Embed Size (px)
Citation preview

Assessing Culturally Competent Diabetes Care with Unannounced
Standardized PatientsKutob RM, Bormanis J, Crago M, Senf J, Gordon P. Shisslak C.
Randa M. Kutob, MD, MPH John Bormanis , PhDDepartment of Family and Community MedicineUniversity of Arizona, College of [email protected]@comcast.net

The Problem More effective diabetes care is desperately needed
and
The provider-patient relationship is a key point of intervention.

Scope of the ProblemDiabetes and Pre-diabetes
18.8 million with diabetes
7.0 million undiagnosed +79.0 million w/pre-diabetes
______________________= 104.8 million!!!!
Centers for Disease Control and Prevention. National Diabetes Fact Sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2011.
Diagnosed DiabetesUndiagnosed Di-abetesPrediabetesThose Unaffected

Diabetes Disparities• African Americans, American Indians, and
Hispanic/Latinos have higher rates of diabetes (CDC, 2011)
• African Americans have a 2–4 times higher rate of renal disease, blindness, and amputations.(Peek, 2007)
• U.S. Latinos have a higher rate renal disease and retinopathy. (Peek, 2007)
• African Americans, American Indians, and Hispanic/Latinos have higher diabetes-related death rates (AHRQ, 2003)
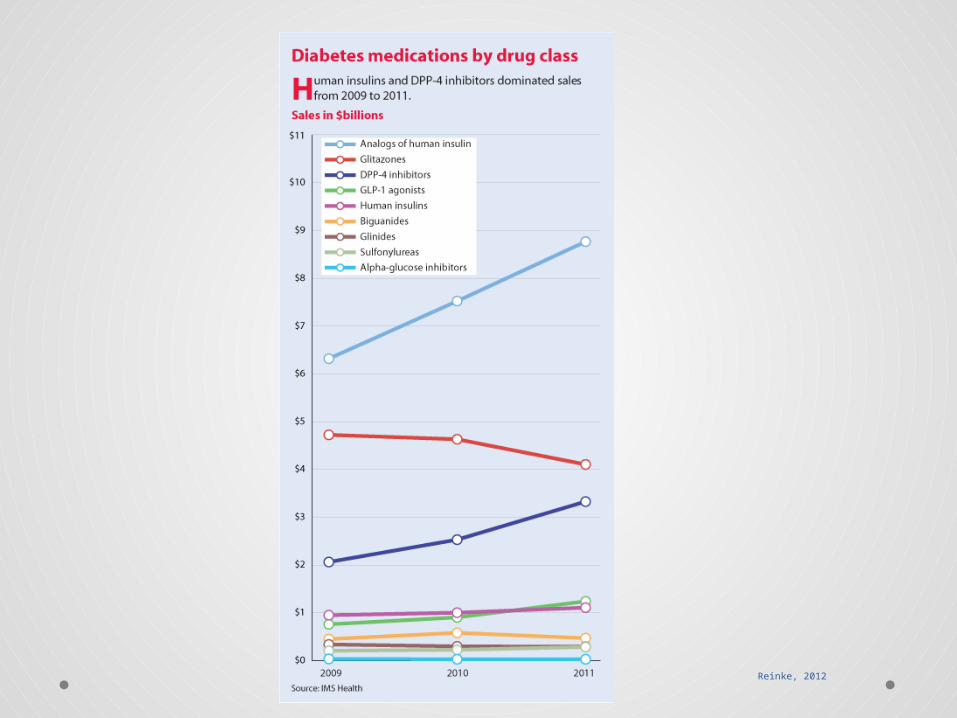
Reinke, 2012

The Medical Office Visit
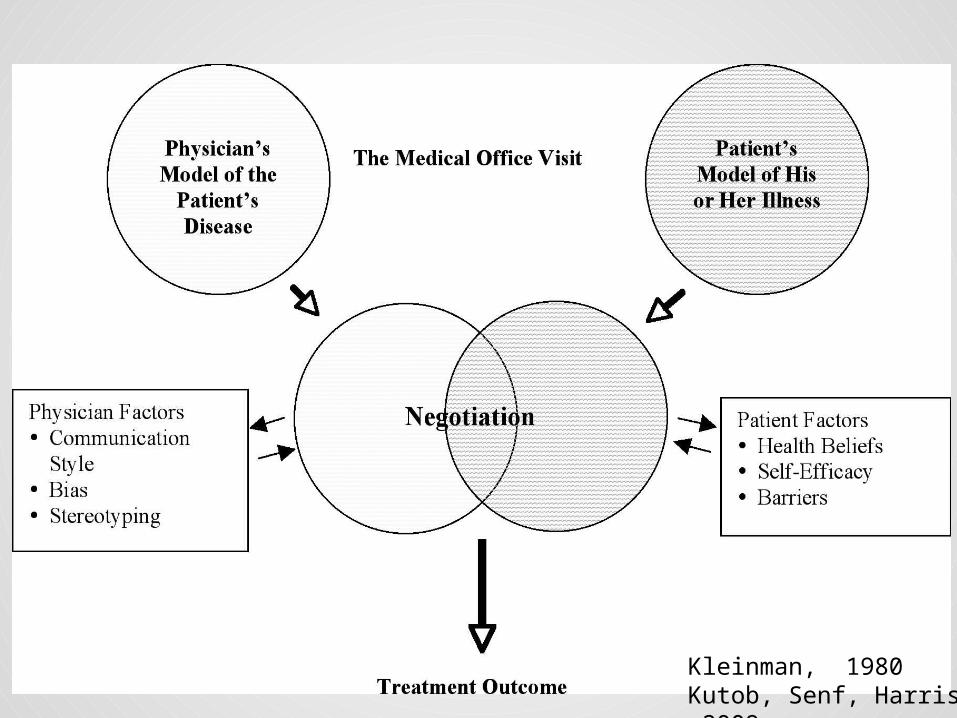
Kleinman, 1980Kutob, Senf, Harris, 2009

Medical Culture

What would a culturally competent physician do during the office visit, and which of these behaviors could be measured by an outside observer?
Unannounced Standardized Patient
(SPs) Study

Standardized Patients (SPs)
• Trained “fake” patients• Used extensively in medical education
oObjective Structured Clinical Examination• Typically students know that they are being
evaluated by a SP• In our study physicians did not know.

Study Design Overview
• Unannounced SPs were sent to the offices of family and internal medicine physicianso 4 University-based clinicso 1 Community-based clinic
• All physicians were consented. Study was approved by the University of Arizona Institutional Review Board.

The Standardized Patient Checklist
• Developed by experts in anthropology, endocrinology, cultural competence, family medicine, internal medicine, Objective Structured Clinical Examination (OSCE) development, pediatrics, ethnic minority health care, and research methodology
• For an adult SP with a chief complaint of diabetes• The checklist included items modeled on Kleinman’s
cross-cultural office visit

SP Checklist: 7 Subscales, 41 dichotomous
Items• Explanatory Model Elicitation• Cultural Knowledge• Non-judgmental behavior• Sharing the Biomedical Model• Patient Empowerment• Diabetes Specific Behaviors• Arizona Clinical Interview Rating Scale

Explanatory Model Elicitation
• Asked the patient’s view of illness• Asked the patient’s view of illness treatment• Asked about patient’s use of other medical/traditional
providers• Asked about family support• Asked about community support• Asked abut gender role in family and how this influences
care

Cultural Knowledge• Indicated knowledge when asked, “Is it true that Mexican
Americans have higher rates of diabetes?”• Addressed health beliefs regarding fatalism• Indicated knowledge when asked, “I have been eating
nopalitos. Have you heard of those.”• MD addressed health beliefs, before patient brought up • MD brought up higher rates of diabetes in Mexican
Americans before SP asked.• MD brought up nopalitos before MD asked

Non-judgmental Behavior
• Did not threaten insulin if did not take medications• Did not condemn use of alternative treatments• Did not condemn use of alternative healers• Was non-judgmental in response to elevated hemoglobin
A1c• Did not threaten complications if did not take
medications

Sharing the Biomedical Model
Shared knowledge about…• The treatment of diabetes• The benefits of exercise• The benefits of weight control/diet• The benefits of glycemic control• The pathophysiology of diabetes• Prevention of diabetes complications

Patient Empowerment
• Asked about patient’s fears about diabetes• Asked patient to set her own goals• Asked about barriers to care

Diabetes Specific Behaviors
• Ordered hemoglobin A1c• Ordered urinary microalbumin• Made appropriate referral to ophthalmology• Performed monofilament test• Put patient on aspirin

The Arizona Clinical Interviewing Scale
• Repeated questions only to verify/clarify• Used no medical terms unless defined immediately
without being asked• Made sure patient understood future plans• Avoided use of leading/multiple/why questions• Avoided giving premature assessment and plan• Avoided verbal/nonverbal judgment cues/reactions• Used appropriate body contact• Was aware of patient’s “space”• Patient was comfortable with eye contact• Gave nonverbal positive reinforcement

The Clinical Scenario
• Mexican American woman who did not have health insurance
• Recently diagnosed with diabetes• Just moved from a different state• Needed to establish care with a new physician• Little understanding of diabetes• Had a glucometer, but not using it• Symptomatic• She thought hemoglobin A1c value was 11

The SPs Explanatory Model
• Derived from qualitative studies in Mexican American populations
• Diabetes ran in her family, and she felt that there was no cure and that it could not be controlled.
• Her spouse and other family members were supportive.• She had consulted her grandmother, a curandera. • She was eating nopalitos.
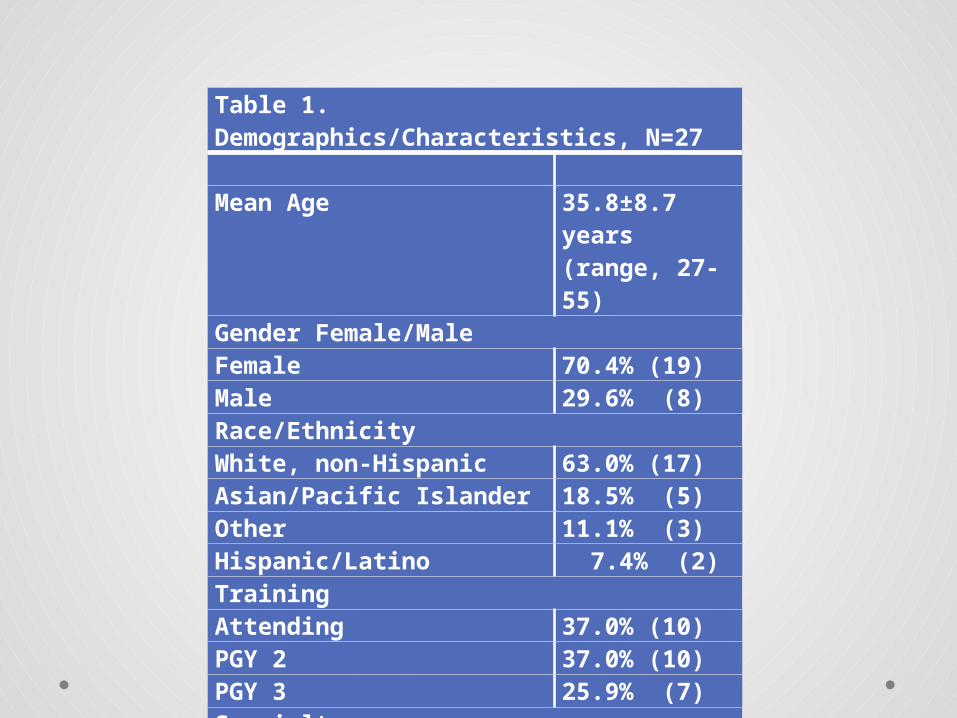
Table 1. Demographics/Characteristics, N=27 Mean Age 35.8±8.7 years
(range, 27-55)Gender Female/MaleFemale 70.4% (19)Male 29.6% (8)Race/EthnicityWhite, non-Hispanic 63.0% (17)Asian/Pacific Islander 18.5% (5)Other 11.1% (3)Hispanic/Latino 7.4% (2)TrainingAttending 37.0% (10)PGY 2 37.0% (10)PGY 3 25.9% (7)SpecialtyFamily Medicine 70.4% (19)Internal Medicine 29.6% (8)

Table 1. Demographics/Characteristics, N=27 Prior Cultural Competence Training<1 hour 14.8% (4)1-3 hours 11.1% (3)4-6 hours 22.2% (6)7-10 hours 14.8% (4)>10 hours 37.0% (10)Patient Panels Race/Ethnicity (mean %)White, non-Hispanic 43.4%Hispanic/Latino 38.5%African American 8.6%Asian/Pacific Islander 5.7%American Indian 2.9%Other 1.7%Conversational SpanishNone 14.8% (4)Poor 11.1% (3)Fair 40.7%(11)Good 22.2% (6)Excellent 11.1% (3)

Table 2. Individual Item Responses, N=27
Subscales and Items Percentage of “Yes”
Responses (n)
Subscale 1: Explanatory Model Elicitation
Asked patient’s view of illness 81.5% (22)
Asked patient’s view of illness treatment 81.5% (22)
Asked about patient’s use of other medical/traditional providers
70.4% (19)
Asked about family support 51.9% (14)
Asked about community support 48.1% (13)
Asked about gender role in family and how this influences care
44.4% (12)
Subscale 1 Total Score 63.0%

Table 2. Individual Item Responses, N=27 Subscale 2: Cultural Knowledge Indicated knowledge when asked, “Is it true that Mexican Americans have higher rates of diabetes?”
96.3% (26)
Addressed health beliefs regarding fatalism 74.1% (20)Indicated knowledge when asked, “I have been eating nopalitos. Have you heard of those?”
70.4% (19)
MD addressed health beliefs, before patient brought up 33.3% (9)MD brought up higher rates of diabetes in Mexican Americans, before SP asked.
0% (0)
MD brought up nopalitos, before SP asked 0% (0)Subscale 2 Total Score 45.7%

Table 2. Individual Item Responses, N=27 Subscale 3: Non-Judgmental BehaviorDid not threaten insulin if did not take medications 85.2% (23)Did not condemn use of alternative treatments 85.2% (23)Did not condemn use of alternative healers 85.2% (23)Was non-judgmental in response to elevated hemoglobinA1c 85.2% (23)Did not threaten complications if did not take medications 81.5% (22)Subscale 3 Total Score 84.4% Subscale 4: Sharing Biomedical ModelShared knowledge about… the treatment of diabetes 96.3% (26)the benefits of exercise 88.9% (24)the benefits of weight control/diet 81.5% (22)the benefits of glycemic control 81.5% (22)the pathophysiology of diabetes 74.1% (20)prevention of diabetes complications 66.7% (18)Subscale 4 Total Score 81.5%

Table 2. Individual Item Responses, N=27 Subscale 5: Patient EmpowermentAsked about patients fears about diabetes 63.0% (17)Asked patient to set her own goals 63.0% (17)Asked about barriers to care 51.9% (14)Subscale 5 Total Score 59.3% Subscale 6: Diabetes Specific BehaviorsOrdered hemoglobin A1c 66.7% (18)Ordered urinary microalbumin 63.0% (17)Made appropriate referral to ophthalmology 44.4% (12)Performed monofilament test 14.8% (4)Put patient on aspirin 11.1% (3)Subscale 6 Total Score 40.0%

Table 2. Individual Item Responses, N=27 Subscales and Items Percentage
of “Yes” Responses
(n)Subscale 7: Arizona Clinical Interview Rating Scale (ACIR)General Communication:Repeated questions only to verify/clarify 96.3% (26)Used no medical terms unless defined immediately without being asked
96.3% (26)
Made sure patient understood future plans 96.3% (26)Avoided use of leading/multiple/why questions 92.6% (25)Avoided giving premature assessment and plan 92.6% (25)Avoid verbal/nonverbal judgment cues/reactions 88.9% (24)Nonverbal communication:Used appropriate body contact 100% (27)Was aware of patient’s “space” 100% (27)Patient was comfortable with eye contact 100% (27)Gave nonverbal positive reinforcement 96.3% (26)Subscale 7 Total Score 95.9%

Total Score • 70.7±11.0%, with a range of 43.9 to 90.2%
• No significant differences by any demographic or other characteristics.

Correlations• Non-Judgmental Behavior and Sharing the Biomedical
Model, Spearman’s rho= -.403, p=.037. • Sharing the Biomedical Model and Patient
Empowerment, rho=.717, p<.001. • Explanatory Model Elicitation and Diabetes-Specific
Behaviors subscale, rho=.466, p=.014. • The item, “Asked patient’s view of illness treatment” was
associated with higher levels of cross-cultural training, p=.032.

Limitations• Small study• One time visit only• Many university-based physicians with high levels of
cultural competence training

Conclusions• Providers asked about explanatory models• Providers asked about social support less frequently• How providers deliver the message (the biomedical
model) is important!• Medical student and resident training in motivational
interviewing

Conclusions
Our results suggest that culturally competent care and good diabetes care are intertwined.

Acknowledgements
• The authors would like to thank Dr. John Harris, Jr. for his contributions to the design of this research project.
• This research was supported by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases (R41 DK62569).
• Dr. Kutob’s time also supported by the Arizona Area Health Education Centers’ Clinical Outcomes and Comparative Effectiveness Research Fellowship.