Embed Size (px)
Citation preview

Mary Ersek, PhD, RNMary Ersek, PhD, RNDirector of ResearchDirector of Research
Swedish Medical CenterSwedish Medical CenterSeattle, WASeattle, WA
[email protected]@swedish.org
Assessing & Managing Pain Assessing & Managing Pain in Older Adults: in Older Adults:
Challenges & OpportunitiesChallenges & Opportunities
2007 ASPMN National Conference
Addison, TX

ObjectivesObjectivesDescribe prevalence and characteristics of Describe prevalence and characteristics of pain in older personspain in older personsDescribe factors that influence pain Describe factors that influence pain perception in older adultsperception in older adultsDiscuss challenges in assessing painDiscuss challenges in assessing painDescribe EB practice guidelines for Describe EB practice guidelines for managing acute pain in older adultsmanaging acute pain in older adultsDescribe EB practice guidelines for Describe EB practice guidelines for managing chronic pain in older adultsmanaging chronic pain in older adults

What is What is ““Old?Old?””


IASP Global Year Against Pain IASP Global Year Against Pain in Older Personsin Older Persons
Proportion of population > 65 years old
0
5
10
15
20
25
30
1996 2006 2025 2050
%
World More developed countries Less developed countries
Source: U.S. Census Bureau, International Programs Center, International Data Base; D. Lussier, IASP, 2006
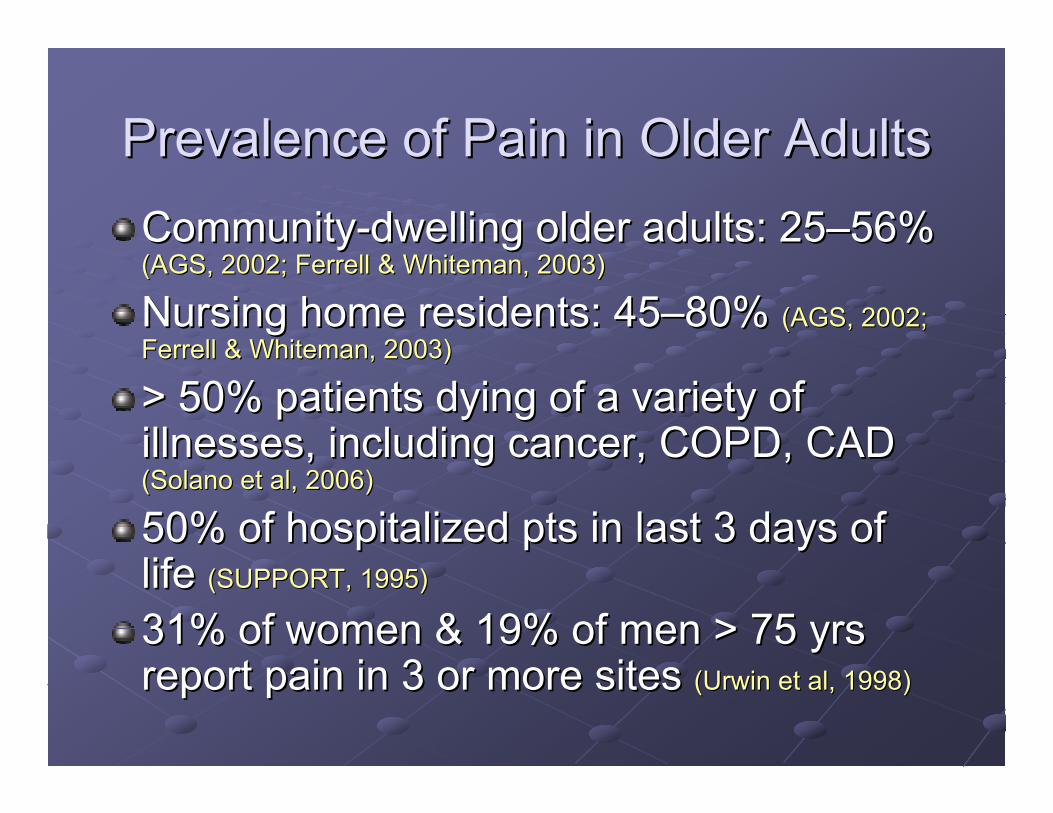
Prevalence of Pain in Older AdultsPrevalence of Pain in Older AdultsCommunityCommunity--dwelling older adults: 25dwelling older adults: 25––56% 56% (AGS, 2002; Ferrell & Whiteman, 2003)(AGS, 2002; Ferrell & Whiteman, 2003)
Nursing home residents: Nursing home residents: 4545––80% 80% (AGS, 2002; (AGS, 2002; Ferrell & Whiteman, 2003)Ferrell & Whiteman, 2003)
> 50% patients dying of a variety of > 50% patients dying of a variety of illnesses, including cancer, COPD, CAD illnesses, including cancer, COPD, CAD (Solano et al, 2006)(Solano et al, 2006)
50% of hospitalized pts in last 3 days of 50% of hospitalized pts in last 3 days of life life (SUPPORT, 1995)(SUPPORT, 1995)
31% of women & 19% of men > 75 yrs 31% of women & 19% of men > 75 yrs report pain in 3 or more sites report pain in 3 or more sites ((UrwinUrwin et al, 1998)et al, 1998)

Prevalence of Acute PainPrevalence of Acute PainUp to 75% of hospitalized adults Up to 75% of hospitalized adults
experience moderate to severe pain at experience moderate to severe pain at some point in their hospitalizationsome point in their hospitalization
19% of older persons admitted to the 19% of older persons admitted to the hospital have moderately or extremely hospital have moderately or extremely
severe painsevere pain
IASP, 2006

The Picture of Pain in Older AdultsThe Picture of Pain in Older AdultsCommon types: Common types: musculoskeletal, neuropathic, musculoskeletal, neuropathic, and cancerand cancer--relatedrelatedIn general, pain is persistent, In general, pain is persistent, multimulti--focal, and multifocal, and multi--factorialfactorialMany hospitalized older adults Many hospitalized older adults will have persistent will have persistent andand acute acute painpainPain in older adults often is not Pain in older adults often is not assessed & underassessed & under--treatedtreated

Pain Treatment in Pain Treatment in Hospitalized Older AdultsHospitalized Older Adults
Cognitively intact elders with hip fractureCognitively intact elders with hip fractureVery severe pain preVery severe pain pre--op: 44%op: 44%Very severe pain postVery severe pain post--op: 42%op: 42%No standing order for analgesic during entire No standing order for analgesic during entire hospital stay: 83%hospital stay: 83%PrePre--op mean op mean dailydaily dose of parenteral dose of parenteral morphine equivalents: 2.6 mg (SD=4.5 mg) morphine equivalents: 2.6 mg (SD=4.5 mg) PostPost--op mean op mean dailydaily dose of parenteral dose of parenteral morphine equivalents: 4.1 mg (SD=5.6 mg) morphine equivalents: 4.1 mg (SD=5.6 mg)
Morrison & Siu, J Pain Sympt Manage, 2000

Unrelieved Pain in NH ResidentsUnrelieved Pain in NH Residents
4545––85% NH residents have 85% NH residents have ““substantial pain substantial pain that is that is undertreatedundertreated”” (AGS, 2002)(AGS, 2002)
29% NH residents with cancer experienced daily 29% NH residents with cancer experienced daily pain; 26% of these residents received no pain; 26% of these residents received no analgesics analgesics ((BernabeiBernabei et al, 1998)et al, 1998)
25% of 25% of NHsNHs experienced daily experienced daily noncancernoncancer pain; pain; 26% of those received no analgesics 26% of those received no analgesics (Won et al, 1999)(Won et al, 1999)
31.8% of bereaved family members reported 31.8% of bereaved family members reported that NH patients did not receive any or enough that NH patients did not receive any or enough help with pain during the last days help with pain during the last days ((TenoTeno et al, 2004)et al, 2004)

Consequences of Persistent PainConsequences of Persistent Pain
Unnecessary sufferingUnnecessary sufferingDepression and anxietyDepression and anxietyImpaired ambulation, gait disturbanceImpaired ambulation, gait disturbanceSleep disturbancesSleep disturbancesImpaired cognitionImpaired cognitionImpaired appetite, weight lossImpaired appetite, weight lossDecreased socializationDecreased socializationIncreased healthcare utilizationIncreased healthcare utilizationIncreased agitation and resistance to careIncreased agitation and resistance to care
AGS Guideline for Persistent Pain, 2002; IASP, 2006; Scherder et al, 1999

Consequences of Unrelieved Acute Consequences of Unrelieved Acute Pain in Older AdultsPain in Older Adults
Impaired ambulation Impaired ambulation Slower functional recoverySlower functional recoveryFunctional disabilityFunctional disabilityHigher rate of postHigher rate of post--op complications (e.g. op complications (e.g. atelectstasis)atelectstasis)Chronic painChronic painIncreased mortalityIncreased mortality↑↑ risk for deliriumrisk for delirium
Morrison et al, 2003; Shea et al 2002; Manku and Leung, 2003; Pasero, Rakel & McCaffery, 2005)
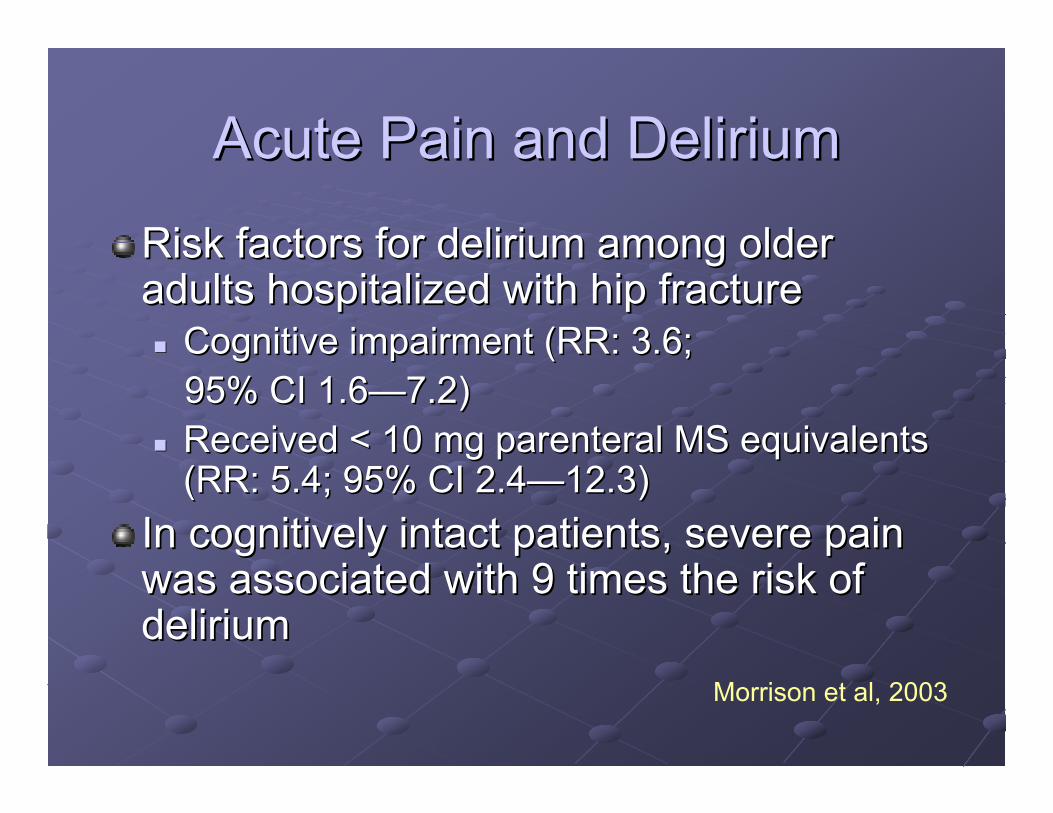
Acute Pain and DeliriumAcute Pain and Delirium
Risk factors for delirium among older Risk factors for delirium among older adults hospitalized with hip fracture adults hospitalized with hip fracture
Cognitive impairment (RR: 3.6; Cognitive impairment (RR: 3.6; 95% CI 1.695% CI 1.6——7.2)7.2)Received < 10 mg Received < 10 mg parenteralparenteral MS equivalents MS equivalents (RR: 5.4; 95% CI 2.4(RR: 5.4; 95% CI 2.4——12.3)12.3)
In cognitively intact patients, severe pain In cognitively intact patients, severe pain was associated with 9 times the risk of was associated with 9 times the risk of delirium delirium
Morrison et al, 2003

The Experience of Pain in Older The Experience of Pain in Older Adults Adults –– is it Different?is it Different?

Effects of Aging on Pain Effects of Aging on Pain Processing in HumansProcessing in Humans
Pain threshold decreases with agePain threshold decreases with ageEEG responses to acute noxious stimuli EEG responses to acute noxious stimuli ↓↓ in in speed & amplitudespeed & amplitude
Pain tolerance decreases with agePain tolerance decreases with ageDegenerative changes in 5HT and NE levels Degenerative changes in 5HT and NE levels may contribute to impaired descending may contribute to impaired descending inhibition and inhibition and ↓↓ pain tolerancepain toleranceDecreased efficacy of endogenous opioid Decreased efficacy of endogenous opioid analgesic systemsanalgesic systems
Gagliese & Farrell, 2005

Pain Coping Strategies Pain Coping Strategies in Older Adultsin Older Adults
In several studies, older adults with chronic pain In several studies, older adults with chronic pain report lower report lower catastrophizingcatastrophizing, although , although catastrophizingcatastrophizing appears to be significantly appears to be significantly associated with poorer outcomes in all age associated with poorer outcomes in all age groupsgroupsOlder adults may use fewer active, problemOlder adults may use fewer active, problem--solving coping strategies solving coping strategies Older adults tend to use more prayer and hopingOlder adults tend to use more prayer and hoping
Gibson, 2005

Challenges to Assessing and Challenges to Assessing and Treating Pain in Older AdultsTreating Pain in Older Adults
IllnessIllness--Related & Physiological BarriersRelated & Physiological BarriersPatient and Caregiver AttitudesPatient and Caregiver AttitudesAtypical presentationAtypical presentationLack of empirical support for assessment Lack of empirical support for assessment and treatments specific to older adultsand treatments specific to older adults

IllnessIllness--Related and Physiological Related and Physiological BarriersBarriers
Sensory deficitsSensory deficitsCognitive impairmentCognitive impairmentIncreased sensitivity to Increased sensitivity to medication effectsmedication effectsPolypharmacyPolypharmacyCoCo--morbiditymorbidityDepressionDepression

Attitudes that Hinder Pain Reporting, Attitudes that Hinder Pain Reporting, Assessment & Treatment in Older Assessment & Treatment in Older
Adults Adults Stoicism, not wanting to be a Stoicism, not wanting to be a ““complainercomplainer””Concerns about addiction, side Concerns about addiction, side effects, toleranceeffects, tolerancePain in old age is inevitable Pain in old age is inevitable Nothing can be done to relieve painNothing can be done to relieve painOlder adults cannot tolerate strong Older adults cannot tolerate strong analgesics analgesics Older adults are less sensitive to Older adults are less sensitive to painpain
Atypical PresentationsAtypical Presentations
““I donI don’’t have any pain, but I sure am t have any pain, but I sure am sore!sore!””““I feel fine I feel fine —— as long as Ias long as I’’m not m not moving!moving!””Pain is what the patient Pain is what the patient says it is says it is –– but what if but what if they canthey can’’t tell us?t tell us?

Nonverbal PatientsNonverbal Patients
ComaComaAdvanced dementiaAdvanced dementiaStatus post strokeStatus post strokeEnd of life End of life Developmentally Developmentally disableddisabledDeliriumDelirium

Cognitive Impairment & Pain Cognitive Impairment & Pain Management: Acute CareManagement: Acute Care
Advanced dementia patients hospitalized Advanced dementia patients hospitalized with hip fracture received 1/3 the amount with hip fracture received 1/3 the amount of opioid analgesia that cognitively intact of opioid analgesia that cognitively intact older patients received older patients received (Morrison & (Morrison & SiuSiu, 2000), 2000)
Cognitively impaired (MMSE < 23) hip Cognitively impaired (MMSE < 23) hip surgery pts received significantly less surgery pts received significantly less opioids than intact older patients despite opioids than intact older patients despite reporting similar pain intensity reporting similar pain intensity ((FeldtFeldt et al, 1998)et al, 1998)

What is Different about the Pain What is Different about the Pain Experience of People with Experience of People with
Advanced Dementia?Advanced Dementia?Tolerance to Tolerance to acuteacute pain pain possiblypossibly increases increases but pain threshold does not appear to change but pain threshold does not appear to change Dementia may blunt ANS response to acute Dementia may blunt ANS response to acute pain pain Cognitive impairment Cognitive impairment maymay decrease the decrease the perceived analgesic effectiveness perceived analgesic effectiveness Pain can negatively affect cognitive functionPain can negatively affect cognitive function

ASPMN Position StatementASPMN Position Statement
Follow ethical principles: beneficence, Follow ethical principles: beneficence, autonomy, autonomy, nonmaleficencenonmaleficence, justice, justiceEstablish a pain assessment procedureEstablish a pain assessment procedureUse Hierarchy of Pain Assessment Use Hierarchy of Pain Assessment TechniquesTechniques““Assume Pain is PresentAssume Pain is Present””Use empirical trialsUse empirical trialsReRe--assess and documentassess and document
Herr et al, Pain Management Nursing, 2006

An Interdisciplinary Expert An Interdisciplinary Expert Consensus Statement onConsensus Statement on
Assessment of Pain in Older Assessment of Pain in Older PersonsPersons
Thomas Hadjistavropoulos, PhD,Keela Herr, PhD, RN, FAAN, et al
Clinical Journal of Pain, 23: S1–S43, 2007

ASPMN Prioritized Pain ASPMN Prioritized Pain Assessment Assessment
1.1. PatientPatient’’s selfs self--report report 2.2. Painful medical conditions Painful medical conditions
or procedures or procedures 3.3. Behaviors (e.g., facial Behaviors (e.g., facial
expressions, crying)expressions, crying)4.4. Report of pain from a Report of pain from a
family member or family member or caregivercaregiver
5.5. Response to empirical Response to empirical therapytherapy
Can Patients with Cognitive Can Patients with Cognitive Impairment Reliably Report Pain?Impairment Reliably Report Pain?CI NH residents slightly underreport pain, but CI NH residents slightly underreport pain, but their reports are valid their reports are valid ((ParmeleeParmelee et al., 1993)et al., 1993)
83% of CI NH residents could reliably 83% of CI NH residents could reliably complete at least one pain scale complete at least one pain scale (Ferrell et al., (Ferrell et al., 1995)1995)
73% of post73% of post--op patients op patients with moderate CI were with moderate CI were able to complete a 4able to complete a 4--point point verbal descriptor scale verbal descriptor scale (Feldt et al., 1998)(Feldt et al., 1998)

Pain Behavior Assessment ToolsPain Behavior Assessment ToolsChecklist for Nonverbal Pain Indicators (CNPI)Checklist for Nonverbal Pain Indicators (CNPI)((FeldtFeldt, 2000), 2000)
NOPAINNOPAIN (Snow et al, 2004)(Snow et al, 2004)
PAINPAIN--ADAD (Warden et al, 2003)(Warden et al, 2003)
Pain Assessment Scale for Seniors with Severe Pain Assessment Scale for Seniors with Severe Dementia (PACSLAC)Dementia (PACSLAC) (Fuchs(Fuchs--LacelleLacelle & & HadjistavropoulosHadjistavropoulos, , 2004)2004)
Also see:Also see: Herr, Decker, & Herr, Decker, & BjoroBjoro (2004). State of the Art (2004). State of the Art Review of Tools for Assessment of Pain in Nonverbal Review of Tools for Assessment of Pain in Nonverbal Older Adults. Older Adults.
Available at: http://Available at: http://www.cityofhope.org/prc/elderly.aspwww.cityofhope.org/prc/elderly.asp

Caregiver ReportCaregiver Report

Assess forpossible pain
behaviors
Ensure basiccomfort needs
are met
Evaluate andtreat new acute
problems(e.g., UTI)
Administeranalgesic
Re-evaluatepain behaviors
Documentassessment and
Rx response Empirical Analgesic Therapy: When in
Doubt, Treat

Evidence for attempting empirical Evidence for attempting empirical analgesic trialanalgesic trial
650 mg TID APAP: 63% decrease in negative 650 mg TID APAP: 63% decrease in negative behaviors, 75% behaviors, 75% psychotropicspsychotropics discontinued discontinued ((DouzjianDouzjian et al, 1998)et al, 1998)
Standardized assessment and treatment Standardized assessment and treatment protocol significantly decreased discomfort protocol significantly decreased discomfort among demented NH residents among demented NH residents (Kovach et al, (Kovach et al, 1999)1999)
Regular analgesic therapy increased Regular analgesic therapy increased social engagement in NH residents social engagement in NH residents (Chibnall et (Chibnall et al, 2005)al, 2005)

Assessing and Managing Assessing and Managing Acute PainAcute Pain
Herr, et al:Herr, et al: EvidenceEvidence--based Practice based Practice Guideline Guideline –– Acute Pain Management Acute Pain Management
Older Adults, University of Iowa College of Older Adults, University of Iowa College of Nursing, 2006Nursing, 2006
Available at:Available at:http://http://www.nursing.uiowa.edu/centers/gnirc/protocols.htmwww.nursing.uiowa.edu/centers/gnirc/protocols.htm

EBP Guidelines for Persistent and EBP Guidelines for Persistent and EOL PainEOL Pain
American Geriatrics SocietyAmerican Geriatrics Society. Management of . Management of persistent pain in older persons, 2002.persistent pain in older persons, 2002.www.americangeriatrics.orgwww.americangeriatrics.orgAmerican Medical Directors Association. American Medical Directors Association. Pain Pain management in the long term care setting, 2003, management in the long term care setting, 2003, www.amda.comwww.amda.comMcLennonMcLennon SM.SM. Persistent pain management. Persistent pain management. Iowa City (IA): University of Iowa Iowa City (IA): University of Iowa GerontologicalGerontologicalNursing Interventions Research Center, 2005 Nursing Interventions Research Center, 2005

Pearls from the GuidelinesPearls from the Guidelines
Minimize reliance on physical signs of painMinimize reliance on physical signs of painInclude cognitive status in your initial pain Include cognitive status in your initial pain assessmentassessmentEstablish the terms the patient uses to Establish the terms the patient uses to describe their pain and documentdescribe their pain and documentEstablish the pain intensity tool that works Establish the pain intensity tool that works for the individual and use it consistentlyfor the individual and use it consistentlyTeach patient and caregiver; assess Teach patient and caregiver; assess barriers and teach appropriatelybarriers and teach appropriately
Pearls from the Guidelines:Pearls from the Guidelines:Using Using PatientPatient--controlled Analgesiacontrolled Analgesia
PCA can be used with older adults esp. during PCA can be used with older adults esp. during the immediate postthe immediate post--procedure period procedure period Screen for cognitive & physical ability to manage Screen for cognitive & physical ability to manage PCAPCAAvoid basal infusion in opioidAvoid basal infusion in opioid--nanaïïve older adults ve older adults unless the patient is awakened by pain during unless the patient is awakened by pain during sleep sleep If using basal, keep low, 0.5 mg/hour of MS or If using basal, keep low, 0.5 mg/hour of MS or equivalent) & monitor sedation & respiratory equivalent) & monitor sedation & respiratory statusstatus

Pearls: Opioids and DeliriumPearls: Opioids and DeliriumDelirium may be caused by factors other than Delirium may be caused by factors other than opioidsopioidsPostPost--op delirium associated with unrelieved pain op delirium associated with unrelieved pain rather than opioid userather than opioid useIf other causes of delirium are not found and If other causes of delirium are not found and pain is effectively managed, consider decreasing pain is effectively managed, consider decreasing the opioid dosethe opioid doseConsider shortConsider short--term use of haloperidol; caution term use of haloperidol; caution –– may mask pain behaviorsmay mask pain behaviors

Pearls from the GuidelinesPearls from the GuidelinesInitiate opioid therapy at a 25% to 50% lower Initiate opioid therapy at a 25% to 50% lower dose than recommended for younger adults dose than recommended for younger adults Always combine analgesic therapy with Always combine analgesic therapy with nondrugnondrugtherapytherapyUse Use NSAIDsNSAIDs with great caution and only for with great caution and only for shortshort--term therapy term therapy Maximize APAP dose (4 gm/day) Maximize APAP dose (4 gm/day) Use empirical analgesic trials for nonverbal Use empirical analgesic trials for nonverbal patientspatientsAvoid use of codeine and Avoid use of codeine and propoxyphenepropoxypheneElicit patient goals for therapy, include functional Elicit patient goals for therapy, include functional goalsgoals