Embed Size (px)
Citation preview

Ashy Shanker July 2009
© Copyright of NHS Doncaster 1
Doncaster Primary Care Trust
Business Case Toolkit

Ashy Shanker July 2009
© Copyright of NHS Doncaster 2
Contents Page
1. Introduction 3
2. The Business Case Process 4
3. Templates 26
4. Training 26
5. Contacts 27

Ashy Shanker July 2009
© Copyright of NHS Doncaster 3
Introduction
As an NHS organisation, NHS Doncaster has finite resources. These resources are managed by the Trust Board through a five year financial strategy taking into account national and local requirements. In order to commission services that represent the best value for money, a robust, responsive and consistent business case process needs to be in place.
The primary aim of the Business Case Toolkit is to clarify the revised business case process within the PCT. It explains the stages involved in developing an idea into a mainstreamed service. In addition it provides a base for service development/ improvement, linking the business development, approval and implementation functions of the PCT.
The Business Case Toolkit is a a dynamic document. As a learning organisation the PCT will acquire and deploy new skills and capabilities to improve services. Complementary to this, the Business Case Toolkit will be reviewed and updated to include ‘tried and tested’ tools and techniques. It will also provide links to agreed templates, training opportunities for service improvement skills, support and guidance to achieve successful outcomes.

Ashy Shanker July 2009
© Copyright of NHS Doncaster 4
7. PBC Consortia /Business Development Group
1.Project idea / need definition/ mandate
6. Partnership Board /SIRT/ responsible group – to consider recommendations
4. Working Group: investigation stage
3. Partnership Board / SIRT* / responsible group
2. Project lead /Sponsor assigned
9. Business Development Group (BDG)
8. Working Group : Business case development stage
10. Commissioning Executive
11. PCT Trust Board – exception
12. Procurement
15. Working Group : mobilisation stage
13.Working Group: evaluation stage
The Business case processNot all stages in the development stage are mandatory
5. Light touch business cases
16. Service delivery & monitoring group
14. Contract awarded
De
ve
lop
me
nt
sta
ge
Ap
pro
va
l s
tag
eIm
ple
me
nta
tio
n s
tag
e
<2 weeks
< 1 mnth
< 2 mnths
< 6 mnths
< 1.5mnths
< 6 mnths
17.Gate 1
18. Gate 2
19.Gate 3
* Service Improvement Re-design Team
Ashy Shanker July 2009
© Copyright of NHS Doncaster 5
Balancing responsiveness and accountability
The Business case toolkit and associated templates represent good practice for the development of a robust proposal to support your work. NHS Doncaster does however recognise the need for the process to reflect the complexity and the financial value of the business case proposed while considering the information received to make a decision regarding allocation of resources.
For business cases requesting resources less than £ 50, 0000 a partially complete business case containing sufficient information for decision making will be considered.
For business cases requesting resources above £50,000, the template pack will be expected to be completed in full.

Ashy Shanker July 2009
© Copyright of NHS Doncaster 6
1.Project idea/need definition/mandate
A project idea could originate from a staff member, a team (Providers / Practice based commissioners, a group) or a member of the public. This needs to be
discussed and agreed with the Project Sponsor( usually and Assistant Director, Deputy Director or Director of the PCT).
The outcome of this stage would be a Project definition/mandate, clarifying the scope of the project, i.e. what is included and not included.
Click here for Project Mandate Template.
2. Project Sponsor and Lead assigned
The Project Sponsor is the person who is responsible for delivering the project in relation to PCT strategic objectives. He/She is also the budget holder of the service area and also has overall responsibility for the project.He/She is usually an Assistant Director/Deputy Director/Director of the PCT.
The idea generator could be the Project lead ,or another member assigned by the Project Sponsor. The Project Sponsor will be responsible for the analysis of current providers to avoid duplication, and the identification of links and dependencies with other areas of service development. This could be initiated by liaising with the PCT contracting leads for acute services, community services and primary care services.
3. Partnership Board / SIRT / responsible group
This is the responsible group that provides strategic guidance and advice to the project. The group will be multi disciplinary , providing expert views covering the
following core functions. •PCT Strategy/Commissioning•Clinical guidance•Patient /User involvement•Provider involvement ( if required)
Their terms of reference will include strategic guidance of the project/ service and monitoring of progress/ delivery. The group must undertake prioritisation and options appraisal of proposals before it is presented to the PCT for approval.
At this stage the group will validate a proposal as appropriate for further investigation and assign a core working group to collect the information to provide
an outline of the business case. Project ideas will be prioritised based on its alignment to NHS Doncaster’s strategy, particularly its link to the Commissioning
Strategy, Strategic plan, Commissioning Prospectus and Vital signs. See appendix for Terms of reference of SIRT/Partnership Board
Business case process

Ashy Shanker July 2009
© Copyright of NHS Doncaster 7
4. Working Group: investigation stage
This group collects and validates qualitative and quantitative information to make a recommendation to the responsible group
(SIRT/Partnership Board) to proceed with the project or not. An options appraisal including financial evaluation is vital at this stage and will be
referenced throughout the life of the project/ service. Functions involved may include
•Risk assessment•Process mapping•Demand & capacity review•Patient & Public involvement•Health needs analysis•Referral review•Options appraisal •Financial evaluation & •Fact finding
5. Light touch business cases
These business cases are small in value and funded from practice based commissioning freed resources. They are identified by Practice Based Commissioning consortia and fast tracked through the PCT’s internal processes. These business cases are approved by the Director of
Commissioning in line with standing financial instructions, with all approvals being reported to the Commissioning Executive.
The criteria of eligibility is as follows:A total cost of no more than £50,000
for a duration of not more than 3 years based on the DoH menu of flexibilities for the use of PBC freed resources.
Business case process

Ashy Shanker July 2009
© Copyright of NHS Doncaster 8
6. Partnership Board /SIRT/ responsible group – to consider recommendations
At this stage a recommendation is reached by the group regarding the prospect of the proposal. It could be considered appropriate or inappropriate to
proceed. If considered inappropriate, the Project Sponsor could still decide to submit proposal to the PCT approval process. However the Business
Development Group and Commissioning Executive will consider the opinions of the responsible group while making their
recommendations/decisions respectively. If considered appropriate, the group will assign a Working Group for formal Business case development.
Any disagreements between the Project Sponsor will be reported to BDG.
Resources to be identified to develop the business case including clinical engagement, training & management requirements . Any issues/delay regarding progress will be escalated to the Assistant Directors/Deputy
Directors forum.
7. PBC Consortia /Business Development Group
SIRT will also make recommendations to / seek advice from the Practice Based Commissioning Consortia and
Business Development Group. However the ultimate decision to progress the project proposal to the approval stage
lies with the Project Sponsor
Business case process

Ashy Shanker July 2009
© Copyright of NHS Doncaster 9
8. Working Group : Business case development stage
During this stage the working Group will complete the suite of agreed documents associated with the business case approval process. This
includes the1. Business case template 2. Finance template 3. Procurement Decisions template 4. Service specification and5. Mandatory Assessment templates like the Equality Impact as
sessment
The core working group will consist of the following functions• Clinical lead• Project lead• Practice Based commissioning • Procurement• Human Resources• Finance( PBC / Business Development/ Contracting)• Quality/ Clinical assurance• Performance
The extended working group may include by exception• Providers (for additional clinical input / MDT/ operational
management input)• Public Health( interpretation of clinical models/ population
profile & advice)• Prescribing support• Patient and Public Involvement• Information• Contracting • Infection control• and other support functions
The working group will need to start with• Agreeing terms of reference• Developing a detailed project plan• Under taking mandatory assessments and taking action if
appropriate• Undertaking Patient and Public involvement work• Agreeing an evaluation team for procurement stage as
appropriate. (Criteria for membership to be determined)• Agreeing evaluation criteria and weightings
Business case process
Ashy Shanker July 2009
© Copyright of NHS Doncaster 10
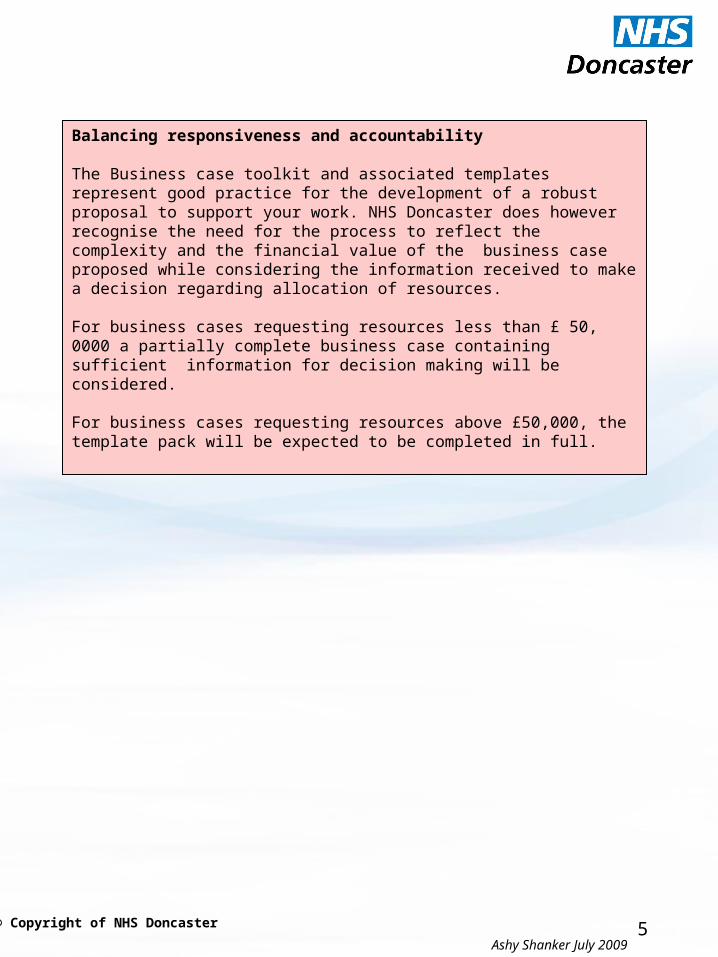
9. Business Development Group
Business case received
Acknowledgement sent
Recommendation Deferred RejectedSHA QA approval
Additional info/clarification
Assess risk/update log
Advice from planning lead and business function reps
PEC advice ?
8. Working Group : Business case development stage
9. Business development Group
Approx 2 weeks
10. Commissioning Executive Report to Commissioning
Executive
Business case process

Ashy Shanker July 2009
© Copyright of NHS Doncaster 11
10. Commissioning Executive
Additional info/clarification
ApprovedRejected
B u s i n e s s c a s e l e a d & c o m m i s s i o n i n g g u a r d i a n n o t i f i e d
Assess risk/update log
SHA QA approval
PEC advice ?
Sta
ge
2
12. Procurement
11. PCT Trust Board – exception
10. Commissioning Executive
9. Business development Group
Approx 2 weeks
8. Working Group : Business case development stage
Business case process
11.PCT Trust Board – by exception
Some Business case proposals will go to PCT Trust Board for approval in accordance with standing financial instructions. Or by exception, the Commissioning Executive may
seek further advice from the Trust Board.

Ashy Shanker July 2009
© Copyright of NHS Doncaster 12
Procurement Thresholds for Goods and ServicesQuotations are required for contract values that are above £10,000 but do not exceed £49,999 including VATCompetitive Tenders are required for contract values that are above £50,000 including VATEuropean Procurement Directives apply to contract values that are above: - £90,319 for Goods and Part A Services - £139,893 for Part B ServicesHealthcare ProcurementUnder the Principles and rules for Cooperation and Competition (DH 13 Dec 2007), PCTs must gain consent of their boards and inform SHAs where they decide not to tender a contract for a new or significantly changed healthcare service. (The NHS in England: The operating framework for 2008/9 Annex D - Principles and rules for co-operation and competition). Relevant guidance for healthcare procurement:Operating Framework 2008/9Principles & Rules For Cooperation & Competition – Annex D Operating FrameworkFramework for Managing Choice, Cooperation & Competition (May 08)PCT Procurement Guide for Health Services (May 08)Key Principles of Good ProcurementPurpose TransparencyObjectivity Proportionality Non discrimination Equality of opportunity AccountabilityConsistency
Note 1 – The open process allows all providers who send in an Expression of Interest (EOI) the right to submit a tender. Following receipt of EOI, Invitations to Tender (ITT) documents are sent out and must all be returned by pre determined date and time.
Note 2 -Evaluation panels should be established for each project but the size of the group should be proportionate to the size, value and strategic importance of the project. This group will meet throughout the process to agree evaluation criteria. Panel members will need to commit to evaluate each tender either independently or as a group and also commit to support the process until the point of award and must prioritise the time for this role.
Note 3-Once approved by the Commissioning Executive/Pct Trust Board the fist consideration may be to service notice on exiting contracts as appropriate. This will reduce delay in the new process being implemented.
12. Procurement
Business case process

Ashy Shanker July 2009
© Copyright of NHS Doncaster 13
Restricted OpenDialogue
Service requirement is advertised via www.supply2health.nhs.uk and/or in appropriate journal/publication to promote sufficient
competition
Completed tenders are returned by given date
Evaluation Panel clarify and evaluate against pre- determined criteria.
See Note 2.
Detailed evaluation of tenders (including clarification, presentations and site visits if
necessary) is completed . Successful tenderer is identified
Expressions of Interest received. Note 1
Contract Awarded
Unsuccessful tenderers are notified and debriefed
Total time required is minimum of 4 months which includes preparation of Invitation documentation following receipt of completed specification. This does not include implementation or TUPE.
Open
Restricted

Ashy Shanker July 2009
© Copyright of NHS Doncaster 14
Note4 – The restricted process allows all providers who send in an Expression of Interest (EOI) to submit a Pre- Qualification Questionnaire (PQQ). The PQQ is used as a short listing mechanism and the basis for this is financial standing, technical capability and quality assurance. The restricted route is used where the commissioner has a clear idea of the requirement and has a detailed specification. Following return of tenders, the process allows for clarification prior to award.
Restricted
Service requirement is advertised in appropriate journal/publication to promote sufficient competition
Completed Pre-Qualification Questionnaires are returned by a given closing date
Evaluation Panel to score & identify a shortlist
from predetermined criteria. Note 2.
Detailed evaluation of tenders including clarification, presentations and site visits if necessary is completed .
Successful tenderer identified
Shortlisted providers are invited to tender.
Expressions of Interest received. Note 3
Contract Awarded
Evaluation Panel evaluate using same criteria
Unsuccessful tenderers are notified and debriefed
Total time required is a minimum of 6 months which includes preparation of Invitation documentation following receipt of completed specification This does not include implementation or TUPE transfers/
Business case process

Ashy Shanker July 2009
© Copyright of NHS Doncaster 15
Dialogue
Service requirement is advertised in appropriate journal/publication to promote sufficient competition
Completed Pre-Qualification Questionnaires are returned by a given closing date
Evaluation Panel to score and identify a shortlist
from predetermined criteriaNote 2.
Outline Solutions submitted and dialogue takes place.
Shortlisted providers (Usually no more than 5) are Invited to Submit Outline Solutions.
Dialogue with providers is ‘opened’
Expressions of Interest received.
Note 4
Contract Awarded
Evaluation Panel evaluate Again using same criteria
Unsuccessful tenderers are notified and debriefed
Total time required is a
minimum of 9 months which
includes preparation of
Invitation documentation
following receipt of completed specification This does not
include implementation,
Public consultation or
TUPE transfers/
Detailed Solutions submitted and dialogue continues. Shortlist to 2 (3) Providers
Invitation to Submit Detailed Solutions sent out
Invitation toSubmitFinal Tender sent out to 2 Providers.
Dialogue Closes
Final Tender received and evaluated.
Evaluation Panel evaluate Again using same criteria
Business case process

Ashy Shanker July 2009
© Copyright of NHS Doncaster 16
Note 5 – The competitive dialogue process allows all providers who send in an Expression of Interest (EOI) to submit a Pre- Qualification Questionnaire (PQQ). The PQQ is a short listing mechanism and the basis is financial standing, technical capability and quality assurance. Competitive Dialogue (CD) is used where the commissioner has a clear idea of what the outcomes for the service are but not the service/treatment model and would like to seek innovative solutions form the market which can be developed with potential providers as part of the CD process. Dialogue remains open throughout the process and detailed solutions can be submitted if required. Dialogue will then close and a formal tendering process follows.
13.Working Group: evaluation stage
At this stage the evaluation team agreed during the Working Group: Business case development stage will evaluate the received bids and agree on a recommendation to
Commissioning Executive/ Trust Board regarding the preferred bidder.
14. Contract awarded
Formal notification is made to the preferred bidder about the decision to award contract.
15. Working Group : mobilisation stage
The working group at the business case development stage will change to become the working group - mobilisation stage, to implement and monitor progress of the
proposal. Core members will include
•Project Lead•Performance lead•Provider representatives
16. Service delivery & monitoring group
This group will monitor the service once it is mainstreamed. Functions may include• Project lead• Performance• Contracting
Business case process

Ashy Shanker July 2009
© Copyright of NHS Doncaster 17
16. Service delivery & monitoring group
Once the service is up and running well, this group will monitor and manage the performance of the service the service on an ongoing basis. It may be a virtual group and elements of the performance management may be undertaken by a
range of people, depending on the nature of the service. The core team will include as a minimum:
• Project lead• Performance lead• Contracting lead• Commissioning lead (if project lead is different)• Other members may include public health and quality
depending on the nature of the service
Functions will include regular monitoring of performance; co-ordination of range of performance indicators from different sources; identification and agreement to actions required regarding performance issues and escalation as appropriate.
It is recognised that it is important to have an overall lead (project lead) but that a range of functions contribute towards performance management as a whole, with a specific function sitting within the contract performance team. The diagram above illustrates how the functions of each team contribute towards performance management as a whole.
Performance management
Performance
Contracting
Commissioning
Public health
Quality

Ashy Shanker July 2009
© Copyright of NHS Doncaster 18
Gated processes:
This is checkpoint within the process where major decision are made regarding the progress of the project. At each gate the Project lead gets the go ahead to continue to the next stage.
Gate 17.At Gate 1 the Partnership Board/SIRT/ responsible group recommends that the proposal/project could be progressed to the next stage for Business case development. This gate therefore recognises the potential for achievement of aims and outcomes of the proposal/idea.
Gate 18.At Gate 2 the PCT makes a decision to support the project, defer the project or reject the project. This gate therefore indicates formal commitment from the PCT to formally support the project.
Gate 19.At Gate 3 the Procurement process is complete and the contract is awarded to the preferred provider. This gate marks the beginning of the implementation process.
Business case process

Ashy Shanker July 2009
© Copyright of NHS Doncaster 19
Templates available to support the process
1. Project mandate / idea template- to be added2. Business case template3. Finance template 4. Procurement Decisions template 5. Service specification6. Equality Impact assessment 7. Service specification template – to be added8. Privacy Impact assessment 9. Environmental Impact assessment– to be added
Any queries please contactAshy ShankerTel: 01302 566137Email: [email protected]
Training available for
1. LEAN Healthcare overview2. Process flow analysis3. 6S Workplace Organisation4. Standard Operating Procedures5. Visual Management6. Capacity and Demand7. Problem Solving
For further details please contact HR Department on
01302 566030

Ashy Shanker July 2009
© Copyright of NHS Doncaster 20
Contacts
Overall process – Ashy ShankerTel: 01302 566137Email: [email protected]
SIRT - Richard MetcalfeTel: 01302 381924Email : [email protected]
Procurement – Claire BurnsTel: 01302 566119Email : [email protected]
Performance – Anne BootheTel: 01302 566065Email : [email protected]
Contracting – Claire HudsonTel: 01302 566142Email : [email protected]
Finance – Anita BlakestonTel: 01302 566014Email : anita.blakeston @doncasterpct.nhs.uk
Clinical quality/ assurance – Karen PriceTel: 01302 566164 Email : [email protected]
Patient and Public engagement – Sarah Atkins WhatleyTel: 01302 566034 Email : [email protected]
Equality and Diversity – Catherine LeggettTel: 01302 566097Email : [email protected]
Public Health – Rupert SucklingTel: 01302 566105Email : [email protected]

Ashy Shanker July 2009
© Copyright of NHS Doncaster 21
Appendix Terms of reference Dated: 30 July 2008
SERVICE IMPROVEMENT RE-DESIGN TEAM (SIRT)1.ROLE/PURPOSE The Service Improvement Re-design team will oversee the delivery of the Service Re-designs identified within the PCT Commissioning Prospectus together with areas of possible service re-design/improvement identified by either PBC or the PCT. SIRT will provide support and share knowledge and expertise around service re-design and will make recommendations to the PCT with regard to each individual Service Re-design project. SIRT will also provide detailed reports and updates to the Commissioning Executive when requested.2.OBJECTIVESOversee areas of Service re-design identified in the Commissioning Prospectus and deliver a uniformed approach and standardsProvide Project Management Support to the PCT/PBCMake recommendations to the PCT/PBC regarding each individual service re-design projectIdentify Project Lead & Project Sponsor for each individual project.Receive service redesign proposals from PBC (others?) and confirm they align to the strategic direction of Doncaster PCTReceive service redesign proposals from PBC (others?) and confirm they meet all requirements before implementation (i.e. ownership)Quality assure the service specifications and business cases before submission to the Commissioning executive?Implement Lean Tools and Techniques within each Directorate Share Knowledge and ExpertiseProvide Clinical expertise/advice to the members of the SIRT group when required on Service Re-design projectsProvide performance information to both the PCT and PBC as to the progress of the individual service re-design projectsPromote partnership working both internally and with external organisations Refer areas of concern, to the PCT and PBC for a decision to be madeEnsure users and carers are involved in the service re-design workEnsure PBC are fully supportive of service redesign proposalsManage the Projects through the PCT Business Case process
2. CHAIR Alaina Challans, Service Development Programme Manager 3. Administration Planned Care Support Officer Agenda to be distributed one week before meeting Minutes to be distributed one week after meeting
Business case process

Ashy Shanker July 2009
© Copyright of NHS Doncaster 22
3.MEMBERSHIPMembership of the group:Service Development Programme Manager Service Development Manager – Planned Care (x 2)GP - Board Member of DCCGP- Board Member of B & CGP - Board Member of DICEHead of Strategic Commissioning Project Manager Unplanned Care Commissioning Manager Unplanned Care Head of Commissioning, Mental Health Commissioning and Planning Manager PBC Project Manager Public Health Public Health Intelligence Unit (?)Primary Care CommissionerPBC FinanceHead of Medicine Prescribing and SupportHuman Resources Procurement Head of Business Development Unit
4.ACCOUNTABILITYDoncaster PCTDoncaster PBC Consortia5. Frequency of meetings Monthly
Business case process
Ashy Shanker July 2009
© Copyright of NHS Doncaster 23
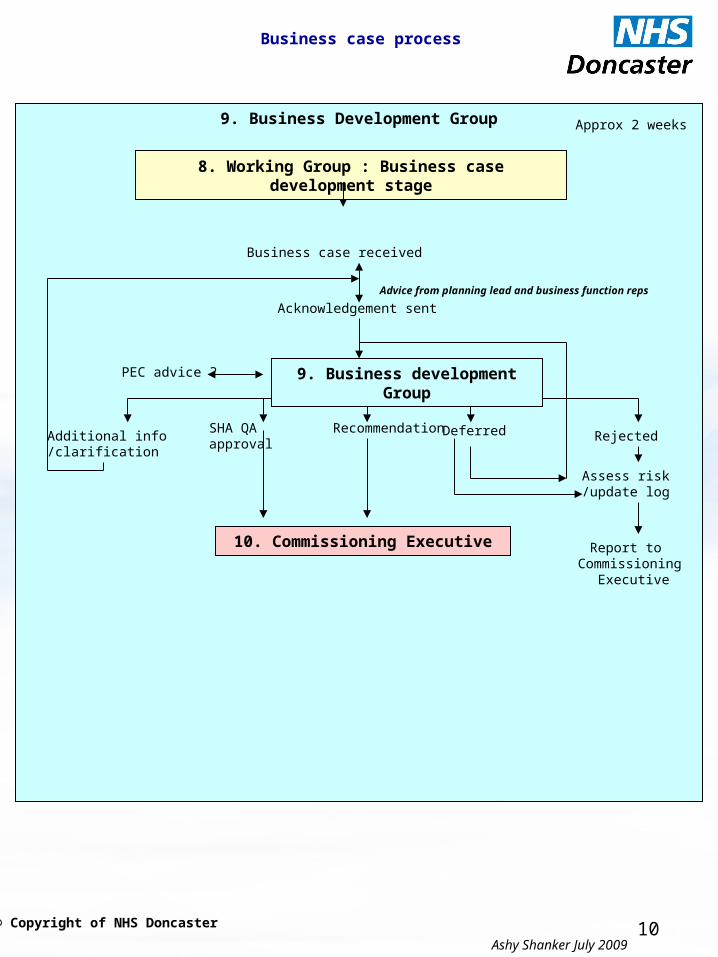
Terms of reference of a Partnership Board
PUBLIC HEALTH PARTNERSHIP BOARDROLE / PURPOSETo protect and improve the health of the people of Doncaster, reduce inequalities in
health and improve access to services.OBJECTIVES2.1 Common Partnership Board ObjectivesUtilise appropriate needs analysis and information to support the development of
strategy and commissioning of services.Anticipate new developments in service delivery, national requirements and new
legislation.Develop and implement strategies for service delivery based on long term
perceptions of the future of services.Develop commissioning priorities through consultation with local stakeholders and
ensure that these are fed into the local delivery planning process.Ensure service users and carers are involved in all aspects of planning and
commissioning of services. Oversee the commissioning, re-design and delivery of services ensuring consistency
in service delivery.Ensure that all services are culturally competent and able to meet the different
cultural needs of all communities in the area. Ensure services are evidence based, efficient, effective and economic and thereby
offer good value for money.Ensure services are provided within available resources, whilst identifying and
reporting the need for additional resources to the Healthier Doncaster Theme Group.
Promote partnership working, service integration and joint commissioning where this will lead to better outcomes for those who use the services.
Monitor and report on service performance and key performance indicators both internally and externally
Make recommendations for additional resources to the Healthier Doncaster Theme Group where new legislation, government guidance or service improvements cannot be met from within existing resources.
Refer matters of concern, or decisions, to the Healthier Doncaster Theme Group where such issues are outside its own delegated responsibility or have a borough wide impact.
Agree an Annual Work Programme with the Healthier Doncaster Theme Group.2.2 Objectives Specific to the Public Health Partnership Board Protect the population of Doncaster from identified current and new hazards to
health by having a planned, prepared and practiced response to incidents and emergency situations which could affect the provision of normal services.
Have systematic and managed disease prevention and health promotion programmes in place which meet the requirements of national plans and address local needs.
Business case process
Ashy Shanker July 2009
© Copyright of NHS Doncaster 24
Ensure that services commissioned take account of public health outcomes and seek to address inequalities by influencing the use of mainstream resources to improve services and outcomes.MEMBERSHIP & QUORACYThe membership will be as follows:Joint Director of Public Health – DMBC/PCT - ChairDeputy Director of Public Health - PCTHead of Strategic Partnerships – PCTRepresentative – Commissioning and Strategic Development – PCTCabinet Member for Public Health - DMBCDirector (Adult Services) - DMBCDirector (Children’s Services) – DMBCDirector (Neighbourhoods & Communities) - DMBCRepresentatives – Community/Voluntary Sector X 2Representative – Rotherham, Doncaster and South Humber Mental Health NHS Foundation TrustRepresentative – Doncaster & Bassetlaw Hospitals NHS Foundation TrustRepresentative – PCT Provider ServicesThe Strategic Partnership Manager will provide support to the Board and its members across the full range of their responsibilities. The Board may co-opt other members at any time if this helps the Board achieve its objectives and it will periodically review its membership to ensure it represents the broad spectrum of views and needs within the local community. The board may require other people to be in attendance for its meetings. The Chair will be the Joint Director of Public Health and the Vice-Chair will be from the Voluntary/Community organisations. The Board may set up such sub-groups as may be required in furtherance of its stated objectives and to plan services effectively. The Board will be deemed quorate if more than 50% of the members are in attendance including the Chair.GOVERNANCE AND ACCOUNTABILITYThe Public Health Partnership Board will be accountable to the Healthier Doncaster Theme Group for the delivery of its work programme and for delivery of the relevant priorities in the Borough Strategy and Local Area Agreement. In fulfilling that accountability the Board will: Produce reports on its financial and operational performance and ensure all relevant matters are reported to the Healthier Doncaster Theme Group and the constituent authorities to ensure compliance with both internal and external reporting requirements.Work closely with other service led Partnership Boards where there is a common interest to ensure services are delivered in as seamless a way as possible and are user focused, promoting equality and diversity.FREQUENCY & FORMAT OF MEETINGS Meetings will be held bi-monthlyREVIEW OF TERMS OF REFERENCE & MEMBERSHIPTerms of reference and membership will be reviewed annually.

Ashy Shanker July 2009
© Copyright of NHS Doncaster 25
WORKING PRINCIPLES
The Board will develop local services on the following principles:Seek to reduce health inequalities and promote people’s health and wellbeing.Work within a framework for neighbourhood planning that supports community partnerships and other community organisations and works towards a co-ordinated approach to service planning in neighbourhoods.Equitable access and social inclusion across the whole communityMaximise peoples choices and promote their quality of lifeEnable people to enjoy their civil rights in order to reduce discriminationProvide person centred support to maximise peoples independence, offering care at home, or as close to home as possible.Provide services through a well-informed and trained workforce.To have regard to how decisions made and business practices affect and impact on local communities and the environment.Ensure consideration is made of adult protection implicationsEnsure consideration is given to the following cross-cutting issues:
HousingCultureEconomy
11th October 2007
Ashy Shanker July 2009
© Copyright of NHS Doncaster 26
Business Development Group Terms of reference 1. CONSTITUTION
The Commissioning Executive (The Committee), which is a sub-committee of the Board, hereby resolves to establish a group to be known as the Business Development Group (The Group). The Group has no executive powers.
2. MEMBERSHIPThe Group shall consist of not less than 7 members to include the following:
Assistant Director of Strategic Development (Chair) / Planning & Commissioning Manager Deputy Director of Finance and ProcurementDeputy Director of Public HealthAssistant Director of Performance ManagementDeputy Director of OD & Corporate AffairsProfessional Executive Committee member Quality and Clinical Assurance representativeA quorum shall be 3 members, this must include the Chair (or their nominated deputy), a clinician and a
finance representative.Where a member cannot attend they should nominate and appropriate deputy or submit written
comments.3. ATTENDANCE
Other directorate members will be invited to attend, as appropriate, but particularly when the Group is discussing areas of risk or operation that are the responsibility of that directorate.
4. FREQUENCYMeetings shall be held not less than 10 times a year. Members are required to attend a
minimum of 75% of meetings.5. AUTHORITY
The Group is authorised by the Commissioning Executive to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Group.
6. DUTIESThe duties of the Group can be categorised as follows:6.1 Governance, Risk Management and Internal Control
Following the agreed Business case process (Commissioning Executive; 22/07/08), evaluate all proposals presented to the Group through a consistent methodology, including risk assessment, to enable recommendations to be made to the Commissioning Executive as to the suitability for funding.
6.1.2 To ensure that proposals are in line with local and national policy including:World Class CommissioningStrategic ObjectivesCommissioning StrategyProcurement StrategyPartnership Board StrategiesDepartment of Health Core Standards and other statutory/regulatory requirementsNHS Litigation Authority/Auditors Local Evaluation risk management standardsValue for MoneyAchievement of Vital Signs, National and Local Targets (both new and existing) as appropriate

Ashy Shanker July 2009
© Copyright of NHS Doncaster 27
6.2 Other Assurance FunctionsTo provide assurance that the business planning process is robust and effective.To monitor the implementation of approved proposals to ensure they are delivered within agreed timescales.
Financial ReportingTo report to the Commissioning Executive on the financial implications of implementing approved proposals.
To monitor expenditure levels and report any significant variation to the Commissioning Executive.
6.4 ReportingThe minutes of Business Development Group meetings shall be formally recorded by the Project Support Officer and submitted to the Commissioning Executive. The Chair of the Group shall draw to the attention of the Commissioning Executive any issues that require disclosure to them or require executive action.
6.8 Other MattersThe Committee shall be supported administratively by the Project Support Officer, whose duties in this respect will include:
Agreement of agenda with the Chair/deputy and attendees and collation of papersTaking the minutes & keeping a record of matters arising and issues to be carried forwardDate of approval:…………………………………………………………………...Approved by:………………………………………………………………………..Review Date: March 2009

Ashy Shanker July 2009
© Copyright of NHS Doncaster 28
DONCASTER PRIMARY CARE TRUSTCOMMISSIONING EXECUTIVE 27TH JANUARY 2009
REVISED TERMS OF REFERENCE 1. INTRODUCTIONAt the September 2008 Trust Board meeting the Board agreed to interim arrangements to facilitate
the conduct of PCT business by delegating authority to the Commissioning Executive to make procurement decisions on behalf of the Board. It was agreed that these arrangements would be reviewed and reconsidered following a three month period. This paper is the output from this review and also constitutes revised Terms of Reference for the Commissioning Executive and was approved by Trust Board at its meeting on 8th January 2009
PURPOSEThe purpose of the Commissioning Executive is to:
Provide strategic input to the commissioning cycle, from high level strategy through to in-year performance
Provide the overarching decision making forum for commissioner-led decisions in the PCTThis role will be fulfilled through undertaking the following on a cyclical basis: Prepare and recommend to the Board the over-arching commissioning strategy and supplementary
commissioning prospectuses for the PCT

Ashy Shanker July 2009
© Copyright of NHS Doncaster 29
Assess business cases within the context of the commissioning strategy (including those from PBC Consortia/provider organisations and the PCT)
Proactively assess the performance and outcomes of services commissioned and take appropriate action
Provide a strategic level prioritisation process for annual investment decisions supported by the LDP process
3. PRINCIPLES FOR WORKING3.1 As the Commissioning Executive is the forum for key decision making regarding
commissioning issues, it is appropriate to establish the Executive as a formal sub-committee of the PCT Trust Board, with devolved decision making powers.
3.2 The Commissioning Executive will have an important relationship with many other agencies, including Social Services, Provider NHS and Foundation Trusts and neighbouring PCTs. However, to keep the Executive small enough to be focused and proactive in tackling the commissioning agenda, it is proposed that relationships with other agencies are managed and maintained through the other formal and informal mechanisms that exist across the locality. Exceptionally, it may still be necessary to invite representatives to the Executive meetings to discuss particular agenda items.
MEMBERSHIPThe core membership of the Commissioning Executive will consist of:
Trust Board Non-Executive Director PCT Director of Commissioning and Strategic Development (Chair)PCT Director of Finance & ProcurementPCT Director of Performance and InformationDirector of Public HealthPCT Deputy Director of Quality and Clinical AssurancePEC ChairTwo additional PEC Members**(if possible from differing clinical background)
The Executive may invite other officers to attend as required. The Assistant Director of Commissioning and Strategic Development will be responsible for co-ordinating and quality assuring the agenda and commissioning cycle for this meeting.
5. DELEGATED AUTHORITY5.1 The Commissioning Executive has delegated authority from Trust Board for healthcare
and non healthcare procurement decisions to a maximum value of £1M per contract, within the provisions of a pre approved financial budget
5.2 The Commissioning Executive has delegated authority from Trust Board for the awarding of contracts, following a procurement decision, to a maximum value of £1M per contract
5.3 The Procurement Guide requires a PCT to agree with its Board a procurement strategy for large, novel, contentious or repercussive tenders. Should the Commissioning Executive consider a tender below £1M in value, to fall into this category, it may seek support for its procurement decision from Trust Board
6. RELATIONSHIP TO OTHER GROUPS6.1 The Doncaster Commissioning Executive will be the single overarching group through
which commissioner led strategic level healthcare and non healthcare investment decisions, within the provisions of a pre approved financial budget, are agreed by the PCT. The Executive will however need to maintain close links to a range of other groups from which it will receive information, support and recommendations.

Ashy Shanker July 2009
© Copyright of NHS Doncaster 30
6.2 Those groups will include, but not exclusively be limited to, the following:The Yorkshire & Humber Specialist Commissioning GroupPartnership Boards, Programme Areas, PBC,PEC,Priorities Advisory Group, Local Commissioning GroupsSLA monitoring groupBusiness Development Group6.3 The relationship between the Executive and the groups will be a 2-way process and as such the Executive will be able to delegate day-to-day commissioning and investment decisions, within clearly defined parameters, to nominated PCT representatives sitting on any other commissioning group.7. THE LOCAL DELIVERY PLANNING APPROACH (LDP)7.1 The Executive will be responsible for overseeing and co-ordinating the Doncaster LDP submission to Yorkshire & Humber Strategic Health Authority (StHA). As such its responsibilities will include:Setting an annual timetable to ensure that the PCT meets all national and StHA LDP deadlines.
Delegating responsibility to relevant PCT officers to ensure key elements of the LDP process are completed and agreed on time.
Agreeing all LDP investment decisions to ensure a financially balanced plan is submitted to the StHA, which meets all key LDP and NHS Plan targets.Agreeing subsequent investment decisions originating within the LDP arena.8. FREQUENCY OF MEETINGS8.1 It is anticipated that throughout the year the Executive will need to meet twice monthly. However, this will be periodically reviewed to ensure appropriateness of frequency. 9. SECRETARIAT9.1 A detailed agenda and papers will be prepared in advance of each meeting of the Executive. Each meeting will also be minuted with minutes and detailed action points being circulated as soon as possible after the meeting. Minutes will be presented to the Trust Board and PEC meetings on a monthly basis and will include an updated schedule of procurement decision.