Embed Size (px)
Citation preview
Assessment of the lower extremities of the elderly client
Item Type text; Thesis-Reproduction (electronic)
Authors King, Patricia Ann, 1933-
Publisher The University of Arizona.
Rights Copyright © is held by the author. Digital access to this materialis made possible by the University Libraries, University of Arizona.Further transmission, reproduction or presentation (such aspublic display or performance) of protected items is prohibitedexcept with permission of the author.
Download date 23/07/2018 17:36:43
Link to Item http://hdl.handle.net/10150/348202

ASSESSMENT OF THE LOWER EXTREMITIES OF THE ELDERLY CLIENT
by-Patricia Ann King
A Thesis Submitted to the Faculty of the .COLLEGE OF NURSING
In Partial Fulfillment of the Requirements For the Degree ofMASTER OF SCIENCE
In the Graduate CollegeTHE UNIVERSITY OF ARIZONA
1 9 7 7

STATEMENT BY AUTHOR
This thesis has been submitted in partial fulfillment of requirements for an advanced degree at The University of Arizona and is deposited in the University Library to be made available to borrowers under rules of the Library.
Brief quotations from this thesis are allowable without special permission, provided that accurate acknowledgment of source is made. Requests for permission for extended quotation from or reproduction of this manuscript in whole or in part may be granted by the head of the major department or the Dean of the Graduate College when in his judgment the proposed use of the material is in the interests of scholarship. In all other instances, however, permission must be obtained from the author.
SIGNED:
APPROVAL BY THESIS DIRECTOR This thesis has been approved on the date shown below:
/OJESSIE V. PERGRINs ? Date
ociate Professor of Nursing

ACKNOWLEDGMENTS
I would like to express my gratitude to all those involved in this research study.
The members of my committee, Dr. Jessie V. Pergrin. Chairperson, Mary Opal Wolanin, Dr. Karen Sechrist, and Dr. Alice J. Longman provided interest, enthusiasm, support and advice.
My family provided patience and understanding throughout the course of the study. In particular, my son, Thomas, deserves recognition for the illustrations he drew for the assessment tool.
Dr. Eleanor Bauwens furnished a valuable suggestion at a critical point in the study.
My gratefulness is also extended, to the nurses and clients who participated in the study.

TABLE OF CONTENTS
PageLIST OF TABLES . . . . . . . . . . . a . . . . . . . . viLIST OF ILLUSTRATIONS . . . . . . . . . . . . . . . . . viiABSTRACT . . o.'o o o . . . o o o . . o . . . . . . . 13» 11. INTRODUCTION . . . . . . . . . . . . . . . . . . . 1
Statement of the Problem . . . . . . . . . . . . . 3Significance of the Problem . . . . . . . . . . . . 3Purpose of the Study . . . . . . . . . . . . . . . 4Conceptual Framework . . . . . . .. . . . . . . . . 4
Structure and Function: of the Human Foot .... . 4The Geriatric Foot . . . . . . . . . . . . . . 6Foot Disability in the Aged . . . . . . . . . . 7
Assumptions . . . . . . . . . . . . . . . . . . . . 16Definitions . . . . . . . . . . . . . ... . . . . . 16Limitations . . . . . . . . . . . . . . . . . . . . 16
2. REVIEW OF THE LITERATURE . . . . . . . . . . . . . 17Foot Problems in the Aged . . . . . . . . . . . . . 17"The Foot" in the Nursing Literature . . . . . . . 24
3. METHODS e e 0 6 6 0 0 e e e e 0 e e e 0 . e e a ee 23Research Design . . . . . . . . . . . . . . . . . . 28The Nursing Assessment Tool . . . . . . . . . . . . 30
Criteria for the Classification Scheme . . . . 31Structure of the Classification Scheme . . . . 32
The Revised Tool . . . . . . . . . . . . . . . . . 35Guide to the Use of the Tool . . . . . . . . . . . 36Population and Sample . . . . . . . . . . . . . . . 36Data Collection . . . . . . . . . . . . . . . . . . 37Data Analysis . . . . . . . . . . . . . . . * . . . 33
4. REPORT OF FINDINGS . . . . . . . . . . . . . . . . 39Pre-Test Phase . . . . . . . . . . . . . . . . . . 39
Characteristics of the Sample . . . . . . . . . 39iv
VTABLE OF CONTENTS (Continued)
PageDescription and Analysis of the Data 40Nurses1 Evaluation of the Tool .« «,,<, = . » 40
TeSt Phase o o o e o o o o o o o o o o o o e : « o o ' 4 2Characteristics of the Sample 42Description and Analysis of the Data . . . . . . 42The Reliability of the Items . . . . . . . . . 48
5. DISCUSSION, CONCLUSIONS, IMPLICATIONS, ANDRECOMMENDATIONS . . . . . . . . . . . . . . . . . 58
F m d m g s . . . . . . . . . . .. .. .. . . . . . 5 9. Reliability of Test Items . . . . . . . . . . . . . 60Nurses * Evaluation of the Tool . . . . . . . . . . 65Cone 1 ulsxons . . . . . . . . . . . . . . . . ., . . . 67Implxcatxons . . . . ... . . . . . * . @ . . . . . 69Recommendations . . . . . . . . . . . . . . . . . . 70
6. SUMMARY . . . . . . ....... . . . . . ' . . . . . . 72APPENDIX A: NURSES' EVALUATION FORM . . . . . . . . . 76APPENDIX B: NURSING ASSESSMENT OF THE
GERIATRIC FOOT . . . . . . . . . . . . . . 77APPENDIX C: REVISED TOOL . . . . . . . . . . . . . . . . 85APPENDIX D: GUIDE TO THE NURSING ASSESSMENT OF
THE,GERIATRIC LOWER EXTREMITY. . . . . . . 91LITERATURE CITED . . . . . . . . . . . . . . . . . . . 92

LIST OF TABLES
Table Page1. Clinical findings from Helfand's (1973)
survey of the foot problems of an elderlyP O p U . l a t r O n ; O' o o o o o o o o o ' o o o e o o o o o 2 2
2 o Sample format of the classificationsexpansion of the category "footgear" , . , , . = 33
3 o Sample format of the classifications . „ expansion of the category "structural
deformities « o o o o o o o o o o o o o o o o o 3 44 o Sample format of the classifications
expansion of the category "dorsalispedis pulse @ 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 * 0 3 5
5. Distributions of mobility status ofelderly clients, by type,of residency .■. » « , . 44
6. Distributions of conditions limiting ambulation of elderly clients, by typeof residency 0 * 0 0 0 0 0 0 0 0 0 0 0 0 0 0 * 0 44
7 o Distribution of clinical findings, byresidency type * * . . * . . . . * . * * * . . . 45
8. Percent agreement between nurse observers in the assessment of elderly clients'lower extremities . . . . . . . . . . . . . . . . 49
9, Percent no response, percent agreement, percent disagreement for items receivingless than 70, percent agreement . * . . * * . . * 52
10. Revised percent agreement between nurse observers in the assessment of elderlyclients' lower extremities . 53
11. Final categorization of the percent agreement between nurse observers in the assessment of elderly clients' lowerextremities 55
vi

LIST OF ILLUSTRATIONS
Figure Page1. Bones of foot, dorsal view 5
2 o Causes of foot pain and disability « ° « . . . , g

ABSTRACT
Recognition of geriatric foot problems by the nurse would be facilitated by an assessment tool which is systematic , clear, and concise. This study focused on the development and testing of such a tool.
Once the tool was developed it was tested for . reliability. Two foot assessments on the same individual were made by a pair of nurses, working independently, within a three day period. Forty-six; clients, and 20 nurses participated in the study.
in measuring the reliability coefficient, a percent agreement was computed for each of the 47 items in the tool, in which a level of .70 was arbitrarily chosen as the lowest acceptable level of reliability. Twenty-nine of the 47 items showed 70 percent or above agreement between the nurse observers and are considered highly reliable.Six items received 65-75 percent agreement and are considered reliable. Six items received 55-65 percent agreement and are moderately reliable, while six items . received 40-55 percent agreement and have low reliability.
The findings suggested that the structured tool provided an objective means of data gathering for those items receiving 65 percent or above agreement.
vxix

CHAPTER 1
INTRODUCTION
Older Americans have often been confronted with foot problems which were "painful and debilitating, but it was not until fairly recently that attention to their needs in relation to foot care have been recognized by health care professionals. In 1961, the Second White House Conference on Aging reported that prophylactic foot care for the aged was conducive to their total well-being.Later, federal legislation was enacted which provided for podiatry services under the Medicare program.
Foot disability can lead to serious consequences for the aged person. Once he is no longer able to ambulate freely, for whatever reason, his independence is curtailed, and his psychological well-being is affected. Feelings of helplessness may curtail his rehabilitation (Helfand, 1970) . Furthermore, his social life space may be confined, making him a potential social isolate. Thus, the importance of foot health for the elderly person is being recognized as essential, not only for his total well-being, but for the prevention of complications that may be associated with chronic disease.

Older persons often have one or more chronic diseases with associated foot problems that go unrecognized for various reasons. For example, poor vision or an arthritic condition may simply prevent the older person from giving attention to his feet. In a general assessment of the elderly client, then, it is important to include inspection of the feet.
Podiatrists have noted the importance of the nurse' role in recognizing foot disorders in the elderly. HeIfand (1971a, p. 30) writes that the "nurse should be trained . . .to identify foot lesions, swellings, and otherirregularities and to notify the podiatrist when they are found." Simko (1974) expressed the same idea when he urged nurses to play a more direct role in teaching, assisting with foot hygiene, and recognizing foot problems„ McGregor (1968) states that since the nurse is very often central to the patient’s life, she serves as a vital link between the patient and the podiatrist.
Recently, in the nursing literature, more attention has been directed to the role of the nurse in feet evaluation. Spencer (1970) and Anderson (1971) both stress the need for nurses to become directly involved in foot assessment. Martin and Smith (1969) and Hopp and Sundberg (1974) have developed foot assessment tools. However, these are limited in scope and do not provide a systematic approach

to assessing the foot. What is needed is a structured tool which can be used by nurses to make accurate observations of the older person's feet.
Statement of the Problem Recognition of geriatric foot problems by the nurse
would be facilitated by an assessment tool which is systematic, clear, and concise. This study focused on the development and testing of such a tool.
Significance of the Problem The writer's interest in the aging foot is the
result of my clinical experience in a podiatry mobile clinic for senior citizens. Seeing and working with the various foot problems of the aged and noting their immense relief after receiving treatment were convincing enough to decide that foot problems are significant for this group. Nurses can play a key role in this area by (1) recognizing the need for foot health maintenance, and, more importantly,(2) becoming directly involved in assessing the foot. By carefully examining the foot in a systematic manner, the nurse can often provide.the. necessary intervention that is crucial in either maintaining or restoring foot health in the aged.

In searching the nursing literature, no systematic tool for assessing the foot was found. The need for such a tool appeared to be indicated.
Purpose of the StudyThe purpose of this study was to develop an instru
ment for Systematic observations of the geriatric foot which was clear, concise, and practical. Once the tool was developed and revised it was tested for reliability.
Conceptual Framework
Structure and Function of the Human Foot
The human foot has been defined as an "intricate mechanism that functions interdependently with other components of the locomotor system" (DuVries, 1973, p. 3). Gamble and Yale (1975, p. 187) define the foot as a "mobile framework of individual bones of correct conformation that are aligned for maximal structural stability and functional efficiency."
The complexity of the foot is apparent when one identifies the structural components. There are 26 bones, which are divided into three groups: the seven tarsalsof the tarsus? the five metatarsals of the metatarsus; and the phalanges of the toes, of which the great toe has two and each of the others has three (see Figure 1). In

5
5 Distal Phalanges
4 Middle Phalanges
5 Proximal Phalanges
1st to 5th Metatarsals
Cuboid1st, 2nd, and 3rd CuneiformNavicular
CalcaneusTalus
Figure 1. Bones of foot, dorsal view.From Henri L. DuVries, Surgery of the Foot, 1959, p. 22.

6
addition, there are accessory bones, six ligaments, and, for the plantar surface, a specialized fascia and four layers of muscle.
Kinetic and static functions are performed by thefoot. When the foot acts to support the body, in standing,it is performing a static function, while its action in "providing leverage for propulsion" during walking is a kinetic function (DuVries, 1959, p. 49).
The Geriatric FootThe geriatric foot shows the effects of the "ravages
of time, abetted by the static stresses imposed by weightbearing and shoes (Jahss, 1971, p. 327). McGregor (1968) has classified the aging foot into two types ? the normal healthy foot and the abnormal unhealthy geriatric foot.
The normal healthy geriatric foot shows signs ofthe physiological changes that occur with aging. The skinis atrophic, dry, and scaly, with loss of hair and skin elasticity (Helfand, 1967). The nails appear striated and brittle (Helfand, 1967; McGregor, 1968). Sensation is diminished (McGregor, 1968) and there is diminished blood supply (McGregor, 1968; Jahss, 1971).
The abnormal, unhealthy foot is one "which brings to its aging phase pre-existing faults which are magnified by the natural aging effects. The pre-existing hammer toe.
7complicated by diabetes and insufficient blood supply, is a good example" (McGregor, 1968, p. 687).
Foot Disability in the Aged
Riccitelli (1966) has classified the major causes of foot pain and disability in the aged and infirm into five categories: mechanical, arthritic, circulatory,dermatologic, and neurotrophic. A model adapted from his classification scheme is shown in Figure 2. Although these categories are somewhat arbitrary, they nevertheless will guide this study. Each of the above factors will be examined , along with the underlying physiology» The circulatory factor is in the greatest detail, since it appears to be the most significant.
Mechanical Stressors and the Feet. Helfand (1971b, p. 379) categorizes mechanical stressors into two types; macrotrauma and microtrauma. The former is due to a sudden injury to the foot resulting in fracture, while the latter results from the life time small injuries to the foot, either from occupational activities, overweight, poor stance, and gait, and poor fitting shoes.
Ligament and muscles are capable of withstanding daily stresses and strain. However, prolonged stretching can lead to pain, as in the case of standing for hours on a hard surface or wearing improper shoes (Riccitelli, 1966).

8
Circulatory Changes
Arthritic Diseases
Mechanical Factors
Neurotrophic Lesions
Dermatologic. Lesions
DiabetesNeurological
lesions
Foot DisabilityFoot Pain
111 fitting shoes
Improper walking habits
Deformities
Improper foot care
Neglect Infections Vascular and
Metabolic Disorders
Diabetes Cardiac
disorders Hypertens ion Peripheral Vascular Disease
Figure 2. Causes of foot pain and disability.This illustration was adapted from Riccitelli * s, 1966, "Foot Problems of the Aged and Infirm".

9Constant pressure or friction in the feet from poorly fitting shoes or improper walking habits may lead to the formation of calluses, corns, or ingrown toenails (Ricci- telli, 1966).
Other mechanical causes of foot strain to the older person include: hallux valgus (displaced great toe), andhammer toes„ "
Arthritic Diseases and the Feet. Chronic arthropathies such as hypertrophic arthritis and osteoarthritis are frequently found with neuropathic and metabolic disturbances, chronic infections or trauma (Riccitelli, 1966, p. 1059). In the parly phase, according to Riccitelli,"bony lipping and spur, formations appear along the articular margins of the bones in the foot" followed by a narrowing of the joint spaces, progressing to marked bony deformities in the advanced phase.
Rheumatoid arthritis commonly affects the feet (Jahss, 1971, p. 328), notably the joints (Riccitelli,1966). Riccitelli states that bone atrophy and degenerative changes in the cartilage occur as the disease progresses, leading to areas of bone destruction, ankylosis, hypertrophy and deformity in the advanced state of the disease.
Gout, also, commonly affects the foot, notably the bones, but unless the great toe is involved , the diagnosis may be missed (Riccitelli, 1966). Jahss (1971, p. 328)

10points out that in the aged, the presence of hallux rigidus is highly suggestive of gout.
Circulatory Changes and Foot, Pain and Disability.Of all the changes, in the aging foot, the diminished blood supply is one of the most significant« Jahss (1971) assumes that there is marked circulatory impairment of the foot from arteriosclerosis in persons past 65 years and from arteriolar sclerosis in diabetics by the time they are 45 years of age. The consequences which follow from this impairment may be severe, according to Jahss. He notes that slight fissures in the skin of diabetics may lead to infection and gangrene. For persons with advanced arterial insufficiency the same effects may follow from.minor trauma, a surgical procedure, or the application of a strong keratolytic agent (Jahss, 1971, pp. 327-328). Wilkins (1967, p. 728) states that "in elderly patients atherosclerosis is the leading cause of ischemic peripheral vascular disease. ” Hoerner (1967, p. 164) notes that: (1) one of the most importantproblems in an aging population is the universal development of arteriosclerotic changes resulting in vascular insufficiency and (2) there exists a high prevalence of diabetes among the aged, in which arteriosclerosis obliterans is the most common complication. Juergens and Bernatz (1972) state that ulceration or gangrene can be caused from

. 11 normal pressure from shoes in ordinary walking, in the case of ischemic toes.
Several authors have noted the importance of the feet in manifesting the first signs of"systemic disease. Wilkins (1967) calls attention to the digits of the extremities as being particularly vulnerable, both because they are situated at the periphery of the vascular tree and because they are often, times subjected to trauma and to variable temperatures. Riccitelli (1969, p. 205) notes that "the feet are often the site of many initial signs and symptoms, not only of peripheral vascular disorders, but also of systemic diseases."
For this study, then, knowledge of the physiology of the peripheral vascular system is not only appropriate but basic to understanding the pathologic changes of peripheral vascular disease.
The circulation performs three functions for peripheral tissue: (1) it furnishes the tissues' metabolicneeds, (2) it removes the tissues' waste products, and(3) it maintains the tissues' temperature within a normal range.
The circulation furnishes tissue needs by supplying "a certain volume of blood to a unit volume of tissue in a unit time (milliliters of blood flow per 100 ml) of tissue per minute" (Wilkins, 1967, p. 724). Thus, the rate of

12blood flow can serve as a key indicator of circulation status, since a "deficiency Of blood flow at rest or a relative deficiency upon demand is the chief cause of the signs and symptoms of peripheral ischemic disease" (Wilkins, 1967, p. 724). Riccitelli (1969, p. 208) states that "most of the signs and symptoms of peripheral vascular disease are due to the inadequate flow of blood."
Both physiologic and pathologic disturbances can lead to a decrease in blood flow, according to Wilkins. Variation in blood flow is dependent upon (1) the pressure gradient and (2) the resistance to flow. Wilkins defines pressure gradient as "arterial to venous fall" and gives . examples of factors which would cause the gradient to lose its stability: either a rise in venous pressure, arisingfrom valve malfunction, or a decrease in local arterial pressure because of a proximal obstructive lesion or an arteriovenous shunt. Peripheral resistance is defined as "the caliber of the arterioles and precapillary sphincter" (Wilkins, 1967, p. 724). These structures are the most. significant in total resistance of the system and are dependent on two forms of control: (1) reflex control and(2) local control.
\Reflex control, vis-a-vis the sympathetic nervous system, generally causes vasoconstriction, which, in turn, increases peripheral resistance. This vasoconstriction

13occurs to a greater degree in the hands and feet, as compared to the muscle of the extremities. Wilkins' (1967)argument for these assertions are that the skeletal system controls its own blood supply, operating, for the most part/ independently of the sympathetic nervous system. Thus, "pathologic overactivity of the sympathetic nervous system usually manifests itself as ischemia first in the skin of feet or hands, rather than in more proximal portions of the . extremities" (Wilkins, 1967, p. 725).
Local control can also affect alterations in peripheral resistance, as in the case of vasodilator metabolites. Other factors affecting muscle directly include: local temperature, epinephrine, nitrite> and histamine.
It is important to note that tissues are more vulnerable to trauma and infection, if there is peripheral vascular impairment (Hoefner, 1967; Riccitelli, 1969).
In summary, the signs and symptoms of peripheral vascular disease are directly related to the degree of blood flow. The greater the deficiency of blood flow, the greater the circulatory disturbance and the greater the manifestations of peripheral vascular disease.
Dermatologic Lesions of the Feet. Riccitelli (1966, p. 1064) states that the older person is more susceptible to bacterial and fungal infections, to trauma, and to cold. In addition, he points out that chronic

14infections, ulcerations, calluses, corns and plantar warts are common in association with vascular and metabolic disorders . Abnormal pressures and irritations from ill-fitting shoes, improper foot care, neglect and infections are singled out as causing most of the skin lesions in the elderly foot.
The presence of hyperkeratotic lesions (corns or callus) at pressure points on the foot are manifestations of internal or external pressure (Helfand, 1971a, p. 382). Rakow and Friedman (1969, p. 137) point out the potential danger of these lesions. According to them, if a corn or callus is allowed to grow, the build up of the stratum corneum may exert pressure on the subcutaneous tissue, resulting in necrosis, and ulceration.
Nail problems in the aged are noteworthy. Three conditions which appear to be most troublesome for the older person are:
(1) Thickening of the nail plate (onychauxis).Helfand (1971b, p. 381) points out that this condition is related to aging, repeated trauma, inflammation, local infection, and various.degenerative diseases, such as arteriosclerosis.
(2) Ingrown toenail (onychocryptosis). According to Helfand, this condition occurs when a fragment of nail penetrates the skin of the nail lip. He lists self treatment

15or external pressure as possible causes and notes the seriousness of this condition for persons with diabetes or arteriosclerosis«
(3) Fungus infection of the nail (onychomycosis). Helfand. (,1971b) states that the nails appear opaque, scaly and hypertrophic and will always remain the focus for infection and reinfection. If a pungent odor or yellow striations are present, suspect a fungus infection (Rakow and Friedman, 1969, p. 136).
Neurotrophic Lesions of the Foot. Kelly and Coventry (1958, p. 388) state that neurotrophic ulcers of the feet are a result of damage to sensation, either peripheral or central in origin. Riccitelli (1966, p.1063) notes that when there is a break in the sensory nerve supply to the foot the superficial tissues are highly susceptible to the slightest trauma, resulting in an indolent ulcer which may become infected. Two important symptoms which, he states, may be the first signs of a serious internal disease are (1) itching and (2) burning of the feet. '
Kelly and, Coventry (1958) point out that diabetes, Complicated by peripheral neuropathy, is the most frequent cause of neurotrophic lesions. However, a neurologic lesion should be suspected whenever one finds abnormal

, 1 6reflexes or changes in tactile or vibratory sensations in the feet (Riccitelli, 1966, p„ 1062)„
Assumptions1. Nurses can play an important role in foot health
maintenance for the elderly„2. Systematic observations of the geriatric foot
require an instrument which is clear, concise, and practical.
Definitions ■1 o Podogeriatrics is defined as "the area of
podiatry dealing with the human foot in the aging process (HeIfand, 1971a, p. 30).
2. Assessment of the geriatric foot refers to the gathering of information (objective and subjective) on the health status of the geriatric foot and the making of decision(s) regarding the deficit (s) or potential deficit(s) in the foot health status of individuals (adapted from Block, 1974).
Limitations1. The age of the clients participating in this
study was limited to those 60 years of age or over.2. The number of clients assessed in this study
was limited by the number of nurses participating in the. study.

CHAPTER 2
. REVIEW OF THE LITERATURE
This chapter reviews the medical, podiatry, and nursing literature for studies on the foot problems of the elderly. In particular, a search was made for assessment tools for the feet.
Foot Problems in the AgedThe foot is perhaps the most neglected area of the
human body. According to F . W. JoneS (1944, p. 3), "it isprobably the experience of most teachers of anatomy that thestudent is generally better acquainted with the intimate structure of the hand than with the foot." In the past, foot pathologies were thought to be caused by fallen arches and treatment was directed at prescribing arch supports, satisfying the practitioner that all that could be done was done, despite the fact that the patient1s feet continued to hurt (DuVries, 1959, p . 13).
The foot is unlikely to be the cause of mortality, but it is often the cause of the site of morbidity, disability, and limitation of activity (Helfand, 1971b, p.377). Foot problems are more likely to manifest themselves in the elderly population. Simko (1974) notes that foot

18problems are ranked as the "fourth most common cause of discomfort in the elderly" in the Veterans Administration Program Guide for Nursing Care of the Long-Term Patient.
The first large scale survey of the foot problems of institutionalized geriatric patients was conducted in 1968. This survey, under the direction of HeIfand (1969) was the first of a five year series directed towards:(1) bringing to the attention of the health services community the high incidence of foot problems in an elderly population and (2) demonstrating a methodological approach for screening foot problems in an elderly population. The sample consisted of all the residents of a state geriatric institution and the foot evaluations were conducted by podiatry students. Podiatric services had been initiated shortly before this survey began, but they were limited to two hours per week.
The initial group was comprised of 551 patients, of which 82 percent were between the ages of 65-79. The clinical findings revealed that a typical patient had one or more foot complaints, one or more reported serious chronic diseases, almost two dermatologic problems involving the foot, more than one sign of fixed foot deformity, and about two symptoms of peripheral vascular disease.
Five years later, HeIfand (1973) reported the results of the longitudinal survey on this group. First,

143 patients remained in the study, or 26 percent of the original group. Second, there was a significant increase in the number of patients who noted past histories of heart disease, high blood pressure, arthritis, circulatory involvement and diabeteso Third, an increase was noted in the percentage of static and functional deformities, as shown in Table 1.
The increase in onychauxis, hallus valgus, digit! flexus, trophic changes, and peripheral vascular impairment led Helfand to conclude that foot care was vital for this group, in order to maintain their ambulatory status. Furthermore, he asserted that the lower infection (2.0-1.3 percent) and ulcer art ion (4. 2-3«5 percent) rates during the five year period showed that a podiatry program could be instrumental in reducing foot complications. (It should be noted that a podiatrist was employed full time in the second year of the survey.)
Another study by HeIfand (1968) focused on the foot problems of a non-institutionalized elderly population in the city of Philadelphia. Over a three year period of time, as part of a "Keep Them Walking Project," 1366 citizens were screened for foot problems. The sample was self- selected (reached through the Senior Citizen Centers) and the average person was over 65, female, living alone, and on a fixed income. The,study results showed that

20Table 1. Clinical findings from Helfand's (1973) survey
of the foot problems of an elderly population.
PercentageProblems First Year (1968)
N = 551Fifth Year (1972)
. N = 143
Onychauxis 41.6 60.1Hallux valgus 37.7 55.2Digiti flexus 30.7 46.9Trophic changes 22.0 37.1Dorsalis pedis
absent.31.2 46.1
approximately 95 percent of all these citizens had some foot problem or pedal manifestation of a systemic disease. Seventy four percent of the study population stated that their feet hurt them at the time of the exam and fewer than 3 percent of the total sample had no foot complaints.Of the clinical findings, hyperkeratosis was found in 1076 cases (78 percent), while onychauxis (thickened nails) was found in 624 cases (45 percent). The latter condition, according to Helfand, may be due to the older person's difficulty in bending and seeing to cut the thickened nails. Fifty percent of the sample had dry skin, while infection was found in 60 cases (4 percent), which largely resulted

21from complications from commercial remedies and self- treatment. Helfand concluded that older people do have multiple foot problems as a result of disease, deformity, impairment, disuse, and degenerative changes from the aging process.
Hsu (1971, pp. 880-885) reviewed the cases of those patients attending the outpatient foot clinic in the Baltimore City Hospitals, over a three year span. Of those reviewed, 62 percent (426) were patients 65 years of age or older. The types of disorders which caused foot pain and disability in this group were: circulatory (31percent), structural (21 percent), nail and skin problems (36 percent), neurogenic (8 percent), and miscellaneous (4 percent). Thus, the greatest percentage of foot problems were due to dermatological conditions, followed very closely by circulatory conditions, which, the author states, were mainly associated with diabetes. In his discussion, Hsu directed attention to the importance of early recognition of foot problems in the aged person, noting that delay can lead to severe consequences, such as, loss of mobility, loss of independence, loss of motivation and self-assurance. In particular, he asks medical, nursing, and paramedical personnel who deal with the aged to "inquire about the condition of the feet . , . no problem, however small or insignificant, should be overlooked" (Hsu, 1971, p. 885).

22The significance of trophic foot changes in the
aged is noted by Rakow and Friedman (1969)„ They reviewed the cases of 201 elderly patients (7 percent were under 60) who entered a chronic disease nursing unit, over a three year period. These residents, upon admission to the unit, were given a foot examination,, followed by periodic evaluation and podiatrie care. They found that a great majority (80 percent of the residents) had pulseless feet and 90 percent had one or more of the following: (1 ) thick,dystrophic or ingrowing nails (or both), (2) hyperkeratosis, either, thick clavi (corns) or excessive callus, and (3) dry skin. in addition, they found that thickening of the toenails' was significantly more prevalent in patients with peripheral arterial disease. They concluded that asymptomatic foot lesions, which may lead to necrosis and infection, are quite common in the elderly and are potentially harmful because of circulatory impairment.
A notable study by HeIfand (1974) focused on a screening program for pedal complications in diabetes.During a ten week period, a random sample of diabetic patients attending a regularly scheduled clinic in a University hospital were evaluated by a podiatric team.A total of 123 patients were screened, of which 52 females and 18 males were 56 years of age or older. In the clinical findings, hyperkeratotic lesions comprised a large majority

of the foot lesions (72.3 percent) while a majority (64.2 percent) had dry skin. In addition, the following problems were noted: onychauxis (42.2 percent); ulceration withvarying degrees of necrosis (6.5 percent); onychomycosis (47.9 percent). The average patient had more than two foot complaints, was being treated for two systemic diseases, and had two overt signs of peripheral vascular involvement. Probably the most significant findings were that a large majority of these patients were not receiving any form of foot care and education on foot care was minimal. This study showed the need for foot assessment and foot health education for diabetic patients and the need for podiatric services in a diabetic care program.
The seriousness of "minor" foot lesions in diabetics is apparent from the investigation conducted by Hoerner (1967). He analyzed the data from 549 diabetics during two time periods: 1936-1941 and 1946-1965. He found thatcorns, calluses, ingrown toenails, fissures and cracks in the skin, and blisters associated with infection, osteomyelitis, or gangrene were the cause of 157 toe amputations, 19 transmetatarsal amputations, 5 amputations below the. knee and 17 above the knee. In his summary, the author (1967, p. 174) stated that "constant attention to foot hygiene and prophylactic care of extremities are essential in order to save the parts."

24"The Foot" in the Nursing Literature
Traditionally, foot care has been given little attention in nursing textbooks. Perfunctory remarks about cleanliness, the use of creams, and exercise are made„ For the most part, the assumption seems to be that the feet, as the invisible appendages of the body, require little nursing care. The exception here would be in the case of the diabetic foot, but here again, stress has been placed mainly on the negative aspects or "don'ts" of foot care rather than on the positive aspects of foot health maintenance.
In recent years, a change from1 this traditional approach has been noted. More,emphasis is being given to foot problems, foot inspection, and foot care.
Bruck and Lambert's (1959) article on common foot disabilities appears to be the first one in the nursing journals. It was their thesis that early attention to foot discomfort and irritation tends to prevent disabling deformities of the feet.
Rietz (1968) notes that the first intensive course in foot care for the elderly, conducted by podiatrists, was held at the University of Nebraska in 1966, for 60 nurses who were working in institutional settings for the aged.

25Spencer (1970) alerted nurses to the importance of
foot health for the elderly and to the nurse's direct role in assessment of the elderly foot. According to her,"nurses in both institutional and public health settings are important figures, in recognizing patients' needs for maintenance and restorative foot care" (p. 76). Spencer's article not only introduced a new term, podogeriatrics, but provided a mini-course in foot care by (!) including three previously published articles on this subject and (2) 'giving details on basic foot inspection and foot exercises for nonambulatory patients. Specific roles recommended for the nurse included: (1) observing and recordingfoot problems, (2) making foot care part of the nursing care plan, (3) initiating communication with a podiatrist, and-(4) including foot care requirements in discharge planning.
Other contributions to the nursing literature on foot inspection are as follows. Anderson (1971) discusses nursing assessment of the foot in relation to peripheral vascular diseases, in which the author advocates a foot inspection at the time of the patient's admission to the hospital and at regular intervals thereafter. Fowler (1974) directs the nurse's attention to the "Great Right Toe" as an important part of the body to assess, since this body part may yield clues to systemic conditions. Simko

26(1974, p. 63), a podiatrist, urged nurses to "examine a patient's feet for neglected corns, calluses, over-developed nails, mycotic nails (fungus nails), fissures, lesions, plantar warts, and athlete's foot or other skin rashes.Until such conditions are relieved, the discomfort they cause may seriously retard the patient's rehabilitation."
An important clinical investigation was conducted by Martin and Smith (1969) on the relationship between patients' knowledge and actual practice of foot care. Twenty-six maturity-onset diabetic,patients, 17 males and 9 females, outpatients at Metropolitan Hospital, New York City, ranging in age from 49-82 years were the subjects of the study. The authors designed two instruments; (1) a questionnaire, which evaluated the patient's knowledge of foot care and (2) an observation tool, which assessed the patient's actual practice of foot care. They found that these patients were not practicing safe foot care and concluded that they were poorly informed about foot care.
A notable study by Hopp and Sundberg (1974) focused on the effects-of soaking and"lotion on dry skin in the feet of the elderly patient. The authors developed a tool for assessing the general condition of the foot, using items relating to skin conditions, such as calluses, lesions, or fissures. In addition, they constructed a dryness scale for assessing the texture of the skin.

27The literature has shown that older persons are
confronted with multiple foot disorders which can lead to disability, limitation of activity, loss of motivation, and self-assurance. In the past, little attention was given to their foot problems, but this situation has changed in recent years. Increasingly," documentation has been given to the needs of the elderly relating to foot care by members of the medical, podiatry, and nursing professions.
Since foot disabilities can be so devastating to the oider person, early recognition of foot problems assumes paramount importance. Screening tools, which facilitate early recognition, have been developed for podiatrists, but. these are inappropriate for nurses to use. No structured nursing assessment tool was found.

CHAPTER 3
METHODS .
This study focused on the development and testing of an assessment tool for the lower extremities of the elderly client. This chapter includes the research design, the general procedure and rationale for developing the assessment tool, the population and sample, and the data analysis.
Research DesignThe first phase of the study dealt with the con
struction of an assessment tool which would assist nurses in making systematic observations of the feet of clients 60 years of age and over. In constructing the tool, the primary aim was to produce an instrument that was relevant, valid, and reliable.
After the tool was completed, it was presented to the following:. (1) five members of the nursing faculty at The University of Arizona, (2) a podiatrist, and (3) a podogeriatric nurse. These experts made recommendations regarding format and content and agreed that the tool had content validity.
28

29The second phase, pre-testing the tool, was then
initiated for the following reasons: (1) to establishareas of the tool needing revision and (2) to determine whether the tool could be used within a limited time period. Following Hamdi and Hutelmyer (1970, p. 356) five pairs of nurses each made independent assessments on two clients, for a total of ten pairs of observations. A comparison of the results was made to evaluate the amount of agreement or disagreement between the pairs of nurse observers.
The nurses^ who.had volunteered, were recruited by the researcher from the following sources: (1) the graduatestudents in the College of Nursing, (2) the faculty in the College of Nursing, and (3) nurses from a licensed health care facility. The older persons, who had also volunteered, were recruited from: (1) a municipally operated complexfor elderly citizens with limited income and (2) a licensed health care facility. The assessments were done within a three day period. After completion of the assessment, each nurse was asked to evaluate the tool (see Appendix A).
Following changes in format, content, and terminology, the third phase, testing the tool for reliability, began. The directors of nursing in two licensed health care facilities were contacted to obtain permission to conduct the study. In one of the facilities, a meeting was held with two of the staff nurses, in which the purposes

of the study was explained and the tool was reviewed. In both of these facilities, copies of the tool were left for staff review.
A total of 41 clients each had two foot assessments by a pair of nurses, working independently, making 41 pairs of observations. One of the assessments was by the researcher and one was by a nurse volunteer, with the following exception. Two clients.from another city were assessed by two nurses from there.
At the conclusion of the study, the reliability of each of the 47 items in the tool was established by comparing the paired observations for agreement or disagreement across, all 41 cases. For each item a percent agreement was computed.
The Nursing Assessment ToolOne of the basic requisites for constructing an
observational instrument is a "linguistic base that is well defined, clearly understood, and systematically used" (Jones, McNitt, and Mcknight, 1974, p. 5). That is, the researcher needs a descriptive schema (Zetterberg, 1965, p. 57) which will be useful to him in observing the phenomena he is interested in. In addition, the need for clarity is particularly significant.. Selltiz et al. (1959, p. 392) recommend simplicity, concreteness, and a

31high degree of specificity in constructing an observational instrument.
The instrument developed by the researcher for assessing the lower extremities of clients 60 years of age and over was composed.of five parts (see Appendix B)„First, socio-demographic information was obtained on the client’s birthdate and sex. Second, a general assessment included questions on medical history, foot complaints, and observations on foot gear, mobility, gait, cleanliness, flat feet, symmetry, and varicosities. The third and fourth, portions dealt with a dermatological and circulatory assessment, respectively, while the last section dealt with an assessment for structural deformities.
The criteria for developing the assessment tool and the structure of the classification were adapted from Jones et al. (1974) .
Criteria for the Classification Scheme
The characteristics of the descriptors are asfollows:
1. They are defined in objective rather than in subjective terms.
2. They are multi-dimensional. The set of categories provide information pertaining to an older person's status from several dimensions: his medical risk status,
32- his socio-demographic status, and his foot status, A
review of the literature relating to foot problems of the aged.was made to establish relevant categories„ Riccitelli’s (1966) classification scheme provided the theoretical basis for the categories„
3» They are relevant to the purposes of this study,
Structure of the Classification Scheme
Categories were constructed in steps which proceeded from the general to the specific. Jones et al. (1974) conceived of a multilevel format, using this method. By proceeding in this manner, they argued that the person making the observations can specify the amount of detail that he considers necessary. For some items, a.minimum of detail is sufficient to describe an attribute of the person, while other items will necessitate expansion of detail to describe an attribute adequately. At the same time, by using standardized terms at each level persons can be compared within levels. The multilevel format of Jones et al. (19.74) was used in the assessment tool. An illustration of this format is shown in Table 2.
In this example, the classification is on the category "footgear". Older persons should wear shoes that are sturdy, comfortable, and well-fitting (Riccitelli,1966, p. 1065). By using the multi-level format these

Table 20 Sample format of the classification; expansion of the category "footgear".
First Level Second Level Third LevelDetail Detail Detail .
Oxford Specifies.type: leather, synthetic
Specifies condition of shoes: good, fair, poor
HeelsTennisCasualSlippersSpecial shoes Specifies type of
modification
characteristics can be identified* At the first level of detail, each person is described as usually wearing one of the following types of footgear:
Oxford shoe, including the slip-on typeLoafersTennis shoesCasual shoes, including open sandalsSlippersSpecial shoes

34For further detail, at the second level, the oxford
type shoes are described as being leather or synthetic. Finally, the condition of the shoes are specified at the third, level as being good, fair, or poor.
Another example of the multi-level format is shown in Table 3. At the first level, the classifier notes whether a deformity is present or not present. If one is present, the second level specifies the type of deformity: hammer toe, hallux valgus, or other. Finally, the third level specifies the location of the deformity— right or left foot.
Table 3. Sample format of the classification: expansion of the category "structural deformities".
First Level Detail
Second Level Detail
Third Level Detail
Not presentPresent Specifies type of
deformity: hammer toe, hallux valgus.
Specifies location of deformity: right or left foot or both

35The Revised Tool
Based on the information obtained during the pretesting phase, the assessment tool was revised in content, form and terminology (see Appendix C). The socio- demographic information was deleted, as well as questionson medical history, and the observation on flat feet. Theother parts of the tool are the same as the original.
The greatest change took place in format. Inorder to make the tool more useable, most of the categories were constructed in such a .manner as to elicit a "Yes-No" response from the nurse observer. This would constitute the first level detail, according to the scheme used in the Original tool. In some categories the second level detail was retained because of the significance of the item. An illustration of this format is shown in Table 4.
Table 4, Sample format of the classification: expansionof the category "dorsalis pedis pulse".
First Level Detail Second Level Detail
PresentNot present Specifies location:
right or left footor both

36Guide to the Use of the Tool
A guide was included with the assessment tool, in the cases where, the researcher was not able to give the instructions directly to the nurse assessor (see Appendix D).
Population and Sample Since the purpose of the study was to test the
reliability of an assessment tool, no representative sample was needed. The goal was to recruit as .many volunteers (both nurses and clients) as possible, since the greater the number, the greater the confidence in the reliability index. Accordingly, the nurses for the test phase of the study were recruited by the researcher from the following sources: (1) the senior students in the College of Nursingwho were registered nurses, (2) the graduate students and faculty in the College of Nursing, and (3) registered nurses currently employed in the local community and in another metropolitan community.
The clients, who were at least 60 years of age, were also volunteers recruited by the researcher from:(1) the residents of a municipally operated complex for elderly citizens and (2) the residents of three licensed health care facilities (two in the. local community and one in another metropolitan community). The purpose of the study, as well as its confidential nature, was

37explained to each of the potential volunteers. All persons recruited had the right to refuse to participate.
Data Collection The tool was explained to all nurses who parti
cipated in the study. In addition, each nurse (except the graduate students in geriatric nursing and the faculty member) received a guide sheet on the use of the tool (see Appendix D), It was assumed that the graduate students and the faculty member did not need additional instructions.
Two nurses, working independently, assessed each client in the study. One of these was a volunteer recruited from the above mentioned sources; the other was the researcher, who was considered the expert. In all the assessments but two, the researcher was part of the assessment pair. In this instance the two nurses were from 'another city where the observations were done.
All nurses used the tool developed for the study in assessing the clients.
The procedure for data collection in the testing phase of the study was as follows. The researcher first recruited clients and nurses for the study. Following this, each of the nurse volunteers were assigned two clients each. Within three days of the volunteer's assessment, the researcher would make another assessment on the same clients.

38Data collection began on March 11, 1976 and was
completed on April 29, 1976 =
Data AnalysisIn order to measure the reliability (consistency)
of an instrument, Kolstoe (1969, p. 174) states that one "needs at least two observations on an individual in order to determine whether the measuring instrument is doing the same thing each time," Accordingly, each of the 41 clients in this study had two foot assessments, making 41 tests of each of the items in the assessment tool.
In this study, th® researcher was interested in the question, will the item produce the same results every time a measurement is taken? Thus, the reliability of the instrument as a whole was not computed. Instead, each of the items in the instrument was considered separately and a reliability coefficient was computed for each item.For this study there were 41 pairs of observations for each of the items in the tool• It was hypothesized that there would be greater agreement between the nurse observers than disagreement on each of the items in the tool.
The reliability coefficient was computed by determining the percent agreement or disagreement, between the nurse observers across all 41 cases for each of the items in the tool. A level of .70 was arbitrarily chosen as the lowest acceptable level of agreement.

CHAPTER 4
REPORT OF FINDINGS'
This study was designed to develop an instrument for assessing the lower extremities of elderly clients.Once the tool was constructed, it was pre-tested to determine whether it was practical, clear, and concise. Following changes in format, content, and terminology the testing phase began in which the reliability of the items in the tool was established. In this chapter, data from both the pre-testing and testing phase of the study are included.
Pre-Test Phase
Characteristics of the Sample
Four graduate students and three faculty members in the College of Nursing as well as two staff nurses working in a local nursing home participated in the pretesting phase. Ten clients, 60 years of age or older, also participated; eight were from a municipally operated complex for persons with low incomes and two were from a local nursing home.
39

40Description and Analysis of the Data
Upon checking the inter-rater reliability of the two nurses' scores from the local nursing home it was determined that there was complete (100 percent) agreement between the two nurse observers on each of the items„Since total agreement is highly unlikely*without collaboration these results were disregarded. This left eight pairs of observations for the pre-testing phase. In evaluating the amount of agreement or disagreement between the remaining eight nurse observers on each of the 51 items in the tool, it was found that the agreement was 70 percent or above in 31 of the 51 items.
Nurses1 Evaluation of the Tool
In pre-testing the tool, each nurse was asked to evaluate it (see Appendix A). Six of the eight nurses Completed the evaluation form.
In regard to the length of time required to use the tool, one spent 30 minutes for the first assessment and 20 minutes for the second one, one spent 20-25 minutes on each assessment, and two spent 15-20 minutes on each assessment. The mean length of time was 22 minutes.
Four of the six nurses gave suggestions on improving the tool.
41Two nurses needed more information on how to iden
tify corns, calluses, and bunions. One nurse suggested organizing the items in such a way that (1) all the examining procedures would be together, and (2) all the questions asked of the client would be together. Another nurse suggested doing the examination before taking the client's history. One nurse questioned the value of taking the posterior tibial pulse. One nurse stated that the tool "would be useful but to be used would have to be condensed to fewer pages."
With respect to changing specific items in the tool, the suggestions were as follows: (1) identification neededas to which toe was #3, 4, or 5, (2) location should bespecified for absent pedal pulses, (3) clarification needed for "Foot Gear" item, (4) establishing a category "other" for describing a condition not included in the tool, and (5) changing the category circulatory disease, since it was not useful from the client's perspective.
Other comments were made regarding the tool by five nurses. Two nurses did not consider the tool time consuming, while one considered it lengthy, but did not know "what could be.left out." Four nurses found the tool easy to use. Additional comments included: "Complete," "Thetool appears very comprehensive and complete," "It is easily understood, except for the need of personal clarity
42of the various skin lesions . „ „," "I think it could be agood one to use just in general patient assessment when a new patient is admitted to the unit," "This tool is very good. I think if one person were doing the exam the results or observations would be more objectiveb"
Test Phase .
Characteristics of the SampleIn addition to the researcher, 20 nurses parti
cipated in the study. One was on the faculty of the College of Nursing, five were graduate students in the College of Nursing, and one was a registered nurse seeking a Bachelor of Science degree in the College of Nursing, In addition,13 were employed in a licensed health care facility, 12 of whom worked in the local community while’the other two worked in another city.
Forty-six clients were asked to participate in the study— 'five refused. Of the 41 clients willing to participate, 29 resided in a licensed health care facility and 13 lived in the local community.
Description and Analysis of the Data
Each of the 41 clients in the study had two assessments , one by the researcher (who was labeled the "expert") - and one by a nurse volunteer (who was labeled "volunteer"),

43with the following exception„ Two clients from Phoenix were assessed by two nurses from there. In this instance, the nurse with the master's degree in geriatric nursing was labeled the "expert" and the staff nurse was labeled the "volunteer”.
Table 5 shows.the mobility status for the 41 clients. Fourteen of the clients were able to walk without assistance, 13 walked with the help of equipment, 10 were confined to the wheelchair while one client was bedfast. Three clients were able to walk without assistance for a short distance, but used equipment such as a cane or walker for longer distances.
Table 6 shows that 18 of the 28 clients (65 percent) living in an institutional setting as compared to four (30 -percent) living in the community complained of a foot problem which limited their ambulation. Paralysis, a circulatory disorder, and painful extremities were most frequently cited as the cause of the limited activity.
Table 7 shows the distribution of clinical findings for the 41 clients evaluated. Almost all the clients (92 percent) had acceptable foot hygiene while almost half (49 percent) wore unacceptable shoes. Six of the clients— ■ five of whom lived in a nursing home— wore circular garters.
In the dermatological assessment. Table 7 shows that a total of 41 skin lesions and 67 toenail abnormalities

44Table 5, Distributions of mobility status of elderly
clients, by type of residency.
ItemLong Term Care Facility N=28
CommunityResidenceN=13
TotalN=41
Mobility Status Walks without
assistance 7 7 14Walks with help .
of equipment 7 6 13Does not walk 10 0 10Bedfast 1 0 1Combination 3 0 3
Total 28 13 41
Table 6. Distributions of conditions limiting ambulation of elderly clients, by type of residency.
ItemLong Term Care Facility N=28
Community Residence N—13
Total N—41
Limitation of Activity Yes 18 4 22No 10 9 13
Total 28 13 41Conditions Limiting Ambulation
Paralysis 3 0 3Circulatory disorder 3 1 4Arthritis 2 0 ‘ 2Neurological disorder 2 0 2Painful extremities 3 1 4Other 5 2 7
Total 18 4 22

45Table 7o Distribution of clinical .findings, by residency
type
Long Term Community’Item Care Facility Residency Total
N—2 8 N=13 N=41
General EvaluationFoot Hygiene Acceptable 26 12 38Stockings Satisfactory
Yes 19 7 26No 0 0 0Not Applicable 9 6 15
Total 28 13 41' "Shoes Satisfactory
Yes 11 8 19No 16 4 20No Response 1 1 2
Total 28 13 41Garters (circular) worn 5 1 6
Dermatological AssessmentSkin LesionsFissure (Toes) 2 0 2Fissure (Heel) 0 0 0Excoriation 5 0 5Corn(s) 11 6 17Callus(es) 11 5 16Plantar Wart 0 0 0Other 1 ; 0 1
Total 30 11 41Itching 1 0 1
Rash 0 0 0
Erythema (Localized) ' 8 1 9Skin Infection 1 0 1

46Table 7. (Continued)
ItemLongCareN=28
TermFacility
CommunityResidencyN=13
TotalN=41
ToenailsIngrown 0 1 1Overgrown 14 5 19Thickened 16 3 19Yellow Discoloration 16 5 21Black Discoloration 5 2 7
Total 51 16 67Circulatory Status
Discoloration (red) 23 3 26Discoloration (brown) 1 0 ' 1Dorsalis pedis pulse
absent 20 7 27Posterior tibial pulse
absent 20 8. 28Dry Skin 18 3 21Edema 17 5 22Feet Different
Temperature 5 0 5,Legs Different
Temperature . . 2 0 2Pain 9 2 11Ulceration 8 2 10Varicosities 7 6 13Total 130 36 166
Structural DeformitiesHallux.Valgus 12 6 18Hammer Toes 13 2 15Overlapping Digits 14 2 16Total 39 10 49
Legs Different Size 13 8 21
Legs Different Length 12 4 16Orthopedic Evaluation
Gait Disturbance 9 2 11

47were found. In addition, there were 166 signs or symptoms of vascular impairment, 49 cases of structural deformities and 11 cases (26 percent) of gait disturbance.
It is interesting to note the differences betwee.n the clients living in a nursing home and those living in the community. In general, those clients living in a nursing home manifested more foot problems than those living in the community. For example. Table 7 shows that they had 30 of the 41 cases (72 percent) of skin lesions,51 of the 67 cases (76 percent) toenail abnormalities,23 of the 26 cases (88 percent) of red foot discoloration,20 of the 27 cases (74 percent) of absent dorsalis pedispulse, 18 of the 21 cases (85 percent) of dry skin, and 8 of the 10 (80 percent) cases of ulceration.
Additional findings are as follows:1. One person living alone stated that she was
afraid to walk because of her fear of falling. She stated that she would, walk,more if she could get someone to walk with her.
2. One person who is wheelchair bound stated that she always wears the same pair of crocheted booties and claimed that they were four years old. (The booties were very malodorous; urine smelling.)
3. One person stated "if your feet hurt, you hurt all over." .

4. One person, living in a nursing home, stated that she could not wear shoes because her "feet are so bad This person had multiple corns and calluses and had one pair of crocheted slippers to wear.
5. One person living in a nursing home stated that her feet "feel like wood". This person has three pairs of good shoes to wear, but does not wear them. Instead, she wears crocheted booties.
The Reliability of the ItemsIn measuring the reliability coefficient of each
of the 47 items in the tool, the paired observations were compared for agreement across all 41 cases. For each item a percent agreement was computed. A level of .70 was arbitrarily chosen as the lowest acceptable level of reliability. '
Table 8 shows the percent agreement between the nurse observers for each of the items. Four groupings are displayed; Group I, items receiving 70 percent or above agreement; Group II, items receiving 60-70 percent agreement; Group III, items receiving 50-60 percent agreement; Group IV, items receiving 40-50 percent agreement.' The 26 items in Group I met the above mentioned
reliability requirement and are considered highly reliable items. The Group II items are less reliable, while the Group IV items are the least reliable.

49Table 8 . Percent agreement between nurse observers in the
assessment of elderly clients' lower extremities.
Number Number PercentItem Cases Agreeing Agreeing
GROUP IMobility 41 29 70.73Foot hygiene 41 30 73.17Stockings 41 30 73.17Garters 41 35 85.37Fissure (Toes) . 41 36 87.80Fissure (Heel) 41 38 92.68Excoriation 41 31 75.61Corn(s) 41 32 78.05Callus (es) 41 34 82.93Wart (s) 41 ■ 39 95.12Other 41 30 73.17Itching 41 31 75.61Rash 41 38 92.68Ingrown nail 41 36 87.80Overgrown nail 41 36 87.80Blacknail 41 30 73.17Discoloration (brown) 41 37 90.24Dry skin 41 33 80.49Feet temperature 41 33 80.49Leg temperature 41 38 . 92.68Nature of pain 41 34 82.93Ulceration 41 32 78.05Ulceration location 41 33 80.49Hallux valgus 41 32 78.05Hammertoes 41 35 85.37Overlapping digits 41 29 70.73
GROUP IILimitation 41 26 63.41Gait 41 25 60.98Shoes 41 25 60.48Shoe condition 41 25 60.48Redness (localized) 41 25 60.48Thickened nail 41 27 65.85Edema 41 28 68.29Pain 41 28 68.29Varicosities 41 25 60.98

50Table 8. (Continued)
Number Number PercentItem Cases Agreeing Agreeing
GROUP IIIRedness location 41 22 53.65Skin infection 41 23 56.10Skin infection location 41 24 58.53Yellow nail 41 21 51.22Posterior tibial pulse 41 23 56.10Leg length 41 . 23 56.10
GROUP IVNature of limitation 41 18 43.90Discoloration (red) 41 20 48.78Dorsalis pedis pulse Location absent dorsalis
41 18 43.90pedis pulse
Location absent posterior41 17 41.48
tibial pulse 41 18 43.90Leg size 41 18 43.90

51For the items receiving less than 70 percent agree
ment it was important to determine the nature of the disagreement between the nurse observers. Did the nurse observers truly disagree or did they fail to make a response to the item? Table 9 shows the "No response" percent rate for the items receiving less than 70 percent agreement.Four groups are displayed; Group I, items receiving 19 percent or above "No Response"? Group II, items receiving 10-19 percent "No Response"; Group III, items receiving 5-10 percent "No Response"? Group IV, items receiving 0-5 percent "No Response".
Items in Group I had a relatively high "No Response" rate while those in Group IV were relatively unaffected by this rate. Thus, the disagreement between the nurse observers is more apparent than real for items in Group I, while there is true disagreement between the nurse observers for the Group II, III, and IV items.
Additional analysis of the items from Table 9 was made by removing the effect of the "No Response" percentage rate and calculating the revised percent agreement, which is shown in Table 10. Four groups emerge from the analysis; Group I, items receiving 70 percent or above agreement; Group'll, items receiving 65-70 percent agreement; Group III, items receiving 55-65 percent agreement; Group IV, items receiving 40-55 percent agreement.

52Table 9. Percent no response, percent agreement, percent
disagreement for items receiving less than 70 percent agreement.
Item Percent Percent PercentNo Response Agreement Disagreement
GROUP IVaricosities 21,95 60,98 17.07Leg size 21,95 43.90 34.15Location redness 21,95 . 53,65 24.39Gait 21,95 60.98 17.07Leg length 19,51 56,10 24.39
GROUP IILocation posterior
tibial pulse 12.20 43.90 43.90Nature of limitation 12.20 43.90 43.90
GROUP IIILimitation 7.32 63.41 29.27Shoe condition 7.32 60.98 31.71Location infection 7.32 58.53 34.15Edema 9.76 68.29 21.95
GROUP IVShoes 4.88 60.98 34.15Redness (localized) 2.44 60.98 36.59Infection 0.00 56.10 43.90Thickened nail 0.00 65.85 34.15Yellow nail 2.44 51.22 46.34Dorsalis pedis pulse 4.88 43.90 51.22Location dorsalis
pedis pulse 0.00 41.48 34.15Posterior tibial
pulse 4.88 56.10 39.02Pain .0.00 68.29 31.71Discoloration (red) 2.44 48.78 48.78

53Table 10. Revised percent agreement between nurse observers
in the assessment of elderly clients' lower extremities.
Percent PercentItem Agreement Agreement
(Revised) (Original)
GROUP IVaricosities 78.13 60.98Gait 78.13 . 60.98Edema 75.68 68.29
GROUP IILeg length 69.07 56.10Redness location 68.75 53.65Limitation 68.42 63.41Pain 68.29 68.29Shoe condition 65.79 60.98Thickened nail 65.85 65.85
GROUP IIIShoes 64.10 60.98Redness (localized) 62.50 60.98Infection location 63.15 58.53Posterior tibial pulse 58.98 56.10Leg size 56.25 43.90Infection 56.10 56.10
GROUP IVYellow nail 52.50 51.22Discoloration (fed) 50.00 50.00Posterior tibial pulse
location 50.00 50.00Nature of limitation 50.00 50.00Dorsalis pedis pulse 46.15 43.90Dorsalis pedis location 41.48 41.48

54Three items in Group I showed over 75 percent agree
ment, after removing the effect of the "No Response" percent rate»
In Table 10, the data reveals that in Group II one item (leg length) increased to 69 percent, three items (redness location, limitation, and pain) increased to 68 percent, one item (shoe condition) increased 65 percent, while one item (thickened nail) remained at 65 percent.The data shows that items in Groups III and IV received a percentage agreement below 65 percent.
It should be noted that all but four items (infection, thickened nail, dorsalis pedis pulse location, and pain) showed an increase in percent agreement, upon removal of the "No Response" percentage rate.
From the above analysis the items in Group I met the reliability requirement established in the study. The Group II items are within 5 percent of the acceptable level' and should be considered reliable items. The items in Group III receiving 55—65 percent agreement show medium reliability while the items receiving 41-55 percent agreement show low reliability. The decision to retain or revise the items in Groups III and IV should be made on an individual basis.
Table 11 shows the final categorization of the reliability of the items. It includes the Group I items

Table'll. Final categorization of the percent agreement between nurse observers in the assessment of elderly clients' lower extremities.
PercentItem Agreement
GROUP IMobility 70.73Foot hygiene . 73.17Stockings 73.17
. Garters 85.37Fissure (Toes) 87.80Fissure (Heel) 92.68Excoriation 75.61Corn(s) 78.05Callus (es) 82.93Wart (s) 95.12Other 73.17Itching 75.61Rash 92.68Ingrown nail 87.80Overgrown nail 87.80Blacknail \ 73.17Discoloration (brown) 90.24Dry skin 80.49Feet temperature 80.49Leg temperature 92.68Nature of pain 82.93Ulceration 78.05Ulceration location 80.49Hallux valgus 78.05Hammertoes 85.37Overlapping digits 70.73Varicosities 78.13*Gait 78.13*Edema 75.68*
GROUP IILeg length 69.07*Redness location 68.75*Limitation 68.42*Pain 68.29*Shoe condition 65.79*Thickened nail 65.85*

56Table 11. (Continued)
ItemPercentAgreement
GROUP IIIShoes .64,10*Redness (localized) 62.50*Infection location 63.15*Posterior tibial pulse 58.98*Leg size 56.25*Infection 56.10*
GROUP IVYellow nail 52.50*Discoloration (red) 50.00*Posterior tibial pulse location 50.00*Nature of limitation 50.00*Dorsalis pedis pulse 46.15*Dorsalis, pedis pulse location 41.48*
*Revised percent agreement from Table 8.
from Table 8 and, the items from Table 10. Four groupings are displayed: Group 1 , items receiving 70 percent or aboveagreement? Group II, items receiving 65-70 percent agreement; Group III, items receiving 55-65 percent agreement? Group IV, items receiving 40-55 percent agreement.
Group I items are considered highly reliable,Group II items are reliable. Group III items are moderately reliable, and Group IV items have low reliability.
CHAPTER 5
DISCUSSION, CONCLUSIONS, IMPLICATIONS,AND RECOMMENDATIONS
This chapter includes a discussion on the theoretical framework for the study, the findings, the conclusions, the implications, and the recommendations.
Nursing assessment involves the gathering of information— objactive and subjective— on the health status of the individual in order to make decisions relating to the losses or potential losses in that status. An observational instrument which is well defined, clearly understood, and systematically used facilitates the assessment process and provides the basis for sound nursing intervention.
This study was designed to develop such an instrument for use by the nurse in assessing the lower extremities of elderly clients. The underlying assumption of the study was that accurate observations of the lower extremities require a tool that is clear, concise, and practical.
Riccitelli's (1966) classification of the major causes of foot pain and disability provided the theoretical framework for the establishment of relevant categories for nursing observation. The descriptors were defined in
58

59objective rattier than in subjective terms and were highly specific. The tool was validated for content validity by a panel of experts.
FindingsStudies have shown that older Americans are often
confronted with multiple foot problems which can be painful and debilitating. The findings from this limited study support this proposition. Twenty-two of the 41 clients (53 percent) stated that they had a foot condition which limited their activity. Of the clinical findings, a total of 41 skin lesions (of which 33 were corns or calluses) and 67 toenail abnormalities were found. There were 166 signs or symptoms of vascular impairment, 49 cases of structural deformities, and 11 clients with a gait disturbance. In particular, those clients living in a nursing home manifested more foot problems than those clients living in the community. The former had 72 percent of the corns or calluses, 76 percent of the toenail abnormalities, 74 percent of the pulseless feet, 85 percent of the cases of dry skin, and 80 percent of the cases of ulceration.
Two'findings with respect to footgear are noteworthy. One client living in a nursing home stated that she Could not wear shoes because her "feet are so bad". This person— diagnosed as having arteriosclerotic heart disease— - had multiple corns and calluses on her feet and had one

6 0pair of crocheted booties to wear» Another client, who was wheelchair bound, living in a nursing home, stated that she always wore the same pair of crocheted booties and claimed that they were four years old.
In summary, the clinical findings showed the need for a nursing assessment of the lower extremities of these elderly clients. Most of the conditions identified could become significant problems. For example, all of the skin lesions pose a risk— infection could develop and would be exacerbated by the circulatory impairment found in so many of these clients. The assessment tool facilitated the recognition of these conditions, many of which are nursing care problems and require nursing intervention.
Reliability of Test ItemsIn measuring the reliability coefficient, the most
straightforward approach was used. A percent agreement was computed for each of the 47 items in the tool, in which the level of .70 was arbitrarily chosen as the lowest acceptable level of reliability. Twenty-six of the 47 items showed 70 percent or above agreement between the nurse observers and are considered highly reliable items (see Table 8). Nine items received 60-70 percent agreement, six items received 50-60 percent agreement and six items received 40-50 percent agreement.

61For the items receiving less than 70 percent agree
ment, an additional analysis was made by removing the effect of the "No Response" percentage rate and calculating the. revised percent agreement. Three more items received 70 percent or above agreement, six items received 65-70 percent agreement, six items received 55—65 percent agreement, and six items received 40-55 percent agreement (see Table 10)„ Thus, the final categorization of the reliability of the items is as follows: Group I, items receiving 70 percentor above agreement; Group II, items receiving 65-70 percent agreement; Group III, items receiving, 55-65 percent agreement; Group IV, items receiving 40-55 percent agreement.
Table,11 shows: the final categorization of the reliability of the items. The Group I items are considered highly reliable, the Group II items are reliable, the Group III items are moderately reliable, and the Group IV items have low reliability.
The items, as a whole, received a rigorous test for reliability. First, 41 clients were assessed by two nurses, working independently, making 41 tests of each of the items in the tool. Second, instead of having two judges make all the assessments, this study used 20 volunteer nurses for the assessments. Third, each of the paired assessments were made within a three day period— with the exception that a week lapsed between two assessments. Considering

62all the above factors, the fact that the results are as high as they are gives the researcher more confidence in the reliability of the items, particularly for those receiving 65 percent or above agreement,
The items receiving 70 percent or above agreement (see Table 8) were straightforward, highly structured-— • with the exception of one open-ended question (#22)— and required little subjective interpretation on the part of the observer. Illustrations were provided for questionable items.
As- stated earlier, an additional analysis was made on the items receiving less than 70 percent agreement by removing the effect of the "No Response” percentage rate. This rate ranged from 0-21 percent (see Table 9), There are various explanations why some of the items failed to receive a response from the assessor: (1) inadequateinstructions to the assessor; (2) a simple act of ommission on the assessor's part; (3) inadequate assessment skill on the assessor1s part.
In reviewing the assessment tool it was quite evident that additional instructions were needed for some items. For example, the item "Gait” (#3) was preceded by these instructions; "Ask the client to walk approximately10 feet, n This instruction held for ambulatory clients only. Instructions should have been provided to cover

' 63those clients who were wheelchair bound or bedfast.Another example of inadequate instruction was for items #27, #28, #29s "Ask the client to stand." Again, this was meaningful for ambulatory clients only.
The assessor may have failed to respond to an item because;of inadequate assessment skill. This appears to be the case for the items "dorsalis pedis" (#16) and "posterior tibial pulse" (#17). Both of these items received a 5 percent "No Response" rate. It was suggested in the guide sheet that the assessor practice taking these pulses before assessing the clients' pulses. However, time constraints may have precluded the implementation of this instruction.
In attempting to account for the variations in the use of the instrument several explanations seem logical. First, the length of time between assessments may have been a factor. A three day interval was allowed between the first and second assessment. The characteristic being measured could have changed between the two assessments and this may account for the disagreement between the nurse observers.
Second, some items were more difficult to assess than others. For example, the pedal pulses are considered difficult to find and require practice to develop the necessary skill in taking them. The researcher did not .

64expect a high, agreement between the observers for this item. It is interesting to note that the expert found the dorsalis pedis pulse (#16) present in 14 cases as compared to 32 cases for the volunteers, while the posterior tibial pulse (#17) was found to be present in 12 cases by the expert as compared to 25 cases for. the volunteers. This difference can partly be accounted for by the fact that the expert recorded very weak pulses as absent.
Third, the clients, themselves, may have responded differently to the item; For example, the item "limitation" (#2) had a disagreement percentage rate of 30 percent, which meant that the client said "yes" to the question on one occasion and "no” on the other occasion.
Fourth, the item was not clearly delineated. This appears to be the case for the following items: "limitation" (#2), "shoes" (#6 ), and "skin infection" (#12). It should be noted that the expert found one case Of skin infection whereas the volunteers found 16 cases. All of these items need to be revised.
Fifth, open-ended questions may have allowed for too much variation in response from the observer. For example, the item "describe the limitation of your activity" (#2) had a 43 percent disagreement between the observers.
Sixth, items may not have been logically correct.For example, the item "mobility" (#1) did not have mutually
exclusive categories. Some clients could walk without assistance for a short distance, but walked with the help of equipment for longer distances.
Lastly, some items may have allowed for more subjective interpretation on the observer’s part. This may have accounted for the relatively high disagreement on these items: "redness (localized)" (#11), "yellow discoloration" (#13d) and "red discoloration" (#14), For these items the degree of discoloration necessary for a positive response was not indicated. A color coded chart would have been helpful.
For the unreliable items in Groups III and IV (see Table 11) the. question arises as to whether they should be kept in the tool. The researcher supports retaining all of these items since they a.re important parameters in the assessment of the lower extremities. The reliability of these items could be increased by (1) providing a more detailed guide sheet for the tool and (2) revising some of the. items as indicated in the above discussion.
Nurses1 Evaluation of the Tool In pre-testing the tool, six of the eight nurses
completed the evaluation form. The mean length of time required to complete the assessment was 22 minutes. For a comprehensive assessment of the extremities this time period did not appear too long, but from a practical

66standpoint it was. In order for staff nurses to use the tool a revision was necessary.
The nurses' comments with respect to the tool were favorable. The. fact that all of them were volunteers who were interested in helping the researcher may have accounted for this. This is not to preclude that the tool did provide information to them which was considered valuable.
Based on the information obtained during the pre-testing phase, the assessment tool was revised in- content, form, and terminology (see Appendix C). The socio-demographic information as well as questions on medical history were deleted, since the information could be obtained in the general assessment of the client. The. greatest change took place in format. Most of the categories were constructed in such a manner as to elicit a "Fixed-Alternative" response on the part of the observer.
Two items were left open-ended. Both were follow up questions. If the client responded "yes" to the question, "Does the condition of your feet or legs limit your activity in any way?" he was then asked to describe the limitation. The second one followed the question, "Does the client have any pain in his legs or feet?" Further clarification was asked for if the client responded "Yes" to this question. In both of these cases, the items would

67have been meaningless without the clients' frame of reference.
During the testing phase volunteers were not asked to evaluate the tool because of the time constraint.
Conclusions1. Almost 75 percent of the items received 65 per
cent or above agreement between the nurse observers. These items yielded approximately the same response with two different measurements. It appears that the structured tool provided an objective means of data gathering for these items.
2. The clinical findings showed the need for- nurses to assess the lower extremities of elderly clients at periodic intervals; The tool facilitated the recognitionof foot disorders as well as identified clients with high risk conditions (#11, #12, #16, #17, #23). The tool may be used as a basis for planning for the maintenance or restoration of foot health in the elderly.
3. The clinical findings from this study showed that those clients living in a nursing home manifested more foot problems than those living in the community.Their need for foot care was particularly acute since a large majority of them had circulatory impairment. The fact that one of these clients could not wear shoes because her "feet were so bad" and another client had very malodorous

68crocheted booties to wear gives further evidence in support of periodic evaluation of the feet.
4. As discussed earlier, the reliability of the . instrument as a whole was not computed. Instead, each of the items in the instrument was considered separately and a reliability coefficient was computed for each item. This was established by determining the percent agreement between the nurse observers on each of the items. A level of .70 was arbitrarily chosen as the lowest acceptable level of agreement. It was hypothesized that there would be greater' agreement between the nurse observers than disagreement on each of the items in the tool. The final categorization of the. reliability of the items is as follows (see Table 11): Group I, items receiving 70 percent or above agreement;Group II, items receiving 65-70 percent agreement; Group III, items receiving 55-65 percent agreement? GrOup IV, items receiving 40—55 percent agreement.
Twenty-nine of the 47 items (62 percent) showed 70 percent or above agreement between the nurse observers and are considered highly reliable items. Six items received 65 to 75 percent agreement and considered reliable. Six items received 55 to 65 percent agreement and are moderately reliable, while six items received 40 to 55 percent agreement and have low reliability. Thus, the hypothesis was confirmed for items in Groups I, II, and III.

695. The items, as a whole, received a rigorous
test for reliability. Forty-one clients participated in the study, making 41 tests of each of the items in the tool. Twenty volunteer nurses made the assessments. . The length of time between.the first and second assessment was usually; three days. Considering all the above factors, the fact that the results are as high as they are gives the researcher more confidence in the reliability of the items.
6. Notwithstanding the above conclusion, there was Variation in response in using the instrument by different observers. To the extent that a higher reliability for the items is desireable the tool should be revised. It should h© noted that the tool is a first attempt to provide nurses with an instrument for assessing the foot problems of elderly clients and as such is unrefined.
Implications1. The tool was designed for use with elderly
clients, but it could be applied more generally to include any adult client, because the descriptors are defined in objective terms.
2. The original tool (see Appendix B) could be used as a teaching aid in in-service education programs, continuing education programs, or in a geriatric nursing course.

703, The revised tool (see Appendix C) could be use
ful in a variety of settings: nursing screening clinics,long term care facilities, and other institutional settings„ It would seem to be very appropriate to use for a newly admitted patient,
4. If the tool has wide-range applicability, and it appears that it does, foot care needs can be documented and intervention planned for maintaining or restoring foot health in the aged.
RecommendationsBased upon the findings in this study> the re
searcher makes the following recommendations.1. To the extent that a higher reliability for
the items is desirable, the tool should be revised. Prior to revision, the tool should be used in a variety of settings, using a more detailed guide sheet and evaluation form. A study could then be done testing this tool for reliability.
2. The present tool's reliability could be increased by removing some of the known sources of error.For example, the assessments should be- made within a 24 hour period, in one institutional setting, so that the situation would be under better control by the researcher.
3. The key question concerning the tool1s usefulness is whether or not it facilitates a systematic

71assessment of the lower extremities. An experimental study should be designed testing this proposition.
4. There should be Space in the tool for a summary of the client's foot problems.
5. Space should be provided in the tool for specifying the location of any foot problem that is identified.

CHAPTER 6
SUMMARY
Foot health for the aged person adds to his total well being. In the past, little attention was given to the older person's foot problems, but, recently, the significance of these problems has been documented by members of the nursing, medical, and podiatry professions. Foot disorders can lead to disability, limitation of activity, loss of motivation, and self-assurance. Since these conditions can be so devastating, to the older person, early recognition of foot problems assumes paramount importance.
Nurses can play a key role in this area by becoming directly involved in assessing the feet. By carefully examining the feet in a systematic manner, the foot cafe needs can be identified and intervention planned for maintaining or restoring foot health in the aged person.
In searching the nursing literature, no structured tool for assessing the feet was found. The need for such a tool appeared to be indicated.
The purpose of.this study was to develop an instrument which would assist nurses in making systematic observations of the lower extremities of elderly clients.
72

73The first phase of the study dealt with the construc
tion of the assessment tool and the presentation of it to a panel of experts for review. They agreed that it had content validity.
The second phase began with the pre-testing of the tool by four graduate students and three faculty members in the College of Nursing. Their evaluation of the tool was favorable with respect to content and form. However, a mean time of 22 minutes was required to complete theassessment. ‘This was considered too long from a practical> - -
standpoint.Following changes in format and content the third
phase, testing the tool for reliability, began. Two foot assessments on the same individual were made by a pair of nurses, working independently, within a three day period.A total of 41 clients participated in the study. Each of them had two foot assessments— one by the researcher and one by a nurse volunteer, with the following exception.Two clients living in a Phoenix nursing home were assessed by two different nurses from there. A total of 20 nurses participated in the study.
For this study, the reliability of the instrument as a whole was not computed. Instead, each of the 47 items in the instrument was considered separately and a reliability coefficient was computed for each item. In measuring this

74coefficient for each of the items, the paired observationswere compared for agreement across all 41 cases. For eachitem, a percent agreement was computed. A level of .70was arbitrarily chosen as the lowest acceptable level of agreement.
The final categorization of. the reliability of the . items yielded four groupings (see Table 11): Group I,items receiving 70 percent or above agreement; Group II, items receiving 65-70 percent agreement; Group III, items receiving 55-65 percent agreement; Group IV, items receiving 40-55 percent agreement.
Twenty-nine of the 47 items (62 percent) showed 70 percent or above agreement between the nurse,.observers, and are considered highly reliable. Six items received 65-75 percent agreement and are considered reliable. •' Six items received 55-65 percent agreement and are moderately reliable, while six items received 40-55 percent agreement and have low reliability.
Seventy-four percent of the items received 65 percent or above agreement between the nurse observers.It appears that the structured tool assisted the nurse observers with an objective means of data gathering for these items.
In the descriptive phase of the study, the clinical findings showed the need for nurses to assess the lower

75extremities of these elderly clients„ The types of disorders found in this group were: skin lesions (47 cases) ,
toenail abnormalities (67 cases) , signs or symptoms of vascular impairment (166 cases), and structural deformities (49 cases)„ High risk conditions identified were: localized redness (9 cases), skin infection (1 case), dorsalis pedis pulse absent (27 cases), posterior tibial pulse absent (28 cases), and ulceration (10 cases). In general those clients living in a licensed health care facility manifested more foot problems than those living in the. community. ■
Several implications appear to follow from the findings in the study., First, the original tool (Appendix B) could be used in educational programs for nurses.Second, the revised tool (Appendix C) could be employed in institutional and noninstitutional settings. Third, the tool could be applied more generally to include any adult client.
To the extent that a higher reliability for the items is desirable, the tool should be revised. Prior to revision, the tool should be used in a variety of settings, using a more detailed guide sheet and evaluation form. A study could then be done testing this tool for reliability.
It is the conclusion of this researcher that foot health for the older person contributes to his physical and emotional well being.

APPENDIX A
NURSES' EVALUATION FORM
Please answer the following questions. Your comments will be appreciated,
1, How long did it take you to use the assessment tool?
2. What suggestions do you have for improvement?
3. Comments;
76

APPENDIX B
NURSING ASSESSMENT OF THE GERIATRIC FOOT
77
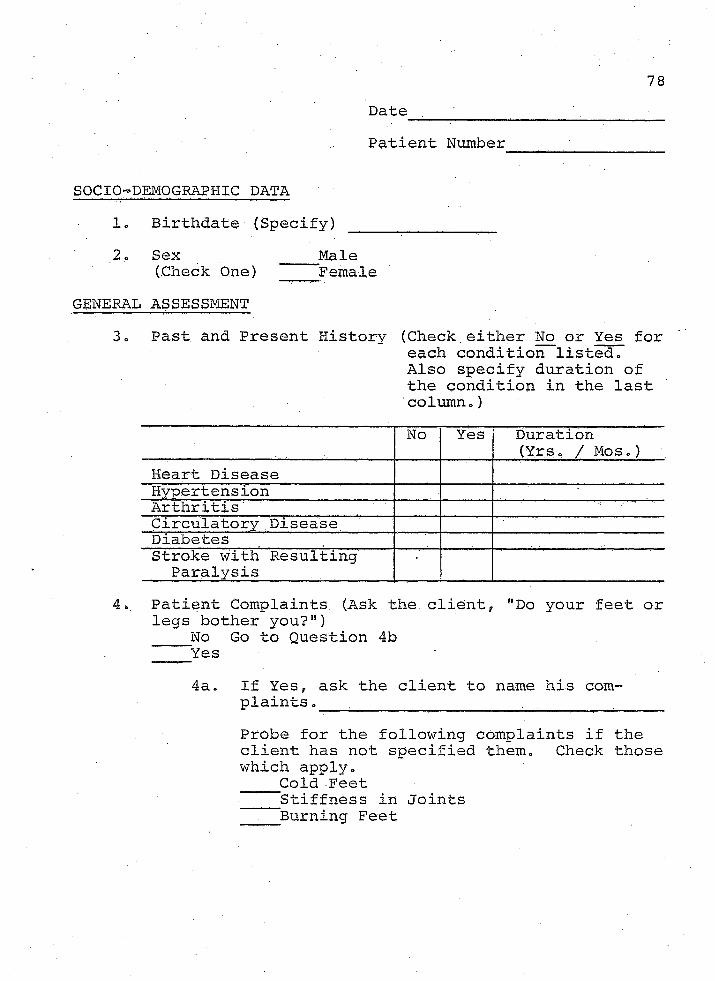
78Date .Patient Number
SOCIO-DEMOGRAPHIC DATA1. Birthdate (Specify) ___2, Sex ____Male
(Check One) FemaleGENERAL ASSESSMENT
3<» Past and Present History (Check either No or Yes foreach condition listed.Also specify duration of the condition in the last column.)No Yes Duration
(Yrs. / Mos.)Heart DiseaseHypertensionArthritisCirculatory DiseaseDiabetesStroke with Resulting Paralysis
4.. Patient Complaints (Ask the client, "Do your feet or legs bother you?")
No Go to Question 4b Yes4a. If Yes, ask the client to name his com
plaints ._____ _Probe for the following complaints if the client has not specified them. Check those which apply. Cold Feet
Stiffness in Joints Burning Feet

794b, (Ask the client, "Are you bothered with
, , , ?" Check those which apply.Cold FeetStiffness in JointsBurning Feet
Foot Gear (Check and complete as applicable)Type ■ Material ConditionOxford Leather GoodSlip-on___________ ^Synthetic Fair
Heels Poor Slipper
Casual Open Toes
Open HeelsOther, Describe
Mobility (Check those which apply)Walks without assistance.Walks with help of equipment, describe_Does not walk
JJses wheelchair Bedfast
7, Gait (Ask the client to walk approximately 10 feet.Observe whether there is any gait disturbance. Check one and complete as applicable)
. Ho gait disturbanceGait disturbance, describeNot applicable
REMOVE THE CLIENT'S SHOES AND STOCKINGS8 . Cleanliness (entire foot) (Check one)
Good Fair Poor9. Stockings (Check those which apply)
Type Length ConditionNylon Over the Knee GoodCotton Knee High Fair White Over the Ankle . Poor
Colored_Synthetic _Other, Describe ""None

8010. Garters (Check and complete as applicable)
Circular Other, DescribeNone
ASK THE CLIENT TO STAND11. Flat Feet (Note whether the soles of the arch
touch the floor. Check one)Absent Present Not Applicable
12. Symmetry (Note whether the legs are the samerelative size and length. Check and complete as applicable)
Legs equal in size L e g s equal in length
Legs unequal in size or length, describe13. Varicosities (Check and complete as applicable)
AbsentPresent, Specify Location
'______ MildModerateSevere
ASK THE CLIENT TO RETURN TO A SITTING POSITION
DERMATOLQGIC ASSESSMENT14. Skin Lesions (Inspect both legs and feet for the
following conditions. Check either No or Yes column for each condition listed. Also specify location in space provided.)
No Yes Location (Legs, feet, toes, heels)
Fissure(s) Between the
Toes Heel
ExcoriationBlister(s)Mole*Bunion(s)Corn(s)Callus(es)Plantar Wart*14a. If yes, has it changed recently?

8115. Itching (Check and complete as applicable.)
Absent Present, Specify site_________ ______
16. Rash (Check and complete as applicable) Absent
Present, Specify site _______ .17. Redness (Localized) (Inspect pressure areas on the
feet for redness. Check and complete as applicable.)
AbsentPresent, Specify location
18. Skin Infection (Inspect legs, feet, and toes forlocalized swelling, warmth, tenderness, redness. Check and complete as applicable.)
No inflammatory area _Inflammatory area, Specify location _____
19. Toenails (Check those which apply and completeas applicable.)
IngrownOvergrown (long nails)Thickening of the nail plate
Material embedded under nail plate Discoloration Yellow Black Other, Describe ____________________ _Lesion, Describe_____ ________ _________
CIRCULATORY STATUS ITEMS20. Skin Color (Inspect feet and ankles for color
changes. Check (/) one and complete as applicable.)
No DiscolorationDiscoloration (Use Table to specify color and
location)Color Location (Feet, Ankles, Toes)RedBlueReddish BlueBrownPallorOther

8221. The Dorsalis Pedis Pulse. Use three fingers on the
dorsum of the foot usually just lateral to the extensor tendon of the great toe. (This pulse is sometimes congenitally absent.) (Fig. 1)(Check One) Present Diminished
Absent
22. The Posterior Tibial Pulse. Curve your fingersbehind and slightly below the medial malleolus of the ankle. (This pulse may also be congenitally absent.) (Fig. 2)(Check One) Present Diminished
Absent
(Figures 1 and 2. Questions 21 and 22. The instructions and illustrations for palpating the dorsalis pedis and the posterior tibial pulses are from A Guide to Physical Examination by Barbara Bates, 1974 , used by permission of J. B. Lippincott Co., publisher.)
Fig. 1 Fig. 2
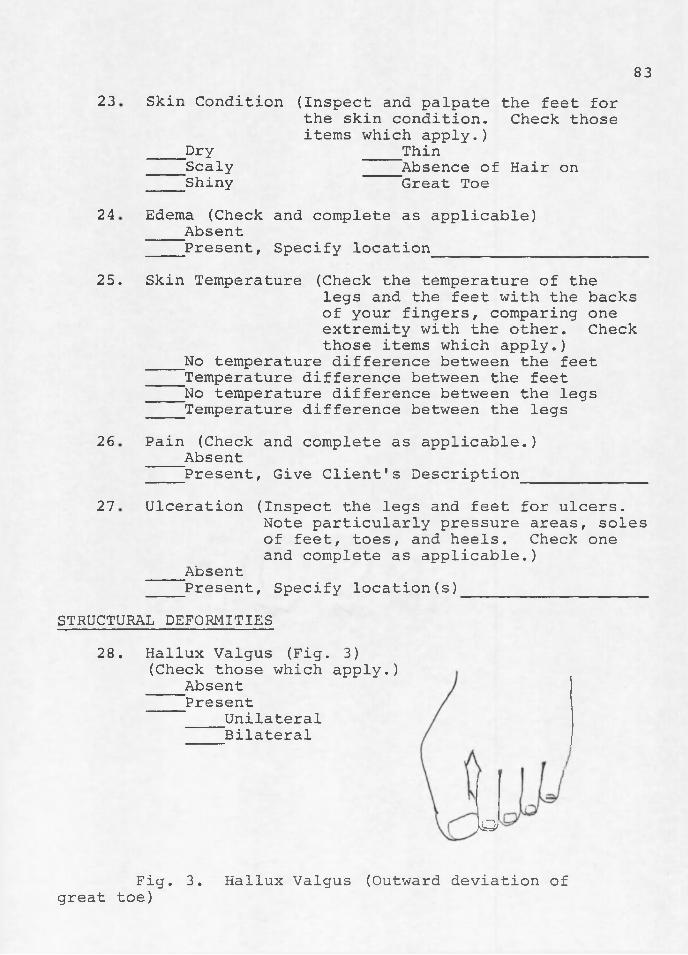
8323
24
26
27
Skin Condition (Inspect and palpate the feet forthe skin condition. Check those items which apply.)
Dry Thin Scaly
ShinyAbsence of Hair on Great Toe
Edema (Check and complete as applicable) Absent Present, Specify location___________
25. Skin Temperature (Check the temperature of thelegs and the feet with the backs of your fingers, comparing one extremity with the other. Check those items which apply.)
No temperature difference between the feet Temperature difference between the feet No temperature difference between the legs Temperature difference between the legsPain (Check and complete as applicable.) Absent Present, Give Client's DescriptionUlceration (Inspect the legs and feet for ulcers.
Note particularly pressure areas, soles of feet, toes, and heels. Check one and complete as applicable.)
Absent Present, Specify location(s)___________________
STRUCTURAL DEFORMITIES28. Hallux Valgus (Fig. 3)
(Check those which apply.) Absent Present
UnilateralBilateral
AO,
Fig. 3. Hallux Valgus (Outward deviation of great toe)
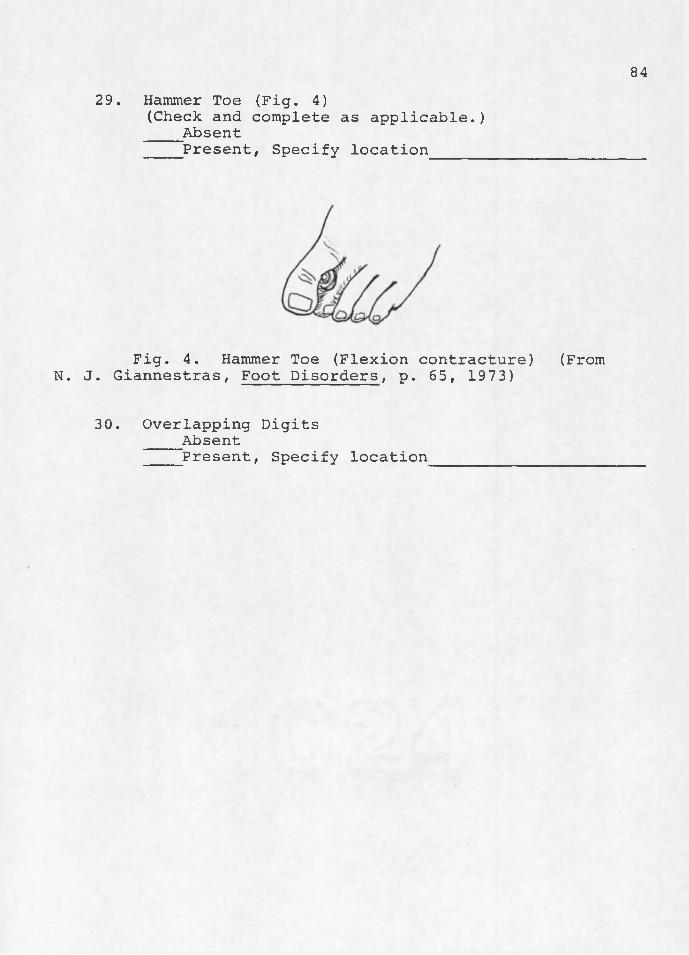
8429. Hammer Toe (Fig. 4)
(Check and complete as applicable.) Absent Present, Specify location_____
Fig. 4. Hammer Toe (Flexion contracture) N. J. Giannestras, Foot Disorders, p. 65, 1973)
30. Overlapping Digits Absent Present, Specify location___________
(From

APPENDIX C
REVISED TOOL
85

86Nursing Assessment of the Geriatric Lower Extremity
Patient. Number DateR«No Number
INSTRUCTIONS: For each item, circle the response in the appropriate column, unless directed otherwise. Clarification of items appears in the far right column.1. Mobility (check one)
Walks without assistance□ Walks with help of equipment D Does not walk - uses wheelchair I I Bedfast
2. Ask the client, "Does the condition of yourfeet or legs limit your activity in any way? YES NOIf YES, describe. _____ '____ .
3. Ask the client to walk approximately 10 feet.Is there any. gait disturbance? .YES NO
REMOVE THE CLIENT'S SHOES AND STOCKINGS.ACCEPT- UNACCEPT-
4. Cleanliness of feet. ABLE ABLE5. Are the stockings a good, fit? YES NO6. Does the client usually wear well fitting,
leather (synthetic) shoes that cover hisfeet completely? YES NOIf YES, are they in good condition? YES NO
7. Does the client wear circular garters? YES NODERMATOLOGICAL ASSESSMENT.8. Skin lesions.
a. Fissure between the toes? YES NOb. Fissure on heel(s)? YES NOc. Excoriation on legs or feet? YES NOd. Corn (s)? (Fig. 1)
(Corn: painful, circular area ofthickened skin, appearing on skin that is normally thin.
e. Callus(es)? YES NO(Callus: thickened skin, occurringon skin that is normally thick, i.e., soles.

87
Figure 1. Corn
O j
Red, thickened
f. Plantar wart? YES NOg. Other, describe___________________________ YES NO
9. Itching on legs or feet? YES NO10. Rash on legs or feet? YES NO11. Inspect pressure areas on the feet for
localized areas of redness. Are anypresent? YES NOIf YES, which foot? RIGHT LEFT
12. Inspect legs, feet, and toes forlocalized swelling, warmth, tenderness, redness.Is any present? YES NOIf YES, specify location. Rt.Leg Lt.Leg
Rt.Ft. Lt.Ft.13. Toenails.
a. Ingrown? YES NO(Ingrown toenail: a "tenderoverhanging nail fold"; Bates,1974)
b. Overgrown (Long)? YES NOc . Thickened? YES NOd. Yellow discoloration? YES NOe. Black discoloration? YES NO
CIRCULATORY STATUS (Questions 14-18 related to FEET ONLY)14. Do the feet have any red, reddish blue,
or bluish discoloration? YES NO15. Is there any brownish discoloration
around the ankles? YES NO

8816. Is the dorsalis pedis present? (Fig. 2) YES NO
If NO, which foot? RIGHT LEFT
Figure 2. Dorsalis pedis pulse.Use three fingers on the dorsum of the foot usually just lateral to the extensor tendon of the great toe. Instructions and illustrations for palpating the pulses are from A Guide to Physical Examination, 1974, by Barbara Bates, M.D., used by permission of J. B. Lippincott Co., publisher .
17. Is the posterior tibial pulse present? YES NO(Fig. 3) If NO, which foot? RIGHT LEFT
Figure 3. Posterior tibial pulse.Curve your fingers behind and slightly below the medial malleolus of the ankle. See Fig. 2 for source.

18. Is the skin dry?THE FOLLOWING RELATE TO BOTH FEET AND LEGS.
89YES NO
19. Is edema present? YESCHECK THE TEMPERATURE OF THE LEGS AND THE FEET WITH THE BACKS OF YOUR FINGERS, COM- PARING ONE EXTREMITY WITH THE OTHER.
20. Are the feet the same temperature? YES21. Are the legs the same temperature? YES22. Does the client have any pain in his
legs or feet? YESIf YES, describe____________________________________INSPECT THE LEGS, SIDES OF ANKLES, SOLES,TOES FOR ULCERATION.
23. Is any ulceration present? YESIf YES, specify location Rt.Leg Lt
Rt.Ft. LtSTRUCTURAL DEFORMITIES.24. Hallux Valgus (Bunion)? (Fig. 4) YES
NO
NONO
NO
NOLegFt.
NO
Figure 4. Hallux Valgus (outward deviation of great toe).

25. Hammer toes? (Fig. 5)90
YES NO
Flexion
Figure 5. Hammer toe.Flexion contracture. From N. J. Giannestras, Foot Disorders, p. 65, 1973.
26. Overlapping digits? YES NOASK THE CLIENT TO STAND.27. Are the legs the same relative size? YES NO28. Are the legs the same relative length? YES NO29. Are varicosities present? YES NOADDITIONAL NOTES:

APPENDIX D
GUIDE TO THE NURSING ASSESSMENT OF THE GERIATRIC LOWER EXTREMITY
This tool is designed to aid the nurse in making systematic observations of the geriatric lower extremity.
The instructions for using the tool appear on the first page of the tool. However, several questions require further clarification. They are as follows.
Question 3. Gait Disturbance. Circle YES if the client shows any difficulty .in walking.
Questions 16 and 17. The dorsalis pedis and posterior tibial pulse. If you have not taken these pulses before, it is suggested that you practice on yourself and perhaps one other person before taking the client’s pulses.
Thank you for your help.
Pat King R.N.
91

LITERATURE CITED
Anderson, Helen C. Newton's Geriatric Nursing. 5th edition.St. Louiss The C. V. Mdsby Company, 1971, pp. 102- 104, 194-201.
Bates, Barbara. A Guide to Physical Examination. Philadelphia : J. B. Lippincott CO., 1974.
Block, Doris. "Some Crucial Terms in Nursings What Do TheyReally Mean?" Nursing Outlook, Nov. 1974, 22(11): 689-694.
Bruck, Helen 0. and Claude N. Lambert. "Common Foot Disabilities." American Journal of Nursing, 1959,59 (11):1580-1583.
DuVries, Henri L. Surgery of the Foot. St. Louiss The C. V. Mosby Co., 1959.
DuVries, Henri L. Surgery of the Foot. St. Louiss The C. V. Mosby Co., 1973.
Fowler, Marsha D. "Behold the Great Right Toe." American Journal of"'Nursing, 1974, 74 (lO)October:1817-1819.
Gamble, Felton 0. and Irving Yale. Clinical Foot Roentgenology. 2nd edition. New York: Krueger Publishing Co., Inc., 1975.
Giannestras, Nicholas J. Foot Disorders: Medical andSurgical Management, 2nd edition. Philadelphia:Lea and Febiger, 1973.
Hamdi, Mary E. and Carol M. Hutelmyer. "A Study of theEffectiveness of an Assessment Tool in the Identification of Nursing Care Problems." Nursing Research, July-August, 1970, 19 (4):355-359.
Helfand, Arthur E. "Podiatry in a Total Geriatric Health Program: Common Foot Problems of the Aged."Journal of the American Geriatrics Society, 1967,15 (6):593-599.
92
93Helfand, Arthur E. "Keep Them Walking," Journal of the
American Podiatry Association, 1968, 58(3)March; 117-126,
HeIfand, Arthur E, "The Foot of South Mountain; A FootHealth Survey of the Residents of a State Geriatric institution," Journal of the American Podiatry, Association, 1969, 59(4)April;133-139,
Helfand, Arthur E. "Podiatry; Essential Nursing Home Care," Nursing Homes, 1970, May;35-36,
Helfand, Arthur E, "Podiatric Considerations for the Aged -Patient,” Nursing Homes, 1971a, November;30-31.
Helfand, Arthur E. "Podiatry and the Elderly Patient."Working with Older People; Clinical Aspects of Aging. U.S.D.H, E.W., Rockville, Maryland, 1971b,4 (July);377-388.
Helfand, Arthur E. "At the Foot of South Mountain."Journal of the American Podiatry Association,1973, 63 (10)October;512-521.
Helfand, Arthur E. "Hunting.Diabetics by Foot." Journal of the American Podiatry Association, 1974,64(6)June;399-406.
Hoerner, M, Tischer. "Minor Foot Lesions with Diabetes Mellitus and Peripheral Vascular Disease."Geriatrics, 1967, April, pp. 164-174.
Hopp, Ruth Ann and Sherrill Sundberg. "The Effects ofSoaking and Lotion on Dryness of the Skin in the Feet of the Elderly Patient." Journal of the American Podiatry Association, ,1974/, Volume 64,No. 10, .October;747-760.
Hsu, John D. "Foot Problems in the Elderly Patient."Journal of the American Geriatric Society, 1971,19 (10);880-885.
Jahss, Melvin H. "Geriatric Aspects of the Foot and Ankle." In Isadore Rossman (ed.) Clinical Geriatrics. Philadelphia: J. B. Lippincott Co., 1971.
Jones, Ellen W., Barbara J. McNitt, and Eleanor M. McKnight."Patient Classification for Long-Term Care: User’sManual." 1974, D.H.E.W. Publication No. HRA 75-3107.

94Jones, Fo Wo Structure and Function as Seen in the Foot.
Londons Bailliere, Tindall, and Cox, 1944.Juergens, J. L. and Bernatz, P. E. "Arteriosclerosis
Obliterans." Chp. 10 In J. F. Fairbairn et al„(eds.) Allen-Baker-Hines Peripheral Vascular Diseases. 4th edition. Philadelphia; W. B. Saunders Co., 1972.
Kelly, P. J. and M. B, Coventry. "Neurotrophic Ulcers ofthe Feet." Journal of the American Medical- Association, 1958 , 168 s 388-393.
Kolstoe, Ralph H. Introduction to Statistics for the Be~ havioral Sciences. 1969, Illinois: The DorseyPress.
Martin, Elizabeth J. and Jane E. D. Smith. "Diabetic Foot Care: Knowledge and Practice." ANA ClinicalSessions, 1969, pp. 143-149.
McGregor, R. R. "Geriatric Foot Care." Nursing Clinics of North America, 1968, (3)December:687-695.
Rakow, Robert B. and Sandor A. Friedman. "The Significance of Trophic Foot Changes." Geriatrics, 1969,May;135-139.
Riccitelli, M. L. "Foot Problems of the Aged and Infirm."Journal of the American Geriatrics Society, 1966,14(10):1058-1066.
Riccitelli, M. L. "Peripheral Vascular Disease in theAged: Modern Concepts and Diagnostic Techniques."Journal of the American Geriatric Society, 1969,17 (2) :205-212.
Rietz, Daniel. "Nebraska Podogeriatrics Training Program for Nursing Home Nurses«," Journal of the American Podiatry Association, 1968, 58(3)March:127-131.
Selltiz, Claire, Marie Jahoda, Morton Deutsch, and Stuart W. Cook. Research Methods in Social Relations.New York: Holt, Rinehart and Winston, 1959, pp.167? 392-395? 401-406.
Simko, Michael V. "Foot Welfare." Nursing and the Aging Patient. New York: American Journal of Nursing,1974, pp. 62-66.

Spencer, Marion G. "Podogeriatrics and the Nurse." ANA Clinical Sessions, 1970, pp. 75-81.
Wilkins, Robert W. "Diseases of the Peripheral Vessels." Cecil-Loeb Textbook of Medicine. 12th edition. Philadelphia: W. B. Saunders Co., 1967.
Zetterberg, Hans L. On Theory and Verification inSociology. 3rd edition. New Jersey: The Bed-minister Press, 1965.

I j i i !
S : i l i- ^
i
■
I. B O
m m
. n
- H3
| - F
ttl vi
F
m ^ I ft i vSBl 1I L11
B H





























