Embed Size (px)
Citation preview

8/3/2019 Assessment of 193 Candidate Genes for thy
http://slidepdf.com/reader/full/assessment-of-193-candidate-genes-for-thy 1/8
CLINICAL SCIENCES
Assessment of 193 Candidate Genes for Retinopathyin African Americans With Type 1 Diabetes
Monique S. Roy, MD; D. Michael Hallman, PhD; Yi-Ping Fu, PhD; Mirta Machado, BS; Craig L. Hanis, PhD
Objective: To report in African Americans with type 1diabetes the association of single-nucleotide polymor-phisms in 193 candidate genes with diabetic retinopa-thy (DR) and/or its progression.
Methods: A custom panel of 1536 single-nucleotide poly-morphisms located on 193 candidate genes for DR wasgenotyped in 437 African Americans with type 1 diabe-tes who participated in the New Jersey 725 study. Clini-
cal evaluations at baseline and follow-up examinationsincluded structured clinical interview, ocular examina-tion, 7-field stereoscopic fundus photographs, and bloodpressure measurements. Severity of DR was determinedvia masked grading of fundus photographs. Biologicalevaluations included blood and urine assays.
Results: Single-nucleotidepolymorphismsin 13candidategenesforDR involvedin glucose metabolism, angiogenesis,inflammation, neurotransmission, hypertension,and reti-naldevelopmentweresignificantlyassociatedwiththepreva-lence of severe DR. Three of these genes were also signifi-cantlyassociatedwithprogression ofDR.Adjusting forsex,durationofdiabetes,glycosylatedhemoglobin, systemichy-pertension, and total cholesterol did not alter the results.
Conclusions:
Our data support the role of genetic fac-tors to account forseverity and/orprogressionof DR in Afri-can Americans with type 1 diabetes and to identify severalprime genes that likely contribute to the risk of DR.
Arch Ophthalmol. 2009;127(5):605-612
DESPITE EFFECTIVE TREAT-ments for the severeforms of diabetic reti-nopathy (DR), the dis-ease remains the leading
cause of blindness in 20- to 64-year-old
persons with diabetesmellitus (DM) in theUnited States.1,2 In this group, prolifera-tive DR (PDR) and macular edema are the2 main causes of visual loss.3 Environ-mental and clinical risk factors for PDRhave been reported previously for vari-ous populations with type 1 DM and in-clude longer durationof diabetes, poor gly-cemic control, systemic hypertension, andproteinuria.3,4 These, however, account foronly a portion of the severe forms of thedisease.5 Familial aggregationof severe DR,independent of theknown clinical risk fac-tors, has been reported in patients with
DM.6-11
Thus, it is likely that genes, pos-sibly combined with environmental fac-tors, account for some of the variance inDR severity.12-14
While the pathophysiology of DR re-mains unclear, a number of metabolicpathways and their associated genes havebeen implicated.13-16 Such candidate genesinclude those involved in glucose metabo-lism and transport, synthesis and degra-dation of basement membranes, angio-
genesis, inflammation, blood pressureregulation, coagulation, and neurotrans-mission. Previously published studies of these candidate genes for DR, however,have yielded conflicting data, most likelythe result of many studies having in-
volvedsmall samplesizes andpoorly char-acterized phenotypes.11,14,16-19 Other po-tential problems may include populationstratification and the possible involve-ment of more than 1 gene.
We previously assembled (baseline),examined (baseline), and reexamined(6-year follow-up) a large, geographi-cally well-defined population of AfricanAmericans with diagnosed type 1 DM: theNew Jersey 725.4,5,20,21 At each examina-tion, patients’ retinal status was well char-acterized using masked grading of the7-field stereoscopic fundus photo-
graphs.22-24
Standard protocols were usedto document diabetic complications andbiological abnormalities. We found thatclinical risk factors associated with eitherany progression of DR or progression toPDR accounted for only 27% of the vari-ance in DR severity.5 Because our New Jer-sey 725 cohort provides a unique oppor-tunity to examine genes associated withDR in African Americans with type 1 DM,we studied the associations between se-
Author Affiliations: TheInstitute of Ophthalmology andVisual Science, University of Medicine and Dentistry, New Jersey Medical School, Newark(Dr Roy); and Human GeneticsCenter, University of TexasHealth Science Center atHouston School of PublicHealth, Houston (Drs Hallman,Fu, and Hanis andMs Machado).
(REPRINTED) ARCH OPHTHALMOL/ VOL 127 (NO. 5), MAY 2009 WWW.ARCHOPHTHALMOL.COM605
©2009 American Medical Association. All rights reserved. on February 15, 2012www.archophthalmol.comDownloaded from

8/3/2019 Assessment of 193 Candidate Genes for thy
http://slidepdf.com/reader/full/assessment-of-193-candidate-genes-for-thy 2/8
vere DR and/or its progression andpolymorphisms in 193candidate genes in this population.
METHODS
STUDY POPULATION
The original cohort consisted of 725 African Americans withtype 1 DM who participated in the New Jersey 725 study be-
tween 1993 and 1998.20
Patients with a discharge diagnosis of DM wereidentified fromthe New Jersey Hospitaldischarge data,which lists all patients who have been admitted to New Jerseyhospitals. This computer-generated list includes demographicinformation about patients, including race. African Ameri-cans with diagnosedDM andtreatedwith insulin before 30 yearsof ageand who were currently taking insulin were further iden-tified from a random review of 13 615 medical records. Exclu-sion criteria were type 2 DM, diagnosis after age 30 years, andmaturity-onset diabetes of youth.25-27 Ethnicity was deter-mined from the hospital record and later confirmed by self-identification. Patients were also asked to confirm that both of their parents were African American. Of the original cohort of 725 subjects, 508 participated in the 6-year follow-up exami-nation between 1999 and 2004. At the 6-year follow-up, 25 of the 508 participants (4.9%) who were no longer receiving in-sulin were excluded from further analyses.21 Of the remaining483 patients, blood was drawn for genetic studies in 337 pa-tients at thetimeof the6-year follow-upand in 82 patients whowere subsequently recalled for blood draws between 2005 and2006. An additional 18 African Americans with type 1 DM werealso recruited for genetic studies using the same inclusion cri-teria asin the patients inthe New Jersey 725 study.20 Thus, therewere 437 patients available for genotyping.
CLINICAL PROCEDURES
Patients were examined in the Eye Clinic of University Hospi-tal in Newark, New Jersey. Upon arrival, informed written con-sent was obtained from each study participant. Patients under-
went a complete eye examination that included dilated retinalexaminationand 7-fieldstereoscopic DiabeticRetinopathyStudyretinal photographs.22 Also obtained were height, weight, andblood pressure measurements. A structured clinical interviewincluded detailed medical and ophthalmologic histories as wellas sociodemographic factors and lifestyle variables. Previousophthalmic medical records were obtained. Dates of all previ-ous ophthalmologic procedures, including panretinallaser pho-tocoagulation and/or pars plana vitrectomy for PDR were re-corded. Venous blood was drawn for measurement of totalglycosylated hemoglobin and high- and low-density lipopro-tein cholesterol and total cholesterol. A 4-hour timed urine col-lection was obtained for measurementof albumin excretionrateand creatinuria. The institutional review board at the Univer-sity of Medicine and Dentistry of New Jersey, New Jersey Medi-cal School, Newark, approved the study.
DR GRADING, SEVERITY, PROGRESSION,AND AGE AT DIAGNOSIS
Color fundus photographs were graded for DR severity in amasked fashion by the Wisconsin Fundus Photograph Read-ing Center in Madison. The modified Early Treatment of Dia-betic Retinopathy Study Airlie House classification of DR wasused.23,24 Level 10 indicates no DR; levels 20 to 53, nonprolif-erative DR of increasing severity; and levels 61 to 85, PDR of increasing severity.24
The following variables were recorded and defined:
Severe DR is defined as an EarlyTreatmentof DiabeticReti-nopathy Study level of 53 or greater in the worse eye or his-tory of panretinallaserphotocoagulationor vitrectomyfor PDR.24
For patients with severe DR, age and duration of DM are re-cordedat thetimethat severe DR wasfirst documented, ie,eitherat the time of the first laser or vitrectomy procedure, as re-corded in the patients’ medical record, or if no procedure hadbeen done at the time of the study examination when severeDR was found. For patients without severe DR, clinical char-
acteristics are those recorded at the time of the last follow-upexamination.
Progression of DR was defined in the337 patients in the New Jersey 725study whohad nonproliferative DR at baseline (ie, DRseverity level in the worse eyeof 61 andno panretinal laser pho-tocoagulation or vitrectomy). For those patients, progression atthe 6-year follow-up was considered absent if DR severity levelin the worse eye remained below 61 and there was either (1) nochange in DR severity level (eg, severity level of 35 at both base-line and 6-year follow-up) or (2) an increase of 2 or fewer sever-ity levels (eg, level 10 at baseline increasing to level 35 at 6-yearfollow-up). Progression wasconsidered severeif DR severity levelat the6-year follow-up either (1)increasedto 61 or higherand/orthe patient had undergone panretinal laser photocoagulation orvitrectomy, or (2) went from level 10 at baseline to level 53 at
the 6-year follow-up. All other patients were considered to haveintermediate progression.Age at diagnosis of DM was defined as the age at which the
diagnosisof DM wasfirst recordedin thepatient’s hospitalrec-ord by a physician. Systemichypertensionwas defined as presentif either the systolic blood pressure was 140 mm Hg or higherand/or the diastolic blood pressure was 90 mm Hg or higher,or if the patient was taking antihypertensive medication. Mi-croproteinuria was considered to be present if the albumin ex-cretion rate was 20 to 200 µg/minute. Overt proteinuria wasconsidered to be present if the baseline albumin excretion ratewas greater than 200 µg/minute or the patient had dialysis orhad had a kidney transplant.
GENOTYPING
Selection of Candidate Genesand Single-Nucleotide Polymorphisms
Single-nucleotide polymorphisms (SNPs) were chosen primar-ily from amonggenes that appear to be good candidates for eitherinvolvement in the metabolic processes underlying the eventsleading to DR or the clinical risk factors for DR as well as fromthose that have previously demonstrated potential associa-tions with DR.13,15,16 Special attention was given to genes in-volved in glucose transport and metabolism, angiogenesis, in-flammation, neurotransmission, hypertension, and retinaldevelopment. A total of 1536 SNPs were selected to constructa GoldenGate Custom Panel (Illumina Inc, San Diego, Cali-fornia).Once a gene wasselected, on average 8 SNPs were cho-
sen based on their distribution across the primary block struc-tures of the gene to capture the haplotype diversity across thegene. A set of tagging SNPs was first selected using Tagger.28
These were then assessed for the availability of a GoldenGateassay(Illumina). Preference was givento nonsynonymous SNPsand those reported to have minor allelefrequenciesgreater than0.10 in more than 1 population. The 5 (1000 base pairs) and3 (2500 base pairs) noncoding regions were included as partof the definition of a gene for SNP selection. Plates were con-structed with duplicate and quality-control samples. Genotyp-ingwas performedat the University of Texas SouthwesternMedi-cal Center’s Microarray Core Facility, Dallas.
(REPRINTED) ARCH OPHTHALMOL/ VOL 127 (NO. 5), MAY 2009 WWW.ARCHOPHTHALMOL.COM606
©2009 American Medical Association. All rights reserved. on February 15, 2012www.archophthalmol.comDownloaded from

8/3/2019 Assessment of 193 Candidate Genes for thy
http://slidepdf.com/reader/full/assessment-of-193-candidate-genes-for-thy 3/8
Assessment of Population Stratification UsingAncestry Informative Markers
The samples have been previously genotyped for 186 ancestrymarkers.29 The same ancestry informative markers have alsobeen genotyped in 1051 individuals from the 51 worldwidepopulations represented in the Human Genome Diversity Pro-
ject–Centre d’Etude du Polymorphisme Humain Human Ge-nome Diversity Cell Line Panel (http://www.cephb.fr
/HGDP-CEPH-Panel). The program structure 2.2 (http://pritch.bsd.uchicago.edu/software.html) has been run simultaneouslyusing the ancestry informative marker genotypes from oursample and the 51 Centre d’Etude du Polymorphisme Hu-main populations to identify population substructure and tocompute individual ethnic factor scores. This ancestry assess-ment showed a lack of substantial substructure with a Euro-pean factor score on average of 0.09 (median, 0.04). Both aMiddle East and an Asian factor had an average score of 0.06(median, 0.04).
STATISTICAL ANALYSIS
All SNPs wereassessed for qualitycontrol, which included test-ing for Hardy-Weinberg equilibrium, call rate, and minor al-lele frequencies. Two strategies were used in the analysis. For
individual SNPs, analyseswere performed irrespectiveof quality-control considerations, but significant SNPs that failed quality-controltestswere eliminated. Forhaplotype analyses, SNPswereremoved prior to analysis based on a minor allele frequency of less than 0.05, a call rate of less than 0.80, or P .001 for de-parture from Hardy-Weinberg equilibrium.
Testing of individual SNPs was done using logistic regres-sion with sex, diabetes duration, glycohemoglobin, and choles-terol as covariates. Haplotype trend regression for 2- to 6-locushaplotypes, usingsliding windows, was alsoperformed, withthesame covariates as with individual SNPs.30 Analyses were con-ducted usingHelixTree (Golden Helix Inc, Bozeman, Montana).
RESULTS
Clinical characteristics of the patients with (n= 128) andwithout (n=309) severe DR are presented in Table 1.Compared with patients without severe DR, those withsevere DR were more likely to have a longer duration of DM (P =.003), systemic hypertension (P .001), overtproteinuria (P .001), higher blood cholesterol levels(P .001), and depression (P .001); and to be older(P .001). There was no significant difference in mean
Table 1. Characteristics of Patients With and Without Severe DR
Characteristic
Mean (SD)
OR (95% CI) P ValuePatients Without Severe DR
(n=309)Patients With Severe DRa
(n=128)
Age at diagnosis of diabetes, y 16.42 (7.85) 17.16 (7.37) 1.01 (0.99-1.04) .36b
Age, y 31.39 (10.94) 34.82 (8.89) 1.03 (1.01-1.05) .001b
Duration of diabetes, y 15.01 (8.12) 17.49 (7.04) 1.04 (1.01-1.07) .003b
Glycosylated hemoglobin, % of total
hemoglobin
12.16 (3.20) 12.40 (3.87) 1.02 (0.96-1.08) .55b
Total cholesterol, mg/dL 195.75 (51.00) 219.99 (57.21) 1.01 (1.00-1.01) .001b
Body mass indexc 28.46 (7.40) 29.35 (9.66) 1.01 (0.99-1.04) .35b
AER, µg/mind 271.81 (845.76) 1201.52 (4533.88) 1.00 (1.00-1.01) .04b
Sex, No. (%)
M 134 (43.47) 46 (35.94) 0.73 (0.48-1.12).15e
F 175 (56.63) 82 (64.06) 1.00
Hypertension, No. (%) f,g
No 196 (64.26) 45 (35.16) 1 [Reference].001e
Yes 109 (35.74) 83 (64.84) 3.32 (2.15-5.11)
Proteinuria, No. (%) f
None 152 (50.84) 25 (20.33) 1 [Reference]
.001eMicroproteinuria 75 (25.08) 28 (22.76) 2.27 (1.24-4.16)
Overt 62 (20.74) 56 (45.53) 5.49 (3.15-9.58)
Dialysis/kidney transplant 10 (3.34) 14 (11.38) 8.51 (3.41-21.25)
Progression of DR, No. (%) f
None 230 (78.23) 4 (5.33) 1 [Reference] .001e
Intermediate/severe 64 (21.77) 71 (94.67) 63.78 (22.44-181.27)
Depression, No. (%) f,h
No 228 (85.07) 85 (67.46) 1 [Reference].001e
Yes 40 (14.93) 41 (32.54) 2.75 (1.66-4.54)
Abbreviations: AER, albumin excretion rate; CI, confidence interval; DR, diabetic retinopathy; OR, odds ratio.SI conversion rate: To convert total cholesterol to millimoles per liter, multiply by 0.0259.a Early Treatment Diabetic Retinopathy Study Research Group classification: in the worse eye, laser grade of 53 or greater24 or previous laser panretinal
photocoagulation or vitrectomy for proliferative DR.b t Test.c Calculated as weight in kilograms divided by height in meters squared.d No proteinuria, less than 20 µg/minute; microproteinuria, 20 to 200 µg/minute; and overt microproteinuria, greater than 200 µg/minute.e2 Test.f Value may vary owing to missing data.g Systolic blood pressure of 140 mm Hg or greater and/or diastolic blood pressure of 90 mm Hg or greater, or use of antihypertensive medication.h A Beck Depression Inventory score of 14 or less indicates no depression; and a Beck Depression Inventory score greater than 14 indicates depression.
(REPRINTED) ARCH OPHTHALMOL/ VOL 127 (NO. 5), MAY 2009 WWW.ARCHOPHTHALMOL.COM607
©2009 American Medical Association. All rights reserved. on February 15, 2012www.archophthalmol.comDownloaded from

8/3/2019 Assessment of 193 Candidate Genes for thy
http://slidepdf.com/reader/full/assessment-of-193-candidate-genes-for-thy 4/8
follow-up between patients in the New Jersey 725 studywith (n=124) and without (n=295) severe DR (mean[standard deviation (SD)], 7.6 [2.1] years vs 7.3 [2.0]years; t417=1.26, P=.2).
A total of 1536 SNPs from 193 retinopathy candidategenes were selected. An overall call rate of 98% was ob-tained. Of the 1536 SNPs, 10 in this sample were mono-morphic and were excluded. Following adjustment forsex, duration of DM, glycosylated hemoglobin, and cho-
lesterol,5 of the1526 were significant at P.001, 12 weresignificant at P .01 but P .001, and 61 were signifi-cant at P .05 but P .01. Of these, 3, 11, and 52 SNPs,respectively, also met all quality-control criteria. Signifi-cant associations between SNPs and severe DR are pre-sented in Table 2 for the genes with at least 1 SNP atP .01. Only the most significant SNP for each gene istabulated after adjustment. Results for all genes and SNPsunder different adjustmentsandtheir quality-control char-acteristics are provided in a supplemental table (http: //www.umdnj.edu/eyeweb/library/supplemental_table
.pdf). These results were largely robust to adjustment forother clinical risk factors for DR (ie, hypertension, pro-teinuria, or depression).
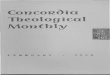
To get a handle on the contribution of variation in eachof these candidate genes to retinopathy susceptibility (asopposed to the contribution of individual SNPs), we useda sliding-window haplotypes approach using windowsthat ranged from 2 to 6 SNPs and we used a graphicalrepresentation of an assessment of P values to examine
results (GrASP31
). Haplotype analysis led to the classifi-cation of 4 genes as being of particular interest: BBS2,HTR1B, a region containing both PROS1 and ARL6, andDRD2. We illustrate the approach based on BBS2(Figure). Fifteen SNPs were genotyped in BBS2. Theflanking SNPs were rs2288056 and rs17841923. In thesingle SNP analysis, 2 SNPs demonstrated significanceat P =.01: rs4784675 (Table 2) and rs12596017. Haplo-type analysis identified a region of BBS2 in which hap-lotypes consistently demonstrated a strong associationwith DR, seemingly centered on rs4784675 with
Table 2. Retinopathy Candidate Genes Having at Least 1 SNP at P .01a
Gene Symbol Gene Name SNP Chromosome P Value
HTR1B Serotonin receptor 1B rs1228814 6 .000107
SLC2A1 Sol ute carrier famil y 2 (facili tated gl ucose transporter), member 1 rs841846 1 .000535
BBS2 Bardet-Biedl syndrome 2 rs4784675 16 .00227
PROS1 Protein S rs13062355 3 .00325
FLT1 FMS-like tyrosine kinase 1 rs622227 13 .00449
ENPP1 Ectonucleotide pyrophosphatase/phosphodiesterase 1 rs1409181 6 .00470
HLA-B Major histocompatibility complex, class I, B rs2523608 6 .00549ROBO2 Roundabout, axon guidance receptor, homologue 2 (Drosophila ) rs10865559 3 .00671
DRD2 Dopamine receptor D2 rs7131056 11 .00716
ANGPT1 Angiopoietin 1 rs1283649 8 .00818
Abbreviation: SNP, single-nucleotide polymorphism.a For each gene, only the most significant SNP is listed with its P value after adjusting for sex, diabetes duration, glycosylated hemoglobin, and cholesterol.
Minimum
.036091
.006962
.000560
.000560
.000463
.000194
.000134
.000134
.000134
.000134
.000134
.001230
.002845
.004705
.004705
P Value
Single SNP
.791241
.009853
.630204
.965396
.801801
.358209
.531698
.002267
.910377
.918290
.169129
.747037
.959504
.256130
.065728
SNP
rs2288056
rs12596017
rs2059288
rs11640452
rs12447395
rs8049949
rs1559452
rs4784675
rs12447295
rs2161738
rs16958311
rs11373000
rs2288058
rs17841922
rs17841923
Figure. Graphical assessment of P values of haplotypes’ sliding window for BBS2 . Significance of each haplotype is represented as a “heat” map, with greenrepresenting nonsignificant results and red, the most significant results. The minimum P value is the lowest across any of the haplotype windows. SNP indicatessingle-nucleotide polymorphism.
(REPRINTED) ARCH OPHTHALMOL/ VOL 127 (NO. 5), MAY 2009 WWW.ARCHOPHTHALMOL.COM608
©2009 American Medical Association. All rights reserved. on February 15, 2012www.archophthalmol.comDownloaded from

8/3/2019 Assessment of 193 Candidate Genes for thy
http://slidepdf.com/reader/full/assessment-of-193-candidate-genes-for-thy 5/8
P=1.3410−4 (Figure). Similar results were obtained forthe other 3 genes/regions. In each instance for these 4candidates, at least 1 of the haplotype analyses amongthe set of all haplotype analyses for that gene exceeded a
Bonferroni-corrected P value of .05. While a comparable set of data is not available for rep-
lication, we analyzed the longitudinal data for progres-sion of DR. In this analysis, those with the most severeDR were excluded, as there was no further progressionto be documented. Individuals were classified as havinglittle or no change vs progressors (either intermediate orprogression to severe disease). In this analysis, 95 SNPswere significant (P =.05) with 76 meeting all quality-control criteria. This includes 4 (3 passing quality con-trol) that were significant at P .001 and 19 (14 passingquality control) at P=.01. Table 3 lists the most signifi-cant SNP in each of the genes that have at least 1 SNP atP .01. Note that SLC2A1, FLT1, and HLA-B have the
highest significance for both prevalent disease as well asfor progression and that the same SNP for both is mostassociated. While HTR1B, BBS2, ROBO2, DRD2, and ANGPT1 have the highest significance for prevalent dis-ease and do not appear in Table 3 with P .01, they eachhave at least 1 SNP that is significant at P =.05 forprogression.
COMMENT
In the present study, we found that SNPs in 10 genes in-volved in glucose transport and metabolism, angiogen-esis, neurotransmission, hypertension, and retinal de-
velopment were significantly associated with severity of DR in African Americans with type 1 DM. Three of thosesamegenes werealsosignificantly associated withthe pro-gression of DR. These data confirm a role of genetic fac-tors in relation to the development of DR and indicatethat more than 1 pathway may be involved.12,14 These re-sults were robust to adjustment for other clinical risk fac-tors for DR in this population. We will not discuss eachgene that demonstrated association. Rather, we will high-light the biological plausibility for several to illustrate themerits and implications of these results.
On chromosome 1, 1 of the glucose transporter genes(SLC2A1 or GLUT1)—a member of a family of sodium-independent glucose transporter proteins—is signifi-cantly associated with both severe DR and progression
of DR. GLUT1 is the predominant glucose transporteracross endothelial cells of the inner blood-retinal bar-rier into the retina.32,33 In DM, increased glucose trans-port and/or GLUT1 expression in endothelial cells is up-regulated by hypoxia, growth factors, and/or cytokines,all of which are present in DR.34-36 GLUT1 is also ex-pressed in the retina in nonvascular cells (ie, glia, gan-glion cells, and photoreceptors).33 In DM,those cells showabnormalities that maycontribute to the vascular changesofDR.37 Because hyperglycemia is 1 of the strongest clini-cal risk factors for progression of DR, GLUT1 is a likelycandidate gene for DR.38 It is noteworthy that polymor-phism of GLUT1 has so far been implicated only in dia-betic nephropathy.16,39,40 Oxidative stress resulting fromhyperglycemia is another potential etiopathogenic fac-tor for DR.13,15 In support of this is our finding that geneswith antioxidant properties, RXRA and CAT , are signifi-cantly associated with progression of DR.41-43
Neovascularization and increased retinal vascular per-meability are present in DR and are the 2 major causesof visual loss.3 In our African American patients with dia-betes, 2 genes related to angiogenesis— ANGPT1 on chro-mosome 8 and FLT1 on chromosome 13—are signifi-cantly associated with severe DR and/or its progression.Angiopoietin 1 is a protein secreted by a variety of cells,including pericytes. It has angiogenic actions that are dis-tinct from those of vascular endothelial growth factor and
are mediated via a tyrosine kinase receptor expressed al-most exclusively on endothelial cells.44,45 Angiopoietin1 also has anti-inflammatory properties, suppressing theexpression of adhesion molecules and blocking vascu-lar permeability through vascular endothelial growth fac-tor inhibition and strengthening of endothelial tight junc-tions.46 FLT1 is a tyrosine kinase receptor, which isexpressed on the surface of retinal vascular endothelialcells and mediates the biological effects of vascular en-dothelial growth factor.47,48 FLT1 is also expressed in pe-ripheral blood monocytes and neutrophils, where it trig-
Table 3. Retinopathy Candidate Genes Having at Least 1 SNP Associated With Progression of Retinopathy at P .01a
Gene Symbol Gene Name SNP Chromosome P Value
RXRA Retinoid X receptor rs3132300 9 .0000911
SLC2A1 Solute carrier family 2 (facilitated glucose transporter), member 1 rs841846 1 .000160
TF Transferrin rs3811647 3 .000531
PLA2G4A Phospholipase A2, group IVA (cytosolic, calcium-dependent) rs932476 1 .00153
CAT Catalase rs566979 11 .00311
PPARG Peroxisome proliferator-activated receptor rs10510419 3 .00478
HLA-B Major histocompatibility complex, class I, B rs2523608 6 .00599SLC2A11 Solute carrier family 2 (faci litated glucose transporter), member 11 rs4822441 22 .00665
INSR Insulin receptor rs10500204 19 .00696
FLT1 FMS-like tyrosine kinase 1 rs622227 13 .00735
ITGB5 Integrin5 rs9865359 3 .00774
SLC24A3 Solute carrier family 24 (sodium/potassium/calcium exchanger), member 3 rs2294895 20 .00778
OLR1 Oxidized low-density lipoprotein (lectin-like) receptor 1 rs2742115 12 .00876
Abbreviation: SNP, single-nucleotide polymorphism.a For each gene, only the most significant SNP is listed with its P value after adjusting for sex, diabetes duration, glycosylated hemoglobin, and cholesterol.
(REPRINTED) ARCH OPHTHALMOL/ VOL 127 (NO. 5), MAY 2009 WWW.ARCHOPHTHALMOL.COM609
©2009 American Medical Association. All rights reserved. on February 15, 2012www.archophthalmol.comDownloaded from

8/3/2019 Assessment of 193 Candidate Genes for thy
http://slidepdf.com/reader/full/assessment-of-193-candidate-genes-for-thy 6/8
gers chemotactic migration.49 Thus, both ANGPT1 andFLT1 have a key role not only in angiogenesis and modu-lation of vascular permeability, but also in inflamma-tion. Clinical and experimental data support the role of inflammation in DR.50 In the present study, other genesinvolved either in inflammation (PLA2G4A, OLR1, andPPARG) or in the immune response (HLA-B) are associ-ated with progression of DR, further underlining the closerelationship of angiogenic and inflammatory pathways
in DR. It is noteworthy, however, that while HLA poly-morphisms have been implicated in the susceptibility totype 1 DM, previouslypublishedstudies investigatingtheirpossible role in the development of DR have yielded con-flicting results.51
The ENPP1 gene on chromosome 6 is a type II trans-membrane glycoprotein that cleaves various substrates,eg, the phosphodiester bonds of nucleotide sugars.52
ENPP1 is thought to inhibit insulin signal transductionby interacting with the insulin receptor subunit.52 Over-expression of ENPP1 results in insulin resistance, a meta-bolic abnormality that is present in type 1 DM and thathas been linked to the vascular complications of DM.52,53
ENPP1 is also a binding partner of integrins—
extracellular matrix proteins involved in cell adhesion,cell communication, and angiogenesis.52,54 In our Afri-can American patients, the integrin 5 gene is associ-ated with progression of DR. Interestingly, the integrin5 protein is expressed in the retinal fibrovascular tis-sue of PDR.55,56
In the present study, dopamine receptors DRD1 andDRD2 (located on chromosomes 5 and 11, respectively)and the serotonin receptor HTR1B (located on chromo-some 6) show an association with severe DR and/or itsprogression, though DRD1 had a minor allele frequencyof less than 0.05. DRD1 and DRD2 are expressed in theretina, where dopamine is the main catecholamine.32,57
Dopamine, in addition to its effects as a neurotransmit-
ter, modulates retinal vessel diameter and retinal bloodflow.58 The DRD1 receptor gene is also involved inblood pressure regulation, and polymorphisms in thisgene have been implicated in essential hypertension.59,60
HTR1B is expressed in ganglion cells in the retina.61 Inaddition to being a neurotransmitter, serotonin is amajor product of platelet activation and inducesendothelium-dependent vasodilation through the for-mation of nitric oxide.61 Thus, DRD1, DRD2, andHTR1B could influence the development of DR eitherthrough signaling within retinal cells or by influencingretinal blood flow. Furthermore, growth factors, eg,vascular endothelial growth factor, appear to affect bothvascular and nervous systems, and this may have poten-
tial relevance to DR.62
Our data also indicate that genes involved in retinaldevelopment are associated with severe DR. In fact, of all the genes reported here, BBS2 shows the strongest as-sociation with severe DR (Figure). Little is known aboutthe functions of the Bardet-Biedl syndrome proteins ex-cept that BBS2 abnormalities have been linked to retinaldegeneration and increased incidence of DM and hyper-tension.63 ROBO2 is an axon-guidance receptor locatedin the cell membrane. It belongs to the immunoglobulinsuperfamily and is expressed in the retina.32,64,65 ROBO2
is also involved in cell adhesion and chemotaxis, bothof which may explain its potential role in DR. The roleof these developmental genes in relation to DR, how-ever, remains to be elucidated.
Strengths of our study include the geographically well-defined diabetic African American population, for whomcross-sectional and longitudinal DR data as well as clini-cal risk factors for DR are available, and in whom single-gene as well as haplotype associations were examined.
While only some of the candidate genes and specificallychosen SNPs were included, the data gathered thus farare unique and provide support for some of the pro-posed mechanisms underlying the development of DR.
Because the pathogenesis of DR likely involves nu-merouspathways,some contributory genes mayhavebeenomitted. Future genome-wide association studies are ex-pected to yield information for identifying additional genesof importance in the development of DR. Our findingsmay be confounded by the use of multiple comparisons,though we have been careful to use conservative P val-ues. Finally, results of the study may not apply to otherpopulations because of racial differences in genetic risksfor the disease. This does not mean, however, that genes
implicated herein cannot affect susceptibility in otherpopulations. A challenge with the present study is thelack of comparable data for replication. The longitudi-nal data collected become valuable in this regard, as onewould expect that some genes contributing to the devel-opment of disease would also contribute to the progres-sion of disease. Thus, those genes implicated in bothTables 2 and 3 would be given higher priority forfollow-up.
To date, efforts to reduce severity of DR have tar-geted clinical risk factors for the disease, aiming specifi-cally at tight glycemic and blood pressure control. Thesechanges are often either not attained or only partiallyachieved. Identifying genes that may be responsible for
severity of the disease may help not only to better un-derstand the pathogenesis but also to develop new ap-proaches to the treatment of DR. The data we reportedherein provide support for a polygenic component of se-vere DR. Additional studies that examine other candi-date genes for the development of DR in our populationof African Americans with type 1 DM are ongoing.
Submitted for Publication: September 8, 2008; final re-vision received December 19, 2008; accepted January 5,2009.Correspondence: Monique S. Roy, MD, The Institute of Ophthalmology and Visual Science, University of Medi-
cine and Dentistry of New Jersey, New Jersey MedicalSchool, 90 Bergen St, Ste 6164, Newark, NJ 07101-1709([email protected]).Author Contributions: Dr Roy had full access to all of the data in the study and takes full responsibility for theintegrity of the data and the accuracy of the data analysis.Financial Disclosure: None reported.Funding/Support: This research was supported by grant8-2004-780 from the Juvenile Diabetes Research Foun-dation and by a Lew Wasserman Merit Award from Re-search to Prevent Blindness.
(REPRINTED) ARCH OPHTHALMOL/ VOL 127 (NO. 5), MAY 2009 WWW.ARCHOPHTHALMOL.COM610
©2009 American Medical Association. All rights reserved. on February 15, 2012www.archophthalmol.comDownloaded from

8/3/2019 Assessment of 193 Candidate Genes for thy
http://slidepdf.com/reader/full/assessment-of-193-candidate-genes-for-thy 7/8
REFERENCES
1. National Society to Prevent Blindness. Vision Problems in the US: Data Analy-
sis,Definitions, DataSources, DetailedData Tables,Analysis, Interpretation. New
York, NY: National Society to Prevent Blindness; 1980.
2. Ferris FL III, Davis M, Aiello L. Treatment of diabetic retinopathy. N Engl J Med .
1999;341(9):667-678.
3. Klein R, Klein B. Vision disorders in diabetes. In: National Diabetes Data Group,
ed. Diabetesin America. 2nded. Bethesda,MD: NationalInstitutes of Health, Na-
tional Institute of Diabetes and Digestive and Kidney Diseases; 1995:293-338.
NIH publication 95-1468.4. Roy MS.Diabeticretinopathyin African-Americanswith type1diabetes: TheNew
Jersey 725, II: risk factors. Arch Ophthalmol . 2000;118(1):105-115.
5. Roy MS, Roy A, Affouf M. Depression is a risk factor for poor glycemic control
and retinopathy in African-Americans withtype 1 diabetes. Psychosom Med . 2007;
69(6):537-542.
6. Leslie RD, Pyke D. Diabetic retinopathy in identical twins. Diabetes . 1982;31(1):
19-21.
7. Diabetes Control and Complications Trial Research Group. Clustering of long-
term complications in families with diabetes in the Diabetes Control and Com-
plications Trial. Diabetes . 1997;46(11):1829-1839.
8. Rema M, SaravananG, Deepa R, Mohan V. Familial clusteringof diabetic retinopa-
thy in South Indian type 2 diabetic patients. Diabet Med . 2002;19(11):910-916.
9. Hallman DM, Huber JC Jr, Gonzalez V, Klein B, Klein R, Hanis C. Familial aggre-
gation of severityof diabetic retinopathyin MexicanAmericansfrom Starr County,
Texas. Diabetes Care . 2005;28(5):1163-1168.
10. Monti MC, Lonsdale J, Montomoli C, Montross R, Schlag E, Greenberg D. Fa-
milial risk factors for microvascular complications and differential male-female
risk ina largecohortof American families with type 1 diabetes. J ClinEndocrinol
Metab . 2007;92(12):4650-4655.
11. Looker HC, Nelson R, Chew E, et al. Genome-wide linkage analyses to identify
loci for diabetic retinopathy. Diabetes . 2007;56(4):1160-1166.
12. Varma R. Diabetic retinopathy: challenges and future directions. AmJ Ophthalmol .
2006;141(3):539-541.
13. Archer DB. Diabetic retinopathy: some cellular, molecular and therapeutic
considerations. Eye . 1999;13(pt 4):497-523.
14. Uhlmann K, Kovacs P, Boettcher Y, Hammes H-P, Paschke R. Genetics of dia-
betic retinopathy. Exp Clin Endocrinol Diabetes . 2006;114(6):275-294.
15. Cai J, Boulton M. The pathogenesis of diabetic retinopathy: old concepts and
new questions. Eye . 2002;16(3):242-260.
16. Warpeha KM, Chakravarthy U. Molecular genetics of microvascular disease in
diabetic retinopathy. Eye . 2003;17(3):305-311.
17. Al-Kateb H, Mirea L, Xie X, et al. Multiple variants in vascular endothelial growth
factor (VEGFA) are risk factors for time to severe retinopathy in type 1 diabetes:The DCCT/EDIC Genetics study. N Engl J Med . 2005;353:2643-2653.
18. Hallman DM, Boerwinkle E, Gonzalez V, Klein B, Klein R, Hanis C. A genome-
widelinkagescan for diabeticretinopathy susceptibility genes in Mexican Ameri-
cans with type 2 diabetes from Starr County, Texas. Diabetes . 2007;56(4):
1167-1173.
19. Churchill AJ, Carter J, Ramsden C, et al. VEGF polymorphisms are associated
with severity of diabetic retinopathy. Invest Ophthalmol Vis Sci . 2008;49(8):
3611-3616.
20. Roy MS.Diabetic retinopathyin African-Americanswith type1 diabetes: TheNew
Jersey 725, I: methodology, population, frequency of retinopathy and visual
impairment. Arch Ophthalmol . 2000;118(1):97-104.
21. Roy MS, Affouf M. Six-year progression of retinopathy and associated risk fac-
tors in African American patients with type 1 diabetes mellitus: the New Jersey
725. Arch Ophthalmol . 2006;124(9):1297-1306.
22. TheDiabeticRetinopathyStudyResearchGroup.A modificationof theAirlie House
classificationof diabetic retinopathy: Diabetic Retinopathy Studyreport number7. Invest Ophthalmol Vis Sci . 1981;21:210-226.
23. Early Treatment of Diabetic Retinopathy Study Research Group. Grading dia-
betic retinopathy from stereoscopic color fundus photographs: an extension of
the modified Airlie Houseclassification. ETDRSreport number10. Ophthalmology .
1991;98(5)(suppl):786-806.
24. Early Treatment of Diabetic Retinopathy Study Research Group (ETDRS). Fun-
dus photographic riskfactors for progression of diabeticretinopathy. ETDRS re-
port number 12. Ophthalmology . 1991;98(5)(suppl):823-833.
25. Councilon ClinicalClassifications. International Classificationof Diseases,Ninth
Revision, Clinical Modification. Vol1. AnnArbor,MI: EdwardsBrothers Inc;1978.
26. Report of the Expert Committee on the diagnosis and classification of diabetes
mellitus. Diabetes Care . 1997;20(7):1183-1197.
27. Winter WE, MacLaren N, Riley W, Clarke D, Kappy M, Spillar R. Maturity-
onset diabetes of youth in black Americans. N Engl J Med . 1987;316(6):285-
291.
28. de Bakker PIW, Yelensky R, Pe’er I, Gabriel SB, Daly MJ, Altshuler D. Effi-
ciency and power in genetic association studies. Nat Genet . 2005;37(11):
1217-1223.
29. Hodgkinson CA,YuanQ, XuK, et al.Addictionsbiology: haplotype-basedanaly-
sis for 130 candidate genes on a single array. Alcohol Alcohol . 2008;43(5):
505-515.
30. Zaykin DV, Westfall PH, Young SS, Karnoub MA, Wagner MH, Ehm MG. Testing
association of statisticallyinferredhaplotypeswith discreteand continuous traits
in samples of unrelated individuals. Hum Hered . 2002;53(2):79-91.31. Mathias RA,Gao P,Goldstein JL,et al.A graphicalassessmentof p-values from
sliding window haplotype tests of association to identify asthma susceptibility
loci on chromosome 11q. BMC Genet . 2006;7:38.
32. Diehn JJ, Diehn M, Marmor M, Brown P. Differential gene expression in ana-
tomical compartments of the human eye. Genome Biol . 2005;6(9):R74.
33. Kumagai AK, Glasgow B, Pardridge W. GLUT1 glucose transporter expression
in the diabetic and nondiabetic human eye. Invest Ophthalmol Vis Sci . 1994;
35(6):2887-2894.
34. TakagiH, KingG, Aiello L. Hypoxiaupregulatesglucosetransport activitythrough
adenosine-mediated increase of GLUT1 expression in retinal capillary endothe-
lial cells. Diabetes . 1998;47(9):1480-1488.
35. Sone H, Deo B, Kumagai A. Enhancement of glucose transport by vascular en-
dothelial growthfactor in retinalendothelialcells. Invest OphthalmolVis Sci . 2000;
41(7):1876-1884.
36. Fernandes R, Suzuki K, Kumagai A. Inner blood-retinal barrier GLUT1 in long-
term diabetic rats: an immunogold electron microscopic study. Invest Ophthal-
mol Vis Sci . 2003;44(7):3150-3154.
37. Gardner TW, Antonetti D, Barber A, LaNoue KF, Levison SW. Diabetic reti-
nopathy: more than meets the eye. Surv Ophthalmol . 2002;47(suppl 2):S253-
S262.
38. The Diabetes Control and Complications Trial Research Group. The effect of in-
tensive diabetes treatment on the progression of diabetic retinopathy in insulin-
dependent diabetes mellitus. Arch Ophthalmol . 1995;113(1):36-51.
39. Tarnow L, Grarup N, Hansen T, Parving H-H, Pedersen O. Diabetic microvascu-
lar complications are not associatedwith twopolymorphismsin the GLUT-1 and
PC-1genes regulatingglucose metabolism in Caucasiantype 1 diabeticpatients.
Nephrol Dial Transplant . 2001;16(8):1653-1656.
40. Hodgkinson AD, Page T, Millward B, Demaine A. A novel polymorphism in the
5 flanking region of the glucose transporter (GLUT1) gene is strongly associ-
ated with diabetic nephropathy in patients with type 1 diabetes mellitus. J Dia-
betes Complications . 2005;19(2):65-69.
41. Nayak MS, Kita M, Marmor M. Protection of rabbit retina from ischemic injury
by superoxide dismutase and catalase. Invest Ophthalmol Vis Sci . 1993;34(6):2018-2022.
42. Chai D,Wang B,Shen L, PuJ, ZhangX, HeB. RXRagonists inhibit high-glucose
induced oxidative stress by repressing PKC activity in human endothelial cells.
Free Radic Biol Med . 2008;44(7):1334-1347.
43. Flekac M, Skrha J, Hilgertova J, Lacinova Z, Jarolimkova M. Gene polymor-
phisms of superoxide dismutases and catalase in diabetes mellitus. BMC Med
Genet . 2008;9:30.
44. Papapetropoulos A, Garcia-Cardena G, Dengler T, Maisonpierre PC, Yancopou-
los GD, Sessa WC. Direct actions of angiopoietin-1 on human endothelium: evi-
dence for network stabilization, cell survival, and interaction with other angio-
genic growth factors. Lab Invest . 1999;79(2):213-223.
45. Wang YL, Hui Y, Guo B, Ma J. Strengthening tight junctions of retinal microvas-
cular endothelial cells by pericytes under normoxia and hypoxia involving an-
giopoietin-1 signal way. Eye . 2007;21(12):1501-1510.
46. SturnDH, FeistritzerC, MosheimerB, et al.Angiopoietinaffectsneutrophil migration.
Microcirculation . 2005;12(5):393-403.47. Kim I, Ryan A, Rohan R, et al. Constitutive expression of VEGF, VEGFR-1,
and VEGFR-2 in normal eyes. Invest Ophthalmol Vis Sci . 1999;40(9):2115-
2121.
48. Caldwell RB, Bartoli M, Behzadian A, et al. Vascular endothelial growth factor
and diabetic retinopathy: role of oxidative stress. Curr Drug Targets . 2005;
6(4):511-524.
49. Usui T, IshidaS, YamashiroK, et al.VEGF164(165)as thepathological form: dif-
ferential leukocyte and endothelial responses through VEGFR1 and VEGFR2. In-
vest Ophthalmol Vis Sci . 2004;45(2):368-374.
50. JoussenAM, PoulakiV, LyLe M,et al. A central role forinflammationin thepatho-
genesis of diabetic retinopathy. FASEB J . 2004;18(12):1450-1452.
51. Wong TY, Cruickshanks K, Klein R, et al. HLA-DR3 and DR4 and their relation to
(REPRINTED) ARCH OPHTHALMOL/ VOL 127 (NO. 5), MAY 2009 WWW.ARCHOPHTHALMOL.COM611
©2009 American Medical Association. All rights reserved. on February 15, 2012www.archophthalmol.comDownloaded from

8/3/2019 Assessment of 193 Candidate Genes for thy
http://slidepdf.com/reader/full/assessment-of-193-candidate-genes-for-thy 8/8
the incidence and progression of diabetic retinopathy. Ophthalmology . 2002;
109(2):275-281.
52. Bollen M, GijsbersR, CeulemansH, Stalmans W, Stefan C. Nucleotide pyrophos-
phatases/phosphodiesterases on the move. Crit Rev Biochem Mol Biol . 2000;
35(6):393-432.
53. DeFronzo RA, Hendler R, Simonson D. Insulin resistance is a prominent feature
in insulin-dependent diabetes. Diabetes . 1982;31(9):795-801.
54. SchwartzMA. Integrinsignalingrevisited. Trends Cell Biol . 2001;11(12):466-470.
55. Roth T, Podesta F, Stepp MA, Boeri D, Lorenzi M. Integrin overexpression in-
duced by high glucose and by human diabetes: potential pathway to cell dys-
function in diabetic microangiopathy. Proc Natl Acad Sci U S A . 1993;90(20):
9640-9644.56. FriedlanderM, TheesfeldC, SugitaM, et al.Involvement of integrinsalpha v beta
3 and alpha v beta 5 in ocular neovascular diseases. Proc Natl Acad Sci U S A.
1996;93(18):9764-9769.
57. MissaleC, NashR, RobinsonSW, JaberM, CaronMG. Dopaminereceptors:from
structure to function. Physiol Rev . 1998;78(1):189-225.
58. HuemerK-H,GarhöferG, Zawinka C, et al.Effects of dopamine onhumanretinal
vessel diameter and itsmodulation during flicker stimulation. AmJ Physiol Heart
Circ Physiol . 2003;284(1):H358-H363.
59. Sato M,SomaM, NakayamaT, Kanmatsuse K.DopamineD1 receptorgenepoly-
morphism is associated with essential hypertension. Hypertension . 2000;36
(2):183-186.
60. Beige J, Bellmann A, Sharma A, Gessner R. Ethnic origin determines the impact
of genetic variants in dopamine receptor gene (DRD1) concerning essential
hypertension. Am J Hypertens . 2004;17(12, pt 1):1184-1187.
61. Yakel J. The 5-HT3 receptor channel: function, activation and regulation. Endo
M, Kurachi Y, Mishina M, eds. Pharmacology of Ionic Channel Function–
Activatorsand Inhibitors: Handbookof Experimental Pharmacology. Berlin, Ger-
many: Springer-Verlag. 2000;147:541-560.
62. RaabS, PlateK. Differentnetworks,commongrowth factors: shared growth fac-
tors and receptors of the vascular and the nervous system. Acta Neuropathol .
2007;113(6):607-626.63. Nishimura DY, Fath M, Mullins R, et al. Bbs-2 null mice have neurosensory defi-
cits, a defect in social dominance, and retinopathy associated with mislocaliza-
tion of rhodopsin. Proc Natl Acad Sci U S A. 2004;101(47):16588-16593.
64. Yue Y, Grossmann B, Galetzka D, Zechner U, Haaf T. Isolation and differential
expression of two isoforms of the ROBO2/Robo2 axon guidance receptor gene
in humans and mice [published online ahead of print July 10, 2006]. Genomics .
2006;88(6):772-778.
65. Carmeliet P, Tessier-Lavigne M. Common mechanisms of nerve and blood ves-
sel wiring. Nature . 2005;436(7048):193-200.
From the Archives of the Archives
D r H. D. Noyes, of New York, began the discus-sionof the chief topic ofthe day, Antisepsisin Ocu-
lar Surgery, in which he detailed all of the minutiæ of modern antiseptic surgery on the eye: of the prelimi-nary care of the patient; soap and water to the face andsurrounding region; boric acid for the same district af-ter the preliminary washing; hot water, carbolized, forthe instruments; a pad to cover the eye to be wet in a 1to 2000 bichloride solution; the instruments to be putinto actually boiling water; then to be placed for a whilein pure alcohol just beforethe operation; next great carefor cleanliness by the operator himself; and sterilizeddressings for the eye after the operation was done.
Thediscussion of thetopic wasthen taken up by manymembers, andof what each one said, a brief resumenow
follows.Dr Randolph, of Baltimore, thought that the use of
too hot applications for the instruments to be used inoperations on the eye was likely to dull the edge of theknives especially, and for that reason he did not put theinstruments into too hot aqueous solutions but into al-cohol. He also paid extreme attention to the conditionof the lachrymal secretions, and irrigated the sac veryfreely with boric acid in distilled water.
Dr E. Jackson, of Philadelphia, thought that ant pre-liminary bandage was bad practice, as it puts the eye intoa worse condition to bear the operation. As the nose is of-ten the starting place for lachrymal difficulties, the nos-trils ought to be carefully examined, and treated wher-ever there is suspicion of lachrymal disease in eyes to be
operated on with a corneal incision. Antisepsis in any op-eration on the lens means also a thorough removal of alllens substance and irrigation of the anterior chamber.
Reference: SpaldingJA. Report of theproceedings of theOphthalmologicalSectionof the Sixty-Fifth Annual Meet-ing of the British Medical Association, at Montreal, Sep-tember 1 to 4, 1897. Arch Ophthalmol. 1897;26:587-589.
(REPRINTED) ARCH OPHTHALMOL/ VOL 127 (NO. 5), MAY 2009 WWW.ARCHOPHTHALMOL.COM612
©2009 American Medical Association All rights reserved on February 15, 2012www.archophthalmol.comDownloaded from