Embed Size (px)
Citation preview

Assessing the Pediatric Trauma Assessing the Pediatric Trauma
Patient Patient –– What imaging is What imaging is
enoughenough
Adela T. CasasAdela T. Casas--Melley, MD, FACS, FAAPMelley, MD, FACS, FAAP
Chief, Pediatric SurgeryChief, Pediatric Surgery
Sanford ChildrenSanford Children’’s Hospitals Hospital
Assistant Medical Director Trauma ServiceAssistant Medical Director Trauma Service
SVP, Surgical and Cardiovascular servicesSVP, Surgical and Cardiovascular services

ObjectivesObjectives
�� Describe the appropriate imaging of the Describe the appropriate imaging of the pediatric trauma patientpediatric trauma patient
�� Evaluate the risks of certain imaging Evaluate the risks of certain imaging modalities and establish criteria for imaging modalities and establish criteria for imaging decision makingdecision making
�� Discuss the likelihood of pediatric spine Discuss the likelihood of pediatric spine injuries and the need for imaginginjuries and the need for imaging
�� List different modalities for abdominal List different modalities for abdominal evaluation of the pediatric trauma patientevaluation of the pediatric trauma patient

Case #1Case #1
�� 11 YO female who was trying to go from one 11 YO female who was trying to go from one
fort to another via a zip line and her hand fort to another via a zip line and her hand
slipped and she fell 18 feet to the ground.slipped and she fell 18 feet to the ground.
�� She landed on her feet and crumpled to the She landed on her feet and crumpled to the
ground.ground.
�� She denies hitting her head, denies loss of She denies hitting her head, denies loss of
consciousness. Remembers the entire accidentconsciousness. Remembers the entire accident
�� Her only complaint is left ankle pain.Her only complaint is left ankle pain.

Case #1Case #1
�� She was evaluated at outside institution and hadShe was evaluated at outside institution and had
�� CT of head CT of head –– negativenegative
�� CT of CCT of C--spine spine –– negativenegative
�� CT of TCT of T--spine spine –– negativenegative
�� CT of LCT of L--spine spine –– negativenegative
�� CT of abdomen CT of abdomen –– negativenegative
�� No plain films obtainedNo plain films obtained
�� What are the consequences of all of these studies?What are the consequences of all of these studies?

Radiologyinfo.org
Radiation Exposure in XRadiation Exposure in X--raysrays
Study OrderedStudy Ordered Equivalent doseEquivalent dose
CT headCT head 20 CXR20 CXR
CT CCT C--SpineSpine 60 CXR60 CXR
CT ChestCT Chest 70 CXR70 CXR
CT Abdomen/PelvisCT Abdomen/Pelvis 100 CXR100 CXR
CC--Spine SeriesSpine Series 15 CXR15 CXR

Radiologyinfo.org
Background RadiationBackground Radiation
StudyStudy Background radiationBackground radiation
CXRCXR 10 days10 days
CT HeadCT Head 8 months8 months
CT CCT C--SpineSpine 2 years2 years
CT ChestCT Chest 2 years2 years
CT Abdomen/PelvisCT Abdomen/Pelvis 3 years3 years
CC--Spine seriesSpine series 6 months6 months

Exposure to this ChildExposure to this Child
�� Equivalent of 300 CXREquivalent of 300 CXR’’s in one days in one day
�� Equivalent to 8 years and 8 months of Equivalent to 8 years and 8 months of
background radiation exposurebackground radiation exposure
�� In a child with no complaints of injury.In a child with no complaints of injury.

Case #2Case #2
�� 2 YO Male who fell through a register 2 YO Male who fell through a register
approximately 9 to 10 feet on to a hard wood approximately 9 to 10 feet on to a hard wood
floor.floor.
�� Cried immediately, complained of headacheCried immediately, complained of headache
�� Became a little somnolent and ended up Became a little somnolent and ended up
intubatedintubated
�� Prior to transfer CT scans obtainedPrior to transfer CT scans obtained

Case #2Case #2
�� Following studies obtainedFollowing studies obtained
�� CT of head CT of head –– left occipital skull fractureleft occipital skull fracture
�� CT of CCT of C--spine spine –– negativenegative
�� CT chest CT chest –– negativenegative
�� CT abdomen and pelvis CT abdomen and pelvis –– negativenegative
�� No plain films obtainedNo plain films obtained
�� CT chest, abdomen and pelvis obtained CT chest, abdomen and pelvis obtained
without contrastwithout contrast

Radiation exposureRadiation exposure
�� Equivalent to 250 CXREquivalent to 250 CXR’’s in a 2 YO child that s in a 2 YO child that
is highly sensitiveis highly sensitive
�� CT of chest abdomen and pelvis obtained CT of chest abdomen and pelvis obtained
without contrast so they are truly useless.without contrast so they are truly useless.
�� Do not have anyone available that can respond Do not have anyone available that can respond
to data so why delay transfer to get itto data so why delay transfer to get it
�� Let the referring physician decide what studies Let the referring physician decide what studies
they needthey need

AJR:176,February 2001
CT CT –– An Increasing Source of An Increasing Source of
Radiation ExposureRadiation Exposure
�� Since 1970Since 1970’’s CT use had increased to about 62 s CT use had increased to about 62
million CTmillion CT’’s a years a year
�� 4 million CT4 million CT’’s in childrens in children
�� Major growth has been driven by decrease Major growth has been driven by decrease
time for CTtime for CT
�� CT contributes disproportionally to radiation CT contributes disproportionally to radiation
dose to populationdose to population
�� 4% of test = 40% of radiation4% of test = 40% of radiation

Radiation ExposureRadiation Exposure
�� Pediatrics represents small fraction of testsPediatrics represents small fraction of tests
�� But fraction is increasingBut fraction is increasing
�� Combination of higher radiation dose and Combination of higher radiation dose and
larger lifetime risk results in a significantly larger lifetime risk results in a significantly
higher lifetime cancer mortality risk.higher lifetime cancer mortality risk.
�� Lifetime risk attributable to single dose is Lifetime risk attributable to single dose is
larger in childrenlarger in children

NEJM:357:2277-2284,November 2007
Lifetime RadiationLifetime Radiation--Induced Risk of Induced Risk of
CancerCancer

AJR:176,February 2001
Radiation RisksRadiation Risks
�� Calculated risk based on atomic bomb Calculated risk based on atomic bomb
radiation patientsradiation patients
�� Extrapolated data to determine organ exposure Extrapolated data to determine organ exposure
based on age at exposurebased on age at exposure
�� On basis of number of scans done and age On basis of number of scans done and age
distribution, the lifetime mortality risks are distribution, the lifetime mortality risks are
calculatedcalculated

AJR:176,February 2001
Radiation RisksRadiation Risks
�� Predicted total numbers of deaths attributable Predicted total numbers of deaths attributable
to 1 year of CT exams in the US areto 1 year of CT exams in the US are
�� 700 for head CT700 for head CT
�� 1800 for CT abdomen and pelvis1800 for CT abdomen and pelvis
�� Children account forChildren account for
�� 170 for head CT170 for head CT
�� 310 for CT abdomen and pelvis310 for CT abdomen and pelvis

AJR:176, February 2001
Radiation RisksRadiation Risks
�� Childhood CT examinations contribute Childhood CT examinations contribute
significantly to overall estimatesignificantly to overall estimate
�� Pediatric CT exams make up only 4% of total Pediatric CT exams make up only 4% of total
test but contribute 20% of total deathstest but contribute 20% of total deaths
�� Lifetime cancer risk of a 1 year old from Lifetime cancer risk of a 1 year old from oneone
CT of abdomen and pelvis is 1 in 550CT of abdomen and pelvis is 1 in 550
�� 1 in 1500 for head CT1 in 1500 for head CT

AJR:176, February 2001
Radiation RiskRadiation Risk
�� If you take 600,000 as average number of CTIf you take 600,000 as average number of CT’’s s
done in children under 15done in children under 15
�� 500 children will ultimately die from the CT 500 children will ultimately die from the CT
scan they receivedscan they received
�� Weigh the risk benefit rationWeigh the risk benefit ration
�� Use alternatives when possibleUse alternatives when possible

NEJM:357:2277-2284, November 2007
Part of the problemPart of the problem
�� Physicians view CT studies in same light as Physicians view CT studies in same light as
other Xother X--raysrays
�� Recent survey of radiologist and ER Recent survey of radiologist and ER
physicians 75% underestimated radiation dose physicians 75% underestimated radiation dose
from CTfrom CT
�� 53% of radiologist and 91% of ER physicians 53% of radiologist and 91% of ER physicians
did not believe CT increased lifetime risk of did not believe CT increased lifetime risk of
cancercancer

3 Ways to reduce exposure3 Ways to reduce exposure
�� Reduce the CT dose Reduce the CT dose –– We are lucky to have We are lucky to have
the first CT scanner with software to reduce the first CT scanner with software to reduce
radiation exposure by 45%radiation exposure by 45%
�� Replace CT when possible Replace CT when possible –– Ultrasound is a Ultrasound is a
very good viable alternative for trauma very good viable alternative for trauma
evaluation in childrenevaluation in children
�� Simply decrease the number of CTSimply decrease the number of CT’’s ordereds ordered

Do you really need that CT?Do you really need that CT?
�� Despite the fact that most CT scans are Despite the fact that most CT scans are associated with favorable ratios of benefit to associated with favorable ratios of benefit to risk there is strong evidence that too many are risk there is strong evidence that too many are being donebeing done
�� CT evaluation for blunt traumaCT evaluation for blunt trauma
�� Practice of defensive medicinePractice of defensive medicine
�� Repeat CTRepeat CT’’s (head injuries, solid organ s (head injuries, solid organ injuries)injuries)
�� Repeat because of lack of communicationRepeat because of lack of communication

AJR:169, October 1997
Impact of CT on patient management Impact of CT on patient management
in blunt traumain blunt trauma
�� Recent study evaluated 1500 consecutive Recent study evaluated 1500 consecutive
children with blunt abdominal traumachildren with blunt abdominal trauma
�� CT findings and decision for operative or non CT findings and decision for operative or non
operative management were recordedoperative management were recorded
�� 388 (26%) of CT scans had abnormal findings388 (26%) of CT scans had abnormal findings
�� 286 solid organ286 solid organ
�� 103 other103 other
�� 30 hollow viscous injury30 hollow viscous injury

AJR:169, October 1997
Impact of CT on patient management Impact of CT on patient management
in blunt traumain blunt trauma
�� 20 of the 286 (7%) of solid organ injury and 25 of 30 20 of the 286 (7%) of solid organ injury and 25 of 30 (83%) of hollow viscous injury children underwent (83%) of hollow viscous injury children underwent surgerysurgery
�� Injury was confirmed in all children with solid organ Injury was confirmed in all children with solid organ injury and 24 of 25 children with hollow viscous injury and 24 of 25 children with hollow viscous injuryinjury
�� Decision for surgery was based on CT findings in Decision for surgery was based on CT findings in 25% of solid organ injury and 68% of hollow viscous 25% of solid organ injury and 68% of hollow viscous injuryinjury
�� But, 74% of children had negative CTBut, 74% of children had negative CT’’ss

AlternativesAlternatives
�� Focused assessment of sonography for trauma Focused assessment of sonography for trauma
(FAST) (FAST) –– Evaluates free fluid around the heart Evaluates free fluid around the heart
and three areas of the abdominaland three areas of the abdominal--pelvic cavitypelvic cavity
�� RUQ RUQ –– Between liver and kidney (MorrisonBetween liver and kidney (Morrison’’s s
pouch)pouch)
�� LUQ LUQ –– Between spleen and kidneyBetween spleen and kidney
�� Subxiphoid area Subxiphoid area –– pericardial sacpericardial sac
�� Suprapubic areas Suprapubic areas –– behind bladder in males, uterus behind bladder in males, uterus
in femalesin females

AlternativesAlternatives
�� Extended version of FAST (EExtended version of FAST (E--FAST) involves FAST) involves
evaluating anterior chest for pneumothoraxevaluating anterior chest for pneumothorax
�� Can determine if there is free fluid in abdomen Can determine if there is free fluid in abdomen
or pericardium in unstable patient to direct or pericardium in unstable patient to direct
intervention.intervention.
�� Does have limitations. Does not evaluate Does have limitations. Does not evaluate
retroperitoneum or hollow viscousretroperitoneum or hollow viscous
�� Convenient, portableConvenient, portable

AlternativesAlternatives
�� Use well documented in adults. Less clear in Use well documented in adults. Less clear in
pediatricspediatrics
�� Very specific to detect hemoperitoneum but Very specific to detect hemoperitoneum but
less sensitive to define less sensitive to define ““positivepositive”” studystudy
�� However, negative ultrasound and negative However, negative ultrasound and negative
exam virtually excludes injury.exam virtually excludes injury.
�� Can use FAST to guide need for CTCan use FAST to guide need for CT

Evaluation of the pediatric spineEvaluation of the pediatric spine
�� NEXUS criteria have been out for many years but NEXUS criteria have been out for many years but
have not been consistently used in pediatric patientshave not been consistently used in pediatric patients
�� Consist of deciding if patients need XConsist of deciding if patients need X--rays if they rays if they
show the followingshow the following
�� Midline cervical tendernessMidline cervical tenderness
�� Focal neurologic deficitsFocal neurologic deficits
�� Altered mental statusAltered mental status
�� Evidence of intoxicationEvidence of intoxication
�� Painful distracting injuryPainful distracting injury

Evaluation of the pediatric spineEvaluation of the pediatric spine
�� NEXUS has been validated multiple times and NEXUS has been validated multiple times and
compared to several other methods with good compared to several other methods with good
resultsresults
�� Sensitivity 99%Sensitivity 99%
�� Specificity 99%Specificity 99%
�� Is the NEXUS criteria valid in children?Is the NEXUS criteria valid in children?

Pediatrics:108:2, August 2001
Evaluation of the pediatric spineEvaluation of the pediatric spine
�� Prospective multicenter study done in pediatric Prospective multicenter study done in pediatric blunt trauma patients (<18 YO)blunt trauma patients (<18 YO)
�� Patient had NEXUS criteria applied during Patient had NEXUS criteria applied during evaluationevaluation
�� Decision to do films was at MDDecision to do films was at MD’’s discretion s discretion and not driven by NEXUS but NEXUS criteria and not driven by NEXUS but NEXUS criteria were documented were documented
�� Presence or absence of injury based on final Presence or absence of injury based on final interpretation of Xinterpretation of X--raysrays

Pediatrics:108:2, August 2001
Evaluation of the pediatric spineEvaluation of the pediatric spine
�� 3065 patients evaluated3065 patients evaluated
�� 30 patients (0.98%) had injury documented30 patients (0.98%) had injury documented
�� Study includedStudy included
�� 88 children under 288 children under 2
�� 817 between 2 and 8817 between 2 and 8
�� 2160 between 8 and 172160 between 8 and 17

Pediatrics:108:2, August 2001
Evaluation of the pediatric spineEvaluation of the pediatric spine
�� 45.9% of injuries were of the lower cervical 45.9% of injuries were of the lower cervical
spinespine
�� No cases of SCIWORANo cases of SCIWORA
�� Only 4 of 30 injured children were younger Only 4 of 30 injured children were younger
than 9than 9
�� None under 2None under 2
�� Most common finding were tenderness and Most common finding were tenderness and
distracting injurydistracting injury

Pediatrics:108:2, August 2001
Evaluation of the pediatric spineEvaluation of the pediatric spine
�� NEXUS correctly identified all pediatric NEXUS correctly identified all pediatric
patients with injurypatients with injury
�� Sensitivity 100%Sensitivity 100%
�� Correctly designated 603 patients as low riskCorrectly designated 603 patients as low risk
�� Negative predictive value 100%Negative predictive value 100%

Pediatrics:108:2, August 2001
Evaluation of the pediatric spineEvaluation of the pediatric spine
�� ConclusionsConclusions
�� Lower cervical spine most common site of injuryLower cervical spine most common site of injury
�� Injury very rare in children under 8Injury very rare in children under 8
�� NEXUS performed well and itNEXUS performed well and it’’s use could reduce s use could reduce 20% of c20% of c--spine filmsspine films
�� No single case in literature of occult injury in child No single case in literature of occult injury in child classified as low risk by NEXUSclassified as low risk by NEXUS
�� All patients with injury report pain, have All patients with injury report pain, have neurologic findings, or have altered mental status neurologic findings, or have altered mental status and get studiesand get studies

Emergency Radiology:10:4, February 2004
CT versus plain filmsCT versus plain films
�� Study to determine value of CT of spine in Study to determine value of CT of spine in
children under 5children under 5
�� 606 patients having cervical spine evaluation 606 patients having cervical spine evaluation
in the ERin the ER
�� Documented age and sex as well as exam Documented age and sex as well as exam
findings and presence of injury on plain films findings and presence of injury on plain films
and CTand CT

Emergency Radiology:10:4, February 2004
CT versus plain filmsCT versus plain films
�� Of the 606 patients studiesOf the 606 patients studies
�� 459 (75.7%) were cleared by combination of 459 (75.7%) were cleared by combination of
exam, and plain filmsexam, and plain films
�� 147 (24.3%) went on to CT imaging for clearing of 147 (24.3%) went on to CT imaging for clearing of
the cervical spinethe cervical spine
�� Of the 147 who had CTOf the 147 who had CT
�� 143 (97.3%) were negative143 (97.3%) were negative
�� 4 (2.7%) were positive. All of these patients had 4 (2.7%) were positive. All of these patients had
positive findings on plain filmspositive findings on plain films

Emergency Radiology:10:4, February 2004
CT versus plain filmsCT versus plain films
�� The yield of CT of the spine in children under The yield of CT of the spine in children under
5 was very low and all patients had the same 5 was very low and all patients had the same
finding of plain films.finding of plain films.
�� CT of the spine is equal to 60 CXR and 4 CCT of the spine is equal to 60 CXR and 4 C--
spine seriesspine series
�� Is it worth the risk?Is it worth the risk?

Pediatr Radiol:38:635-644, 2008
CT versus plain filmsCT versus plain films
�� A study to evaluate the radiation exposure of A study to evaluate the radiation exposure of
children who had CT of the cchildren who had CT of the c--spine was done spine was done
in Atlanta.in Atlanta.
�� Retrospective review of all children who had Retrospective review of all children who had
CT of the spine in the ER after traumaCT of the spine in the ER after trauma
�� 992 children were evaluated992 children were evaluated
�� Only 181 (18%) had prior COnly 181 (18%) had prior C--spine seriesspine series

Pediatr Radiol:38:635-644, 2008
CT versus plain filmsCT versus plain films
�� Divided the study into three groupsDivided the study into three groups
�� 00--4 YO4 YO
�� 55--8 YO8 YO
�� >8 YO>8 YO
�� They used anthropomorphic dosimetry They used anthropomorphic dosimetry
phantoms for group 1 and 2phantoms for group 1 and 2

Pediatr Radiol:38:635-644, 2008
CT versus plain filmsCT versus plain films
�� Evaluated exposure for CEvaluated exposure for C--spine seriesspine series
�� Series 1 Series 1 –– laterallateral
�� Series 2 Series 2 –– Four viewsFour views
�� Series 3 Series 3 -- Seven viewsSeven views
�� Evaluated exposure for CTEvaluated exposure for CT
�� CT headCT head
�� CT CCT C--spinespine

Pediatr Radiol:38:635-644, 2008
CT versus plain filmsCT versus plain films
�� They calculated radiation exposure of the They calculated radiation exposure of the
phantoms and then retrospectively calculated phantoms and then retrospectively calculated
the radiation exposure of the children in the the radiation exposure of the children in the
studystudy
�� They then calculated a relative risk of thyroid They then calculated a relative risk of thyroid
cancer based on comparison of previous study cancer based on comparison of previous study
of children exposed to radiation in the 50of children exposed to radiation in the 50’’s for s for
treatment of tinea capitistreatment of tinea capitis

Pediatr Radiol:38:635-644, 2008
CT versus plain filmsCT versus plain films
�� Results showed Results showed
�� 992 patients992 patients
�� 435 had C435 had C--spine xspine x--rays onlyrays only
�� 181 had C181 had C--spine and CTspine and CT
�� 376 had CT only376 had CT only
�� Radiation dose for CT of the CRadiation dose for CT of the C--spinespine
�� Group 1 Group 1 –– 200X more than from C200X more than from C--spine seriesspine series
�� Group 2 Group 2 –– 90X more than from C90X more than from C--spine seriesspine series

Pediatr Radiol:38:635-644, 2008
CT versus plain filmsCT versus plain films
�� Relative risk for developing thyroid cancerRelative risk for developing thyroid cancer
�� Group 1 Group 1 –– none from conventional Cnone from conventional C--spine seriesspine series
�� Group 1 Group 1 –– relative risk from CT head was 0.03 but relative risk from CT head was 0.03 but
relative risk of 2 for CT of Crelative risk of 2 for CT of C--spinespine
�� Group 2 Group 2 –– no increase from Cno increase from C--spine seriesspine series
�� Group 2 Group 2 –– relative risk from CT head 0.02 but relative risk from CT head 0.02 but
increased to 0.07 for CT Cincreased to 0.07 for CT C--spinespine

What alternatives do we haveWhat alternatives do we have
�� Evaluate the patient and determine if there is Evaluate the patient and determine if there is need for radiologic studiesneed for radiologic studies
�� Do not get studies because of a knee jerk Do not get studies because of a knee jerk decision of what is done on all trauma patientsdecision of what is done on all trauma patients
�� Evaluation of children can be very difficult. If Evaluation of children can be very difficult. If you think the child has significant injuries and you think the child has significant injuries and you are unable to get a good exam or feel you are unable to get a good exam or feel uncomfortable, send them to someone with uncomfortable, send them to someone with experienceexperience

What alternatives do we haveWhat alternatives do we have
�� Get baseline studies firstGet baseline studies first
�� Do not scan head to toe, rarely ever neededDo not scan head to toe, rarely ever needed
�� Use alternative studies when you canUse alternative studies when you can
�� Never delay transfer to another institution to Never delay transfer to another institution to
get scans. The accepting docs will determine get scans. The accepting docs will determine
what they need. Stabilize and sendwhat they need. Stabilize and send
�� If you do get CT, please use contrast so we can If you do get CT, please use contrast so we can
actually use dataactually use data
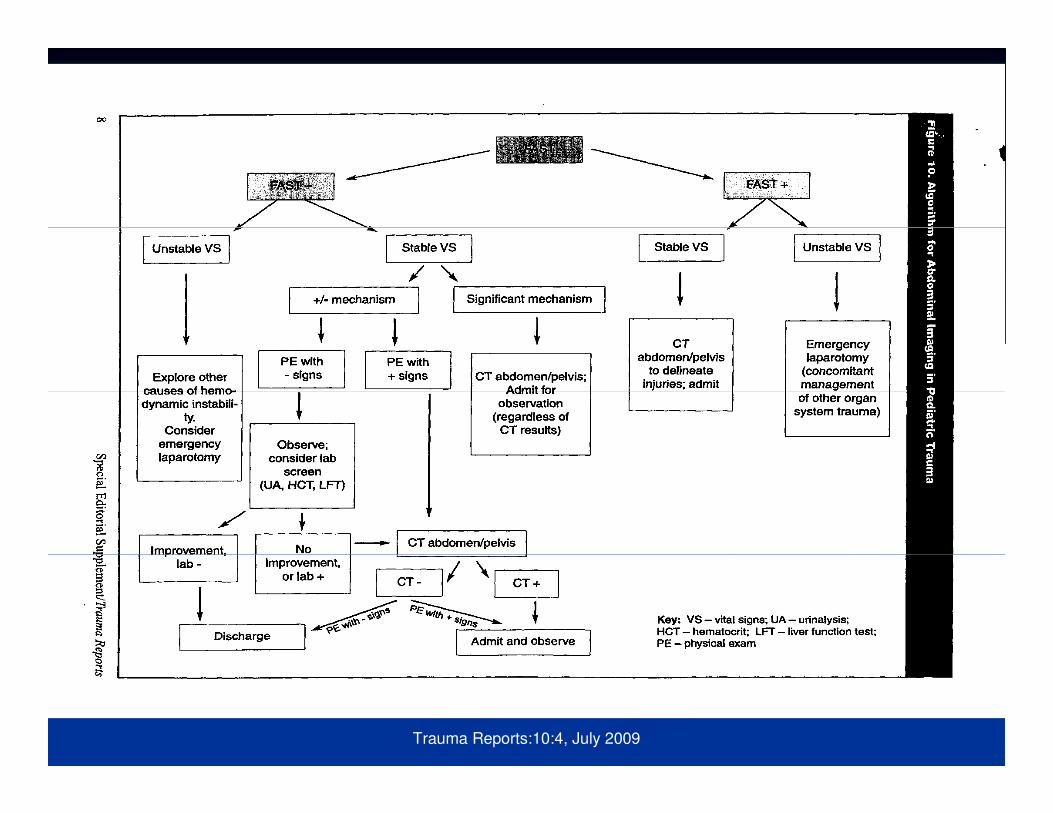
Trauma Reports:10:4, July 2009

What about CWhat about C--spinespine
�� Evaluate patient and determine NEXUS criteriaEvaluate patient and determine NEXUS criteria
�� Calm the child down and do a physical examCalm the child down and do a physical exam
�� Obtain plain films firstObtain plain films first
�� If you feel you need a CT by all means get it, but do If you feel you need a CT by all means get it, but do
not get it because it is a child and you feel not get it because it is a child and you feel
uncomfortable with the exam.uncomfortable with the exam.
�� You still need an exam before clearing the spine You still need an exam before clearing the spine
anyway. A negative CT does not clear the spineanyway. A negative CT does not clear the spine


Imaging of the pediatric trauma Imaging of the pediatric trauma
patientpatient
�� Hope this data has made you think about how Hope this data has made you think about how
many children we are exposing to risky doses many children we are exposing to risky doses
of radiationof radiation
�� This also applies to evaluation of the pediatric This also applies to evaluation of the pediatric
patient for abdominal painpatient for abdominal pain

QuestionsQuestions
??








![Trauma Reach Workshop - Pediatric Trauma.pptx [Read-Only]...Pediatric Trauma Trauma REACH Workshop May 5th, 2015 Tamer A. Ahmed, MD Pediatric Trauma Medical Director Upstate’s GolisanoChildren’s](https://img.dokumen.tips/doc/110x75/5fe9ec9ba1b3915c9800251e/trauma-reach-workshop-pediatric-read-only-pediatric-trauma-trauma-reach.jpg)




















