Embed Size (px)
Citation preview

Asthma
Mohammad Ruhal AinR Ph, PGDPRA, M Pharm (Clin.
Pharm)Department of Clinical
Pharmacy

DefinitionChronic inflammatory disease of the airways
Develops under the allergens influence Characterized by dyspnea, breathlessness, cough, wheezing, chest tightness and *sibilant ralesAssociated with bronchial hyperresponsivenessReversible
A whistling sound heard on auscultation and caused by the presence of a viscid secretion narrowing the lumen of a bronchus.

Asthma is a chronic inflammatory disease of the airways which develops under the influence of allergens and characterized by dyspnea, breathlessness, cough, wheezing, chest tightness and sibilant rales more expressed at breathing-out. It is reversible.The inflammation also causes an increase in bronchial hyperresponsiveness(BHR) to a variety of stimuli.
Definition

SABA
LABA
Case Study
Case 1 B.W. is a 20-year-old woman who attends the
university. She joined a fitness club to lose weight; she has
never exercised before. She comes to the clinic today because she coughs and has some trouble breathing ( Shortness of breath , Wheezing , Cough , chest tightness ) in the new aerobics class that she attends twice weekly; however, it does not limit her activity.
Later on , she was diagnosed with exercise induced asthma

Q. Which one of the following classifies B.W.’s asthma?A. Intermittent.B. Mild persistent.C. Moderate persistent.D. Severe persistent.


Q. Which one of the following classifies B.W.’s asthma?A. Intermittent.B. Mild persistent.C. Moderate persistent.D. Severe persistent.
Note:-Because her symptoms are caused by exercise, exercise-induced asthma should be considered.



Table 4

Q. Which one of the following medications is the best option for B.W., from case 1, in addition to albuterolMDI 1–2 puffs before exercise?
A. AlbuterolMDI 1 or 2 puffs 4 times/day as needed.
B. Montelukast10 mg/day. C. Omalizumab150 mg subcutaneously
every 4 weeks. D. MometasoneMDI 220 mcg/puff 1 puff/day.
Since patient has intermittent Asthma , so it’s step 1 ! She only needs SABA PRN

Table 5
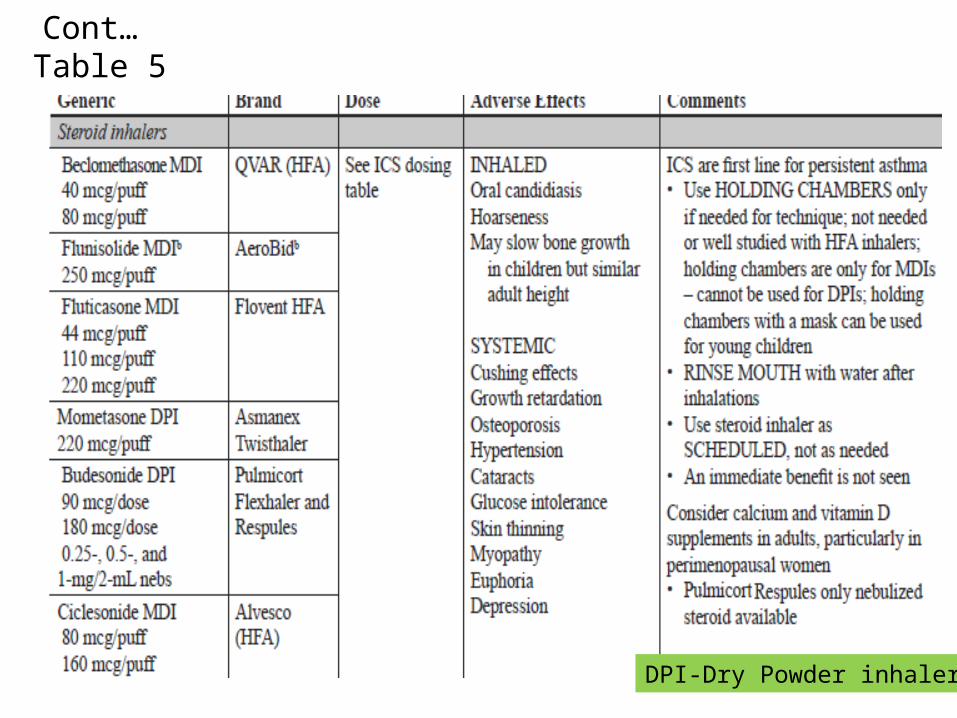
Cont… Table 5
DPI-Dry Powder inhaler

Cont… Table 5
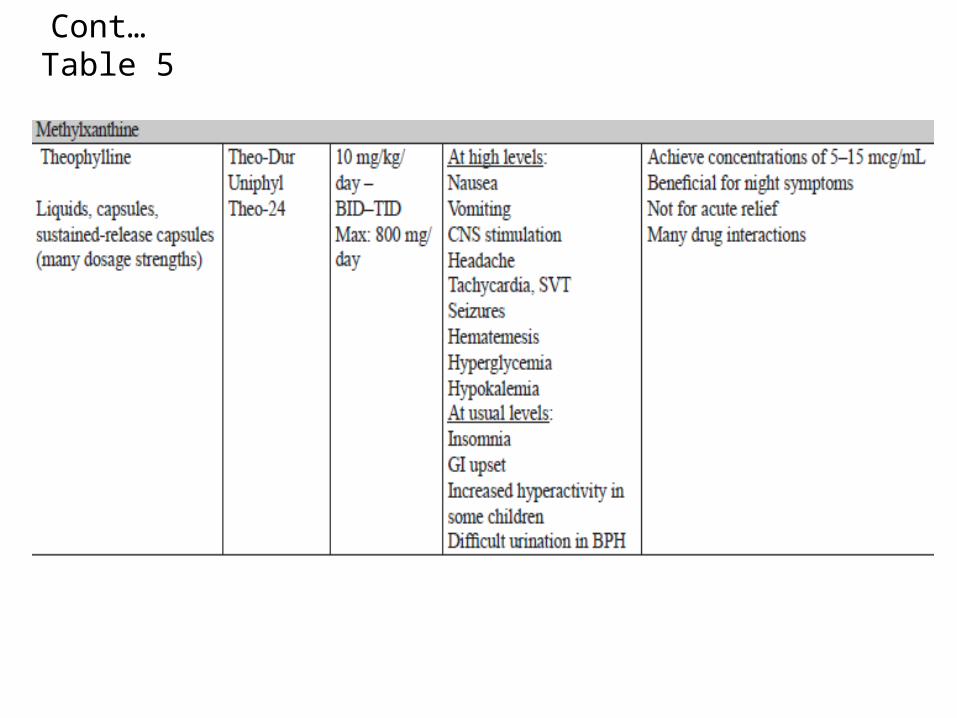
Cont… Table 5

A. Budesonide-formoterolMDI 80/4.5 2 puffs 2 times/day.
B. Montelukast10 mg/day.C. Salmeterol MDI 2 puffs 2 times/day.D. Fluticasone110 mcg/puff 1 puff 2
times/day.
Q. Your recommendation has slightly improved her symptoms. However, she has now begun coughing at night once weekly. Which one of the following is the preferred treatment?

A. Budesonide-formoterolMDI 80/4.5 2 puffs 2 times/day.
B. Montelukast10 mg/day.C. SalmeterolMDI 2 puffs 2 times/day.D. Fluticasone 110 mcg/puff 1 puff 2
times/day.
Q. Your recommendation has slightly improved her symptoms. However, she has now begun coughing at night once weekly. Which one of the following is the preferred treatment?
Step 2 Refer Table 2

Q. B.W. returns 1 month later. She is no longer awakening at night. She uses her albuterol inhaler once weekly to treat her symptoms. She also uses her albuterol inhaler 2 puffs 5 days/week before she works out at the gym. She does not have symptoms while working out. Which one of the following is the correct action to take at this time?
A. No medication change is needed.B. Increase fluticasoneto 110 mcg/puff 2 puffs 2
times/day.C. Add formoterolinhale 1 capsule 2 times/day.D. Add montelukast10 mg/day

Q. B.W. returns 1 month later. She is no longer awakening at night. She uses her albuterol inhaler once weekly to treat her symptoms. She also uses her albuterol inhaler 2 puffs 5 days/week before she works out at the gym. She does not have symptoms while working out. Which one of the following is the correct action to take at this time?
A. No medication change is needed. (Well controlled)B. Increase fluticasoneto 110 mcg/puff 2 puffs 2
times/day.C. Add formoterolinhale 1 capsule 2 times/day.D. Add montelukast10 mg/day

Case 2
Q. D.B. is a 16-year-old boy who has asthma symptoms once or twice a week. He is awakened twice weekly at night with coughing and trouble breathing. Which one of the following is his asthma severity classification?
A. Intermittent.B. Mild persistent.C. Moderate persistent.D. Severe persistent.

• Long-Acting β2-Agonists (LABAs): The U.S. Food and Drug Administration (FDA) issued a safety announcement June 2010 because of safety concerns with LABAs
1. Use of a LABA alone without a long-term asthma control drug, such as an inhaled corticosteroid (ICS), is contraindicated.
2. LABAs should not be used in patients whose asthma is adequately controlled on low-or medium-dose ICSs.
3. LABAs should only be used as additional therapy for patients who are currently taking, but are not adequately controlled on, a long-term asthma control agent, such as an ICS.
4. Once asthma control is achieved and maintained, patients should be assessed at regular intervals and step down (e.g., discontinue the LABA), if possible, and the patient should continue to be treated with a long-term asthma control agent, such as an ICS.
5. Pediatric and adolescent patients who require a LABA and an ICS should use a combination product to ensure adherence with both medications.

Case 3
Q. R.D. is a 25-year-old man who presents to the emergency department with shortness of breath at rest. He is having trouble with conversation. He used 4 puffs of his albuterol MDI at home with no resolution of symptoms. His FEV1 is checked, and it is 38% of predicted. Which one of the following is his severity of asthma exacerbation?
A. Mild.B. Moderate.C. Severe.D. Life threatening


Case 3
Q. R.D. is a 25-year-old man who presents to the emergency department with shortness of breath at rest. He is having trouble with conversation. He used 4 puffs of his albuterol MDI at home with no resolution of symptoms. His FEV1 is checked, and it is 38% of predicted. Which one of the following is his severity of asthma exacerbation?A. Mild.B. Moderate.C. Severe.D. Life threatening

Q. Which one of the following is the best initial therapy for R.D. in the emergency department, in addition to oxygen?
A. Oxygen alone is sufficient.B. Inhaled albuterol MDI 8 puffs every 20
minutes for 1 hour.C. Inhaled albuterol plus ipratropium by
nebulizer every 20 minutes for 1 hour plus intravenous corticosteroids.
D. Inhaled albuterol plus ipratropium by nebulizer every 20 minutes for 1 hour plus OCS


Few Terms

CaseQ.C., a 6-year-old, 20-kg girl, presents to the ED with complaints of:-Dyspnea and coughing that have progressively worsened over the past 2 days. These symptoms were preceded by 3 days of symptoms of a viral upper respiratory tract infection (sore throat, rhinorrhea, and coughing). -She has experienced several bouts of bronchitis in the last 2 years and was hospitalized for pneumonia 3 months ago. -Physical examination reveals an anxious-appearing young girl in moderate respiratory distress with audible expiratory wheezes;- occasional coughing; a prolonged expiratory phase; a hyperinflated chest; and suprasternal, supraclavicular, and intercostal retractions. -Bilateral inspiratory and expiratory wheezes with decreased breath sounds on the left side are heard on auscultation. -Q.C.'s vital signs are as follows: respiratory rate (RR), 30 breaths/minute; blood pressure (BP), 110/83 mmHg; heart rate, 130 beats/minute; temperature, 37.8°C; and pulsus paradoxus, 18 mmHg. Her arterial oxygen saturation (SaO2) by pulse oximetry is 90%. Q.C. is given O2 to maintain SaO2 >90% and 2.5 mg of albuterol by nebulizer Q 20 minutes for three doses.

Q1- After the initial treatment, Q.C. claims some subjective improvement and appears to be more comfortable; however, wheezing on auscultation becomes louder. Does increased wheezing after albuterol indicate failure of the medication? - Asthma is an obstructive lung disease; therefore, the primary limitation to airflow occurs during expiration. This outflow obstruction leads to the classic findings of dyspnea, expiratory wheezes, and a prolonged expiratory phase during the ventilatory cycle. -Wheezing is a whistling sound produced by turbulent airflow through a constricted opening and usually is more prominent on expiration. Thus, the audible expiratory wheezing in Q.C. is compatible with bronchial obstruction. It is important to realize that the classic symptom of wheezing requires turbulent airflow; therefore, effective therapy of acute asthma actually may result in increased wheezing initially as airflow increases throughout the lung. As a result, Q.C.'s increased wheezing on auscultation is compatible with her clinical improvement following the albuterol nebulizer treatments.
Q2. Q.C. may require hospitalization. Which clinical test is predictive of the need for admission or whether Q.C. will relapse if sent home from the ED? Are Q.C.'s signs and symptoms predictive of whether she will relapse and return to the ED if not hospitalized?
The most useful predictive tool is the FEV1 or PEF response to initial treatment. Patients who do not improve to at least 40% of predicted FEV1 or PEF after initial intensive therapy are more likely to require hospitalization.
Although Q.C. is not able to perform spirometry, she is able to execute the PEF maneuver, and the plan is to check her PEF after 1 hour of therapy. Signs and symptom scores alone are not adequate to predict outcome of ED treatment of asthma, but scores along with pulse oximetry and PEF or FEV1 are helpful predictors.
Short-Acting Inhaled β-Adrenergic Agonist TherapyShort-Acting Inhaled β-Agonists Compared With Other Bronchodilators

Q3. Why was a SABA selected as the bronchodilator of first choice in preference to other bronchodilators such as aminophylline or ipratropium for Q.C.?
Because of their potency and rapidity of action, inhaled β2-agonists are considered the first choice for the treatment of acute asthma.The bronchodilatory properties of SABAs are particularly effective in reversing early-phase asthma responses. Aminophylline (a theophylline salt) is not as efficacious and has more risks for serious adverse effects than inhaled albuterol.Similarly, the bronchodilation from the anticholinergic drug ipratropium is of smaller magnitude than with short-acting inhaled β2-agonists. However, an early addition of inhaled ipratropium in adequate doses to SABAs will improve pulmonary function tests and reduce the rate of hospitalization in severely ill patients, Q.C.'s physician chose to use only inhaled short-acting β2-agonists initially because Q.C. was not severely ill.





























