Embed Size (px)
Citation preview

ASSESSING DEHYDRATION
IN CHILDREN
INTRODUCTION
Children are particularly susceptible to dehydration with acute gastroenteritis or other illnesses that cause vomiting, diarrhoea and fever. Considerable care is required in the assessment and management of dehydration in children, because underestimation of dehydration may lead to inadequate management and therefore complications, while overestimation of fluid deficit can result in inappropriate rehydration therapy.
It is therefore essential to make an accurate assessment of the degree of dehydration in children in order to make appropriate treatment decisions
DEFINITION OF
DEHYDRATION
Dehydration is a condition that can occur with excess loss of water and other body fluids. Dehydration results from decreased intake, increased output (renal, gastrointestinal or insensible losses), a shift of fluid (e.g. ascites, effusions), or capillary leak of fluid (e.g. burns and sepsis).
CAUSES OF
DEHYDRATION

Gastroenteritis
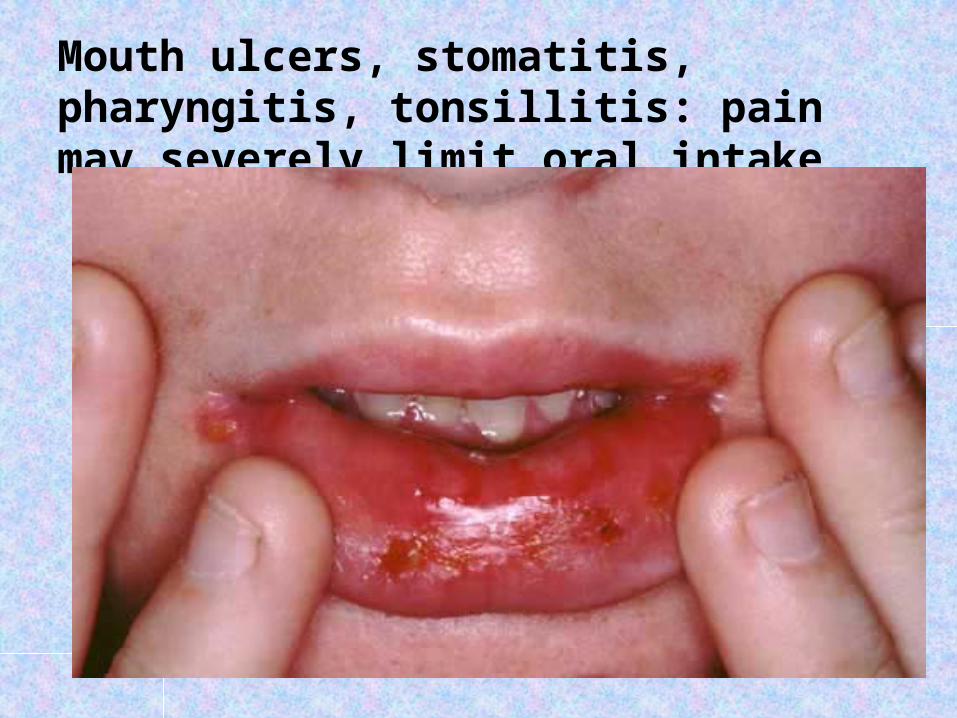
Mouth ulcers, stomatitis, pharyngitis, tonsillitis: pain may severely limit oral intake
Diabetic ketoacidosis (DKA)Febrile illness: fever causes increased insensible fluid losses.

Burns: fluid losses may be extreme and require aggressive fluid management
Congenital adrenal hyperplasia: may have associated hypoglycaemia, hypotension, hyperkalaemia, and hyponatraemia.
Gastrointestinal obstruction, e.g. pyloric stenosis: often associated with poor intake, vomiting.
Bowel ischaemia may cause extensive capillary leak and shock.

Cystic fibrosis: excessive sodium and chloride losses in sweat.
Diabetes insipidus: excessive output of very dilute urine.
Thyrotoxicosis: increased insensible losses and diarrhoea.
ASSESSMENT
Clinical assessment of dehydration can be difficult, especially in young infants, and rarely predicts the exact degree of dehydration accurately.
The most useful individual signs for predicting 5% dehydration in children are an abnormal capillary refill time, abnormal skin turgor and abnormal respiratory pattern.
Combinations of examination signs provide a much better method than any individual signs in assessing the degree of dehydration.


Of the clinical indicators used, the pinch test (skin turgor) has been shown to be the most reliable in several studies but is still not a reliable test when used without other clinical indicators.
One proposed assessment scale using general appearance, eyes, mucous membranes, and tears, has been shown to be effective in assessing dehydration in children
The assessment of dehydration in diabetic ketoacidosis (DKA) is particularly difficult in view of extravascular and intravascular dehydration, metabolic acidosis affecting the clinical signs of dehydration, and the overall catabolic state of the patient. The majority of patients with DKA have moderate (4% to 8%) dehydration, but clinical assessment overestimates the percent dehydration in two thirds of patients
The history and laboratory tests provide only modest benefit in assessing dehydration.
Clinical assessment therefore comprises some of the following indicators of dehydration
Loss of body weight:
oNormal: no loss of body weight.oMild dehydration: 5-6% loss of body weight.oModerate: 7-10% loss of body weight.oSevere: over 10% loss of body weight.

Clinical features of mild-to-moderate dehydration; 2 or more of:
Restlessness or irritability.
Sunken eyes (also ask the parent). Thirsty and drinks eagerly


Clinical features of severe dehydration; 2 or more of:
Abnormally sleepy or lethargic.
Sunken eyes.
Drinking poorly or not at all
PINCH TEST (SKIN TURGOR):

Skin turgor is assessed by pinching the skin of the abdomen or thigh longitudinally between the thumb and the bent forefinger.
The sign is unreliable in obese or severely malnourished children.
Normal: skin fold retracts immediately.Mild or moderate dehydration: slow; skin fold visible for less than 2 seconds.

Mild or moderate dehydration: slow; skin fold visible for less than 2 seconds.
Severe dehydration: very slow; skin fold visible for longer than 2 seconds.
Other features of dehydration include dry mucous membranes, reduced tears and decreased urine output.
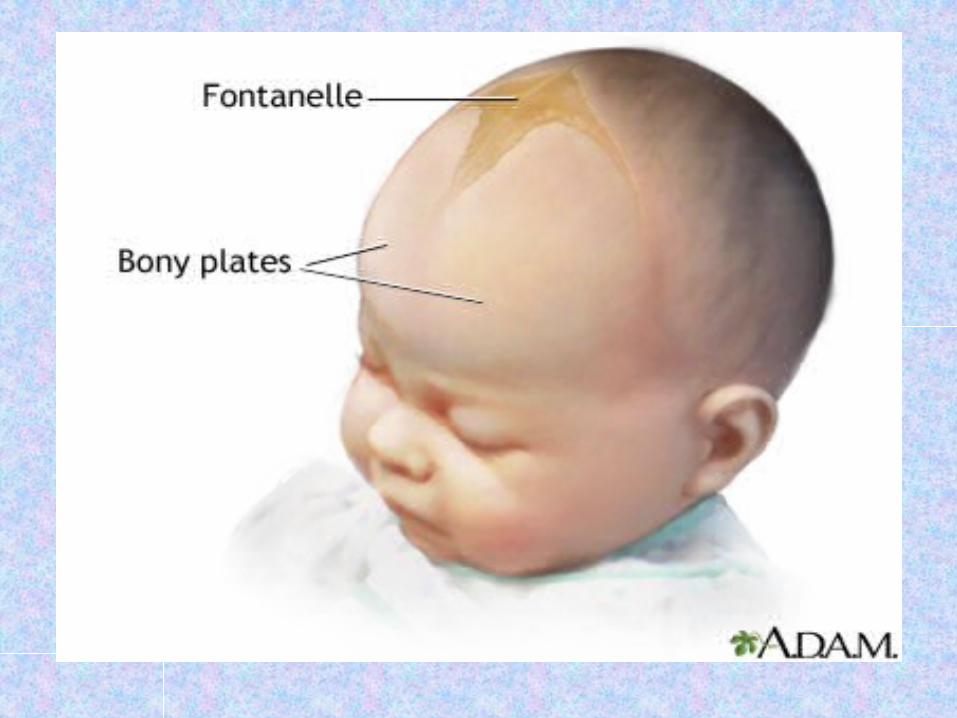
Additional signs of severe dehydration include circulatory collapse (e.g. weak rapid pulse, cool or blue extremities, hypotension), rapid breathing, sunken anterior fontanels
CLINICAL ASSESSMENT
OF DEHYDRATION
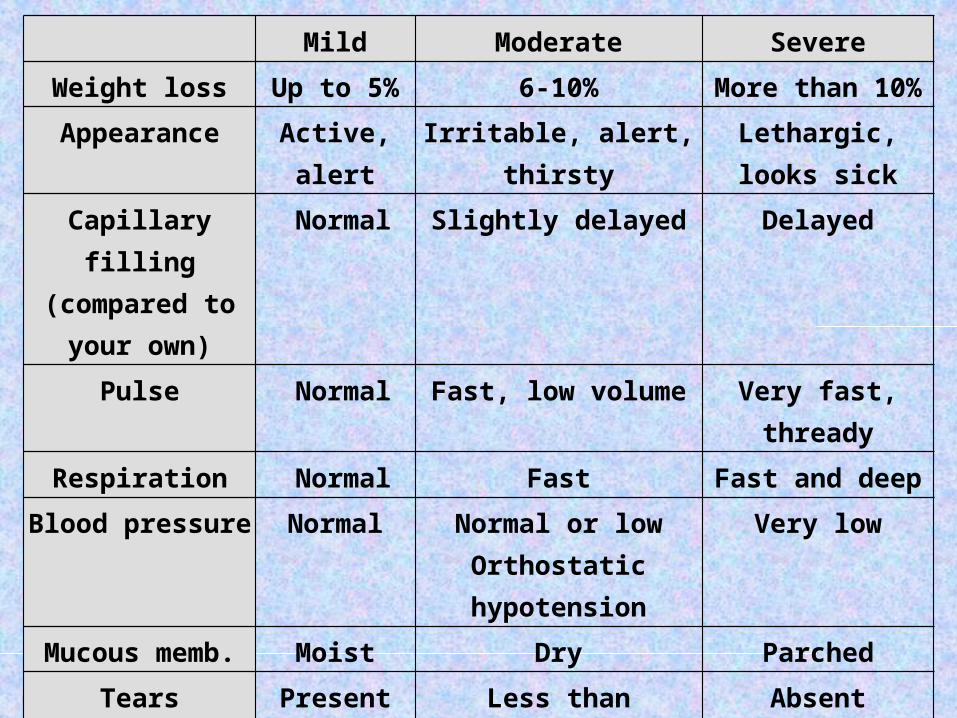
Mild Moderate Severe
Weight loss Up to 5% 6-10% More than 10%
Appearance Active, alert Irritable, alert, thirsty Lethargic, looks sick
Capillary filling (compared to your
own)
Normal Slightly delayed Delayed
Pulse Normal Fast, low volume Very fast, thready
Respiration Normal Fast Fast and deep
Blood pressure Normal Normal or low Orthostatic hypotension
Very low
Mucous memb. Moist Dry Parched
Tears Present Less than expected Absent
Eyes Normal Normal Sunken
Pinched skin Springs back Tents briefly Prolonged tenting
Fontanel (infant sitting)
Normal Sunken slightly Sunken significantly
Urine flow Normal Reduced Severely reduced

When we talk of 5% dehydration, it means that the child has lost an amount of fluid equal to 5% of the body weight. So,
A 10 kg child who is 5% dehydrated will weigh 9.5 kg.A 10 kg child who is 10% dehydrated will weigh 9 kg.A 5 kg child who is 10% dehydrated will weigh 4.5 kg.
The child's current (dehydrated) weight can be used for calculation of dehydration and maintenance fluids. After all, clinical assessment of dehydration, and therefore the volume needed for correction, is approximate!
ORAL REHYDRATION
SOLUTION (ORS)


Recipe 1
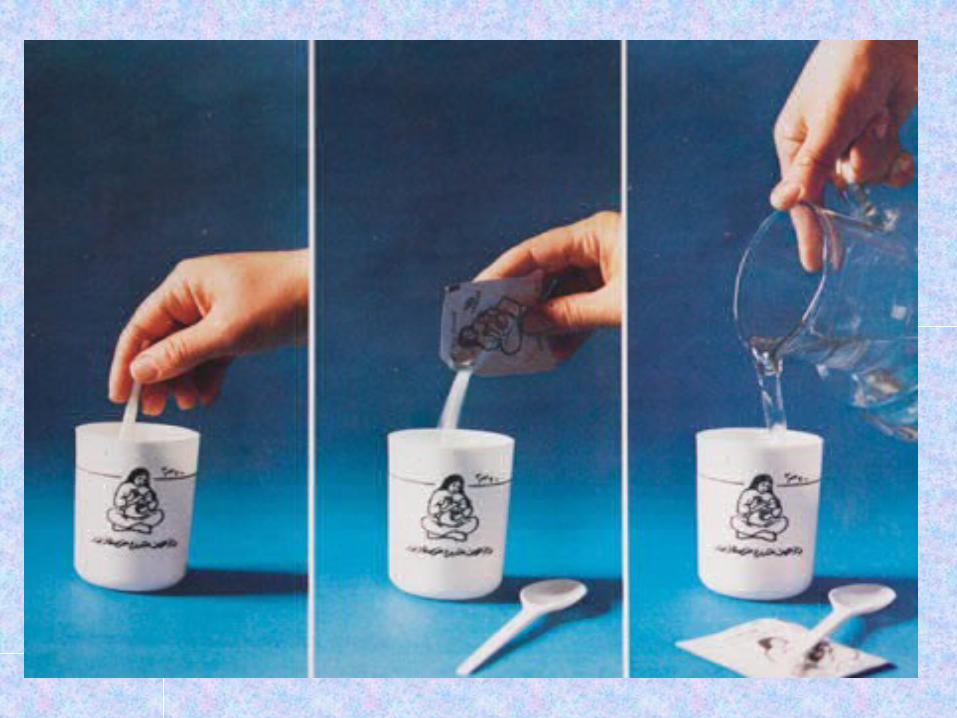
Making a 1 (one) litre solution using Salt, Sugar and Water
Ingredients:• One level teaspoon of salt• Eight level teaspoons of sugar• One litre of clean drinking or boiled water and then cooled5 cupfulls (each cup about 200 ml.)
Preparation Method:Stir the mixture till the salt and sugar dissolve

Recipe 2
Making a 1/2 (half) liter solution usingSalt, Sugar and Water
Ingredients:A 3 finger pinch of salt ( approx. 1.75 gms.)A scoop of sugar ( approx. 20 gms.)1/2 (half) liter of clean drinking or boiled
water2.5 cupfuls (each cup about 200 ml.)
PREPARATION METHOD:
Pour 1/2 (half) liter of clean drinking or boiled water, after it has cooled, into a large vessel.
Add a 3-finger pinch of salt (approx. 1.75gms).
Taste the solution. It shouldn't be more salty than yourtears.
Add a scoop of sugar ( approx. 20 gms.)
Stir the mixture till the salt and sugar dissolve.