Embed Size (px)
Citation preview

J Oral Maxillofac Surg
43:163-172. 1985
Artifacts in Oral Biopsy Specimens
JOSEPH E. MARGARONE, DDS,* JOSEPH R. NATIELLA, DDS,t AND CAROLE D. VAUGHAN, HT(ASCP)t
The problem of artifacts introduced into biopsies of oral tissue are dis- cussed. The different types of artifacts are described and illustrated, and suggestions for prevention are given.
The importance of the proper handling of biopsy specimens cannot be over-emphasized. Specimens removed from the oral cavity are often small, and the possibility of producing artifact is thus en- hanced. It must be understood that routine histo- technical procedures used in processing tissues also result in alteration of normal morphologic and cy- tologic features. In addition, there are other circum- stances that result in artifact. These include errors by the surgeon or assistant in handling the tissue at the time of biopsy, problems in the transport of tissue to the laboratory, and faulty tissue pro- cessing.
In 1978 Zegarelli’ published an article dealing with common problems in biopsy procedure. It is surprising that few additional studies have appeared on the subject. The purpose of this report is to il- lustrate some of the important artifacts in tissue specimens, especially those that prevent accurate diagnosis, and to suggest some techniques for al- leviating these problems.
Materials and Methods
Representative cases were selected from the bi- opsy files of the Oral Pathology Department at the State University of New York at Buffalo. Photo- micrographs were taken of paraffin-embedded spec- imens, sectioned at 6 km and stained with hema- toxylin and eosin, that showed specific artifacts. In addition, the right and left buccal mucosa of four Macaca nemestrina monkeys were used as sites for surgical methods that were predicted to produce tissue artifact. After an elliptical incision measuring
Received from The State University of New York at Buffalo School of Dentistry, Buffalo, New York.
* Clinical Associate Professor and Chairman, Department of Oral and Maxillofacial Surgery.
t Professor, Department of Oral Pathology. $ Technical Specialist, Department of Oral Pathology. Address correspondence and reprint requests to Dr. Marga-
rone: 408 Woodward Cresent. West Seneca, NY 14224.
163
3.0 x 0.5 cm was made in the mucosa, biopsies were taken sequentially from the tissue, with each specimen being subjected to either mechanical, chemical, or thermal alteration during removal. Me- chanical alteration and damage of specimens was produced with the instruments that are commonly used by practitioners for biopsy procedures; namely, the Kelly hemostat and mosquito hemostat, Adson forceps with and without teeth, atraumatic forceps, and the Allis clamp. Injection of large amounts of local anesthetic (lidocaine 2% with epi- nephrine 1: 100,000) into the biopsy area was also studied. Electrocautery, using both coagulation and cutting electrodes, was used to produce thermal damage. Finally, the last specimens were subjected to liberal application of Betadine solution (Perdue Frederick Co., Norwalk, Conn.) as a preoperative preparation.
Biopsy specimens were immediately fixed in 10% neutral buffered formalin. Other segments of normal, untreated buccal mucosa were sources of excisional biopsies that were subjected to the fol- lowing conditions: delay in fixation for 30 minutes; fixation in water for 24 hours; fixation in 70% and absolute alcohol; freezing for 24 hours; washing after biopsy with immediate fixation in 10% neutral buffered formalin; no washing after biopsy with im- mediate fixation in 10% neutral buffered formalin.
Results
Significant alterations were noted in both the clin- ical and experimental material. However, Betadine scrub and washing and nonwashing prior to fixation produced no recognizable changes in the speci- mens.
Forceps Artifacts
When the teeth of the instrument penetrated the specimen, it resulted in voids or tears and com- pression of the surrounding tissue (Fig. 1). The sur-

164 TISSUE ARTIFACTS
FIGURE 1. Artifact created by excessive force with tissue for- ceps. The teeth of the instrument have created three voids within the connective tissue (arrows). In addition, the surrounding stroma is compressed, making exact in- terpretation difficult (human, he- matoxylin and eosin, magnifica- tion x25).
FIGURE 2. Squeeze artifact that has produced “microcysts” resulting from mechanical pene- tration of surface epithelium (ar- rows). An accurate assessment of epithelial pathology would be im- possible (human, hematoxylin and eosin, magnification x 25).
FIGURE 3. This tissue has been grasped with a hemostat. The dis- tortion that results to the epithe- lium surfacing this specimen makes accurate sectioning vir- tually impossible. The epitheiium appears hyperplastic, but this is an artifact of the plane of sec- tioning (human, hematoxylin and eosin, magnification x 40).
MARGARONE ET AL 165
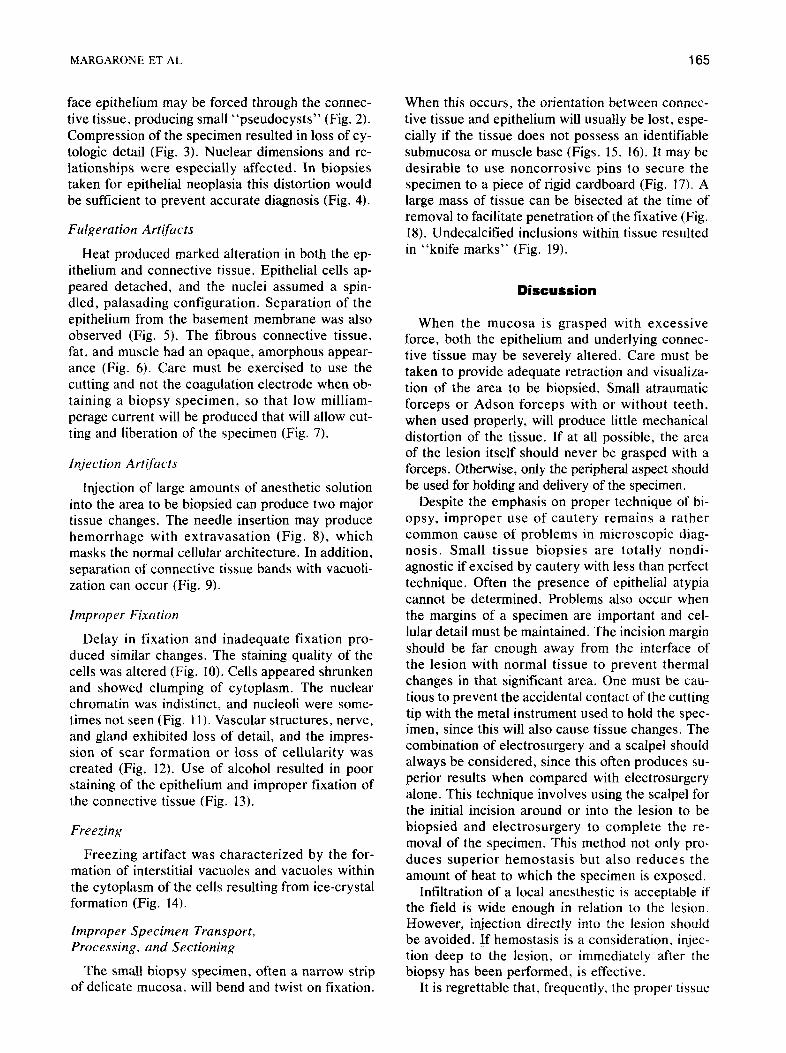
face epithelium may be forced through the connec- tive tissue, producing small “pseudocysts” (Fig. 2). Compression of the specimen resulted in loss of cy- tologic detail (Fig. 3). Nuclear dimensions and re- lationships were especially affected. In biopsies taken for epithelial neoplasia this distortion would be sufficient to prevent accurate diagnosis (Fig. 4).
Fulgerution Artifacts
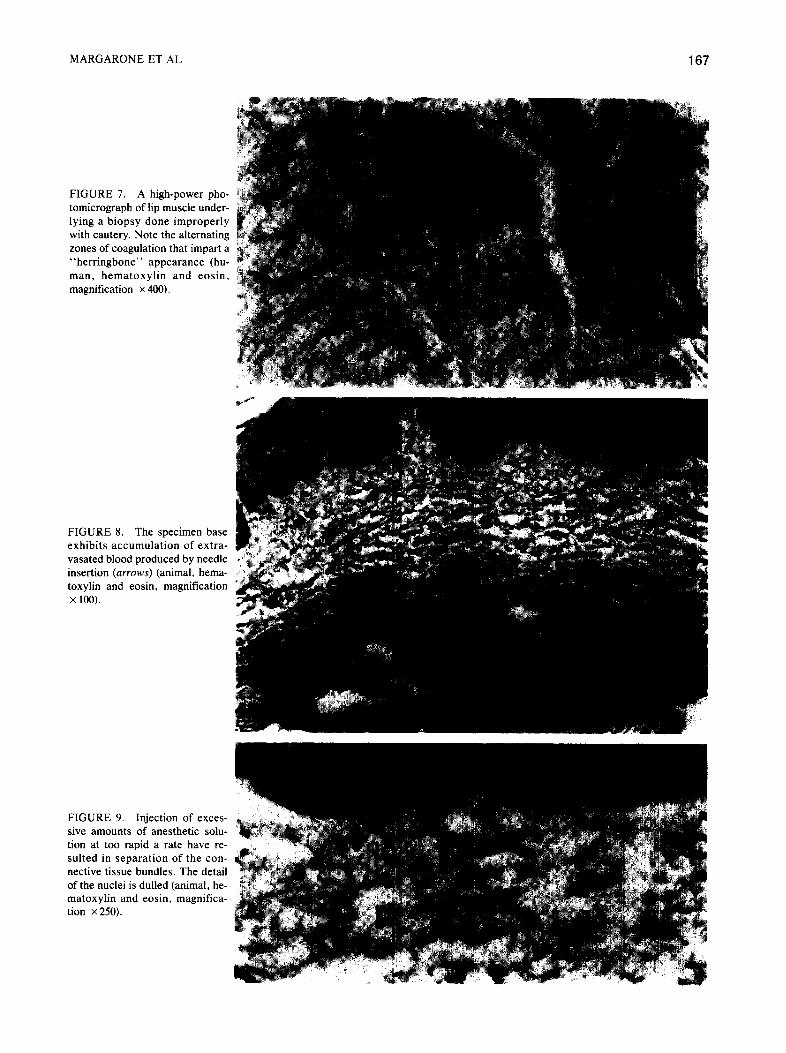
Heat produced marked alteration in both the ep- ithelium and connective tissue. Epithelial cells ap- peared detached, and the nuclei assumed a spin- dled, palasading configuration. Separation of the epithelium from the basement membrane was also observed (Fig. 5). The fibrous connective tissue, fat, and muscle had an opaque, amorphous appear- ance (Fig. 6). Care must be exercised to use the cutting and not the coagulation electrode when ob- taining a biopsy specimen, so that low milliam- perage current will be produced that will allow cut- ting and liberation of the specimen (Fig. 7).
fnjection Artifacts
Injection of large amounts of anesthetic solution into the area to be biopsied can produce two major tissue changes. The needle insertion may produce hemorrhage with extravasation (Fig. S), which masks the normal cellular architecture. In addition, separation of connective tissue bands with vacuoli- zation can occur (Fig. 9).
Improper Fixation
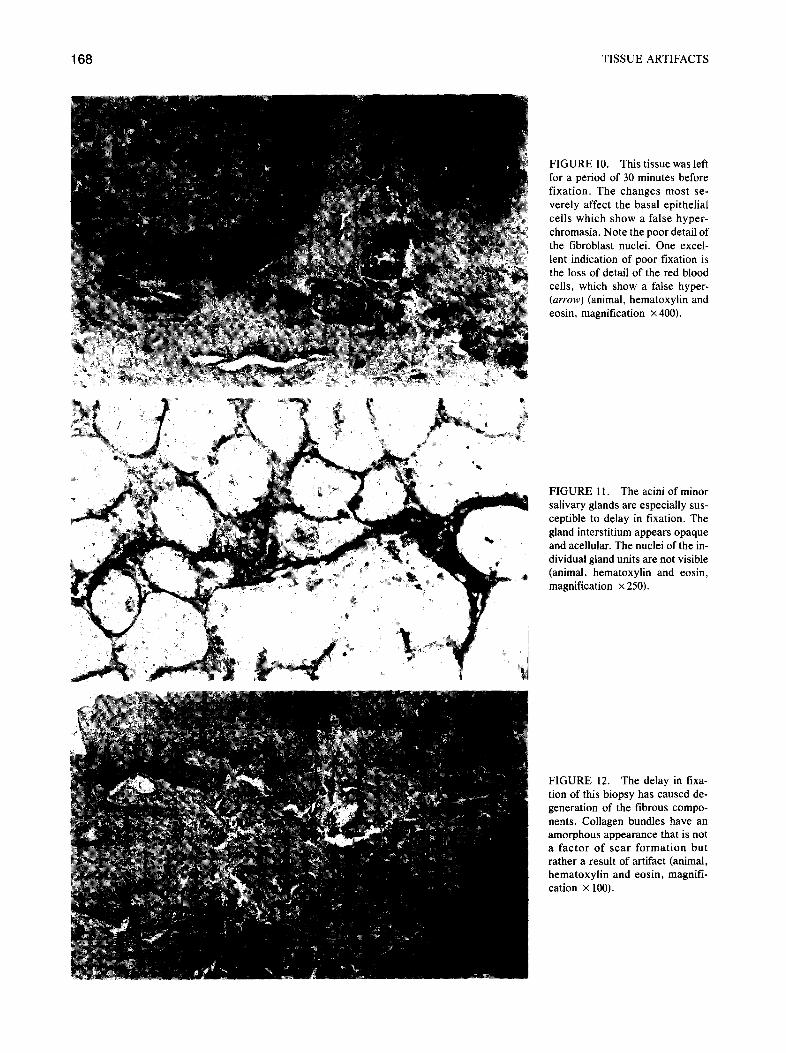
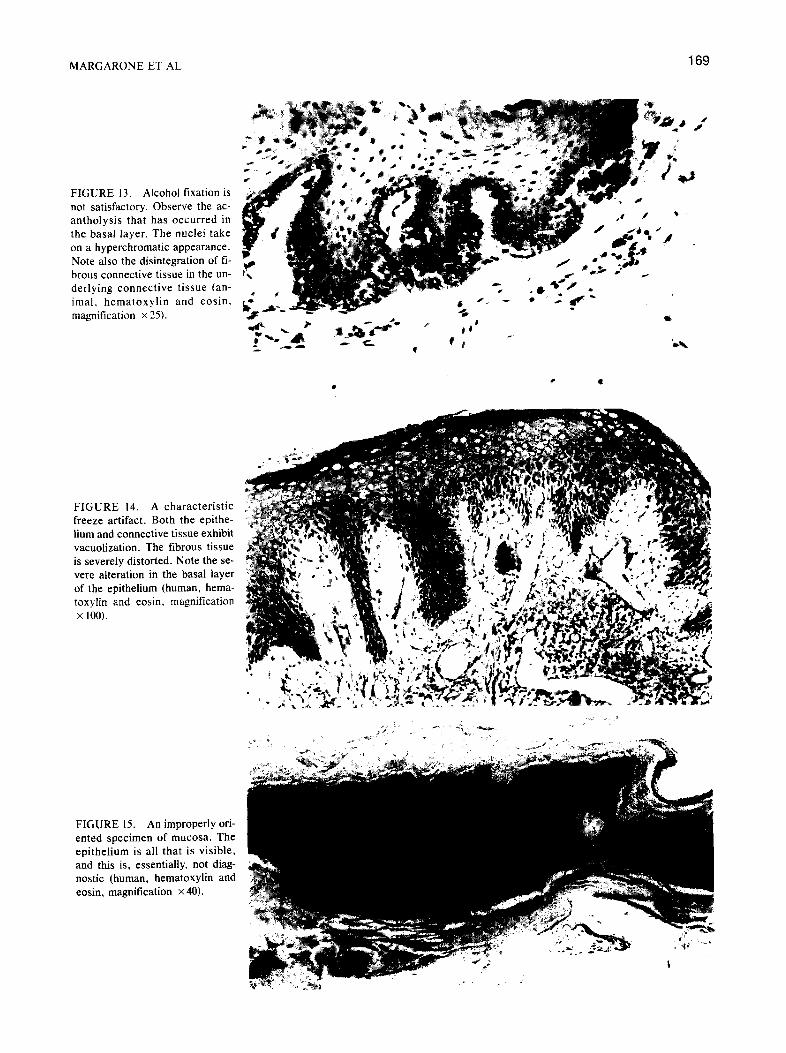
Delay in fixation and inadequate fixation pro- duced similar changes. The staining quality of the cells was altered (Fig. 10). Cells appeared shrunken and showed clumping of cytoplasm. The nuclear chromatin was indistinct, and nucleoli were some- times not seen (Fig. 11). Vascular structures, nerve, and gland exhibited loss of detail, and the impres- sion of scar formation or loss of cellularity was created (Fig. 12). Use of alcohol resulted in poor staining of the epithelium and improper fixation of the connective tissue (Fig. 13).
Freezing
Freezing artifact was characterized by the for- mation of interstitial vacuoles and vacuoles within the cytoplasm of the cells resulting from ice-crystal formation (Fig. 14).
Improper Specimen Transport, Processing. and Sectioning
The small biopsy specimen, often a narrow strip of delicate mucosa, will bend and twist on fixation.
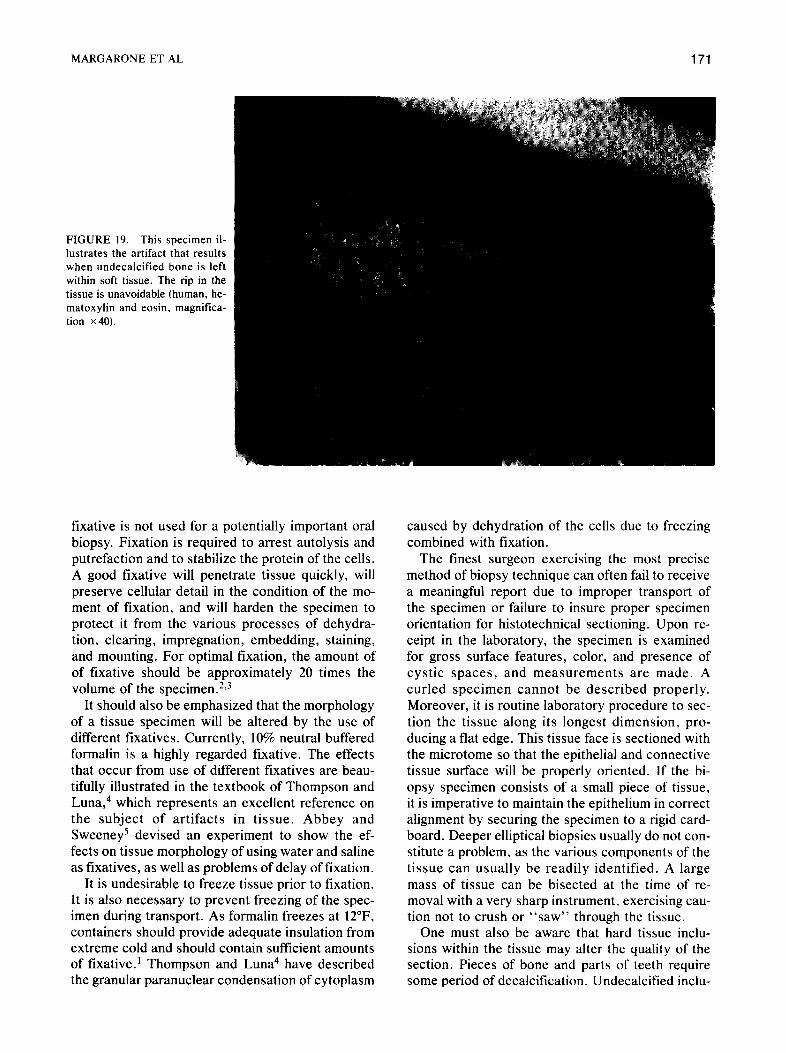
When this occurs, the orientation between connec- tive tissue and epithelium will usually be lost, espe- cially if the tissue does not possess an identifiable submucosa or muscle base (Figs. 15. 16). It may be desirable to use noncorrosive pins to secure the specimen to a piece of rigid cardboard (Fig. 17). A large mass of tissue can be bisected at the time of removal to facilitate penetration of the fixative (Fig. 18). Undecalcified inclusions within tissue resulted in “knife marks” (Fig. 19).
Discussion
When the mucosa is grasped with excessive force, both the epithelium and underlying connec- tive tissue may be severely altered. Care must be taken to provide adequate retraction and visualiza- tion of the area to be biopsied. Small atraumatic forceps or Adson forceps with or without teeth, when used properly, will produce little mechanical distortion of the tissue. If at all possible, the area of the lesion itself should never be grasped with a forceps. Otherwise, only the peripheral aspect should be used for holding and delivery of the specimen.
Despite the emphasis on proper technique of bi- opsy, improper use of cautery remains a rather common cause of problems in microscopic diag- nosis. Small tissue biopsies are totally nondi- agnostic if excised by cautery with less than perfect technique. Often the presence of epithelial atypia cannot be determined. Problems also occur when the margins of a specimen are important and cel- lular detail must be maintained. The incision margin should be far enough away from the interface of the lesion with normal tissue to prevent thermal changes in that significant area. One must be cau- tious to prevent the accidental contact of the cutting tip with the metal instrument used to hold the spec- imen, since this will also cause tissue changes. The combination of electrosurgery and a scalpel should always be considered, since this often produces su- perior results when compared with electrosurgery alone. This technique involves using the scalpel for the initial incision around or into the lesion to be biopsied and electrosurgery to complete the re- moval of the specimen. This method not only pro- duces superior hemostasis but also reduces the amount of heat to which the specimen is exposed.
Infiltration of a local anesthestic is acceptable if the field is wide enough in relation to the lesion. However, injection directly into the lesion should be avoided. If hemostasis is a consideration, injec- tion deep to the lesion, or immediately after the biopsy has been performed, is effective.
It is regrettable that, frequently, the proper tissue
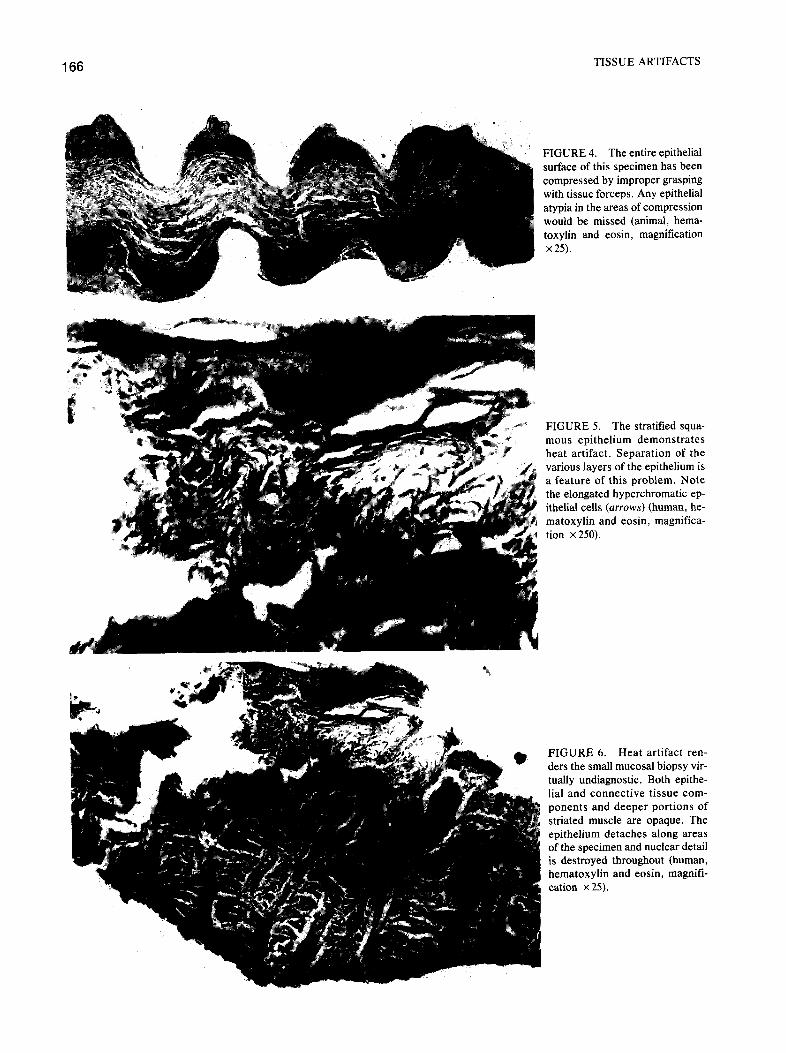
FIGURE 4. The entire epithelial surface of this specimen has been compressed by improper grasping with tissue forceps. Any epithelial atypia in the areas of compression would be missed (animal, hema- toxylin and eosin, magnification
TISSUE ARTIFACTS
FIGURE 5. The stratified squa- mous epithelium demonstrates heat artifact. Separation of the various layers of the epithelium is a feature of this problem. Note the elongated hyperchromatic ep- ithelial cells (arrows) (human, he- matoxylin and eosin, magnifica- tion x 250).
FIGURE 6. Heat artifact ren- ders the small mucosal biopsy vir- tually undiagnostic. Both epithe- ha1 and connective tissue com- ponents and deeper portions of striated muscle are opaque. The epithelium detaches along areas of the specimen and nuclear detail is destroyed throughout (human, hematoxylin and eosin, magnifi- cation X 25).
MARGARONE ET AL 167
FIGURE 7. A high-power pho- tomicrograph of lip muscle under- lying a biopsy done improperly with cautery. Note the alternating zones of coagulation that impart a “herringbone” appearance (hu- man, hematoxylin and eosin. magnification X 400).
FIGURE 8. The specimen base exhibits accumulation of extra- vasated blood produced by needle insertion (arrows) (animal, hema- toxylin and eosin. magnification x 100).
FIGURE 9. Injection of exces- sive amounts of anesthetic solu- tion at too rapid a rate have re- sulted in separation of the con- nective tissue bundles. The detail of the nuclei is dulled (animal, he- matoxylin and eosin, magnifica- tion x 250).
TISSUE ARTIFACTS
FIGURE 10. This tissue was left for a period of 30 minutes before fixation. The changes most se- verely affect the basal epithelial cells which show a false hyper- chromasia. Note the poor detail of the fibroblast nuclei. One excel- lent indication of poor fixation is the loss of detail of the red blood cells, which show a false hyper- (arrow) (animal, hematoxylin and eosin, magnification X 400).
FIGURE 11. The acini of minor salivary glands are especially sus- ceptible to delay in fixation. The gland interstitium appears opaque and acellular. The nuclei of the in- dividual gland units are not visible (animal, hematoxylin and eosin, magnification X 250).
FIGURE 12. The delay in lixa- tion of this biopsy has caused de- generation of the fibrous compo- nents. Collagen bundles have an amorphous appearance that is not a factor of scar formation but rather a result of artifact (animal, hematoxylin and eosin, magnifi- cation X 100).
MARGARONE ET AL 169
FIGURE 13. Alcohol fixation is not satisfactory. Observe the ac- antholysis that has occurred in the basal layer. The nuclei take on a hyperchromatic appearance. Note also the disintegration of fi- brous connective tissue in the un- derlying connective tissue (an- imal, hematoxylin and eosin, magnification X 35).
FIGURE 14. A characteristic freeze artifact. Both the epithe- lium and connective tissue exhibit vacuolization. The fibrous tissue is severely distorted. Note the se- vere alteration in the basal layer of the epithelium (human, hema- toxylin and eosin, magnification x 100).
.
FIGURE 15. An improperly ori- ented specimen of mucosa. The epithelium is all that is visible, and this is, essentially, not diag- nostic (human, hematoxylin and eosin, magnification X 40).

TISSUE ARTIFACTS
FIGURE 16. This is the same specimen illustrated in Figure 15. It has been properly embedded and sectioned. Note that the epi- thelial thickness can now be ac- curately assessed (human, hema- toxylin and eosin, magnification x40).
FIGURE 17. This is a biopsy that measured 3.5 mm. It was pinned so that the narrow strip did not rotate on itself. Embedding was accurate despite the size (human, hematoxylin and eosin, magnification x 40).
FIGURE 18. This biopsy of a mucocele was sectioned at the time of removal to allow adequate fixation and subsequent proper orientation for sectioning. Even the mucous remains intact and all elements of the mucosa are readily identified (human, hema- toxylin and eosin, magnification x 10).
MARGARONE ET AL
FIGURE 19. This specimen il- lustrates the artifact that results when undecalcified bone is left within soft tissue. The rip in the tissue is unavoidable (human, he- matoxylin and eosin, magnifica- tion X40).
fixative is not used for a potentially important oral biopsy. Fixation is required to arrest autolysis and putrefaction and to stabilize the protein of the cells. A good fixative will penetrate tissue quickly, will preserve cellular detail in the condition of the mo- ment of fixation, and will harden the specimen to protect it from the various processes of dehydra- tion, clearing, impregnation, embedding, staining, and mounting. For optimal fixation, the amount of of fixative should be approximately 20 times the volume of the specimen.2,3
It should also be emphasized that the morphology of a tissue specimen will be altered by the use of different fixatives. Currently, 10% neutral buffered formalin is a highly regarded fixative. The effects that occur from use of different fixatives are beau- tifully illustrated in the textbook of Thompson and Luna,4 which represents an excellent reference on the subject of artifacts in tissue. Abbey and Sweeney’ devised an experiment to show the ef- fects on tissue morphology of using water and saline as fixatives, as well as problems of delay of fixation.
It is undesirable to freeze tissue prior to fixation. It is also necessary to prevent freezing of the spec- imen during transport. As formalin freezes at 12”F, containers should provide adequate insulation from extreme cold and should contain sufficient amounts of fixative.’ Thompson and Luna4 have described the granular paranuclear condensation of cytoplasm
caused by dehydration of the cells due to freezing combined with fixation.
The finest surgeon exercising the most precise method of biopsy technique can often fail to receive a meaningful report due to improper transport of the specimen or failure to insure proper specimen orientation for histotechnical sectioning. Upon re- ceipt in the laboratory, the specimen is examined for gross surface features, color, and presence of cystic spaces, and measurements are made. A curled specimen cannot be described properly. Moreover, it is routine laboratory procedure to sec- tion the tissue along its longest dimension, pro- ducing a flat edge. This tissue face is sectioned with the microtome so that the epithelial and connective tissue surface will be properly oriented. If the bi- opsy specimen consists of a small piece of tissue, it is imperative to maintain the epithelium in correct alignment by securing the specimen to a rigid card- board. Deeper elliptical biopsies usually do not con- stitute a problem, as the various components of the tissue can usually be readily identified. A large mass of tissue can be bisected at the time of re- moval with a very sharp instrument, exercising cau- tion not to crush or “saw” through the tissue.
One must also be aware that hard tissue inclu- sions within the tissue may alter the quality of the section. Pieces of bone and parts of teeth require some period of decalcification. Undecalcified inclu-

172 TISSUE ARTIFACTS
sions within tissue can result in tears and rips, which may cause problems in proper interpretation. Indication of the possibility of calcification in a soft tissue mass should therefore be made on the biopsy slip that accompanies the specimen.
Summary
More than proper surgical technique is required to facilitate the proper diagnosis of an oral biopsy specimen. The proper preparation of the tissue for microscopic analysis depends on steps taken by the surgeon, assistant, and histotechnician to reduce the inclusion of artifacts. There are many ways that the exact interpretation of tissue specimens can be
compromised. Unfortunately, many practitioners seem to be unaware of the extent of this problem, as well as how easily artifacts can be prevented.
References
1. Zegarelli D: Common problems in biopsy procedure. J Oral Surg 36644, 1978
2. Lynch MJ, Raphael SS, Mellor LD, et al: Medical Labora- tory Technology and Clinical Pathology, 2nd ed. Phila- delphia, WB Saunders, 1969
3. Sheehan DC, Hrapchak BB: Theory and Practice of Histo- technology, 2nd ed. St. Louis, CV Mosby, 1980
4. Thompson SW, Luna LG: An Atlas of Artifacts Encountered in the Preparation of Microscopic Tissue Sections. Springfield, Charles C Thomas, 1978
5. Abbey L, Sweeney T: Fixation artifacts in oral biopsy spec- imens. VA Dent J 49:31, 1972





























