates at PACO! = 55 mmHg.
Group comparisons for all of the data were made withan unpaired t test.
Attenuation of Chemoreceptor Function with Age 1813
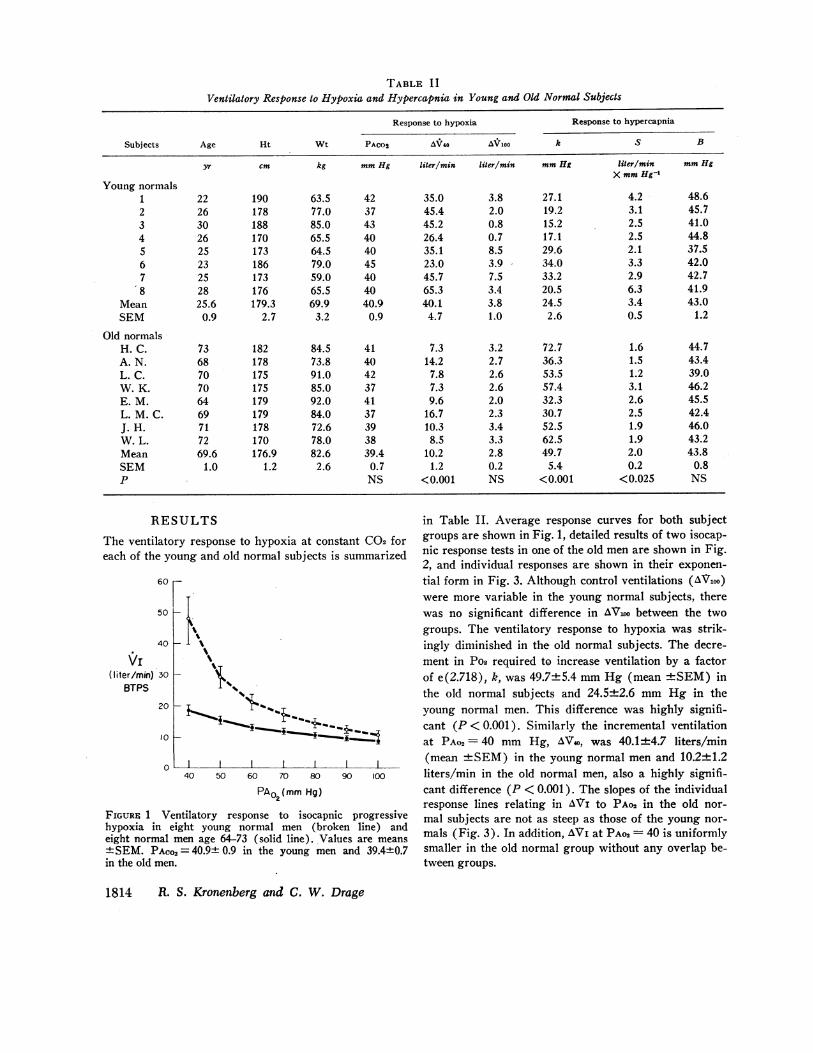
TABLE IIVentilatory Response to Hypoxia and Hypercapnia in Young and Old Normal Subjects
Response to hypoxia Response to hypercapnia
Subjects Age Ht Wt PACO2 AVo4 A/Vloo k S B
yr cm kg mmHg liter/min liter/min mmHg liter/min mmHgX mmHg-1
Young normals12345678
MeanSEM
Old normalsH. C.A. N.L. C.W. K.E. M.L. M. C.J. H.W. L.MeanSEMp
63.577.085.065.564.579.059.065.569.9
3.2
84.573.891.085.092.084.072.678.082.6
2.6
423743404045404040.9
0.9
414042374137393839.4
0.7NS
35.045.445.226.435.123.045.765.340.1
4.7
7.314.2
7.87.39.6
16.710.3
8.510.2
1.2<0.001
3.8 27.12.0 19.20.8 15.20.7 17.18.5 29.63.9 - 34.07.5 33.23.4 20.53.8 24.51.0 2.6
3.2 72.72.7 36.32.6 53.52.6 57.42.0 32.32.3 30.73.4 52.53.3 62.52.8 49.70.2 5.4NS <0.001
4.2 48.63.1 45.72.5 41.02.5 44.82.1 37.53.3 42.02.9 42.76.3 41.93.4 43.00.5 1.2
1.61.51.23.12.62.51.91.92.00.2
<0.025
44.743.439.046.245.542.446.043.243.8
0.8NS
RE;'The ventilateeach of the ye
60
50
40
20
10
0
FIGURE 1 Vihypoxia in c
eight normal+ SEM. PACcin the old mer
SULTS in Table II. Average response curves for both subject
ry response to hypoxia at constant C02 for groups are shown in Fig. 1, detailed results of two isocap-oung and old normal subjects is summarized nic response tests in one of the old men are shown in Fig.
2, and individual responses are shown in their exponen-tial form in Fig. 3. Although control ventilations (AVioo)were more variable in the young normal subjects, therewas no significant difference in AV100 between the twogroups. The ventilatory response to hypoxia was strik-ingly diminished in the old normal subjects. The decre-ment in Pos required to increase ventilation by a factorof e(2.718), k, was 49.7±5.4 mmHg (mean +SEM) inthe old normal subjects and 24.5±2.6 mmHg in theyoung normal men. This difference was highly signifi-cant (P < 0.001). Similarly the incremental ventilationat PAO2= 40 mmHg, AV4o, was 40.1±4.7 liters/min
t I I (mean +SEM) in the young normal men and 10.2±1.240 50 60 70 80 90 100 liters/min in the old normal men, also a highly signifi-
PAO2(mmHg) cant difference (P < 0.001). The slopes of the individualresponse lines relating in AVi to PAo2 in the old nor-
entilatory response to isocapnic progressive mal subjects are not as steep as those of the young nor-eight young normal men (broken line) andmen age 64-73 (solid line). Values are means mals (Fig. 3). In addition, AVi at PAo2= 40 is uniformlyD2= 40.9± 0.9 in the young men and 39.4±0.7 smaller in the old normal group without any overlap be-I.. tween groups.
1814 R. S. Kronenberg and C. W. Drage
222630262523252825.6
0.9
736870706469717269.6
1.0
190178188170173186173176179.3
2.7
182178175175179179178170176.9
1.2
VI(liter/min)
BTPS30
30 30 F-
25
20 h
VI(liter/min) 15
BTPS
10
5
0
20
xx x
x
xx x
AV, =
VI -0.85Vio0(liter/min )
BTPSx K xx
87654
3
2
40 50 60 70 80 90 100 110
PA02(mmHg)
7KK
X\
_ \x
Xx X
X
K
40 50 60 70 80 90 100 110
PA02(mmHg)
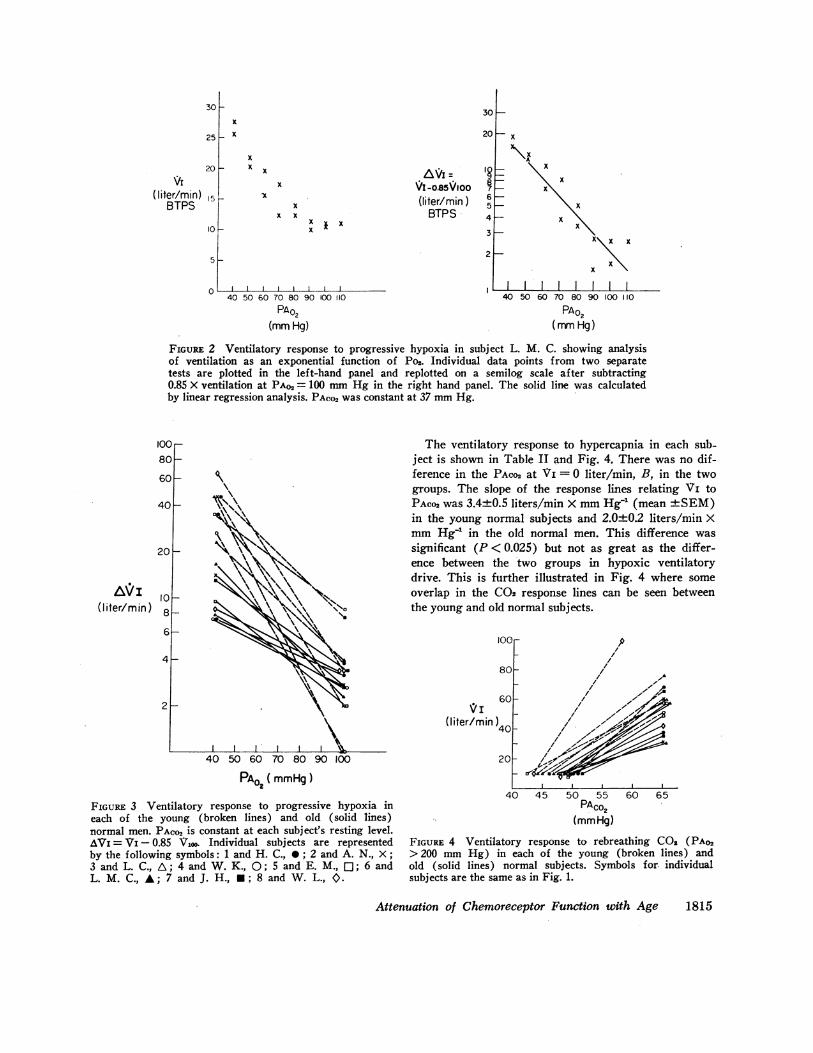
FiGuRE 2 Ventilatory response to progressive hypoxia in subject L. M. C. showing analysisof ventilation as an exponential function of Po2. Individual data points from two separatetests are plotted in the left-hand panel and replotted on a semilog scale after subtracting0.85 X ventilation at PAo, = 100 mmHg in the right hand panel. The solid line was calculatedby linear regression analysis. PAco2 was constant at 37 mmHg.
The ventilatory response to hypercapnia in each sub-ject is shown in Table II and Fig. 4. There was no dif-ference in the PAco2 at Vi = 0 liter/min, B, in the twogroups. The slope of the response lines relating Vi toPACo2 was 3.4±0.5 liters/min X mmHg' (mean +SEM)in the young normal subjects and 2.0±0.2 liters/min XmmHg1 in the old normal men. This difference wassignificant (P < 0.025) but not as great as the differ-ence between the two groups in hypoxic ventilatorydrive. This is further illustrated in Fig. 4 where someoverlap in the C02 response lines can be seen betweenthe young and old normal subjects.
loor
80-
50 60 70 80 90
PA02 (mmHg)
FIGURE 3 Ventilatory response to progressive hypoxia ineach of the young (broken lines) and old (solid lines)normal men. PAco2 is constant at each subject's resting level.AVi = VI - 0.85 ViOO. Individual subjects are representedby the following symbols: 1 and H. C., 0; 2 and A. N., X;3 and L. C., A; 4 and W. K., 0; 5 and E. M., 1:; 6 andL. M. C., A; 7 and J. H., *; 8 and W. L., O.
60V;I
(liter/min) 40
20
lp
/
1A
// --I./ --a-,.1
/1/0.
/~.
40 45 50 55 60PACO2
(mmHg)
65
FIGURE 4 Ventilatory response to rebreathing COs (PAo2> 200 mmHg) in each of the young (broken lines) andold (solid lines) normal subjects. Symbols for. individualsubjects are the same as in Fig. 1.
Attenuation of Chemoreceptor Function with Age
)
)
)
IO(8C
6C
4C
20
(l iter/m)in)108
6
4
2
1815
TABLE I I IHeart Rate Response to Hypoxia and Hypercapnia in Young and Old Normal Subjects
Response to hypoxia Response to hypercapnia
PAO2 Percent PACO2 PercentSubjects Control = 40 mmHg change Control = 55 mmHg change
per min per min % per min per min %Young normals
1 105 156 47 79 91 152 101 160 58 84 100 193 97 125 29 90 98 94 92 106 15 90 98 95 83 102 23 100 117 176 99 142 30 66 68 37 92 115 25 96 124 298 103 150 46 84 100 19
Mean 96.5 132.0 34.1 86.1 99.5 15.0SEM 2.5 8.1 5.2 3.7 5.9 2.8
Old normalsH. C. 68 81 16 65 66 2A.N. 72 84 17 68 66 -3L. C. 66 68 3 63 60 -5W. K. 69 78 13 67 69 3E. M. 69 81 17 69 69 0L. M. C. 90 104 15 84 84 0J.H. 91 100 10 71 68 -4W. L. 95 96 1 90 90 0Mean 77.5 86.5 11.5 72.1 71.5 -0.9SEM 4.3 4.4 2.2 3.4 3.6 1.0P <0.005 <0.001 <0.005 <0.025 <0.005 <0.001
The heart rate response to hypoxia and hypercapniais shown in Table III. In both instances the control heartrates were significantly higher (P < 0.005 for hypoxiaand < 0.025 for hypercapnia) in the young normal sub-jects. Hypoxia (PAO2= 40 mmHg) produced a heartrate of 132±8/min (mean +SEM) in the young nor-mal men and 87±4/min in the old normal subjects,a highly significant difference (P < 0.001). The per-centage increase in heart rate due to hypoxia was34+5% in the young normals and 12±2% in the oldnormals (P < 0.001). The percentage increase in heartrate between control at the start of the rebreathing testand PACo2= 55 mmHg was 15±3% (mean +SEM) inthe young normal men. In contrast to this modest in-crease in the young normals, hypercapnia produced nochange in the heart rate of the old normal men. In factthe average response was a decrease of 1 +±1 % (mean+SEM) in the old normal group. The difference betweengroups both in actual rate and percentage change dueto hypercapnia were highly significant (P < 0.005 foractual rate and P < 0.001 for percentage change).
DISCUSSIONThe data presented in this study indicate that hypoxicand hypercapnic ventilatory drive diminishes with in-
creasing age. Since this observation is new, it is neces-sary to consider the possibility that it was producedartifactually by the testing methods, data analysis, or sub-ject selection.
The use of progressive hypoxia at constant Pco2 as atechnique for determining the ventilatory response tohypoxia was described by Loeschcke and Gertz (18).More recently, Weil et al. used a slightly longer versionof this technique than that used in this study in 10 youngnormal men (11). They calculated an average AV740 inthis group of 17.0±1.5 (mean ±SEM) liters/min Xm-' BTPS, a value very similar to the 21.5±2.7 liters/min X m-2 in our young normal subjects. (Note the cor-rection for body surface area.) Several methods for ana-lyzing the relationship between ventilation and Po2 aredescribed in the literature. These include the hyperbolicshape parameter of Weil et al. (11) and the AV40 indexof Severinghaus et al. (13). Calculation of the ventila-tory response to hypoxia in our subjects using either ofthese indices does not alter the difference between theyoung and old normal groups. The high oxygen re-breathing CO2 response test is a well accepted techniqueused both in normal subjects (16) and patients (19).The average slope in our young normal men of 3.4±0.5,
1816 R. S. Kronenberg and C. W. Drage

(mean ±SEM) compares closely with that obtainedby Read of 2.7±0.3 in 21 normal subjects of unspecifiedage (16). Recently Patrick and Howard found that theslope of the line relating ventilation to tidal volume dur-ing hyperoxic rebreathing C02 response was inverselyrelated to age (20). The slope of the response line re-lating ventilation to PACo2 was also decreased in theirolder as compared with their younger subjects, but thedifference was not significant. Further comparison be-tween this study and ours is difficult because their oldersubjects were only 44±5 yr (mean +SD). Although noinformation is available on how transient tests of hy-poxic and hypercapnic ventilatory response compare withsteady-state methods in older subjects, it appears un-likely that testing methods or analytical techniques canaccount for the response differences in young and oldsubject groups. Since arterial blood samples were notobtained in the old normal men, it is not possible to quan-titate the exact humoral stimulus to the chemoreceptorsin the two subject groups. Mellengaard (21) and Raineand Bishop (22) found that alveolar to arterial oxygendifference increased with age. Since all the subjects wereexposed to an alveolar Po2 of 40 mmHg, it is likely thatthe old normal men received a greater humoral stimulusthan the young men during the hypoxic response testsand that our data actually underestimates the extent thathypoxic ventilatory drive diminishes with age.
There remains the possibility that other factors unre-lated to chemoreceptor function were operating in theold normal subjects. Several alterations in pulmonarymechanics are known to occur with increasing age.Among these changes are loss of elastic recoil and a de-crease in vital capacity with an increase in residual vol-ume and no change in total lung capacity (23-25).Brodovsky, MacDonell, and Cherniack (26) and Milic-Emili and Tyler (27) have found that mechanical workis a more accurate gauge of the respiratory response toCO than ventilation. Although alterations in mechani-cal lung function may account for some of the diminishedventilatory response to hypoxia and C02 seen in the oldnormal men, it seems unlikely that they can entirely ex-plain their marked attenuation in chemoreceptor func-tion. The old normal subject group was carefullyscreened to be free of detectable heart and lung disease.In addition, the maximum ventilations reached by theold normal subjects are generally considerably less thantheir expected maximum breathing capacity calculatedby multiplying their FEV1 X 30 (28). Thus the conclu-sion remains that age in some way directly attenuateschemoreceptor function.
Although there are isolated normal individuals with noventilatory response to hypoxia (1, 6), the only condi-tions previously reported to be associated with attenua-tion of chemoreceptor function are hypoxia from birth
(29-32), prolonged exposure to hypoxia in adulthood,(3, 33) and athletic physical conditioning (4). Byrne-Quinn, Weil, Sodal, Filley, and Grover found that hy-poxic ventilatory drive was reduced by 65% and hyper-capnic drive by 53% in 13 athletes studied at rest ascompared with non-athlete controls (4). Weil, Byrne-Quinn, Sodal, Filley, and Grover found comparable re-ductions of 57% for hypoxic drive and 35% for hyper-capnic drive in 10 long-term non-native residents ofLeadville, Colo. (3,100 m) when compared with nativesof Denver, Colo. (1,600 m) (3). Hypoxic ventilatorydrive was reduced by an average of 51 %and hypercapnicdrive by an average of 41 % in the old normal men ofthis study. The pattern of attenuation of chemoreceptorfunction is reasonably similar in all three of these situa-tions and suggests the possibility that some of the fac-tors responsible for the loss of hypoxic and hypercapnicventilatory drive lie within the peripheral chemorecep-tors themselves or in the integrating pathways for theperipheral chemoreceptor impulses within the centralnervous system. This premise is based on the assumptionthat the peripheral chemoreceptors account for about halfof the hypercapnic drive in man (34), and the findingsof Sorensen and Cruz (35) and Lefrancois et al. (36)that high altitude natives have a decreased response torapid step increases in C02. Although the precise defectin the pathway of the peripheral chemoreceptor impulsescannot be determined by this or the other studies cited,it is apparent that virtually all of the peripheral chemo-receptor contribution to hypercapnic ventilatory drive islost while considerable hypoxic ventilatory drive is re-tained. This implies either a highly selective effect ofage on the peripheral chemoreceptors or, more likely,that alterations in peripheral chemoreceptor functionmay be one of multiple factors responsible for diminishedhypoxic and hypercapnic ventilatory drive in our oldnormal subjects.
Wade et al. found that hypoxia at constant PACO2 in-creased systolic blood pressure before and decreased itafter bilateral carotid body denervation in four patientsundergoing bilateral carotid endarterectomy (14). Thesefindings were later confirmed by Lugliani, Whipp, andWasserman in eight asthmatics with bilateral carotidbody resection (37). Lugliani et al. also found that thetachycardia of hypoxia was not affected by carotid bodyresection. Both Wade et al. (14) and Lugliani, Whipp,Seard, and Wasserman (38) report intact baroreceptorfunction after chemoreceptor denervation in their sub-jects. It is possible that the diminished heart rate re-sponse to hypoxia in the old normal men indicates a lossof both baroreceptor and chemoreceptor function withage.
The precise mechanism for the attenuation of the ven-tilatory and heart rate response to hypoxia and hyper-
Attenuation of Chemoreceptor Function with Age 1817
capnia with aging cannot be elicited from this study.It is likely that multiple factors such as chemoreceptorfunction, baroreceptor function, and possibly the sym-pathetic nervous system may all play a role. Regardlessof the mechanism involved, the finding that the ventila-tory and heart rate responses to hypoxia and hyper-capnia diminish with increasing age is of considerableclinical importance. First, it exposes one more variablethat must be considered in the regulation of respirationin patients or normal individuals particularly if they arealso exposed to chronic hypoxia. Secondly, it suggeststhat the process of aging is associated with the loss ofthis potentially important protective mechanism. Thus,the patient population most often exposed to hypoxicdisease states is also least able to respond to this threat.Further, the usual diagnostic clues indicating the onsetof hypoxia may be absent. Hypoxia in the elderly pa-tient might not be signaled by either respiratory distressor tachycardia.
ACKNOWLEDGMENTS
The authors thank Mrs. Elizabeth Dugan for her technicalassistance and Doctors Henry L. Taylor and Henry Black-burn for obtaining the elderly normal subj ects. This workwas supported by grants RO1-HL-13714 and HL0499712from the National Heart and Lung Institute and a grantfrom the Minnesota Respiratory Health Association.
REFERENCES
1. Dripps, R. D., and J. H. Comroe, Jr. 1947. The effectof the inhalation of high and low oxygen concentra-tions on respiration, pulse rate, ballistocardiogram andarterial oxygen saturation (oximeter) of normal in-dividuals. Am. J. Physiol. 149: 277.
2. Kronenberg, R. S., and J. W. Severinghaus. 1971. Chem-ical control of ventilation: man. In Handbook of Respi-ration and Circulation. P. L. Altman and D. S. Dittmer,editors. Federation of American Societies for Ex-perimental Biology. Bethesda, Md. 102.
3. Weil, J. V., E. Byrne-Quinn, I. E. Sodal, G. F. Filley,and R. F. Grover. 1971. Acquired attenuation of chemo-receptor function in chronically hypoxic man at altitude.J. Clin. Invest. 50: 186.
4. Byrne-Quinn, E., J. V. Weil, I. E. Sodal, G. F. Filley,and R. F. Grover. 1971. Ventilatory control in the ath-lete. J. Appl. Physiol. 30: 91.
5. Keys, A., H. L. Taylor, H. Blackburn, J. Brozek, J. T.Anderson, and E. Simonsen. 1963. Coronary heart dis-ease among Minnesota business and professional menfollowed 15 years. Circulation. 28: 381.
6. Kronenberg, R., F. N. Hamilton, R. Gabel, R. Hickey,D. J. C. Read, and J. W. Severinghaus. 1972. Com-parison of three methods for quantitating respiratoryresponse to hypoxia in man. Resp. Physiol. 16: 109.
7. Boren, H. G., R. C. Kory, and J. C. Syner. 1966. TheVeterans Administration-Army cooperative study ofpulmonary function: II. The lung volume and its sub-divisions in normal men. Am. J. Med. 41: 96.
8. Kory, R. C., R. Callahan, H. G. Boren, and J. C. Syner.1961. The Veterans Administration-Army cooperative
study of pulmonary function: I. Clinical spirometry innormal men. Am. J. Med. 30: 243.
9. Teculescu, D. B., and D. C. Stanescu. 1970. Lung dif-fusing capacity. Normal values in male smokers andnon-smokers using the breath-holding technique. Scand.J. Resp. Dis. 51: 137;
10. Severinghaus, J. W., and F. N. Hamilton. 1970. End-tidal gas sampler. J. Appl. Physiol. 28: 244.
11. Weil, J. V., E. Byrne-Quinn, I. E. Sodal, W. 0. Frie-sen, B. Underhill, G. F. Filley, and R. F. Grover. 1970.Hypoxic ventilatory drive in normal man. J. Clin. In-vest. 49: 1061.
12. Byrne-Quinn, E., I. E. Sodal, and J. V. Weil. 1972. Hy-poxic and hypercapnic ventilatory drives in childrennative to high altitude. J. Appl. Physiol. 32: 44.
13. Severinghaus, J. W., C. R. Bainton, and A. Carcelen.1966. Respiratory insensitivity to hypoxia in chronicallyhypoxic man. Resp. Physiol. 1: 308.
14. Wade, J. G., C. P. Larson, Jr., R. F. Hickey, W. K.Ehrenfeld, and J. W. Severinghaus 1970. Effect of caro-tid endarterectomy on carotid chemoreceptor and baro-receptor function in man. N. Engl. J. Med. 282: 823.
15. Brunk, H. D. 1965. An Introduction to MathematicalStatistics. Blaisdell Publishing Company, Waltham,Mass.
16. Read, D. J. C. 1967. A clinical method for assessingthe ventilatory response to carbon dioxide. Aust. Ann.Med. 16: 20.
17. Cormack, R. S., D. J. C. Cunningham, and J. B. L. Gee.1957. The effect of carbon dioxide on the respiratoryresponse to want of oxygen in man. Quart. J. Exp.Physiol. 42: 303.
18. Loeschcke, H. H., and K. H. Gertz. 1958. Einfluss des02-Druckes in der Einatmungsluft auf die Atemtaitigkeitdes Menschen, gepruft unter Konstanthaltung des al-veolaren C02-Druckes. Pfluegers Arch. gesamte Physiol.267: 460.
19. Clark, T. J. H. 1968. The ventilatory response to C02in chronic airways obstruction. Clin. Sci. 34: 559.
20. Patrick, J. M., and A. Howard. 1972. The influence ofage, sex, body size and lung size on the control andpattern of breathing during C02 inhalation in cau-casians. Resp. Physiol. 16: 337.
21. Mellengaard, K. 1966. The alveolar-arterial oxygendifference: its size and components in normal man.Acta Physiol. Scand. 67: 10.
22. Raine, J. M., and J. M. Bishop. 1963. A-a difference in02 tension and physiological dead space in normal man.J. Appl. Physiol. 18: 284.
23. Turner, J. M., J. Mead, and M. E. Wohl. 1968. Elas-ticity of human lungs in relation to age. J. Appl. Phys-iol. 25: 664.
24. Pierce, J. A., and R. V. Ebert. 1958. The elastic prop-erties of the lungs in the aged. J. Lab. Clin. Med. 51:63.
25. Permutt, S., and H. B. Martin. 1960. Static pressure-volume characteristics of lungs in normal males. J.Appl. Physiol. 15: 819.
26. Brodovsky, D., J. A. MacDonell, and R. M. Cherniack.1960. The respiratory response to carbon dioxide inhealth and emphysema. J. Clin. Invest. 39: 724.
27. Milic-Emili, J., and J. M. Tyler. 1963. Relation betweenwork output of respiratory muscles and end-tidal CO2tension. J. Appl. Physiol. 18: 497.
1818 R. S. Kronenberg and C. W. Drage

28. Bates, D. V., P. T. Macklem, and R. V. Christie. 1971.Respiratory Function in Disease. W. B. Saunders Co.,Philadelphia, Pa.
29. Sorensen, S. C., and J. W. Severinghaus. 1968. Irre-versible respiratory insensitivity to acute hypoxia in manborn at high altitude. J. Appl. Physiol. 25: 217.
30. Lahiri, S., F. F. Kao, T. Velasquez, C. Martinez, andW. Pezzia. 1969. Irreversible blunted respiratory sensi-tivity to hypoxia in high altitude natives. Resp. Physiol.6: 360.
31. Edelman, N. H., S. Lahiri, L. Braudo, N. S. Cherniack,and A. P. Fishman. 1970. The blunted ventilatory re-sponse to hypoxia in cyanotic congenital heart disease.N. Engl. J. Med. 282: 405.
32. Sorensen, S. C., and J. W. Severinghaus. 1968. Respira-tory insensitivity to acute hypoxia persisting after cor-rection of Tetralogy of Fallot. J. Appl. Physiol. 25: 221.
33. Forster, H. V., J. A. Dempsey, M. L. Birnbaum, W.G. Reddan, J. Thoden, R. F. Grover, and J. Rankin.1971. Effect of chronic exposure to hypoxia on ven-
tilatory response to C02 and hypoxia. J. Appl. Physiol.31: 586.
34. Dejours, P. 1962. Chemoreflexes in breathing. Physiol.Rev. 42: 335.
35. Sorensen, S. C., and J. C. Cruz. 1969. Ventilatory re-sponse to a single breath of C02 in 02 in normal manat sea level and high altitude. J. Appl. Physiol. 27:186.
36. Lefrancois, R., H. Gautier, P. Pasquis, A. M. Cevaer,M. F. Hellot, and J. Leroy. 1972. Chemoreflex ventila-tory response to C02 in man at low and high altitudes.Resp. Physiol. 14: 296.
37. Lugliani, R., B. J. Whipp, and K. Wasserman. 1972. Arole for the carotid body in cardiovascular control inman. Clin. Res. 20: 385. (Abstr.)
38. Lugliani, R., B. J. Whipp, C. Seard, and K. Wasserman.1971. Effect of bilateral carotid-body resection on ven-tilatory control at rest and during exercise in man.N. Engl. J. Med. 285: 1105.
Attenuation of Chemoreceptor Function with Age 1819

















![Measurement of Heart Rate Using …measure another vital sign, heart rate. Apart from indicating the soundness of the heart, heart rate helps assessing the cardiovascular system [1]](https://img.dokumen.tips/doc/110x75/5e52a390a714512a3519c177/measurement-of-heart-rate-using-measure-another-vital-sign-heart-rate-apart-from.jpg)