Embed Size (px)
Citation preview

www.wjpps.com Vol 9, Issue 9, 2020.
1892
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
ASSESSMENT OF PRESCRIBING, DISPENSING AND PACKAGING
PATTERNS OF ANTIBIOTICS IN TERTIARY CARE HOSPITAL
Ayesha Jamal1*, Parisa Peivand Kermani
1, Mahendra Kumar B. J.
2, Nisar Ahmed
3 and
Shahid Ashraf
1Pharm D Interns, Department of Pharmacy Practice, Farooqia College of Pharmacy, Mysore,
Karnataka, India.
2Professor and Head, Department of Pharmacy Practice, Farooqia College of Pharmacy,
Mysore, Karnataka, India.
3Assistant Professor, Department of Pharmacy Practice, Farooqia College of Pharmacy,
Mysore, Karnataka, India.
ABSTRACT
Introduction: A Study on "Assessment of Prescribing, Dispensing
And Packaging patterns of Antibiotics In Tertiary Care hospital" was
carried out to find out indiscriminate use, drug misuse, and Incorrect
prescribing of antibiotics that have resulted in drug- drug interaction,
sub-optimal therapy, poly-pharmacy, medication failure, non-
compliance, increased healthcare expenditure, multiple drug resistance
as well as financial pressure on households and communities and most
importantly increased occurrence of antibiotic resistance.
Methodology: A prospective, observational and descriptive research
was conducted for six months from Sept 2018 to Feb 2019 in the in-
patient Departments of General medicine, Obstetrics and gynecology,
Pediatrics, ICU and Surgery in CSI Holdsworth Memorial (Mission) hospital, a tertiary care
hospital in Mysore District and in community pharmacies in Mysore, with the aim to evaluate
the prescribing, dispensing and packaging patterns of antibiotics. The data on prescribing
pattern of antibiotics by physicians, patient’s demographic details, complaints, past medical
history, current medications along with their ADRs, dispensing pattern of antibiotics in
pharmacies by pharmacists, and packaging patterns of antibiotics by manufacturers was
collected. The Potential drug–drug interactions (DDIs) were identified using Medscape drug
interaction checker. The data was Analyzed utilizing MS EXCEL and MS WORD. Results:
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 7.632
Volume 9, Issue 9, 1892-1916 Research Article ISSN 2278 – 4357
Article Received on
01 July 2020,
Revised on 21 July 2020,
Accepted on 11 August 2020
DOI: 10.20959/wjpps20209-17063
*Corresponding Author
Ayesha Jamal
Pharm D Interns,
Department of Pharmacy
Practice, Farooqia College
of Pharmacy, Mysore,
Karnataka, India.

www.wjpps.com Vol 9, Issue 9, 2020.
1893
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
This research features polypharmacy, overuse and inappropriate prescribing of antibiotics
without prior culture sensitivity in hospital situations. Distributing antibiotics without
prescription and by non-pharmacists are widespread in this sector. In the manufacturing
sector, we invariably figured dissimilarity among the measure of doses and frequency of
antibiotics prescribed by the physicians, when compared to the regular packaging sizes
available as approved by guidelines for the most typically prescribed antibiotics. The research
also indicates irrational use of antibiotics which may lead to antibiotic resistance.
Conclusion: Public attention, sensitization of physicians, pharmacists and manufacturers for
modification of prescribing, dispensing and packaging patterns of antibiotics is necessary for
rational use of antibiotics. Excellence in healthcare can be boosted by improving the
prescribing, dispensing and packaging pattern of antibiotics by physicians, pharmacists and
by manufacturers in healthcare system. Establishing ideas and evaluating the excellence of
care through performance analysis is the need of the hour in everyday hospital practice.
KEYWORDS: Pharmacist, Tertiary care hospital, prescribing patterns, dispensing patterns,
packaging patterns, irrational use.
INTRODUCTION
Antibiotics are certainly miracle drugs that have protected millions of lives either as
prophylaxis agents or as therapeutics agents.[1]
Unfortunately, indiscriminate usage, drug
misusage, and Incorrect prescribing of antibiotics have resulted in drug- drug interaction, sub-
optimal therapy, poly-pharmacy, medication failure, multiple drug resistance, non-
compliance, increased healthcare expense and financial burden on households and
communities and most importantly heightened occasion of antibiotic resistance.[2]
At first, antibiotic discovery were extremely successful; this implied that if drug resistance
developed, a new drug was always accessible to deal with the increasingly resistant bacteria.
But now this resistance is expanding and antibiotic advancement is holding up. The prudent
usage of antibiotics is therefore an important way to reduce antimicrobial resistance.[3]
Prescribing patterns of antibiotics indicate the clinical judgment of the clinicians. Examining
prescribing patterns keenly will help minimize adverse drug reactions and give expense-
effective medications.[4]
Thus antibiotic prescribing pattern has an important consequence on
the outcome of patient’s constraint. Hence, to withstand antimicrobial resistance,
interventions on improper antibiotic usage have to be analyzed occasionally so that
interventions can be enforced if essential to guarantee careful antibiotic usage. These signs
www.wjpps.com Vol 9, Issue 9, 2020.
1894
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
for warning on the way of prescribers and pharmacists and the need for understanding of
methods that can be utilized by practitioners for perceiving drug medication issues.[5]
Today the WHO indexes abuse of antibiotics as one of the three biggest dangers to human
health. Widespread Incorrect usage of antibiotics has created intensifying resistance
pathogens, spoiling much of the improvement made against infectious organisms in the last
50 years. Clinicians and healthcare experts worldwide must vigorously attempt to strengthen
the potency, span and practical life of existing antibiotics. It is advisable for pharmacists to
examine the availability of a once-daily single tablet, fixed-dose combination of antibiotics to
decrease pill burden, boost adherence and reduce the expense and complexness of medication
regimen. The main reason we see 'antibiotic resistance' is because of the misuse of antibiotics
in a population that does not need antibiotics, for instance, in viral infections. "Deliberate
usage of antibiotics stimulates the spread of 'antibiotic resistance'; smart usage of antibiotics
is the key to repealing its spread".
Practical antibiotic prescription is essential to prevent multiple drug resistance, medication
failure, non-compliance and increased expense on medications. Incorrect usage of antibiotics
is allowing usage of an antibiotic when it is not really required. It is also providing the
appropriate antibiotic for an inaccurate interval, i.e., too long or too short at a time. In some
cases, the correct antibiotics can be provided in combination with medicines that interact with
the antibiotic, in that case, the therapeutic advantages are undervalued.
Numerous outcomes result from the incorrect usage of antibiotics; one of them is the
occurrence of 'antibiotic resistance'. Microbes are no longer exterminated by antibiotics that
managed to exterminate them. Higher doses need to be employed to achieve minimum
inhibitory concentrations. Another significant outcome is the alarming expenses incurred by
the government, insurance schemes and on patients when antibiotics are misused.
Governments invest a lot of capital to deal with resistant strains because they lead to
extended hospital stays and prolonged antibiotic use of costly antibiotics. It is important to
utilize the most relevant antibiotics for infectious circumstances.
This emphasizes the serious need for vigilant surveillance, formulation of standard antibiotic
regulation policies and enforcement of policies for antibiotic usage, stringent infection
control strategies as well as logical antibiotic prescribing patterns to facilitate the careful
usage of these drugs that will have a significant positive financial privilege and boost the
www.wjpps.com Vol 9, Issue 9, 2020.
1895
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
excellence of care being delivered to patients. So, we recommend studying the antibiotic
prescribing, dispensing, and packaging patterns of antibiotics to relatively withstand the
unfair usage of antibiotics and decrease antibiotic resistance growth.
METHODOLOGY
Study design: This study was a prospective, observational and descriptive study.
Study site: This study was carried out in various Departments such as General Medicine,
Pediatrics, OBG, Surgery, ICU of CSI Holdsworth Memorial (Mission) hospital, Mysore,
Karnataka, India.
Study period: The study was performed for 6 months from September 2018to February
2019.
Research approval: The Institutional Ethics Committee of Farooqia College of Pharmacy,
Mysore, Karnataka, India, approved the study before commencement of the research.
Search strategy: Searched from Medline, Pubmed, Plusone, Winley Online Data Base,
Journal of Applied Pharmaceutical Science and many other articles were collected and
referred. The keywords used in Google search engines were prescribing patterns, dispensing
patterns and packaging patterns.
Sources of data: Patient data for the study were collected from the following sources:
Prescriptions from patient’s medication charts were collected.
Pharmacists from different community pharmacies were interviewed.
Nurses gave information about the route of administration and frequency of
administration.
Case records: Patient care notes, medication charts, past medical history.
Culture sensitivity tests were referred
Patient data collection forms which includes demographic details (Name, Age, Gender)
Current diagnosis from doctor’s notes was referred.
Medication prescribed (dose, route of administration, strength, frequency, indication,
therapy interval).
Study protocol
A Protocol for the project titled “Assessment of Prescribing, Dispensing and Packaging
patterns of Antibiotics in tertiary care hospital” was prepared.
Submitted protocol for ethical committee clearance.

www.wjpps.com Vol 9, Issue 9, 2020.
1896
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
A well-designed data collection form was prepared. Data collection form included the
following details: Demographics of patients like patient name, age, gender, weight, IP
number, ward, unit, date of admission, date of discharge, extent of hospital stay.
Computerization of data collection forms using Microsoft ® access 2007 was created for
the documentation of collected data and also for easy accessibility, retrieval and analysis
of collected data.
Analyzed patient medication charts for prescribing, dispensing and packaging patterns of
antibiotics.
Percent occurrence on hospital parameters on the packaging of antibiotics was collected
by review of different antibiotic products obtained from pharmacies located in Mysore.
Observational study was done to view and record the data. Prospective analysis was
performed to examine the result.
All the collected information was subjected for statistical analysis.
Data was analyzed, and percentages were calculated.
Based on the results of the present study and discussions from previous researchers
conclusion was reported.
RESULTS
In a total of 550 patients medication charts analyzed, details of medication charts without
antibiotics were found in 93 (17%) medication charts, one antibiotic in 230 (42%)
medication charts, two antibiotics in 150 (27%) medication charts, three antibiotics in 59
(11%) medication charts and four antibiotics in 18(3%) of medication charts (Figure 01).

www.wjpps.com Vol 9, Issue 9, 2020.
1897
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Gender distribution of patients
Out of 550 patients, 215(39%) females and 335(61%) males were found (Figure no-2).
www.wjpps.com Vol 9, Issue 9, 2020.
1898
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
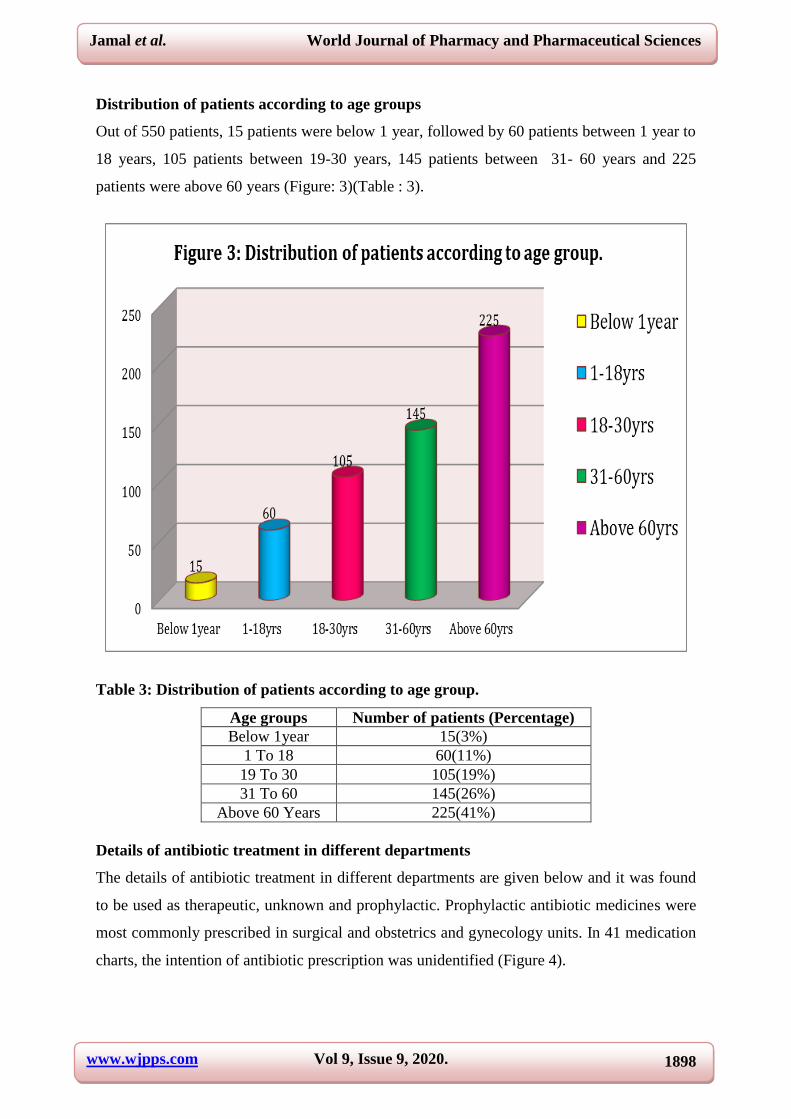
Distribution of patients according to age groups
Out of 550 patients, 15 patients were below 1 year, followed by 60 patients between 1 year to
18 years, 105 patients between 19-30 years, 145 patients between 31- 60 years and 225
patients were above 60 years (Figure: 3)(Table : 3).
Table 3: Distribution of patients according to age group.
Age groups Number of patients (Percentage)
Below 1year 15(3%)
1 To 18 60(11%)
19 To 30 105(19%)
31 To 60 145(26%)
Above 60 Years 225(41%)
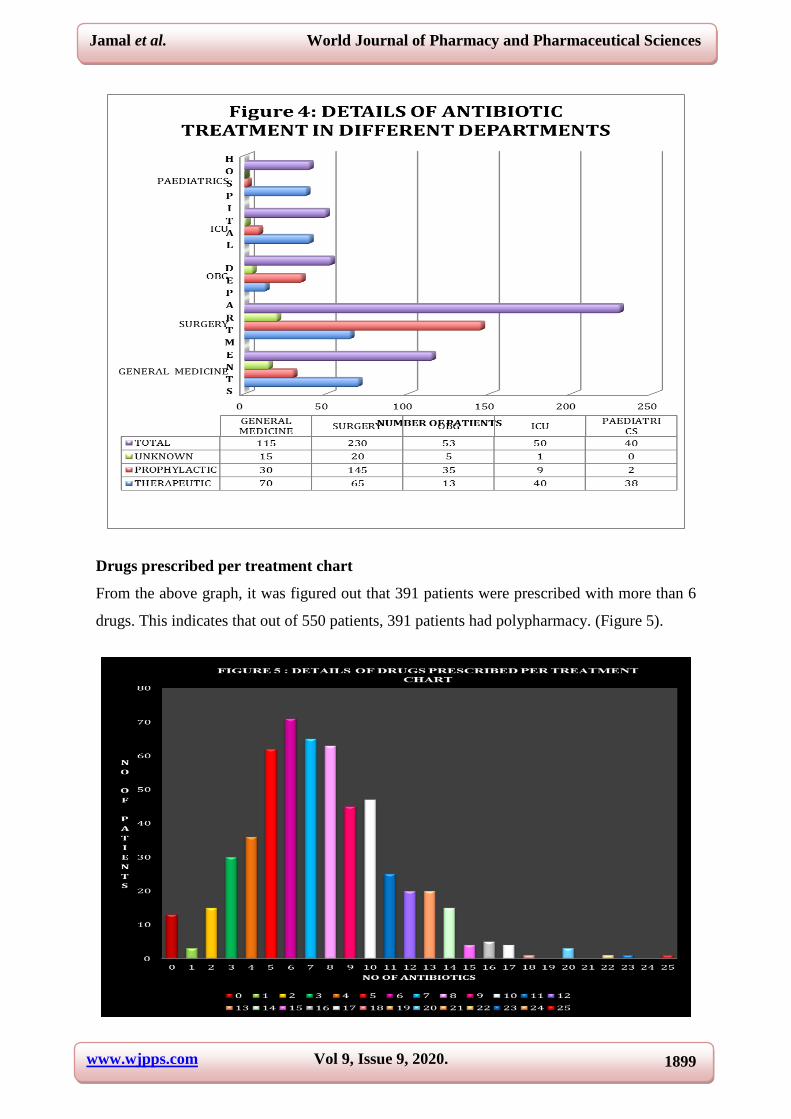
Details of antibiotic treatment in different departments
The details of antibiotic treatment in different departments are given below and it was found
to be used as therapeutic, unknown and prophylactic. Prophylactic antibiotic medicines were
most commonly prescribed in surgical and obstetrics and gynecology units. In 41 medication
charts, the intention of antibiotic prescription was unidentified (Figure 4).
www.wjpps.com Vol 9, Issue 9, 2020.
1899
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Drugs prescribed per treatment chart
From the above graph, it was figured out that 391 patients were prescribed with more than 6
drugs. This indicates that out of 550 patients, 391 patients had polypharmacy. (Figure 5).
www.wjpps.com Vol 9, Issue 9, 2020.
1900
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Table 4: different antibiotics prescribed.
Ceftriaxone 115 Metronidazole 67
Cefixime 52 Azithromycin 38
Ciprofloxacin 22 Albendazole 7
Cefuroxime 80 Moxifloxacin 1
Clindamycin 8 Ofloxacin 4
Ampicillin 6 Levofloxacin 16
Doxycycline 23 Cefperazone 5
Cefpodoxime 2 Amikacin 28
Gentamycin 20 Rifaximin 3
Vancomycin 10 Meropenem 10
Cefotaxim 22 Cefadroxyl 8
Cefaclox-xl 15 Cefpodroxyl 5
Netlimycin 1 Amoxycillin 30
Linezolid 4 Tinidazole 1
Cefalexin 1 Rifampicin 1
Table 5: details of combination of antibiotics prescribed.
Ofloxacin +tinidazole 1
Amoxycillin+ clavulanic acid 30
Cefaperazone+ sulbactum 38
Ciprofloxacin + tinidazole 25
Cefpodoxime + clavulanic acid 1
Cefepime + tazobactum 2
Ceftriaxone + sulbactum 15
Ofloxacin +tinidazole 1
Details of pharmacological classification of antibiotics prescribed
Out of 724 antibiotics prescribed in the study, 369 (60%) cephalosporin’s, 49 (8%)
aminoglycosides, 14 (2%) quinolones, 38 (6%) macrolides, 6 (1%) penicillins, 10 (2%) beta
lactamase inhibitors, 23 (4%) tetracyclins, 4 (1%) linezolid, 10 (2%) vancomycin, 10 (2%)
meropenem,, 8 (1%) anthelmentics, 8 (1%) lincomycin, 3 (0%) rifaximin, 67 (11%)
metronidazole. (Figure 6).

www.wjpps.com Vol 9, Issue 9, 2020.
1901
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Frequency of anttibiotics administration
All the medications were administered based on various regimens such as twice daily (1-0-1),
once daily (1-0-0), thrice daily (1-1-1), STAT, SOS and also by giving half dose or divided
dose as required (Figure: 7).
www.wjpps.com Vol 9, Issue 9, 2020.
1902
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
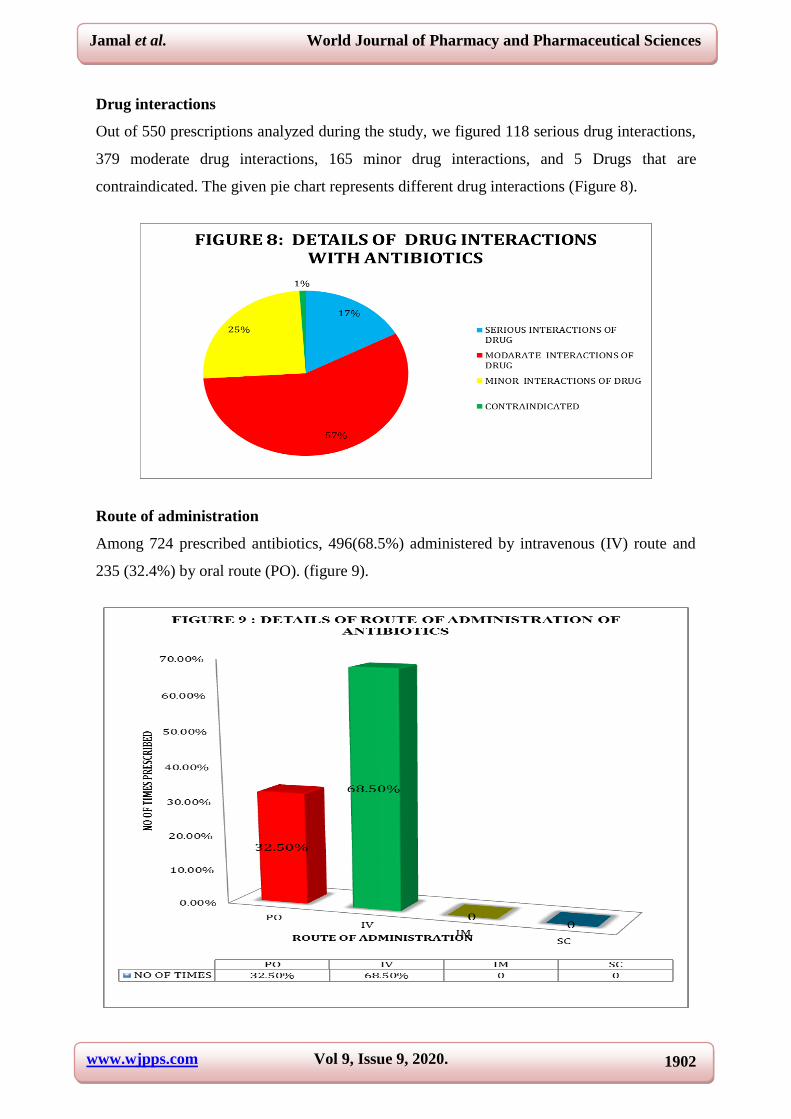
Drug interactions
Out of 550 prescriptions analyzed during the study, we figured 118 serious drug interactions,
379 moderate drug interactions, 165 minor drug interactions, and 5 Drugs that are
contraindicated. The given pie chart represents different drug interactions (Figure 8).
Route of administration
Among 724 prescribed antibiotics, 496(68.5%) administered by intravenous (IV) route and
235 (32.4%) by oral route (PO). (figure 9).
www.wjpps.com Vol 9, Issue 9, 2020.
1903
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Dispensing patterns of antibiotics
Out of 50 pharmacists interviewed from 10 clinics and 20 community pharmacies, we figured
out the dispensing patterns of antibiotics. The results are shown below:
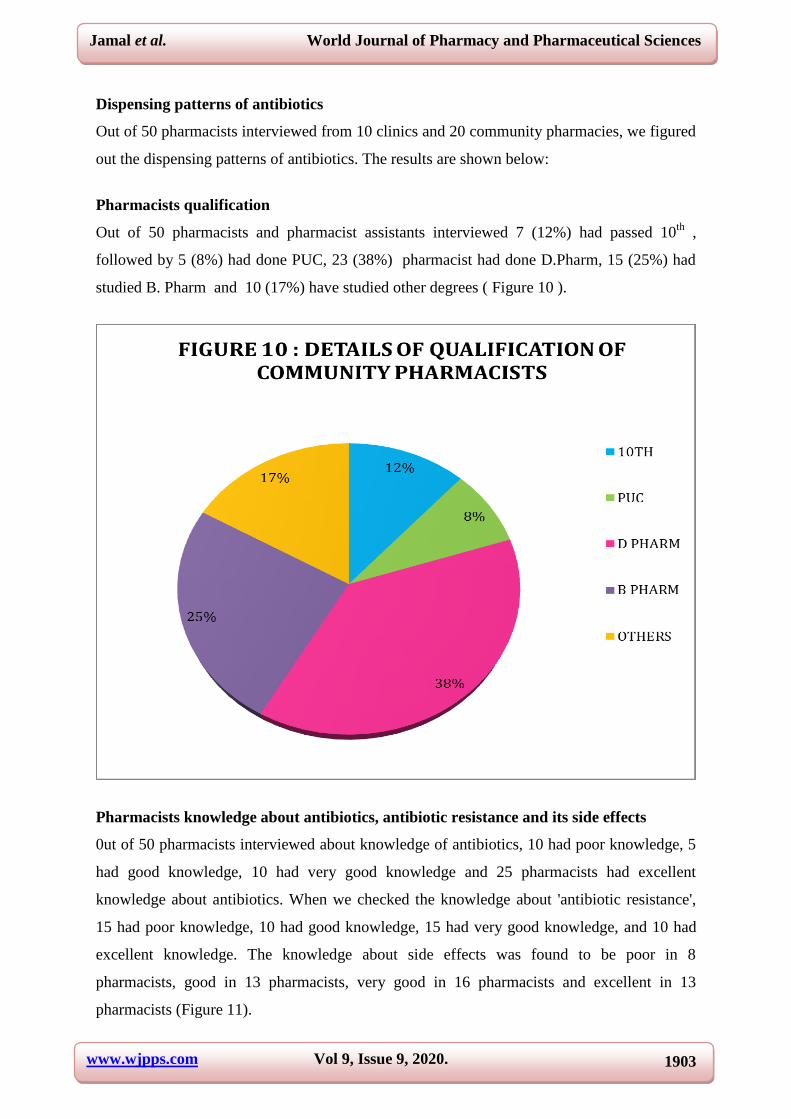
Pharmacists qualification
Out of 50 pharmacists and pharmacist assistants interviewed 7 (12%) had passed 10th
,
followed by 5 (8%) had done PUC, 23 (38%) pharmacist had done D.Pharm, 15 (25%) had
studied B. Pharm and 10 (17%) have studied other degrees ( Figure 10 ).
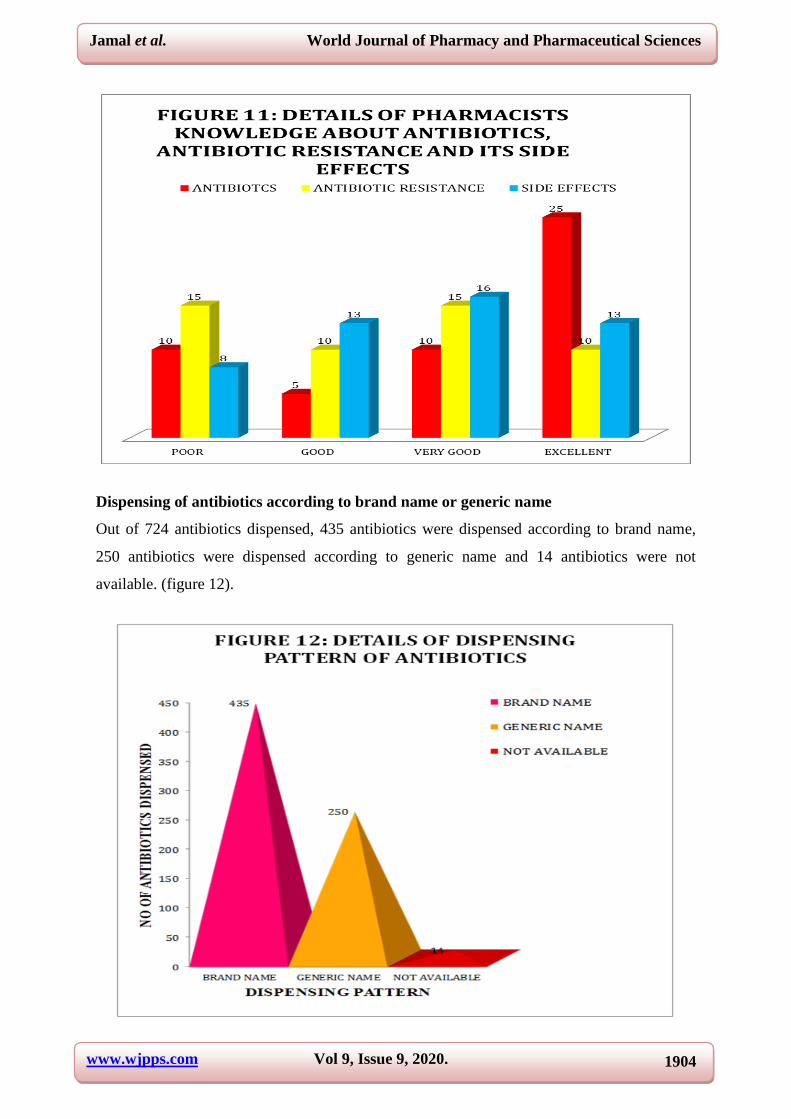
Pharmacists knowledge about antibiotics, antibiotic resistance and its side effects
0ut of 50 pharmacists interviewed about knowledge of antibiotics, 10 had poor knowledge, 5
had good knowledge, 10 had very good knowledge and 25 pharmacists had excellent
knowledge about antibiotics. When we checked the knowledge about 'antibiotic resistance',
15 had poor knowledge, 10 had good knowledge, 15 had very good knowledge, and 10 had
excellent knowledge. The knowledge about side effects was found to be poor in 8
pharmacists, good in 13 pharmacists, very good in 16 pharmacists and excellent in 13
pharmacists (Figure 11).
www.wjpps.com Vol 9, Issue 9, 2020.
1904
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
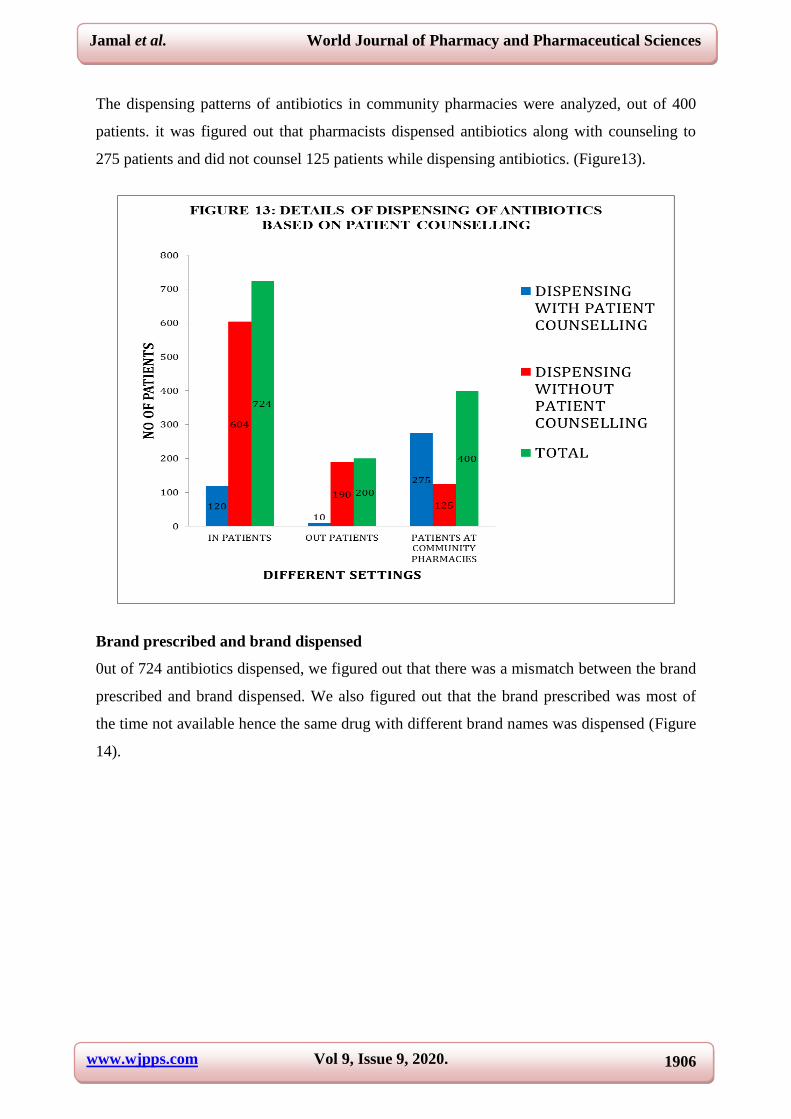
Dispensing of antibiotics according to brand name or generic name
Out of 724 antibiotics dispensed, 435 antibiotics were dispensed according to brand name,
250 antibiotics were dispensed according to generic name and 14 antibiotics were not
available. (figure 12).

www.wjpps.com Vol 9, Issue 9, 2020.
1905
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Antibiotics dispensing pattern
Dispensing of antibiotics was analyzed and it was figured out that the dispensing of
antibiotics is done according to the number of units prescribed or based on patients needs.
Table 7: details of antibiotics dispensing patterns.
Antibiotics in generics No of units prescribed and dispensed
Cefuroxime Same
Ceftriaxone Same
Metronidazole Same
Ampicillin Same
Gentamycin Same
Vancomycin Same
Ciprofloxacin Different
Cefpodoxime Different
Cefotaxim Same
Azithromycin Same
Cefpodroxyl Same
Cefaperazone Same
Cefixime Same
Cefadroxyl Different
Amikacin Same
Rifaximin Different
Cefpodem Different
Levofloxacin Different
Netlimycin Same
Meropenem Same
Ofloxacin Different
Linezolid Same
Cefalexin Different
Tinidazole Same
Albendazole Same
Ramizole Same
Cefpodoxime Same
Amoxycyllin+ clavulanic acid Same
Cefaperazone+ sulbactum Same
Ciprofloxacin + tinidazole Same
Cefepime + tazobactum Same
Ceftriaxone + sulbactum Same
Cefpodoxime + clavulanic acid Same
Ofloxacin + ornidazole Different
Dispensing of antibiotics based on patient counseling
Dispensing patterns of antibiotics figured that only 190 out-patients out of 200 patients were
counseled about antibiotic usage, whereas 500 in- patients out of 550 patients were not
counseled about antibiotic usage.
www.wjpps.com Vol 9, Issue 9, 2020.
1906
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
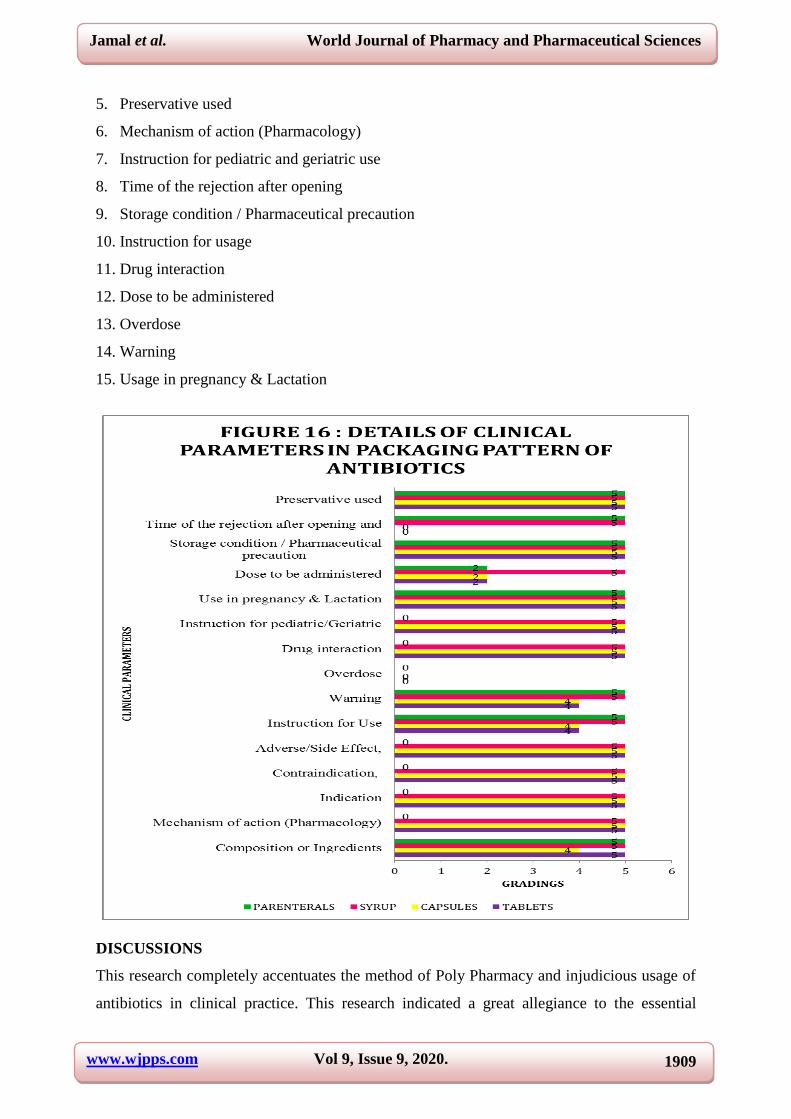
The dispensing patterns of antibiotics in community pharmacies were analyzed, out of 400
patients. it was figured out that pharmacists dispensed antibiotics along with counseling to
275 patients and did not counsel 125 patients while dispensing antibiotics. (Figure13).
Brand prescribed and brand dispensed
0ut of 724 antibiotics dispensed, we figured out that there was a mismatch between the brand
prescribed and brand dispensed. We also figured out that the brand prescribed was most of
the time not available hence the same drug with different brand names was dispensed (Figure
14).

www.wjpps.com Vol 9, Issue 9, 2020.
1907
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Packaging patterns
The major and minor packaging commodities of 550 antibiotics were assembled. A whole of
32 major and minor packaging substances of all commodities have been accessed,
Common Regulatory parameters
Medical parameters.
The common regulatory parameters are
1) Generic Name
2) Brand Name
3) Date of manufacturing
4) Manufacturer name
5) Mailing Address of the Manufacturer
6) Legibility of the inserts
7) Product volume,
8) Quantity of the package (net weight, amount)
9) Supply of label

www.wjpps.com Vol 9, Issue 9, 2020.
1908
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
10) Sterility profile
11) Maximum Retail Price
12) License of the product (DAR No.)
13) Manufacturing License
14) Batch No/Lot No
15) Date of Expiry
16) Type of Dosage form
17) Bilinguality.
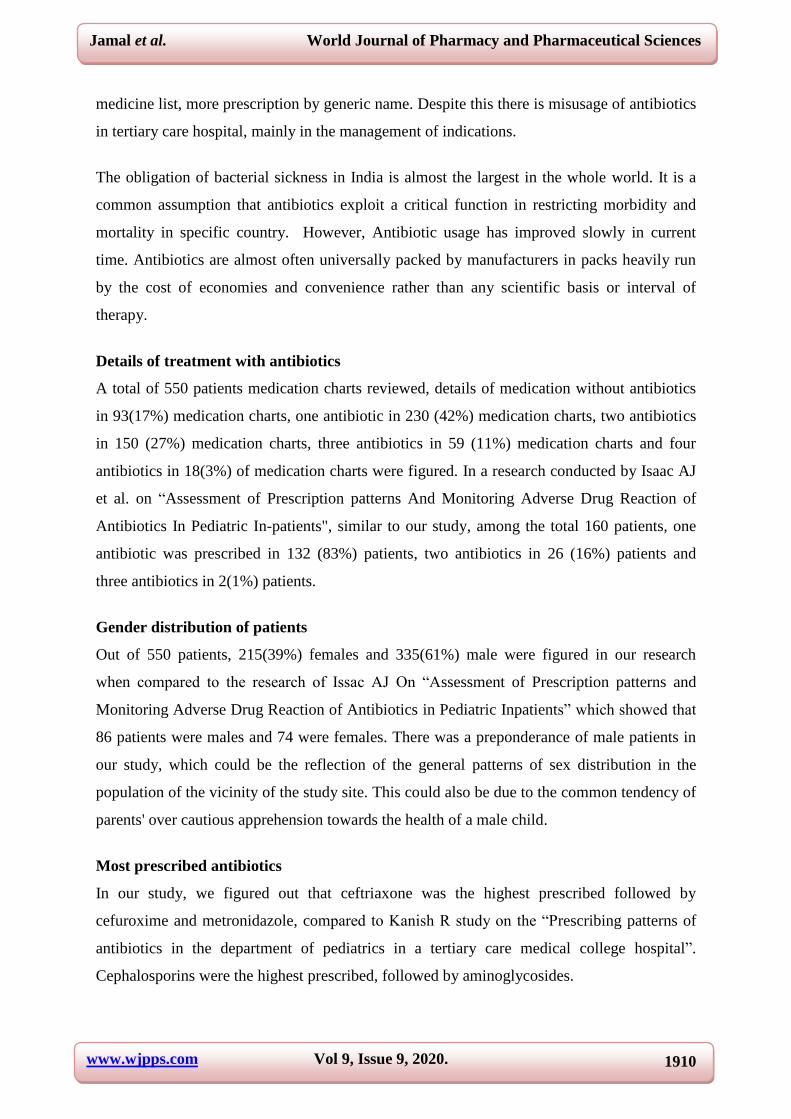
The hospital parameters are
1. Indication
2. Contraindication
3. Composition or Ingredients
4. Adverse/Side Effect
www.wjpps.com Vol 9, Issue 9, 2020.
1909
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
5. Preservative used
6. Mechanism of action (Pharmacology)
7. Instruction for pediatric and geriatric use
8. Time of the rejection after opening
9. Storage condition / Pharmaceutical precaution
10. Instruction for usage
11. Drug interaction
12. Dose to be administered
13. Overdose
14. Warning
15. Usage in pregnancy & Lactation
DISCUSSIONS
This research completely accentuates the method of Poly Pharmacy and injudicious usage of
antibiotics in clinical practice. This research indicated a great allegiance to the essential
www.wjpps.com Vol 9, Issue 9, 2020.
1910
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
medicine list, more prescription by generic name. Despite this there is misusage of antibiotics
in tertiary care hospital, mainly in the management of indications.
The obligation of bacterial sickness in India is almost the largest in the whole world. It is a
common assumption that antibiotics exploit a critical function in restricting morbidity and
mortality in specific country. However, Antibiotic usage has improved slowly in current
time. Antibiotics are almost often universally packed by manufacturers in packs heavily run
by the cost of economies and convenience rather than any scientific basis or interval of
therapy.
Details of treatment with antibiotics
A total of 550 patients medication charts reviewed, details of medication without antibiotics
in 93(17%) medication charts, one antibiotic in 230 (42%) medication charts, two antibiotics
in 150 (27%) medication charts, three antibiotics in 59 (11%) medication charts and four
antibiotics in 18(3%) of medication charts were figured. In a research conducted by Isaac AJ
et al. on “Assessment of Prescription patterns And Monitoring Adverse Drug Reaction of
Antibiotics In Pediatric In-patients", similar to our study, among the total 160 patients, one
antibiotic was prescribed in 132 (83%) patients, two antibiotics in 26 (16%) patients and
three antibiotics in 2(1%) patients.
Gender distribution of patients
Out of 550 patients, 215(39%) females and 335(61%) male were figured in our research
when compared to the research of Issac AJ On “Assessment of Prescription patterns and
Monitoring Adverse Drug Reaction of Antibiotics in Pediatric Inpatients” which showed that
86 patients were males and 74 were females. There was a preponderance of male patients in
our study, which could be the reflection of the general patterns of sex distribution in the
population of the vicinity of the study site. This could also be due to the common tendency of
parents' over cautious apprehension towards the health of a male child.
Most prescribed antibiotics
In our study, we figured out that ceftriaxone was the highest prescribed followed by
cefuroxime and metronidazole, compared to Kanish R study on the “Prescribing patterns of
antibiotics in the department of pediatrics in a tertiary care medical college hospital”.
Cephalosporins were the highest prescribed, followed by aminoglycosides.
www.wjpps.com Vol 9, Issue 9, 2020.
1911
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Distribution of antibiotics according to pharmacological classification of drugs
Out of 724 antibiotics prescribed in the study, 369 (60%) cephalosporins, 49
(8%)aminoglycosides, 14 (2%) quinolones, 38 (6%) macrolides, 6 (1%) penicillins, 10 (2
beta lactamase inhibitors, 23 (4%) tetracyclins, 4(1%) linezolid, 10 (2%) vancomycin, 10
(2%) meropenem, 8 (1%) antihelmentics, 8 (1%) lincomycin, 3 (0%) rifaximin, 67 (11%)
metronidazole. When compared to the study conducted by Issac A J the total antibiotics
prescribed contains cephalosporin 152 (80%), aminoglycoside 18 (9%), quinolones 13 (7%),
antibiotic combination 4 (2%), B-lactamase inhibitors 2 (1%), macrolide antibiotics 1 (1%)
each. cephalosporin comprised 80% of the prescribed antibiotics, which includes cefixime
1% and ceftriaxone 99%. The mostly used aminoglycoside antibiotic was amikacin, and the
widely used quinolone antibiotics were ofloxacin.
Details of antibiotic treatments in different departments
The detail of antibiotic medication in different departments in our study was figured to be
used as therapeutic, unknown and prophylactic. Prophylactic antibiotic medications were
most commonly experienced in surgical and obstetrics and gynecology units. In 41
medications, the intention was unspecified. Surgery department showed a high prophylactic
prescription of antibiotics. The study conducted by V.K.G Lim on the “Patterns of Antibiotic
Use in Hospitals in Malaysia” indicated that roughly two-thirds of all treatments were for the
purpose of treatment and the others for prophylaxis. The main intention to prescribing
antibiotics was therapeutic in 1,263 (66%) prescriptions and in 32% (614), the purpose was
prophylactic. Prophylactic medications were also more popular assortments of antibiotics.
In 25% of cases antibiotics were prescribed based on culture reports and in most of case
sheets, culture results were not mentioned. It is important to perform prior culture sensitivity
test before prescribing any antibiotics. This can impede the growth of 'antibiotic resistance',
reduce the side effects of drugs, and decrease medication expenses. Moreover this will help
with the selection of appropriate antibiotics. In the current research, 98% of medicines were
prescribed from the WHO list of necessary medicine 2013, which is also related to Kanish et
al research. Strict antibiotic prescribing policy significantly overcome the overuse of
antibiotics and reduces the development of resistance to antibiotics. Prescription pattern
analysis or auditing types of studies are to be conducted on a large scale in different health
sectors. The study will then be more effective and help make local policy for antibiotics
prescription in pediatric and other specialties.

www.wjpps.com Vol 9, Issue 9, 2020.
1912
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Dispensing patterns
Distributing antibiotics without valid prescription and by non-pharmacists are usual in this
particular area. This research also figured various cases of irrational dispensing of antibiotics.
Thus, there has an essential need to deal with these matters and stimulate correct methods of
dispensing of antibiotics.
We also found out that in some pharmacies a different brand of antibiotic was dispensed than
the actual prescribed one without the consultation of physicians. This reveals the commercial
attitude of community pharmacies. In general, a community pharmacy must be like a
professional service provider rather than a business or a trade. We also found that rarely
pharmacists undergo any training or continuous pharmacy education to update themselves for
their professional development. Hence there is need to educate pharmacist on rational use of
antibiotics
Packaging patterns
We invariably found a mismatch between the amount of doses prescribed by the physicians
and the standard packaging sizes available for most common prescribed antibiotics. This type
of packaging pattern may lead to strip cutting, which results in cutting off the medicines
name, date of manufacturing, date of expiry, and sometimes it is difficult to identify which
medicine it is used for. Some patients terminate prescription whenever their signs develop as
well, rather than completing the whole process. This formulates the chance of reutilizing the
symmetry medication for forthcoming usage, boosting the probability of the medication’s
misusage to deal with the non-susceptible organisms.
Medicines dispensed in the original fixed packaging may result in under- or oversupplies of
antibiotics are leading to either suboptimal interval of medication or 'leftover' antibiotics.
Even if general practitioners try to fulfill the approaches, complications in conforming
diagnoses and striving to adjust package size with directions is a significant barrier to
perform very effectively.
Such mismanagement in an interval between guidelines and dictated by packaging may
symbolize that as a substantial amount of antibiotics are allocated and not expended for the
prescribed acute sickness, contributing to redundant antibiotic doses in society. Prescribers
should ensure their attention about the mismatch between antibiotic pack sizes and guideline
suggestions for their interval is contributing to 'antibiotic resistance' in the society.

www.wjpps.com Vol 9, Issue 9, 2020.
1913
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Besides, antibiotics are almost universally packaged by manufacturers in packs that are
heavily run by expense of economies and convenience rather than by any scientific basis or
interval of therapy, individualized packaging adds to the healthcare charge, specifically when
medicines are out-of-pocket charges for clients.
Comprehensive civil insight and sensitization of physicians and modification of hospital
medication system is the necessity of the time to make the modifications at all apparent levels
for the long term and better healthcare result in hospital exercise.
Resistance of Antibiotic is not only a danger issue for a particular sufferer; it decreases the
persuasiveness of traditional medication and serves a prominent danger to civil health by
improving the complexness and outlay of medication and lowering the percentage of a
successful result.
CONCLUSION
In this study, antibiotic prescription and dispensing pattern was not rational as there is poly
pharmacy, overuse and inappropriate use of antibiotics, prescription of antibiotics without
prior culture sensitivity tests, and dispensing of antibiotics without counseling by non
pharmacists. Cephalosporins classes of antibiotics were commonly prescribed and parenteral
route of drug administration was highly used in this research. Average drug encountered per
patient were high (6) which increases the risk of drug interactions and leads to polypharmacy.
Strict antibiotic prescribing policy significantly overcome the overuse of antibiotics and
reduces the development of resistance to antibiotics. Prescribing drugs by generic name and
only after culture sensitivity test and writing prescriptions by the physicians in capital letters
can significantly reduce medication errors and antibiotic resistance. There is a need to switch
over from parenteral to oral route of antibiotics as soon as possible when the clinical
condition permits; this would reduce the cost associated with drug therapy.
General public awareness, sensitization of health care professionals and revision of clinical
drug policy is the need of the hour to bring the changes at all possible level for the long term
and better clinical outcome in medical practice.
Quality of life can be improved by enhancing standards of medical treatment at all levels of
the health care delivery system. Setting standards and assessing the quality of care through
performance review should become part of everyday clinical practice.

www.wjpps.com Vol 9, Issue 9, 2020.
1914
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Proper information on the products packaging material is essential as it may lead to
mislabeling, mismarking or change in the original package and deletion of expiry dates from
the bottles or vials of pharmaceutical products. So, the manufacturers of pharmaceutical
products should be careful in designing the primary and secondary packaging items of
antibiotic drug products.
This emphasizes the urgent need for vigilant surveillance, formulation of strict antibiotic drug
policies, implementation of standard protocols for antibiotics usage, stringent infection
control practices as well as rational antibiotic prescription in order to streamline the judicious
use of antibiotics which will have a significant positive economic benefit and improved
quality of care being delivered to patients.
Public attention, sensitization of physicians, pharmacists and manufacturers for modification
of prescribing, dispensing and packaging patterns of antibiotics is necessary for rational use
of antibiotics. Excellence in healthcare can be boosted by improving the prescribing,
dispensing and packaging pattern of antibiotics by physicians, pharmacists and by
manufacturers in healthcare system. Establishing ideas and evaluating the excellence of care
through performance analysis is the need of the hour in everyday hospital practice.
BIBLIOGRAPHY
1. Adepu R, N. B. Attitudes and behaviours of practicing community pharmacists towards
patient counseling. Indian Journal of Pharmaceutical Sciences, 2009; 71(3): 285-289.
2. Anderson C, B. A. Feedback from community pharmacy users on the contribution of
community pharmacy to improving the public’s health: A systematic review of the peer-
reviewed and non-peer reviewed literature 1990–2002. Health Expect, 2004; 7: 191–202.
3. Anitha Nandagopal, A. K. Rational drug prescribing structure in geriatric patients.Indian
Journal of Pharmacy Practice, 2017; 10(3): 1071-1075.
4. Anong DN, A. J. Prescribing structures and associated factors of antibiotic prescription in
primary healthcare systems of Kumbo East and Kumbo West Health Districts, North
West Cameroon, 2018; 13(3): 1-18.
5. Asmelashe Gelayee D, B. M. Practice and barriers towards provision of health promotion
services among community pharmacists in Gondar, Northwest Ethiopia. Bio-Med Res Int.
Article, 2017; Id: 7873951.
6. El Hajj M S, S. S. Public’s attitudes towards community pharmacy in Qatar: A pilot
study. Patient Prefer. Adherence, 2011; 5: 405.

www.wjpps.com Vol 9, Issue 9, 2020.
1915
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
7. Gopalakrishnan Sekharan, G. P. Assessment of prescribing practices among urban and
rural general practitioners in Tamil Nadu. IndianJournal of Pharmacology, 2013; 45(3):
252-257.
8. Jose J, A. S. Public’s perception and satisfaction on the roles and services provided by
pharmacists–Cross-sectional survey in Sultanate of Oman. Saudi Pharm J, 2015; 23:
635–641.
9. Kanish R, G. K. Prescribing structure of antibiotics in the department of pediatricsin
tertiary care medical college clinical in Northern India. Asian Journal of Medical
Sciences, 2014; 5(4): 69-7.
10. Lea V M, C. S. Workload and its impact on community pharmacist’s job satisfaction and
stress: A review of the literature. Int J Pharm Pract, 2012; 20: 259–271.
11. lor C, B. L. Antimicrobial resistance: risk associated with antibiotic overuse andinitiatives
to reduce the problem. Therapeutic advances in drug safety, 2014; 5: 229–41.
12. McIntosh J, R. S. Changing oral contraceptives from prescription to over- the-counter
status: An opinion statement of the Women’s Health Practice and Research Network of
the American College of Clinical Pharmacy. Pharmacother J Hum Pharm, 2011; 31:
424–437.
13. Northey A, M. T. Patients antibiotic knowledge: A trial assessing the impact of verbal
education. Int J Pharm Pract, 2015; 23: 158–160.
14. Sakeena M, B. A. Enhancing pharmacist’s role in developing countries to overcome the
challenge of antimicrobial resistance: A narrative review. Antimicrob Resist Infect
Control, 2018; 7: 63.
15. Saramunee K, K. J. How to enhance public health service utilization in community
pharmacy? General public and health providers perspectives. Res Soc Adm Pharm, 2014;
10: 272–284.
16. T. K. Challenges to pharmacy and pharmacy practice in Pakistan. Australias Med J.,
2011; 4: 230.
17. Watson M C, B. C. Factors are predicting the guideline compliant supply (or non-supply)
of non-prescription medicines in the community pharmacy setting. BMJ Qual Saf, 2006;
15: 53–57.
18. Watson M C, H. J. Exploring the supply of non-prescription medicines from community
pharmacies in Scotland. Pharm. World Sci, 2008; 30: 526–535.

www.wjpps.com Vol 9, Issue 9, 2020.
1916
Jamal et al. World Journal of Pharmacy and Pharmaceutical Sciences
19. Yang S, K. D. A comparison of patients and pharmacists satisfaction with medication
counseling provided by community pharmacies: A cross-sectional survey. BMC Health
Serv Res, 2016; 16: 131.