Embed Size (px)
Citation preview

The Science of the Total Environment 307(2003) 1–9
0048-9697/03/$ - see front matter� 2002 Elsevier Science B.V. All rights reserved.PII: S0048-9697Ž02.00504-1
Editorial
Asbestos: old foe in 21st century developing countries
Abstract
While use of asbestos materials in developed nations has been decreasing because of the harmful health effects ofasbestos dust mining, processing and use of the ancient material in developing countries is increasing. The regulatorymechanism for use, handling and disposal of asbestos and associated waste in developing countries are weak andinformation on asbestos-related diseases is scanty but emerging. We identify lack of epidemiological data on asbestoshealth effects as a major gap to be bridged in the promotion of occupational and environmental health in developingcountries. Without data on local situations, diseases such as asbestosis and mesothelioma remain too obscure to assistthe campaign for appropriate regulation of asbestos usage or attracting attention to abominable industrial practicesgenerally.� 2002 Elsevier Science B.V. All rights reserved.
Keywords: Asbestos; Environmental health; Occupational safety
1. Introduction
Whereas asbestos materials have been used forover a millennium, mounting evidence for respi-ratory diseases associated with occupational andenvironmental exposure to asbestos fibers has ledto diminishing demand for products containing thefibers (Virta, 2002). In developed nations, whereuse of asbestos products is either banned or veryrestricted(ILO, 1984; Becklake, 1998; US Envi-ronmental Protection Agency, 2000; ILO, 2001;ICFTUyTUAC, 2002), requirements for properhandling, use and disposal of asbestos are backedby compensation schemes and frameworks forexpensive punitive litigation for offenders(Chem-istry in Britain, 2001). In addition to assistingvictims of past asbestos exposure and their familiesthese measures, having generated a vibrant andaggressive litigation industry, have served as vitalenforcement and compliance tools for asbestoshealth and safety regulations.
These measures and the ban asbestos movement(Ban asbestos, 2002) have been so successful in
developed countries that the large USA asbestosdeposits remain unexploited(Virta, 2002) whileCanada is the only developed country that produc-es, almost entirely for export, significant quantitiesof asbestos fibers. In 2000 Canada, the secondlargest producer(behind the Commonwealth ofIndependent States, CIS) and the world’s leadingexporter of Chrysotile, produced approximately18% of the world’s Chrysotile(Virta, 2002). Muchof the rest(f74%) came from four developingcountries—China, Brazil, Zimbabwe and Kazakhs-tan (;38%) along with the economicallydepressed CIS(;36%) (Virta, 2002).
The success of the international ban-asbestoslobby, especially in Europe(Ban Asbestos Europe,2002), is viewed as a major reason for the gradualdecline in global Chrysotile asbestos production—with 2000 levels estimated to be 13% lowerrelative to those of 1995. Accordingly, CanadianChrysotile production over the same period fell byapproximately 34%. However, in sharp contrast tothis trend, Chrysotile production levels in the CIS

2 Editorial
were expected to increase by 10% while that ofBrazil remained essentially unchanged. The pro-duction levels in China were also expected toremain unchanged relative to 1995 levels butproduction levels had increased by 19% in 1998before dropping back to the 1995 level. Addition-ally, significant reduction in Chrysotile asbestosproduction among other developing countries hasoccurred in Zimbabwe(35%) and, more dramati-cally, in neighboring South Africa(79%). How-ever, South Africa has had a much publicizedmajor asbestos pollution and asbestos-related dis-ease problem that is being openly tackled, includ-ing by use of litigation. China, Brazil and the CIShave significant local markets for their asbestoswhile more developing countries such as Thailand,India, South Korea and Iran are major importersof asbestos. For example, the 17 top Chrysotileasbestos consuming countries, consume 20 000 ormore tones of Chrysotile asbestos to reach acumulative total of 2 021 000 tones(AsbestosInstitute, 1999). To this total, developing countriescontributed 45% and CIS 35%; consumption inindividual developing countries was: China(11%),Brazil (9%), Thailand(8%), India (6%) and Iran(4%).
The emerging picture therefore, is that of majorasbestos mining, processing and manufacturinginstallations flourishing in developing countrieswhile in developed nations, they are under intensepublic pressure to cease activity altogether.
2. Asbestos usage in developing countries
There are over 3000 different types of commer-cial products containing varying concentrations ofasbestos depending on ultimate usage. Asbestosproducts still popular in developing countriesinclude construction products such as roofing andsiding shingles, asbestos cement pipes, materialsused in stoves, vinyl carpets and floor tiles. Thereare also other products used in soundproofing(lecture theatres), thermal insulation (e.g. hotwater and steam pipe) and fireproofing(e.g. inbank vaults), adhesives, filers, brake shoe andclutch linings, floor tiles, and several textileproducts.
The continued use of asbestos in developingcountries, notwithstanding increasing support forthe ‘ban asbestos’ campaign in developed countriesand more recently in some developing ones too, ismisguidedly justified for the industrially desirablecharacteristics(high tensile strength, fire and heatresistance) of the asbestos fibers and their relative-ly low cost. While we believe that eventuallyasbestos should be replaced by less harmful mate-rials, our principle concerns with asbestos usageand pollution in developing countries relate toimproper use, handling and disposal of asbestos,asbestos containing materials and waste. In thisregard, there is evidence that asbestos plants indeveloping countries are run without proper safetyprocedures (Sunday Times, 2000; Iran DailyNewspaper, 2001).
3. Asbestos exposure in developing countries
There is no doubt that developing countrieshave many serious economic, social and politicalproblems. When governments and nations withinadequate resources have to deal with socio-political challenges presented by the HIVAIDSpandemic, debilitating diseases like malaria; waterbone diseases associated with consumption ofuntreated water and shortage of decent shelter,occupational and environmental pollutants that areperceived to be killing relatively few people overa long period of time are unlikely to receivepriority attention. Low attention to such problemsmeans that the full impact of adverse health effectsof occupational and environmental exposure topotentially harmful pollutants remains largelyobscure. Most importantly, low attention levels tooccupational health and safety means that:(a)regulatory procedures may be non-existent or notenforced;(b) mechanisms for identifying injuries,ailments and deaths arising from occupationalexposure to harmful materials may not be in place;and (c) precautionary measures that could savelives may not be adopted at the work place. Thus,the relative paucity of documented asbestos dis-eases in developing countries does not at all meanthat these diseases are minimal nor does it meanthat these countries are practicing safe asbestosuse, handling and disposal procedures. Asbestos-

3Editorial
related disease incidents are low in developingcountries because epidemiological questions of thisnature have not been systematically researched inmany of those countries.
For example, a report(Mitchev, 2001) to theAnnual Congress of the European RespiratorySociety, held in September 24, 2001, indicates that‘one in seven people in western societies mayhave been adversely affected by exposure to asbes-tos’. In just this one study, researchers performed160 autopsies at the Erasmus Hospital in Brusselsbetween 1998 and 2000 and found ‘pleuralplaques’ in 14% of the women, and in 20% of themen’. Such intense studies have not been reportedfor developing countries, except South Africa(Kielkowski et al., 2000), where over 7500 suffer-ers of asbestos-related diseases have been identi-fied. Thus, while asbestos usage in developingcountries has been known for a while and isincreasing, information about concomitant healtheffects is limited because research activity in theseareas has been low. Within this regime of poorlyunderstood ill-health effects of asbestos use indeveloping countries, promotion of asbestos usageby business interests and those trying to escaperesponsibility for past bad asbestos handling prac-tices flourishes unchallenged. It must be noted thateven in developed countries with significant casesof asbestos-related diseases, better monetaryresources, regulatory frameworks and compensa-tion mechanisms, there are persistent difficultiesfaced by asbestos victims in seeking and receivingcompensation, healthcare and protection from otheremployers or owners of offending manufacturingplants (Workers Online, 2001). It is thereforeconceivable that the challenges faced by asbestosvictims and their governments are more formidablein developing countries, where asbestos is stillmarketed aggressively(IBAS, 2002) and utilized,while regulations and controls are not as good asthose of developed countries. In such a confusedstate, advocates and luminaries of occupationaland environmental safety and health can find ithard to operate. At best, they can be readilyignored or dismissed as media attention seekersand at worst harassed with considerable careerending possibilities as was the case for Dr Joshi,
an Indian advocate of banning asbestos(Kazan-Allen, 2002).
4. Questioning the perception of ‘jobs or health’
Amazingly, the issues of jobs or health can bevery touchy in developing countries. Recently, theZimbabwe Congress of Trade Unions(ZCTU) hadto defend itself against charges that it backed aban asbestos call at the 2002 International LabourOrganization (ILO) conference(The ZimbabweIndependent, 2002). In denying the allegations theZCTU officials claimed that to the contrary, ‘theAfrican group agreed that asbestos should not bebanned until there was scientific proof of itsharmfulness’. The ZCTU official also added that‘everyone from Zimbabwe agreed that we cannotjust have our people thrown out of their jobsbefore there is scientific evidence of asbestosharmfulness’. With all the evidence available glob-ally and, in particular, from neighboring SouthAfrica and Swaziland, it is not clear what kind ofscientific evidence Zimbabwe can be waiting forbefore acknowledging the health dangers associ-ated with improper asbestos mining, processing,handling and disposal. While acknowledging thepotential of asbestos to cause harm Madava of theSouthern Africa News Features(Madava, 1999)also lamented the imminent collapse of SouthAfrican and Zimbabwean economies because ofthe global asbestos ban. But the report also statedthat authorities in Zimbabwe have in recent timesignored health complaints from residents of areasnear asbestos mines. One would have expected thehealth complaints to be investigated and actedupon in some way that satisfies both healthysafetyand economic concerns; but economic considera-tions clearly seem to be overwhelming.
A further example of economic considerationsoverwhelming health concerns, is found in thedangerous shipbreaking practice which has beenreported in several developing countries(Kanthakand Jayaraman, 2001). Shipbreaking is carried outby ill-informed workers under poorly regulatedconditions without due regard to proper healthsafeguards for both the workers and the environ-ment. The operations are so unsafe that asbestos

4 Editorial
is reported to have been found in workers’residences!
5. Misconceptions about the cost of properasbestos management
The view that the management of occupationaland environmental health is tremendously expen-sive is totally misguided, and is better replaced bythe belief in, and adoption of, the maxim ‘preven-tion is better than cure’. This in our view isespecially pertinent in the case of asbestos use indeveloping countries. Technologies for reducingairborne asbestos dust levels by wet methods,excluding asbestos fibers from inhaled air usingdurable facemasks and disposal of asbestos byburial are simple, cheap and available. Thus,deaths and ill-health miseries associated with prev-entable asbestos-related diseases in developingcountries are unacceptable and cannot be justifiedby poverty.
What is brazenly dangerous is the accommoda-tion of unsafe practices in asbestos mining, proc-essing and manufacturing activities as well asimproper handling and disposal of asbestos waste,which in developing countries seems to be theresult of a complex web of factors. Poverty is ofcourse overarching, but other important factorsare: unavailability of information on asbestos-related diseases among the exposed local popula-tion, inadequate dissemination of information onadverse health effects of asbestos, ignorance of ornon-compliance with simple worker protectivemeasures, lack of resources to implement relevantlegislation, callous attitudes of those who knowbetter and lack of punitive and litigation possibil-ities. Accordingly, unsafe mining, processing, useand disposal of asbestos in developing countriesare wide spread, and so are helpless victims, whoin some cases are reported to have lost their jobsonce they were diagnosed with asbestos-relateddisease. Better-documented examples are found inSouth Africa,(Kielkowski et al., 2000) and Swa-ziland (Coakley, 2000). For the Caribbean Region,recent reports and studies of asbestos-related prob-lems and have included Jamaica(Reid and Kahwa,1995) and US Virgin Islands(Weekend Observer,2002). Asbestos-related diseases were reported in
Brazil (Cauchon, 1999), China (Sun et al., 2001;Wen et al., 2001a,b), Iran (Koorosh, 2001), Uru-guay (De Stefani et al., 1996) and other develop-ing countries(Cauchon, 1999).
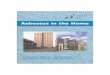
Some asbestos multinational companies haveabandoned their mining or manufacturing opera-tions in developing countries, leaving behind dan-gerous improperly disposed asbestos waste, whichpose health hazards for innocent and, often, unsus-pecting citizens. It begs the question—who isgoing to accept responsibility, in developing coun-tries, for adverse health effects caused by asbestosafter these companies are long gone. These are notjust distant probabilities as children playing onabandoned dump heaps in South Africa(HazardsMagazine, 2001) and Jamaica can attest(Fig. 1).Fig. 1 shows children in a squatter family com-pound in Jamaica located on a former asbestoswaste dump, polluted with asbestos cement waste,including crocidolite. The dangerous waste wasleft behind when two asbestos-cement plants oper-ating in Jamaica were closed in the early 1980sdue to pressure from trade unions and environmen-tal NGOs.
What the above account suggests is that the truecost of improper mining, processing, handling anddisposal of asbestos and asbestos waste in devel-oping countries is likely to be much higher thanthe cost of putting in place the necessary controls.
6. Managing the risk of asbestos in developingcountries
There is some good news in the asbestos pol-lution problem in developing countries. A culturaltransformation, which promotes occupationalhealth and safety as well as environmental health,is possible and the asbestos pollution problemappears to be a simple, readily comprehensibleand an effective educational tool for this transfor-mation. A reflection of this in Jamaica is thecollaboration between the University of the WestIndies, Mona Campus(UWI) and the JamaicaConfederation of Trade Unions(JCTU) to imple-ment a series of workplace workshops on theasbestos pollution identified in an earlier study byUWI researchers(Reid and Kahwa, 1995). Theworkshops have focused especially on health

5Editorial
Fig. 1. Asbestos pollution in the compound of a family squatting on a former asbestos waste dump in Old Harbour, Jamaica.
effects of asbestos, relevant personal protectionprocedures and devices, management of old asbes-tos installation and a review of relevant ILOconventions, as well as other related environmentalconventions and standards. Funding for this projectcame from the Environmental Foundation ofJamaica(EFJ), a non-governmental organizationin Jamaica, with technical support from ILO,(itsWorkers Division Branch and the CaribbeanOffice). Local professional support also came fromIndustrial Safety professionals and Environmental-ists from the Ministry of Health, the trade unionmovement, the Departments of Chemistry andCommunity Health and Psychiatry of the UWI,the Ministry of Labour and the National Environ-ment and Planning Agency.
This project, in fact, is part of greater alliancebetween the UWI and JCTU aimed at addressingoccupational safety and health concerns in theCaribbean region. This is a unique collaboration,as it is the first time that workers and the academiccommunity in Jamaica are specifically focusing,by way of a seminar series, on addressing safeuse, handling and disposal of asbestos. The mainobjectives and components of this joint UWI–JCTU Enterprise-based educational project are to:(a) print and distribute educational materials onthe health risk of asbestos;(b) promote safe use,
handling and disposal of asbestos;(c) raise con-cerns about asbestos problems and foster new waysof thinking among trade union members, manage-ment and the public by linking job security withoccupational and environmental health;(d) assistparticipants in identifying suspect asbestos andasbestos containing materials.
We found workers, including those who handleasbestos products regularly, to be very ignorant ofasbestos dangers; less than 20% of the participantswere somewhat aware or had seen some of therelevant information we have repeatedly publishedin both print and electronic media. In many cases,the workers’ expression was one of anger anddisgust when the magnitude of the occupationalhealth risks they have taken over time in theircareers became clear. But enthusiasm for and betterunderstanding of the subject matter quickly fol-lowed this; a willingness to take and effect requiredcorrective measured was something easily graspedby the workshop participants. Most importantlythe workers displayed a clear desire to use theinformation gathered at the workshops to put inplace occupationally healthy and secure work-places for future generations of workers, eventhough clearly the life-saving information mayhave come too late for them. ‘We are walkingdead because of asbestos but our children should

6 Editorial
not’, said many of the participants. The partici-pants’ support and favourable response to thisproject, has provided a natural lobby base for thenext phase of the programme, in which we shallpress the state to comply with and ratify all theILO conventions on asbestos, occupational safetyand health as well as other environmental standardsand convention.
7. A culture of occupational and environmentalhealth and safety
We thus believe that a culture that promotes theconcept of a safe workplace in developing coun-tries is achievable. However, the paucity of quan-titative data on the local impact of occupationalmalpractices on workers’ and environmental healthin developing countries makes the asbestos(andother pollution) problems appear deceivinglyminor than they possibly are. Without firm occu-pational health data it is difficult to convincinglydemonstrate the need and urgency for managingthe asbestos and other occupational safety andhealth problems. Advocates of the ban asbestosmovement or its safe use who are armed with justanecdotal evidence may easily be dismissed asmischievous and irrelevant to the ‘tough develop-ment struggle’. Further, new research approachesare needed because government-run reportingmechanisms may not be working well. Forinstance, in Jamaica, reporting of asbestos relateddiseases to the Ministry of Labour is mandatory.However, official ministry records show no caseof occupational asbestosis while at least two casesof locally contracted occupational asbestosis areknown (Reid and Kahwa, 1995). Refereed journalreports on the extent of the asbestos pollutionproblems in developing countries and their healtheffects are few; much more effort is required tobuild reliable data banks on occupational andenvironmental health and safety in developingcountries.
International agencies such as the ILO, theWorld Health Organization(WHO), the WorldBank, the United Nations Environment Programme(UNEP) and philanthropies can help enormouslyby assisting local organizations, NGOs and uni-versity researchers in developing countries to
obtain firm independent occupational health dataand use them to educate, mobilize and assistworkers and businesses to promote workplacesafety and health. This is one way the developingworld can be assisted to obtain, learn and usescientific information to transform national lifeand protect workers’ and environmental health.
8. Prevention and compensation
It can only be fair that the principle that ‘polluterpays’ be upheld, even if the polluter may havemigrated to other countries. It is therefore gratify-ing that the 7500 South African sufferers of asbes-tos related diseases successfully took their case toCape plc’s UK home base and got serious legalattention and recently obtained settlement, albeit asymbolic one (ACTSA, 2001). Encouraged bythese developments 450 asbestos related diseasesufferers in Swaziland have sought compensationfrom an asbestos mining international companythat left Swaziland in the early 1980s(Coakley,2000). In this regard, the globalization of theasbestos litigation industry(Global Attorney,2002) is a welcome development for sufferers ofasbestos-related diseases in developing countries,especially when offending multinational compa-nies, which are traceable to their home baseanywhere in the world, are involved. After all,global free trade and investment ought to comewith global responsibility!
It is plausible, that attorneys in small developingeconomies require mutual accommodation withmajor companies and governments for businesssurvival. Thus, local attorneys with entrenchedinterests in government and private sector busi-nesses might value such relationships more thanrepresentation of poor sufferers of asbestos-relateddiseases. Further, governments with poorly man-aged asbestos installations may have an interest innot vigorously pushing for promulgation, imple-mentation and enforcement of serious asbestosregulatory frameworks. For example, of the 175ILO member states, only 26 have ratified the ILOAsbestos Convention No. 162 and indeed only 37countries have ratified the Occupational Safety andHealth ILO Convention No. 155(OccupationalSafety and Health Convention, 1981) (ILO, Con-

7Editorial
ventions, 2002). This is further compounded by asimilar pattern of non-ratification, particularly indeveloping countries like Jamaica, of other inter-national standards, including the Basel Conventionon the Transboundary Movement of HazardousWaste and their Disposal(Basel Convention,1992) and the Rotterdam Conventions on PriorInformed Consent Procedure for Certain HazardousChemical and Pesticide in International Trade(Rotterdam Convention, 1998).
It would be interesting to establish why theseConventions have not been ratified by developingcountries and what would happen if they wereratified and implemented. In developed countriesthere are several mechanisms for the protection ofthe environment and worker heath, so the negativeimpact of unratified ILO conventions is less dra-matic because information is more readily availa-ble and meritorious justice can still be achievedthrough the courts. But in developing countrieswith emerging democratic and governance struc-tures it is the governments that workers and citi-zens can look to for protection from occupationaland environmental hazards. When government-runoperations are themselves hazardous and protectivelegislations are not promoted, citizens’ health islikely to be compromised. Ironically, ILO conven-tions offer a cost effective basis for occupationalsafety and health policy initiatives because poorcountries do not have to pay for the requisiteresearch. The requisite data are usually availablethrough ILO background studies and the ensuingtripartite (Trade Unions, Employers and Govern-ments) discussions, which lead to the adoption ofconvention proposals at annual InternationalLabour Conferences. Thus, ILO conventions notdebated and ratified by developing countries rep-resent a wasted critical opportunity for people inthese countries to learn safe occupational andenvironmental practices and use them to improvetheir well being. ILO Convention No. 162 has notbeen taken up by many developing countries; ILOshould seek to establish the social cost of thisindifference. Even more disappointing is the factthat organizations, like the ILO, do offer technicalassistance to those countries wishing to put theirhouses in order as well as effect administrativeand legislative changes to facilitate compliance
with these conventions. Often countries undertakethe initial approach in preliminary fact-findingconferences and workshops, but fail to sustaintheir efforts to the end to ensure ratification.
For all of these reasons, activities of experiencedaggressive international asbestos attorneys indeveloping countries are a welcome developmentat this time, even though they might regrettablybe a potential drain of funds from poor to richcountries. International litigation activities stand abetter chance of changing key institutional dynam-ics in the asbestos pollution issue and cultivatemore responsible occupational and environmentalhealth practices in developing countries. Govern-ments that fail to put in place protective regulationsfor workers and the public should also be targetedfor litigation. Ignorance should no longer be avalid excuse at that level, even though there maybe plenty of it.
9. Conclusion
Asbestos mining, processing and usage areincreasing in developing countries, yet the healthimpact of these activities remains obscure. Thisobscurity enables the pro-asbestos businesses tomount poorly challenged promotions(The Finan-cial Gazette, 2001; Ramaseshan, 1995) of asbestosuse while weakening the case for regulating asbes-tos usage. Epidemiological studies seeking toestablish reliably the health effects of asbestosmining, processing and usage in developing coun-tries are needed. It is results of such studies thatwill galvanize people and their institutions andinto making a persuasive case for legislativereforms that protect the environment and workersfrom asbestos and other pollutants. Internationalagencies and philanthropies can help greatly toassist people working under difficult and some-times risky conditions to get the essential epide-miological data and take the message of theirfindings to the people and galvanize them to takecorrective action.
Acknowledgments
We thank the Environmental Foundation ofJamaica for funding and the International Labour

8 Editorial
Organization (Workers’ Division and CaribbeanOffice) for technical support. We also thank Nor-bert Campbell(Ministry of Health), Robert Chung(Ministry Labour and Social Security), WayneSucklal (National Environment and PlanningAgency) and Milton Pinnock (Department ofCommunity Health and Psychiatry, UWI) for theirspirited contribution to the workplace workshopson asbestos.
References
Action for Southern Africa(ACTSA) Saturday December 21,2001. Victory for South African asbestos claimants. Avail-able from: http:yywww.actsa.orgyCapeycape_report.pdf,http:yywww.acta.orgynewsypress_releasey211201_cape.html.
Asbestos Institute. Available from: http:yywww.chrysotile.comyenychrysoyprodcons.html. This site provides updatefor the year 1999 in terms of regional aggregate cosump-tions. Previously data for 1994 were posted in country bycountry format and these data were used here; 1999.
Ban asbestos. In the main Ban Asbestos movement is led bythe International Ban Asbestos Secretariat, Ban AsbestosNetwork, the International Trade Union and EnvironmentalCommunities. These groups are largely active in developedcountries but activity in developing countries is picking up.2002.
Ban Asbestos Europe. Member countries are free to enforcebans before the 2005 target date. In fact bans have alreadybeen implemented in Denmark, Finland, Belgium, Austria,France, Germany, Italy, the Netherlands, Sweden and GreatBritain. 2002.
Becklake MR. Asbestos related diseases. In: Stellman JM,editor. Encyclopedia of occupational health and safety, vol.1, 4th ed. Geneva: International Labour Organization, 1998.(Chapter 10).
Basel Convention; 1992. Available from: http:yywww.basel.inty or http:yywww.unep.org.
Cauchon D. The asbestos epidemic—a global crisis. In: USATODAY 8–2–99. Available from: http:yywww.chem.unep.chypopsyPOPs_Incypress_releasesypressrel-99ypr03.htm.Discusses findings of a study done in 20 countries. Thereare also many Web reports of asbestos related diseases indeveloping countries. 1999.
Chemistry in Britain; 2001. Asbestos alert. Chemistry inBritain, News Review, November 2001, p. 8. Potential payout to asbestos victims worldwide is estimated at US$200billion.
Coakley GJ. The Mineral Industry of Swaziland. In: USgeological survey minerals yearbook, Ruston, VA: Depart-ment of the Interior, US Geological Survey; 2000. pp. 27.1–2.
De Stefani E, Kogevinas M, Boffetta P, Ronco A, Mendila-harsu M. Occupation and the risk of lung cancer in Uruguay.Scand J Work Environ Health 1996;22(5):346.
Global Attorney. Searching for ‘‘asbestos attorney’’ on theweb will turn out information on many attorneys litigatingasbestos cases in several countries. 2002.
Hazards Magazine, Issues 76(October–December 2001), pp.8–9.
IBAS. See numerous reports on the International Ban AsbestosSecretariat Website www.ibas.btinternet.co.uk; 2002.
ICFTUyTUAC Trade Union Advisory Committee to theOECD—‘‘Improving Health and Safety Management at theWorkplace: an important step towards sustainable develop-ment’’. (Presentation on behalf of workers and trade unionsat the XVI the World Congress on Safety and Health atWork—May 26–31, 2002 Vienna, Austria), ICFTU websi-te—www.icftu.org.
ILO. Safety in the use of asbestos: an ILO code of practice,International Labour Organization, Geneva; 1984.
ILO. Guidelines on occupational safety and health managementsystems, ILO-OSH 2001, Geneva: International LabourOrganization; 2001.
ILO Conventions—See list of countries that have ratified theILO conventions at http:yyilolex.ilo.ch:1567ycgi-lexyrat-ice.pl?C162 and 155. 2002.
Iran Daily Newspaper. Asbestos cement plants warned. IranDaily Newspaper August 14, 2001. Available from: http:yywww.irancement.comye-news.html.
Kanthak J, Jayaraman N. Ships for scraps: steel and toxicwaste for Asia. Hamburg, Germany: Greenpeace Germany2001; 33.
Kazan-Allen L. Indian asbestos industry fails to silence critics.Asbestos update. International Ban asbestos Secretariathttp:yywww.btinternet.comy;ibasylka_india_sil_crit.htm.2002.
Kielkowski D, Nelson G, Rees D. Risk of mesothelioma fromexposure to crocidolite asbestos: a 1995 update of a SouthAfrican mortality study. Occup Environ Med 2000;57:563–567.
Koorosh P. Abrupt appearance of mesothelioma after usingacrylic. In: American industrial hygiene association 2001Abstracts, Case Study 403. Available from: http:yywww.aiha.orgyabs01y01ycs3.html.
Madava T. Health versus economy: the asbestos debate inSouthern Africa. Southern African News Features, a SARDCService, 15 September 1999. http:yywww.sardc.netyeditori-alysanfy1999y09y15-09-1999-nf1.htm.
Mitchev K. In a presentation to the 11th Annual Congress ofthe European Respiratory Society(ERS), Berlin 24th Sep-tember 2001, Special session entitled: A time bomb in thelungs: the ravages of asbestos. Press release at: http:yywww.ersnet.orgy4y3y4_3_5_1.asp.
Ramaseshan VK. India launches successful asbestos promotioncampaign. Available from: http:yywshiivx.med.uoeh-u.ac.jpyasbestosyindia.htlml. Author is Chairman, AsbestosInformation Centre(India). See also related story at the

9Editorial
Asbestos Institute Website: http:yywww.asbestos-insti-tute.cayindia.html. 1995.
Reid HO, Kahwa IA. Potential asbestos problems in Jamaica.Occup Environ Med 1995;52:241.
Rotterdam Convention, 1998. Available from: http:yywww.pic.inty http:yywww.fao.org or http:yywww.agrifoods_forums.net.
Sun T, Shin A, Zhang X, et al. Survey on the mortality ofmalignant tumors in female workers with manual spinningof asbestos. China Occup Med 2001;28(4). Available from:http:yywww.gdpcc.comyjournalyjournal(E)_28(4).htm.
Asbestos manufacturer carries on regardless. The SundayTimes (Sri Lanka) News Section, July 16, 2000. Availablefrom: http:yywww.lacnet.orgysuntimesy000716ynewsm.html.
The Financial Gazette, Zimbabwe(2001), ‘‘Task force makesHeadway against anti-asbestos lobby.’’ Staff Reporter, theFinancial Gazette, Zimbabwe 7y12y22001. Available from:http:yywww.fingaz.co.zwyfingazy2001yjulyyjuly12y2245.shml.
The Zimbabwe Independent(2002). Staff Writer. ZCTU onasbestos. Friday 21, June 2002. http:yywww.theindependent.co.zwynewsy2002yJuneyFriday21y472.html.
US Environmental Protection Agency. Asbestos, AsbestosWorker Protection: Federal Register. 2000;65(221), Novem-ber 15, p. 69209–17.
Virta RL. Asbestos. In: US Geological survey, minerals com-modity summary, Ruston, VA: Department of the Interior,US Geological Survey, January 2002: 26–7.
Weekend Observer 2002. Reported in the Weekend Observer(Jamaica) (Friday, July 5, 2002, Page 31). The report
indicated that testing found unsafe levels of asbestos at afederal demolition site in the US Virgin Islands. Investiga-tion is being conducted to determine whether the siteviolated regulations for safe disposal of the substance.
Wen CP, Luo S, Liu X, Tsai, SP. Asbestos-related diseasesfrom environmental exposure to crocidolite in Da-Yao,China I: review of epidemiological and cohort data. TheUnited States Environmental Protection Agency, 2001Asbestos Health Effects Conference, May 24–5, 2001,Oakland California. Available from: http:yywww.epa.govyswemmsyahecyabstractsywen1.pdf.
Wen CP, Luo S, Liu X, Tsai SP, Wang, JT. Asbestos-relateddiseases from environmental exposure to crocidolite in Da-Yao, China II: a case-control study of mesothelioma. TheUnited States Environmental Protection Agency, 2001Asbestos Health Effects Conference, May 24–5, 2001,Oakland California. Available from: http:yywww.epa.govyswerrimsyahecysummaryyabstractsywen2.pdf.
Workers Online 2001: Asbestos Protest. Workers on Line:News:2001 Issue 88: Activist Notebook page 1, March 16,2001. Available from: http:yyworkers.labor.net.auy88ynews9_activist.html.
The Guest Editors:Lilieth V. Harris
Jamaica Confederation of Trade Unions,1a Hope Boulevard, Kingston 6, Jamaica, West Indies
E-mail address: [email protected] A. Kahwa
Chemistry Department, University of the West Indies,Mona Campus, Kingston 7, Jamaica, West Indies