Embed Size (px)
Citation preview

Association of Occupational and Association of Occupational and Environmental ClinicsEnvironmental Clinics
Edward W. Cetaruk, M.D.Edward W. Cetaruk, M.D.Toxicology AssociatesToxicology AssociatesUniversity of Colorado Health Sciences CenterUniversity of Colorado Health Sciences CenterDenver, Colorado, USADenver, Colorado, USA
Worker Preparedness Worker Preparedness and Response and Response
to Bioterrorismto Bioterrorism

Section 1Section 1An Overview of Biological WeaponsAn Overview of Biological Weapons
Objectives:Objectives:
1)1) To be able to list biological agents that may To be able to list biological agents that may be weaponizedbe weaponized
2)2) To describe the process of weaponizationTo describe the process of weaponization
3)3) To develop an understanding of the To develop an understanding of the bioterrorist threatbioterrorist threat
4)4) To be able to recognize a biological attackTo be able to recognize a biological attack

POTENTIALIMPACT
PROBABILITY/LIKELIHOOD
NUCLEARWEAPON
IMPROVISEDNUCLEAR
DEVICE
RADIOACTIVEMATERIAL
CHEMICAL AGENTOR TOXIC
INDUSTRIALCHEMICAL
BIOLOGICALAGENT
Probability vs. Potential ImpactProbability vs. Potential Impact

• Oldest of the NBC triad of agents• Used for > 2,000 years
• Sieges of middle ages• Smallpox blankets given to Native
Americans• Germany in World War I• Japan in World War II• Modern Bioterrorism
History of Biological WarfareHistory of Biological Warfare

• Sarin Nerve Agent attacks 1994 and 1995Sarin Nerve Agent attacks 1994 and 1995• Attempted Botulinum Toxin release multiple timesAttempted Botulinum Toxin release multiple times• Anthrax released multiple timesAnthrax released multiple times• Attempted to obtain Ebola virus in ZaireAttempted to obtain Ebola virus in Zaire
Aum Shinrikyo CultAum Shinrikyo Cult

Anthrax LettersAnthrax LettersUnited StatesUnited States

• AnthraxAnthrax• Botulinum Toxin ABotulinum Toxin A• BrucellosisBrucellosis• GlandersGlanders• Marburg VirusMarburg Virus• PlaguePlague• Q FeverQ Fever
• SalmonellaSalmonella• SmallpoxSmallpox• Staph Enterotoxin BStaph Enterotoxin B• Monkey PoxMonkey Pox• RicinRicin• TularemiaTularemia• VEEVEE• VHFsVHFs
Weaponized Biowarfare Weaponized Biowarfare AgentsAgents

Biological Agents of Highest ConcernBiological Agents of Highest ConcernCategory ACategory A
• Variola majorVariola major (Smallpox) (Smallpox)• Bacillus anthracisBacillus anthracis (Anthrax) (Anthrax)• Yersinia pestisYersinia pestis (Plague) (Plague)• Francisella tularensisFrancisella tularensis (Tularemia) (Tularemia)• Botulinum toxin (Botulism)Botulinum toxin (Botulism)• Filoviruses and Arenaviruses (Viral hemorrhagic fevers)Filoviruses and Arenaviruses (Viral hemorrhagic fevers)• ALLALL suspected or confirmed cases should be reported to suspected or confirmed cases should be reported to
health authorities health authorities immediatelyimmediately

Anthrax 1-5 Days++
Plague 2-3 Days
Q Fever 10-40 Days
Tularemia 2-10 Days
Smallpox 7-17 Days
Viral encephalitides V(2-6d); E&W (7-14 d)
VHFs 4-21 Days
Botulinum toxin 1-5 Days
Staph. enterotoxin B 1-6 Hours
Incubation Periods of Selected Biological Agents

Anthrax 8,000 (or fewer) spores
Plague 100-500 organisms
Q Fever 1-10 organisms
Tularemia 10-50 organisms
Smallpox 10-100 organisms
Viral encephalitides 10-100 organisms
VHFs 1-10 organisms
Botulinum toxin 0.001 ug/kg
Infective Aerosol Doses of Selected Biological Agents

18-20
15-18
7-12
4-6(bronchioles)
1-5 (alveoli)
Infection Severity
Particle Size (Micron, Mass
Median Diameter)The ideal aerosol contains a
homogeneous population
of 2 or 3 micron particulates that contain
one or more viable organisms
Maximum human respiratory infection
is a particle that falls within the 1 to 5
micron size
Less Severe
More Severe
Aerosol Size and InfectivityAerosol Size and Infectivity

• Large epidemic with high illness and death rate• Immunocompromised individuals may have first
susceptibility• Respiratory symptoms predominate• Infection non-endemic for region• Multiple, simultaneous outbreaks• Multi-drug-resistant pathogens• Sick or dead animals • Delivery vehicle or intelligence information
Epidemiologic CluesEpidemiologic Clues

• Travel history• Local• Distant
• Infectious contacts• Employment history• Activities over the
preceding 1 to 2 weeks
Epidemiologic InformationEpidemiologic Information

Section 2Section 2Bioterrorism and the WorkplaceBioterrorism and the WorkplaceObjectives:Objectives:
1)1) To be able to develop practices and To be able to develop practices and procedures to defend workers and the procedures to defend workers and the workplace from a bioterrorist attackworkplace from a bioterrorist attack
2)2) To respond the unique risks faced by first To respond the unique risks faced by first respondersresponders
3)3) To be able to choose and use the correct To be able to choose and use the correct PPE needed for biological weaponsPPE needed for biological weapons

Bioterrorism Educational Needs Bioterrorism Educational Needs of the Workerof the Worker
• AwarenessAwareness• Fundamental understanding of biowarfare Fundamental understanding of biowarfare
agentsagents• Recognition and handling of suspicious Recognition and handling of suspicious
mail or dissemination devicesmail or dissemination devices• PPE and workplace safetyPPE and workplace safety• Recognition of bioterrorist attackRecognition of bioterrorist attack• Post exposure managementPost exposure management

• Primary Care PersonnelPrimary Care Personnel• Hospital ER StaffHospital ER Staff• Public Health ProfessionalsPublic Health Professionals• Emergency Response PersonnelEmergency Response Personnel• Laboratory PersonnelLaboratory Personnel• Law EnforcementLaw Enforcement• PublicPublic• MilitaryMilitary
BioterrorismBioterrorism::Who are First Responders?Who are First Responders?
First RespondersFirst Responders
• Often dealing with unknown agent(s)Often dealing with unknown agent(s)• May be exposed to infectious agentMay be exposed to infectious agent• May be exposed to infectious patientsMay be exposed to infectious patients• May be targeted with secondary devicesMay be targeted with secondary devices• May be first to notice the epidemiological May be first to notice the epidemiological
pattern of a bioweapons attackpattern of a bioweapons attack

Emergency PlanEmergency Plan• All Hazards ApproachAll Hazards Approach• Identify areas with risk of exposureIdentify areas with risk of exposure• Develop controls to minimize riskDevelop controls to minimize risk
• Engineering ControlsEngineering Controls• Administrative ControlsAdministrative Controls• Housekeeping ControlsHousekeeping Controls
• PPE for workersPPE for workers• Develop response and recovery planDevelop response and recovery plan• Training and ExercisesTraining and Exercises

Emergency PlanEmergency PlanExposure to Biological AgentExposure to Biological Agent
• Policies and Procedures for handling Policies and Procedures for handling suspicious mail or packagessuspicious mail or packages
• Plan for facility responsePlan for facility response• Plan for involving appropriate authoritiesPlan for involving appropriate authorities• Medical SurveillanceMedical Surveillance• Training and ExercisesTraining and Exercises

Handling of Suspicious MailHandling of Suspicious Mail• Do not shake, empty contentsDo not shake, empty contents• Do not carry, show others, or allow others Do not carry, show others, or allow others
to examine itto examine it• Do not sniff, touch, look closely at it, or any Do not sniff, touch, look closely at it, or any
contents that may have spilledcontents that may have spilled• Leave on stable surface, alert others, leave Leave on stable surface, alert others, leave
area, close doors, shut off ventilationarea, close doors, shut off ventilation• Wash hands with soap and waterWash hands with soap and water• Notify law enforcementNotify law enforcement• Create list of persons with potential contactCreate list of persons with potential contact

Personal Protective EquipmentPersonal Protective Equipment
Level A Level A • SCBA, Encapsulation SCBA, Encapsulation • Level of protection for entering contaminated, Level of protection for entering contaminated,
unsecured sceneunsecured scene Level BLevel B Level CLevel C Level DLevel D

Personal Protective EquipmentPersonal Protective EquipmentRespiratorsRespirators
Powered Air-Purifying Respirator (PAPR)Powered Air-Purifying Respirator (PAPR)• HEPA filter face masks (N95, N100)HEPA filter face masks (N95, N100)• Respirators must be in compliance with Respirators must be in compliance with
OSHA respiratory standard OSHA respiratory standard
(29 CFR 1910.134)(29 CFR 1910.134)• Respirators must be fit testedRespirators must be fit tested

Powered Air Purifying RespiratorPowered Air Purifying Respirator((PAPR)PAPR)

PPEPPERespiratorsRespirators
• Respirators should be used in accordance with a respiratory-protection program that complies with the OSHA respiratory-protection standard (29 CFR 1910.134).
N95N95 N100N100

The respirator is properly positioned over your The respirator is properly positioned over your nose and mouth at all timesnose and mouth at all times The top strap or head harness assembly is The top strap or head harness assembly is positioned high on the back of the headpositioned high on the back of the head The lower strap is worn at the back of the neck The lower strap is worn at the back of the neck below the earsbelow the ears The straps are snug enough to keep the respirator The straps are snug enough to keep the respirator from moving but not overly tightfrom moving but not overly tight Nothing (beards, head coverings, etc.) passes Nothing (beards, head coverings, etc.) passes between the skin of the face and the respirator’s between the skin of the face and the respirator’s sealing edgesealing edge
Personal Protective EquipmentPersonal Protective EquipmentRespiratorsRespirators

PPEPPEDermal ProtectionDermal Protection
• Disposable Disposable • ReusableReusable• Overgarments, Booties, Hoods, GlovesOvergarments, Booties, Hoods, Gloves• All PPE should be decontaminated prior to All PPE should be decontaminated prior to
leaving potentially contaminated arealeaving potentially contaminated area• PPE should be removed and discarded prior PPE should be removed and discarded prior
to removing face maskto removing face mask

Section 3Section 3Anthrax as a Biological WeaponAnthrax as a Biological WeaponObjectives:Objectives:
1)1) To understand the microbiology and To understand the microbiology and epidemiology of anthraxepidemiology of anthrax
2)2) To understand the pathophysiology of the To understand the pathophysiology of the different anthrax clinical syndromesdifferent anthrax clinical syndromes
3)3) To be able to recognize cutaneous anthraxTo be able to recognize cutaneous anthrax
4)4) To be able to recognize an intentional To be able to recognize an intentional anthrax releaseanthrax release
5)5) To be able to treat patients with anthraxTo be able to treat patients with anthrax

• Bacterium• Spores may survive > 100 yrs• Worldwide soil distribution• Common disease of herbivores• Herbivores in USA vaccinated• Man infected via animal products• Woolsorter’s Disease
AnthraxAnthraxMicrobiology & EpidemiologyMicrobiology & Epidemiology

Source: WHO World Anthrax Data SiteSource: WHO World Anthrax Data Site
AnthraxWorldwide Occurrence

• Spore enters skin, GI tract, or lung• Germinates in macrophage• Transported to regional lymph nodes• Local production of toxins• Swelling and Tissue Death• Toxemia
AnthraxAnthraxPathophysiologyPathophysiology

• Cutaneous• Gastrointestinal• Inhalational
Multiple forms can be
seen as the result of a BW attack
Anthrax Anthrax Clinical SyndromesClinical Syndromes
AnthraxAnthraxGastrointestinalGastrointestinal
• Abdominal pain, usually accompanied by Abdominal pain, usually accompanied by bloody vomiting or diarrhea, followed by bloody vomiting or diarrhea, followed by fever and signs of sever infectionfever and signs of sever infection
• GI anthrax is sometimes seen as mouth GI anthrax is sometimes seen as mouth and throat ulcerations with tender neck and throat ulcerations with tender neck glands and feverglands and fever
• Develops after ingestion of contaminated, Develops after ingestion of contaminated, poorly cooked meat.poorly cooked meat.
• Incubation period: 1–7 daysIncubation period: 1–7 days • Case-fatality: 25–90% (role of early Case-fatality: 25–90% (role of early
antibiotic treatment is undefined)antibiotic treatment is undefined)

Anthrax:Anthrax:CutaneousCutaneous
• Begins as a papule, progresses through a Begins as a papule, progresses through a vesicular stage to a depressed black necrotic ulcer vesicular stage to a depressed black necrotic ulcer (eschar)(eschar)
• Edema, redness, and/or necrosis without Edema, redness, and/or necrosis without ulceration may occurulceration may occur
• Form most commonly encountered in naturally Form most commonly encountered in naturally occurring casesoccurring cases
• Incubation period: 1–12 daysIncubation period: 1–12 days • Case-fatality: Case-fatality:
• Without antibiotic treatment:Without antibiotic treatment: 20%20%• With antibiotic treatment:With antibiotic treatment: 1%1%

JAMA. 2002;287:869-874
Hospital Day 5
2 months after discharge
Hospital Day 12
Cutaneous Anthrax

• Incubation Period: 1-6 daysIncubation Period: 1-6 days• A brief prodrome resembling a “viral-like” A brief prodrome resembling a “viral-like”
illness, characterized by muscle aches, fatigue, illness, characterized by muscle aches, fatigue, fever, with or without respiratory symptoms, fever, with or without respiratory symptoms, nausea, vomiting, abdominal painnausea, vomiting, abdominal pain
• Early Symptoms: malaise, fever, fatigue, non-Early Symptoms: malaise, fever, fatigue, non-productive cough, chest discomfortproductive cough, chest discomfort
• Confusion, neck stiffness, and headache suggest Confusion, neck stiffness, and headache suggest meningitis (seen in 50% of patients)meningitis (seen in 50% of patients)
Inhalational Anthrax Inhalational Anthrax Clinical PresentationClinical Presentation

Inhalational Anthrax Inhalational Anthrax Clinical PresentationClinical Presentation
• After initial onset of illness, symptoms may remain mild or even improve slightly before worsening
• Terminal Phase: dyspnea, stridor, cyanosis, shock, chest wall edema, meningitis, widened mediastinum with effusion with overall toxic/septic clinical picture

Presenting SymptomsPresenting SymptomsSymptoms n=10Fever, chills 10Sweats, often drenching 7Fatigue, malaise, lethargy 10Cough 9Nausea or vomiting 9Dyspnea 8Chest discomfort or pleurisy 7Myalgias 6Headache 5Confusion 4Abdominal pain 3Sore throat 2Rhinorrhea 1
Emerg Infect Dis Emerg Infect Dis vol.7, no. 6, 2001vol.7, no. 6, 2001

• Clinical picture of sudden onset of respiratory distress with mediastinal widening on x-ray
• A small number of patients may present with GI or cutaneous anthrax
• Gram stain of blood and blood cultures - but these may be late findings in the course of the illness
• ELISA, FA, PCR and immunohistology testing may confirm diagnosis but samples must go to reference laboratory
Anthrax DiagnosisAnthrax Diagnosis

Acute Treatment
• Usually futile in severe mediastinitis patients who inhaled or ingested spores
• Ciprofloxacin - 400 mg IV q 8 to 12 hr
• Doxycycline - 100 mg IV q 12 hr
• Vaccination
Post-exposure
• Oral prophylaxis
• Ciprofloxacin (500 mg PO q12 h) X 60 days and until 3 doses of vaccine
• Doxycycline (100 mg PO q12 h) X 60 days and until 3 doses of vaccine
• Vaccination
Anthrax TreatmentAnthrax Treatment

• FDA approved 1970FDA approved 1970• Cell Free filtrate (NO organisms, dead or alive)Cell Free filtrate (NO organisms, dead or alive)• Adverse effects 1-3%Adverse effects 1-3%• Bioport CorporationBioport Corporation
Anthrax VaccineAnthrax Vaccine

Laboratory WorkersLaboratory Workers• Increased number of highly pathogenic Increased number of highly pathogenic bacterial and viral samplesbacterial and viral samples• Increased need for universal precautionsIncreased need for universal precautions• Increased need for security, including Increased need for security, including maintaining chain of custody for forensic maintaining chain of custody for forensic samplessamples• Increased need for decontamination proceduresIncreased need for decontamination procedures• Laboratory Response Network (LRN)Laboratory Response Network (LRN)

Laboratory WorkersLaboratory WorkersDecontamination and DisinfectionDecontamination and Disinfection
Effective sporicidal solutions:Effective sporicidal solutions:• Commercially-available bleach diluted to Commercially-available bleach diluted to
0.5% Sodium hypochlorite (1 part household 0.5% Sodium hypochlorite (1 part household bleach to 9 parts water) bleach to 9 parts water)
• Rinse off concentrated bleach to avoid Rinse off concentrated bleach to avoid caustic effectscaustic effects
• Approved sporicidal agentsApproved sporicidal agents

Section 4Section 4Plague as a Biological WeaponPlague as a Biological Weapon
Objectives:Objectives:
1)1) To be able to describe the pathophysiology To be able to describe the pathophysiology and epidemiology of plague.and epidemiology of plague.
2)2) To be able to recognize and treat the To be able to recognize and treat the different clinical forms of plague.different clinical forms of plague.
3)3) To be able to control the secondary To be able to control the secondary transmission of plaguetransmission of plague

PlaguePlagueHistoryHistory
• 200,000,000 deaths • Biblical (I Sam.) - 1320 BC, Philistines• Major Pandemics
• 541 - Plague of Justinian• 1346 - ‘Black Death’• 1894 - Modern Pandemic

Plague DistributionPlague Distribution• 1894 - Began in China• 1898 - Southwest to India• 1898 - South to Vietnam• 1900 - Trans-Pacific to United States

PlaguePlagueEpidemiologyEpidemiology
Vector: fleas, >80 species• Xenopsylla cheopis (Oriental rat flea)• Fleas feed on plague-infected mammal• Bacteria multiply in gut• Coagulum blocks gut• Plague organisms are
regurgitated into bite wound with next feeding
Photo: Ken Gage, Ph.D., CDC, Fort Collins, CO
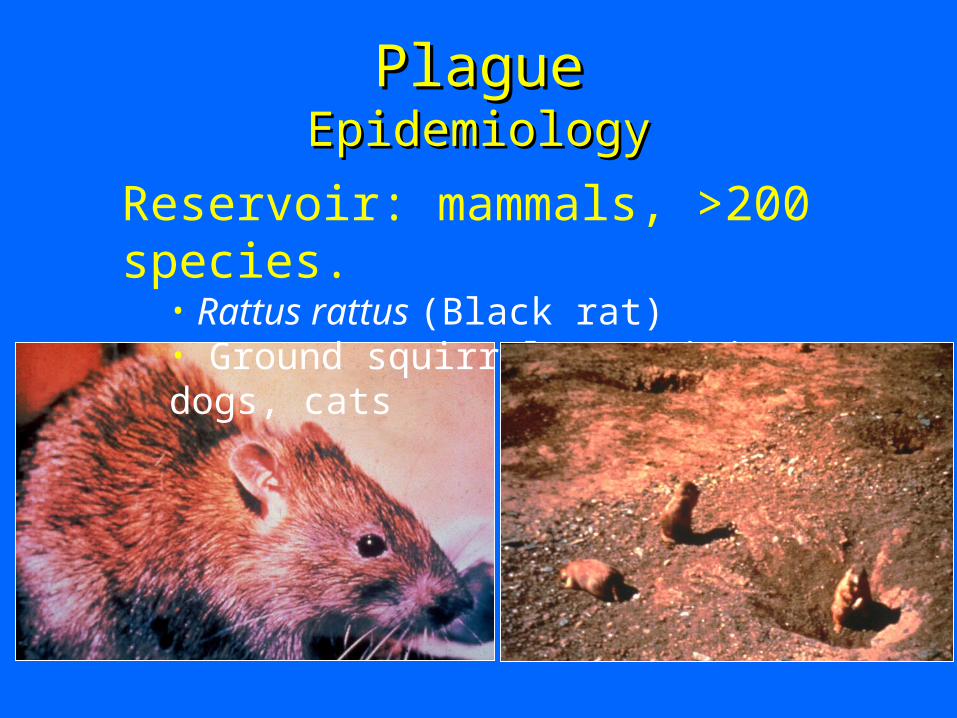
Reservoir: mammals, >200 species.• Rattus rattus (Black rat)• Ground squirrels, prairie dogs, cats
PlaguePlagueEpidemiologyEpidemiology

PlaguePlaguePathogenesisPathogenesis
• Yersinia pestisYersinia pestis - a Gram negative, nonmotile, - a Gram negative, nonmotile, nonsporulating bacteria nonsporulating bacteria
• Size: 0.5–0.8 × 1.5–2.0 µmSize: 0.5–0.8 × 1.5–2.0 µm• Normally a disease of rodentsNormally a disease of rodents• Virulence Factors: antiphagocytic fraction 1 Virulence Factors: antiphagocytic fraction 1
capsule, pH 6 antigen, antiphagocytic Yops capsule, pH 6 antigen, antiphagocytic Yops H and E, V antigens, Yop M, and H and E, V antigens, Yop M, and plasminogen activatorplasminogen activator

PlaguePlaguePathophysiologyPathophysiology
LungMeningesLiverSpleen
Inoculation or inhalation(1-10 organisms) (100-20,000 organisms)
Macrophage
Lymphatics
Regional lymph nodesBlood

Bubonic PlagueBubonic PlagueClinical PresentationClinical Presentation
• Incubation 1-8 days (mode 3-5 days)
• Sudden onset of flu-like syndrome • (Fever, rigors, malaise, myalgias, nausea)
• Bubo formation - within 24 hours• Swollen, infected lymph node (very painful!)
• Cutaneous findings in 25% of cases• Mortality: Untreated 60%
Treated <5%

Photographs: Ken Gage, Ph.D., Centers for Disease Control and Prevention, Fort Collins, CO
Bubonic PlagueBubonic Plague

Pneumonic PlaguePneumonic PlagueClinical PresentationClinical Presentation
• 2 to 3 day incubation period followed by high fever, muscle aches, chills, headache
• Cough with bloody sputum within 24 hours• pneumonia progresses rapidly – shortness of breath, stridor,
cyanosis, difficulty breathing, chest pain• respiratory failure, shock, bleeding
• In contrast to anthrax, Plague pneumonia and sepsis develop acutely and may be fulminant
• Patchy lung infiltrates or consolidation seen on chest x-ray

Pneumonic PlaguePneumonic Plague
Photograph by Ken Gage, Ph.D., Centers of Disease Control and Prevention, Fort Collins, CO.

Plague TransmissionPlague Transmission
PNEUMONIC
BUBONIC and
SEPTICEMIC
SECONDARYPNEUMONIC
andOROPHARYNGEAL
Fleas
(active or dormant)
Rodent
Aerosol
Surface contact

PlaguePlagueDiagnosisDiagnosis
• Gram stain and culture of lymph node aspirates, sputum, or CSF samples
• Bipolar staining “Safety Pin” may be present
• Immunoassays are also availablePhotomicrograph: Ken Gage, Ph.D., Centers for
Disease Control and Prevention, Fort Collins, CO.

Plague - TreatmentPlague - Treatment
Antibiotic Therapy:• Streptomycin (choice)15-30 mg/kg IM bid x
10 days• Gentamicin - 2 mg/kg IV then 1.0-1.5 mg/kg
q8h or 5 mg/kg IV q24h x 10 days • Doxycycline - 200 mg IV then
100 mg bid x 10-14 days• Ciprofloxacin - 400 mg IV q12h x 10 days

PlaguePlagueControl of Secondary TransmissionControl of Secondary Transmission
Secondary transmission is possible and likely
• Standard, contact, and aerosol precautions for at least 48 hrs until sputum cultures are negative or pneumonic plague is excluded
Section 5Section 5Smallpox as a Biological WeaponSmallpox as a Biological Weapon
Objectives:Objectives:
1)1) To be able to describe the epidemiology To be able to describe the epidemiology and microbiology of smallpoxand microbiology of smallpox
2)2) To be able to recognize clinical smallpoxTo be able to recognize clinical smallpox
3)3) To be able control the secondary To be able control the secondary transmission of smallpoxtransmission of smallpox
4)4) To describe treatment and vaccination To describe treatment and vaccination options for smallpox.options for smallpox.

SmallpoxSmallpox
• The world’s first eradicated diseaseThe world’s first eradicated disease• 1977- last endemic case in Somalia1977- last endemic case in Somalia• 1978- two laboratory cases in Britain1978- two laboratory cases in Britain• 1980- WHO declares global 1980- WHO declares global
eradication of smallpoxeradication of smallpox

SmallpoxSmallpox
• Variola (Var-ï-óla) virus: an Orthopox virus, both minor and major forms of smallpox exist
• Structure is a large DNA virus• Declared eradicated in 1980
and the U.S. stopped its civilian vaccination in 1981, U.S. military stopped in 1985

• 1763- French & Indian War• Fort Ticonderoga• Lord Jeffrey Amherst
• World War II• Unit 731 experiments in China
• Cold War• USSR arsenal
Smallpox as a BioweaponSmallpox as a Bioweapon

• Infectious via aerosol• Vaccination discontinued• Decreased potency of vaccine stocks• Severe morbidity and mortality• Transmissible• Clinical inexperience• “Brand-name” recognition
Why would smallpox Make A Why would smallpox Make A Good Biological Weapon?Good Biological Weapon?

• Incubation 7-17 days (mean 12)• Infection of respiratory mucosa• Minor viremia: seeding of liver, spleen• Major viremia: seeding of skin• Acute onset fever, rigors, headache,
vomiting• Virus cultured from blood
Clinical SmallpoxClinical Smallpox ProdromeProdrome

• Enanthem• Exanthem
• begins on face, hands, forearms• spreads to lower extremities• centrifugal distribution• Macules papules vesicles pustules
scabs/crusts scars
Clinical SmallpoxClinical Smallpox

Breman & Henderson, Breman & Henderson, NEJM, NEJM, 346(17), April, 2002346(17), April, 2002

SmallpoxSmallpoxDay 3 of RashDay 3 of Rash
From: Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and Its Eradication. Geneva, Switzerland: World Health Organization; 1988: 10–14. Photographs by I. Arita.

SmallpoxSmallpoxDay 5 of RashDay 5 of Rash
From: Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and Its Eradication. Geneva, Switzerland: World Health Organization; 1988: 10–14. Photographs by I. Arita.

SmallpoxSmallpoxDay 7 of RashDay 7 of Rash
From: Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and Its Eradication. Geneva, Switzerland: World Health Organization; 1988: 10–14. Photographs by I. Arita.

SmallpoxSmallpox

SmallpoxSmallpoxClinical FormsClinical Forms
• Variola Major• 30% fatal in unvaccinateds• 3% fatal in vaccinateds
• Variola Minor• Flat-Type Smallpox• Hemorrhagic Smallpox• Modified-Type Smallpox• Variola Sine Eruptione

Variola Variola MinorMinor
From: Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and Its Eradication. Geneva, Switzerland: World Health Organization; 1988: 10–14. Photographs by I. Arita.

Flat-type SmallpoxFlat-type Smallpox
From Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and Its Eradication. Geneva, Switzerland: World Health Organization; 1988: 33. Photograph by F. Dekking

Hemorrhagic SmallpoxHemorrhagic Smallpox
From Herrlich A, Mayr A, Munz E, Rodenwaldt E. Die pocken; Erreger, Epidemiologie und klinisches Bild. 2nd ed. Stuttgart, Germany: Thieme; 1967.

Smallpox vs. ChickenpoxSmallpox vs. Chickenpox
VariolaVariola VaricellaVaricella
IncubationIncubation 7-17 days7-17 days 14-21 days14-21 days
ProdromeProdrome 2-4 days2-4 days minimalminimal
DistributionDistribution centrifugalcentrifugal centripetalcentripetal
EvolutionEvolution synchronoussynchronous asynchronousasynchronous
Scabs FormScabs Form 10-14 days10-14 days 4-7 days4-7 days
Scabs SeparateScabs Separate 14-28 days14-28 days <14 days<14 days
InfectivityInfectivity separationseparation scabbingscabbing

SmallpoxSmallpoxManagement of ContactsManagement of Contacts
• Immediate vaccination or boostingImmediate vaccination or boosting• VIG 0.6 ml/kgVIG 0.6 ml/kg
• Pregnant patientsPregnant patients• Dermatoses patientsDermatoses patients• ?? Normal hosts?? Normal hosts• Limited data: Vaccine + VIG better than Limited data: Vaccine + VIG better than
vaccine alone?vaccine alone?
• STRICTSTRICT quarantine x 17 days quarantine x 17 days

VaccinationVaccination
• Employs Vaccinia virus• Given by scarification• One dose protective for 5-10 years• Must keep vaccinia immunoglobulin
(VIG) on hand to treat complications of vaccination

Complications of VaccinationComplications of Vaccination
• Normal host• Inadvertent Autoinoculation (skin, eye)• Generalized vaccinia• Erythema multiforme• Encephalitis
• Pregnancy - fetal vaccinia• Dermatoses/Burns - eczema vaccinatum• Immunocompromised - vaccinia necrosum

From Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and Its Eradication. Geneva, Switzerland: World Health Organization; 1988: 298. Photograph by C. H. Kempe
OcularOcular VacciniaVaccinia

From Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and Its Eradication. Geneva, Switzerland: World Health Organization; 1988: 298. Photograph by C. H. Kempe
Vaccinia Vaccinia NecrosumNecrosum

Eczema VaccinatumEczema Vaccinatum
N Engl J Med, Vol. 346, No. 17, April 25, 2002

• Public health emergency• Supportive care• Vaccinia Immunoglobulin• Strict quarantine until scabs off
• At least 17 days• Codofovir
SmallpoxSmallpoxTherapyTherapy

Section 6Section 6Other Viruses as Biological Other Viruses as Biological
WeaponsWeaponsObjectives:Objectives:
1)1) To become familiar with viral hemorrhagic To become familiar with viral hemorrhagic fever viruses (VHFs) and Venezuelan equine fever viruses (VHFs) and Venezuelan equine encephalitis virus pathophysiologyencephalitis virus pathophysiology
2)2) To be familiar with necessary PPE to able to To be familiar with necessary PPE to able to limit the secondary spread of VHFlimit the secondary spread of VHF
3)3) To be able to treat victims of these biological To be able to treat victims of these biological agentsagents

Viral Hemorrhagic Fevers Viral Hemorrhagic Fevers MicrobiologyMicrobiology
• RNA viruses causing high fevers and generalized vascular damage
• Filoviruses (Ebola, Marburg)
• Human infections by insect bites or by contact with blood
and body fluidsPhotograph: Robert Swanepoel, PhD, DTVM, MRCVS,
National Institute of Virology, Sandringham, South Africa.

• RNA viruses causing high fevers and generalized vascular damage
• May be spread by aerosol, on fomites, and by oral secretions and eye drainage in animals
• Human infections by contact with blood and body fluids
Viral Hemorrhagic Fevers Viral Hemorrhagic Fevers (VHFs)(VHFs)

VHF PathogenesisVHF Pathogenesis• Fever, muscle aches, prostration• Cases evolve into shock and generalized mucous
membrane hemorrhage• Conjunctival injection, petechial hemorrhage, and
hypotension• Abnormal kidney and liver function tests poor
prognosis• Mortality varies; 50 - 80% Ebola Zaire
• Disease severity and survival depends on various host factors; target organ is the blood vessel system.

• 1976 - First reported case in Sudan• 1989 - Reston, VA health facility
among imported monkeys• April 1995 - Ebola epidemic Kikwit, Zaire• 1996 - Ebola outbreak in Alice, TX - monkeys• 1996 - Gabon patient infection transferred to
Johannesburg clinic healthcare worker• 50 to 80% mortality rate in humans - extensive
hemorrhage, shock, and end organ failure• 2002 – Gabon – most recent outbreak
Ebola VirusEbola Virus

VHF VHF TreatmentTreatment
• Blood pressure resuscitation and monitoring• Careful fluid management
• Use of colloids (e.g. plasma)• Vasopressors and inotropes• Cautious sedation and analgesia• No anti-platelet drugs or IM injections• Coagulation studies and replacement of
clotting factors, platelet transfusions

Prevention of Secondary VHF Prevention of Secondary VHF TransmissionTransmission
• Animal studies indicate aerosol transmission possible• Single room with adjoining anteroom as only
entrance• Handwashing station with decontamination solution
• Negative air pressure room if possible• Strict barrier precautions (PPE):
• Gloves, gown, mask. shoe covers, protective eyeware/faceshield
• Consider HEPA respirator (e.g. N95) for severe hemorrhage, vomiting, diarrhea, cough

Prevention of Secondary VHF Prevention of Secondary VHF TransmissionTransmission
• Chemical toilet
• All body fluids disinfected
• Disposable equipment/sharps into rigid containers and autoclaved/incinerated
• Double-bag refuse-outside bag disinfected
• Electronic/mechanical equipment must be disinfected

Venezuelan Equine EncephalitisVenezuelan Equine Encephalitis(VEE)(VEE)
• Alphavirus spread by mosquitoesAlphavirus spread by mosquitoes• Endemic to Central and South America, Endemic to Central and South America,
Mexico, and FloridaMexico, and Florida• Highly infectious - 100% of exposed Highly infectious - 100% of exposed
individuals develop symptomsindividuals develop symptoms• Low mortality rate - 1%Low mortality rate - 1%

Section 7Section 7Toxin WeaponsToxin Weapons
Objectives:Objectives:1)1) To be able to explain how each of the To be able to explain how each of the
presented toxin weapons actpresented toxin weapons act
2)2) To be able to recognize victims to toxin To be able to recognize victims to toxin weapon poisoningweapon poisoning
3)3) To understand that toxin weapons are To understand that toxin weapons are NOT infectious and CANNOT be NOT infectious and CANNOT be secondarily spreadsecondarily spread

• Neurotoxin produced by Clostridium botulinum - Botulism
• Most lethal compound per weight (15,000 times more toxic than the nerve agent VX)
• Different toxicity if inhaled or ingested
Botulinum ToxinBotulinum Toxin

Botulinum ToxinBotulinum ToxinNormal Muscle ContractionNormal Muscle Contraction
Acetylcholine
MUSCLE CONTRACTIONMUSCLE CONTRACTION
Motor NerveMotor Nerve
MuscleMuscle
NMJNMJ

Botulinum ToxinBotulinum ToxinBotulinum-Paralyzed MuscleBotulinum-Paralyzed Muscle
BBOOTTOOXX
NONO MUSCLE CONTRACTION MUSCLE CONTRACTION
NMJNMJ
Motor NerveMotor Nerve
MuscleMuscle

• Descending paralysisDescending paralysis• Bulbar Palsies Bulbar Palsies
• Blurred visionBlurred vision• Dilated pupilDilated pupil• Double visionDouble vision• Drooping eyelidsDrooping eyelids• Light intoleranceLight intolerance• Difficulty swallowingDifficulty swallowing• Difficulty speakingDifficulty speaking
• Respiratory failureRespiratory failure
BotulismBotulismSigns & SymptomsSigns & Symptoms
“Floppy” baby flaccid paralysis

• Clinical diagnosis: bulbar palsies with descending paralysis
• Mouse neutralization assay confirms diagnosis• Treatment is supportive
• Long-term mechanical ventilation• Antitoxins are available but must be
administered early to be effective• CDC vaccine protective for A,B and E toxins
BotulismBotulism Diagnosis and TreatmentDiagnosis and Treatment

RicinRicin• Potent toxin - a protein Potent toxin - a protein
byproduct of castor bean byproduct of castor bean processing for castor oilprocessing for castor oil
• 5 times more toxic per 5 times more toxic per weight than VXweight than VX
• Blocks protein synthesis Blocks protein synthesis within the cell, causes within the cell, causes cell death, and airway cell death, and airway tissue death and swelling tissue death and swelling when inhaledwhen inhaled

RicinRicinDiagnosis & TreatmentDiagnosis & Treatment
• Fever, chest tightness, cough.Fever, chest tightness, cough.• Shortness of breath, nausea, and joint pain.Shortness of breath, nausea, and joint pain.• Ingestion causes severe diarrhea, Ingestion causes severe diarrhea,
hemorrhage, and necrosis of the liver, spleen, hemorrhage, and necrosis of the liver, spleen, and kidneys - shock and death within 3 daysand kidneys - shock and death within 3 days
• Treatment is supportive, including airway Treatment is supportive, including airway management management
• No antitoxin or vaccine availableNo antitoxin or vaccine available

• Common cause of food poisoning in Common cause of food poisoning in improperly handled foodsimproperly handled foods
• 80% of exposed individuals develop 80% of exposed individuals develop symptomssymptoms
• Symptoms vary by route of exposure - Symptoms vary by route of exposure - can be aerosolized or introduced into can be aerosolized or introduced into food systemfood system
Staphylococcal Enterotoxin BStaphylococcal Enterotoxin B(SEB)(SEB)

• Sudden onset of high fever, headache, chills, Sudden onset of high fever, headache, chills, muscle aches, and non-productive cough, and muscle aches, and non-productive cough, and malaise.malaise.
InhalationalInhalational:: Severe shortness of breath & Severe shortness of breath & chest pain with larger doseschest pain with larger doses
IngestionIngestion: : Nausea, vomiting, and diarrhea Nausea, vomiting, and diarrhea
SEBSEBSigns & SymptomsSigns & Symptoms

• Supportive Care: Oxygenation Supportive Care: Oxygenation Hydration Hydration
• Most victims will recoverMost victims will recover• No vaccine availableNo vaccine available• No antibiotic is effectiveNo antibiotic is effective
SEBSEBTreatmentTreatment




















![[Toxicology] toxicology introduction](https://img.dokumen.tips/doc/110x75/55c46616bb61ebb3478b4643/toxicology-toxicology-introduction.jpg)